Phys · haematological
Haematopoietic Stem Cell Transplantation
Also known as stem cell transplant · HSCT · bone marrow transplant · autologous transplant · allogeneic transplant · haematopoietic cell transplantation · graft-versus-host disease · GVHD · reduced-intensity conditioning · haploidentical transplant
Consultant-physician-depth guide to autologous and allogeneic haematopoietic stem cell transplantation for FRACP DWE and DCE — mobilisation and harvest, conditioning intensity, engraftment, and the timeline of complications from mucositis and veno-occlusive disease through acute and chronic GVHD to secondary malignancy and endocrine late effects.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Haematopoietic Stem Cell Transplantation

The answer first
Haematopoietic stem cell transplantation (HSCT) is the infusion of haematopoietic stem cells after high-dose chemotherapy (and sometimes radiotherapy) to rescue marrow function and, in allogeneic transplantation, to generate a new immune system that fights the underlying disease. It is offered for diseases where escalating chemotherapy doses can overcome resistance (autologous) or where a new immune system can eliminate residual disease (allogeneic). Two bedside rules change outcome: [1]
- Autologous versus allogeneic is the single most important distinction. An autologous transplant uses the patient's own previously collected stem cells — there is no graft-versus-host disease (GVHD), transplant-related mortality is 1 to 2 per cent, and the graft-versus-leukaemia (GVL) effect is absent. An allogeneic transplant uses a donor's cells — there is a real risk of GVHD, mortality is 10 to 30 per cent, but the GVL effect can cure disease that chemotherapy alone cannot [8].
- Complications follow a predictable timeline. The first 30 days are dominated by mucositis, neutropenic fever, veno-occlusive disease (sinusoidal obstruction syndrome) and haemorrhagic cystitis. Days 30 to 100 are dominated by acute GVHD, CMV reactivation and opportunistic infection. Beyond day 100 the patient enters the chronic phase, defined by chronic GVHD, secondary malignancy and endocrine late effects.
For autologous transplant the conditioning backbone is disease-specific: melphalan 200 mg/m2 for myeloma, BEAM (carmustine, etoposide, cytarabine, melphalan) for lymphoma. For allogeneic transplant the conditioning choice trades toxicity against relapse: myeloablative regimens are total body irradiation (TBI) plus cyclophosphamide, or busulfan plus cyclophosphamide or fludarabine [10]; reduced-intensity regimens are fludarabine plus lower-dose busulfan or melphalan, relying more on the GVL effect and suitable for older or comorbid patients.
Engraftment is defined as an absolute neutrophil count over 0.5 times 10 to the 9 per litre for three consecutive days, with platelet recovery over 20, typically 10 to 20 days after infusion. Engraftment failure, infection, GVHD and recurrence of the original disease are the dominant concerns in the first year. Long-term, the transplant survivor becomes a chronic-disease patient with endocrine, bone, malignancy and psychosocial needs. [1]
