Phys · hepatic
Viral Hepatitis (HAV, HBV, HCV, HDV, HEV)
Also known as hepatitis A · hepatitis B · hepatitis C · hepatitis D · hepatitis E · HBV · HCV · HDV · chronic viral hepatitis · hepatocellular carcinoma · HCC surveillance
Consultant-physician-depth guide to the five hepatotropic viruses — acute versus chronic hepatitis, HBV serology interpretation, the four phases of chronic HBV, HCV DAA therapy, HDV and HEV, acute liver failure, and hepatocellular carcinoma surveillance. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Viral Hepatitis (HAV, HBV, HCV, HDV, HEV)
The answer first
Viral hepatitis is liver inflammation caused by five distinct hepatotropic viruses — A, B, C, D and E — that share a name and a target organ but differ in everything that matters clinically. The single concept that organises the whole topic is this: some viruses cause only acute hepatitis, others cause chronic infection; the chronic ones (B and C) are what kill your patient through cirrhosis and hepatocellular carcinoma. [1]
Know the table below cold. It is the highest-yield page in viral hepatitis and answers most MCQ stems at a glance. [1]
| Virus | Genome | Route | Chronic? | Prevention | Key drug |
|---|---|---|---|---|---|
| HAV | RNA | Faecal-oral | No | Vaccine | Supportive |
| HBV | DNA | Blood, sexual, perinatal | Yes (5 to 10 percent adults; 90 percent perinatal) | Vaccine + HBIG | Tenofovir, entecavir |
| HCV | RNA | Blood (IVDU) | Yes (75 to 85 percent) | No vaccine | DAAs (SOF/VEL, GLE/PIB) |
| HDV | RNA (defective) | Blood; needs HBV | Yes (with HBV) | HBV vaccine prevents it | Bulevirtide, pegIFN |
| HEV | RNA | Faecal-oral (zoonotic) | Only if immunosuppressed | Vaccine (China) | Ribavirin (chronic) |
DWE high-yield: HAV and HEV are enteric and do not cause chronic hepatitis (except HEV in the immunosuppressed). HBV, HCV and HDV are bloodborne and do. If an MCQ describes an immunosuppressed transplant patient with chronic hepatitis from an enteric virus, the answer is chronic HEV — it is the one enteric virus that persists. [1]
Hepatitis A — enteric, acute, vaccine-preventable
Hepatitis A is an RNA picornavirus transmitted by the faecal-oral route. It causes acute hepatitis only — there is no chronic carrier state and no hepatocellular carcinoma risk. The disease is preventable by a highly effective vaccine. [1]
Clinical course
The incubation period is 2 to 6 weeks. The illness has three phases: [1]
- Prodrome — flu-like illness, anorexia, nausea, fatigue, arthralgia. This is the infective phase — the patient sheds virus in stool before jaundice appears.
- Icteric phase — dark urine, pale stools, jaundice, right upper quadrant discomfort. The transaminases peak (often above 1000 U/L).
- Recovery — symptoms resolve over weeks; full clinical recovery in nearly all patients. [1]
Serology: anti-HAV IgM confirms acute infection; anti-HAV IgG indicates past infection or vaccination and is lifelong. [1]
Fulminant hepatitis A
Fulminant hepatic failure from HAV is rare (below 1 percent overall) but the risk rises steeply with age — a patient over 50 or with pre-existing chronic liver disease has appreciable mortality. Acute HAV superimposed on chronic liver disease (especially cirrhosis) is dangerous; this is one reason hepatitis A vaccination is recommended in all patients with chronic liver disease. [1]
Prevention
- Hepatitis A vaccine — inactivated, two doses 6 months apart, greater than 95 percent seroprotection. Universal childhood vaccination is routine in many countries; travel, men who have sex with men, injecting drug use, chronic liver disease and clotting disorders are adult indications.
- Post-exposure prophylaxis — for close contacts of a confirmed case within 2 weeks of exposure: a single dose of hepatitis A vaccine (preferred for healthy people aged 1 to 40) plus normal human immunoglobulin for those over 40, immunocompromised, or with chronic liver disease. [1]
DCE trap: A patient with known cirrhosis who has never been vaccinated against HAV or HBV is a classic long-case finding. Both vaccines are safe in cirrhosis and should be given — superinfection with HAV in a cirrhotic patient is a preventable cause of decompensation and death. [1]
Hepatitis B — the high-yield virus
HBV is a DNA hepadnavirus and the single most testable virus in hepatology. Three things make it unique: it has a complex serological panel that examiners love; it runs in immunological phases that dictate treatment; and it is the leading cause of hepatocellular carcinoma worldwide, even without cirrhosis. [1]
Transmission
HBV is transmitted by three routes, and the route predicts the chronicity risk: [1]
- Perinatal — the dominant route in high-endemicity regions (East Asia, sub-Saharan Africa). Up to 90 percent of infants infected at birth become chronic carriers, which is why universal birth-dose vaccination is the cornerstone of global elimination.
- Percutaneous / blood-borne — injecting drug use, unscreened transfusion (rare now), unsafe medical injections, occupational needlestick. Adult-acquired infection has a chronicity rate of only 5 to 10 percent because the mature immune system clears the virus in most cases.
