Phys · haematological
Multiple Myeloma
Also known as myeloma · multiple myeloma · plasma cell myeloma · Kahler disease · medullary plasmacytoma · monoclonal gammopathy
Consultant-physician-depth guide to multiple myeloma for FRACP DWE and DCE — IMWG diagnostic criteria, the CRAB and biomarker myeloma-defining events, MGUS versus smouldering versus active disease, cast nephropathy and the myeloma-defining free-light-chain ratio, R-ISS staging, transplant-eligible VRd induction with autologous transplant and lenalidomide maintenance, transplant-ineligible daratumumab-based regimens, proteasome inhibitors and anti-CD38 therapy, and supportive care including bisphosphonates and cord-compression emergencies.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Multiple Myeloma
The answer first
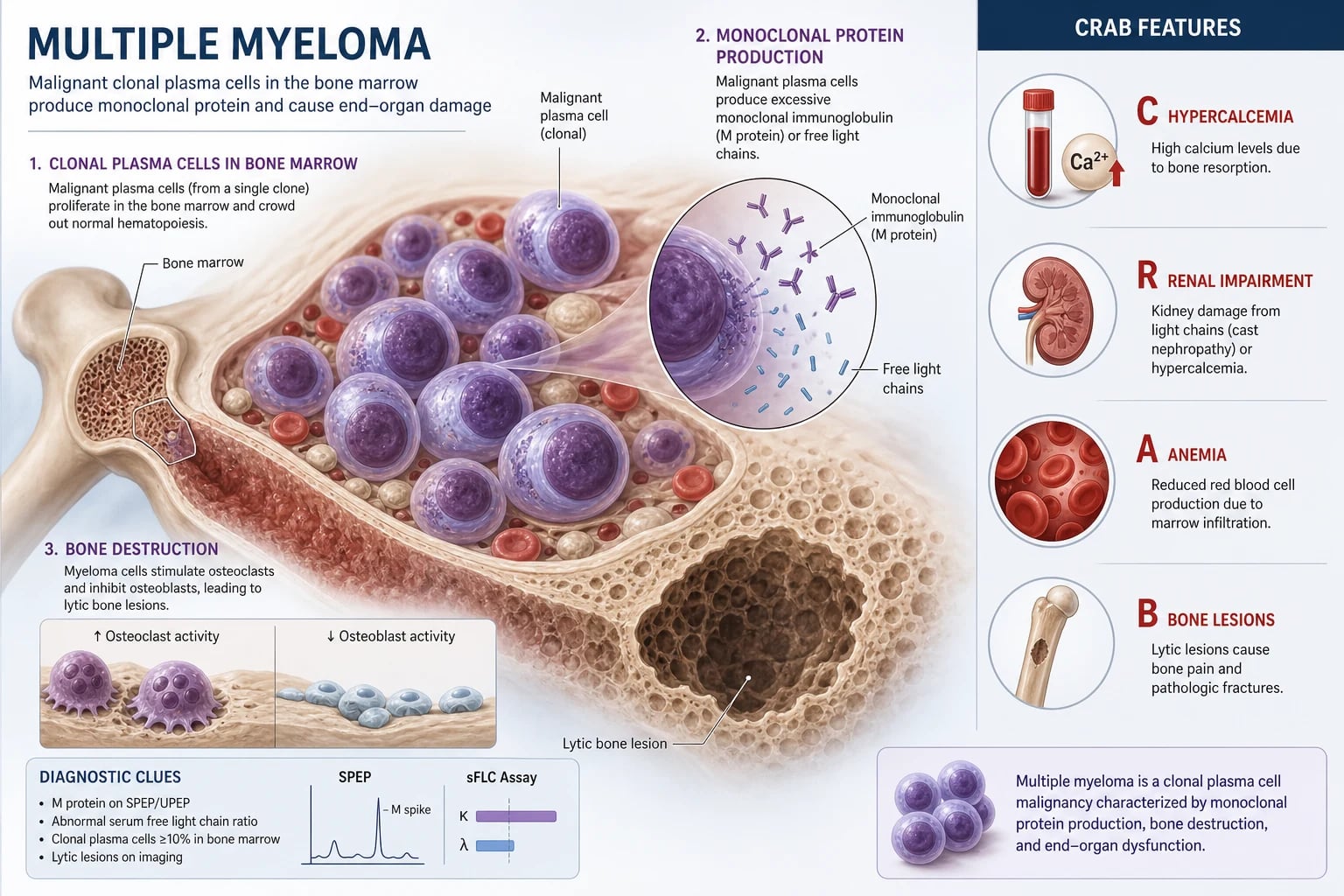
Multiple myeloma is a clonal expansion of malignant plasma cells in the bone marrow that produces a monoclonal immunoglobulin (the paraprotein or M-protein) and causes end-organ damage. The diagnosis rests on the International Myeloma Working Group (IMWG) 2014 criteria: clonal bone marrow plasma cells at or above 10 per cent (or a biopsy-proven plasmacytoma), plus one or more myeloma-defining events [1]. Those events are the CRAB features (hyperCalcaemia, Renal impairment, Anaemia, Bone lesions) and the three biomarkers that allow treatment before end-organ damage — marrow plasma cells at or above 60 per cent, an involved-to-uninvolved serum free light chain ratio at or above 100, or more than one focal lesion on MRI.
Three rules that change outcome: [1]
- Send serum free light chains and serum electrophoresis on every older patient with unexplained back pain, anaemia, renal impairment or hypercalcaemia. Cast nephropathy is reversible if caught early; the best predictor of renal recovery is a falling free light chain with prompt treatment. The ESR is characteristically very high (often over 100); a normal ESR does not exclude myeloma because some patients are hypogammaglobulinaemic.
- Acute back pain with neurological signs in myeloma is malignant epidural spinal cord compression — urgent MRI whole spine and dexamethasone now. Do not wait for plain films or CT. This is an oncological emergency that can leave a patient paraplegic within hours.
- Hypercalcaemia of myeloma responds to bisphosphonates, not just fluids. Give aggressive intravenous hydration, then zoledronic acid 4 mg intravenously (or denosumab if renal failure precludes a bisphosphonate). Calcitonin works within hours for the symptomatic patient while the bisphosphonate takes 48 to 72 hours. [1]
For a transplant-eligible patient (broadly under 70 with good performance status and no major comorbidity) the modern standard is bortezomib-lenalidomide-dexamethasone (VRd) induction, then high-dose melphalan with autologous stem cell transplant, then lenalidomide maintenance [4][5][7]. For the transplant-ineligible patient the standard is now a daratumumab-based triplet such as daratumumab-lenalidomide-dexamethasone (DRd), which improves both progression-free and overall survival over lenalidomide-dexamethasone [8].
