Phys · haematological
Thrombophilia and Venous Thromboembolism
Also known as venous thromboembolism · VTE · deep vein thrombosis · DVT · pulmonary embolism · thrombophilia · Factor V Leiden · antiphospholipid syndrome · APS · heparin-induced thrombocytopenia · HIT · prothrombin G20210A · protein C deficiency · protein S deficiency · antithrombin deficiency · lupus anticoagulant
Consultant-physician-depth guide to inherited and acquired thrombophilia and venous thromboembolism (VTE) for FRACP DWE and DCE — Factor V Leiden and prothrombin G20210A, protein C/S and antithrombin deficiency, antiphospholipid syndrome (lupus anticoagulant, anticardiolipin, beta-2 glycoprotein I), when to test and when not to test, DVT diagnosis (Wells score, D-dimer, compression ultrasound), DOACs first-line, warfarin for APS, LMWH for pregnancy and cancer, HIT (4T score, PF4 antibody), cerebral and splanchnic vein thrombosis, and the TRAPS, EINSTEIN-CHOICE, SELECT-D, Hokusai-CANVAS and Caravaggio trials.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Thrombophilia and Venous Thromboembolism
The answer first
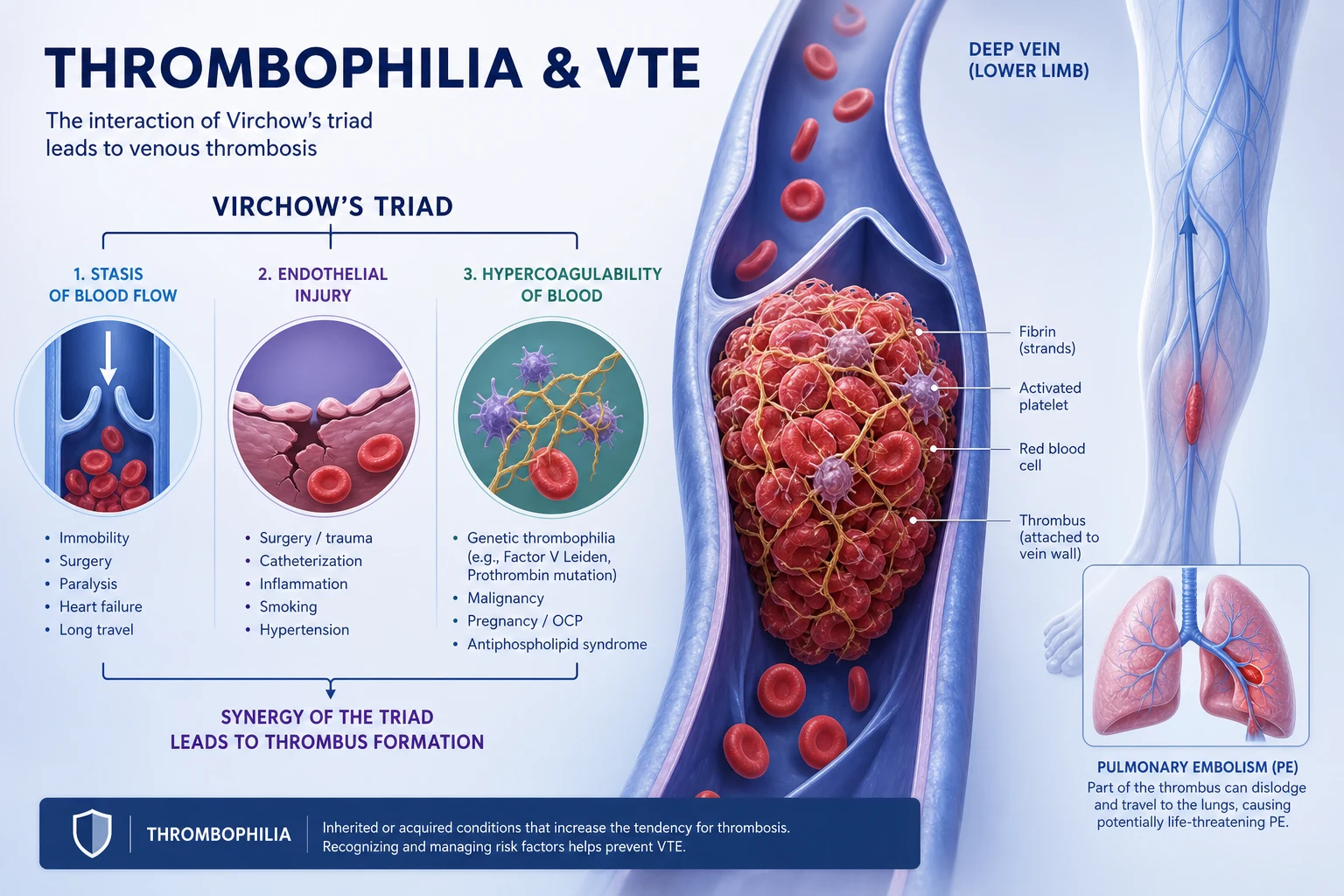
Venous thromboembolism (VTE) — deep vein thrombosis (DVT) and pulmonary embolism (PE) — arises when Virchow's triad (venous stasis, endothelial injury, hypercoagulability) converges. Most clots are provoked by a transient risk factor (surgery, immobility, cancer, pregnancy, oestrogen). A minority occur unprovoked, and it is in this group that a thrombophilia — inherited or acquired — may be lurking. The diagnosis of DVT rests on the Wells pretest probability combined with D-dimer and compression ultrasound [4].