- Sexual — heterosexual and homosexual transmission; HBV is far more infectious than HIV per needlestick exposure. [1]
Serology — the panel you must master
The HBV serology panel is the most frequently examined investigation in hepatology. Learn it by understanding what each marker means, not by rote. [1]
| Marker | What it is | Clinical meaning |
|---|---|---|
| HBsAg | Surface antigen | Present means infection (acute or chronic). The first marker to appear; persists beyond 6 months means chronic. |
| Anti-HBs | Antibody to surface antigen | Protective immunity — from vaccination or resolved infection. |
| Anti-HBc IgM | IgM antibody to core antigen | Acute infection (or reactivation). The core antigen itself is not measured in serum. |
| Anti-HBc IgG (total) | IgG antibody to core | Past or ongoing infection — present for life after any exposure. Never appears after vaccination. |
| HBeAg | E-antigen (secreted core protein) | Marker of high infectivity and active replication (HBeAg-positive phase). |
| Anti-HBe | Antibody to e-antigen | Seroconversion — usually marks transition to lower-replication phase. |
| HBV DNA | Viral load | The direct measure of viral replication; guides treatment decisions. |
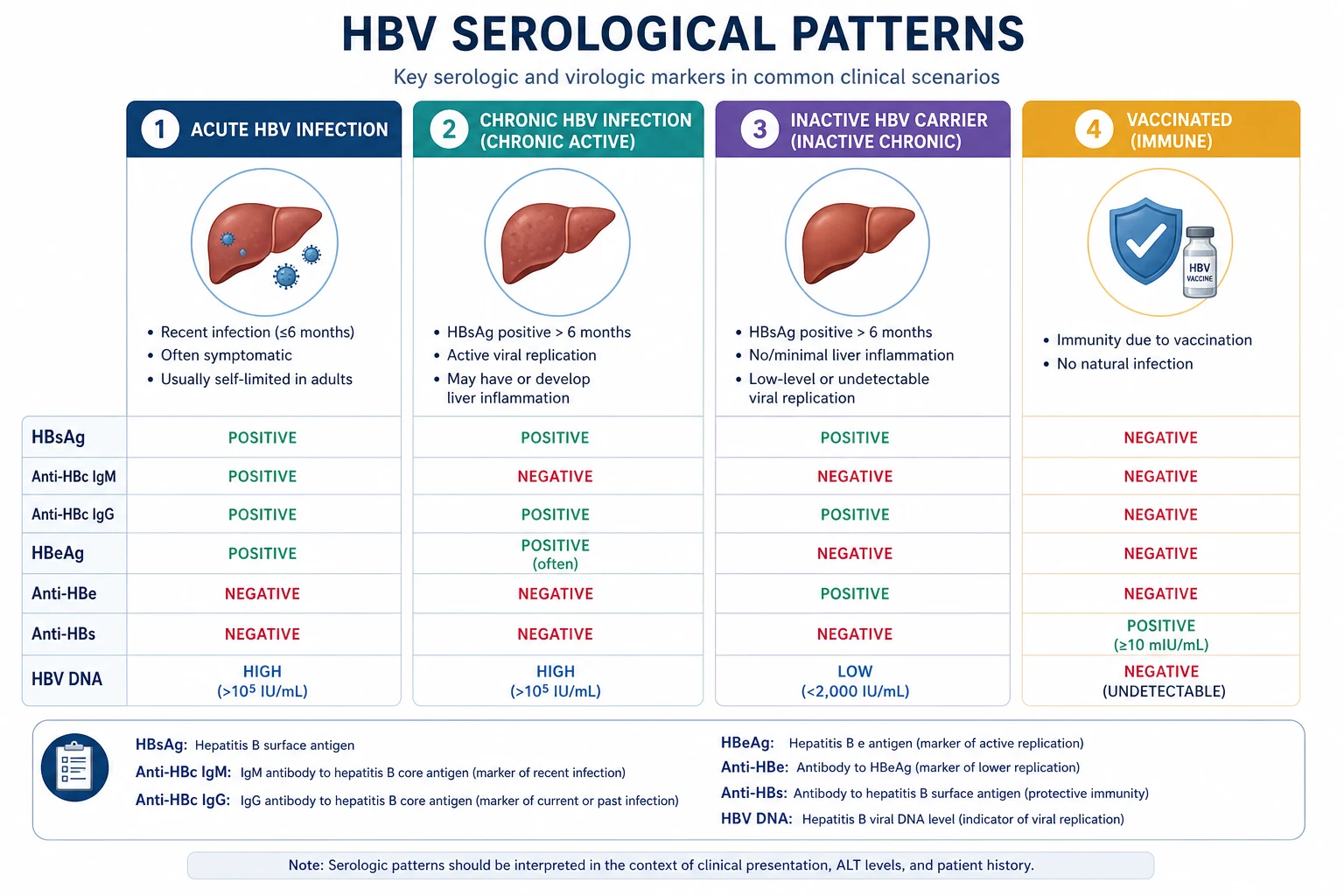
Five patterns to recognise instantly: [1]
| Pattern | HBsAg | Anti-HBs | Anti-HBc | HBeAg | Interpretation |
|---|---|---|---|---|---|
| Susceptible | Negative | Negative | Negative | — | Never exposed, never vaccinated |
| Immune (vaccine) | Negative | Positive | Negative | — | Vaccine-induced immunity |
| Immune (past infection) | Negative | Positive | Positive | Negative | Resolved natural infection |
| Acute infection | Positive | Negative | IgM positive | Positive or negative | Acute hepatitis B |
| Chronic infection | Positive | Negative | IgG positive | Variable | Chronic hepatitis B |
DWE high-yield trap: The single most tested distinction is anti-HBs alone (vaccinated) versus anti-HBs plus anti-HBc (past infection). Anti-HBc is the tell — it is never present after vaccination because the vaccine contains only surface antigen (recombinant HBsAg), so a vaccinated person never makes anti-core antibody. If anti-HBc is present, the patient had real infection. [1]
The window period and isolated anti-HBc
During acute infection there is a window period — HBsAg has been cleared but anti-HBs has not yet appeared. During this gap, anti-HBc IgM is the only positive marker. This is the "isolated anti-HBc" pattern. It can also represent: [1]
- Resolved infection where anti-HBs has waned below detection (most common).
- Occult HBV infection (HBV DNA detectable in liver, low-level replication).