Myeloma is treatable but, in nearly all patients, not yet curable. Median overall survival has improved from about 3 years in the melphalan-prednisone era to over 8 to 10 years with modern combinations, autologous transplant and maintenance — and the trajectory continues to improve with anti-CD38 antibodies, CAR-T cell therapy and bispecific antibodies entering earlier lines. [1]
Classification — MGUS, smouldering and active myeloma
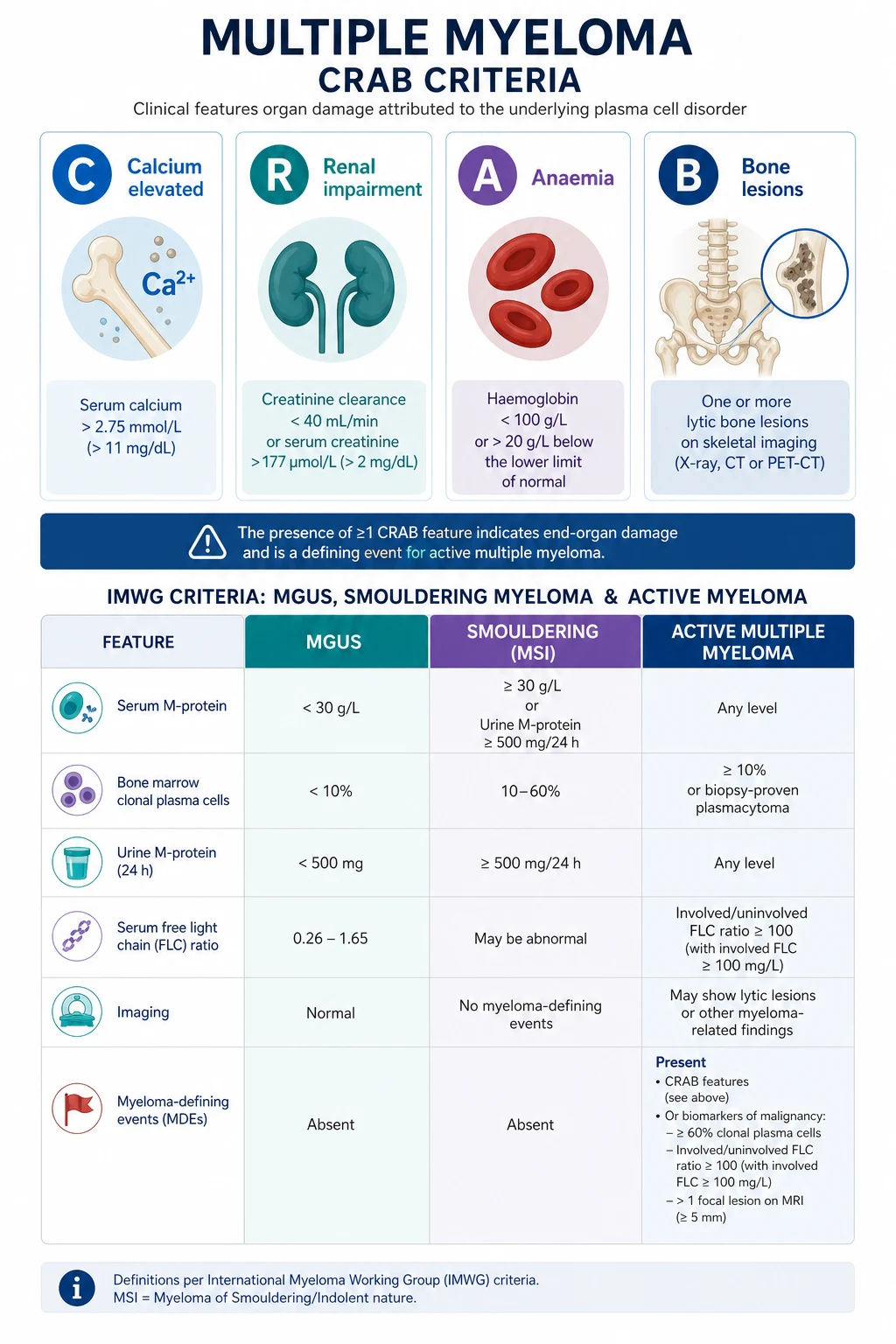
The plasma cell disorders form a spectrum from a benign incidental finding (MGUS) through an asymptomatic intermediate (smouldering myeloma) to symptomatic disease requiring treatment. The IMWG criteria give precise, examinable thresholds [1].
| Disorder | Clonal marrow plasma cells | Monoclonal protein | End-organ damage (CRAB) | Action |
|---|---|---|---|---|
| MGUS | Under 10 per cent | Serum M-protein under 30 g/L (and urinary under 500 mg/24h); free light chain ratio normal | Absent | Observe; risk-stratify by the IMWG 3-factor model |
| Smouldering myeloma | At least 10 per cent (or 60 per cent or more — see below) | Serum M-protein 30 g/L or more, or urinary monoclonal protein 500 mg or more per 24 hours, or abnormal free light chain ratio (under 0.26 or over 1.65) | Absent | Observe closely; patients with high-risk features are trial candidates for early treatment |
| Multiple myeloma | At least 10 per cent (or biopsy-proven plasmacytoma) | Any | Present — any CRAB feature attributable to the plasma cell disorder, or any one of the three biomarkers | Treat |
DWE high-yield: The CRAB criteria are specific thresholds, not vague concepts — calcium over 2.75 mmol/L (corrected), creatinine clearance under 40 mL/min or serum creatinine over 177 micromol/L, haemoglobin more than 20 g/L below the lower limit of normal or under 100 g/L, and one or more lytic bone lesions on imaging. The 2014 update added the three biomarkers because patients with these markers progress to CRAB within a median of under 2 years and treating earlier prevents irreversible organ damage. [1]
The three biomarker myeloma-defining events (the 2014 update)
- Clonal bone marrow plasma cells at or above 60 per cent. The single strongest predictor of imminent progression — about 95 per cent of these patients progress within 2 years.
- Serum involved-to-uninvolved free light chain ratio at or above 100, provided the involved (clonal) free light chain level is at least 100 mg/L. A kappa-to-lambda ratio of 100 (or its inverse) is highly specific for a clonal process and predicts renal cast formation.