Two bedside rules that change outcome: [1]
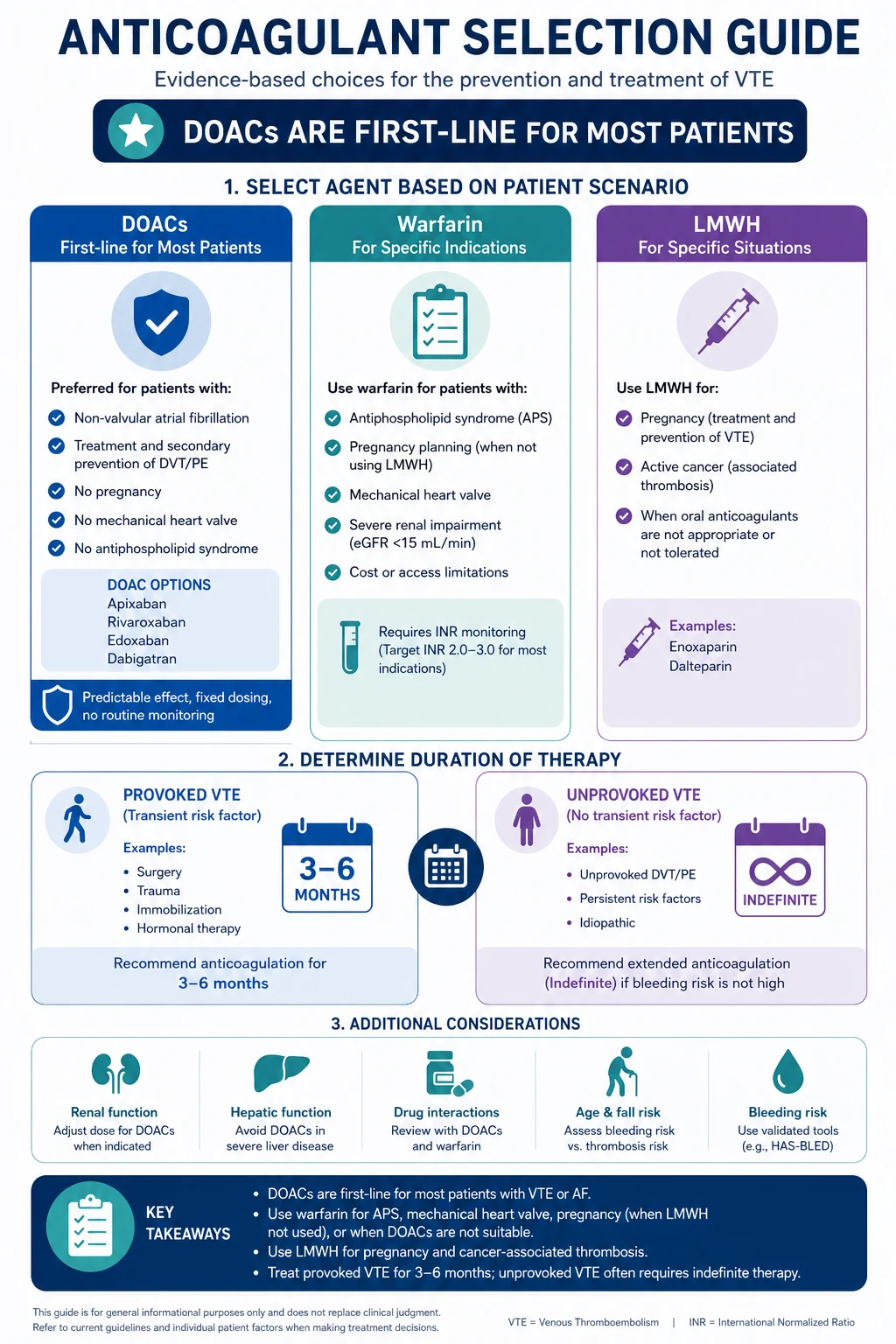
- First-line anticoagulation is a DOAC (apixaban, rivaroxaban, dabigatran or edoxaban), not warfarin, for most patients with VTE — UNLESS there is antiphospholipid syndrome, pregnancy, a mechanical heart valve, or severe renal failure. In triple-positive APS, warfarin is preferred because the TRAPS trial showed excess thrombosis with rivaroxaban [6].
- Duration follows the trigger. Provoked VTE gets 3 to 6 months. Unprovoked VTE gets at least 6 months, with consideration of indefinite therapy if bleeding risk is acceptable. Cancer-associated VTE is indefinite while the cancer is active.
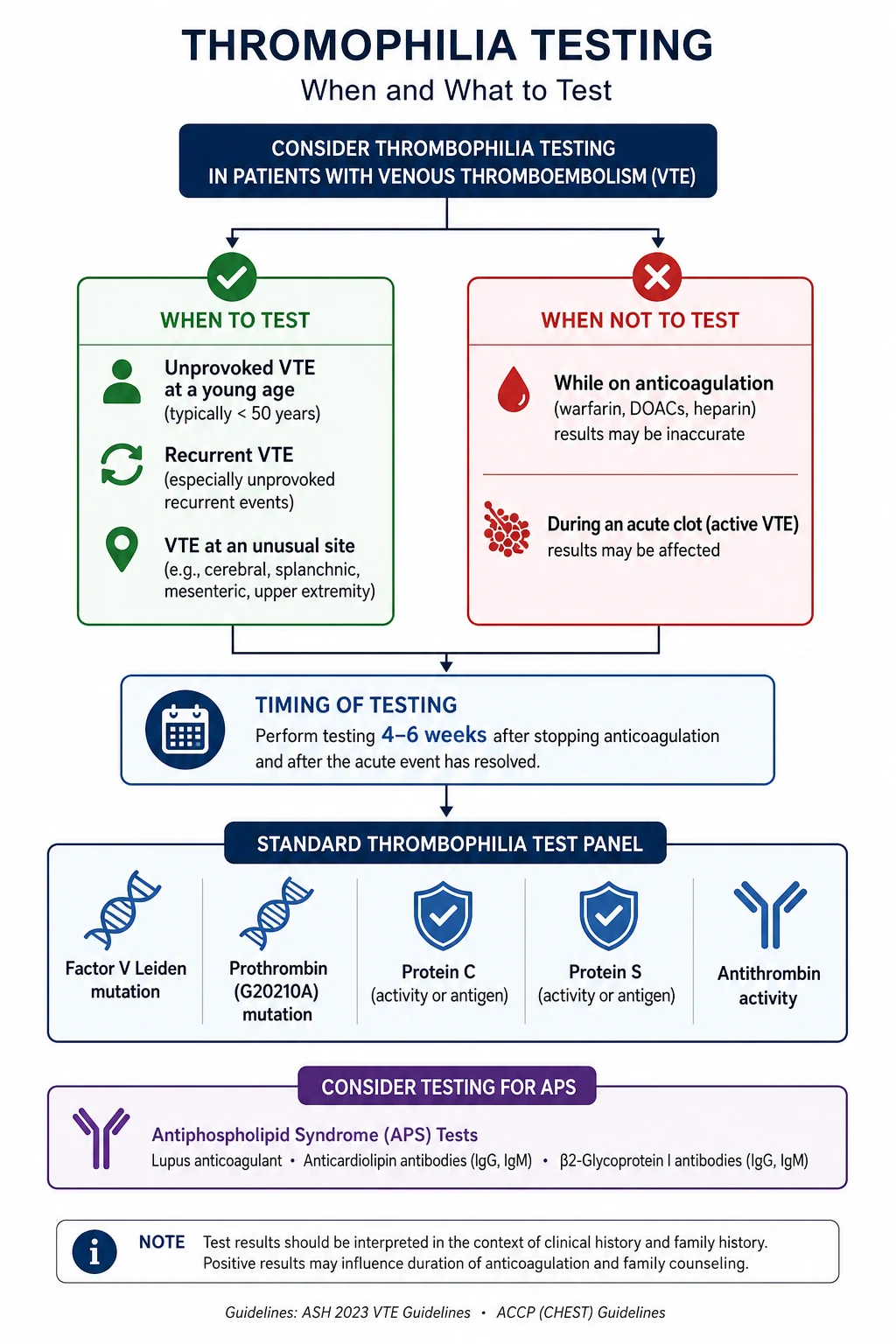
Thrombophilia testing is not a blanket investigation. It is reserved for selected patients — unprovoked VTE at a young age, recurrent events, unusual sites (cerebral, splanchnic), and a strong family history — and it must be timed correctly: not during the acute clot or while on anticoagulation, because both distort the assays. Test 4 to 6 weeks after stopping anticoagulation if practical [3].