- False positive (especially with rheumatoid factor or in low-prevalence populations). [1]
In practice, isolated anti-HBc with normal ALT needs no action unless the patient is immunosuppressed (reactivation risk) — then check HBV DNA. [1]
The four phases of chronic HBV
Chronic HBV is not a static disease. After perinatal or early acquisition it passes through immunological phases, and the phase — not the mere presence of HBsAg — determines whether you treat. This is the central management concept. [1]
-
Immune tolerant phase — HBeAg positive, very high HBV DNA (often above 1 million IU/mL), normal ALT, minimal necroinflammation on biopsy. Common in perinatally acquired infection; the immune system has not yet "recognised" the virus. Do not treat. Reassess ALT every 6 months. This phase may last decades. [1]
-
HBeAg-positive immune active phase (immune clearance) — the immune system begins attacking infected hepatocytes. ALT rises, HBV DNA is high (above 20,000 IU/mL), liver biopsy shows inflammation. This is when HBeAg seroconversion may occur (loss of HBeAg, gain of anti-HBe). Treat if this phase is sustained. [1]
-
Inactive carrier phase — HBeAg negative, anti-HBe positive, HBV DNA below 2000 IU/mL, normal ALT. The virus is suppressed but not gone. Low risk of progression; monitor with annual ALT and HBV DNA. Do not treat. [1]
-
HBeAg-negative immune active phase (reactivation) — HBeAg negative but HBV DNA is 2000 to 20,000 IU/mL with raised ALT. Caused by precore or basal core promoter mutants that stop producing HBeAg but keep replicating. This phase tends to be relapsing and progressive. Treat. [1]
DCE long-case trap: "Should you treat a patient with HBV DNA of 2 million IU/mL and a normal ALT?" The answer is no — this is the immune tolerant phase. Treating with nucleos(t)ide analogues achieves viral suppression but does not induce HBeAg seroconversion in this phase, and stopping risks flare. The exception is the patient over 30 to 40 with high DNA and evidence of fibrosis — then consider treatment or biopsy, because the "tolerant" label may be hiding smouldering disease. [1]
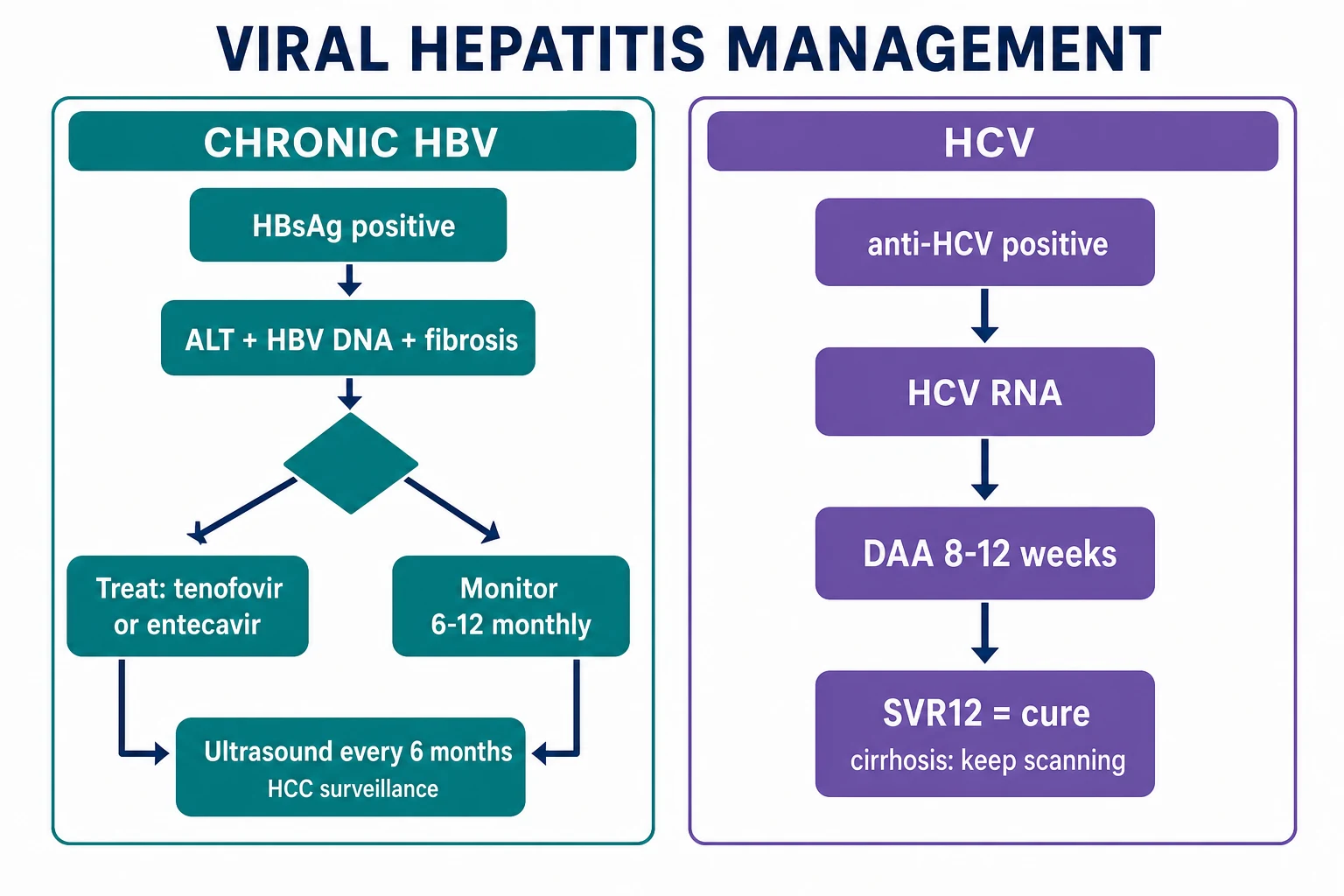
Who to treat (treatment indications)
Treat chronic HBV when there is active liver disease — the three indications per AASLD/EASL guidance [4]:
- HBeAg-positive immune active disease — HBV DNA above 20,000 IU/mL, ALT above twice the upper limit of normal (or histological activity), for more than 3 to 6 months.
- HBeAg-negative immune active disease — HBV DNA 2000 to 20,000 IU/mL with raised ALT and/or fibrosis.
- Cirrhosis and detectable HBV DNA — treat regardless of ALT or HBeAg status. The goal is to prevent decompensation and HCC. For decompensated cirrhosis, avoid entecavir (rare lactic acidosis); tenofovir is preferred, and refer for transplant. [1]
Also treat in specific situations: HBV reactivation risk (chemotherapy, rituximab, bone marrow transplant), pregnancy with high viral load (to prevent perinatal transmission), and coinfection with HCV or HIV by the relevant protocol. [1]
First-line antivirals
Two classes of treatment: nucleos(t)ide analogues (oral) and pegylated interferon (injectable). Oral agents are now first-line for the vast majority. [1]
Nucleos(t)ide analogues — the workhorses: [1]
| Drug | Dose | Resistance barrier | Notes |
|---|---|---|---|
| Entecavir | 0.5 mg daily (1 mg if lamivudine-resistant) | High (in treatment-naive; 1 percent at 5 years) | First-line; reduce dose in renal impairment |
| Tenofovir disoproxil fumarate (TDF) | 300 mg daily | Very high (zero resistance at 8 years in trials) | First-line; monitor renal function and bone density |
| Tenofovir alafenamide (TAF) | 25 mg daily | Very high | Renal and bone safety superior to TDF; preferred in renal impairment and osteoporosis |
The Marcellin trial established tenofovir as a potent first-line agent with high rates of HBV DNA suppression and histological improvement [2], and entecavir (Lai et al) demonstrated superior viral suppression with a high genetic barrier to resistance compared with lamivudine [3]. Lamivudine and adefovir are now not recommended as first-line because of high resistance rates.
