Phys · hepatic
Acute Liver Failure
Also known as fulminant hepatic failure · fulminant liver failure · acute hepatic failure · subacute liver failure · hyperacute liver failure · King's College Criteria · ceruloplasmin · hepatic encephalopathy
Consultant-physician-depth guide to acute liver failure — the definition (encephalopathy and coagulopathy within 26 weeks, without pre-existing liver disease), the causes by category (paracetamol, idiosyncratic drug, viral, autoimmune, Wilson disease, ischaemic, Budd-Chiari, pregnancy-related, mushroom poisoning), the King's College Criteria for transplant (paracetamol versus non-paracetamol), the full ICU management algorithm, and the complications with cerebral oedema as the leading cause of death. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Acute Liver Failure

The answer first
Acute liver failure is severe acute liver injury with coagulopathy (INR above 1.5) and encephalopathy, developing within 26 weeks of symptom onset, in a patient without pre-existing liver disease. Every word of that definition earns its place. The coagulopathy and the encephalopathy are the two mandatory criteria — a patient with jaundice and ALT of 3000 but a normal INR and normal mentation has acute severe hepatitis, not acute liver failure (ALF). The 26-week boundary separates ALF from chronic and subacute presentations. And the absence of pre-existing liver disease is essential, because acute decompensation of cirrhosis runs a different course and a different management pathway. [1]
The single organising principle for the whole topic: ALF is a time-critical emergency in which the cause determines the specific treatment, the King's College Criteria determine the transplant decision, and cerebral oedema is the leading cause of death. Everything else is detail hung on those three hooks. [1]

Know the causes table cold. It is the highest-yield page in ALF and answers most aetiology MCQ stems at a glance. [1]
| Cause | Key clue | Specific treatment | Prognosis (transplant-free) |
|---|---|---|---|
| Paracetamol | Overdose history, level, high AST/ALT | N-acetylcysteine | Best (over 60 percent) |
| Idiosyncratic drug | Onset days to weeks after new drug | Stop the drug, NAC empirically | Poor |
| Viral (HAV, HBV, HEV) | Serology, travel, pregnancy (HEV) | Supportive, antiviral for HBV | Moderate |
| Autoimmune | ANA, SMA, high IgG | Corticosteroids (selected) | Moderate |
| Wilson disease | Young, haemolysis, low ALP | Chelation, urgent transplant | Worst (near 100 percent medical mortality) |
| Ischaemic (shock liver) | Hypotension, cardiac arrest | Restore perfusion | Good if perfusion restored |
| Budd-Chiari | Ascites, hepatomegaly, thrombosis | Anticoagulation, transplant | Variable |
| Pregnancy-related (AFLP, HELLP) | Third trimester, hypertension | Deliver the baby | Good after delivery |
| Mushroom (Amanita phalloides) | Foraging history, GI prodrome | Penicillin G, silibinin | Variable |
DWE high-yield: In the West, paracetamol is the most common cause of ALF. In the developing world, viral hepatitis (especially HEV) dominates. The US ALFSG cohort (Ostapowicz, 308 patients) found paracetamol in 39 percent, idiosyncratic drugs in 13 percent, and hepatitis A and B together in only 12 percent [3]. This is the aetiological landscape an examiner expects you to know.
The three temporal subtypes
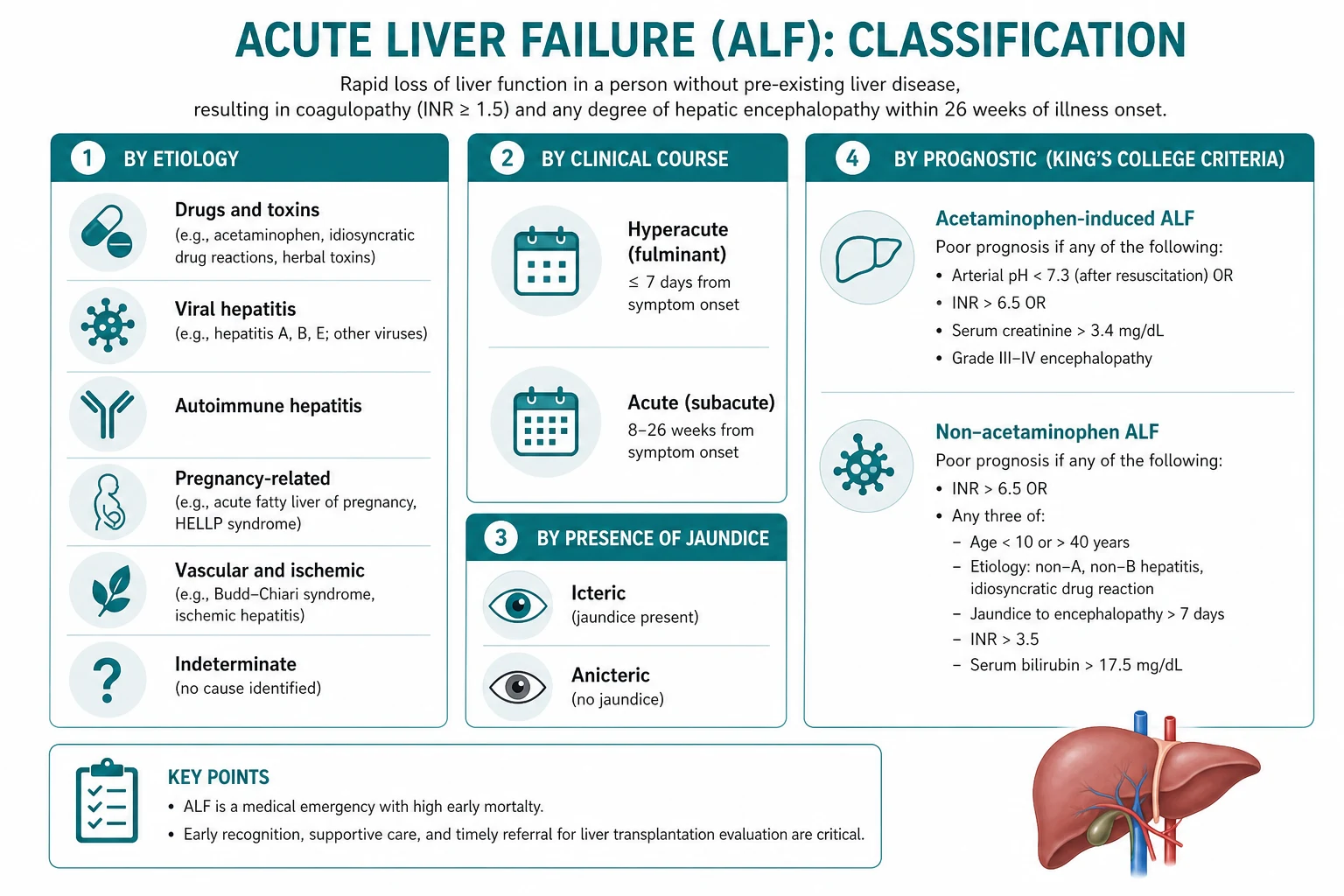
ALF is not one disease — it is a syndrome with three temporal patterns, and the pattern predicts both the cause and the prognosis [8].
