Phys · hepatic
Hepatocellular Carcinoma
Also known as hepatocellular carcinoma · HCC · hepatoma · primary liver cancer · liver cell carcinoma · Barcelona Clinic Liver Cancer · BCLC · LI-RADS · Milan criteria · transarterial chemoembolisation · TACE · radiofrequency ablation · RFA · sorafenib · lenvatinib · atezolizumab bevacizumab · alpha-fetoprotein · AFP
Consultant-physician guide to hepatocellular carcinoma — the cirrhosis-driven malignancy whose entire management hangs on the Barcelona Clinic Liver Cancer (BCLC) staging system. Covers the at-risk populations requiring six-monthly surveillance (all cirrhosis, selected chronic HBV without cirrhosis), LI-RADS imaging-based diagnosis without biopsy in the cirrhotic liver, BCLC stage-by-stage treatment allocation (resection, ablation, transplant within Milan criteria, TACE, and the systemic therapy ladder from atezolizumab-bevacizumab through sorafenib, lenvatinib and second-line TKIs), management of the underlying liver disease, and the prognosis by treatment modality. Structured for FRACP DWE and DCE, MRCP, and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Hepatocellular Carcinoma

The answer first
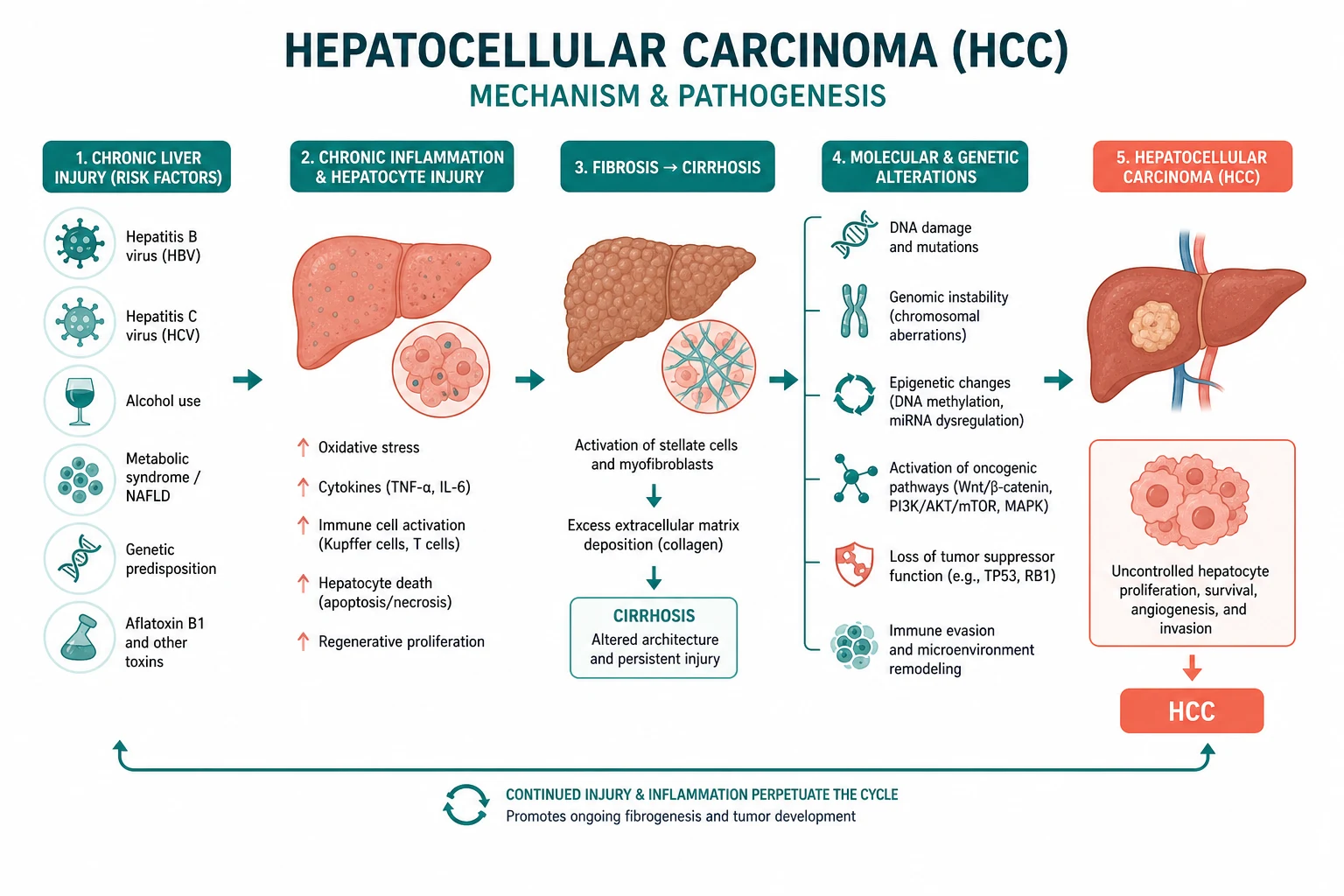
Hepatocellular carcinoma (HCC) is a primary malignancy of the hepatocyte that arises, in the great majority of cases, on the background of cirrhosis. It is the sixth most common cancer worldwide and the third leading cause of cancer-related death. Its incidence is rising, driven by the non-alcoholic fatty liver disease (NAFLD/MASLD) epidemic in Western populations alongside persistent HBV and HCV burdens globally [1].