DWE high-yield: The two first-line oral agents are entecavir and tenofovir (TDF or TAF). Both have a high barrier to resistance and are safe long-term. The exam wants you to know that lamivudine is obsolete because resistance develops in 70 percent by 5 years, and adefovir is inferior and nephrotoxic. [1]
Pegylated interferon alfa-2a: [1]
- Regimen — 180 micrograms subcutaneously once weekly for 48 weeks.
- Advantages — finite duration; no resistance; higher rate of HBeAg and HBsAg seroconversion than oral agents.
- Disadvantages — influenza-like symptoms, marrow suppression, depression, autoimmune activation; contraindicated in decompensated cirrhosis, pregnancy and autoimmune disease.
- Predictors of response — high ALT, low HBV DNA, genotype A or B, high HBsAg decline on therapy. [1]
The Lau trial showed pegIFN alfa-2a achieved HBeAg seroconversion in roughly 32 percent versus 19 percent with lamivudine at the end of follow-up [1]. It is now reserved for selected patients who want finite therapy and fit the response profile.
Pregnancy and perinatal transmission prevention
This is a guaranteed exam topic. Without intervention, up to 90 percent of infants born to HBeAg-positive, high-viraemic mothers become chronic carriers. Prevention is layered: [1]
- Universal birth-dose hepatitis B vaccine — given within 24 hours of birth to every infant. This is the single most important intervention and is the basis of global elimination strategy.
- Hepatitis B immune globulin (HBIG) — 100 to 200 IU intramuscularly within 12 hours of birth, for infants of HBsAg-positive mothers. Provides passive immunity during the window before the vaccine works.
- Maternal antiviral therapy — for mothers with HBV DNA above 200,000 IU/mL (some guidelines use 200,000 IU/mL or above), add tenofovir 300 mg daily from 28 to 32 weeks of gestation until delivery or up to 4 weeks postpartum. [1]
The Pan trial randomised HBeAg-positive mothers with high viral load to tenofovir versus placebo from 30 to 32 weeks and showed a significant reduction in mother-to-child transmission at postpartum week 28, with no difference in birth defects or safety outcomes [5]. Tenofovir is safe in pregnancy and breastfeeding; entecavir is not recommended.
DWE high-yield: The mother is HBeAg positive with HBV DNA of 8 million IU/mL at 30 weeks. What do you do? Start tenofovir 300 mg daily now, ensure the infant receives birth-dose vaccine plus HBIG within 12 hours, and support breastfeeding (it is safe on tenofovir once the infant is immunised). [1]
Hepatitis B reactivation
HBV reactivation is a potentially fatal complication of immunosuppression. The virus lurks in the liver even after apparent recovery (anti-HBc positive, HBsAg negative = occult HBV), and any profound immunosuppression can reactivate it. The classic triggers: [1]
- Rituximab (anti-CD20) — the highest-risk drug; reactivation can occur even in HBsAg-negative, anti-HBc-positive patients (occult HBV).
- Chemotherapy — especially for haematological malignancies.
- Corticosteroids — high-dose or prolonged.
- TNF inhibitors, integrated kinase inhibitors, budesonide in inflammatory bowel disease. [1]
Screen every patient starting chemotherapy, rituximab or other high-risk immunosuppression for HBsAg and anti-HBc. Management: [1]
- HBsAg positive — prophylactic antiviral (entecavir or tenofovir) for the duration of immunosuppression plus 6 to 12 months after.
- HBsAg negative but anti-HBc positive — monitor HBV DNA and ALT, or give prophylaxis depending on the immunosuppression intensity (prophylaxis for rituximab). [1]
DCE trap: A patient on rituximab for lymphoma with "isolated anti-HBc" develops a transaminitis flare and rising HBV DNA two months after the last dose. This is HBV reactivation from occult infection. The prevention is prophylactic entecavir or tenofovir started before rituximab and continued for at least 12 months afterward. Missing this is a fatal and avoidable error. [1]
Hepatitis C — the curable virus
Hepatitis C is an RNA flavivirus and the leading bloodborne chronic infection in most countries. The arrival of direct-acting antivirals (DAAs) transformed it from a chronic, slowly progressive disease into one that is curable in over 95 percent of patients with 8 to 12 weeks of oral therapy. The exam now tests DAA selection, not interferon regimens. [1]
Transmission
HCV is transmitted almost exclusively by the bloodborne route: [1]
- Injecting drug use — the dominant route in Australia, the UK and North America.
- Blood transfusion before screening (introduced 1990 to 1992 in most countries) — a cohort of older patients acquired HCV this way.
- Needlestick injury — occupational risk roughly 1.8 percent per needlestick from an HCV-positive source (much lower than HBV).
- Tattooing, body piercing, medical procedures in unregulated settings.
- Sexual — uncommon in heterosexuals but recognised in HIV-positive men who have sex with men.
- Perinatal — vertical transmission rate is 5 to 6 percent, higher with high viral load and HIV coinfection. [1]
Serology and diagnostic algorithm
The HCV diagnostic algorithm is two-step and is itself a favourite MCQ: [1]
- Anti-HCV antibody — the screening test. Positive means the patient has been exposed, but it cannot distinguish current (active) infection from resolved infection. It is also positive for life after cure.