- Hyperacute — encephalopathy within 7 days of jaundice. Most often paracetamol. Paradoxically, despite the dramatic and rapid presentation, this group has the best spontaneous survival (over 60 percent transplant-free), because the liver, if it survives the insult, regenerates briskly.
- Acute — encephalopathy 7 to 21 days from jaundice. Often viral hepatitis (HAV, HBV, HEV) or paracetamol. Intermediate prognosis.
- Subacute — encephalopathy 21 days to 26 weeks from jaundice. Often indeterminate or idiosyncratic drug reactions. Worst transplant-free survival (often below 20 percent), because the slow evolution lulls both the clinician and the hepatic regenerative capacity into failure. [1]
DCE trap: A patient with subacute liver failure who looks well on the ward can deteriorate catastrophically over hours. The slow tempo is deceptive. Subacute failure demands a lower threshold for transplant referral because the spontaneous survival is poor. [1]
Pathophysiology — why ALF kills
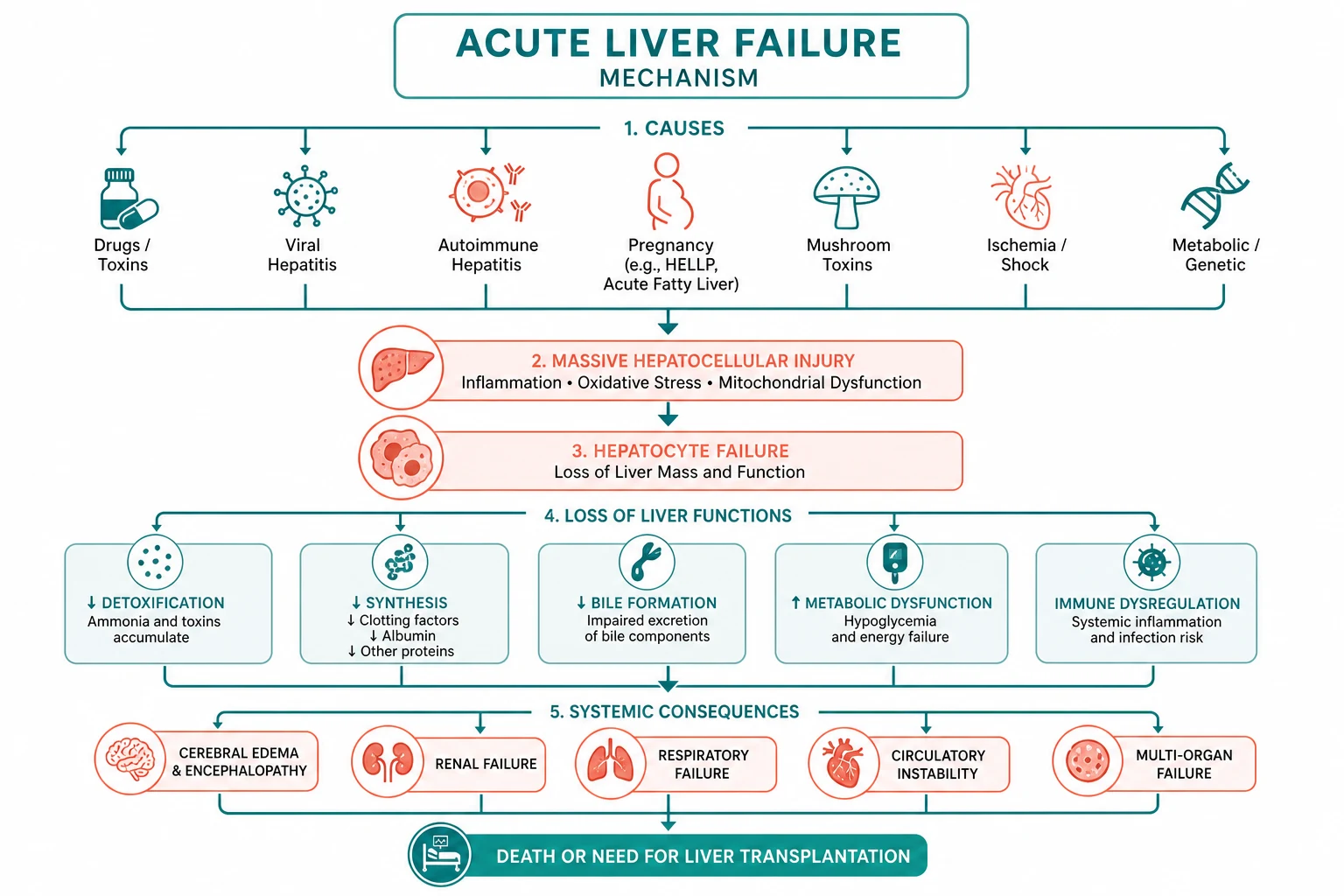
ALF is not just a liver problem. Massive hepatocyte necrosis (or, less commonly, severe hepatocyte dysfunction without overt necrosis, as in microvesicular steatosis or mitochondrial toxicity) releases damage-associated molecular patterns (DAMPs) that trigger a systemic inflammatory response syndrome (SIRS). The failing liver fails to clear ammonia, inflammatory mediators and gut-derived toxins, and the result is a multi-organ cascade [7].