Classification
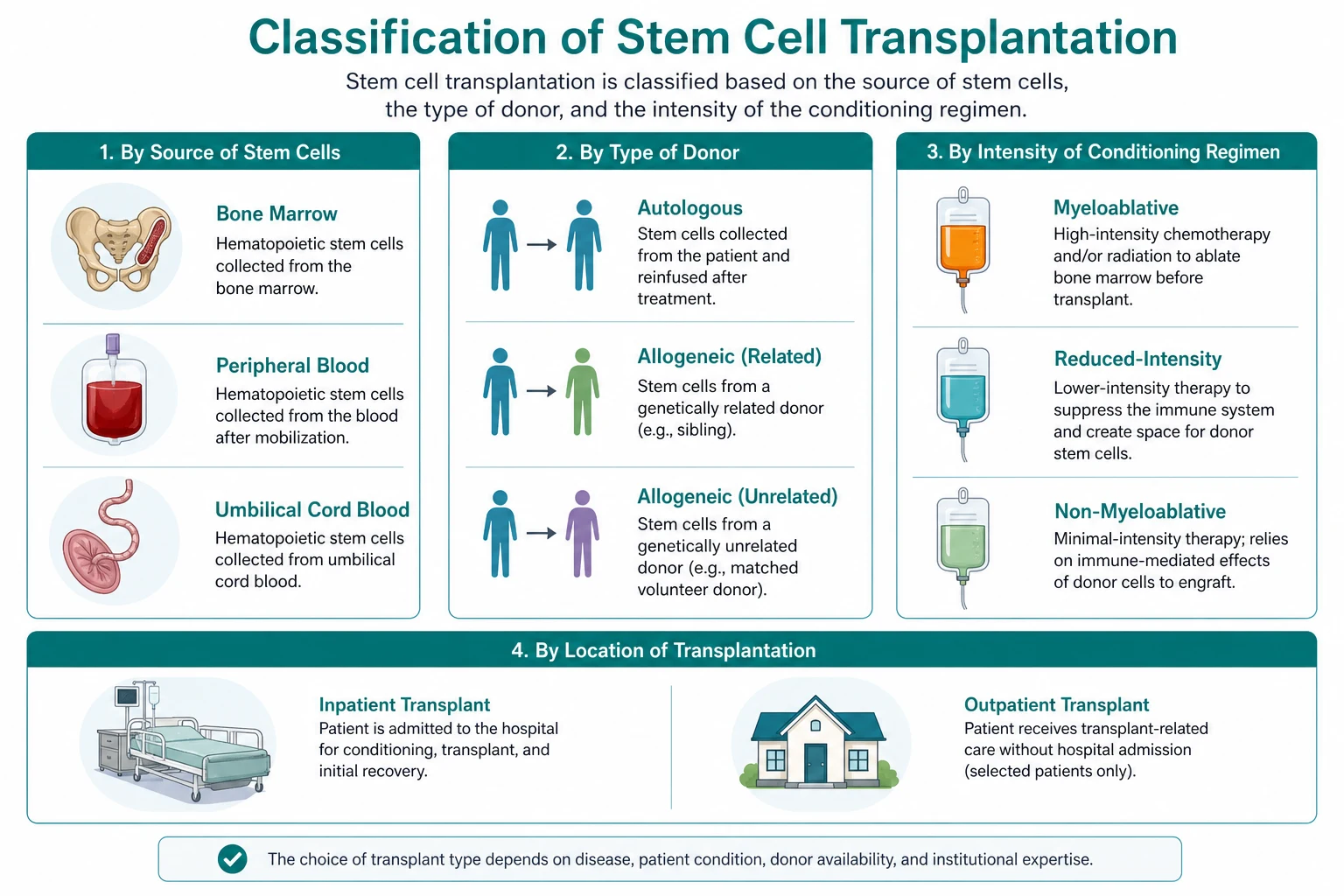

Autologous versus allogeneic — the foundational distinction
| Feature | Autologous | Allogeneic |
|---|---|---|
| Stem cell source | Patient's own previously collected cells | A donor (related, unrelated, haploidentical, cord blood) |
| Principal indications | Multiple myeloma, relapsed Hodgkin and non-Hodgkin lymphoma, selected solid tumours | Acute leukaemia, myelodysplasia, aplastic anaemia, relapsed indolent disease after autograft, inherited marrow failure and metabolic disorders |
| GVHD risk | None | Significant (acute 30 to 50 per cent, chronic 30 to 70 per cent) |
| Transplant-related mortality | 1 to 2 per cent | 10 to 30 per cent depending on donor, conditioning and comorbidity |
| GVL or graft-versus-tumour effect | Absent | Present — the donor's immune cells recognise residual malignancy |
| Immune reconstitution | Rapid — own immune system returns within weeks | Slow — 6 to 12 months, longer with chronic GVHD |
| Principal complications | Mucositis, neutropenic sepsis, secondary myelodysplasia, infertility | GVHD, opportunistic infection, veno-occlusive disease, secondary malignancy, infertility, endocrine failure |
DWE high-yield: If a vignette describes a patient with multiple myeloma or relapsed lymphoma receiving high-dose melphalan or BEAM followed by reinfusion of their own cells, that is autologous — there is no GVHD. If a vignette describes a donor graft, immunosuppression, rash or diarrhoea in the weeks after, that is allogeneic — and GVHD is the complication to manage. [1]
Allogeneic donor sources
The donor source shapes GVHD, engraftment speed and access, and the choice is dictated by HLA matching, urgency and patient comorbidity. [1]
| Donor source | Match | GVHD risk | Engraftment | Notes |
|---|---|---|---|---|
| HLA-matched sibling (MRD) | 8 of 8 HLA-A, B, C, DRB1 | Lowest | Fastest | Only about 25 to 30 per cent of patients have a matched sibling; historically the gold standard |
| HLA-matched unrelated donor (MUD) | 8 of 8 by high-resolution typing | Intermediate | Slightly slower | Available through registries; more GVHD than sibling but comparable long-term outcomes |
| Haploidentical family donor | Half-matched (a parent, child or sibling) | Modulated by post-transplant cyclophosphamide | Similar to MUD with modern platforms | Available for nearly every patient since the advent of post-transplant cyclophosphamide [8] |
| Umbilical cord blood | Less stringent matching permitted | Lower than expected given mismatch | Slower (delayed neutrophil recovery) | Limited cell dose; often double-cord grafts in adults; favours younger patients |
DWE conceptual: Why does post-transplant cyclophosphamide make haploidentical transplantation safe when it was historically a graveyard of GVHD? Cyclophosphamide given on days 3 and 4 after transplant selectively deletes the rapidly proliferating alloreactive T-cells that cause GVHD, while sparing the resting regulatory T-cells (Tregs) and the haematopoietic stem cells, both of which express the detoxifying enzyme aldehyde dehydrogenase. The result is tolerance across the HLA barrier, dramatically reduced GVHD and graft failure, and a donor for nearly every patient [8].