- HCV RNA (viral load) — the confirmatory test. A detectable HCV RNA confirms active infection and is the indication for treatment. If anti-HCV is positive but HCV RNA is undetectable, the patient has resolved infection (spontaneous clearance or prior treatment cure). [1]
DWE high-yield: The most common serology error is treating a positive anti-HCV antibody as proof of active infection. It is not — roughly 15 to 30 percent of exposed patients clear the virus spontaneously. You must confirm with HCV RNA before treating. An MCQ will show a patient with positive anti-HCV and undetectable RNA; the answer is resolved infection, no treatment needed. [1]
A false-negative anti-HCV can occur in immunosuppressed patients (HIV, dialysis) — in these, test HCV RNA directly if suspicion is high. [1]
Genotypes and why they matter (less than they used to)
HCV has six major genotypes (1 to 6) with distinct global distributions: genotype 1 is most common in Europe, North America and Australia; genotype 3 is common in South Asia and is associated with steatosis and faster fibrosis; genotype 4 is common in the Middle East and Africa. [1]
Genotype historically dictated interferon-based therapy duration and response. With pangenotypic DAAs, genotype matters far less — sofosbuvir/velpatasvir and glecaprevir/pibrentasvir are effective across all genotypes. Genotyping is still useful for decompensated cirrhosis (where protease inhibitors are contraindicated) and for confirming the rare genotype 3 with cirrhosis that may need longer therapy or ribavirin. [1]
Direct-acting antivirals (DAAs) — the current standard
The two pangenotypic regimens that cover virtually every patient: [1]
Sofosbuvir / velpatasvir (400/100 mg once daily):
- Duration — 12 weeks for most patients; add ribavirin or extend to 24 weeks for decompensated cirrhosis or treatment-experienced genotype 3.
- Mechanism — sofosbuvir is an NS5B nucleotide polymerase inhibitor; velpatasvir is an NS5A inhibitor.
- Evidence — the ASTRAL-1 trial demonstrated SVR12 (sustained virologic response at 12 weeks after therapy) in 99 percent of treatment-naive patients with genotypes 1, 2, 4, 5 and 6, with a placebo-level side-effect profile [6].
- Safe in decompensated cirrhosis — the NS5A and NS5B targets are not protease inhibitors, so there is no hepatic metabolism concern. This is the regimen of choice for Child-Pugh B and C cirrhosis.
Glecaprevir / pibrentasvir (300/120 mg once daily, 3 tablets): [1]- Duration — 8 weeks for treatment-naive patients without cirrhosis; 12 weeks for those with compensated cirrhosis or treatment-experienced.
- Mechanism — glecaprevir is a protease (NS3/4A) inhibitor; pibrentasvir is an NS5A inhibitor.
- Evidence — the ENDURANCE-1 trial showed SVR rates above 99 percent with 8 weeks in genotype 1 without cirrhosis [7].
- Contraindicated in decompensated cirrhosis — all protease inhibitors carry a risk of liver failure in Child-Pugh B/C; use sofosbuvir/velpatasvir instead.
What SVR means and why it matters
A sustained virologic response (SVR) is undetectable HCV RNA 12 weeks after completing therapy (SVR12). SVR equals cure — the risk of relapse after SVR12 is below 1 percent. The clinical benefits: [1]
- Reduced all-cause and liver-related mortality.
- Reduced risk of cirrhosis, decompensation and HCC — but the risk does not fall to zero, especially in those who already have cirrhosis at the time of cure.
- Improved quality of life and extrahepatic manifestations — cryoglobulinaemic vasculitis and glomerulonephritis often resolve. [1]
DWE high-yield: A patient with HCV cirrhosis achieves SVR after DAA therapy. Does their HCC surveillance stop? No. Once cirrhosis is established, the HCC risk persists even after HCV cure. Surveillance continues with 6-monthly ultrasound and AFP. This is a classic and common exam trap. [1]
Who to treat — essentially everyone
Current AASLD/IDSA and EASL guidance: treat all patients with active HCV infection (detectable HCV RNA), regardless of fibrosis stage, including those with decompensated cirrhosis (using sofosbuvir/velpatasvir, not protease inhibitors), active injecting drug use, HIV coinfection and after liver transplant. The only exceptions are patients with a life expectancy too short to benefit. [1]
Cirrhosis surveillance and HCV elimination
After SVR, manage the patient by fibrosis stage: [1]
- No cirrhosis (F0 to F2) — discharge from hepatology; re-infection prevention counselling.
- Cirrhosis (F4) — continue 6-monthly HCC surveillance (ultrasound plus AFP), variceal screening, and reconsider the diagnosis (fibrosis can regress but cirrhosis remains a clinical risk). [1]
The WHO 2030 hepatitis elimination targets aim for 90 percent of infections diagnosed, 80 percent of eligible patients treated, and a 65 percent reduction in mortality. DAA scale-up makes this achievable for HCV — Australia was an early adopter of unrestricted DAA access from 2016 and is on track. The remaining barriers are case-finding (the undiagnosed cohort) and re-infection among people who inject drugs. [1]
Hepatitis D — the severe satellite
Hepatitis D (delta virus) is a defective RNA virus that requires HBsAg to assemble and release its virions — it cannot infect without HBV. HDV is the most severe form of chronic viral hepatitis, with faster fibrosis progression, higher cirrhosis rates and greater HCC risk than HBV alone. [1]
Coinfection versus superinfection (the key distinction)
This distinction determines outcome and is a guaranteed exam point: [1]
- Coinfection — HDV and HBV acquired simultaneously. Usually presents as severe acute hepatitis. The chronicity rate is the same as acute HBV alone (around 5 percent) because the immune system usually clears both viruses together.
- Superinfection — HDV acquired on top of established chronic HBV. This is the dangerous scenario. It suppresses HBV replication (HDV dominates) but produces severe acute hepatitis on a chronically infected liver, and chronicity approaches 90 percent. Superinfection carries a high risk of fulminant hepatic failure and rapid progression to cirrhosis. [1]
DWE high-yield: A patient with known chronic HBV (HBsAg positive for years) presents with an acute severe hepatitis flare — ALT 2000, jaundice, coagulopathy. The HBV DNA is unexpectedly low (suppressed). The diagnosis is HDV superinfection, not HBV reactivation or acute HAV. The low HBV DNA is the tell — HDV takes over replication machinery and suppresses HBV. Test anti-HDV and HDV RNA. [1]
Diagnosis
- Anti-HDV (total antibody) — the screening test; test every HBsAg-positive patient at least once (HDV prevalence is under-recognised).
- HDV RNA — confirms active replication; the measure of active HDV infection. [1]
Screening for HDV is underdone. International guidance now recommends testing all HBsAg-positive patients for anti-HDV at least once, because HDV prevalence is 5 to 10 percent even in non-endemic areas and it changes management entirely. [1]
Treatment
HDV is the hardest of the hepatotropic viruses to treat: [1]
- Pegylated interferon alfa — the only historically licensed therapy, 180 micrograms weekly for 48 weeks. Response rate is poor (roughly 25 to 30 percent achieve sustained virologic response off therapy) and side effects are substantial. It does not eradicate HDV in most.