- More than one focal lesion on MRI (or PET-CT). A focal lesion represents a nest of clonal plasma cells; more than one predicts imminent CRAB events. [1]
Examiner trap: A patient with 65 per cent marrow plasma cells and a small paraprotein but no CRAB features still has multiple myeloma requiring treatment under the IMWG 2014 criteria. Older candidates often answer "smouldering, observe" — this is wrong. The biomarker rule supersedes the absence of end-organ damage. [1]
MGUS risk stratification — who progresses
The long-term Mayo Clinic cohort established that MGUS carries an absolute progression risk of about 1 per cent per year, persisting for decades [9]. The risk is stratified by three factors — the IMWG risk model:
- M-protein size at least 15 g/L (1.5 g/dL)
- Non-IgG isotype (IgA or IgM)
- Abnormal serum free light chain ratio (under 0.26 or over 1.65) [1]
Low risk (none of these) carries about a 5 per cent lifetime progression; high risk (all three) about a 60 per cent risk at 20 years. The clinical implication is surveillance — a low-risk MGUS needs only annual bloods for life; a high-risk MGUS should be seen in a haematology clinic with closer monitoring for evolution into smouldering or active disease. [1]
Pathophysiology
Clonal plasma cell expansion
Myeloma arises from a post-germinal-centre B cell that has undergone somatic hypermutation and class switch recombination and then homes back to the bone marrow as a long-lived plasma cell. The malignant clone accumulates in the marrow, secretes a monoclonal immunoglobulin (IgG in about half, IgA in a fifth, light-chain-only in a fifth, with IgD, IgM and IgE rare), and crowds out normal haematopoiesis. The non-clonal immunoglobulins fall — hence hypogammaglobulinaemia and the characteristic susceptibility to encapsulated bacterial infections. [1]
Primary cytogenetic lesions divide myeloma into hyperdiploid (chromosomes 3, 5, 7, 9, 11, 15, 19, 21 — generally better prognosis) and non-hyperdiploid, the latter driven by IgH translocations involving chromosome 14q32. Three translocations are high-risk adverse: t(4;14) (FGFR3-MMSET), t(14;16) (c-MAF) and t(14;20) (MAFB). Deletion 17p (loss of the TP53 locus) is the most adverse lesion of all, associated with early relapse, extramedullary disease and poor survival. Gain of 1q (1q21 amplification) is also adverse. These lesions are detected by FISH on CD138-selected plasma cells and are now mandatory at diagnosis because they drive treatment intensity. [1]
The bone marrow microenvironment — RANKL and osteoblast inhibition
Lytic bone disease is the hallmark of myeloma and reflects a profound uncoupling of bone remodelling: [1]
- Osteoclast activation: Myeloma cells stimulate osteoclasts by upregulating RANKL (receptor activator of nuclear factor kappa-B ligand) on marrow stromal cells and by suppressing its decoy receptor osteoprotegerin (OPG). The RANKL-to-OPG ratio rises, osteoclasts mature and resorb bone, and calcium is released — the basis of hypercalcaemia.
- Osteoblast inhibition: Myeloma-secreted DKK1 (Dickkopf-1) and other Wnt-pathway inhibitors suppress osteoblast differentiation. The lytic lesions therefore do not heal even when the myeloma is in remission — the bone turnover markers remain disordered and pathological fractures continue to occur unless bisphosphonates or denosumab are given. [1]
The clinical consequence is purely lytic bone disease. Plain radiographs show punched-out lesions (skull "raindrop", vertebral collapse, rib fractures); unlike most metastatic disease there is no osteoblastic reaction, so a bone scan is often falsely normal — a classic exam point. Whole-body low-dose CT and PET-CT are the modern standards, both more sensitive than the older skeletal survey. [1]
The monoclonal protein — what each type does
- Intact immunoglobulin (IgG, IgA) — the serum paraprotein. Measured by serum protein electrophoresis (the M-spike) and quantified by densitometry. Tracked as the primary disease marker in IgG/IgA disease.
- Free light chains — kappa or lambda. In most myeloma the malignant clone also produces excess free light chains that are small enough to be filtered by the glomerulus. Overwhelmed tubular reabsorption leads to nephron toxicity (cast nephropathy). The serum free light chain assay quantifies both and the ratio; the involved-to-uninvolved ratio at least 100 is a myeloma-defining biomarker.
- Bence-Jones protein — the historic name for urinary monoclonal free light chains, detected by urine electrophoresis of a 24-hour collection. Largely superseded by the serum free light chain assay but still part of the IMWG workup. [1]
Clinical presentation
The CRAB cluster
The four classical myeloma-defining end-organ effects, each with a mechanism: [1]
| CRAB | Threshold (IMWG) | Mechanism |
|---|---|---|
| C — Calcium | Corrected serum calcium more than 0.25 mmol/L above the upper limit of normal, or over 2.75 mmol/L | Osteoclastic bone resorption driven by RANKL; also PTHrP in some patients |
| A — Anaemia | Haemoglobin more than 20 g/L below the lower limit of normal, or under 100 g/L | Marrow infiltration by plasma cells; also reduced erythropoietin from renal impairment and the anaemia of chronic disease |
