Phys · haematological
Transfusion Medicine
Also known as blood transfusion · blood component therapy · packed red cells · PRC · FFP · cryoprecipitate · massive transfusion · transfusion reaction · TACO · TRALI
Consultant-physician-depth guide to blood component therapy — restrictive transfusion thresholds and their trial evidence, platelet/plasma/cryoprecipitate indications, acute transfusion reactions with the TACO–TRALI discriminator, massive transfusion, and transfusion safety — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Transfusion Medicine
The answer first
Modern transfusion is component therapy, given restrictively, against evidence-based thresholds — never whole blood, and never "because the number looks low". Three rules carry you through almost every DWE question and every ward decision [5]:
- Transfuse components, not numbers. Each product (red cells, platelets, plasma, cryoprecipitate) has its own indication and its own evidence base. A low haemoglobin in a stable, asymptomatic patient is a reason to investigate, not to transfuse [5].
- Restrictive is the default. Across ICU, septic shock, hip surgery and cardiac surgery, a restrictive red-cell strategy (transfuse around Hb 70–80 g/L) is as safe as a liberal one — and uses less blood. The main exception still being refined is acute coronary syndrome [1] [4].
- Transfusion kills through process failure and cardiopulmonary reactions, not through viruses. The dominant causes of transfusion-associated death in haemovigilance data are wrong-patient errors (almost always clerical), TACO and TRALI — not HIV or hepatitis. The bedside identity check and early reaction recognition are where safety lives [19].
Blood components — what you are actually giving
A donated unit of whole blood is separated into components so one donation treats several patients and each patient gets only what they need. Australian and New Zealand components are leucodepleted (white cells filtered out), which is why febrile reactions and CMV transmission are now uncommon here [5].
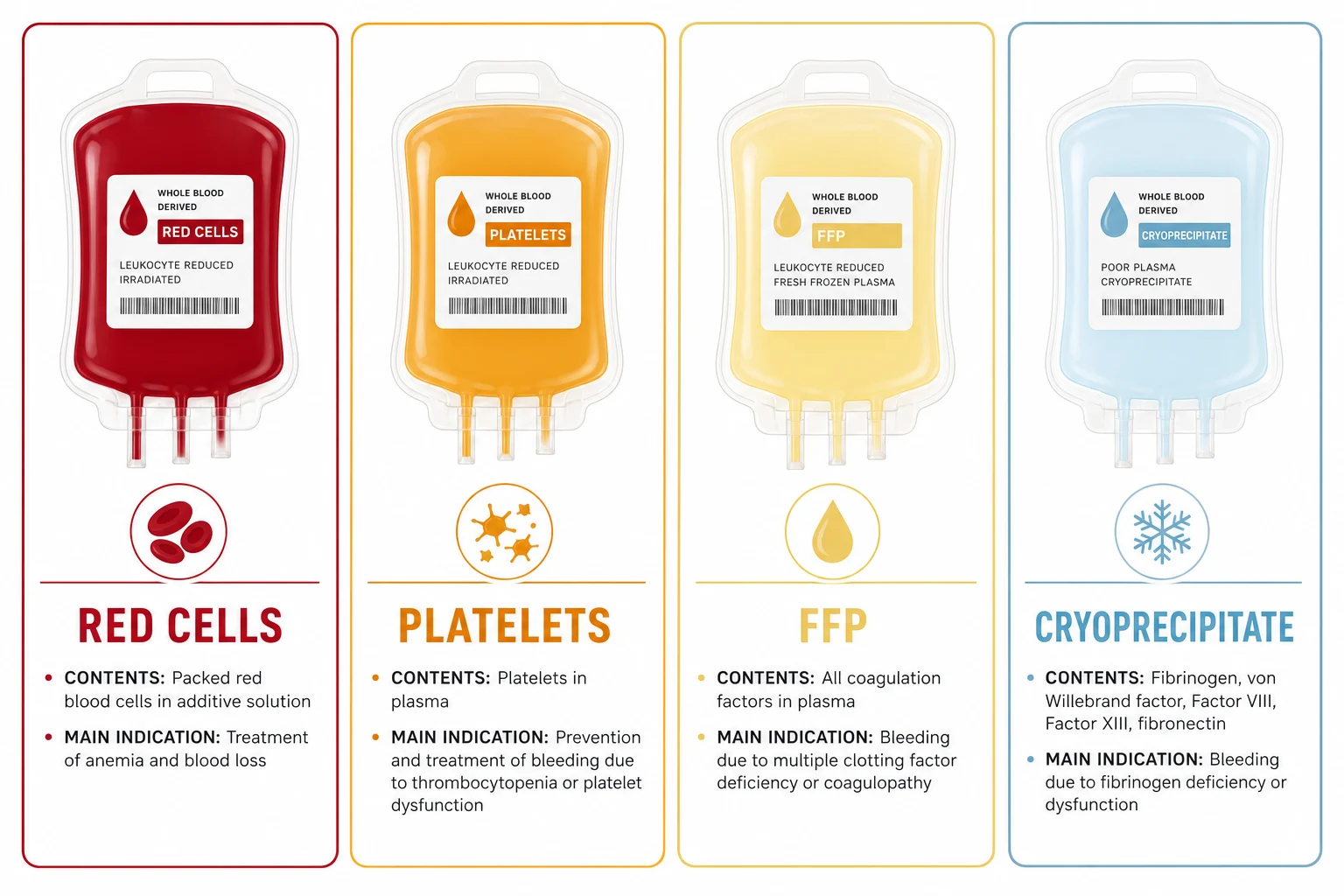
| Component | What it is | Classic indication | Expected effect in an adult |
|---|---|---|---|
| Packed red cells (PRC) | Red cells, minimal plasma | Symptomatic anaemia; Hb below threshold; acute bleeding | 1 unit raises Hb by about 10 g/L [5] |