- Bulevirtide — a novel entry inhibitor (blocks NTCP, the bile acid transporter HBV/HDV uses to enter hepatocytes). Given as 2 mg subcutaneously daily. The MYR301 phase 3 trial showed that 48 weeks of bulevirtide significantly reduced HDV RNA and normalised ALT compared with no treatment, with a favourable safety profile [8]. Bulevirtide has conditional approval in Europe (2020) and is a major advance, though it suppresses rather than cures HDV in most patients and may need long-term therapy.
DCE insight: For a long case with chronic HBV/HDV coinfection, the management is: confirm with HDV RNA, assess fibrosis (the patient probably has cirrhosis), treat with bulevirtide or pegIFN where available, ensure HBV nucleos(t)ide analogue coverage if HBV DNA is also detectable, and institute HCC surveillance. Acknowledge that HDV is the most aggressive chronic viral hepatitis and that transplant may be needed. [1]
Hepatitis E — enteric, usually acute, sometimes chronic
Hepatitis E is an RNA hepevirus transmitted by the faecal-oral route, typically through contaminated water or (in developed countries) undercooked pork and game — it is a zoonosis. Like HAV it causes acute self-limited hepatitis, with two key differences that examiners test: [1]
- HEV can become chronic in immunosuppressed patients — solid-organ transplant recipients, HIV with low CD4, haematological malignancy on therapy. Chronic HEV causes progressive fibrosis and can lead to cirrhosis. This is the one enteric virus that persists.
- HEV in pregnancy (genotype 1, common in South Asia and Africa) causes fulminant hepatic failure with mortality up to 20 to 25 percent — a distinctive and dangerous phenotype. [1]
Diagnosis
- Anti-HEV IgM — acute infection.
- HEV RNA — active infection; needed to confirm chronic infection in immunosuppressed patients (antibody responses are blunted). [1]
Management
- Acute HEV in immunocompetent — supportive; full recovery is the rule.
- Chronic HEV in immunosuppressed — first, reduce immunosuppression if possible (this alone clears infection in some transplant recipients). If it persists, ribavirin for 3 months. The Kamar case series in solid-organ transplant recipients showed ribavirin monotherapy (median 600 mg daily for 3 months) achieved HEV RNA clearance in 95 percent at end of therapy and sustained virologic response in 78 percent [9].
- HEV in pregnancy — supportive with monitoring; severe cases need hepatology and obstetric input.
DWE high-yield: An immunosuppressed kidney transplant recipient presents with persistently abnormal liver enzymes for 4 months. Anti-HAV IgM negative, HBsAg negative, anti-HCV negative. The answer is test for HEV RNA — chronic HEV is the under-recognised cause of chronic hepatitis in the immunosuppressed, and antibody testing alone may miss it. [1]
Acute liver failure from viral hepatitis
Acute liver failure (ALF) — coagulopathy and encephalopathy within 8 weeks of onset in a patient without pre-existing liver disease — is the most feared complication of acute viral hepatitis. The viral causes: HBV (most common viral cause worldwide), HAV (rare, mainly elderly), HEV (genotype 1 in pregnancy), and HDV superinfection. HCV rarely causes ALF. [1]
Recognition
The hallmarks are coagulopathy (INR above 1.5) and encephalopathy in the setting of acute hepatitis. Other features: jaundice, transaminases often above 1000 U/L (may fall as the liver fails — a falling ALT with rising INR is a deterioration sign, not improvement), hypoglycaemia, metabolic acidosis, renal failure and sepsis. [1]
Management principles
- Manage in an intensive care or specialist liver unit — ALF has high mortality and needs multi-organ support.