| B — Bone | One or more osteolytic lesions on skeletal radiography, CT or PET-CT | RANKL-driven osteoclast activation with osteoblast suppression; classic purely lytic lesions |
Bone pain — the presenting symptom in two-thirds
Bone pain is the most common presenting symptom, classically in the back (lumbar then thoracic), ribs, pelvis and proximal long bones. The pain is often persistent, worse at night and unrelated to activity — a useful discriminator from mechanical back pain. Pathological fractures (vertebral compression, rib fracture on minimal trauma, femoral neck) are common. Acute severe back pain with leg weakness, urinary retention or a sensory level indicates malignant epidural spinal cord compression — an oncological emergency (see Complications). [1]
Hypercalcaemia — symptomatic and dangerous
Myeloma hypercalcaemia is symptomatic at lower levels than primary hyperparathyroidism because it develops quickly. The patient describes the "bones, stones, groans and psychic moans" of hypercalcaemia — bone pain, renal colic (less common in myeloma), constipation and abdominal pain, and confusion or lethargy. Severe hypercalcaemia causes dehydration (a nephrogenic diabetes insipidus-like state), acute kidney injury and arrhythmia. The ECG shows a shortened QT interval. [1]
Renal impairment — the reversible emergency
About a third of myeloma patients have renal impairment at diagnosis, and a further fraction develop it during the disease course. The dominant mechanism is cast nephropathy (myeloma kidney): filtered monoclonal free light chains form obstructing casts with Tamm-Horsfall protein in the distal nephron, with surrounding giant-cell reaction and tubular injury. Other mechanisms include AL amyloidosis (presents with nephrotic-range proteinuria, macroglossia and a low-voltage ECG), light-chain deposition disease (membranoproliferative-like glomerulopathy), hypercalcaemic nephropathy, uric-acid nephropathy, and drug toxicity (NSAIDs, contrast, calcineurin inhibitors). [1]
DWE discriminator: The single most reversible cause of myeloma-related renal failure is cast nephropathy with a high free light chain burden. Prompt cytoreduction with a bortezomib-based regimen plus high-cutoff haemodialysis in selected patients can recover renal function; delay beyond a few weeks makes recovery unlikely. Never give an NSAID to a myeloma patient — it precipitates or worsens cast nephropathy by reducing renal blood flow. [1]
Recurrent infection — hypogammaglobulinaemia
The malignant plasma cell clone suppresses normal polyclonal immunoglobulin production, and the disease and its treatment (bortezomib in particular) impair cellular immunity. Patients develop recurrent bacterial infections, especially with encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae), and herpes zoster reactivation (the rationale for aciclovir prophylaxis on bortezomib). Pneumonia and pyelonephritis are common; infection is one of the leading causes of death in myeloma. Vaccination (influenza, COVID-19, pneumococcal, influenza, recombinant zoster) should be given, ideally before treatment starts. [1]
Hyperviscosity — the IgM lesson
Hyperviscosity syndrome (visual disturbance, headache, mucosal bleeding, neurological symptoms, retinal venous engorgement with "sausage-link" vessels) is uncommon in IgG or IgA myeloma and typically requires a very high paraprotein (over about 100 g/L for IgG, or over about 70 g/L for IgA). It is classically a feature of Waldenstrom macroglobulinaemia — the IgM-secreting lymphoplasmacytic lymphoma — because IgM is a pentamer with high intrinsic viscosity at lower concentrations. Treatment is urgent plasmapheresis to lower the paraprotein quickly, then definitive cytoreduction. [1]
Other presenting features
- Fatigue from anaemia and the disease itself.
- Peripheral neuropathy at presentation is rare (it is more often a treatment side effect of bortezomib or thalidomide, or of amyloidosis) but POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell disorder, skin changes) is a recognised variant with a sclerotic rather than lytic bone lesion and an AIDP-like neuropathy.
- Extramedullary plasmacytoma — a soft-tissue mass of plasma cells (upper respiratory tract, skin, liver) — may precede or accompany marrow disease.
- Amyloidosis features — macroglossia, easy bruising (periorbital "raccoon eyes"), restrictive cardiomyopathy with a low-voltage ECG and thick echocardiographic walls, nephrotic syndrome, hepatomegaly. [1]
Differential diagnosis of a paraprotein or lytic bone disease
Causes of a monoclonal protein (the M-spike)
| Condition | Discriminating features |
|---|---|
| MGUS | M-protein under 30 g/L, marrow plasma cells under 10 per cent, no CRAB, no biomarkers |
| Multiple myeloma | Meets IMWG criteria (CRAB or biomarkers with clonal plasma cells at least 10 per cent) |
| Waldenstrom macroglobulinaemia | IgM paraprotein with lymphoplasmacytic lymphoma on marrow; symptoms of hyperviscosity; no lytic bone disease |
| Solitary plasmacytoma | Single bony or extramedullary lesion, no clonal marrow plasma cells, no CRAB; M-protein absent or small |
| AL amyloidosis | Systemic light-chain deposition; Congo-red-positive biopsy; often low-level paraprotein |