- Cerebral oedema — ammonia crosses the blood-brain barrier, is metabolised by astrocyte glutamine synthetase to glutamine, which accumulates in astrocytes and causes astrocyte swelling. In grade 3 to 4 encephalopathy, intracranial pressure rises and cerebral herniation follows. This is the leading cause of early death in ALF, complicating up to 80 percent of grade 4 encephalopathy.
- Coagulopathy — the failing liver synthesises fewer clotting factors (elevated INR), but also fewer anticoagulants (protein C, protein S, antithrombin). The patient is in a rebalanced haemostatic state and is NOT auto-anticoagulated. Thromboelastography often shows a normal or even hypercoagulable tracing despite a high INR. This is why routine INR correction with FFP is wrong — it destroys the prognostic signal and the patient is not actually bleeding.
- Renal failure — from hepatorenal physiology, ATN from hypoperfusion, or direct nephrotoxicity (especially paracetamol).
- Immunoparesis — reduced complement, opsonisation and Kupffer cell function; infection (bacterial and fungal) is common and precipitates encephalopathy.
- Haemodynamic collapse — vasodilatory shock from accumulated vasoactive mediators, requiring noradrenaline. [1]
DWE high-yield: The question "why is the INR misleading in ALF?" is a classic. The answer: the patient loses both procoagulant AND anticoagulant factors, so the INR overstates the bleeding risk. Thromboelastography is a better functional test. Do NOT auto-treat a high INR with FFP. [1]
Causes — the full aetiological workup
Identifying the cause is not academic — it determines the specific treatment and the prognosis. Run the aetiological workup in parallel with resuscitation, because the answer changes management immediately [9].
Paracetamol (the leading cause in the West)
Paracetamol causes dose-related centrilobular (zone 3) hepatocellular necrosis through its toxic metabolite NAPQI. The four-stage clinical course, the nomogram, and the N-acetylcysteine regimen are covered in detail on the paracetamol toxicity page. The ALF-specific points: check a paracetamol level even if the patient denies overdose (staggered and inadvertent overdose is common), start NAC immediately if there is any evidence of hepatotoxicity, and continue NAC beyond 21 hours in established failure because Keays showed it improves survival even after fulminant failure is established [5].
Idiosyncratic drug-induced liver injury (DILI)
Unpredictable, dose-independent hepatocellular or cholestatic injury. The classic culprits: anti-TB drugs (isoniazid, rifampicin, pyrazinamide — the leading cause of DILI worldwide), statins (usually mild but occasionally severe), amoxicillin-clavulanate (the leading cause of DILI in the West, usually cholestatic and delayed), halothane hepatitis (now rare, but the classic exam answer), antiepileptics (phenytoin, valproate, carbamazepine), methotrexate, and herbal and dietary supplements (the rising epidemic — black cohosh, kava, green tea extract, Ayurvedic and traditional Chinese remedies). Management: stop the offending drug immediately, give NAC empirically, and apply the non-paracetamol King's College Criteria. [1]
Viral hepatitis
HBV is the most common viral cause of ALF worldwide. The viral causes are covered in detail on the viral hepatitis page. The ALF-specific points: acute HBV can present with a low or undetectable HBV DNA (the immune response has cleared the virus but the liver is destroyed — test anti-HBc IgM, which is the diagnostic marker); HAV is rare but more severe in the elderly and in those with chronic liver disease; HEV genotype 1 is dangerous in pregnancy (mortality 20 to 25 percent in the third trimester); and HSV hepatitis is rare but lethal in the immunocompromised, in pregnancy, and with a misleadingly normal bilirubin — treat empirically with high-dose intravenous aciclovir while awaiting PCR [7].
Autoimmune hepatitis
Autoimmune hepatitis can present de novo as ALF. Check ANA, smooth muscle antibody (SMA), anti-liver-kidney microsomal antibody (anti-LKM) and IgG. A liver biopsy (transvenous, given the coagulopathy) may show plasma cell infiltration and interface hepatitis. Corticosteroids (prednisolone 40 to 60 mg daily) may be used in selected cases, but the response in fulminant presentation is unreliable and these patients often need transplant. Do not let a trial of steroids delay transplant referral. [1]
Wilson disease — the high-yield diagnosis not to miss
Wilson disease is the cause of ALF that every examiner wants you to spot, because it changes the management entirely. The clues: [1]
- Age under 40 (Wilson rarely presents after 40).
- Coombs-negative haemolytic anaemia — the copper released from the necrotic liver damages red cell membranes; a dropping haemoglobin with a normal or high reticulocyte count and a negative Coombs test in a young patient with liver failure is Wilson until proven otherwise.
- Low or normal alkaline phosphatase — counterintuitively low for the degree of liver injury. A ratio of ALP to bilirubin below 2 (in international units) is a validated discriminator.