| Platelets | Pooled or apheresis concentrate | Bleeding with thrombocytopenia; prophylaxis below threshold | 1 adult dose raises platelets by about 20–40 × 10⁹/L |
| Fresh frozen plasma (FFP) | All coagulation factors | Bleeding with multiple factor deficiency (DIC, massive transfusion, liver disease) | Replaces factors transiently — not a volume expander |
| Cryoprecipitate | Fibrinogen, factor VIII, vWF concentrate | Bleeding with low fibrinogen (DIC, massive haemorrhage) | A pooled adult dose raises fibrinogen by about 0.5–1.0 g/L |
Red cells: who actually benefits
The restrictive-versus-liberal question is one of the best-studied questions in transfusion. The trials, in the order examiners expect you to know them [1]:
| Trial | Population | Restrictive vs liberal trigger | Result | What it changed |
|---|---|---|---|---|
| TRICC (1999) | Critically ill adults | 70 vs 100 g/L | Restrictive at least as safe; signals of benefit in less-ill and non-cardiac patients | Established restrictive practice in the ICU [1] |
| FOCUS (2011) | Hip surgery, cardiovascular risk | 80 vs 100 g/L | No difference in death or functional recovery | Extended restrictive practice to perioperative elderly [3] |
| TRISS (2014) | Septic shock | 70 vs 90 g/L | No mortality difference | Safe in sepsis [2] |
| TRICS III (2017) | Cardiac surgery | 75 vs 95 g/L | Non-inferior composite outcome | Safe on-pump and post-op [9] |
| REALITY (2021) | Acute MI with anaemia | 80 vs 100 g/L | Non-inferiority met, but per-protocol favoured liberal | First crack in the restrictive wall for ACS [11] |
| MINT (2023) | Acute MI with anaemia | ~70–80 vs 100 g/L | Composite death/MI numerically favoured liberal, not statistically significant | ACS thresholds are now genuinely contested [4] |
AABB red-cell thresholds and the working exceptions
The AABB guideline recommends 70 g/L for stable hospitalised adults and 80 g/L for patients undergoing orthopaedic or cardiac surgery, or with pre-existing cardiovascular disease — and it deliberately does not give a firm number for acute coronary syndrome, where MINT and REALITY leave genuine uncertainty [5] [4] [11].
Give one unit, then reassess (symptoms and Hb) before the next. The Australian Patient Blood Management guidelines make single-unit transfusion the default for non-bleeding patients — each additional unit adds risk without adding evidence [5].