Conditioning intensity
Conditioning is the chemotherapy (plus or minus radiotherapy) given immediately before the stem cell infusion. Its jobs are to ablate the recipient marrow, to suppress host immunity sufficiently to prevent graft rejection (allogeneic only), and to deliver anti-tumour cytoreduction. [1]
| Intensity | Examples | Indications | Trade-off |
|---|---|---|---|
| Myeloablative | TBI 12 Gy plus cyclophosphamide 120 mg/kg; busulfan plus cyclophosphamide or fludarabine [10]; TBI plus etoposide (for ALL) | Young, fit patients with aggressive disease | Maximum anti-tumour effect; highest mucositis, infertility, late malignancy and organ toxicity |
| Reduced-intensity (RIC) | Fludarabine plus melphalan 140 mg/m2; fludarabine plus busulfan 8 mg/kg; fludarabine plus low-dose TBI | Older patients (over 55 to 60) or those with comorbidity | Sufficient immunosuppression for engraftment, relying on GVL; higher relapse risk in aggressive disease |
| Non-myeloablative | Low-dose TBI (2 Gy) plus fludarabine; fludarabine plus cyclophosphamide plus antithymocyte globulin (aplastic anaemia) | Patients unsuited to either of the above; aplastic anaemia | Minimal cytoreduction; depends almost entirely on GVL; highest risk of graft rejection |
DCE long-case trap: Conditioning intensity is not the same as curative intent. A reduced-intensity regimen is chosen when the patient's comorbidity or age precludes myeloablative conditioning, not because the disease is less aggressive. The GVL effect compensates for reduced cytoreduction, but in chemosensitive aggressive disease (high-risk AML, advanced lymphoma) the relapse risk is higher with RIC. The registrar's job is to align conditioning with the patient's disease biology, comorbidity (HCT-specific comorbidity index) and goals. [1]
Pathophysiology
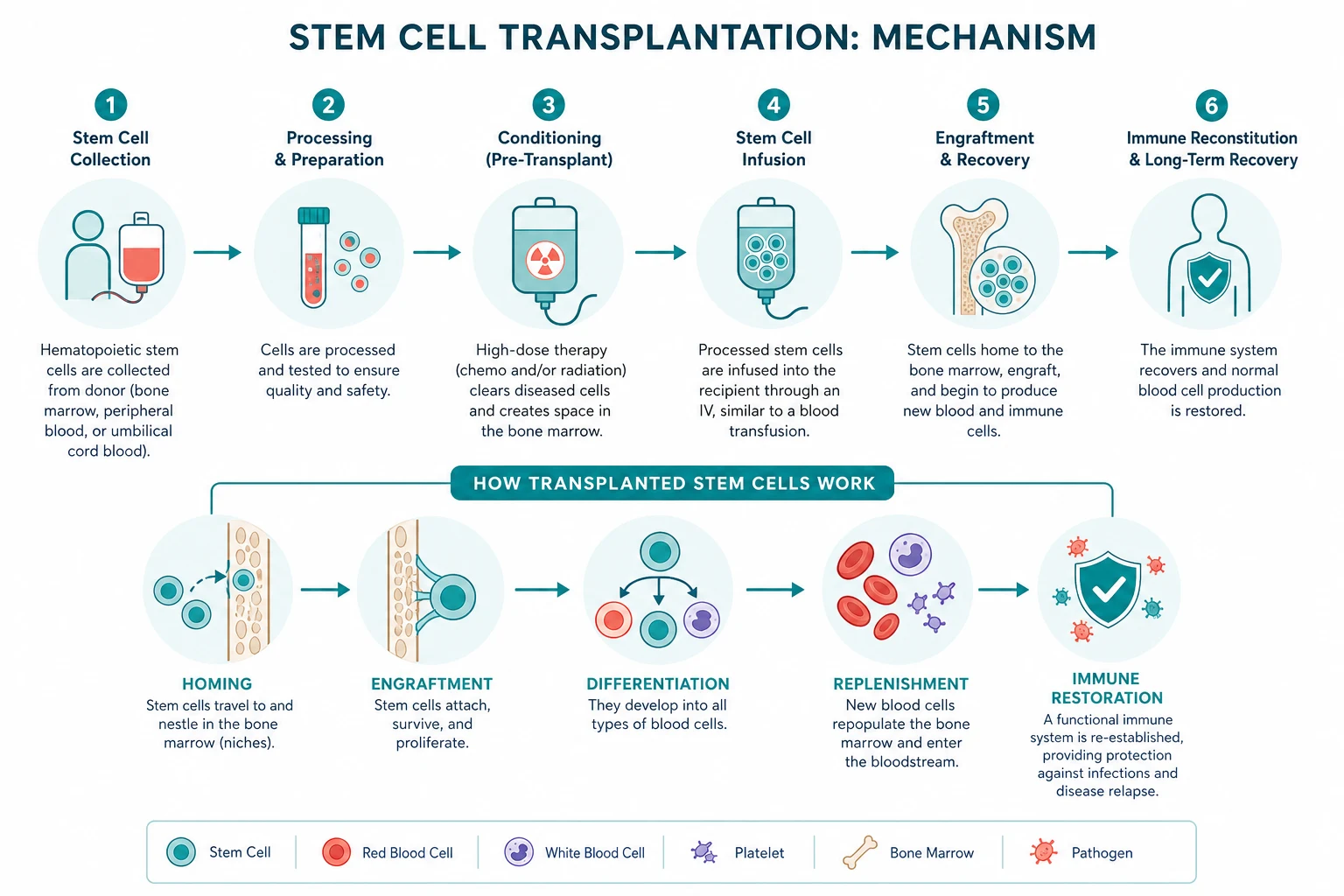
Mobilisation, harvest and the stem cell niche
Haematopoietic stem cells normally live in the marrow, tethered to osteoblasts and stromal cells by the SDF-1/CXCR4 axis. Mobilisation forces these cells into the peripheral blood so they can be collected by apheresis. [1]
- G-CSF (filgrastim, 10 micrograms/kg per day subcutaneously) expands the CD34-positive pool and downregulates the adhesion molecules that tether stem cells, releasing them into the circulation.
- Plerixafor (240 micrograms/kg subcutaneously) is a CXCR4 antagonist that blocks the SDF-1 anchor and enhances egress. The plerixafor trials in multiple myeloma and non-Hodgkin lymphoma showed that adding plerixafor to G-CSF significantly increased the proportion of patients who reached the target collection and proceeded to autograft [5][6]. It is reserved for predicted or actual poor mobilisers (older age, extensive prior chemotherapy, prior radiation, certain lymphoma subtypes).
- Bone marrow harvest under general anaesthetic is an alternative when peripheral mobilisation fails or is inappropriate (some aplastic anaemia or inherited disease protocols), but peripheral blood has largely replaced it because engraftment is faster.