| POEMS syndrome | Peripheral neuropathy, sclerotic bone lesion, endocrinopathy, high VEGF |
| Heavy-chain diseases (alpha, gamma, mu) | Rare; malabsorption (alpha), lymphadenopathy (gamma) |
| Reactive (polyclonal) gammopathy** | No M-spike on immunofixation; polyclonal rise on serum electrophoresis from chronic infection, autoimmune disease or liver disease |
Causes of lytic bone lesions (the differential when the imaging shows a hole in the bone)
- Metastatic carcinoma — breast, lung, thyroid, kidney, prostate (the latter more often sclerotic). Metastases are the most important differential; a tissue biopsy settles it.
- Brown tumours of hyperparathyroidism.
- Langerhans cell histiocytosis (in younger patients).
- Bone lymphoma.
- Infection — osteomyelitis, tuberculosis. [1]
DWE discriminator: A bone scan isotope scintigram is often normal in myeloma because the lesions are purely lytic with no osteoblastic reaction. The modern standard is whole-body low-dose CT (more sensitive than plain radiographs and now the IMWG-recommended first-line imaging) or PET-CT (functional information, prognostic for residual disease). MRI is the modality of choice for suspected spinal cord compression and for diffuse marrow infiltration without focal lytic lesions. [1]
Investigations
Essential investigations for every patient with suspected myeloma
| Investigation | Why |
|---|---|
| Full blood count and film | Anaemia (normocytic normochromic); rouleaux on the film from high immunoglobulin; leucopenia and thrombocytopenia in advanced disease |
| ESR and CRP | ESR often very high (over 100) from the paraprotein; CRP is an acute-phase marker that may reflect disease activity |
| Urea, electrolytes, creatinine, eGFR | Renal impairment (CRAB-R); baseline before nephrotoxic treatment |
| Corrected calcium, albumin, phosphate | Hypercalcaemia (CRAB-C); albumin to correct the calcium |
| Liver function tests, total protein, albumin | The gap between total protein and albumin suggests a paraprotein |
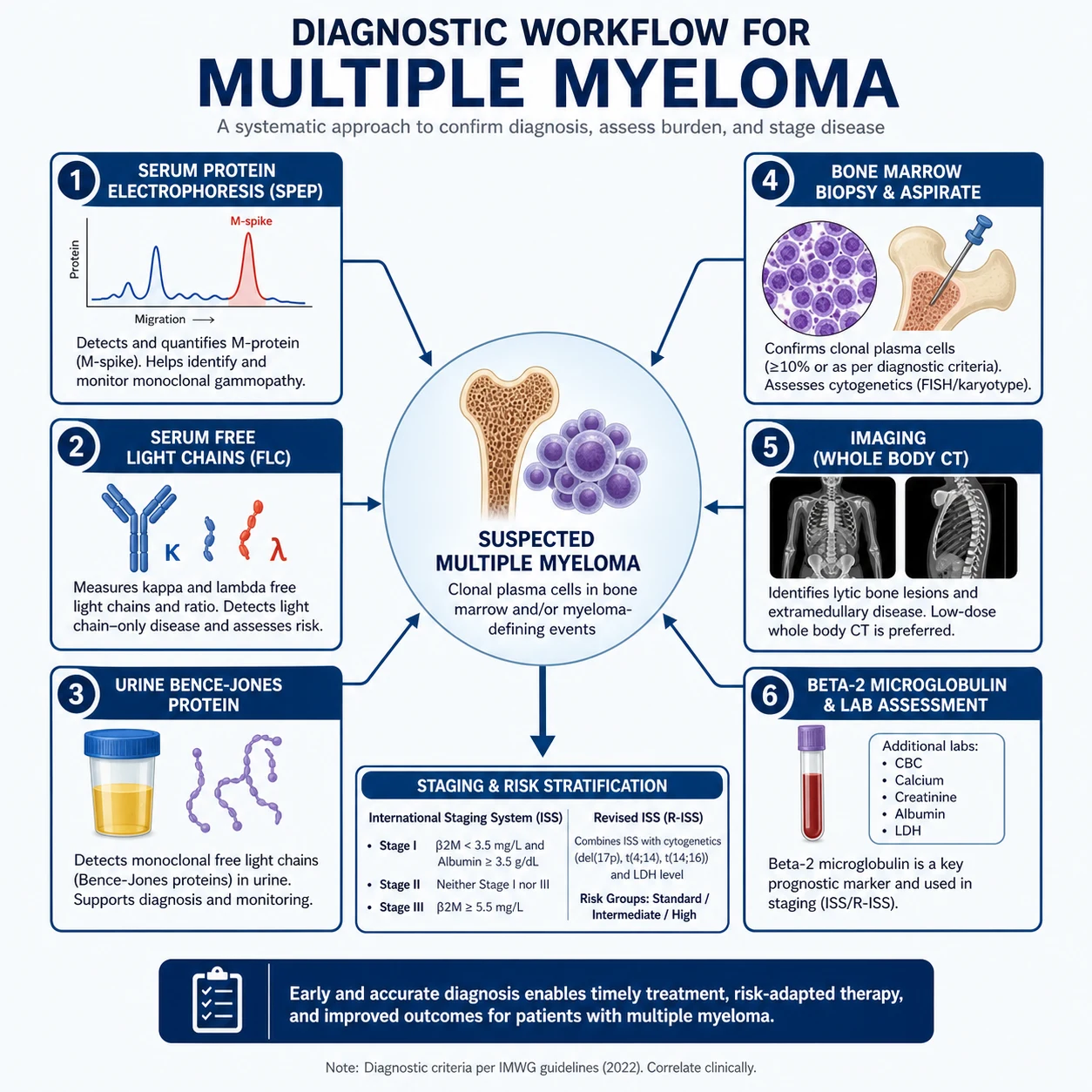
| Serum beta-2 microglobulin and LDH | The staging markers (ISS and R-ISS); beta-2 microglobulin is also a renal marker |
| Serum protein electrophoresis and immunofixation | Quantify the M-protein (the M-spike) and identify the heavy and light chain isotype |
| Serum free light chain assay (kappa and lambda, with ratio) | The critical assay for diagnosis, prognosis and monitoring of light-chain disease; the involved-to-uninvolved ratio at least 100 is myeloma-defining |
| Urine protein electrophoresis and immunofixation (24-hour collection) | Bence-Jones protein (urinary monoclonal free light chains); the modern serum free light chain assay has reduced but not replaced this |
| Bone marrow aspirate and trephine | Plasma cell percentage (the 10 and 60 per cent thresholds), morphology, immunophenotype (CD138, CD38, CD56 aberrant, light-chain restriction), and FISH for cytogenetics |
| Whole-body low-dose CT or PET-CT | Modern standard imaging for lytic lesions (replaced the skeletal survey) |
| MRI whole spine (if cord compression suspected or diffuse disease) | The modality of choice for spinal cord compression, diffuse marrow infiltration and focal lesions |
| Beta-hCG, HIV, hepatitis B and C serology | Pre-treatment workup; daratumumab interferes with blood-typing crossmatch (CD48 on red cells) — request "daratumumab-treated patient" on the group-and-save |
Cytogenetics on the bone marrow — what you must order
FISH on CD138-selected plasma cells (conventional karyotyping misses many lesions because plasma cells divide slowly) for: [1]
| Lesion | FISH finding | Prognostic impact |
|---|---|---|
| del(17p) (TP53 loss) | 17p13 deletion | High-risk adverse; early relapse, extramedullary disease, poor survival |
| t(4;14) | IgH-FGFR3/MMSET translocation | High-risk adverse; improves with proteasome inhibitor-based therapy |
| t(14;16) | IgH-c-MAF translocation | High-risk adverse |
| t(14;20) | IgH-MAFB translocation | High-risk adverse |
| Gain 1q (1q21 amplification) | Extra copy of 1q | Adverse |
| t(11;14) | IgH-cyclin D1 translocation | Standard risk; the "cyclin D1" group; the group most likely to respond to venetoclax |
| Hyperdiploidy | Multiple trisomies | Standard risk to favourable |
DWE discriminator: The single most adverse cytogenetic lesion is del(17p) — loss of the TP53 locus. In an MCQ, a young patient with high-risk del(17p) disease drives the recommendation toward aggressive therapy (autologous transplant, then consideration of maintenance intensification and possibly allogeneic transplant in selected patients). [1]
Imaging — what to order and why
The IMWG replaced the plain-film skeletal survey with whole-body low-dose CT as the first-line imaging modality because it detects lytic lesions in about a quarter of patients with a "normal" skeletal survey [1]. PET-CT adds functional information (active lesions are FDG-avid) and is prognostic — residual FDG-avid disease after induction predicts poorer outcomes. MRI is essential for spinal cord compression (urgent, whole-spine) and for diffuse marrow disease without focal lytic lesions. Plain radiographs retain a limited role but should not be the sole imaging.