- Low caeruloplasmin (below 0.2 g/L) — though a normal caeruloplasmin does NOT exclude Wilson, because it is an acute-phase reactant and can be falsely normal in acute inflammation.
- Kayser-Fleischer rings on slit-lamp examination (present in the majority).
- High urinary copper (above 100 micrograms per 24 hours; in ALF it may be dramatically elevated above 1000). [1]
DWE high-yield trap: The combination of acute liver failure plus Coombs-negative haemolytic anaemia plus low alkaline phosphatase is virtually pathognomonic for Wilson disease. The medical mortality approaches 100 percent — urgent transplant referral is the only option. Chelation (penicillamine, trientine) rarely reverses established ALF but is started while awaiting transplant. [1]
Ischaemic hepatitis (shock liver)
Massive transaminase elevation (often above 5000) following a hypotensive episode — cardiac arrest, severe sepsis, profound heart failure. The transaminases fall rapidly over days once perfusion is restored (unlike viral or drug hepatitis, which fall more slowly). The key clue is the temporal relationship to a hypotensive event and the rapid fall. Coagulopathy and encephalopathy are less common than in paracetamol but can occur. Management: restore and maintain perfusion; the prognosis is good if the underlying haemodynamic insult is corrected. [1]
Budd-Chiari syndrome
Hepatic venous outflow obstruction (thrombosis of the hepatic veins or inferior vena cava) presents with the triad of abdominal pain, hepatomegaly and ascites, often in a patient with a thrombophilic disorder (myeloproliferative neoplasm, antiphospholipid syndrome, inherited thrombophilia) or on hormonal therapy. Doppler ultrasound (loss of hepatic vein flow, caudate lobe hypertrophy) is diagnostic. Management: anticoagulation, treatment of the underlying thrombophilia, and transplant if fulminant. [1]
Pregnancy-related causes
Two conditions unique to pregnancy: [1]
- Acute fatty liver of pregnancy (AFLP) — third trimester, with malaise, nausea, vomiting, hypoglycaemia, coagulopathy, hyperammonaemia and often polyuria and polydipsia (transient diabetes insipidus). Associated with a high Swansea score. Management: deliver the baby (the definitive treatment), manage the liver failure and coagulopathy in ICU, and refer for transplant if the King's College Criteria are met.
- HELLP syndrome (haemolysis, elevated liver enzymes, low platelets) — associated with pre-eclampsia and hypertension, presenting with right upper quadrant pain. Management: deliver the baby, control blood pressure, manage the coagulopathy and platelet count. [1]
DWE high-yield: A pregnant woman in the third trimester with liver failure — the answer is deliver the baby. Both AFLP and HELLP resolve after delivery, though the liver failure can progress for days so continued monitoring is essential. [1]
Mushroom poisoning (Amanita phalloides)
Amanita phalloides poisoning has a characteristic three-phase course: a GI prodrome (nausea, vomiting, profuse watery diarrhoea) at 6 to 24 hours, a deceptive "silent" phase at 24 to 72 hours when the patient looks well but transaminases are rising, and hepatocellular failure at 3 to 5 days. The key clue is a foraging history (mushroom picking, usually in autumn in Europe and North America). Management: aggressive fluid resuscitation (typically 1 L per hour of normal saline in the first 12 to 24 hours to maintain urine output and flush the toxin), penicillin G (250 mg/kg/day, the antidote of choice though evidence is limited) and silibinin (intravenous milk thistle extract, where available), and apply the non-paracetamol King's College Criteria for transplant [2].
The King's College Criteria for transplant
The King's College Criteria (KCC), derived from O'Grady's 1989 retrospective analysis of 588 patients, are the best-validated bedside tool for predicting non-survival and triggering urgent liver transplant referral [1]. They are etiology-specific — the criteria for paracetamol ALF differ from those for non-paracetamol ALF, because the prognostic indicators differ.

Paracetamol-induced ALF — transplant if ANY ONE of:
- Arterial pH below 7.3 after adequate fluid resuscitation, OR
- ALL THREE of: INR above 6.5 (PT above 100 seconds), creatinine above 300 micromol/L, grade 3 to 4 encephalopathy. [1]
DWE high-yield trap: For paracetamol ALF, the arterial pH below 7.3 is alone sufficient for transplant referral — you do NOT need the triad. And the triad requires all three components (INR above 6.5 AND creatinine above 300 AND grade 3 to 4 encephalopathy). A common error is applying only one or two of the triad. [1]
Non-paracetamol ALF — transplant if:
- INR above 6.5 (PT above 100 seconds) ALONE, OR
- ANY THREE of the following five: age under 10 or over 40 years; etiology non-A non-B hepatitis or idiosyncratic drug reaction; duration of jaundice before encephalopathy above 7 days; INR above 3.5 (PT above 50 seconds); bilirubin above 300 micromol/L (approximately 18 mg/dL). [1]
DWE high-yield trap: For non-paracetamol ALF, the INR above 6.5 is alone sufficient (it does not require encephalopathy or any other criterion). The five-variable limb requires any three of the five, not all five. Learn the distinction between the two limbs cold. [1]
The lactate adjunct
The King's College Criteria are highly specific (above 90 percent) but less sensitive (around 70 percent), meaning they miss some patients who will die. Bernal showed that arterial lactate above 3.5 mmol/L on early admission, or above 3.0 mmol/L after fluid resuscitation, identifies non-survivors with similar accuracy to the criteria combined but a median of 6 hours earlier — 4 hours versus 10 hours [4]. In a patient with a high lactate, contact the transplant unit before the formal criteria are met, to buy time for workup and transfer. The lactate is an early-warning adjunct, not a replacement for the criteria.