Platelets, plasma and cryoprecipitate
Each non-red component answers a different question, and each has its own misuse pattern to avoid [13].
| Component | Prophylactic threshold | Therapeutic indication | Classic misuse to avoid |
|---|---|---|---|
| Platelets | 10 × 10⁹/L in stable marrow failure; higher before procedures (about 20 for lumbar puncture, 50 for major surgery or neuraxial block) | Bleeding with thrombocytopenia or platelet dysfunction | Giving platelets for immune-consumptive thrombocytopenias — TTP and HIT — where they can worsen thrombosis [13] |
| FFP | Not given prophylactically for a number | Bleeding with multiple factor deficiency (DIC, massive transfusion); urgent reversal when PCC unavailable | "Correcting" an isolated raised INR without bleeding, and volume resuscitation [6] |
| Cryoprecipitate | Not given for a number alone | Bleeding with fibrinogen below about 1.5–2.0 g/L (DIC, massive haemorrhage, obstetric bleeding) | Treating it as generic factor replacement when fibrinogen is normal [14] |
For platelet prophylaxis in haematological malignancy, TOPPS showed that a no-prophylaxis strategy (treat only when bleeding) led to more WHO grade 2–4 bleeding than prophylaxis at 10 × 10⁹/L — which is why 10 remains the standard trigger on the haematology ward [12]. The AABB platelet guideline adds the procedure thresholds: about 10 for routine central line placement, 20 for elective lumbar puncture, and 50 for major non-neuraxial surgery, acknowledging the evidence here is thin [13].
