Phys · hepatic
Portal Hypertension
Also known as portal HTN · portosystemic hypertension · variceal bleeding · oesophageal varices · gastric varices · portal hypertensive gastropathy · refractory ascites · spontaneous bacterial peritonitis · hepatorenal syndrome · hepatic encephalopathy
Consultant-physician-depth guide to portal hypertension — HVPG thresholds, pathophysiology, variceal bleeding, ascites, SBP, hepatorenal syndrome, and hepatic encephalopathy — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Portal Hypertension
The answer first
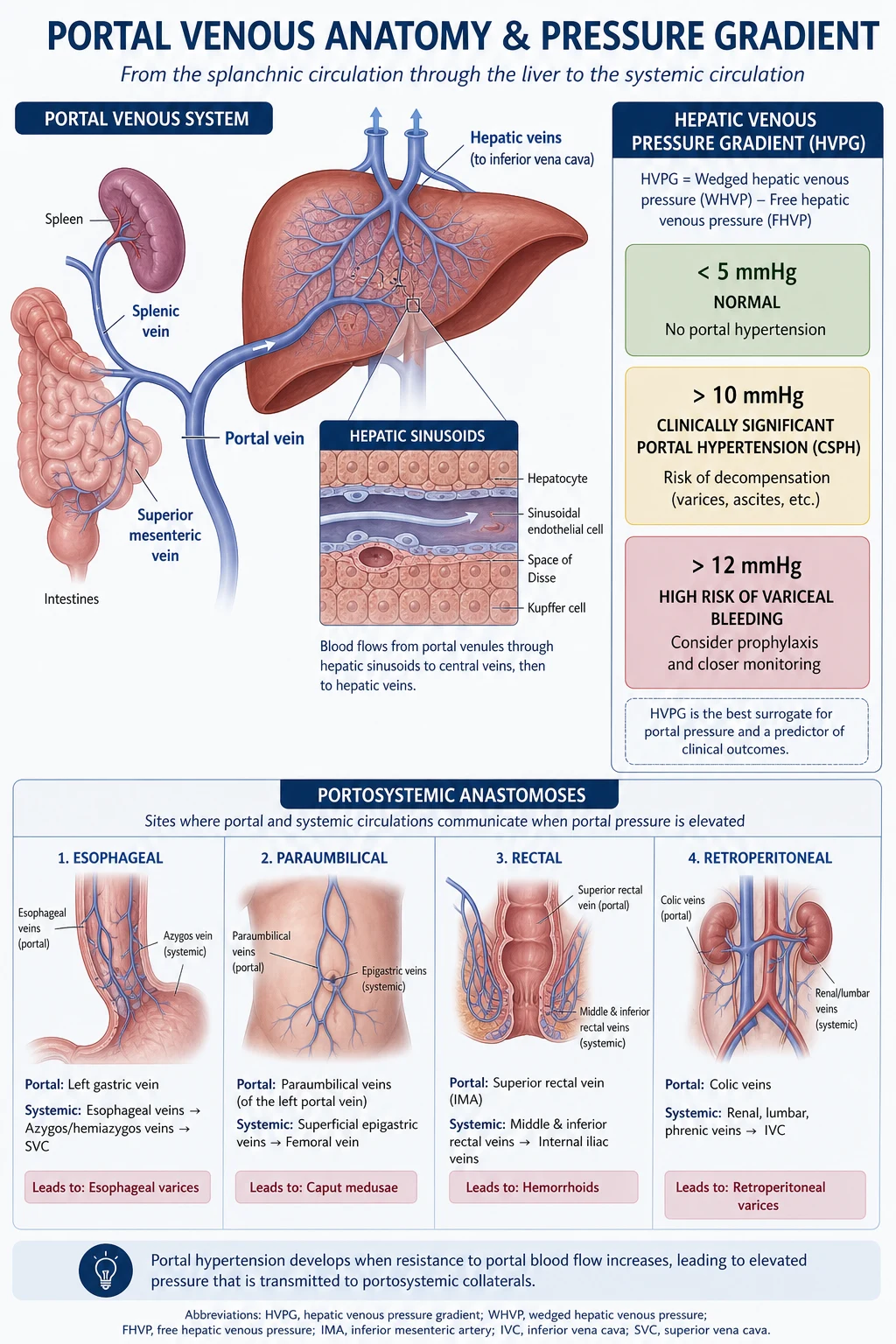
Portal hypertension is the pathophysiological driver of nearly every complication of cirrhosis. It is defined by an elevated hepatic venous pressure gradient (HVPG) — the pressure difference between the portal vein and the inferior vena cava, measured by hepatic venous catheterisation. The normal HVPG is 3 to 5 mmHg. [1]
Four thresholds define the clinical landscape and must be memorised: [1]
| HVPG | Clinical significance | Action |
|---|---|---|
| Greater than 5 mmHg | Portal hypertension present | Identify cause; screen for varices |
| Greater than or equal to 10 mmHg | Clinically significant portal hypertension (CSPH) — varices form, decompensation risk begins | NSBB to prevent first decompensation |
| Greater than 12 mmHg | Variceal bleeding threshold — varices rupture at this pressure | Primary prophylaxis (NSBB or EVL) |
| Greater than or equal to 20 mmHg | Acute bleeding treatment failure — high early rebleeding and mortality risk | Consider early pre-emptive TIPS |
The management logic flows from these thresholds: lower the gradient pharmacologically (non-selective beta-blockers), mechanically (endoscopic band ligation), or by shunting (TIPS), and treat each downstream complication — varices, ascites, spontaneous bacterial peritonitis, hepatorenal syndrome, and hepatic encephalopathy — as part of an integrated plan. [1]
Pathophysiology
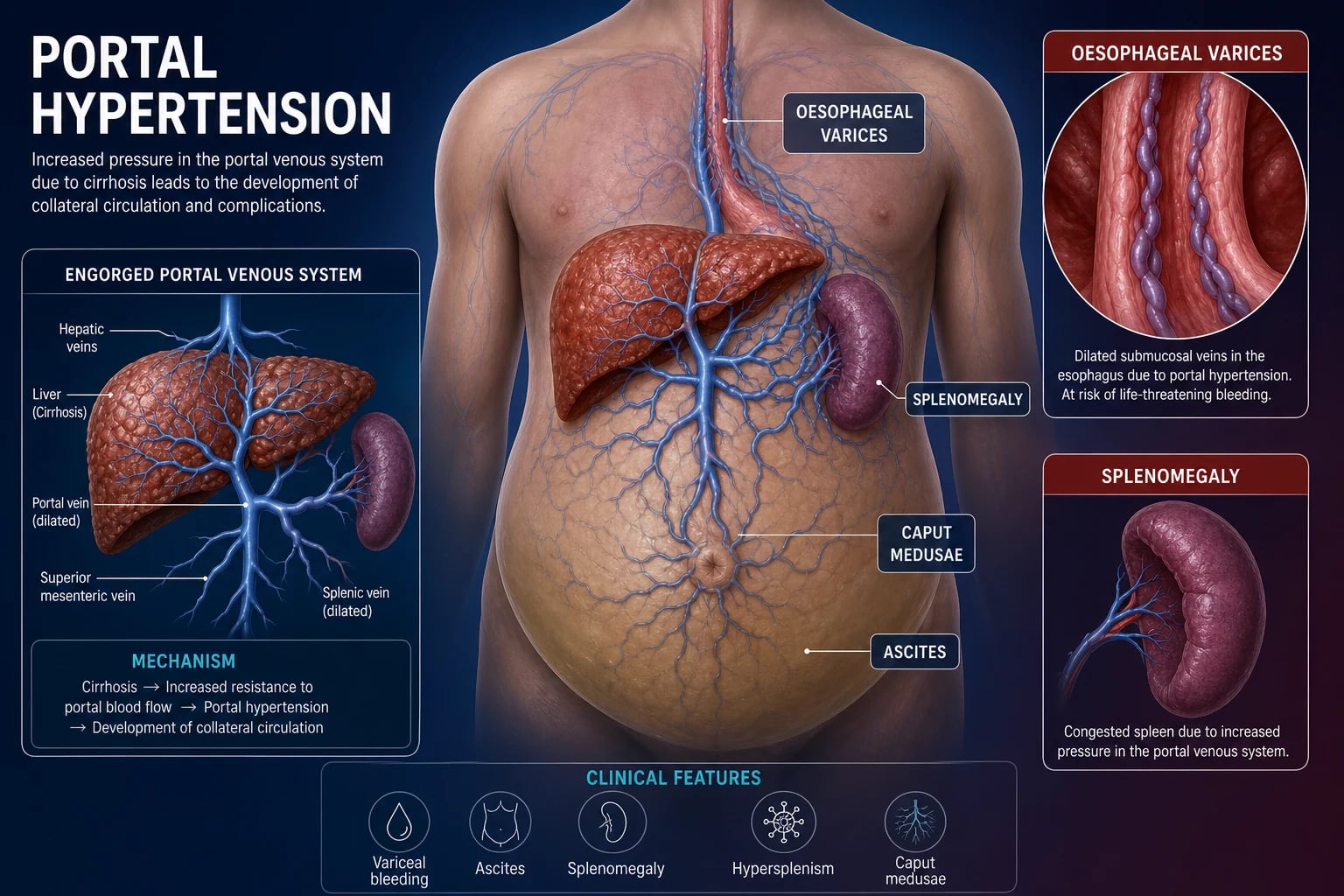
Portal pressure is determined by the product of portal blood flow and intrahepatic resistance. In cirrhosis, both increase: resistance rises from structural distortion (fibrosis, regenerative nodules) and functional sinusoidal constriction (activated hepatic stellate cells), while splanchnic blood flow rises from vasodilatory mediators (nitric oxide, glucagon) that create a hyperdynamic circulation. [1]