- Identify and treat the cause — viral serology (HBsAg, anti-HBc IgM, anti-HAV IgM, anti-HEV IgM, HEV RNA), paracetamol level, autoimmune and metabolic screen. Nucleos(t)ide analogue therapy (entecavir or tenofovir) for HBV-related ALF.
- King's College Criteria — the prognostic tool that triggers transplant referral. For non-paracetamol ALF (including viral), fulfil the criteria if INR is above 6.5 alone, or any three of: age under 10 or over 40, aetiology non-A non-B hepatitis or drug-induced, duration of jaundice before encephalopathy over 7 days, INR above 3.5, bilirubin above 300 micromol/L.
- Early transplant referral — ALF is a transplant indication. Refer early; do not wait to meet criteria, because workup and graft allocation take time the patient may not have. [1]
DCE trap: In a patient with suspected acute viral hepatitis, the two findings that change the trajectory from "admit for supportive care" to "urgent transplant referral" are encephalopathy and coagulopathy (INR above 1.5). A patient with jaundice and ALT 1500 but a normal INR and normal mentation has acute hepatitis, not acute liver failure. The INR is the dividing line. [1]
Hepatocellular carcinoma surveillance in chronic viral hepatitis
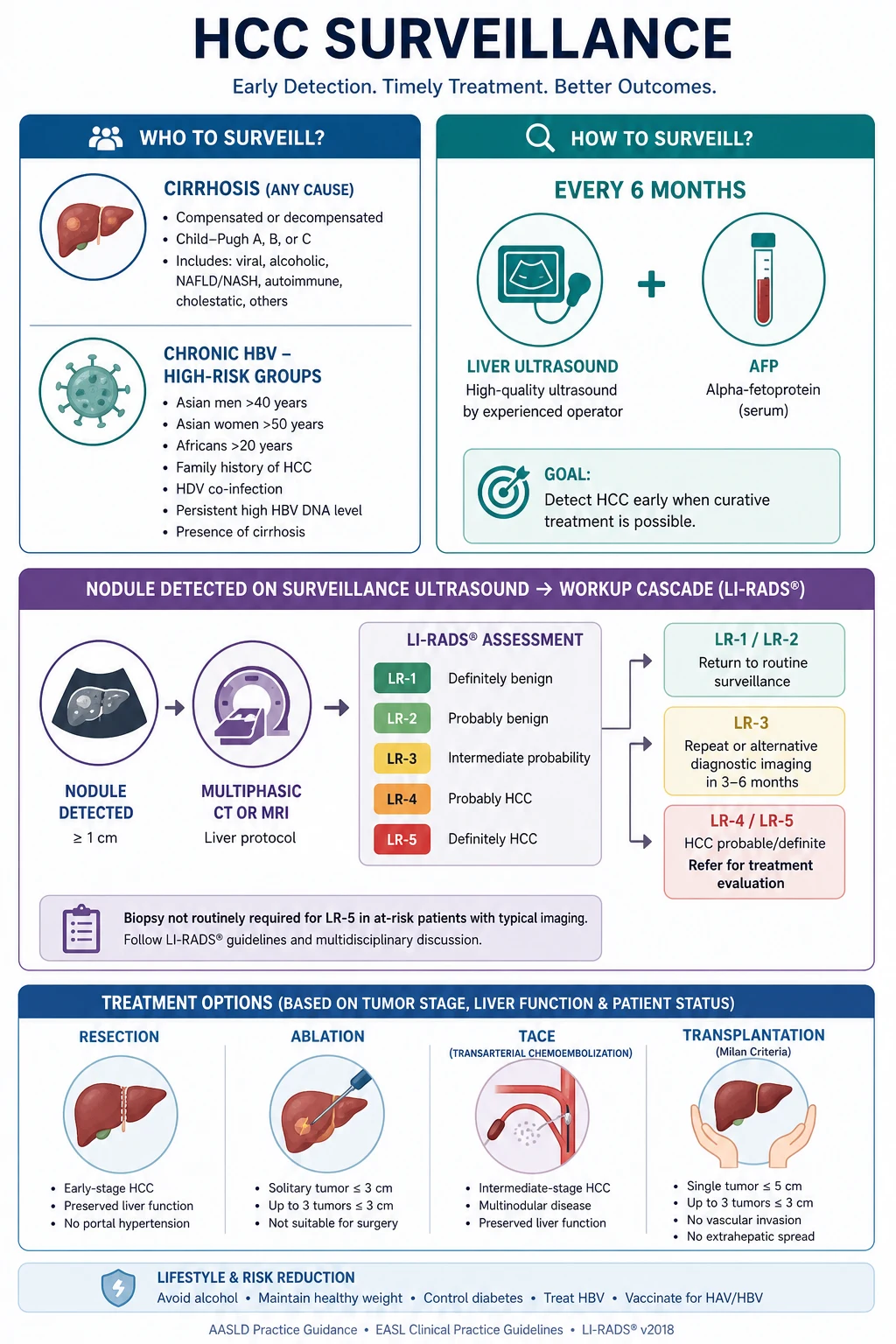
Chronic HBV and HCV are the leading causes of hepatocellular carcinoma (HCC) worldwide. HCC surveillance detects tumours at an earlier, treatable stage and improves survival. The AASLD guidance standardises the approach [10].
Who to surveil
- All patients with cirrhosis from any cause (including cured HCV with residual cirrhosis).
- Chronic HBV without cirrhosis in high-risk groups: Asian men over 40, Asian women over 50, Africans over 20, patients with a family history of HCC, and those with high HBV DNA or established fibrosis. HBV causes HCC even without cirrhosis (via integration), which is why HBV has broader surveillance criteria than HCV. [1]
The surveillance protocol
- 6-monthly liver ultrasound plus alpha-fetoprotein (AFP).
- The interval is 6 months because the doubling time of HCC is roughly 4 to 6 months — annual is too long, more frequent than 6-monthly adds little.
- AFP alone is not adequate — it misses up to 30 percent of HCCs. Ultrasound plus AFP is the surveillance standard; cross-sectional imaging (CT or MRI) is reserved for diagnostic confirmation, not surveillance. [1]
Diagnostic cascade
A nodule detected on surveillance triggers staged imaging: [1]
- Nodule below 1 cm — repeat ultrasound at 3 to 6 months (most are not HCC).
- Nodule at least 1 cm — multiphase CT or MRI. Apply LI-RADS criteria: arterial phase hyperenhancement plus washout in a cirrhotic liver is diagnostic of HCC without biopsy in nodules above 1 cm.
- Biopsy is reserved for lesions where imaging is non-diagnostic. [1]
DWE high-yield: Two classic MCQ traps here. First: "What is the surveillance modality?" — answer is 6-monthly ultrasound plus AFP, not annual CT and not AFP alone. Second: "Does a patient with HCV cirrhosis who achieved SVR still need HCC surveillance?" — yes, because established cirrhosis carries persistent HCC risk even after viral cure. [1]
Investigations — the complete viral hepatitis workup
When a patient presents with abnormal liver enzymes or suspected viral hepatitis, structure the workup: [1]
First-line viral screen (in every patient with unexplained hepatitis or chronic liver disease):
- HBsAg, anti-HBs, anti-HBc (total)
- Anti-HCV (and HCV RNA if positive)
- Anti-HAV IgG (immune status) and IgM if acute
- If HBsAg positive: HBeAg, anti-HBe, HBV DNA, and test for HDV (anti-HDV)
- HEV serology / RNA if immunosuppressed or relevant travel [1]
Fibrosis staging (non-invasive):
- FIB-4 score (age, AST, ALT, platelets) — a cheap first triage; below 1.45 excludes significant fibrosis in most.
- Transient elastography (FibroScan) — measures liver stiffness; above 12 to 15 kPa suggests cirrhosis.