For cryoprecipitate, the interesting nuance is CRYOSTAT-2: giving early empirical cryoprecipitate to all major trauma haemorrhage patients did not improve survival — so the practice is fibrinogen-guided replacement (viscoelastic testing or fibrinogen level), not blind empiricism [14].
The process — where transfusion safety is won or lost
Most fatal acute haemolytic reactions are clerical errors — the right blood hung on the wrong patient. Every step below exists because a named catastrophe happened to someone [19].
The safe transfusion sequence
Consent
Benefits, material risks (reactions, infection), and alternatives — documented before the product is ordered
Group and screen (or crossmatch)
ABO/Rh group plus antibody screen; an electronic crossmatch suffices if the screen is negative
Prescribe like a drug
Component, dose, rate, indications, any special requirements (irradiated, CMV-seronegative)
Bedside identity check
Two identifiers, checked by two people against the compatibility label and the patient's wristband — at the bedside, every unit
Baseline and 15-minute observations
Temperature, pulse, BP, respiratory rate, oxygen saturation before starting and at 15 minutes — most severe reactions declare early
Document and trace
Unit number, times, observations; every unit must be traceable donor-to-patient
Acute transfusion reactions
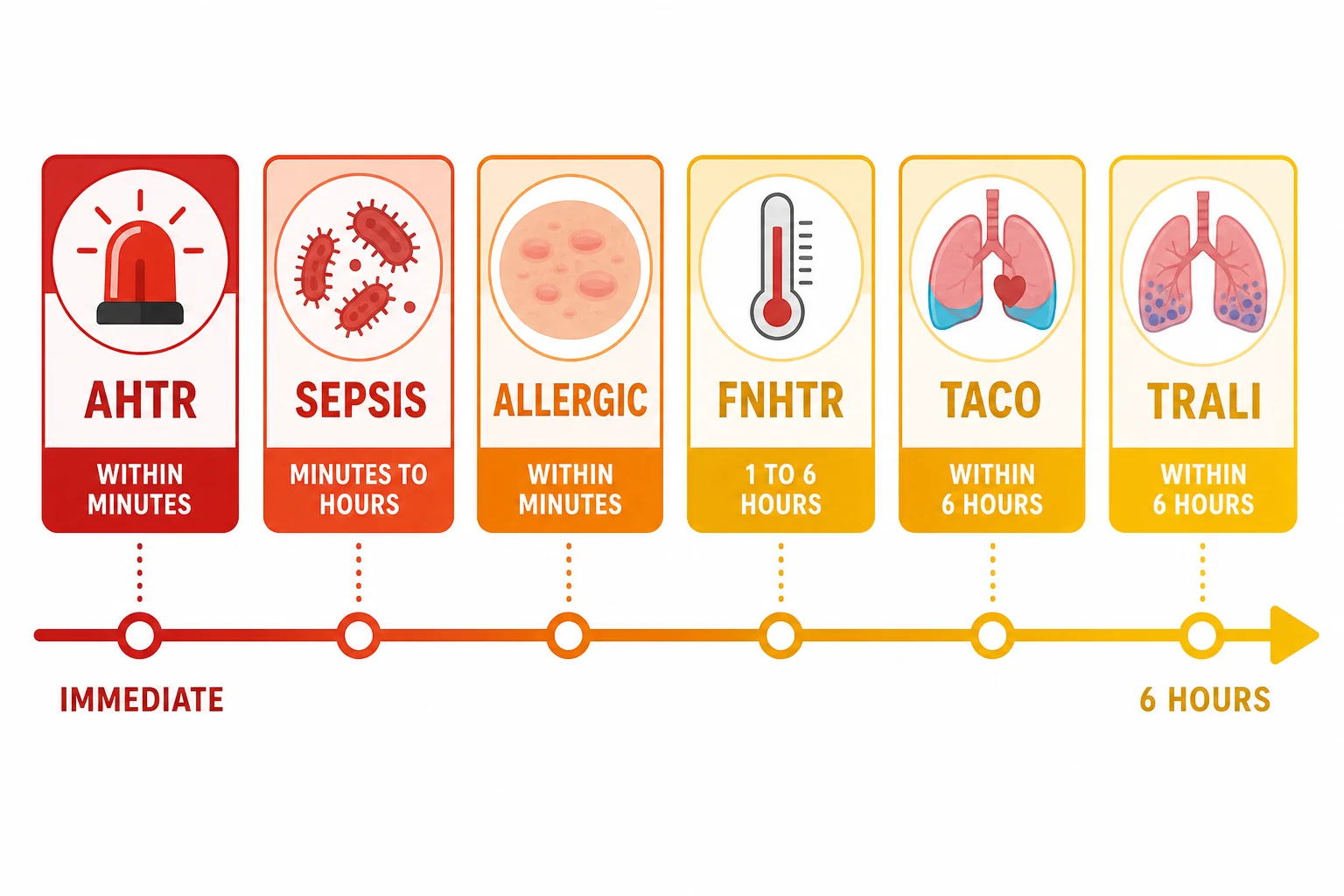
Acute reactions present within 24 hours; the dangerous ones present within minutes to 6 hours. Know the six cold — onset time is the fastest discriminator at the bedside [18].
| Reaction | Onset | Mechanism | Hallmark features | First-line management |
|---|---|---|---|---|