Epidemiology and risk factors
Virchow's triad — the unifying framework
Every venous clot can be traced to one or more arms of Virchow's triad: [1]
| Arm of triad | Mechanism | Common clinical triggers |
|---|---|---|
| Venous stasis | Slowed blood flow allows clotting factors to accumulate | Immobility, surgery, long-haul travel, plaster cast, heart failure, obesity |
| Endothelial injury | Damage exposes tissue factor and subendothelial collagen | Surgery, trauma, fractures, indwelling catheters, previous VTE |
| Hypercoagulability | Increased clotting tendency — inherited or acquired | Thrombophilia, cancer, pregnancy, oestrogen, sepsis, inflammatory disease |
Transient (provoking) risk factors
These are the commonest causes of VTE and carry a finite, reversible risk: [1]
- Surgery — especially major orthopaedic (hip and knee replacement), major abdominal, and cancer surgery. The risk is highest in the first 2 to 4 weeks.
- Hospitalisation and immobility — the dominant risk in medical inpatients; the rationale for VTE prophylaxis (LMWH or mechanical).
- Cancer — active malignancy increases VTE risk 4- to 7-fold, and cancer-associated VTE requires long-term, often indefinite, anticoagulation.
- Pregnancy and the puerperium — a hypercoagulable state driven by increased fibrinogen and factors VII, VIII and X, plus venous stasis from the gravid uterus. The puerperium carries the highest risk.
- Oestrogen therapy — combined oral contraceptive pill and hormone replacement therapy both increase VTE risk 2- to 4-fold.
- Long-haul travel — risk increases after flights over 4 hours, especially in those with other risk factors. [1]
Persistent risk factors
These carry ongoing risk and often justify extended or indefinite anticoagulation: [1]
- Active cancer — see cancer-associated VTE below.
- Inherited thrombophilia — see below.
- Antiphospholipid syndrome — an acquired thrombophilia that mandates warfarin, not DOACs, in high-risk patients.
- Chronic medical conditions — heart failure, chronic obstructive pulmonary disease, inflammatory bowel disease, nephrotic syndrome, myeloproliferative neoplasms. [1]
DWE conceptual: The key clinical question is not "does this patient have a clot?" (a diagnostic question answered by Wells score and imaging) but "why did this clot occur, and what is the risk of recurrence?" The answer to the second question determines the duration of anticoagulation and whether to test for thrombophilia. [1]
Inherited thrombophilias
Inherited thrombophilias are genetic variants that increase the tendency to venous thrombosis. They are divided into low-penetrance (common, modest risk — Factor V Leiden, prothrombin G20210A) and high-penetrance (rare, high risk — antithrombin, protein C, protein S deficiency). The important point for the physician is that finding a low-penetrance thrombophilia rarely changes management, because the duration of anticoagulation is driven by the clinical event, not the genotype. [1]
Factor V Leiden — the most common inherited thrombophilia
Factor V Leiden is a point mutation (G1691A) in the Factor V gene that substitutes glutamine for arginine at position 506. This residue is one of the sites where activated protein C cleaves and inactivates Factor Va. The mutation makes Factor V resistant to activated protein C (APC resistance), so the procoagulant Factor Va persists longer, generating more thrombin [1].
- Prevalence: about 5 per cent of Caucasian populations (the highest of any inherited thrombophilia); rare in African, Asian and Indigenous populations.
- Heterozygotes: relative risk of VTE about 3- to 8-fold compared with non-carriers. Absolute annual risk is low — about 1 per cent per year.
- Homozygotes: relative risk up to 80-fold; a more aggressive thrombophilia.
- Inheritance: autosomal dominant with incomplete penetrance. Most heterozygous carriers never have a thrombosis. [1]
Prothrombin G20210A mutation
A G-to-A substitution at nucleotide 20210 in the 3-prime-untranslated region of the prothrombin gene, leading to elevated plasma prothrombin levels and a hypercoagulable state [2].
- Prevalence: about 2 to 3 per cent of Caucasian populations; second most common inherited thrombophilia after Factor V Leiden.
- Relative risk of VTE: about 2- to 5-fold for heterozygotes.
- Inheritance: autosomal dominant with incomplete penetrance. [1]
Protein C, protein S and antithrombin deficiency — high-penetrance thrombophilias
These three are less common but carry a higher risk of thrombosis and a stronger family history: [1]
| Deficiency | Mechanism | Prevalence | Relative VTE risk | Key points |
|---|---|---|---|---|
| Antithrombin deficiency | Antithrombin is the natural inhibitor of thrombin and Factor Xa; deficiency removes a key brake on coagulation | Rare (about 0.02 per cent) | 10- to 50-fold | Highest-risk inherited thrombophilia; may be resistant to heparin |
| Protein C deficiency | Protein C (activated by thrombomodulin-thrombin) inactivates Factors Va and VIIIa; deficiency allows sustained coagulation | About 0.2 per cent | 5- to 10-fold | Warfarin can cause skin necrosis if started without heparin overlap; a pharmacology trap |
| Protein S deficiency | Protein S is the cofactor for activated protein C; its deficiency mimics protein C deficiency functionally | About 0.1 to 0.2 per cent | 5- to 10-fold | Levels fall in pregnancy and with oestrogen — difficult to interpret in these states |
DWE high-yield trap: Warfarin-induced skin necrosis occurs in protein C deficiency because warfarin depletes the vitamin K-dependent natural anticoagulants (protein C and S) within 24 to 48 hours — before it depletes the procoagulant factors (II, VII, IX, X, which have longer half-lives). This creates a transient procoagulant window. The answer is to start warfarin only after the patient is therapeutic on heparin (overlap for at least 5 days and until INR is therapeutic for 2 consecutive days) and to avoid loading doses. [1]
Penetrance and the family history
The most important concept in inherited thrombophilia is variable penetrance. Two siblings with the same Factor V Leiden heterozygous mutation may have entirely different clinical courses — one with multiple clots by age 40, the other never thrombosing. Penetrance is modified by co-existing risk factors (oestrogen, obesity, surgery, additional thrombophilic mutations). This is why a family history of VTE in a first-degree relative is itself a risk factor regardless of genotype. [1]
Acquired thrombophilia — antiphospholipid syndrome (APS)
APS is the most important acquired thrombophilia and the only one that routinely changes the choice of anticoagulant. It is defined by the Sydney (revised Sapporo) criteria, which require at least one clinical criterion AND one laboratory criterion, with the laboratory test positive on two occasions at least 12 weeks apart [3].
Classification criteria
Clinical criteria (one or more): [1]
- Vascular thrombosis — one or more clinical episodes of arterial, venous or small-vessel thrombosis, in any tissue or organ, confirmed by imaging or histology.
- Pregnancy morbidity — one of: (a) three or more unexplained consecutive spontaneous miscarriages before 10 weeks; (b) one or more unexplained fetal deaths at or beyond 10 weeks; (c) one or more premature births before 34 weeks due to eclampsia, severe pre-eclampsia or placental insufficiency. [1]
Laboratory criteria (one or more, on two or more occasions at least 12 weeks apart): [1]
- Lupus anticoagulant (LA) — detected by a panel of phospholipid-dependent coagulation tests (e.g. dilute Russell viper venom time, activated partial thromboplastin time) that fail to correct on mixing study but correct with excess phospholipid.