Staging — the ISS and R-ISS
The International Staging System (ISS)
The original ISS, derived from over 10,000 patients and based on two cheap serum markers, stratifies survival cleanly [3]:
| Stage | Criteria | Median OS (pre-novel-agent era) |
|---|---|---|
| I | Beta-2 microglobulin under 3.5 mg/L and albumin at least 35 g/L | 62 months |
| II | Neither I nor III (beta-2M under 3.5 with low albumin, or beta-2M 3.5 to 5.5) | 44 months |
| III | Beta-2 microglobulin at least 5.5 mg/L | 29 months |
The Revised International Staging System (R-ISS)
The 2015 revision incorporates LDH and high-risk cytogenetics to give a more accurate modern prognosis [2]:
| Stage | Criteria | 5-year OS |
|---|---|---|
| I | ISS stage I, normal LDH, no high-risk cytogenetics [del(17p), t(4;14), t(14;16)] | About 82 per cent |
| II | Not I and not III | About 62 per cent |
| III | ISS stage III and high LDH or high-risk cytogenetics | About 40 per cent |
DWE high-yield: The R-ISS is the modern prognostic system to quote. Stage I disease (good-risk) carries a 5-year survival of over 80 per cent with modern therapy; stage III disease (high-risk) under 40 per cent. The stage is driven by beta-2 microglobulin, albumin, LDH and FISH cytogenetics — all of which you must order at diagnosis. [1]
Management

Principle 1 — Decide transplant eligibility first
The single most important initial decision is whether the patient is transplant-eligible. Eligibility is determined by fitness, not age alone — a fit 72-year-old may be eligible; a frail 60-year-old with severe comorbidity may not. Typical ANZ criteria: age up to about 70, ECOG performance status 0 to 1, adequate cardiac, hepatic and renal function, and the absence of uncontrolled comorbidity. Stem cells are collected (by peripheral collection after cyclophosphamide and G-CSF mobilisation, sometimes with plerixafor) early in the treatment course, and the transplant is performed after 3 to 4 cycles of induction. Tandem transplant (a second transplant 3 to 6 months after the first) is used in selected patients with less than complete response after the first, but is uncommon in the modern era of maintenance. [1]
Principle 2 — Induction for the transplant-eligible patient: VRd
The current standard induction for a fit, transplant-eligible patient is bortezomib, lenalidomide and dexamethasone (VRd). SWOG S0777 established that the VRd triplet improves both progression-free and overall survival over lenalidomide-dexamethasone (Rd) [4]. IFM 2009 confirmed that, after VRd induction, adding high-dose melphalan with autologous transplant further improves progression-free survival (though with no overall survival difference at early follow-up) [5]. Typical doses: bortezomib 1.3 mg/m2 subcutaneously on days 1, 4, 8 and 11 of a 21-day cycle; lenalidomide 25 mg orally days 1 to 14; dexamethasone 40 mg weekly (with reduced-dose dexamethasone, e.g. 20 mg weekly, in older or frail patients to limit steroid toxicity). A typical induction is 4 cycles.
Bortezomib is given subcutaneously, not intravenously, since the subcutaneous route reduces peripheral neuropathy without loss of efficacy (a standard exam point). Aciclovir prophylaxis is given for herpes zoster reactivation. Bortezomib is dose-modified or held for worsening neuropathy, and switched to carfilzomib (an intravenous next-generation proteasome inhibitor with less neuropathy, but with a small risk of cardiac and pulmonary toxicity) in patients with pre-existing neuropathy. [1]
Why bortezomib in renal failure? Because it is hepatically cleared and not nephrotoxic, and it is the most effective agent for rapidly lowering the free light chain burden in cast nephropathy. A bortezomib-based regimen is the standard of care for myeloma-related renal failure. [1]
Principle 3 — Autologous stem cell transplant
After 3 to 4 cycles of induction, peripheral blood stem cells are collected (target at least 2 to 4 million CD34+ cells per kg), and the patient undergoes a single autologous transplant: high-dose melphalan 200 mg/m2 intravenously as conditioning, then reinfusion of the stem cells. The procedure takes about 2 to 3 weeks in hospital with the main toxicities being mucositis, cytopenias and infection. Transplant-related mortality is now under 1 to 2 per cent in modern series. EMN02/HO95 confirmed that autologous transplant improves progression-free survival over bortezomib-melphalan-prednisone (VMP) in the modern era, with median PFS about 57 versus 42 months [6].
Is transplant curative? No — it produces a deep response (often complete response or very good partial response) and prolongs progression-free survival, but nearly all patients relapse. It is therefore followed by maintenance. The role of transplant is being re-examined as induction regimens intensify; current guidance continues to recommend it for eligible patients because of the consistent PFS benefit and a manageable toxicity profile. [1]
Principle 4 — Maintenance: lenalidomide
After transplant, lenalidomide maintenance (10 to 15 mg daily, days 1 to 21 of a 28-day cycle, until progression) improves both progression-free and overall survival, established by the CALGB 100104 trial and a subsequent meta-analysis of three large trials [7]. The main toxicities are cytopenias, infection, rash, fatigue and a small increase in second primary malignancies (particularly solid tumours and myelodysplasia) — a recognised but net-beneficial trade-off. Lenalidomide is dose-reduced for renal impairment.
Principle 5 — The transplant-ineligible patient: daratumumab-based therapy
For patients who are not transplant candidates (older age, frailty, comorbidity), the modern standard is a daratumumab-based triplet. The MAIA trial established that daratumumab plus lenalidomide and dexamethasone (DRd) improves both progression-free and overall survival over lenalidomide-dexamethasone alone in transplant-ineligible newly diagnosed myeloma [8]. At 5-year follow-up the PFS advantage is large. An alternative is bortezomib-melphalan-prednisone (VMP) — historically the standard for older patients (the VISTA trial) — or VRd-lite (a reduced-intensity bortezomib-lenalidomide-dexamethasone schedule) for intermediate-fitness patients.
Daratumumab is a monoclonal antibody against CD38 on the plasma cell surface. Its notable practical issues are: (1) infusion reactions during the first dose (premedication with steroids, paracetamol and an antihistamine is mandatory; the subcutaneous formulation markedly reduces these); (2) interference with the blood crossmatch — daratumumab binds CD38 on donor red cells, causing a panreactive antibody screen; the blood bank must be told the patient is on daratumumab; and (3) interference with the serum free light chain and paraprotein assays — the daratumumab itself appears as an M-spike on immunofixation, requiring the newer mass-spectrometry-based monitoring or the DIRA (daratumumab-specific immunofixation reflex assay) to distinguish residual disease from drug. [1]
Principle 6 — Relapsed and refractory disease
Myeloma nearly always relapses. The relapsed setting uses the agents not yet used or reused in combination: [1]
- Carfilzomib (an intravenous proteasome inhibitor with less neuropathy) with lenalidomide-dexamethasone or dexamethasone alone.
- Pomalidomide (a more potent immunomodulator, effective after lenalidomide failure) with dexamethasone.