| Acute haemolytic (AHTR) | Minutes | ABO incompatibility → IgM complement-mediated intravascular haemolysis | Fever, flank/back pain, red-brown urine, hypotension, DIC, AKI | Stop, aggressive saline, maintain urine output, support, DIC screen |
| Allergic / anaphylaxis | Minutes | Recipient IgE (or IgA-deficiency anti-IgA) against donor plasma proteins | Urticaria, itch → wheeze, stridor, hypotension in anaphylaxis | Mild: stop, antihistamine. Anaphylaxis: stop, IM adrenaline, supportive care |
| Bacterial contamination | Minutes to hours | Cold-growing organisms, classically in platelets stored at room temperature | High fever, rigors, rapid shock | Stop, broad-spectrum antibiotics, cultures of patient AND unit |
| FNHTR | 1–6 hours | Donor leucocyte antigens / accumulated cytokines | Fever and rigors WITHOUT haemolysis or shock | Stop, paracetamol; a diagnosis of exclusion — rule out haemolysis and sepsis first |
| TACO | Within 6 (up to 12) hours | Hydrostatic pulmonary oedema from volume | Dyspnoea, hypertension, raised JVP, positive fluid balance | Stop, sit up, oxygen, diuretics; slow rates and single units to prevent |
| TRALI | Within 6 hours | Donor anti-HLA/HNA antibodies → neutrophil-mediated capillary leak | Dyspnoea, hypoxia, bilateral infiltrates, normal or low BP, often fever | Stop, oxygen, respiratory support (often ICU); diuretics do NOT help [10] |
TACO versus TRALI — the exam discriminator
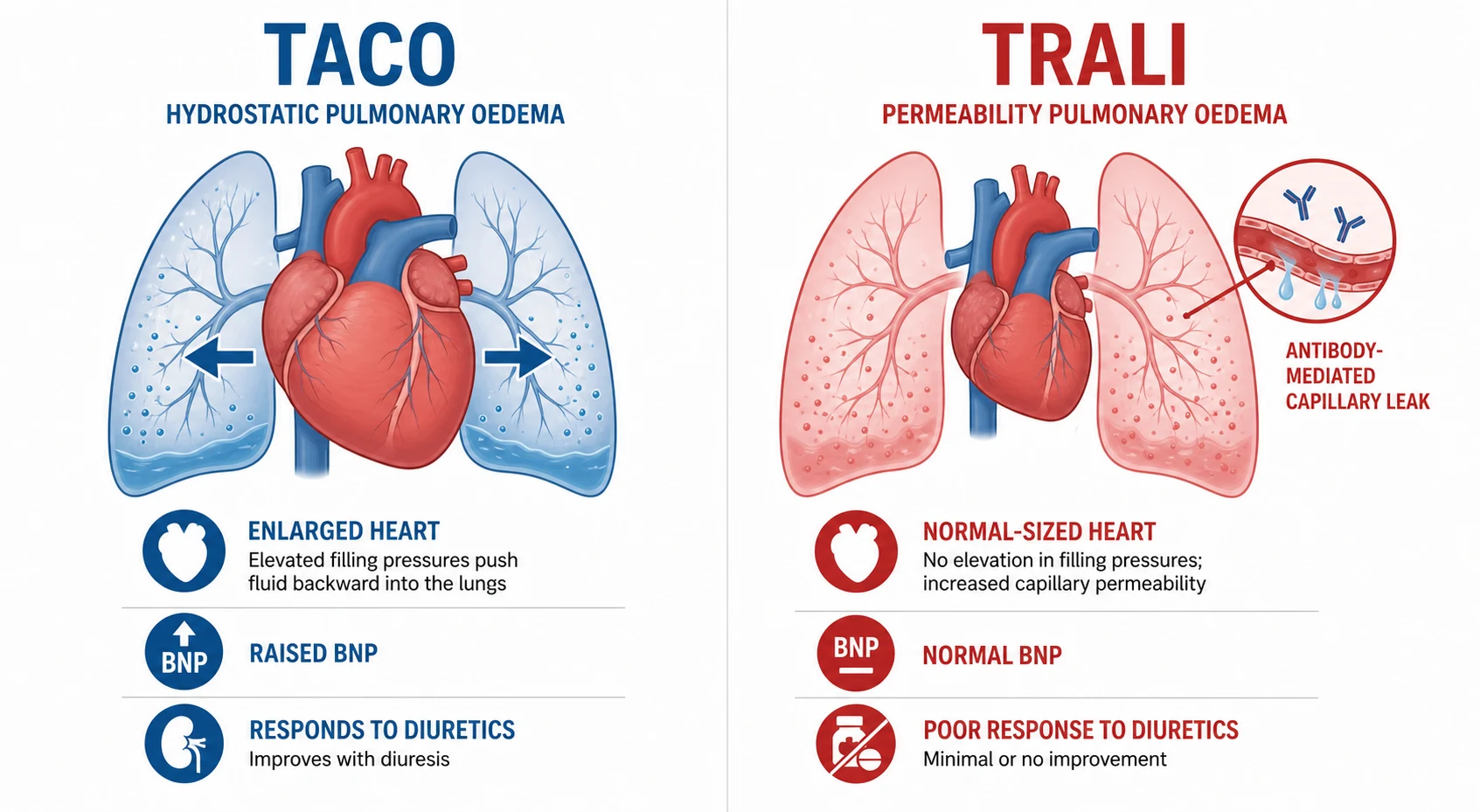
Both cause acute respiratory distress with bilateral chest infiltrates within 6 hours of transfusion. The entire DWE/DCE game is telling them apart, because the mechanisms — and the treatments — are opposite [18].