This is the forward flow theory: portal hypertension is not just a plumbing obstruction. Splanchnic vasodilatation drives ever-increasing portal inflow, worsening pressure even as collaterals (varices) form to decompress the system. Understanding this is essential — vasoactive drugs (terlipressin, octreotide, somatostatin) work by constricting splanchnic arterioles and reducing portal inflow, not by acting on the liver itself. [1]
Classification by site of obstruction
| Level | Examples | Key discriminator |
|---|---|---|
| Prehepatic | Portal or splenic vein thrombosis, congenital atresia | Liver architecture normal; isolated varices without cirrhosis |
| Intrahepatic — presinusoidal | Schistosomiasis (commonest worldwide), primary biliary cholangitis early, sarcoidosis | Preserved synthetic function; varices precede cirrhosis |
| Intrahepatic — sinusoidal | Cirrhosis (commonest in ANZ/UK/US), alcoholic hepatitis | Classic combination: varices plus impaired synthetic function |
| Intrahepatic — postsinusoidal | Veno-occlusive disease (sinusoidal obstruction syndrome), right heart failure late stage | Hepatomegaly, ascites |
| Posthepatic | Budd-Chiari syndrome, right heart failure, constrictive pericarditis, severe tricuspid regurgitation | JVP elevated (cardiac causes); acute presentation with painful hepatomegaly (Budd-Chiari) |
Exam tip: If the question describes varices with a normal liver biopsy and preserved synthetic function, think prehepatic or presinusoidal. Schistosomiasis is the world's commonest cause of presinusoidal portal hypertension. [1]
Varices — formation, screening, and endoscopic classification
Varices are portosystemic collaterals that develop when portal pressure exceeds 10 mmHg. They form at four main sites: [1]
- Oesophagogastric (distal oesophagus and gastric fundus) — the clinically dominant site, responsible for most variceal bleeding
- Periumbilical (caput medusae via the recanalised umbilical vein)
- Rectal (anorectal varices — distinct from haemorrhoids)
- Retroperitoneal [1]
Screening and surveillance
Every patient diagnosed with cirrhosis should have an upper endoscopy to screen for varices. If no varices are found, repeat in 2 to 3 years; if small varices, repeat in 1 to 2 years. [1]
Baveno VII refined this with non-invasive rules that spare many patients endoscopy: [1]
- Rule out varices needing treatment (sensitivity above 90 percent): liver stiffness measurement (LSM) below 25 kPa plus platelet count above 150, with no prior decompensation — these patients can avoid endoscopy.