The single organising principle: HCC management is driven by the Barcelona Clinic Liver Cancer (BCLC) staging system, which links tumour burden, liver function (Child-Pugh score) and performance status (ECOG) to a treatment allocation. Know the BCLC algorithm and you know HCC. Everything else — surveillance, LI-RADS imaging, the systemic therapy ladder — feeds into the staging decision [2][1].
The treatment ladder, by stage: [1]
- BCLC 0 (very early) and BCLC A (early) — curative: resection, thermal ablation (RFA or MWA), or liver transplant (within Milan criteria).
- BCLC B (intermediate) — transarterial chemoembolisation (TACE) for multinodular disease without vascular invasion.
- BCLC C (advanced) — systemic therapy: first-line atezolizumab plus bevacizumab (for Child-Pugh A), or sorafenib or lenvatinib as single-agent TKI alternatives; second-line regorafenib, cabozantinib, or ramucirumab.
- BCLC D (terminal) — best supportive care. [1]
DWE high-yield: The answer to almost every HCC management question is "apply the BCLC stage." A cirrhotic patient with a single lesion under 5 cm, Child-Pugh A and ECOG 0 is BCLC A — curative therapy (resection, ablation, or transplant). A patient with portal vein invasion is BCLC C — systemic therapy. A patient with Child-Pugh C and no transplant option is BCLC D — best supportive care [2][1].
Epidemiology and risk factors
HCC is the sixth most commonly diagnosed cancer worldwide and the third leading cause of cancer death (after lung and colorectal cancer). The global incidence is rising, and the rise in Western countries is disproportionately driven by NAFLD/MASLD-associated cirrhosis, alongside ageing HCV cohorts and the ongoing HBV burden in sub-Saharan Africa and East and Southeast Asia [1].
The cirrhosis substrate — and the exceptions
Cirrhosis from any cause is the single most important risk factor for HCC, present in 80 to 90 percent of cases. Whatever injures the liver chronically — viral, metabolic, toxic, autoimmune, cholestatic, or genetic — drives the regenerative nodularity and genomic instability that culminate in HCC. The annual incidence of HCC in cirrhosis is 1 to 8 percent, varying by aetiology [1].
The one major exception is hepatitis B, which can cause HCC in the absence of cirrhosis through direct viral oncogenesis (HBV DNA integration into the host genome, the HBx protein, and chronic immune-mediated injury). This is why HBV carriers are offered HCC surveillance even without cirrhosis, and why the HBV vaccine is the only vaccine that prevents a human cancer. [1]
| Risk factor | Mechanism | HCC risk |
|---|---|---|
| Cirrhosis (any cause) | Genomic instability, regenerative nodules | 1 to 8 percent per year |
| Hepatitis B | DNA integration, HBx oncogenesis; HCC even without cirrhosis | High, especially in endemic regions |
| Hepatitis C | Cirrhosis-mediated; HCV eradication reduces but does not abolish risk | 1 to 4 percent per year once cirrhotic |
| Alcohol | Cirrhosis; synergistic with viral hepatitis and obesity | 1 percent per year in alcoholic cirrhosis |
| NAFLD/MASLD | Metabolic syndrome, insulin resistance, lipotoxicity; fastest-rising cause in the West | Rising rapidly; can occur without cirrhosis (rare) |
| Aflatoxin (B1) | Direct DNA damage (p53 R249S mutation); synergistic with HBV | High in exposed populations (grain, nuts in tropical climates) |
| Haemochromatosis | Iron-mediated oxidative DNA damage | High if untreated; reduced by venesection |
| Alpha-1-antitrypsin deficiency | Protein accumulation, cirrhosis | Moderate (in ZZ phenotype with cirrhosis) |
DWE trap: HCC can occur in non-cirrhotic NAFLD and HBV. A fatty liver or a chronic HBV carrier with a liver lesion still needs HCC workup even if there is no clinical or radiological cirrhosis. Do not dismiss the lesion as benign on the basis of "no cirrhosis" alone. [1]
Surveillance — who, how, and how often
Surveillance aims to detect HCC at an early stage when curative therapy is still possible. The Singal 2014 meta-analysis of 47 studies and over 15 000 cirrhotic patients showed that surveillance with ultrasound (with or without AFP) was associated with early-stage detection (OR 2.08), receipt of curative treatment (OR 2.24), and improved overall survival (OR 1.90), with the survival benefit persisting after adjustment for lead-time bias [3].
Who gets surveillance?