Apheresis collects the mononuclear cell fraction, and the CD34-positive cell count is the surrogate for the stem cell dose. The minimum target is 2 million CD34-positive cells per kilogram; the ideal is over 5 million per kilogram, which speeds engraftment and lowers graft failure. [1]
Conditioning and the marrow niche
Conditioning ablates the recipient marrow, creating physical and cytokine space for the graft. In allogeneic transplant, conditioning also provides host immunosuppression so the new immune system is not rejected. Myeloablative regimens cause irreversible infertility and prolonged cytopenia; reduced-intensity regimens preserve some host immunity and the graft gradually replaces (mixed chimerism) over weeks to months. [1]
Engraftment and chimerism
Infused CD34-positive cells home to the marrow via the SDF-1/CXCR4 axis, seed the niche, and proliferate and differentiate. Neutrophil engraftment is declared when the absolute neutrophil count exceeds 0.5 times 10 to the 9 per litre for three consecutive days. Platelet engraftment is a sustained count over 20 times 10 to the 9 per litre unsupported by transfusion. Both typically occur 10 to 20 days post-infusion, faster with peripheral blood grafts and G-CSF mobilisation, slower with cord blood. [1]
Chimerism analysis — short tandem repeat (STR) PCR quantifying the proportion of donor versus recipient cells in the marrow or blood — confirms engraftment and detects graft rejection, relapse or mixed chimerism. Falling donor chimerism prompts consideration of donor lymphocyte infusion (to push the GVL effect) or, conversely, reassessment for relapse. [1]
The graft-versus-leukaemia effect
The GVL effect is the immune-mediated recognition and killing of residual malignant cells by donor T-cells and NK cells. It is why relapse is lower after allogeneic than autologous transplant, why T-cell depletion (to prevent GVHD) paradoxically raises relapse risk, and why donor lymphocyte infusion (DLI) can reinduce remission in a patient who relapses after allogeneic transplant. It is most powerful in chronic phase CML, less so in acute leukaemia and many lymphomas. The two faces of donor immunity — GVL (beneficial) and GVHD (harmful) — are inseparable in practice and are the central tension of allogeneic transplantation. [1]
Clinical presentation — the complication timeline

The complications of HSCT follow a predictable calendar. The patient in front of you is best understood by asking "what day is it?" — the day count after the stem cell infusion. [1]
Early phase (0 to 30 days)
| Complication | Presentation | Key features |
|---|---|---|
| Mucositis | Oral pain, dysphagia, drooling, inability to eat; occurs 5 to 14 days after conditioning | Severity scales with conditioning intensity; major portal for bacteraemia; pain control (opioid PCA), oral hygiene and parenteral nutrition are mainstays |
| Neutropenic fever | Fever in a patient with an absolute neutrophil count under 0.5 | Medical emergency — cultures then empiric antipseudomonal beta-lactam within one hour; do not wait for consultant review |
| Veno-occlusive disease (sinusoidal obstruction syndrome) | Weight gain, tender hepatomegaly, rising bilirubin, ascites, often with renal and respiratory failure, within 21 days of conditioning | Modified Seattle or Baltimore criteria; defibrotide is the only proven therapy [4] |
| Engraftment syndrome | Fever, rash, weight gain, pulmonary infiltrates and hypoxia at the moment of neutrophil recovery | Self-limiting, steroid responsive; must be distinguished from neutropenic sepsis and acute GVHD |
| Haemorrhagic cystitis | Gross haematuria, bladder pain, clot retention | Cyclophosphamide-related (within 48 hours, prevented by mesna and hyperhydration) or viral (BK virus or adenovirus, later) |
Mid phase (30 to 100 days) — acute GVHD and viral reactivation
| Complication | Presentation | Key features |
|---|---|---|
| Acute GVHD | Skin rash (maculopapular, palms and soles, ears, progressing to bullae and desquamation), gastrointestinal involvement (anorexia, nausea, watery diarrhoea, abdominal pain, bleeding), liver involvement (cholestatic pattern with rising bilirubin) | Glucksberg-Przepiorka grading I to IV [9]; first-line is corticosteroid, second-line ruxolitinib (REACH1, REACH2) [3][1] |
| CMV reactivation | Often asymptomatic on surveillance PCR; can cause colitis (diarrhoea), pneumonitis (dyspnoea, infiltrates), retinitis, marrow suppression | Managed by surveillance PCR and preemptive valganciclovir or foscarnet; universal prophylaxis with letermovir is increasingly used |
| Other opportunistic infection | Pneumocystis (PJP), invasive fungal (Aspergillus, Candida), HSV and VZV reactivation, adenovirus, respiratory viruses (RSV, influenza, parainfluenza) | Prophylaxis: co-trimoxazole for PJP, posaconazole for mould [7], aciclovir for HSV/VZV |
| Engraftment failure | Persistent cytopenias beyond day 28 (primary) or after initial recovery (secondary) | Assess chimerism; consider donor lymphocyte infusion, second transplant, or alternative donor in primary graft failure |
Late phase (beyond day 100) — chronic GVHD and the late effects
| Complication | Presentation | Key features |
|---|---|---|
| Chronic GVHD | Scleroderma-like skin thickening, lichenoid oral lesions and mucositis, sicca syndrome (dry eyes and mouth), hepatic cholestasis, oesophageal web and strictures, bronchiolitis obliterans (progressive dyspnoea), joint contractures, fasciitis, autoimmune cytopenias | NIH criteria for diagnosis and staging; first-line corticosteroid plus calcineurin inhibitor, second-line ruxolitinib (REACH3) [2], extracorporeal photopheresis, ibrutinib or belumosudil |
| Opportunistic infection | Encapsulated bacteria (pneumococcal sepsis), viral respiratory infections, fungal, CMV, EBV | Prophylaxis continues while immunosuppression continues — co-trimoxazole, penicillin V for splenic dysfunction or chronic GVHD, antiviral and antifungal cover |
| Secondary malignancy | Post-transplant lymphoproliferative disorder (EBV-driven, within months); solid tumours (skin, thyroid, breast, oral cavity) rising over years | PTLD: reduce immunosuppression then rituximab; solid tumour surveillance lifelong |
| Endocrine late effects | Hypothyroidism, gonadal failure and infertility, growth impairment in children, metabolic syndrome | Hormone replacement; fertility counselling before transplant; growth monitoring in paediatric survivors |
| Bone disease | Osteoporosis, avascular necrosis (hip, shoulder) | Bone density surveillance; bisphosphonate; arthroplasty for advanced AVN |
| Cardiovascular and psychosocial | Premature atherosclerosis, metabolic syndrome; anxiety, depression, sexual dysfunction, return-to-work challenges | Risk-factor modification, psychological support, sexual health counselling |
Differential diagnosis — distinguishing the transplant complications
The registrar on the transplant unit is constantly asked "is this GVHD, infection, drug toxicity, or relapse?" A structured approach to the differential saves time and lives. [1]
Jaundice in the first three weeks — is it veno-occlusive disease?
| Cause | Discriminating features |
|---|---|
| Veno-occlusive disease (SOS) | Weight gain (over 5 per cent), tender hepatomegaly, rising bilirubin within 21 days of conditioning; refractory ascites, renal and respiratory failure; modified Seattle or Baltimore criteria positive |
| Sepsis and cholestatic jaundice | Fever, positive cultures, hypotension; known infection focus |
| Drug hepatotoxicity | Cyclosporine, azoles, antibiotics, total parenteral nutrition; pattern varies by drug; improves on withdrawal |
| Acute GVHD of the liver | Usually after engraftment (day 14 onwards), often with skin and gut involvement; cholestatic pattern |
| Biliary disease | Right upper quadrant pain, fever; ultrasound for stones or sludge; considers fungal infection of the biliary tree in the immunocompromised |
| Viral hepatitis | Hepatitis B or C reactivation, adenovirus, HSV; viral PCR and serology |
DWE discriminator: The modified Seattle criteria for veno-occlusive disease require bilirubin over 34 micromol per litre plus two of hepatomegaly, ascites and weight gain of at least 5 per cent, occurring within 21 days of transplant. The Baltimore criteria are stricter, requiring bilirubin over 34 plus at least two of hepatomegaly, ascites, weight gain of at least 5 per cent. Calculate these criteria daily in the first three weeks — early defibrotide changes outcome [4].