- Anticardiolipin antibodies — IgG and/or IgM in medium or high titre (over 40 GPL/MPL or above the 99th percentile).
- Anti-beta-2 glycoprotein I antibodies — IgG and/or IgM in titre above the 99th percentile. [1]
The paradox of the lupus anticoagulant
The lupus anticoagulant is so named because it prolongs phospholipid-dependent coagulation tests in the laboratory (aPTT, dRVVT) — it appears anticoagulant in vitro. But in the body it is prothrombotic. This paradox is a favourite exam question. The mechanism: these antibodies bind beta-2 glycoprotein I and prothrombin on phospholipid surfaces, interfering with the natural anticoagulant and fibrinolytic pathways, activating complement, and triggering endothelial and platelet activation. [1]
DWE high-yield trap: A patient with a prolonged aPTT that does not correct on mixing study AND a history of thrombosis — think lupus anticoagulant / APS. The prolonged aPTT is not a bleeding tendency; it is a marker of a prothrombotic antibody. [1]
Clinical features of APS
- Venous thrombosis — DVT and PE are the commonest manifestations.
- Arterial thrombosis — stroke and transient ischaemic attack in a young person are a hallmark; APS should be in the differential of any young patient with an unexplained stroke.
- Recurrent pregnancy loss — the specific pregnancy morbidity pattern defined in the criteria.
- Thrombocytopenia — often mild, 100 to 150.
- Livedo reticularis — a mottled, net-like skin discolouration; a useful bedside clue.
- Cardiac valve lesions — Libman-Sacks endocarditis (non-bacterial verrucous vegetations).
- Nephropathy — renal vascular thrombosis and thrombotic microangiopathy. [1]
Catastrophic APS — a medical emergency
Catastrophic APS (CAPS) affects less than 1 per cent of APS patients but carries a mortality of 30 to 50 per cent. It is defined by thrombosis in three or more organs systems simultaneously or within one week, with histopathological confirmation of microvascular thrombosis and persistent antiphospholipid antibodies. The presentation is multi-organ failure — renal, cerebral, pulmonary, cardiac, cutaneous, adrenal. Precipitants include infection, surgery, pregnancy and withdrawal of anticoagulation. [1]
The treatment of CAPS is combination therapy: therapeutic anticoagulation, high-dose corticosteroids, plasma exchange and intravenous immunoglobulin (IVIG). Early recognition and aggressive treatment in an intensive care setting is essential. This is a viva favourite. [1]
When to test for thrombophilia (and when not to)
Thrombophilia testing is one of the most over-requested investigations in general medicine. The question is not just whom to test, but when and why — the result must be something that changes management. [1]
Who SHOULD be tested
| Clinical scenario | Why test |
|---|---|
| Unprovoked VTE at a young age (under 50) | Higher yield of inherited thrombophilia; may affect family counselling and duration decisions |
| Recurrent VTE (especially unprovoked, or despite anticoagulation) | Raises suspicion of APS or high-penetrance thrombophilia |
| VTE at an unusual site — cerebral venous sinus, splanchnic (portal, mesenteric, hepatic), renal | These sites are strongly associated with APS and myeloproliferative neoplasms |
| Strong family history — one or more first-degree relatives with VTE at a young age | May identify a high-penetrance deficiency (antithrombin, protein C, protein S) |
| Recurrent pregnancy loss or late pregnancy loss | Screen for APS — a positive result changes pregnancy management |
| Arterial thrombosis at a young age — unexplained stroke, MI under 50 | Screen for APS |
Who should NOT be tested (or testing will not change management)
- VTE provoked by a major transient risk factor (surgery, trauma, prolonged immobility) — the recurrence risk is low and a thrombophilia result does not change the 3- to 6-month duration.
- Elderly patients with first VTE — low yield of inherited thrombophilia; management is dictated by the clinical scenario.
- Asymptomatic relatives of patients with low-penetrance thrombophilia (heterozygous Factor V Leiden or prothrombin G20210A) — the absolute risk is too low to justify prophylactic anticoagulation; counselling on risk avoidance (oestrogen, smoking, hydration) is more useful. [1]
When to test — the timing trap
Thrombophilia testing must be timed correctly because both the acute thrombotic event and the anticoagulant drugs distort the assays: [1]
| Factor | Distortion | Corrective action |
|---|---|---|
| Acute thrombosis | Consumes antithrombin, protein C and protein S — falsely low levels | Wait until the acute event has settled (at least 2 to 4 weeks) |
| Heparin (UFH and LMWH) | Lower antithrombin levels; interferes with LA assays | Do not interpret antithrombin or LA while on heparin |
| Warfarin | Lowers protein C and protein S (vitamin K dependent); interferes with LA through vitamin K-dependent factor depletion | Do not interpret protein C, S, or LA on warfarin; retest 4 to 6 weeks after stopping |
| DOACs | Can interfere with LA assays and clot-based assays, producing false positives | Stop the DOAC for at least 2 to 3 days before testing (or longer with renal impairment) |
| Pregnancy and oestrogen | Lower protein S levels | Do not interpret protein S deficiency in pregnancy or on the OCP |
DWE high-yield trap: The single most common error is ordering a thrombophilia screen (including protein C, protein S and antithrombin) in a patient who is actively thrombosing and on heparin or warfarin. The results will be misleadingly low, leading to false diagnoses and unnecessary anxiety. The correct approach is to defer testing until the acute event has resolved and anticoagulation has been paused for at least 4 to 6 weeks, or to test selectively (Factor V Leiden and prothrombin G20210A are genetic tests that are NOT affected by anticoagulation or acute thrombosis — these can be done at any time). [1]
DVT diagnosis
The Wells pretest probability score
The Wells score stratifies patients with suspected DVT into low, moderate and high probability. It was validated in the landmark 1997 Lancet study that combined clinical assessment with compression ultrasound [4].
| Component | Points |
|---|---|
| Active cancer (treatment within 6 months or palliative) | 1 |
| Paralysis, paresis or recent plaster cast immobilisation of lower extremity | 1 |
| Recently bedridden 3 or more days or major surgery within 12 weeks requiring general or regional anaesthesia | 1 |
| Localised tenderness along the distribution of the deep venous system | 1 |
| Entire leg swollen | 1 |
| Calf swelling 3 cm or more larger than the asymptomatic side (measured 10 cm below the tibial tuberosity) | 1 |
| Pitting oedema confined to the symptomatic leg | 1 |
| Collateral non-varicose superficial veins | 1 |
| Previously documented DVT | 1 |
| Alternative diagnosis at least as likely as DVT | subtract 2 |
Interpretation: [1]
- 0 or less — DVT unlikely (probability about 5 per cent). Check D-dimer; if negative, DVT excluded; if positive, do ultrasound.