The AASLD and EASL define the at-risk groups who benefit from surveillance [2]:
| Group | Surveillance recommended? |
|---|---|
| All patients with cirrhosis (Child-Pugh A and B) | Yes — the core group |
| HBV carriers — Asian male over 40 | Yes (even without cirrhosis) |
| HBV carriers — Asian female over 50 | Yes (even without cirrhosis) |
| HBV carriers — African descent over 20 | Yes (even without cirrhosis; high early incidence) |
| HBV carriers with family history of HCC | Yes |
| Stage 4 primary biliary cholangitis | Yes (selected) |
| Non-cirrhotic NAFLD | No (routine surveillance not recommended) |
| Child-Pugh C cirrhosis, not a transplant candidate | No (no survival benefit) |
The age thresholds for HBV surveillance are set because HBV-related HCC incidence varies by sex, geography and ethnicity — Asian men and African-descent patients develop HCC at younger ages and higher rates, justifying surveillance from younger ages and even in the absence of cirrhosis. [1]
How and how often?
Six-monthly liver ultrasound plus serum alpha-fetoprotein (AFP). This is the surveillance standard. The interval is based on HCC tumour doubling times: a six-monthly interval detects most tumours before they exceed curative thresholds [2][3].
The AFP is added because ultrasound alone misses small HCCs, particularly in obese patients or those with a nodular cirrhotic liver. An AFP above 20 nanograms per millilitre warrants further investigation, though AFP has limited sensitivity and specificity (it is elevated in only 60 to 70 percent of HCCs and can be raised in chronic hepatitis without HCC). [1]
When surveillance finds a lesion — LI-RADS
When a surveillance ultrasound detects a nodule (typically any lesion at or above 1 cm), the patient proceeds to multiphase contrast-enhanced CT or MRI of the liver. The findings are reported using the Liver Imaging Reporting and Data System (LI-RADS), a standardised algorithm for categorising liver observations in patients at risk for HCC [2].

LI-RADS — the imaging-based diagnosis
LI-RADS categorises liver observations from LR-1 (definitely benign) to LR-5 (definitely HCC). The genius of LI-RADS is that in a cirrhotic liver, a LI-RADS 5 lesion is diagnostic of HCC without a biopsy — the imaging features are so characteristic that histological confirmation is unnecessary. This is the principle of non-invasive diagnosis that underpins HCC management in cirrhosis [2][1].
The LI-RADS categories
| Category | Meaning | Action |
|---|---|---|
| LR-1 | Definitely benign | No further action |
| LR-2 | Probably benign | No further action |
| LR-3 | Intermediate probability | Short-interval follow-up imaging (3 to 6 months) |
| LR-4 | Probably HCC | Multidisciplinary review; biopsy or treat depending on context |
| LR-5 | Definitely HCC | Diagnose HCC non-invasively; proceed to staging and treatment |
| LR-M | Malignant, not specific for HCC | Biopsy (could be a non-HCC malignancy) |
| LR-TIV | Tumour in vein | HCC with vascular invasion — staging and treatment |
The arterial phase hyperenhancement hallmark
The key imaging feature of HCC is arterial phase hyperenhancement (the tumour lights up brighter than the surrounding liver when contrast first arrives, because HCC develops its own arterial blood supply as it dedifferentiates from a regenerative nodule). This is followed by washout in the portal venous or delayed phase (the tumour loses contrast faster than the surrounding liver). The combination of arterial hyperenhancement, washout, and a capsule or size threshold defines LI-RADS 5 [2].
DWE high-yield: The three-step imaging sequence for HCC is arterial phase hyperenhancement followed by portal venous washout, in a cirrhotic liver, on multiphase CT or MRI. That triad, in a lesion of sufficient size, is LI-RADS 5 and is diagnostic of HCC without biopsy [2].
When is biopsy needed?
Biopsy is not the default — the non-invasive imaging criteria suffice in cirrhosis. Biopsy is reserved for: [1]
- Non-cirrhotic liver — the imaging criteria are less reliable without the cirrhotic substrate; histology is needed.
- Atypical imaging — a lesion that does not meet full LI-RADS 5 criteria, or a lesion that looks malignant but not characteristic of HCC (LR-M or LR-4).
- When the diagnosis would change management — for example, distinguishing HCC from a metastasis or a cholangiocarcinoma, which have different treatment algorithms. [1]
Biopsy carries a small risk of tumour seeding along the needle track (1 to 3 percent), which is one reason non-invasive diagnosis is preferred when possible [2].