- Daratumumab monotherapy or in combination (the POLLUX and CASTOR trials established daratumumab combinations in relapse).
- Isatuximab (another anti-CD38 antibody).
- Selinexor (an exportin-1 inhibitor, oral).
- Belantamab mafodotin (an anti-BCMA antibody-drug conjugate, with ocular toxicity).
- CAR-T cell therapy (idecabtagene vicleucel and ciltacabtagene autoleucel, both anti-BCMA) — now approved for relapsed refractory disease after at least two to four prior lines, with deep but not universally durable responses and the risks of cytokine release syndrome and neurotoxicity.
- Bispecific T-cell engagers (teclistamab, elranatamab — anti-BCMA x CD3) — off-the-shelf T-cell redirecting therapies that are transforming the late-line landscape. [1]
Venetoclax, a BCL-2 inhibitor, has a striking activity in the t(11;14) subgroup of myeloma — these patients over-express BCL-2 — and is being incorporated into biomarker-driven trials. [1]
Principle 7 — Supportive care for every patient
Supportive care is as important as the anti-myeloma therapy and applies at every stage: [1]
- Bone health — bisphosphonates (zoledronic acid 4 mg IV monthly, or pamidronate) reduce skeletal events, bone pain and hypercalcaemia and improve survival (the MRC Myeloma IX trial). Denosumab (a RANKL inhibitor, 120 mg subcutaneously monthly) is an alternative, especially in renal impairment, and is non-inferior to zoledronic acid for skeletal events. Both require calcium and vitamin D supplementation to prevent hypocalcaemia. Osteonecrosis of the jaw is a recognised complication of both — a dental check before starting is standard.
- Renal protection — aggressive hydration, avoid NSAIDs (the cardinal rule), avoid nephrotoxic contrast where possible, manage hypercalcaemia, and consider high-cutoff haemodialysis in severe cast nephropathy.
- VTE prophylaxis — lenalidomide, thalidomide and pomalidomide (the IMiDs) carry a thrombotic risk, especially when combined with dexamethasone or doxorubicin. The IMWG recommends aspirin for standard-risk patients and low-molecular-weight heparin or warfarin for high-risk patients (prior VTE, immobility, high platelets, kidney disease).
- Infection prophylaxis — aciclovir for herpes zoster on bortezomib; cotrimoxazole for Pneumocystis on dexamethasone-heavy regimens; vaccination (influenza, COVID-19, pneumococcal, recombinant zoster — ideally before treatment, since response is blunted during therapy); intravenous immunoglobulin for selected patients with recurrent severe infection and hypogammaglobulinaemia.
- Anaemia — erythropoiesis-stimulating agents have a limited role (and carry a thrombotic risk in myeloma); transfusion for symptomatic anaemia.
- Neuropathy — dose-modification of bortezomib (subcutaneous route, reduced frequency) or switch to carfilzomib; gabapentinoids for symptom control.
- Palliative radiotherapy — for painful focal lesions, pathological fractures or spinal cord compression, local radiotherapy is highly effective for pain control. [1]
Complications and emergencies
Malignant epidural spinal cord compression
Acute or worsening back pain with a neurological sign (leg weakness, sensory level, urinary retention, faecal incontinence) in a myeloma patient is malignant epidural spinal cord compression until proven otherwise. Urgent MRI of the whole spine (the lesion may be at multiple levels) and dexamethasone 10 to 16 mg intravenously immediately to reduce oedema. Urgent clinical oncology review for radiotherapy or, in selected cases with spinal instability or a single-level lesion, neurosurgical decompression. This is an oncological emergency — delay causes permanent paraplegia. [1]
Symptomatic hypercalcaemia
Aggressive intravenous normal saline (3 to 6 litres over 24 hours, guided by volume status), then a bisphosphonate (zoledronic acid 4 mg IV over 15 minutes; dose-reduced for renal impairment). Calcitonin 4 to 8 IU/kg subcutaneously every 12 hours works within hours for symptomatic relief while the bisphosphonate takes effect over 48 to 72 hours. Denosumab (120 mg subcutaneously) is an alternative in renal failure because it is not renally cleared. Avoid thiazide diuretics (they retain calcium); a loop diuretic is used only for volume overload. [1]
Acute kidney injury from cast nephropathy
The reversible emergency. Hydrate aggressively (intravenous normal saline, target a urine output of at least 100 mL/hour), withdraw all nephrotoxins immediately (NSAIDs, ACE inhibitors or ARBs if hypoperfusing, contrast, aminoglycosides), treat hypercalcaemia, and start a bortezomib-based regimen urgently to lower the free light chain burden. In selected patients with very high free light chain levels and dialysis-dependent renal failure, high-cutoff haemodialysis (a modified dialysis that removes free light chains) may improve the chance of renal recovery, though its routine use remains debated. The best predictor of renal recovery is a 50 per cent reduction in the serum free light chain within 21 days. [1]
Hyperviscosity syndrome
Visual disturbance, headache, mucosal bleeding, neurological symptoms and the characteristic retinal venous engorgement with "sausage-link" vessels. More typical of Waldenstrom macroglobulinaemia (IgM) than of typical IgG or IgA myeloma. Urgent plasmapheresis to lower the paraprotein acutely (1.0 to 1.5 plasma volumes), then definitive cytoreduction. The plasma viscosity (above about 4 centipoise, or serum viscosity above 6) supports the decision, but the trigger is clinical, not a number. [1]
Amyloidosis
Systemic AL amyloidosis complicates about 10 to 15 per cent of myeloma cases and may also occur without overt myeloma. The clinical clues are nephrotic-range proteinuria (especially with a small paraprotein), macroglossia (the tongue is enlarged and indented by the teeth), periorbital purpura ("raccoon eyes"), restrictive cardiomyopathy (low-voltage ECG with thick echocardiographic walls — the opposite of hypertensive heart disease), hepatomegaly and a bleeding tendency (factor X binding). Diagnosis is by biopsy (abdominal fat pad, bone marrow, or involved organ) with Congo-red staining showing apple-green birefringence. Treatment is the same anti-myeloma therapy (bortezomib-based, daratumumab-based), directed at the clonal plasma cell. [1]
Peripheral neuropathy
Bortezomib and thalidomide cause a length-dependent sensorimotor neuropathy. Prevention is by the subcutaneous bortezomib route and dose-reduction. The IMWG recommends holding bortezomib for grade 2 or worse neuropathy and reintroducing at a lower dose once recovered. Amyloidosis also causes neuropathy (autonomic and sensory) and is suspected when the paraprotein is small and the syndrome is systemic. [1]
Prognosis and follow-up
Median overall survival in myeloma has improved dramatically with modern therapy, from about 3 years in the melphalan era to over 8 to 10 years in the current era. Prognosis is driven by the R-ISS stage, the depth of response (the IMWG response categories — complete response, very good partial response, partial response — are tied to the paraprotein and free light chain levels), and the cytogenetic risk. Patients with standard-risk disease who achieve a complete response and remain on lenalidomide maintenance can expect progression-free survival of 4 to 6 years and overall survival of over 10 years. Patients with high-risk disease (del(17p), R-ISS stage III) have a much shorter survival despite modern therapy, and are candidates for clinical trials, intensified maintenance and possibly allogeneic transplant. [1]
Follow-up is lifelong. The disease is monitored by the serum paraprotein (for IgG/IgA disease) and the serum free light chain ratio (for light-chain and oligosecretory disease) every 1 to 3 months during treatment and every 3 to 6 months on maintenance. The bone marrow is repeated to confirm complete response (less than 5 per cent plasma cells) and for measurable (minimal) residual disease testing by multiparameter flow cytometry or next-generation sequencing — MRD negativity is the strongest predictor of durable remission. Imaging is repeated for new bone pain or rising disease markers. Vaccination, bone health, infection prophylaxis and psychosocial support continue throughout. [1]
Exam traps and high-yield discriminators
- The single most common DWE error is failing to send serum free light chains in an older patient with unexplained renal impairment, anaemia or back pain. The serum free light chain assay is part of the myeloma screen alongside serum protein electrophoresis; without it, light-chain myeloma (which has no serum paraprotein) is missed.