- Rule in CSPH: LSM at or above 25 kPa is highly predictive of CSPH.
- LSM and platelets should be reassessed annually; if platelet drops or LSM rises, endoscopy is indicated. [1]
Endoscopic classification of oesophageal varices
Size is the primary determinant of bleeding risk: [1]
| Size | Description | Approximate bleeding risk per year (without prophylaxis) |
|---|---|---|
| Small (F1) | Minimally elevated above mucosa | Low (5 to 8 percent) |
| Medium (F2) | Occupies less than one-third of lumen | Moderate (10 to 15 percent) |
| Large (F3) | Occupies more than one-third of lumen | High (15 to 30 percent) |
Red signs indicate elevated bleeding risk independent of size: red wale marks (longitudinal dilated venules on the varix), cherry-red spots, and diffuse erythema. Large varices with red wale signs carry the highest bleeding risk. [1]
High-risk varices = medium or large varices, or small varices with red signs, in a Child-Pugh C patient. [1]
Gastric varices — Sarin classification
Gastric varices bleed less frequently but more severely than oesophageal varices. The Sarin classification: [1]
| Type | Location | Notes |
|---|---|---|
| GOV1 | Gastro-oesophageal, along lesser curvature | Commonest; often extension of oesophageal varices |
| GOV2 | Gastro-oesophageal, along greater curvature (fundus) | Higher bleeding risk |
| IGV1 | Isolated gastric, fundus | Associated with splenic vein thrombosis — consider splenectomy |
| IGV2 | Isolated gastric, elsewhere (antrum/body) | Rare |
Exam tip: IGV1 (isolated fundal varices) with normal liver should prompt investigation for splenic vein thrombosis (classically from pancreatitis or pancreatic cancer). Treatment is splenectomy, not TIPS or endoscopic therapy. [1]
Primary prophylaxis of variceal bleeding
Primary prophylaxis prevents the first variceal bleed in patients with high-risk varices (or CSPH without varices, per PREDESCI). [1]
Who gets primary prophylaxis?
- Medium/large varices (with or without red signs)
- Small varices with red signs or in Child-Pugh C patients
- Any patient with CSPH (HVPG at or above 10 mmHg), even without high-risk varices — PREDESCI showed NSBB prevent decompensation [1]
Non-selective beta-blockers (NSBB)
NSBB reduce portal pressure by two mechanisms: unopposed beta-2 vasodilatation causes splanchnic vasoconstriction (reducing portal inflow), and reduced cardiac output (beta-1 blockade) reduces splanchnic perfusion. [1]
| Agent | Starting dose | Titration | Target |
|---|---|---|---|
| Propranolol | 20 to 40 mg orally BID | Increase gradually | Resting HR 55 to 60; not below 55 |
| Nadolol | 40 mg orally OD | Increase to 80 to 160 mg OD | Resting HR 55 to 60 |
| Carvedilol | 6.25 mg orally OD | Increase to 12.5 mg OD (max) | Resting HR 55 to 60; systolic BP above 90 |
Carvedilol is increasingly preferred because it adds anti-alpha-1 vasodilatation, producing a greater HVPG reduction (about 20 percent vs 10 to 15 percent for propranolol). It is better tolerated at low dose but causes more hypotension — avoid in refractory ascites or systolic BP below 90. [1]
Endoscopic variceal ligation (EVL)
EVL is an alternative to NSBB for primary prophylaxis in patients with medium/large varices. Sessions are performed every 2 to 4 weeks until variceal eradication (typically 2 to 4 sessions), then surveillance endoscopy every 3 to 6 months. [1]
NSBB vs EVL — how to choose
- Either NSBB or EVL is acceptable for primary prophylaxis of high-risk varices.
- NSBB preferred if CSPH without high-risk varices (PREDESCI benefit extends to ascites prevention and decompensation reduction — EVL only prevents bleeding).