BCLC staging — the treatment allocation system
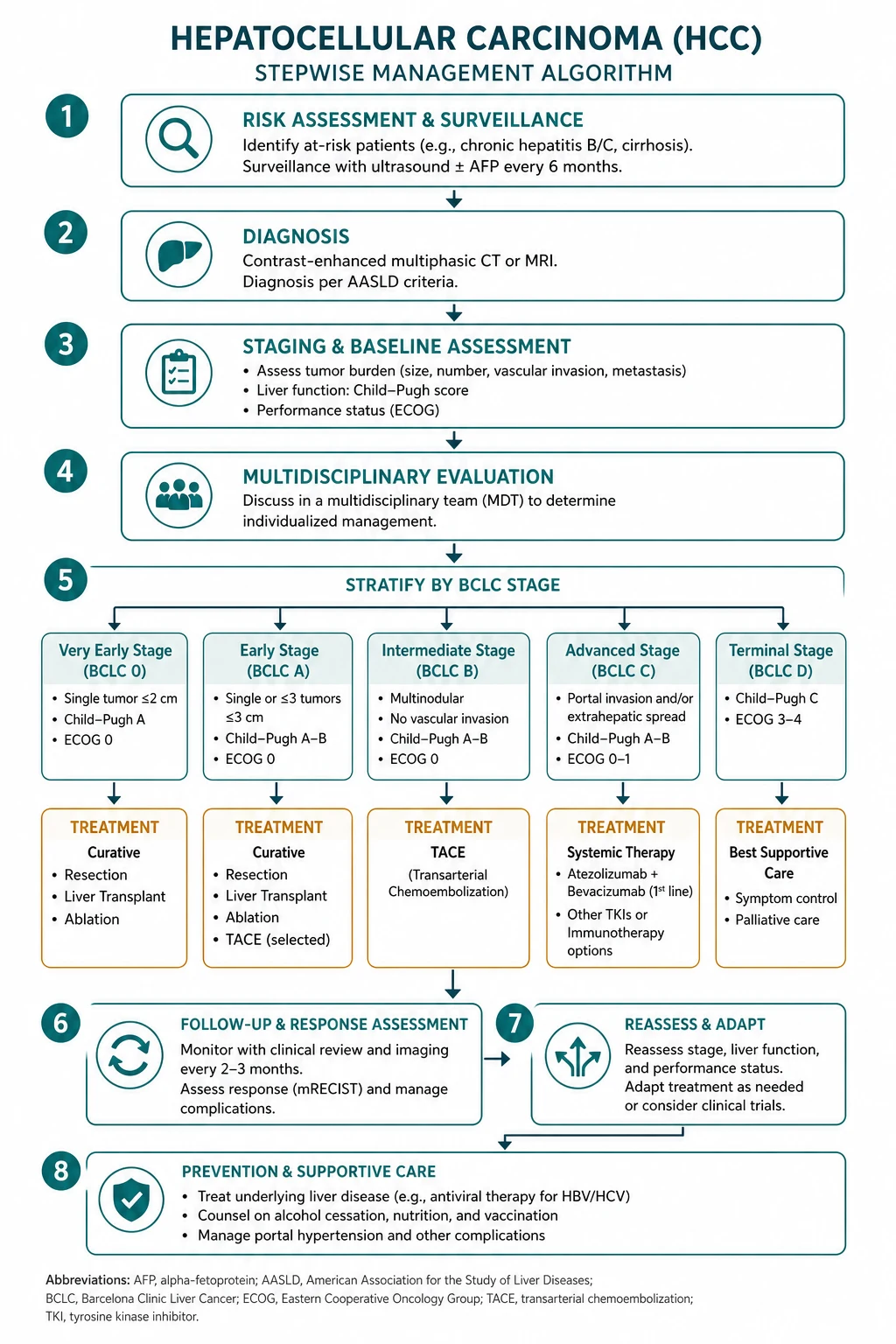
The Barcelona Clinic Liver Cancer (BCLC) staging system is the global standard for HCC because it integrates the three dimensions that determine treatment and prognosis: tumour burden, liver function (Child-Pugh score), and performance status (ECOG). It links each stage to a specific first-line treatment [2][1].