- 1 or more — DVT likely (probability about 30 per cent). Proceed directly to compression ultrasound (D-dimer not helpful in this group because a positive result does not adequately lower the probability). [1]
D-dimer
D-dimer is a fibrin degradation product. It is highly sensitive (a negative result usefully rules out VTE in low-probability patients) but poorly specific (elevated in cancer, pregnancy, infection, inflammation, post-surgery, and advancing age). A D-dimer is only useful when it is negative in a patient with a low pretest probability. A positive D-dimer in a high-probability patient adds nothing. [1]
DWE conceptual: The D-dimer is a "rule-out" test, not a "rule-in" test. Ordering it in a high-probability patient is unhelpful because a negative result is unlikely and a positive result does not confirm DVT. The combination that safely excludes DVT is: low pretest probability (Wells 0 or less) AND negative D-dimer. [1]
Compression ultrasound
The gold standard imaging for proximal DVT is whole-leg or proximal compression ultrasonography. The diagnosis rests on non-compressibility of the deep veins (the probe cannot compress the vein lumen — it is filled with clot). A negative ultrasound in a high-probability patient should be repeated at 1 week to catch an extending calf clot. [1]
Differential of a swollen leg
| Condition | Discriminating features |
|---|---|
| Cellulitis | Erythema, warmth, systemic features (fever, leucocytosis); unilateral; often a skin break or tinea pedis entry |
| Ruptured Baker cyst | Sudden calf pain, often with a history of knee osteoarthritis; pseudothrombophlebitis |
| Heart failure | Bilateral, dependent oedema; elevated JVP, basal crackles |
| Lymphoedema | Non-pitting, chronic, usually bilateral; Stemmer sign positive (inability to pinch the skin at the base of the second toe) |
| Post-phlebitic syndrome | Chronic leg swelling, pain, discolouration after a previous DVT; a common long-term complication |
| Compartment syndrome | Pain out of proportion, tense leg, paraesthesia, decreased pulses — a surgical emergency |
Pulmonary embolism diagnosis
PE shares the same diagnostic framework as DVT — a pretest probability score (Wells or revised Geneva for PE), D-dimer for low-probability cases, and imaging. The imaging of choice is CT pulmonary angiography (CTPA), which directly visualises the filling defect in the pulmonary arterial tree. [1]
Cross-reference the pulmonary embolism topic for the full diagnostic algorithm, the PERC rule, the YEARS algorithm, risk stratification (simplified PESI), and the decision to thrombolyse, anticoagulate or consider embolectomy. [1]
DWE discriminator: Massive PE with haemodynamic instability (hypotension, shock) is treated with systemic thrombolysis (alteplase) if there are no absolute contraindications — do not delay for confirmatory imaging if the patient is critically unstable. Submassive PE (right ventricular strain on imaging or biomarkers, but normotensive) is a nuanced decision — anticoagulation first, with thrombolysis reserved for deterioration. [1]
Anticoagulation — the agents
Direct oral anticoagulants (DOACs) — first-line for most VTE
DOACs (also called NOACs or direct-acting oral anticoagulants) have replaced warfarin as first-line therapy for most patients with VTE. They include: [1]
| Agent | Class | Mechanism | Standard dosing for VTE | Renal clearance |
|---|---|---|---|---|
| Apixaban | Factor Xa inhibitor | Directly inhibits Factor Xa | 10 mg twice daily for 7 days, then 5 mg twice daily | About 27 per cent renal |
| Dabigatran | Direct thrombin inhibitor | Binds and inhibits thrombin | 150 mg twice daily (after 5 to 10 days of parenteral anticoagulation) | About 80 per cent renal |
| Edoxaban | Factor Xa inhibitor | Directly inhibits Factor Xa | 60 mg once daily (after 5 to 10 days of parenteral anticoagulation) | About 50 per cent renal |
DWE pharmacology: Apixaban and rivaroxaban can be started immediately at diagnosis without a lead-in of heparin (they are "single-drug approach"). Dabigatran and edoxaban require 5 to 10 days of parenteral anticoagulation (LMWH or unfractionated heparin) before switching — starting them immediately is ineffective because they take time to reach steady state. This is a common MCQ discriminator. [1]
Advantages of DOACs over warfarin: fixed dosing, no routine INR monitoring, fewer drug and food interactions, lower rates of major bleeding (especially intracranial haemorrhage), and faster onset/offset. [1]
Limitations of DOACs: not suitable for pregnancy (teratogenic), not preferred for triple-positive APS (TRAPS trial), not suitable for mechanical heart valves (RE-ALIGN showed harm with dabigatran), dose reduction needed in renal impairment, and the lack of a routine monitoring assay (though specific anti-Xa levels and thrombin time can be used in selected situations). [1]
Warfarin — still essential in selected situations
Warfarin inhibits vitamin K epoxide reductase, depleting the vitamin K-dependent factors (II, VII, IX, X) and the natural anticoagulants (protein C, protein S). It requires INR monitoring, has a narrow therapeutic window, and interacts with many drugs and foods (especially those high in vitamin K). [1]
Warfarin is preferred over DOACs in: [1]
- Triple-positive antiphospholipid syndrome — the TRAPS trial showed excess thrombosis with rivaroxaban in high-risk (triple-positive) APS patients [6]. Target INR 2.0 to 3.0; consider 3.0 to 4.0 for recurrent events despite therapeutic INR.
- Pregnancy — warfarin is teratogenic (first trimester) and associated with fetal bleeding (third trimester), so LMWH is used during pregnancy, and warfarin is switched to postpartum (safe in breastfeeding).
- Mechanical heart valves — the RE-ALIGN trial showed harm with dabigatran in mechanical valve patients; warfarin is the only approved anticoagulant.
Warfarin initiation: start with heparin overlap (LMWH or UFH) for at least 5 days and until INR is therapeutic (2.0 to 3.0) for 2 consecutive days. Avoid loading doses (e.g. 10 mg) in patients who may have protein C or S deficiency — warfarin-induced skin necrosis. [1]
Low molecular weight heparin (LMWH)
LMWH (enoxaparin, dalteparin, tinzaparin) inhibits Factor Xa via antithrombin. It is the preferred agent in: [1]
- Pregnancy — does not cross the placenta, well tolerated, dose-adjusted by weight throughout pregnancy and for 6 weeks postpartum.
- Cancer-associated VTE — historically the standard of care; now challenged by edoxaban (Hokusai-CANVAS) and apixaban (Caravaggio) [7][8][9]. LMWH remains preferred in patients with gastrointestinal or genitourinary cancers at high bleeding risk, in thrombocytopenic patients, and in pregnancy with cancer.
Duration of anticoagulation
Provoked VTE — 3 to 6 months
If the clot was provoked by a major transient risk factor (surgery, trauma, prolonged immobility, oestrogen) that has now resolved, 3 months of anticoagulation is sufficient. The recurrence risk after stopping is low (under 5 per cent per year). Oestrogen-containing contraception should be discontinued permanently. [1]
Unprovoked VTE — at least 6 months, often indefinite
An unprovoked VTE carries a higher recurrence risk (about 10 per cent per year after stopping anticoagulation). After the initial 3 to 6 months, the decision to continue indefinitely is a shared decision balancing: [1]
- Factors favouring indefinite anticoagulation: male sex (higher recurrence than female), elevated D-dimer after stopping, proximal DVT or PE, obesity, chronic inflammatory disease, presence of high-risk thrombophilia.