DCE insight: "How do you use the lactate in your transplant decision?" The answer: as an early trigger for the transplant conversation. I would contact the transplant unit when the lactate is above 3.5 on admission, even if the formal KCC are not yet met, because the workup and transfer logistics take time and the window for salvage is narrow. [1]
Management — the ICU algorithm
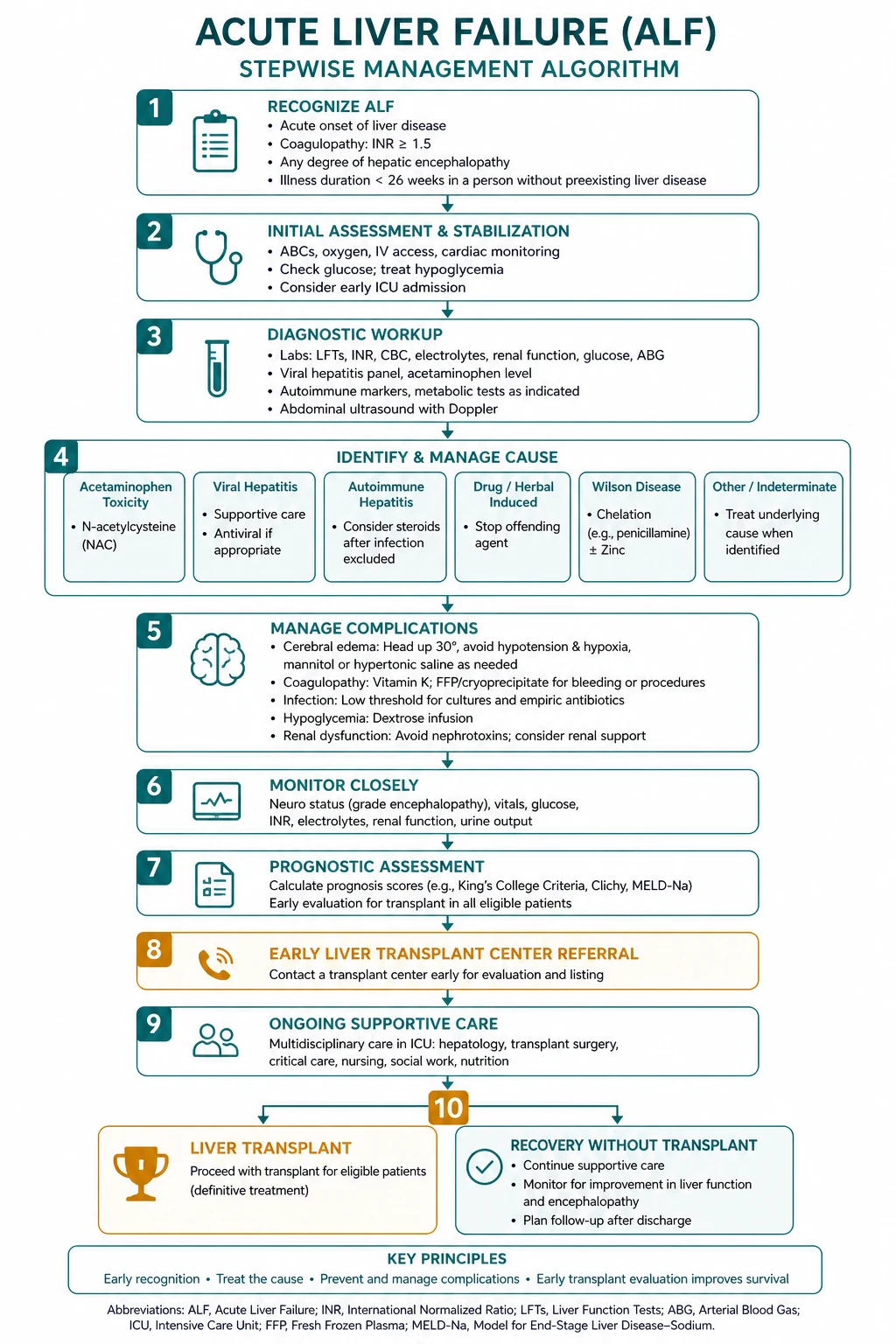

ALF management is the simultaneous pursuit of four goals: resuscitate, identify and treat the cause, provide organ support, and make the transplant decision. All four run in parallel from the moment of presentation [8].
Step 1 — Resuscitation and ICU admission
- Admit to an ICU or a specialist liver unit. ALF has high mortality and needs multi-organ support.
- Secure the airway if encephalopathy is grade 3 or above (intubation protects the airway and allows controlled ventilation for cerebral oedema management).
- Establish invasive monitoring: arterial line, central venous access, urinary catheter, frequent GCS and pupillary assessment.
- Correct hypoglycaemia with 10 per cent dextrose infusion and hourly glucose monitoring. Hypoglycaemia is both a complication and a poor prognostic sign.
- Treat hypovolaemia and vasodilatory shock with cautious crystalloid and noradrenaline (the preferred vasopressor; it preserves splanchnic perfusion better than adrenaline or vasopressin, though terlipressin is used in hepatorenal physiology). [1]
Step 2 — Identify and treat the cause
| Cause | Immediate specific treatment |
|---|---|
| Paracetamol | 21-hour IV N-acetylcysteine, continue beyond 21 hours in established failure |
| Non-paracetamol (unknown) | NAC empirically (Lee 2009 transplant-free survival benefit in early stage) |
| HBV | Nucleos(t)ide analogue (entecavir or tenofovir) |
| HSV | High-dose IV aciclovir (10 mg/kg every 8 hours) |
| Wilson disease | Chelation AND urgent transplant referral |
| Budd-Chiari | Anticoagulation, consider TIPS |
| AFLP/HELLP | Deliver the baby |
| Amanita phalloides | Penicillin G, silibinin, aggressive fluids |
| Ischaemic | Restore and maintain perfusion |
DWE high-yield: In non-paracetamol ALF of unknown cause, give N-acetylcysteine empirically. The Lee 2009 RCT (173 patients) showed that while overall survival was not improved, transplant-free survival was significantly better in patients with early-stage (grade 1 to 2) encephalopathy [6]. NAC is cheap, safe and has a plausible mechanism (free-radical scavenging and improved microcirculatory oxygen delivery), so most hepatology units use it empirically while awaiting the aetiological workup.