Diarrhoea after transplant — is it acute GVHD?
| Cause | Discriminating features |
|---|---|
| Acute GVHD of the gut | Watery diarrhoea, often litre-volume, after engraftment, with or without skin and liver involvement; rectal biopsy shows epithelial apoptosis |
| Infectious colitis | Cytomegalovirus (PCR and biopsy), Clostridioides difficile (toxin assay), Campylobacter, Salmonella, norovirus, adenovirus; stool culture and PCR panel |
| Conditioning-related mucositis | Usually resolves within two weeks; upper GI symptoms predominate |
| Drug-related | Mycophenolate, antibiotics (especially broad-spectrum), magnesium, proton pump inhibitors |
| Engrament syndrome | Around neutrophil recovery, with rash and fever; self-limiting |
Rash after transplant — is it acute GVHD?
| Cause | Discriminating features |
|---|---|
| Acute GVHD of the skin | Maculopapular rash involving palms, soles and ears after engraftment; progresses to bullae and desquamation in severe disease |
| Drug rash | Morbilliform, often trunk and proximal limbs; temporally related to a new drug; eosinophilia may be present |
| Viral exanthem | HSV, VZV, measles, adenovirus; distribution and systemic features differ |
| Engraftment syndrome | Fever, rash, pulmonary infiltrates at neutrophil recovery; resolves spontaneously or with low-dose steroid |
| Sweet syndrome or leukaemia cutis | Relapse of underlying disease; skin biopsy required |
DWE high-yield: Acute GVHD rash characteristically involves the palms, soles and ears — areas often spared by ordinary drug rashes. A registrar who examines the palms and soles in a post-transplant patient with a rash is thinking correctly. [1]
Investigations
The pre-transplant workup
| Investigation | Why |
|---|---|
| Disease reassessment — marrow aspirate, imaging, measurable residual disease | Confirm remission or acceptable disease burden; transplant in active relapse has poor outcomes |
| HLA typing — patient and siblings (allogeneic); registry search if no matched sibling | Determines donor source; high-resolution typing at HLA-A, B, C, DRB1 |
| Comorbidity scoring — HCT-specific comorbidity index (HCT-CI) | Stratifies non-relapse mortality; informs conditioning intensity |
| Organ function — cardiac (ECG, echocardiogram), pulmonary (spirometry, gas transfer), renal (eGFR), hepatic (LFTs) | Baseline before potentially toxic conditioning; influences regimen choice |
| Viral serology — CMV, EBV, HSV, VZV, HBV, HCV, HIV | CMV serostatus determines surveillance strategy; HBV and HCV may need treatment before transplant |
| Fertility and psychosocial — sperm or oocyte banking, psychosocial assessment, caregiver planning | Fertility preservation before gonadotoxic conditioning; caregiver capacity is a transplant requirement |
| Dental review | Eliminate infection foci before profound neutropenia |
| Line placement and vaccination history | Central line for conditioning and infusion; revaccination plan post-transplant |
Monitoring during and after transplant
| Investigation | When | Why |
|---|---|---|
| Daily blood count | Throughout | Engraftment kinetics; cytopenia triggers transfusion |
| CMV quantitative PCR | Weekly from engraftment to day 100 (longer if high risk) | Preemptive therapy threshold; prevents symptomatic CMV disease |
| EBV viral load | In high-risk transplants (T-cell depleted, haploidentical, ATG) | Early detection of PTLD |