- Factors favouring stopping: high bleeding risk (HAS-BLED, prior intracranial haemorrhage, thrombocytopenia, concurrent antiplatelet therapy), patient preference, frailty. [1]
The EINSTEIN-CHOICE trial demonstrated that for patients who have completed 6 to 12 months of anticoagulation and remain at risk, low-dose rivaroxaban (10 mg daily) or standard-dose (20 mg daily) is superior to aspirin for preventing recurrence, with no significant increase in major bleeding [5]. This supports extended anticoagulation over aspirin when continuation is chosen.
Cancer-associated VTE — indefinite (while cancer is active)
Cancer-associated VTE has a recurrence rate of about 10 to 20 per cent per year despite anticoagulation. Anticoagulation is continued indefinitely while the cancer is active (reassessed every 6 months) or until the cancer is cured or in durable remission. LMWH (dalteparin at full therapeutic dose for the first month, then 75 per cent) was the historical standard. The Hokusai-CANVAS and Caravaggio trials now support edoxaban or apixaban as effective oral alternatives [8][9].
| Trial | Comparison | Key result | Bleeding signal |
|---|---|---|---|
| SELECT-D [7] | Rivaroxaban vs dalteparin | Rivaroxaban reduced recurrent VTE | Higher CRNMB; more GI bleeding with GI cancers |
| Hokusai-CANVAS [8] | Edoxaban vs dalteparin | Edoxaban non-inferior for composite of recurrent VTE or major bleeding | More GI bleeding, especially with GI cancers |
| Caravaggio [9] | Apixaban vs dalteparin | Apixaban non-inferior for recurrent VTE | No significant increase in major bleeding |
Practical approach to cancer-associated VTE: For most patients, a DOAC (apixaban or edoxaban) is first-line, with LMWH (dalteparin) preferred in patients with GI or GU cancers at high bleeding risk, in thrombocytopenia (platelets under 50), in pregnancy, or in severe renal impairment. [1]
Special situations
Antiphospholipid syndrome — warfarin over DOACs
In triple-positive APS (positive for lupus anticoagulant, anticardiolipin and anti-beta-2 glycoprotein I simultaneously), the TRAPS trial was terminated early because rivaroxaban was associated with excess thrombotic events compared with warfarin [6]. The current recommendation is:
- First VTE in APS: warfarin, target INR 2.0 to 3.0.
- Recurrent VTE despite therapeutic INR: increase target INR to 3.0 to 4.0, or add low-dose aspirin for arterial events.
- DOACs: may be considered in non-triple-positive APS patients who cannot tolerate or access warfarin, but not as first choice in high-risk patients. [1]
Pregnancy — LMWH throughout, warfarin postpartum
- LMWH (enoxaparin 1 mg/kg twice daily or 1.5 mg/kg once daily, or dalteparin 200 IU/kg daily) is the anticoagulant of choice during pregnancy. It does not cross the placenta. Dose is weight-adjusted and increased as the pregnancy advances. [1]- Warfarin is teratogenic (weeks 6 to 12 — nasal hypoplasia, limb abnormalities, CNS abnormalities) and causes fetal bleeding in the third trimester. It is avoided during pregnancy.
- DOACs are contraindicated in pregnancy (teratogenic, and excreted in breast milk).
- Postpartum: switch to warfarin for 6 weeks to 6 months postpartum; warfarin is safe in breastfeeding.
- Aspirin (low dose) is added in APS with recurrent pregnancy loss, started before conception or in early pregnancy. [1]
Cancer-associated VTE
See the duration section above. The key decision is DOAC (apixaban or edoxaban) vs LMWH (dalteparin), balanced by bleeding risk and GI cancer status. [1]
Cerebral venous sinus thrombosis (CVST)
CVST presents with headache (the commonest symptom, over 90 per cent), often with seizures, focal neurological deficits, papilloedema, and occasionally reduced consciousness. Risk factors include pregnancy, the puerperium, oral contraceptives, APS, inherited thrombophilia, and local infection (otitis, mastoiditis). [1]
- Diagnosis: MR or CT venography shows the absent venous sinus flow void.
- Treatment: anticoagulate even if there is haemorrhagic infarction on imaging (the bleeding is from venous congestion and the clot needs to be cleared). LMWH initially, transitioning to warfarin or a DOAC for 3 to 6 months (longer if APS or thrombophilia).
- Prognosis: the ISCVT study showed an overall mortality of about 8 per cent and full recovery in about 80 per cent [10].
- Thrombophilia testing: strongly indicated in CVST — APS, Factor V Leiden, prothrombin mutation, and JAK2 (for myeloproliferative neoplasms) should all be considered.
Splanchnic vein thrombosis
Thrombosis of the portal, mesenteric or hepatic veins (Budd-Chiari syndrome) is strongly associated with myeloproliferative neoplasms (especially JAK2-positive), APS, paroxysmal nocturnal haemoglobinuria, and inherited thrombophilia. Every patient with splanchnic vein thrombosis should be evaluated for an underlying myeloproliferative neoplasm with JAK2 V617F testing, even if the blood count is normal (the so-called "latent" MPN). [1]
Heparin-induced thrombocytopenia (HIT)
HIT is a prothrombotic immune adverse effect of heparin. It is caused by IgG antibodies against the complex of platelet factor 4 (PF4) and heparin. These antibodies activate platelets via the Fc receptor, causing both thrombocytopenia (platelet consumption) and a paradoxical thrombotic tendency — arterial and venous thrombosis, skin necrosis at heparin injection sites, and systemic reactions after IV heparin boluses. The cardinal paradox: thrombocytopenia with thrombosis, not bleeding. [1]
Type I vs Type II HIT
- Type I (non-immune): a mild, transient platelet fall in the first 1 to 2 days of heparin, due to direct platelet activation. Benign, self-resolving, does not require stopping heparin. Not "true" HIT.