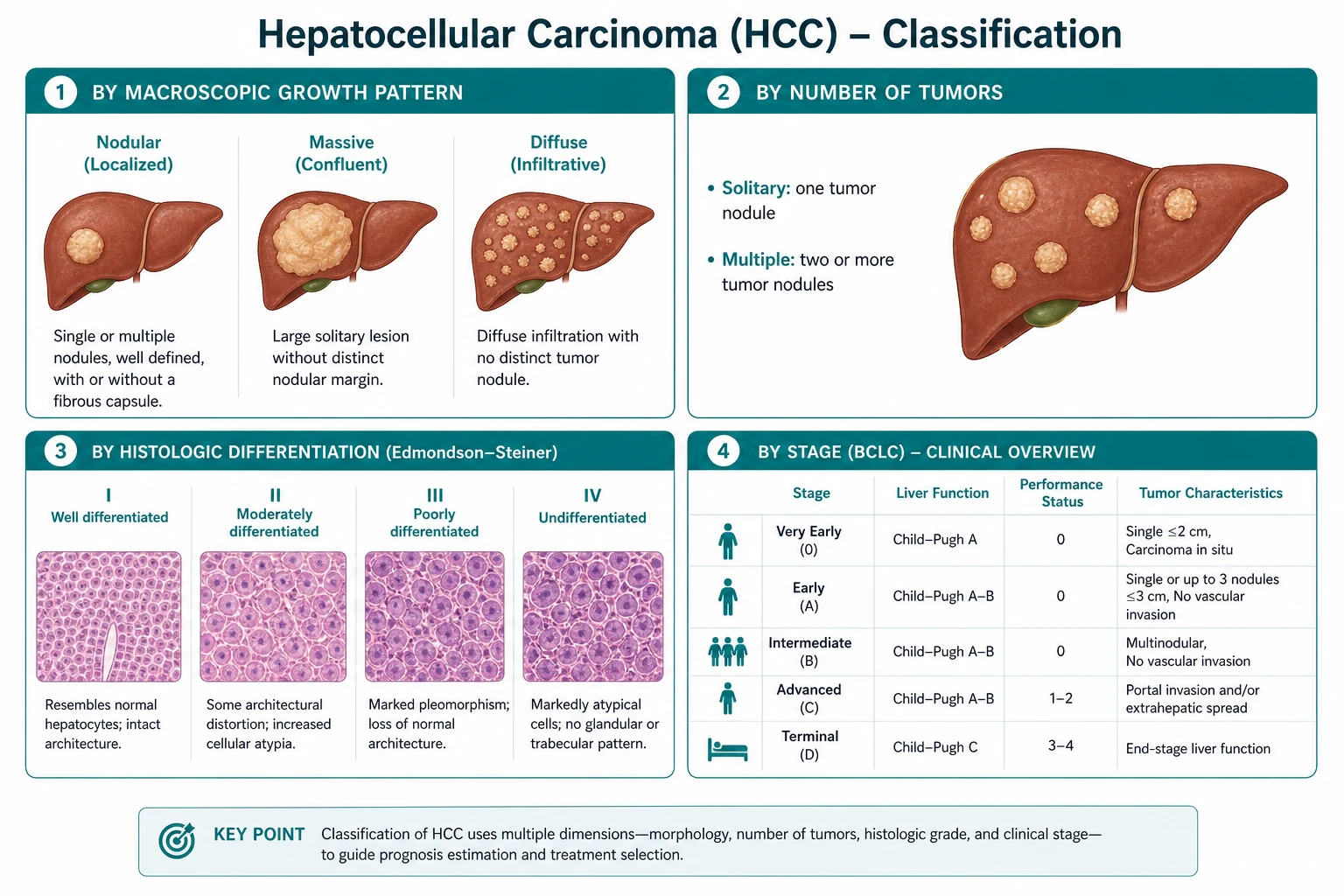
| BCLC stage | Tumour burden | Liver function | Performance status (ECOG) | First-line treatment |
|---|---|---|---|---|
| 0 (very early) | Single, under 2 cm | Child-Pugh A | 0 | Ablation or resection |
| A (early) | Single or up to 3 nodules each under 3 cm | Child-Pugh A-B | 0 | Resection, ablation, or transplant |
| B (intermediate) | Multinodular, no vascular invasion | Child-Pugh A-B | 0 | TACE |
| C (advanced) | Vascular invasion or extrahepatic spread | Child-Pugh A-B | 1 to 2 | Systemic therapy |
| D (terminal) | Any | Child-Pugh C | Above 2 | Best supportive care |

DWE high-yield: Memorise this table. The BCLC stage determines the treatment in the vast majority of MCQs and long-case discussions. The discriminators between adjacent stages are: A to B is multinodular (no longer curative); B to C is vascular invasion, extrahepatic spread, or ECOG 1 to 2 (no longer amenable to locoregional therapy); C to D is Child-Pugh C or ECOG above 2 (liver too sick or patient too unwell for active treatment) [2][1].
Child-Pugh score — the liver function dimension
The Child-Pugh score (also called Child-Turcotte-Pugh) grades liver function using five parameters: bilirubin, albumin, INR, ascites, and encephalopathy. The score assigns Child-Pugh A (5 to 6 points, compensated), B (7 to 9, decompensated), or C (10 to 15, end-stage). Most active HCC treatments — resection, TACE, systemic therapy — are reserved for Child-Pugh A patients, because the liver reserve must withstand the insult. Child-Pugh C cirrhosis with HCC is BCLC D unless the patient is a transplant candidate [2].
Treatment by BCLC stage
Stage 0 and A — curative therapy
The goal in early-stage HCC is cure. Three modalities achieve it: surgical resection, thermal ablation, and liver transplant. The choice depends on the tumour characteristics, the liver function, and the portal pressure [2][1].