| Feature | TACO (hydrostatic) | TRALI (permeability) |
|---|---|---|
| Blood pressure | Typically hypertensive | Normal or hypotensive |
| JVP / fluid balance | Raised JVP, positive balance | Normal JVP, neutral balance |
| Fever | Absent | Often present |
| BNP | Elevated | Not elevated [17] |
| Diuretic response | Improves | No response (can worsen) |
| Mechanism | Volume exceeds cardiac reserve | Donor anti-HLA/HNA antibodies → capillary leak [10] |
| Core treatment | Sit up, oxygen, diurese, slow future transfusions | Oxygen and respiratory support; most recover in 48–96 hours |
| Prevention | Single units, slow rates, diuretic cover in at-risk patients | Blood bank investigation of the donor; defer implicated donors |
Suspected reaction: the universal first moves
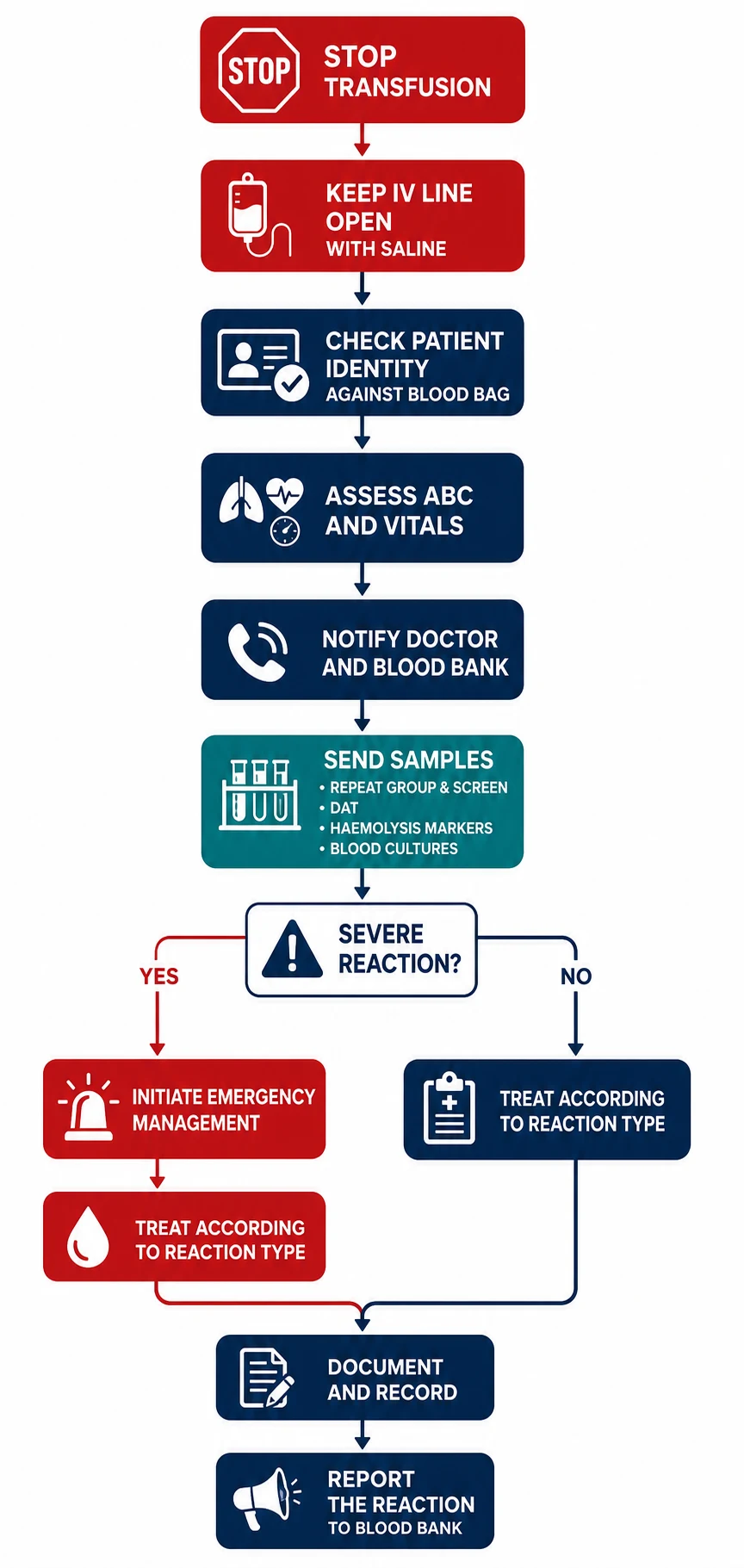
Whatever the reaction turns out to be, the first minute looks the same. This sequence is a complete DWE answer by itself [18].