- Type II (immune): the clinically significant form. Onset 5 to 14 days after heparin exposure (or sooner if prior heparin exposure within 30 to 100 days). Platelet fall of 50 per cent or more from baseline, with thrombosis risk. This is what clinicians mean by "HIT." [1]
The 4T score
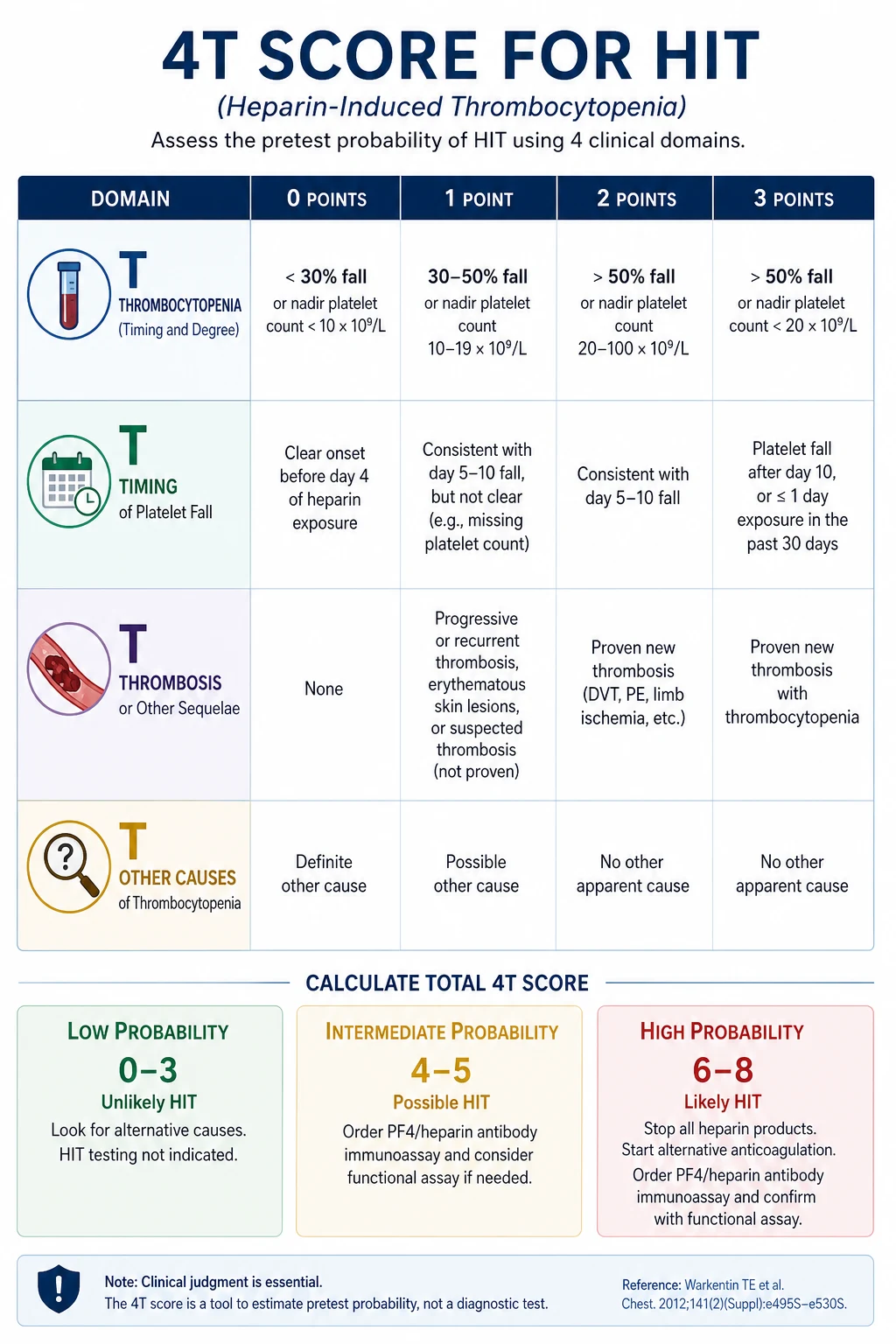
The 4T score estimates the pretest probability of HIT using four parameters: [1]
| Parameter | 2 points | 1 point | 0 points |
|---|---|---|---|
| Thrombocytopenia | Platelet fall over 50 per cent and nadir at least 20 | Fall 30 to 50 per cent or nadir 10 to 19 | Fall under 30 per cent or nadir under 10 |
| Timing of onset | Clear onset days 5 to 10, or within 1 day if heparin exposure in past 30 days | Consistent but not clear; or after day 10; or within 1 day if past exposure 30 to 100 days | No fall, or fall within 4 days with no recent heparin |
| Thrombosis or other sequelae | New confirmed thrombosis, skin necrosis, or acute systemic reaction after IV bolus | Progressive or recurrent thrombosis; suspected (not proven) thrombosis | None |
| Other causes of thrombocytopenia | None apparent | Possible | Definite |
Interpretation: [1]
- 0 to 3 — low probability: HIT very unlikely (negative predictive value over 99 per cent). Do NOT need to test or stop heparin.
- 4 to 5 — intermediate probability: HIT possible. Stop heparin, switch to a non-heparin anticoagulant, and send a PF4 antibody / serotonin release assay.
- 6 to 8 — high probability: HIT likely. Stop all heparin immediately, switch to a non-heparin anticoagulant, and confirm with laboratory testing. [1]
Laboratory confirmation
- PF4 enzyme immunoassay (ELISA): detects anti-PF4/heparin IgG antibodies. High sensitivity, moderate specificity. A negative ELISA usefully excludes HIT.
- Serotonin release assay (SRA) or heparin-induced platelet activation (HIPA): the functional gold standard — high sensitivity and specificity but not available in all laboratories and takes days. [1]
Management of confirmed or suspected HIT
- Stop ALL heparin — unfractionated heparin, LMWH, heparin flushes, heparin-coated lines. The patient must not receive heparin in any form.
- Start a non-heparin anticoagulant:
- Argatroban (a direct thrombin inhibitor, IV, hepatically cleared — preferred in renal failure).
- Danaparoid (an indirect Factor Xa inhibitor, available in Australia and UK).
- Bivalirudin (for percutaneous coronary intervention).
- Fondaparinux (a synthetic pentasaccharide Factor Xa inhibitor, subcutaneous).
- DOACs (especially apixaban or rivaroxaban) are increasingly used in stable patients with HIT.
- Do NOT transfuse platelets unless the patient is bleeding or needs an urgent procedure — platelet transfusion can fuel the thrombotic process.
- Transition to warfarin only after the platelet count has recovered to at least 150 (typically over 150), with a slow overlap of at least 5 days of non-heparin anticoagulant. Starting warfarin during the acute HIT phase can cause venous limb gangrene and skin necrosis.
- Screen for thrombosis — about 30 to 50 per cent of HIT patients develop a thrombosis. Lower limb ultrasound is often warranted. [1]
DWE high-yield trap: The most common error is confusing HIT with other causes of thrombocytopenia in a hospitalised patient (sepsis, DIC, drug reaction, marrow failure). The distinguishing features of HIT are: timing (5 to 14 days after heparin, or sooner with recent exposure), a fall of 50 per cent or more (not necessarily below 150), and the presence of thrombosis. The 4T score exists precisely to avoid over-diagnosing HIT and unnecessarily stopping heparin in patients who do not have it. [1]
VTE prevention (prophylaxis)
Every hospitalised adult patient should undergo a VTE risk assessment on admission (the Caprini score for surgical patients, the Padua score for medical patients). Prophylaxis options: [1]
- Pharmacological: LMWH (enoxaparin 40 mg subcutaneously daily, dose-reduced in renal impairment), unfractionated heparin (5000 units subcutaneously every 8 to 12 hours), or fondaparinux.
- Mechanical: graduated compression stockings (TEDS), intermittent pneumatic compression (IPC) — used when pharmacological prophylaxis is contraindicated (active bleeding, severe thrombocytopenia, planned neuraxial procedure).