Step 3 — Supportive organ support
Cerebral oedema and raised intracranial pressure (the leading cause of death): [1]
- Elevate the head of the bed to 30 degrees.
- Maintain normocapnia (PaCO2 35 to 40), normoglycaemia, normothermia, and adequate oxygenation and perfusion.
- Hypertonic saline to a serum sodium of 145 to 155 mmol/L for grade 3 to 4 encephalopathy (prophylactic and therapeutic). [1]- Mannitol 0.5 g/kg IV bolus for established intracranial hypertension (monitor the serum osmolal gap; stop if above 320 mOsm/kg, or if the patient is not passing urine).
- Consider induced hypothermia to 33 to 34 degrees or intracranial pressure monitoring in grade 4 encephalopathy.
- Do NOT use corticosteroids — dexamethasone and methylprednisolone are ineffective for the cytotoxic cerebral oedema of ALF (unlike the vasogenic oedema of brain tumours) and are not recommended [9].
DWE high-yield trap: The question "what osmotherapy do you use for ALF cerebral oedema?" has a specific answer: hypertonic saline and mannitol. If an option lists corticosteroids (dexamethasone), it is WRONG. This is a guaranteed exam point because steroids are effective for so many other causes of cerebral oedema — the trap is assuming ALF is the same. [1]
Coagulopathy: [1]
- Do NOT routinely correct the INR with FFP — the INR is the prognostic marker that drives the King's College Criteria and the transplant decision [8].
- Give vitamin K 10 mg IV to correct any reversible vitamin K deficiency.
- Reserve fresh frozen plasma, cryoprecipitate (to a fibrinogen above 1.5 g/L) and platelets for active bleeding or immediately before invasive procedures.
- Use prothrombin complex concentrate rather than FFP for rapid pre-procedure reversal (it is volume-sparing and faster).
Renal failure: [1]
- Use continuous renal replacement therapy (CVVHDF), not intermittent haemodialysis — continuous avoids haemodynamic swings and intracranial pressure surges.
- Avoid nephrotoxic drugs (NSAIDs, aminoglycosides, contrast where avoidable).
- Renal recovery usually follows hepatic recovery or transplant. [1]
Infection: [1]
- Surveil with daily cultures (blood, urine, sputum, line sites).
- Have a low threshold for broad-spectrum antibiotics (sepsis precipitates encephalopathy and is frequently fatal).
- Consider antifungal cover (candida) in the prolonged ICU patient. [1]
Encephalopathy: [1]
- Lactulose (15 to 30 mL two to three times daily, titrated to two to three soft bowel motions per day) for ammonia lowering — but be aware it can cause dehydration and hypernatraemia if overzealous, which worsens cerebral oedema.
- Rifaximin is added for refractory encephalopathy (though evidence is strongest in chronic liver disease).
- Avoid sedatives unless intubated (they mask the encephalopathy grade, which is a prognostic and King's College Criterion). [1]
Step 4 — The transplant decision
Apply the King's College Criteria continuously from admission and at every reassessment, because the criteria may be met at any time as the clinical course evolves. The moment any criterion is met, refer urgently to the liver transplant unit — the workup (blood group, imaging, psychosocial assessment, listing, donor matching, transfer) takes time, and the window for salvage is narrow. A patient who meets the criteria and does not receive a transplant has a survival of around 20 percent; with transplant, one-year survival exceeds 75 percent [1].
DCE insight: "When do you call the transplant unit?" The answer is early and often. I would make contact at the point of admission in any patient with ALF, have a low threshold for formal referral when the King's College Criteria are approached (not just when they are met), and use the lactate as an early trigger. The transplant team would rather hear from you too early than too late. [1]
Complications and prognosis
The complications of ALF are the multi-organ failure cascade: cerebral oedema (the leading cause of early death), acute kidney injury, infection (bacterial and fungal), coagulopathy and bleeding, hypoglycaemia, metabolic acidosis, and haemodynamic collapse. Each is managed as described above. [1]
Prognosis is driven by three factors [3]:
- The cause — paracetamol has the best spontaneous recovery (transplant-free survival over 60 percent); ischaemic hepatitis is good if perfusion is restored; Wilson disease and subacute indeterminate failure have the worst (medical mortality near 100 percent).
- The tempo — hyperacute failure has the best recovery (the liver regenerates if it survives); subacute has the worst.
- The depth of encephalopathy — grade 3 to 4 carries the risk of cerebral oedema and the worst outcomes. [1]
With modern ICU care, NAC, and timely transplant, overall survival (transplanted and non-transplanted) is now above 70 percent in specialist centres [7].