Surgical resection is the first choice for a patient with preserved liver function (Child-Pugh A), a single tumour, no clinically significant portal hypertension, and no extrahepatic disease. The normal portal pressure is essential because resection removes functional liver volume, and a patient with portal hypertension is at high risk of post-hepatectomy liver failure and decompensation. In well-selected patients, five-year survival after resection is 50 to 70 percent. Resection is the default curative option for HCC in a non-cirrhotic liver (where portal hypertension is absent and liver reserve is generous). [1]
Thermal ablation — radiofrequency ablation (RFA) or microwave ablation (MWA) — is the first choice for tumours under 3 cm (especially under 2 cm, BCLC 0), where it achieves complete necrosis in over 90 percent of cases and rivals surgery. It is particularly suitable for patients who are not resection candidates (because of comorbidity, liver function, or tumour location). For a single tumour under 2 to 3 cm in a Child-Pugh A patient, ablation and resection offer comparable outcomes. [1]
Liver transplant is the theoretically ideal treatment because it removes both the tumour and the diseased liver (eliminating the field defect from which new tumours arise). It is reserved for patients within the Milan criteria: a single tumour under 5 cm, or up to 3 tumours each under 3 cm, with no vascular invasion or extrahepatic spread. Within these criteria, five-year post-transplant survival is around 70 percent with a recurrence rate under 15 percent. Transplant is the treatment of choice for HCC in a patient with decompensated cirrhosis (who cannot tolerate resection) — the tumour must be within Milan criteria, and the patient must otherwise be a transplant candidate [2][1].
DWE high-yield — the Milan criteria: single lesion under 5 cm OR up to 3 lesions each under 3 cm, no macrovascular invasion, no extrahepatic spread. Within Milan criteria, a patient with HCC and decompensated cirrhosis gets a liver transplant. This is one of the most frequently tested facts in hepatology exams [2].
Stage B — TACE
Transarterial chemoembolisation (TACE) is the standard first-line treatment for BCLC B (intermediate): multinodular HCC without vascular invasion or extrahepatic spread, in a patient with preserved liver function (Child-Pugh A-B) and good performance status. TACE works by delivering chemotherapy (typically doxorubicin or cisplatin) directly into the hepatic artery feeding the tumour, followed by embolisation of the artery to cut off the blood supply and trap the drug. HCC is uniquely dependent on the hepatic artery (normal liver is predominantly portal-venous, but HCC is arterial), which is the biological rationale for TACE [2][1].
TACE is repeated at intervals (typically every 6 to 8 weeks) until the tumour is controlled, then continued as needed. Five-year survival with TACE is 20 to 30 percent. The complications include post-embolisation syndrome (fever, pain, nausea — common and self-limiting), and more seriously hepatic decompensation (TACE sacrifices some liver function with each treatment, so Child-Pugh C patients are excluded). Absolute contraindications to TACE include portal vein thrombosis (the portal vein must be patent because the hepatic artery embolisation devascularises the tumour, and the liver relies on the portal vein), total bilirubin above 2 to 3 mg/dL (around 35 to 50 micromol/L), and Child-Pugh C cirrhosis. [1]
DWE trap: TACE requires a patent portal vein. If the portal vein is thrombosed (whether by tumour or bland thrombus), TACE is contraindicated because embolising the hepatic artery in this setting risks total hepatic ischaemia. Portal vein tumour thrombus also upstages the patient to BCLC C. [1]
Stage C — systemic therapy
BCLC C (advanced) HCC — defined by vascular invasion (most commonly portal vein tumour thrombus), extrahepatic spread, or cancer-related symptoms (ECOG 1 to 2) — is treated with systemic therapy. The landscape has been transformed in the last five years [5][4][6].
First-line — atezolizumab plus bevacizumab: The IMbrave150 trial (Finn 2020) established the combination of atezolizumab (a PD-L1 inhibitor) and bevacizumab (a VEGF inhibitor) as the new first-line standard for unresectable HCC in Child-Pugh A patients. The combination significantly improved overall survival compared to sorafenib (median OS 19.2 months vs 13.4 months with sorafenib; HR 0.66) [5]. Before starting this regimen, every patient must have an upper GI endoscopy to identify and treat varices — bevacizumab's anti-VEGF effect can precipitate catastrophic variceal bleeding from untreated varices. This is a high-yield safety point.
First-line alternatives — sorafenib and lenvatinib: For patients who cannot receive or decline atezolizumab-bevacizumab, the single-agent tyrosine kinase inhibitors remain the alternative first-line options. Sorafenib was the first agent to show a survival benefit in advanced HCC, in the landmark SHARP trial (Llovet 2008): median OS 10.7 months vs 7.9 months with placebo [4]. Lenvatinib was shown to be non-inferior to sorafenib in the REFLECT trial (Kudo 2018), with a median OS of 13.6 months vs 12.3 months for sorafenib [6]. Lenvatinib cannot be used if the tumour involves the bile duct, if there is tumour occupation of more than 50 percent of the liver, or in main portal vein invasion.
| First-line systemic agent | Trial | Key result | Cautions |
|---|---|---|---|
| Atezolizumab + bevacizumab | IMbrave150 (2020) | Median OS 19.2 months (vs sorafenib 13.4) | Must scope for varices first; autoimmune disease; bleeding risk |
| Lenvatinib | REFLECT (2018) | Median OS 13.6 months (non-inferior to sorafenib) | Excludes main bile duct invasion, over 50 percent liver occupation |
| Sorafenib | SHARP (2008) | Median OS 10.7 months (vs placebo 7.9) | Hand-foot skin reaction, diarrhoea, hypertension |
Second-line options: For patients who progress on or cannot tolerate first-line therapy, second-line agents include regorafenib (the RESORCE trial, Bruix 2017, showed improved OS after sorafenib progression: median OS 10.6 months vs 7.8 months with placebo [7]), cabozantinib (a TKI targeting MET and VEGFR), and ramucirumab (a VEGFR2 antibody, particularly useful in patients with a high AFP above 400 ng/mL). These second-line options extend survival in selected patients.