- EVL preferred if NSBB contraindicated (asthma, severe bradycardia, hypotension) or not tolerated.
- Combination (NSBB plus EVL) is not recommended for primary prophylaxis — no benefit over monotherapy and more adverse events. [1]
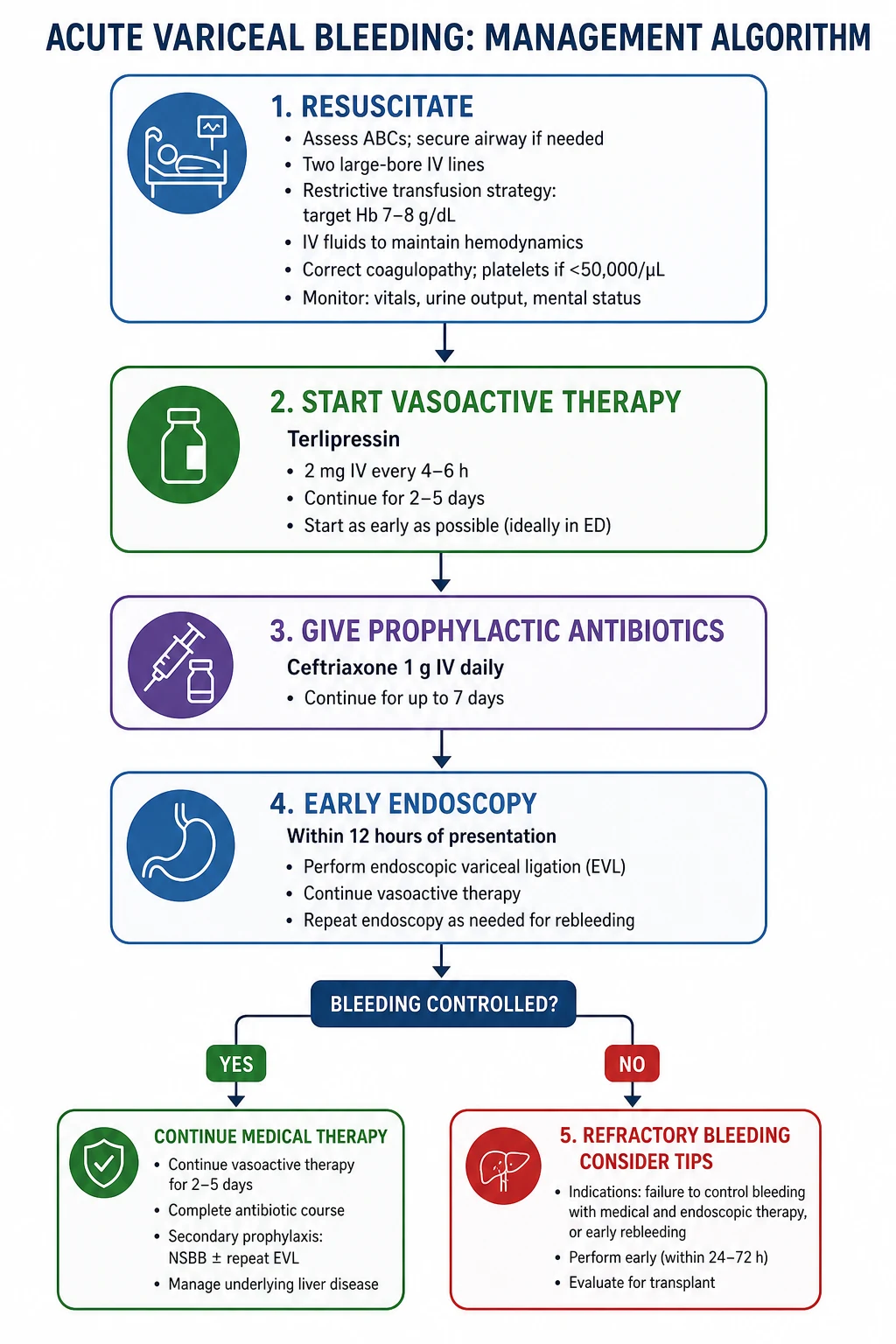
Acute variceal bleeding — the 6-hour algorithm
Acute variceal haemorrhage is a medical emergency with 15 to 25 percent six-week mortality. The evidence-based approach combines simultaneous resuscitation, vasoactive therapy, antibiotics, and endoscopic intervention within a tight time window. [1]
Step 1 — Resuscitation (immediate)
- Airway, breathing, circulation. Two large-bore IV cannulae.
- Restrictive transfusion strategy: transfuse to haemoglobin 70 to 80 g/L (target 80 to 90 g/L if active bleeding, cardiovascular disease, or elderly). Over-transfusion raises portal pressure and worsens rebleeding.
- Correct coagulopathy judiciously: do not routinely correct INR with fresh frozen plasma — it expands volume and raises portal pressure. Give platelets only if count below 50 and active bleeding. Give vitamin K 10 mg IV if INR elevated.
- Do not delay endoscopy for normalisation of INR — this never happens completely in cirrhosis and time is critical. [1]
Step 2 — Vasoactive drugs (start immediately, before endoscopy)
Begin vasoactive therapy at the time of suspected variceal bleed — do not wait for endoscopic confirmation. These drugs reduce portal inflow by constricting splanchnic arterioles and should continue for 2 to 5 days. [1]
| Drug | Dose | Notes |
|---|---|---|
| Terlipressin (preferred if available) | 2 mg IV every 4 hours for 48 hours, then 1 mg every 4 hours (total 2 to 5 days) | Most effective; side effects: ischaemia (digital, mesenteric, cardiac), respiratory failure in volume overload |
| Octreotide | 50 mcg IV bolus, then 50 mcg/hour continuous infusion | Less evidence than terlipressin but widely available in ANZ; side effects: hyperglycaemia, abdominal cramps |
| Somatostatin | 250 mcg IV bolus, then 250 mcg/hour infusion | Alternative where terlipressin unavailable |
Step 3 — Prophylactic antibiotics (start immediately)
Antibiotic prophylaxis is one of the few interventions proven to reduce mortality (not just infection) in cirrhosis with GI bleeding. Bacterial translocation and infection drive rebleeding and renal failure. [1]
- Ceftriaxone 1 g IV daily for 7 days is preferred, particularly in high-risk patients (Child-Pugh C, prior quinolone prophylaxis, hospital-acquired bleeding). Ceftriaxone is superior to norfloxacin (Fernandez, PMID 17030175).
- Oral norfloxacin 400 mg BID or ciprofloxacin 500 mg BID for 7 days is an alternative in low-risk patients. [1]
Exam trap: Forgetting antibiotics is a common and lethal error. They must be started at admission, not after infection develops. [1]
Step 4 — Endoscopic band ligation (within 12 hours)
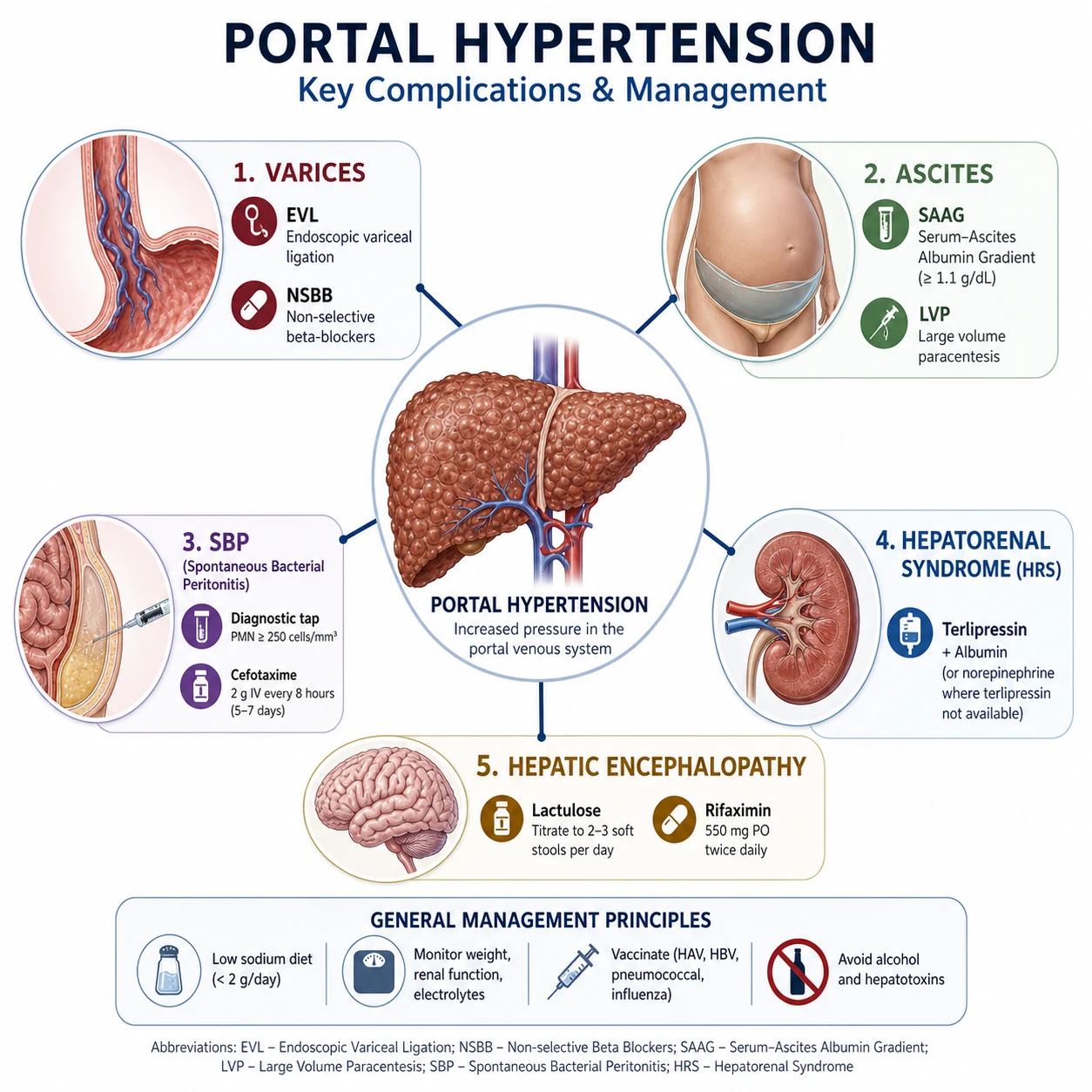
Urgent upper endoscopy within 12 hours of presentation, after resuscitation. Endoscopic band ligation (EVL) is first-line therapy for oesophageal variceal bleeding. Sclerotherapy is no longer preferred — it has higher complication rates (oesophageal ulceration, strictures, mediastinitis). [1]
For gastric variceal bleeding, cyanoacrylate (glue) injection is preferred over EVL (EVL has high rebleeding rates in gastric varices). [1]
Step 5 — Balloon tamponade or self-expanding metal stent (bridge only)
If bleeding is uncontrolled despite vasoactive drugs and before endoscopy, or if endoscopic therapy fails: [1]