- Combined: in the highest-risk patients (major orthopaedic surgery, trauma), pharmacological and mechanical prophylaxis are used together. [1]
DOACs (rivaroxaban, apixaban, dabigatran) are now widely used for post-orthopaedic VTE prophylaxis (hip and knee replacement), replacing LMWH or warfarin. [1]
Long-term complications
Post-thrombotic syndrome (PTS)
About 20 to 50 per cent of patients with proximal DVT develop post-thrombotic syndrome — chronic leg pain, swelling, heaviness, discolouration and occasionally venous ulcers — from damage to the venous valves and chronic venous hypertension. Graduated compression stockings were historically recommended for prevention, but the SOX trial challenged this; current practice focuses on optimising body weight and encouraging regular exercise. Severe PTS (ulceration) may benefit from endovascular intervention. [1]
Chronic thromboembolic pulmonary hypertension (CTEPH)
About 0.5 to 4 per cent of patients after PE develop CTEPH — persistent pulmonary arterial obstruction by organised thrombus causing pulmonary hypertension and right heart failure. Present with exertional dyspnoea that does not resolve after the acute PE. Diagnosis rests on ventilation-perfusion scan (showing segmental mismatches) and right heart catheterisation. The treatment is pulmonary endarterectomy (a curative surgical procedure in selected patients) or riociguat (a soluble guanylate cyclase stimulator) for inoperable disease. [1]
Anticoagulation-related bleeding
The major complication of anticoagulation is bleeding. Management: [1]
- Minor bleeding: continue anticoagulation, investigate the source.
- Major bleeding (GI, intracranial): stop the anticoagulant, give supportive care. For dabigatran, give idarucizumab (a specific reversal agent). For apixaban and rivaroxaban, give andexanet alfa (a specific reversal agent) or prothrombin complex concentrate (PCC). For warfarin, give vitamin K (10 mg IV) and PCC.
- Life-threatening bleeding: activate the massive transfusion protocol, give blood products and reversal agents, and involve haematology and interventional radiology. [1]
Exam traps and high-yield discriminators
- The paradox of the lupus anticoagulant: prolonged aPTT that does not correct on mixing, with thrombosis, not bleeding. Think APS.
- Warfarin-induced skin necrosis in protein C deficiency: start warfarin with heparin overlap, avoid loading doses.
- Timing of thrombophilia testing: do not test during acute thrombosis or on anticoagulation — the results are false. Defer for 4 to 6 weeks after stopping, except for genetic tests (Factor V Leiden, prothrombin G20210A).
- DOACs vs warfarin in APS: the TRAPS trial — warfarin is preferred in triple-positive APS. DOACs cause excess thrombosis.
- Dabigatran and edoxaban require a lead-in of heparin: unlike apixaban and rivaroxaban, which can be started immediately. A common MCQ discriminator.
- HIT is thrombocytopenia with thrombosis, not bleeding: the cardinal paradox. Stop heparin, switch to argatroban or danaparoid, do NOT give platelet transfusions.
- The 4T score: a low score (0 to 3) has a negative predictive value of over 99 per cent — you do not need to stop heparin or test for HIT.
- Cancer-associated VTE is indefinite: while the cancer is active. DOACs (apixaban or edoxaban) are now first-line, with LMWH for GI cancers or thrombocytopenia.
- Cerebral venous sinus thrombosis: anticoagulate even with haemorrhagic infarction. The bleeding is from venous congestion.
- Pregnancy and anticoagulation: LMWH throughout pregnancy, warfarin postpartum. DOACs are contraindicated. [1]
Regional guideline anchoring
- ANZ: NHMRC, the Therapeutic Guidelines (eTG), Australian Commission on Safety and Quality in Health Care VTE prevention guidelines, HSANZ consensus statements. The ANZ preference is for DOACs first-line in non-pregnant, non-APS VTE, with apixaban or rivaroxaban as the most commonly prescribed.
- UK: NICE NG158 (Venous thromboembolic diseases, 2020) — DOACs first-line, warfarin for APS and pregnancy, thrombophilia testing for selected patients.
- US: ASH 2018 guidelines (DOACs over VKAs for most VTE); CHEST/ACCP guidelines; ASCO/ITAC guidance for cancer-associated thrombosis.
- Global: ITAC (International Initiative for Management of Cancer) guidance for cancer-associated thrombosis — DOACs preferred over LMWH for most patients. [1]
Follow-up and surveillance
After the acute event, patients on DOACs require: [1]
- Renal function every 6 to 12 months (more frequently if declining) — dose adjust or switch agent.
- Full blood count — monitor for anaemia (occult bleeding) and thrombocytopenia.
- Adherence review — DOACs have a short half-life and missed doses are clinically significant (unlike warfarin, where a single missed dose is partly buffered by the long half-life of Factor II).
- Bleeding review and risk reassessment at each visit.
- Duration decision review at 3 months (provoked) and 6 months (unprovoked) — shared decision on continuation. [1]
Patients on warfarin require: [1]
- INR monitoring: intensive at initiation (every 2 to 3 days, then weekly, then every 2 to 4 weeks once stable).
- Education on diet (consistent vitamin K intake), drug interactions, and bleeding signs.
- Periodic review of the indication and duration. [1]
References and guidelines
ASH 2018 guidelines for management of VTE (DOACs preferred over VKAs); NICE NG158 (Venous thromboembolic diseases, 2020); BSH guidelines on heritable thrombophilia testing; Miyakis Sydney criteria for APS [3]; Bertina Factor V Leiden [1]; Poort prothrombin G20210A [2]; Wells DVT clinical model [4]; TRAPS trial (warfarin over rivaroxaban in triple-positive APS) [6]; EINSTEIN-CHOICE (rivaroxaban over aspirin for extended therapy) [5]; SELECT-D [7], Hokusai-CANVAS [8], Caravaggio [9] (DOACs in cancer-associated VTE); ISCVT (cerebral venous sinus thrombosis prognosis) [10].
References
- [1]Bertina RM, Koeleman BP, Koster T, et al. Mutation in blood coagulation factor V associated with resistance to activated protein C Nature, 1994.PMID 8164741
- [2]Poort SR, Rosendaal FR, Reitsma PH, Bertina RM. A common genetic variation in the 3'-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis Blood, 1996.PMID 8916933
- [3]Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J Thromb Haemost, 2006.PMID 16420554
- [4]Wells PS, Anderson DR, Bormanis J, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management Lancet, 1997.PMID 9428249
- [5]Weitz JI, Lensing AWA, Prins MH, et al. Rivaroxaban or Aspirin for Extended Treatment of Venous Thromboembolism N Engl J Med, 2017.PMID 28316279
- [6]Pengo V, Denas G, Zoppellaro G, et al. Efficacy and safety of rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome: Rationale and design of the Trial on Rivaroxaban in AntiPhospholipid Syndrome (TRAPS) trial Lupus, 2016.PMID 26466613
- [7]Young AM, Marshall A, Thirlwall J, et al. Comparison of an Oral Factor Xa Inhibitor With Low Molecular Weight Heparin in Patients With Cancer With Venous Thromboembolism: Results of a Randomized Trial (SELECT-D) J Clin Oncol, 2018.PMID 29746227
- [8]Raskob GE, van Es N, Verhamme P, et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism N Engl J Med, 2018.PMID 29231094
- [9]Agnelli G, Becattini C, Meyer G, et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer N Engl J Med, 2020.PMID 32223112
- [10]Ferro JM, Canhao P, Stam J, et al. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT) Stroke, 2004.PMID 14976332