DWE high-yield: The current first-line systemic therapy for advanced HCC in a fit patient with Child-Pugh A cirrhosis is atezolizumab plus bevacizumab. The pre-treatment requirement that examiners love is the upper GI endoscopy — untreated varices plus bevacizumab equals a catastrophic bleed. For patients who cannot receive immunotherapy, sorafenib or lenvatinib are the single-agent TKI alternatives [5][4][6].
Stage D — best supportive care
BCLC D (terminal) HCC — Child-Pugh C cirrhosis that is not a transplant candidate, or ECOG performance status above 2 — has a median survival under 3 months. Active anti-cancer treatment offers no benefit and carries harm. The management is best supportive care: pain control, nutritional support, management of ascites and encephalopathy, psychological support, and palliative care involvement. If the patient is within transplant criteria and otherwise suitable, even Child-Pugh C patients can be considered for transplant — but the BCLC D label applies to those who are NOT transplant candidates [2].
Management of the underlying liver disease
Treating the HCC without treating the underlying liver disease is incomplete management. The liver disease determines the treatment options, the treatment tolerance, and the risk of future HCC in the remaining liver. [1]
| Underlying cause | Action |
|---|---|
| Hepatitis C | Antiviral therapy (DAAs) to achieve sustained virological response; reduces but does not eliminate HCC risk |
| Hepatitis B | Antiviral suppression (entecavir or tenofovir); reduces HCC incidence |
| Alcohol | Abstinence; alcohol support services; nutrition |
| NAFLD/MASLD | Weight loss, metabolic optimisation (diabetes, lipids, blood pressure) |
| Haemochromatosis | Venesection to deplete iron stores |
| Portal hypertension | Optimise — non-selective beta-blocker or endoscopic band ligation for variceal prophylaxis; this is mandatory before starting bevacizumab |
A critical point: successful HCV eradication reduces but does not eliminate the HCC risk in a cirrhotic patient. Surveillance must continue after a sustained virological response (SVR) because the cirrhosis (the field defect) persists [1].
Prognosis
HCC prognosis depends on the stage at diagnosis and the treatment received. The five-year survival figures by treatment modality are high-yield for exams: [1]
| Treatment modality | Five-year survival | Median OS (advanced) |
|---|---|---|
| Surgical resection (well-selected) | 50 to 70 percent | — |
| Liver transplant (within Milan criteria) | Around 70 percent | — |
| Thermal ablation (small single tumour) | Comparable to resection for tumours under 2 to 3 cm | — |
| TACE | 20 to 30 percent | — |
| Atezolizumab + bevacizumab | — | Median OS 19.2 months |
| Sorafenib | — | Median OS 10.7 months |
| Lenvatinib | — | Median OS 13.6 months |
| Best supportive care (BCLC D) | — | Under 3 months |
The prognosis is also shaped by the underlying liver disease — a patient with a resected early HCC but Child-Pugh B cirrhosis has a higher risk of liver-related death (decompensation, a second HCC) than a patient with a resected early HCC in a non-cirrhotic liver [1][2].
HCC rupture — the acute presentation
Spontaneous HCC rupture is a dramatic and life-threatening presentation: sudden severe abdominal pain, haemodynamic instability, and peritonism in a patient with known or occult cirrhosis. It is more common in advanced tumours and in Asian populations. The management is resuscitation (fluids, blood products, correction of coagulopathy), followed by urgent transarterial embolisation (TAE) to control the bleeding — TACE's non-chemotherapy cousin, focused purely on haemostasis. Surgical ligation or packing is a last resort. After stabilisation, the patient is staged and treated according to the BCLC system, with the caveat that ruptured HCC is generally advanced. [1]
The common exam traps
- Diagnosing HCC with biopsy in a cirrhotic liver — the diagnosis is imaging-based (LI-RADS 5 on multiphase CT or MRI). Biopsy is reserved for non-cirrhotic livers, atypical lesions, or when histology would change management. Biopsy risks tumour seeding.
- Treating a BCLC C patient with TACE — TACE is for BCLC B (multinodular, no vascular invasion). Vascular invasion upstages to BCLC C, where systemic therapy is the answer. The patent portal vein requirement is the key contraindication.
- Starting atezolizumab-bevacizumab without scoping for varices — untreated varices plus bevacizumab can cause catastrophic haemorrhage. Upper GI endoscopy is mandatory before starting this regimen.
- Offering transplant outside Milan criteria — transplant is for a single tumour under 5 cm or up to 3 tumours each under 3 cm, without vascular invasion or extrahepatic spread. Outside these criteria, the recurrence rate is prohibitive.