- Sengstaken-Blakemore or Minnesota tube provides temporary tamponade. Inflate gastric balloon first (150 to 200 mL air/wair), apply traction, and inflate oesophageal balloon only if gastric balloon fails. Maximum 24 hours (oesophageal balloon deflated every 8 to 12 hours to prevent pressure necrosis). Intubation required for airway protection.
- Self-expanding covered metal oesophageal stents are an alternative bridge with lower complication rates and can remain in situ up to 7 days. [1]
These are bridges to definitive therapy (TIPS), not definitive treatment. [1]
Step 6 — TIPS for refractory or high-risk bleeding
Rescue TIPS is indicated for:
- Failure to control bleeding after EVL and vasoactive therapy
- Early rebleeding within 5 days despite therapy [1]
Pre-emptive (early) TIPS within 72 hours of admission — not rescue — is indicated for:
- Child-Pugh C score 10 to 13 (not above 13 — futile)
- Child-Pugh B score 8 to 9 with active bleeding observed at endoscopy [1]
The Garcia-Pagan trial (PMID 20573925) showed early TIPS in these high-risk groups reduced treatment failure (3 percent vs 50 percent) and improved one-year survival (86 percent vs 61 percent). This is a must-know DWE fact. [1]
Exam trap: Early TIPS is for Child-Pugh C (10 to 13) or Child-Pugh B with active bleeding — NOT for every bleeder. Applying it to low-risk patients exposes them to unnecessary HE risk without benefit. [1]
Secondary prophylaxis after variceal bleeding
Once a patient has bled from varices, the one-year rebleeding risk without prophylaxis is 60 to 70 percent. All survivors of variceal bleeding require lifelong secondary prophylaxis. [1]
Combination therapy is standard: NSBB plus serial EVL is superior to either alone. [1]
- NSBB (propranolol, nadolol, or carvedilol) — titrate to HR 55 to 60 or max tolerated dose
- Serial EVL every 2 to 4 weeks until eradication, then surveillance every 3 to 6 months
- Continue NSBB even after variceal eradication — it reduces portal pressure and protects against portal hypertensive gastropathy, ascites, and HE [1]
If the patient rebleeds on combination therapy, refer for TIPS or consider liver transplant assessment. [1]
Ascites — SAAG, large-volume paracentesis, refractory ascites
Ascites is the commonest first decompensation event in cirrhosis. Its pathophysiology is sinusoidal portal hypertension (forcing fluid into the peritoneal space) plus splanchnic vasodilatation (causing effective arterial underfilling, RAAS activation, sodium and water retention). [1]
Serum-ascites albumin gradient (SAAG)
The SAAG distinguishes portal hypertension-related ascites from other causes: [1]
SAAG = serum albumin minus ascitic fluid albumin [1]
| SAAG | Cause |
|---|---|
| Greater than or equal to 11 g/L (portal hypertension) | Cirrhosis, heart failure, Budd-Chiari, massive hepatic metastases |
| Below 11 g/L (peritoneal disease) | Peritoneal carcinomatosis, tuberculous peritonitis, nephrotic syndrome, pancreatic ascites |
Exam tip: A high SAAG does not confirm cirrhosis — cardiac ascites and Budd-Chiari also give high SAAG. Check the fluid: protein above 25 g/L suggests cardiac/Budd-Chiari; low protein (below 25 g/L) suggests cirrhosis. [1]
Management of uncomplicated ascites
- Sodium restriction (88 mmol or approximately 2 g sodium per day) — the foundation
- Diuretics: spironolactone 100 mg OD plus frusemide 40 mg OD (ratio 100:40 maintains normokalaemia). Titrate upward (max spironolactone 400 mg, frusemide 160 mg). Target weight loss: 0.5 kg/day (no peripheral oedema) or 1 kg/day (with oedema).