Investigations — the complete ALF panel
| Panel | Tests |
|---|---|
| Baseline (every patient) | FBC, INR/PT, fibrinogen, AST, ALT, bilirubin, albumin, gamma-GT, ALP, urea, creatinine, electrolytes, glucose, arterial blood gas with lactate, phosphate, amylase, ammonia (if available) |
| Aetiology — paracetamol | Paracetamol level, salicylate level |
| Aetiology — viral | HBsAg, anti-HBc IgM, anti-HAV IgM, anti-HEV IgM and HEV RNA, HSV PCR, EBV PCR, CMV PCR |
| Aetiology — autoimmune | ANA, smooth muscle antibody, anti-LKM, IgG |
| Aetiology — Wilson | Caeruloplasmin, 24-hour urinary copper, slit-lamp for Kayser-Fleischer rings |
| Aetiology — pregnancy | Beta-hCG, full blood count, platelets, blood film for HELLP |
| Aetiology — vascular | Doppler ultrasound of hepatic vessels (hepatic veins, portal vein, hepatic artery) |
| Prognosis | King's College Criteria (continuous), arterial lactate, arterial ammonia, phosphate, MELD |
Differential diagnosis — when it is not ALF
Always confirm the aetiology. The most important distinction is ALF from acute decompensation of chronic liver disease (cirrhosis) — the presence of portal hypertension, splenomegaly, spider naevi, a small nodular liver, or a known history of liver disease points to chronic disease, not ALF, and the management and prognosis differ entirely. Other mimics: sepsis with hepatic dysfunction (the liver is an innocent bystander in severe sepsis; treat the sepsis), non-hepatic causes of altered consciousness (uremic encephalopathy, drug intoxication, Wernicke encephalopathy — the liver injury is coincidental), and non-hepatic causes of coagulopathy (DIC, warfarin, vitamin K deficiency). [1]
DWE high-yield: A patient with jaundice, confusion and INR of 2.5, who has known cirrhosis and has splenomegaly and spider naevi on examination — this is acute decompensation of cirrhosis, not ALF. The management (which includes portal hypertensive bleeding, spontaneous bacterial peritonitis prophylaxis, and hepatorenal syndrome) is on the chronic liver disease page. The two conditions share laboratory abnormalities but not the underlying pathophysiology, the prognosis, or the transplant pathway. [1]
DCE long-case approach
Opening statement (SASPOP)
"This is Ms C, a 19-year-old university student presenting with a one-week history of progressive jaundice, confusion and easy bruising, found to have acute liver failure — AST 1800, ALT 1500, INR 3.8, bilirubin 280, grade 2 encephalopathy — on a background of Wilson disease, confirmed by a Coombs-negative haemolytic anaemia, a low caeruloplasmin of 0.08, a 24-hour urinary copper of 480 micrograms, and Kayser-Fleischer rings on slit-lamp examination. [1]
Her main problems are:
- Wilson disease acute liver failure with a near-universal medical mortality — I have referred her urgently for liver transplant.
- Grade 2 encephalopathy with the risk of progression to cerebral oedema — I am managing with head elevation, hypertonic saline and close neurological monitoring.
- Coagulopathy (INR 3.8) — I am NOT correcting the INR because it is a prognostic marker; I have given vitamin K.
- Coombs-negative haemolytic anaemia (haemoglobin 72) — I have cross-matched blood.
- The genetic and family implications of Wilson disease (autosomal recessive). [1]
My integrated management plan is to admit her to the liver ICU, start chelation and NAC empirically, manage her encephalopathy and the complications of ALF, and proceed to urgent liver transplant, which is the only curative option for Wilson ALF. I am involving her family in the genetic counselling and the transplant consent." [1]
Integrated management plan
- Urgent transplant referral — Wilson ALF has a medical mortality approaching 100 percent; transplant is the only cure. Contact the transplant unit immediately for workup, listing and donor matching.
- ICU supportive care — head elevation, hypertonic saline, NAC empirically, vitamin K, no routine INR correction, renal and haemodynamic support, infection surveillance.
- Chelation — penicillamine or trientine is started but rarely reverses established ALF; it is continued while awaiting transplant.
- Family counselling — Wilson disease is autosomal recessive; siblings should be screened with caeruloplasmin, urinary copper and genetic testing. [1]
DCE examiner probing questions you must anticipate:
- "Why is her alkaline phosphatase normal?" → Wilson disease causes a low or normal ALP despite severe liver injury; the ratio of ALP to bilirubin is below 2.
- "Why does she have a haemolytic anaemia?" → The copper released from the necrotic liver damages red cell membranes; the Coombs test is negative because it is not immune-mediated.
- "What is her prognosis without transplant?" → Near-universal medical mortality; transplant is the only option.
- "How do you counsel her family?" → Autosomal recessive; siblings have a 25 percent chance of being affected and should be screened. [1]
DCE short-case approach: encephalopathy grading and abdominal examination
The short-case instruction is typically "Examine this patient's abdomen and assess for encephalopathy." In an ALF patient, the critical task is to grade the encephalopathy (which is a prognostic marker and a King's College Criterion) and to distinguish ALF from chronic liver disease (the stigmata of chronic disease are absent in ALF). [1]
Systematic routine
- End of bed — jaundice, drowsiness, agitation, asterixis, the rate and depth of breathing, bruising, any monitoring or lines.
- Hands and arms — liver flap (asterixis on sustained wrist extension with the arms outstretched), palmar erythema, bruising, finger-prick marks.
- Face and chest — fetor hepaticus (sweet musty breath), icteric sclerae, spider naevi (absent in pure ALF — their presence suggests chronic disease), gynaecomastia (absent in ALF), parotid enlargement (absent in ALF).
- Abdomen — tender hepatomegaly (common in acute hepatitis and paracetamol injury), a small or absent liver (massive necrosis), ascites (uncommon in ALF, common in Budd-Chiari).