- Stopping HCC surveillance after HCV SVR — the cirrhosis persists after viral eradication, and so does the HCC risk. Surveillance continues for life.
- Missing HBV-related HCC without cirrhosis — HBV causes HCC by direct oncogenesis, not only through cirrhosis. The HBV surveillance criteria (Asian male over 40, Asian female over 50, African over 20, family history) apply even without cirrhosis.
- Confusing Child-Pugh C with transplant contraindication — Child-Pugh C is BCLC D only if the patient is NOT a transplant candidate. Within Milan criteria, a Child-Pugh C patient may be an urgent transplant candidate.
- Overusing AFP as a diagnostic test — AFP is a surveillance adjunct, not a standalone diagnostic test. It is normal in 30 to 40 percent of HCCs and elevated in non-malignant liver disease. Diagnosis is imaging-based. [1]
Regional guideline anchoring
- ANZ (GESA, TSANZ) — BCLC staging as the framework, six-monthly US plus AFP surveillance for cirrhosis and selected HBV, LI-RADS imaging diagnosis, multidisciplinary management. Transplant criteria broadly aligned with Milan. Systemic therapy access via PBS for atezolizumab-bevacizumab, sorafenib, lenvatinib, and second-line TKIs under specific criteria.
- UK (BSG, NICE) — BCLC staging, surveillance as above, NICE guidelines on HCC management. London and regional liver centres manage transplant and systemic therapy.
- US (AASLD) — the 2018 Practice Guidance (Marrero) is the key reference; updated 2023 guidance incorporates the systemic therapy advances. LI-RADS is an ACR/AASLD-endorsed system.
- Europe (EASL) — the EASL Clinical Practice Guidelines on HCC, broadly aligned with the AASLD guidance; BCLC is the European-originated staging system. [1]
Drug doses are verified; the ANZ regimen is primary where it differs. Systemic therapy dosing: sorafenib 400 mg twice daily, lenvatinib 8 mg daily (above 60 kg) or 12 mg daily (below 60 kg), atezolizumab 1200 mg plus bevacizumab 15 mg/kg every 3 weeks, regorafenib 160 mg daily (weeks 1 to 3 of a 4-week cycle). [1]
Summary
Hepatocellular carcinoma is a cirrhosis-driven malignancy whose entire management hangs on the BCLC staging system — the framework that links tumour burden, liver function (Child-Pugh) and performance status (ECOG) to a treatment allocation. Surveillance with six-monthly ultrasound plus AFP targets all cirrhotic patients and selected HBV carriers. Diagnosis is imaging-based (LI-RADS 5 on multiphase CT or MRI) in the cirrhotic liver, without biopsy. Treatment by stage: BCLC 0 and A are curative (resection, ablation, or transplant within Milan criteria); BCLC B gets TACE; BCLC C gets systemic therapy (first-line atezolizumab-bevacizumab, with sorafenib and lenvatinib as single-agent alternatives); BCLC D is best supportive care. Manage the underlying liver disease alongside the tumour, and never stop surveillance after HCV eradication — the cirrhosis persists. [1]
One-line answer for the viva: "I manage hepatocellular carcinoma by the Barcelona Clinic Liver Cancer staging system. The cirrhotic patient with a single lesion under 5 cm, Child-Pugh A and ECOG 0 is BCLC A — I offer curative therapy, choosing between resection, ablation and transplant (within Milan criteria). Multinodular disease without vascular invasion is BCLC B — TACE. Portal vein invasion or metastasis is BCLC C — systemic therapy, first-line atezolizumab plus bevacizumab after I scope for varices, with sorafenib or lenvatinib as alternatives. Child-Pugh C without a transplant option is BCLC D — best supportive care. I diagnose non-invasively with LI-RADS on multiphase imaging, I manage the underlying liver disease alongside the tumour, and I continue surveillance for life." [1]
Sources
Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers 2021;7:6 [1]; Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the AASLD. Hepatology 2018;68(2):723-750 [2]; Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLoS Med 2014;11(4):e1001624 [3]; Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in Advanced Hepatocellular Carcinoma. N Engl J Med 2008;359(4):378-390 [4]; Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med 2020;382(20):1894-1905 [5]; Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma. Lancet 2018;391(10126):1163-1173 [6]; Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE). Lancet 2017;389(10064):56-66 [7].
AASLD 2018 Practice Guidance on Hepatocellular Carcinoma; EASL Clinical Practice Guidelines on Hepatocellular Carcinoma; LI-RADS (American College of Radiology); GESA hepatology guidelines. [1]
References
- [1]Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma Nat Rev Dis Primers, 2021.PMID 33479224
- [2]Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases Hepatology, 2018.PMID 29624699
- [3]Singal AG, Pillai A, Tiro J Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis PLoS Med, 2014.PMID 24691105
- [4]Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma N Engl J Med, 2008.PMID 18650514
- [5]Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma N Engl J Med, 2020.PMID 32402160
- [6]Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial Lancet, 2018.PMID 29433850
- [7]Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial Lancet, 2017.PMID 27932229