The first five minutes of any suspected reaction
STOP the transfusion
This is always the first answer. Do not slow it — stop it
Keep the line open
Run normal saline through a new giving set — preserve IV access for resuscitation
Check identity
Patient wristband against the unit label — is this the right blood for this patient?
Assess and stabilise
Airway, breathing, circulation, full vital signs; call for help early if compromised
Notify the doctor and the blood bank
The blood bank guides the workup and initiates lookback on the unit
Send samples
Repeat group and screen, DAT, haemolysis markers (LDH, haptoglobin, bilirubin, free Hb), FBC, coagulation, cultures if septic; return the unit and giving set to the lab
Treat the specific reaction, document, report
Reaction-specific management, then a formal incident and haemovigilance report
The post-reaction DAT (direct antiglobulin test) deserves a line of its own: a newly positive DAT with falling haemoglobin and rising LDH supports immune haemolysis; a negative DAT with high fever and shock points you toward contamination or TRALI instead [10].
Massive haemorrhage and the MTP
Massive transfusion is most commonly defined as 10 or more red-cell units in 24 hours, or replacement of about one blood volume. In practice the trigger is gestalt: uncontrolled bleeding, shock, and the expectation of that volume. Activate the protocol early — the evidence and every trauma system agree that delayed, dribbling component therapy loses patients [6].
The modern protocol is ratio-based: plasma, platelets and red cells in approximate 1:1:1 packs. PROPPR compared 1:1:1 with 1:1:2 in severe trauma and found no overall mortality difference, but fewer deaths from exsanguination in the first 24 hours with 1:1:1 — which is why most major haemorrhage protocols now default to it [6].
| Target | Why | Working goal |
|---|---|---|
| Fibrinogen | Falls early; predicts ongoing bleeding | Keep above about 1.5–2.0 g/L with cryoprecipitate, guided by levels or viscoelastic testing [14] |
| Platelets | Dilutional and consumptive thrombocytopenia | Above 50 × 10⁹/L while bleeding |
| Ionised calcium | Citrate in stored blood chelates calcium → myocardial depression | Monitor and replace per protocol |
| Temperature | Hypothermia cripples the coagulation cascade | Warm the patient and the fluids |
| pH | Acidosis impairs factor function | Perfusion first — correct the shock, not the number |
Tranexamic acid is the one drug with mortality-level evidence here. CRASH-2 showed that TXA (1 g over 10 minutes, then 1 g over 8 hours) given within 3 hours of injury reduced all-cause mortality in bleeding trauma patients — and harmed when given late [7]. WOMAN extended this to postpartum haemorrhage: 1 g early (repeatable once), reducing death from bleeding without increasing thromboembolic events [8].
Delayed reactions and special situations
Acute reactions kill quickly; delayed ones appear on the ward round a week later, or years into a transfusion program [16].
| Delayed problem | Timeline | Mechanism and signature | What to do |
|---|---|---|---|
| Delayed haemolytic reaction | 5–10 days | Anamnestic alloantibody response (often Kidd) to a previously undetected antigen | Recognise the triad: falling Hb, jaundice, newly positive DAT after recent transfusion; support, and flag the antibody for all future units |
| Transfusion-associated graft-versus-host disease | 1–6 weeks | Viable donor lymphocytes engraft in a susceptible host | Almost always fatal — the entire strategy is prevention with irradiated products |
| Alloimmunisation | Cumulative | Antibodies against red-cell, HLA or platelet antigens | Extended phenotyping for chronic programs (MDS, thalassaemia); harder crossmatches over time |
| Iron overload | After about 20 units | Each red-cell unit carries about 200–250 mg of iron with no physiological exit route | Chelation (desferrioxamine, deferasirox, deferiprone) guided by ferritin and organ imaging in chronic transfusion [15] |
| Infection | Window-period residuals | Bacterial contamination exceeds viral transmission in frequency; leucodepletion and nucleic-acid testing have made HIV/HCV/HBV transmission extremely rare in Australia | Culture-driven management; report all suspected transmissions |
The patient who refuses blood. A competent adult — classically a Jehovah's Witness — can refuse blood products, and that refusal stands even if refusal leads to death. The physician's job is precision about which products are refused (many accept fractions or recombinant products), meticulous documentation, and aggressive bloodless management: treat iron and B12 deficiency early, use tranexamic acid for surgical or traumatic bleeding [7], minimise phlebotomy, and consider cell salvage and erythropoietin in the perioperative setting. In a true emergency with an incapacitated adult and no available advance directive, the default is to preserve life; with minors, seek urgent legal advice rather than delaying life-saving care.