- Stop NSAIDs, ACE inhibitors, ARBs — they worsen renal perfusion. [1]
Large-volume paracentesis (LVP)
For tense ascites or diuretic-resistant ascites:
- LVP removing 5 to 10 litres provides immediate symptomatic relief.
- Albumin replacement: give 8 g of albumin per litre of ascites removed if more than 5 litres removed (6 to 8 g/L if less). This prevents post-paracentesis circulatory dysfunction (PPCD), which causes renal impairment and increased mortality. [1]
Refractory ascites
Diuretic-refractory: ascites cannot be mobilised or recurs rapidly despite max diuretics and sodium restriction. Diarytic-intractable: diuretic complications (encephalopathy, renal impairment, hyponatraemia below 125) prevent effective diuretic use. [1]
Management of refractory ascites:
- Serial LVP with albumin — the practical mainstay
- TIPS — reduces portal pressure and improves sodium excretion; best in patients with MELD below 18 and without severe HE or cardiac failure. Improves quality of life; effect on survival is debated.
- Alfapump (automated low-flow ascites pump) — reinfuses ascites into the bladder; considered in selected patients unsuitable for TIPS
- Liver transplant assessment — the definitive treatment for refractory ascites [1]
Spontaneous bacterial peritonitis (SBP)
SBP is infection of ascitic fluid without an obvious intra-abdominal surgical source. It arises from bacterial translocation — gut bacteria cross the oedematous, permeable intestinal wall into mesenteric lymph nodes and then the peritoneal fluid. Impaired reticuloendothelial function in cirrhosis permits this. [1]
Diagnosis
Diagnostic paracentesis is mandatory for:
- Any patient with cirrhosis and ascites who is admitted to hospital
- New-onset or worsening ascites
- Clinical features suggesting infection (fever, abdominal pain, altered mental state, renal impairment, leucocytosis) — but SBP may be asymptomatic [1]
Diagnostic criterion: ascitic fluid polymorphonuclear leucocyte (PMN) count at or above 250 cells/microL. [1]
Send fluid for:
- Cell count (PMN)
- Culture (in blood culture bottles — inoculate at bedside to improve yield)
- Albumin (for SAAG calculation)
- Optional: total protein, glucose, lactate dehydrogenase, cytology, ADA (if TB suspected) [1]
Treatment
- Third-generation cephalosporin: cefotaxime 2 g IV every 12 hours, or ceftriaxone 2 g IV daily, for 5 to 7 days. Cover typical organisms (Gram-negative enterics — E. coli, Klebsiella — and Gram-positive streptococci).
- Albumin: 1.5 g/kg on day 1, then 1 g/kg on day 3. The Sort trial (PMID 10432325) showed albumin reduces renal impairment (10 percent vs 33 percent) and mortality (10 percent vs 29 percent in-hospital). Give albumin particularly if creatinine above 88, BUN above 30, or total bilirubin above 68.
- Repeat tap at 48 hours: PMN should fall by at least 25 percent. If not, reconsider diagnosis (secondary peritonitis from perforation) and broaden antibiotics. [1]
Secondary prophylaxis
After one episode of SBP, the one-year recurrence rate is 70 percent without prophylaxis. Give:
- Norfloxacin 400 mg orally daily (preferred) or ciprofloxacin 500 mg orally daily, indefinitely
- Primary prophylaxis (before first SBP): consider in patients with ascitic fluid protein below 15 g/L with impaired renal function (creatinine above 106, BUN above 25) or low total bilirubin — discuss with hepatology [1]
Hepatorenal syndrome (HRS-AKI)
HRS is a form of functional renal failure in cirrhosis caused by extreme splanchnic vasodilatation. As the splanchnic bed pools blood, effective circulating volume falls, triggering intense renal vasoconstriction (via RAAS, sympathetic nervous system, endothelin). The kidneys are structurally normal — they fail because they are being told to conserve every drop. [1]
Diagnostic criteria — ICA 2015 consensus (PMID 25638527)
The old "type 1 / type 2 HRS" classification has been replaced by HRS-AKI, aligned with KDIGO: [1]
Diagnosis of HRS-AKI requires all of:
- Cirrhosis with ascites
- AKI per ICA criteria: serum creatinine increase of at least 26.5 micromol/L within 48 hours, or at least 50 percent rise from baseline within 7 days
- No response after 2 consecutive days of diuretic withdrawal and albumin (1 g/kg/day, max 100 g/day) [1]4. Absence of shock
- No current or recent nephrotoxic drugs (NSAIDs, aminoglycosides, contrast)
- No structural kidney disease — no proteinuria above 500 mg/day, no microhaematuria above 50 RBC/HPF, normal renal ultrasound [1]
Key change from older criteria: the fixed creatinine threshold (above 133 or above 221 micromol/L) has been removed. HRS is now a dynamic diagnosis based on creatinine change — any cirrhotic with ascites and rising creatinine needs an HRS workup. [1]
Management of HRS-AKI
- Identify and treat precipitants: SBP (50 percent of HRS is triggered by SBP), large-volume paracentesis without albumin, over-diuresis, GI bleeding, nephrotoxic drugs, alcoholic hepatitis.
- Albumin challenge: stop diuretics, give albumin 1 g/kg/day (max 100 g) for 2 consecutive days. If no response, proceed to vasoconstrictor therapy. [1]3. Terlipressin plus albumin (first-line): terlipressin 1 to 2 mg IV every 4 to 6 hours, with albumin 20 to 40 g/day. Continue for up to 14 days or until creatinine below 133, to a max of 2 weeks. The CONFIRM trial (PMID 33657294) confirmed terlipressin achieves verified HRS reversal in 32 percent vs 17 percent with placebo.
- Noradrenaline is an alternative in ICU settings where terlipressin is unavailable.
- Monitor closely: terlipressin causes ischaemia (digital, mesenteric, cardiac) and respiratory failure — the major CONFIRM safety signal. Contraindicate in volume overload, hypoxia, or ischaemic heart disease.
- Relapsed HRS: after initial response, up to 50 percent relapse. Retreat with terlipressin.