| Liver function, coagulation | Daily during conditioning, then regularly | Veno-occlusive disease surveillance |
| Skin, rectal or liver biopsy | When GVHD suspected | Histology of epithelial apoptosis; often non-specific but supports clinical diagnosis |
| Pulmonary function tests | Baseline and if symptomatic | Bronchiolitis obliterans surveillance in chronic GVHD |
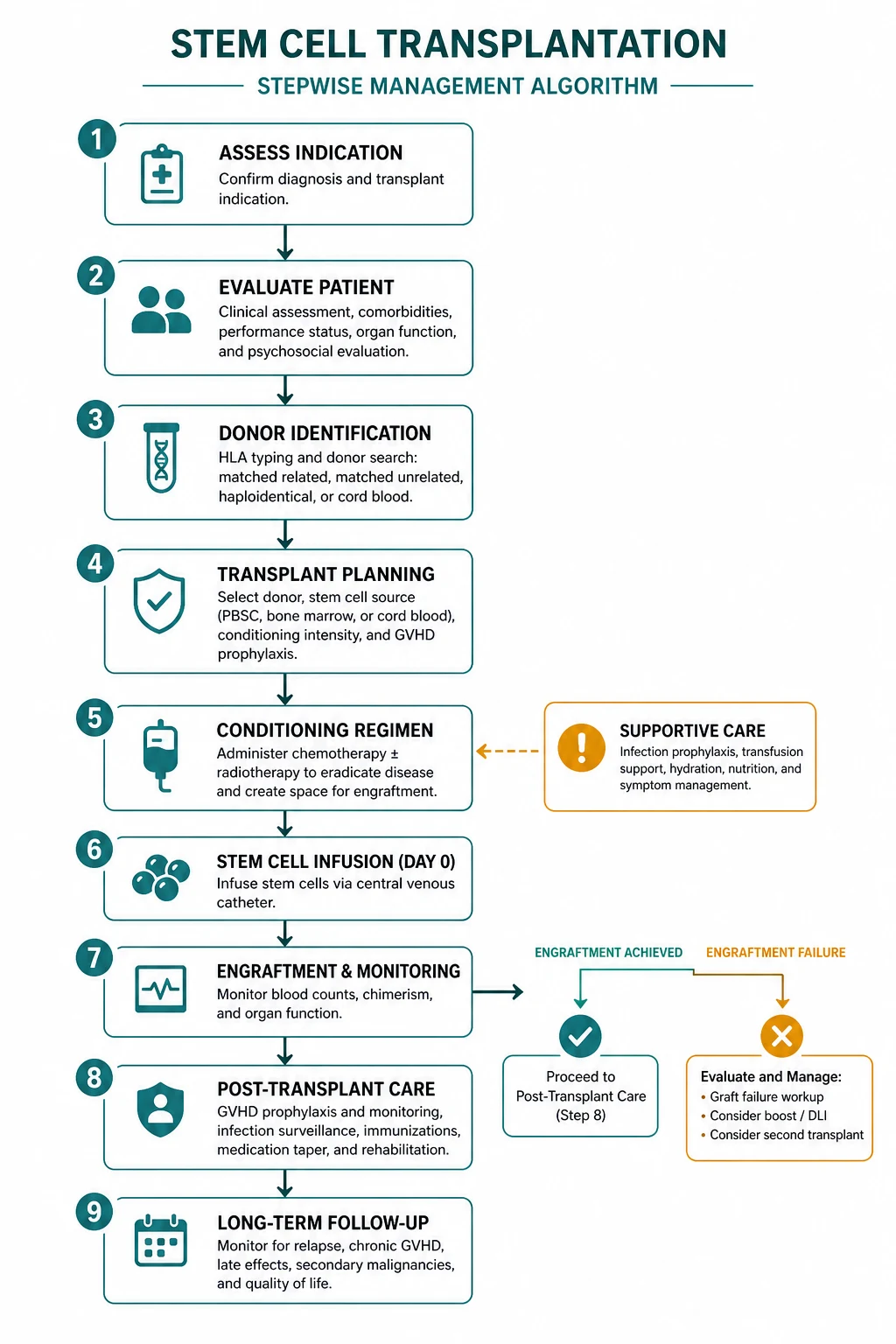
Management
Autologous transplant — the procedure
- Mobilisation — G-CSF 10 micrograms/kg per day subcutaneously, with plerixafor 240 micrograms/kg added for predicted or actual poor mobilisers.
- Collection by apheresis — target at least 2, and ideally over 5, million CD34-positive cells per kilogram. The product is cryopreserved.
- Conditioning — disease-specific. Melphalan 200 mg/m2 intravenously for myeloma; BEAM (carmustine, etoposide, cytarabine, melphalan) for lymphoma. [1]4. Infusion of the thawed cryopreserved graft on day 0.
- Supportive care through neutropenia — antimicrobial prophylaxis, transfusion, mucositis care, neutropenic fever pathway.
- Engraftment at 10 to 14 days; discharge once engrafted, afebrile, orally tolerant and safe. [1]
Allogeneic transplant — the procedure
- Donor selection — HLA-matched sibling first; otherwise matched unrelated donor (registry), haploidentical family donor (with post-transplant cyclophosphamide), or cord blood.
- Conditioning — myeloablative (TBI plus cyclophosphamide, or busulfan plus fludarabine), reduced-intensity (fludarabine plus melphalan or busulfan), or non-myeloablative.
- GVHD prophylaxis — calcineurin inhibitor (tacrolimus or cyclosporine) plus short-course methotrexate (days 1, 3, 6, 11) for matched donor; post-transplant cyclophosphamide 50 mg/kg on days 3 and 4 (with a calcineurin inhibitor) for haploidentical transplant; antithymocyte globulin added for unrelated donor in many protocols. [1]4. Infusion of fresh or cryopreserved graft on day 0.
- Engraftment at 12 to 20 days (slower with cord blood); chimerism at day 28.
- Long-term immunosuppression taper and surveillance for GVHD, infection, relapse and late effects. [1]
Neutropenic fever
The door-to-antibiotic time is a measurable survival determinant. On any fever in a neutropenic patient: [1]
- Cultures from each lumen of any central line and peripherally, plus urine and sputum.
- Empiric antipseudomonal beta-lactam — piperacillin-tazobactam 4.5 g intravenously, ceftazidime, or meropenem — within one hour. [1]- Add vancomycin for suspected line infection, haemodynamic instability, mucositis, or known colonization with resistant organisms.
- Assess for septic shock — early IV fluids, vasopressors and ICU as required.
- Do not delay antibiotics for imaging, review or results. [1]
Venous-occlusive disease (sinusoidal obstruction syndrome)
- Recognise early: calculate the modified Seattle or Baltimore criteria daily in the first three weeks.
- Supportive care: fluid and sodium restriction, analgesia, correction of coagulopathy (carefully — over-transfusion worsens volume overload), renal and respiratory support, paracentesis for tense ascites.
- Defibrotide 6.25 mg/kg intravenously every six hours for at least 21 days — the only agent with proven benefit in severe SOS with multiorgan failure. The phase 3 trial showed improved day 100 survival (38 versus 25 per cent against historical controls) [4].