The long-case integration. The classic DCE long case is the transfusion-dependent patient — myelodysplasia or thalassaemia — where the examiner's interest moves quickly from the blood to the program: how you individualise the threshold to symptoms, monitor iron (ferritin trends, liver or cardiac MRI), decide when chelation starts, manage alloantibodies, and weigh transfusion against disease-modifying therapy. Have a framework that moves from product, to program, to prognosis [15].
Exam traps, collected
References
- [1]Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group N Engl J Med, 1999.PMID 9971864
- [2]Holst LB, Haase N, Wetterslev J, et al. Lower versus higher hemoglobin threshold for transfusion in septic shock N Engl J Med, 2014.PMID 25270275
- [3]Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery N Engl J Med, 2011.PMID 22168590
- [4]Carson JL, Brooks MM, Abbott JD, et al. Restrictive or Liberal Transfusion Strategy in Myocardial Infarction and Anemia N Engl J Med, 2023.PMID 37952133
- [5]Carson JL, Guyatt G, Heddle NM, et al. Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage JAMA, 2016.PMID 27732721
- [6]Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial JAMA, 2015.PMID 25647203
- [7]CRASH-2 trial collaborators Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial Lancet, 2010.PMID 20554319
- [8]WOMAN Trial Collaborators Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial Lancet, 2017.PMID 28456509
- [9]Mazer CD, Whitlock RP, Fergusson DA, et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery N Engl J Med, 2017.PMID 29130845
- [10]Kleinman S, Caulfield T, Chan P, et al. Toward an understanding of transfusion-related acute lung injury: statement of a consensus panel Transfusion, 2004.PMID 15584994
- [11]Ducrocq G, Gonzalez-Juanatey JR, Puymirat E, et al. Effect of a Restrictive vs Liberal Blood Transfusion Strategy on Major Cardiovascular Events Among Patients With Acute Myocardial Infarction and Anemia: The REALITY Randomized Clinical Trial JAMA, 2021.PMID 33560322
- [12]Stanworth SJ, Estcourt LJ, Powter G, et al. A no-prophylaxis platelet-transfusion strategy for hematologic cancers N Engl J Med, 2013.PMID 23656642
- [13]Kaufman RM, Djulbegovic B, Gernsheimer T, et al. Platelet transfusion: a clinical practice guideline from the AABB Ann Intern Med, 2015.PMID 25383671
- [14]Davenport R, Curry N, Fox EE, et al. Early and Empirical High-Dose Cryoprecipitate for Hemorrhage After Traumatic Injury: The CRYOSTAT-2 Randomized Clinical Trial JAMA, 2023.PMID 37824155
- [15]Cappellini MD, Porter JB, El-Beshlawy A, et al. Tailoring iron chelation by iron intake and serum ferritin: the prospective EPIC study of deferasirox in 1744 patients with transfusion-dependent anemias Haematologica, 2010.PMID 19951979
- [16]Treleaven J, Gennery A, Marsh J, et al. Guidelines on the use of irradiated blood components prepared by the British Committee for Standards in Haematology blood transfusion task force Br J Haematol, 2011.PMID 21083660
- [17]Roubinian NH, Looney MR, Kor DJ, et al. NT-proBNP levels in the identification and classification of pulmonary transfusion reactions Transfusion, 2020.PMID 32905629
- [18]Roubinian NH Transfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung Injury: Etiology and Prevention Hematol Oncol Clin North Am, 2019.PMID 31466603
- [19]Bolton-Maggs PHB Transfusion errors - can they be eliminated? Br J Haematol, 2020.PMID 31792932