- Liver transplant is the definitive treatment. HRS reverses after transplant if caught before structural renal damage. [1]
Prognosis
HRS-AKI without treatment has a median survival of approximately 2 weeks. With terlipressin response, survival extends toward transplant candidacy. The key is early recognition — any cirrhotic with ascites and rising creatinine needs immediate HRS workup, not a nephrology referral for "AKI of unknown cause." [1]
Hepatic encephalopathy (HE)
Hepatic encephalopathy is a reversible syndrome of impaired brain function in cirrhosis, caused by the accumulation of neurotoxins (principally ammonia) that the failing liver cannot clear and that portosystemic shunts bypass. [1]
West Haven grading
| Grade | Features |
|---|---|
| 0 (minimal HE) | No clinical signs; detectable only on psychometric testing |
| 1 | Mild lack of awareness, euphoria/anxiety, shortened attention, impaired addition/subtraction, sleep disturbance |
| 2 | Lethargy, apathy, disorientation, inappropriate behaviour, obvious personality change, dyspraxia (asterixis) |
| 3 | Somnolent but rousable, unable to perform mental tasks, disorientation about time and place, marked confusion, amnesia, occasional rage, speech incomprehensible |
| 4 | Coma with or without response to painful stimuli |
Asterixis (flapping tremor) is the hallmark physical sign of grade 2 to 3 HE: ask the patient to hold their hands dorsiflexed with arms extended for 30 seconds; a rapid flexion-extension flap indicates asterixis. It is not specific — also seen in uraemia, hypercapnia, and cardiac failure. [1]
Precipitants — always find and treat
HE rarely occurs spontaneously in compensated cirrhosis. The common precipitants: infection (SBP, pneumonia, UTI — commonest), GI bleeding (protein load drives ammonia), constipation, electrolyte disturbance (hypokalaemia, hyponatraemia from over-diuresis), CNS depressants (opioids, benzodiazepines, alcohol), HCC, portal vein thrombosis, and TIPS (new HE in 20 to 40 percent post-TIPS). [1]
Management
Acute HE (grade 2 to 4):
- Identify and treat the precipitant — this is the single most important intervention. Most HE reverses when the precipitant is treated.
- Lactulose (non-absorbable disaccharide): 15 to 30 mL orally TID, titrated to produce 2 to 3 soft bowel motions per day. Lactulose works by acidifying the colon (pH below 5), converting absorbable ammonia (NH3) to non-absorbable ammonium (NH4+), and acting as a laxative to expel it. In coma, give 300 mL lactulose as a retention enema.
- Rifaximin 550 mg orally BID — add for patients who fail lactulose alone or for secondary prophylaxis. Bass (PMID 20335583) showed rifaximin reduces breakthrough HE over 6 months (22 percent vs 46 percent with placebo) and HE-related hospitalisation. More than 90 percent of patients in the trial were already on lactulose — it is an add-on therapy. [1]
Secondary prophylaxis: Continue lactulose indefinitely; add rifaximin 550 mg BID after a second episode or if first was severe. [1]
Refractory HE: Consider TIPS occlusion/reduction (if HE developed post-TIPS), embolisation of large portosystemic shunts, zinc supplementation (zinc sulphate 600 mg/day — zinc deficiency impairs the urea cycle), or LOLA. Avoid benzodiazepines for agitation — flumazenil is not routine. [1]
Portopulmonary hypertension (PoPH) and hepatopulmonary syndrome (HPS)
These are distinct pulmonary vascular complications of portal hypertension — both are indications for liver transplant consideration. [1]
Portopulmonary hypertension (PoPH)
Pulmonary arterial vasculopathy in the setting of portal hypertension. Diagnostic criteria:
- Portal hypertension present
- Mean pulmonary artery pressure (mPAP) above 50 mmHg (strictly, above 20 mmHg at rest by right heart catheterisation)
- Pulmonary vascular resistance (PVR) above 240 dyn.s/cm5 (or 3 Wood units)
- Pulmonary capillary wedge pressure below 15 mmHg (excluding left heart failure) [1]
The high PVR distinguishes PoPH from the volume-overload pulmonary hypertension of cirrhosis (which has normal PVR). [1]
Management: pulmonary arterial vasodilator therapy (prostacyclin analogues, endothelin receptor antagonists, phosphodiesterase-5 inhibitors). mPAP above 45 to 50 mmHg is a contraindication to liver transplant (unacceptable perioperative mortality). Treatment to reduce mPAP can make transplant possible. [1]
Hepatopulmonary syndrome (HPS)
The triad:
- Liver disease (chronic or acute)
- Increased alveolar-arterial oxygen gradient (A-a gradient above 20 mmHg, or above 15 if over 64 years) on room air
- Intrapulmonary vasodilatation demonstrated by contrast echocardiography (bubble study showing delayed appearance of bubbles in the left heart after 3 to 6 cardiac cycles, indicating intrapulmonary shunt) or technetium-99m MAA brain uptake scan [1]
Characteristic clinical features: platypnoea (dyspnoea worse when upright, relieved by lying flat) and orthodeoxia (desaturation when upright, improved lying flat) — because basal pulmonary vasodilatation worsens V/Q mismatch in the upright position. Cyanosis and clubbing may be present. [1]
Management: supplemental oxygen (the only supportive therapy). Liver transplant is the only definitive treatment — HRS reverses in most patients post-transplant. Severity (PaO2 below 50 to 60 mmHg) confers additional transplant priority in many allocation systems. [1]
The TIPS decision — indications, contraindications, complications
Transjugular intrahepatic portosystemic shunt (TIPS) creates a channel between the portal vein and hepatic vein via a stent placed under fluoroscopic guidance, decompressing the portal system. Covered stents (polytetrafluoroethylene) are preferred for patency. [1]
Indications
| Setting | Indication |
|---|---|
| Acute variceal bleeding | Rescue for uncontrolled bleeding; pre-emptive (early) TIPS for Child-Pugh C 10 to 13 or Child-Pugh B with active bleeding |
| Secondary prophylaxis | Recurrent bleeding despite NSBB plus EVL |
| Refractory ascites | Diuretic-refractory ascites (MELD below 18 preferred) |
| Hepatic hydrothorax | Refractory hepatic hydrothorax |
| Budd-Chiari syndrome | As a bridge or definitive therapy |
| Hepatorenal syndrome | Selected cases (less established) |
Contraindications
Absolute: severe heart failure (TIPS increases venous return — can precipitate pulmonary oedema), severe tricuspid regurgitation, severe pulmonary hypertension (mPAP above 45), uncontrolled systemic infection, unrelieved biliary obstruction, massive polycystic liver disease. [1]
Relative: recurrent HE, portal vein thrombosis (though TIPS can sometimes recanalise), hepatocellular carcinoma (especially central), severe coagulopathy (INR above 5) or thrombocytopenia (below 20), MELD above 18 to 20 (high post-TIPS liver failure and mortality risk). [1]
Complications
- Hepatic encephalopathy (new or worsened): occurs in 20 to 40 percent; usually mild and manageable, but severe refractory HE may require TIPS occlusion or reduction. Risk is higher in older patients, prior HE, and large shunt diameter.