- A normal bone scan does not exclude myeloma. The lesions are purely lytic with no osteoblastic reaction. The modern standard is whole-body low-dose CT or PET-CT.
- del(17p) (TP53 loss) is the most adverse cytogenetic lesion and drives high-risk treatment. FISH on CD138-selected marrow plasma cells is mandatory at diagnosis.
- Back pain with neurological signs in known or suspected myeloma is malignant epidural spinal cord compression — urgent MRI whole spine and dexamethasone. Do not delay for plain films or CT.
- Never give NSAIDs to a myeloma patient. The risk of precipitating or worsening cast nephropathy outweighs any analgesic benefit. Use paracetamol, opioids and local radiotherapy for bone pain.
- The involved-to-uninvolved free light chain ratio at least 100, marrow plasma cells at least 60 per cent, or more than one focal MRI lesion are myeloma-defining biomarkers under the IMWG 2014 criteria — the patient requires treatment even without CRAB features.
- Daratumumab interferes with the blood crossmatch and with the serum paraprotein assay. Tell the blood bank, and use mass-spectrometry or the DIRA assay for response assessment.
- Bortezomib is given subcutaneously, not intravenously, to reduce peripheral neuropathy; aciclovir prophylaxis is given for herpes zoster.
- Hyperviscosity is classically a feature of Waldenstrom macroglobulinaemia (IgM), not typical IgG/IgA myeloma, but can occur with very high paraproteins. The treatment is urgent plasmapheresis.
- The R-ISS is the modern staging system — it adds LDH and high-risk cytogenetics to the ISS (beta-2 microglobulin and albumin). Quote it, not the ISS alone, in a viva.
- Lenalidomide maintenance after autologous transplant improves overall survival — established by the CALGB 100104 trial. The main toxicity to counsel on is second primary malignancy.
- VRd is the standard induction for transplant-eligible myeloma (SWOG S0777), and autologous transplant further improves PFS (IFM 2009, EMN02/HO95). For transplant-ineligible disease, a daratumumab-based regimen (DRd, MAIA) is now standard. [1]
Cross-links
- Acute kidney injury — cast nephropathy is a reversible cause; see the renal topic for the AKI framework.
- Anaemia — systematic workup — the normocytic anaemia of chronic disease from marrow infiltration.
- Sodium disorders and Acid-base disorders — the renal and electrolyte complications of myeloma and its treatment.
- Chronic kidney disease — long-term outcome of myeloma kidney.
- Acute leukaemia — the differential of marrow infiltration. [1]
References and guidelines
IMWG 2014 diagnostic criteria (Rajkumar, Lancet Oncol) [1]; R-ISS (Palumbo, JCO 2015) [2]; ISS (Greipp, JCO 2005) [3]; SWOG S0777 VRd (Durie, Lancet 2017) [4]; IFM 2009 transplant with RVd (Attal, NEJM 2017) [5]; EMN02/HO95 transplant versus VMP (Cavo, Lancet Haematol 2020) [6]; CALGB 100104 lenalidomide maintenance (McCarthy, NEJM 2012) [7]; MAIA daratumumab (Facon, NEJM 2019) [8]; MGUS long-term progression (Kyle, NEJM 2018) [9]. NCCN Multiple Myeloma Guidelines; ESMO Clinical Practice Guidelines; Myeloma Australia and HSANZ/eviQ protocols.
References
- [1]Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma Lancet Oncol, 2014.PMID 25439696
- [2]Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group J Clin Oncol, 2015.PMID 26240224
- [3]Greipp PR, San Miguel J, Durie BG, et al. International staging system for multiple myeloma J Clin Oncol, 2005.PMID 15809451
- [4]Durie BG, Hoering A, Abidi MH, et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): a randomised, open-label, phase 3 trial Lancet, 2017.PMID 28017406
- [5]Attal M, Lauwers-Cances V, Hulin C, et al. Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma N Engl J Med, 2017.PMID 28379796
- [6]Cavo M, Gay F, Beksac M, et al. Autologous haematopoietic stem-cell transplantation versus bortezomib-melphalan-prednisone, with or without bortezomib-lenalidomide-dexamethasone consolidation therapy, and lenalidomide maintenance for newly diagnosed multiple myeloma (EMN02/HO95): a multicentre, randomised, open-label, phase 3 study Lancet Haematol, 2020.PMID 32359506
- [7]McCarthy PL, Owzar K, Hofmeister CC, et al. Lenalidomide after stem-cell transplantation for multiple myeloma N Engl J Med, 2012.PMID 22571201
- [8]Facon T, Kumar S, Plesner T, et al. Daratumumab plus Lenalidomide and Dexamethasone for Untreated Myeloma N Engl J Med, 2019.PMID 31141632
- [9]Kyle RA, Larson DR, Therneau TM, et al. Long-Term Follow-up of Monoclonal Gammopathy of Undetermined Significance N Engl J Med, 2018.PMID 29342381