Acute GVHD — grading and treatment

The Glucksberg-Przepiorka system stages each organ and combines them into an overall grade [9]:
| Overall grade | Skin (body surface area) | Liver (bilirubin, micromol/L) | Gut (diarrhoea volume) | Management |
|---|---|---|---|---|
| I (mild) | Stage 1 to 2 (under 50 per cent) | Stage 0 | Stage 0 | Topical steroid; continue prophylaxis |
| II (moderate) | Stage 1 to 3 | Stage 1 to 2 (34 to 102) | Stage 1 to 2 (over 1 litre per day, or persistent nausea) | Topical plus systemic corticosteroid 1 mg/kg per day |
| III (severe) | Stage 2 to 3 | Stage 2 to 3 (102 to 255) | Stage 2 to 3 (over 1.5 litres per day) | Methylprednisolone 1 to 2 mg/kg per day; early ruxolitinib if no response at day 28 |
| IV (life-threatening) | Stage 4 (generalised erythroderma with bullae and desquamation) | Stage 4 (over 255) | Stage 4 (severe abdominal pain with or without ileus or bleeding) | Methylprednisolone 2 mg/kg per day; ruxolitinib; consider extracorporeal photopheresis; palliative discussion in refractory disease |
First-line for grade II or higher acute GVHD is methylprednisolone 1 to 2 mg/kg per day, tapered on response. Second-line for steroid-refractory disease (progression after three days, or no response by day seven to 14) is ruxolitinib 5 to 10 mg twice daily, supported by the REACH1 (phase 2) and REACH2 (phase 3) trials [3][1]. REACH2 showed an overall response rate at day 28 of 62 per cent with ruxolitinib versus 39 per cent with best available therapy. Extracorporeal photopheresis is a steroid-sparing option, especially for skin and gut disease. Prophylaxis throughout is a calcineurin inhibitor (tacrolimus or cyclosporine) plus methotrexate or mycophenolate; for haploidentical transplant, post-transplant cyclophosphamide.
Chronic GVHD — diagnosis and treatment
Chronic GVHD is diagnosed by NIH criteria: diagnostic manifestations (poikiloderma, lichen sclerosis, joint stiffness, bronchiolitis obliterans) alone suffice, or distinctive manifestations confirmed on biopsy (lichenoid oral lesions, sicca, oesophageal web). It is staged by organ (0 to 3 across eight organs) into mild, moderate or severe global severity. [1]
- Mild — topical corticosteroid, topical calcineurin inhibitor; continued prophylactic immunosuppression.
- Moderate to severe — systemic corticosteroid (prednisolone 1 mg/kg per day) plus a calcineurin inhibitor; wean as tolerated.
- Steroid-refractory — ruxolitinib 10 mg twice daily (REACH3 showed an overall response rate at week 24 of 50 per cent versus 26 per cent with best available therapy) [2], extracorporeal photopheresis, ibrutinib, belumosudil, or abatacept for selected cases.
Opportunistic infection prophylaxis
| Infection | Prophylaxis | Duration |
|---|---|---|
| Pneumocystis (PJP) | Co-trimoxazole 480 mg daily (or 960 mg three times weekly); alternatives include dapsone, atovaquone or pentamidine inhalation | At least six months, and longer while on immunosuppression |
| HSV and VZV | Aciclovir 400 mg twice daily (or valaciclovir) | At least one year, longer if chronic GVHD |
| Fungal (Candida, Aspergillus) | Posaconazole 200 mg three times daily or 300 mg once daily (delayed release); fluconazole is inadequate for mould cover in GVHD [7] | During neutropenia and during systemic corticosteroid for GVHD |
| CMV | Letermovir 480 mg daily (universal prophylaxis increasingly used in seropositive recipients); otherwise surveillance PCR with preemptive valganciclovir or foscarnet | Day 0 to day 100, longer if high risk |
CMV reactivation — preemptive therapy
- Monitor quantitative whole blood CMV PCR weekly from engraftment to day 100, and longer in high-risk patients (seropositive recipient, T-cell depletion, haploidentical, steroid-treated GVHD).
- A rising PCR or a threshold viral load triggers preemptive therapy — valganciclovir 900 mg twice daily for 14 to 21 days then maintenance once daily until one or two negative PCRs, or intravenous ganciclovir, or foscarnet for ganciclovir resistance or myelosuppression.
- Continue PCR monitoring during and after therapy, with secondary prophylaxis in high-risk patients.
- Symptomatic CMV disease (colitis, pneumonitis, retinitis, marrow suppression) is treated as disease, not as reactivation — higher threshold and longer therapy. [1]
Post-transplant lymphoproliferative disorder
EBV-driven, occurs in T-cell depleted, haploidentical, or ATG-containing transplants and in patients on heavy immunosuppression. Monitor EBV viral load in high-risk patients. The diagnosis is made by imaging for masses, tissue biopsy showing a lymphoid proliferation, flow cytometry and EBV-encoded RNA in situ hybridisation. [1]
Management: first, reduce immunosuppression as far as the underlying disease and GVHD risk permit. Second, rituximab 375 mg/m2 weekly for four doses. Cytotoxic chemotherapy (such as CHOP) is reserved for refractory or aggressive CD20-negative disease. [1]
Late effects — the survivorship clinic
The long-term transplant survivor is a chronic-disease patient. The survivorship clinic addresses: [1]
- Infection prophylaxis — wean off at six months if no chronic GVHD; continue indefinitely in chronic GVHD or ongoing immunosuppression.
- Vaccination — revaccinate from six months (influenza annually, pneumococcal, Haemophilus influenzae, hepatitis B, tetanus, polio); live vaccines (measles-mumps-rubella, varicella) only when off immunosuppression and at least two years post-transplant.
- Endocrine — annual thyroid function; gonadal hormone replacement for premature ovarian or testicular failure; growth monitoring in children.
- Bone density — baseline and serial DEXA; bisphosphonate for osteoporosis; consider avascular necrosis surveillance in patients on prolonged steroids.
- Secondary malignancy — annual skin examination; thyroid ultrasound; breast cancer screening from eight years post-transplant or age 40 (whichever first) for patients who received chest radiation; oral cavity examination.
- Cardiovascular — aggressive risk-factor modification; consider the transplant survivor as a high-risk patient.