- Heart failure: TIPS increases venous return and cardiac output; can precipitate failure in pre-existing cardiac dysfunction.
- Liver decompensation: shunting diverts blood away from hepatocytes; precipitates failure in advanced disease (hence MELD caution).
- Shunt stenosis or thrombosis: less common with covered stents; surveillance Doppler every 6 to 12 months.
- Haemolysis (fragmentation haemolysis from stent trauma — a rare cause of anaemia post-TIPS). [1]
Integrated management — the decompensated patient
A patient with portal hypertension rarely has one problem in isolation. The four decompensation events are variceal bleeding, ascites, hepatic encephalopathy, and jaundice — each carries worsening prognosis and they frequently coexist. The integrated plan addresses: [1]
- Etiological treatment — the single most important intervention. HCV eradication, HBV suppression, alcohol cessation, weight loss for MASLD. Baveno VII's recompensation concept: removing the cause can partially reverse portal hypertension.
- NSBB for CSPH — prevents bleeding, ascites, and decompensation. Reduce or cease only if systolic BP below 90, HRS-AKI, or refractory ascites with hypotension (the window hypothesis).
- Variceal surveillance — serial endoscopy and EVL per Baveno VII non-invasive rules.
- SBP prophylaxis — if low ascitic protein, prior SBP, or active GI bleeding.
- HE prophylaxis — lactulose; add rifaximin after episodes.
- HRS surveillance — monitor creatinine; any rise triggers HRS workup.
- General: vaccinations (HAV/HBV, influenza, pneumococcal), HCC surveillance (ultrasound plus AFP every 6 months), nutrition (high protein 1.2 to 1.5 g/kg/day — sarcopenia worsens outcomes).
- Liver transplant assessment — trigger when decompensation occurs. MELD-Na (bilirubin, INR, creatinine, sodium) predicts 90-day mortality and guides prioritisation. Rising MELD-Na above 15 to 18 prompts referral. Assess abstinence (typically 6 months for alcohol-related cirrhosis) and screen comorbidities. [1]
High-yield exam traps
- HVPG thresholds: 5 (portal HTN), 10 (CSPH), 12 (bleeding), 20 (treatment failure). These four numbers are the most tested fact in portal hypertension MCQs.
- Antibiotics in variceal bleeding reduce mortality, not just infection. Ceftriaxone, not norfloxacin, in high-risk patients.
- Early TIPS is for high-risk bleeders (Child-Pugh C 10 to 13, or Child-Pugh B with active bleeding) — given within 72 hours, not as rescue. This is underutilised in practice and over-tested in exams.
- SAAG at or above 11 = portal hypertension. But cardiac ascites also has high SAAG — check fluid total protein to distinguish.
- SBP diagnosis: PMN at or above 250 cells/microL. Do not wait for culture — treat immediately if PMN threshold met. Send culture in blood culture bottles.
- HRS-AKI is now a dynamic diagnosis (creatinine change), not a fixed threshold. The old "type 1/type 2" nomenclature is obsolete per ICA 2015.
- Terlipressin and respiratory failure: the CONFIRM trial safety signal — contraindicate in volume overload or hypoxia.
- Carvedilol over propranolol for CSPH prevention (greater HVPG reduction, PREDESCI), but avoid in hypotension or refractory ascites.
- The window hypothesis: NSBB are good in compensated and early decompensated cirrhosis, but may be harmful in refractory ascites or HRS with hypotension — dose-reduce or stop if systolic BP below 90.
- Hepatopulmonary syndrome presents with platypnoea/orthodeoxia; the only cure is liver transplant. PoPH (mPAP above 50) is a transplant contraindication until treated with PAH therapy. [1]
References
- [1]de Franchis R, Bosch J, Garcia-Tsao G, et al. Baveno VII - Renewing consensus in portal hypertension J Hepatol, 2022.PMID 35120736
- [2]Villanueva C, Albillos A, Genesca J, et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): a randomised, double-blind, placebo-controlled, multicentre trial Lancet, 2019.PMID 30910320
- [3]Garcia-Pagan JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding N Engl J Med, 2010.PMID 20573925
- [4]Moreau R, Jalan R, Gines P, et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome N Engl J Med, 2021.PMID 33657294
- [5]Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy N Engl J Med, 2010.PMID 20335583
- [6]Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis N Engl J Med, 1999.PMID 10432325
- [7]Fernandez J, Ruiz del Arbol L, Gomez C, et al. Norfloxacin vs ceftriaxone in the prophylaxis of infections in patients with advanced cirrhosis and hemorrhage Gastroenterology, 2006.PMID 17030175
- [8]Sarin SK, Wadhawan M, Agarwal SR, et al. Endoscopic variceal ligation plus propranolol versus endoscopic variceal ligation alone in primary prophylaxis of variceal bleeding Am J Gastroenterol, 2005.PMID 15784021
- [9]Angeli P, Gines P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites J Hepatol, 2015.PMID 25638527
- [10]Kaplan DE, Ripoll C, Thacker L, et al. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis Hepatology, 2024.PMID 37870298
- [11]Bosch J, Abraldes JG, Berzigotti A, Garcia-Pagan JC The clinical use of HVPG measurements in chronic liver disease Nat Rev Gastroenterol Hepatol, 2009.PMID 19724251