- Neurological — grade the encephalopathy (see below), assess GCS, check for the signs of cerebral oedema (Cushing reflex, pupillary changes, posturing) in grade 4. [1]
Grading hepatic encephalopathy (West Haven)
| Grade | Mental state | Signs |
|---|---|---|
| 0 (covert) | No clinical signs; only on psychometric testing | None at bedside |
| 1 | Mild confusion, euphoria, anxiety, shortened attention, altered sleep | Slight tremor |
| 2 | Lethargy, apathy, disorientation | Asterixis, slurred speech |
| 3 | Marked somnolence or semi-stupor, responsive to stimuli | Gross disorientation, muscular rigidity |
| 4 | Coma with or without response to painful stimuli | Decerebrate posturing, signs of cerebral oedema |
Presentation template
"I examined Ms C, a 19-year-old woman who is drowsy but rousable at the end of the bed, icteric, with a flapping tremor on sustained wrist extension consistent with grade 2 hepatic encephalopathy. She has fetor hepaticus. The pulse is 96 regular, blood pressure 100/60, and her Glasgow Coma Scale is 13. The hands show a liver flap and several bruises but no palmar erythema. There are NO spider naevi and NO gynaecomastia — the absence of chronic liver disease stigmata is consistent with acute, not chronic, liver failure. The abdomen reveals a tender liver edge palpable 2 cm below the costal margin, with no ascites and no splenomegaly. The neurological examination is consistent with grade 2 encephalopathy. These findings, with an INR of 3.8 and an AST of 1800 in a young woman with Coombs-negative haemolysis and a low caeruloplasmin, are consistent with Wilson disease acute liver failure. I would monitor the encephalopathy grade and the INR against the King's College Criteria for transplant referral, and I would refer her urgently for transplant." [1]
Key DWE MCQ patterns
- The definition — INR above 1.5 AND encephalopathy within 26 weeks AND no pre-existing liver disease. A patient with jaundice and ALT of 3000 but normal INR and normal mentation has acute severe hepatitis, not ALF.
- The King's College Criteria — paracetamol (pH below 7.3 alone OR the triad) versus non-paracetamol (INR above 6.5 alone OR any three of five). The single most tested set of criteria in hepatology.
- Wilson disease recognition — young patient plus Coombs-negative haemolysis plus low ALP. The answer is Wilson; the next step is urgent transplant referral.
- The lactate adjunct — arterial lactate above 3.5 on admission (or above 3.0 after fluids) identifies non-survivors earlier than the KCC.
- Cerebral oedema management — hypertonic saline and mannitol, NOT corticosteroids. A guaranteed exam point.
- Coagulopathy management — do NOT routinely correct the INR with FFP; give vitamin K and reserve FFP for bleeding or procedures.
- NAC in non-paracetamol ALF — empirically in early-stage encephalopathy (Lee 2009 transplant-free survival benefit).
- Pregnancy-related ALF — deliver the baby for AFLP and HELLP.
- Amanita phalloides — foraging history, GI prodrome, penicillin G and silibinin.
- Hyperacute versus subacute — hyperacute (paracetamol, best survival) versus subacute (indeterminate, worst survival). [1]
References
[1] O'Grady (1989) — Derived the King's College Criteria from 588 patients with fulminant hepatic failure; etiology-specific criteria for paracetamol and non-paracetamol ALF. [2] Lee WM (1993) — Authoritative NEJM review of ALF; definition, causes, pathophysiology and management. [3] Ostapowicz / US ALFSG (2002) — Prospective study of 308 ALF patients at 17 US centres; paracetamol 39 percent, idiosyncratic drugs 13 percent, viral 12 percent; transplant-free survival 67 percent. [4] Bernal (2002) — Arterial lactate above 3.5 on admission or above 3.0 after fluids identifies non-survivors a median of 6 hours before the King's College Criteria. [5] Keays (1991) — IV NAC improves survival in established paracetamol-induced fulminant hepatic failure, even when given after injury is established. [6] Lee (2009) — IV NAC improves transplant-free survival in early-stage non-acetaminophen ALF (173 patients, 24 US centres). [7] Stravitz and Lee (2019) — Lancet Seminar on ALF; modern pathophysiology (DAMPs, SIRS-CARS), management and outcomes. [8] Bernal and Wendon (2013) — NEJM review; comprehensive management of ALF including the rebalanced haemostasis concept and the contraindication to routine INR correction. [9] Tujios, Stravitz and Lee (2022) — Management of ALF update; cerebral oedema (no corticosteroids), cause-specific treatment, and the early transplant referral principle.
AASLD Practice Guidance on Acute Liver Failure (2023); EASL Clinical Practice Guidelines on acute liver failure; GESA hepatology guidelines; ANZLIC (Australian and New Zealand Liver Intensive Care) guidance. [1]
References
- [1]O'Grady JG, Alexander GJM, Hayllar KM, Williams R Early indicators of prognosis in fulminant hepatic failure Gastroenterology, 1989.PMID 2490426
- [2]Lee WM Acute liver failure N Engl J Med, 1993.PMID 8305063
- [3]Ostapowicz G, Fontana RJ, Schiodt FV, et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States Ann Intern Med, 2002.PMID 12484709
- [4]Bernal W, Donaldson N, Wyncoll D, Wendon J Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure: a cohort study Lancet, 2002.PMID 11867109
- [5]Keays R, Harrison PM, Wendon JA, et al. Intravenous acetylcysteine in paracetamol induced fulminant hepatic failure: a prospective controlled trial BMJ, 1991.PMID 1954453
- [6]Lee WM, Hynan LS, Rossaro L, et al. Intravenous N-acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure Gastroenterology, 2009.PMID 19524577
- [7]Stravitz RT, Lee WM Acute liver failure Lancet, 2019.PMID 31498101
- [8]Bernal W, Wendon J Acute liver failure N Engl J Med, 2013.PMID 24369077
- [9]Tujios SR, Stravitz RT, Lee WM Management of Acute Liver Failure: Update 2022 Semin Liver Dis, 2022.PMID 36001996