- Psychosocial and sexual health — anxiety, depression, return to work, sexual function, relationships, fertility — address explicitly at each visit. [1]
Long-term outcomes and prognosis
| Setting | Approximate outcome |
|---|---|
| Autologous HSCT for multiple myeloma (with modern induction and lenalidomide maintenance) | Median overall survival 5 to 7 years; transplant-related mortality under 2 per cent |
| Autologous HSCT for relapsed Hodgkin lymphoma | 5-year progression-free survival 50 to 60 per cent with salvage and transplant |
| Allogeneic HSCT for AML in first complete remission | 5-year overall survival 50 to 70 per cent (favourable risk), 40 to 60 per cent (intermediate), 20 to 30 per cent (adverse) |
| Allogeneic HSCT for ALL in first complete remission (high risk) | 5-year overall survival 40 to 60 per cent in adults |
| Severe acute GVHD (grade III to IV) | Mortality 50 to 70 per cent for grade IV despite modern therapy |
| Severe chronic GVHD | Substantial morbidity; mortality driven by infection and bronchiolitis obliterans |
| Severe veno-occlusive disease with multiorgan failure | Mortality 80 to 100 per cent without defibrotide; 30 to 50 per cent with early defibrotide [4] |
| Allogeneic HSCT for aplastic anaemia (young, matched sibling) | 5-year overall survival over 85 per cent |
Common exam traps and high-yield discriminators
- Autologous has no GVHD. A vignette that asks about a rash or diarrhoea after an autologous transplant is pointing to drug, infection or engraftment syndrome — not GVHD. This is a guaranteed MCQ trap.
- The 100-day boundary. Acute GVHD is within 100 days; chronic GVHD is after 100 days. A vignette describing a scleroderma-like rash at day 140 is chronic GVHD, not acute.
- CMV is managed by surveillance and preemptive therapy, not universal prophylaxis (although letermovir prophylaxis in seropositive recipients is increasingly standard). A rising PCR triggers valganciclovir or foscarnet before symptomatic disease.
- Veno-occlusive disease triad — weight gain, tender hepatomegaly, rising bilirubin within 21 days of conditioning. The treatment is defibrotide. A registrar who attributes the picture to "sepsis" or "drug" without applying the criteria misses the window.
- Post-transplant cyclophosphamide is given on days 3 and 4 after a haploidentical transplant — not before. It selectively deletes alloreactive T-cells while sparing regulatory T-cells. This is exam law and a common MCQ discriminator.
- PJP prophylaxis with co-trimoxazole continues for at least six months and longer with chronic GVHD or ongoing immunosuppression. Stopping at the standard time in a chronic GVHD patient is a common error.
- The GVL effect is why allogeneic can cure what autologous cannot. Donor lymphocyte infusion exploits the GVL effect to reinduce remission in relapsed disease. A registrar who understands GVL understands why allogeneic transplant is curative despite its toxicity. [1]- The conditioning regimens to memorise. Myeloablative: TBI plus cyclophosphamide, or busulfan plus cyclophosphamide or fludarabine. Reduced-intensity: fludarabine plus melphalan or busulfan. Autologous myeloma: melphalan 200. Autologous lymphoma: BEAM. Do not confuse them.
- Engraftment thresholds. Neutrophils over 0.5 for three consecutive days. Platelets over 20 unsupported. Typically 10 to 20 days. A guaranteed MCQ.
- The survivorship plan is the long-case differentiator. The candidate who addresses infection prophylaxis, vaccination, endocrine replacement, bone density, malignancy surveillance and psychosocial health demonstrates the integrated care the DCE long case rewards. [1]
Regional guideline anchoring
- ANZ primary: HSANZ (Haematology Society of Australia and New Zealand) clinical practice guidelines; eviQ protocols for mobilisation, conditioning, GVHD prophylaxis and supportive care.
- UK secondary: BSH (British Society for Haematology) stem cell transplantation guidelines; EBMT (European Society for Blood and Marrow Transplantation) handbook.
- US tertiary: NCCN guidelines for haematopoietic growth factors, prevention of infections, and transplant indications; ASBMT (now ASTCT) consensus.
- Global: WHO and EBMT activity surveys; CIBMTR (Center for International Blood and Marrow Transplant Research) registry outcomes. [1]
References and further reading
EBMT Handbook of Haematopoietic Stem Cell Transplantation; HSANZ and eviQ clinical protocols; NCCN Clinical Practice Guidelines in Oncology (Hematopoietic Growth Factors; Prevention of Infections); ASH Education Program — Stem Cell Transplantation; CIBMTR registry outcome reports. [1]
References
- [1]Zeiser R, von Bubnoff N, Butler J, et al. Ruxolitinib for Glucocorticoid-Refractory Acute Graft-versus-Host Disease N Engl J Med, 2020.PMID 32320566
- [2]Zeiser R, Lee SJ, Padmanabhan S, et al. Ruxolitinib for Glucocorticoid-Refractory Chronic Graft-versus-Host Disease N Engl J Med, 2021.PMID 34260836
- [3]Jagasia M, Perales MA, Schroeder MA, et al. Ruxolitinib for the treatment of steroid-refractory acute GVHD (REACH1): a multicenter, open-label phase 2 trial Blood, 2020.PMID 32160294
- [4]Richardson PG, Riches ML, Kass SL, et al. Phase 3 trial of defibrotide for the treatment of severe veno-occlusive disease and multi-organ failure Blood, 2016.PMID 26825712
- [5]DiPersio JF, Stadtmauer EA, Nademanee A, et al. Plerixafor and G-CSF versus placebo and G-CSF to mobilize hematopoietic stem cells for autologous stem cell transplantation in patients with multiple myeloma Blood, 2009.PMID 19363221
- [6]DiPersio JF, Micallef IN, Stiff PJ, et al. Phase III prospective randomized double-blind placebo-controlled trial of plerixafor plus granulocyte colony-stimulating factor compared with placebo plus granulocyte colony-stimulating factor for autologous stem-cell mobilization and transplantation for patients with non-Hodgkin's lymphoma J Clin Oncol, 2009.PMID 19720922
- [7]Ullmann AJ, Lipton JH, Vesole DH, et al. Posaconazole or fluconazole for prophylaxis in severe graft-versus-host disease N Engl J Med, 2007.PMID 17251530
- [8]McCurdy SR, Luznik L How we perform haploidentical stem cell transplantation with posttransplant cyclophosphamide Blood, 2019.PMID 31751485
- [9]Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading Bone Marrow Transplant, 1995.PMID 7581076
- [10]Russell JA, Tran HT, Quinlan D, et al. Once-daily intravenous busulfan given with fludarabine as conditioning for allogeneic stem cell transplantation: study of pharmacokinetics and early clinical outcomes Biol Blood Marrow Transplant, 2002.PMID 12374451