- Liver biopsy — reserved for when non-invasive tests are discordant, the aetiology is unclear, or autoimmunity is suspected. [1]
Severity and complications (if cirrhosis confirmed): full blood count (thrombocytopenia suggests portal hypertension), coagulation, albumin, bilirubin — calculate Child-Pugh and MELD-Na; upper endoscopy for varices; HCC surveillance (ultrasound plus AFP) if criteria met. [1]
Differential diagnosis — when it is not viral
Always confirm the aetiology, because treatment is cause-specific. The differential of acute hepatitis: drug-induced liver injury (paracetamol, amoxicillin-clavulanate, isoniazid, statins, herbal supplements — eosinophilia and a temporal drug relationship support DILI), alcoholic hepatitis (AST to ALT ratio above 2, gamma-GT elevation), ischaemic hepatitis (transaminases over 1000 with rapid fall after hypotension), autoimmune hepatitis (high IgG, positive ANA and smooth muscle antibody) and Wilson disease (young patient, low caeruloplasmin, Kayser-Fleischer rings). The differential of chronic hepatitis: MASLD/MASH (metabolic syndrome, the rising epidemic), alcohol-related liver disease, haemochromatosis (high ferritin and transferrin saturation, HFE genetics), primary biliary cholangitis (AMA positive, cholestatic enzymes) and alpha-1-antitrypsin deficiency. [1]
DWE high-yield: "An asymptomatic patient has an ALT of 90 on routine bloods. HBV and HCV serology are negative." Do not stop — work through the chronic hepatitis differential (ferritin and transferrin saturation for haemochromatosis, AMA and immunoglobulins for PBC, ANA and IgG for autoimmune hepatitis, caeruloplasmin if young, lipid profile and glucose for MASLD, alcohol history). A common exam trap is stopping after a negative viral screen. [1]
Prognosis
Prognosis is now driven by treatment access. HCV is curable in over 95 percent with DAAs; cure restores near-normal life expectancy if cirrhosis is not established. HBV is suppressible lifelong; cirrhosis and HCC risk fall substantially with viral suppression but never to zero, especially in those infected from birth. HDV carries the worst prognosis — faster fibrosis, higher HCC and mortality — with bulevirtide offering new hope. HAV and HEV (immunocompetent) mean full recovery; fulminant failure is rare except in the elderly (HAV) and pregnancy (HEV genotype 1). [1]
DCE long-case approach
Opening statement (SASPOP)
"Mr Nguyen is a 54-year-old Vietnamese-born man referred with abnormal liver enzymes found on insurance bloods. He migrated to Australia at age 30 and works as a mechanic. [1]
He is known to have chronic hepatitis B, diagnosed at age 25, but has never received treatment. He drinks minimal alcohol. [1]
His main problems are:
- Chronic hepatitis B — HBeAg-negative immune active phase (HBV DNA 45,000 IU/mL, ALT 120)
- Compensated cirrhosis (liver stiffness 18 kPa, platelets 110, small oesophageal varices)
- Hepatocellular carcinoma risk — requires 6-monthly surveillance
- Metabolic syndrome — type 2 diabetes and obesity (overlapping MASLD) [1]
My integrated management plan is to start tenofovir to suppress HBV and reduce HCC risk, institute 6-monthly ultrasound and AFP surveillance, perform variceal screening and primary prophylaxis, address his metabolic risk, and counsel his family about testing and vaccination." [1]
Integrated management plan
- Antiviral therapy — tenofovir 300 mg daily (he has cirrhosis with detectable HBV DNA, an absolute indication); lifelong, with annual renal monitoring and HBV DNA to confirm suppression. [1]2. HCC surveillance — 6-monthly ultrasound plus AFP, indefinitely.
- Portal hypertension management — endoscopy to screen for varices; start carvedilol or EVL primary prophylaxis if high-risk varices are present.
- Vaccinate the family — test spouse and children for HBsAg and anti-HBs; vaccinate susceptible contacts; this is a public-health obligation.
- Address cofactors — weight loss and diabetes control to reduce MASLD overlap and HCC risk; alcohol abstinence counselling. [1]
DCE examiner probing questions you must anticipate:
- "Why tenofovir and not pegylated interferon?" → Cirrhosis and high DNA favour a potent oral agent; interferon is contraindicated in significant fibrosis and less practical.
- "Does he still need HCC surveillance if his viral load suppresses?" → Yes — cirrhosis is established; HCC risk persists despite viral suppression.
- "His wife is HBsAg negative and anti-HBs negative. What do you do?" → Vaccinate her; she is susceptible. Check post-vaccine anti-HBs to confirm seroprotection. [1]
DCE short-case approach: abdominal examination in chronic liver disease
The short-case instruction is typically "Examine this patient's abdominal system." In a chronic viral hepatitis patient, elicit the stigmata systematically and, critically, state which group each sign belongs to — chronic liver disease, portal hypertension, or hepatic failure. [1]
Systematic routine
- End of bed — cachexia, muscle wasting (sarcopenia), spider naevi on chest, loss of body hair, parotid enlargement (alcohol overlap), gynaecomastia.
- Hands — palmar erythema, Dupuytren contracture, leuconychia, clubbing, asterixis (hepatic failure).
- Face and chest — spider naevi (superior vena cava distribution), loss of axillary hair, gynaecomastia.
- Abdomen — distension (ascites), caput medusae, hepatomegaly or shrunken hard liver, splenomegaly (portal hypertension), testicular atrophy.
- Complete the examination — peripheral oedema, and mention a stethoscope check for a hepatic bruit. [1]
Presentation template
"I examined Mr Nguyen's abdominal system. He is thin, with several spider naevi over the anterior chest wall in the superior vena cava distribution, and loss of axillary hair. On the hands there is palmar erythema sparing the central palm. There is no asterixis. [1]
The abdomen is soft. The liver edge is firm and irregular, palpable 3 cm below the costal margin. The spleen is enlarged 4 cm below the left costal margin. There is no ascites. There is peripheral oedema to the mid-shin bilaterally. [1]
These findings are consistent with chronic liver disease complicated by portal hypertension. The spider naevi and palmar erythema indicate chronic liver disease; the splenomegaly indicates portal hypertension. I would like to take a full viral hepatitis and alcohol history, organise liver function tests, a viral hepatitis screen, a FibroScan, and screening endoscopy." [1]
Key DWE MCQ patterns
- HBV serology interpretation — the isolated anti-HBs (vaccinated) versus anti-HBs plus anti-HBc (past infection) versus HBsAg positive (chronic) distinction is the single most common pattern.
- Which phase of chronic HBV to treat — immune active (raised ALT plus high DNA), not immune tolerant (high DNA, normal ALT).
- HCV two-step diagnosis — anti-HCV screens, HCV RNA confirms active infection; never treat on antibody alone.
- First-line HBV drugs — entecavir and tenofovir; lamivudine is obsolete due to resistance.
- DAA choice in cirrhosis — sofosbuvir/velpatasvir (no protease inhibitor) for decompensated; glecaprevir/pibrentasvir only if compensated.
- Perinatal HBV prevention — birth-dose vaccine plus HBIG plus maternal tenofovir when viral load is high.
- HDV superinfection — severe acute flare with low HBV DNA in a known chronic HBV patient; test anti-HDV.
- HCC surveillance post-SVR — continues in cirrhosis; the cure does not erase the cancer risk.
- HBV reactivation with rituximab — prophylactic antiviral for HBsAg positive; monitor or prophylax if anti-HBc positive.
- Acute liver failure — INR above 1.5 plus encephalopathy defines it; King's College criteria guide transplant. [1]
References
[1] Lau (2005) — PegIFN alfa-2a achieved HBeAg seroconversion in roughly 32 percent versus 19 percent with lamivudine for HBeAg-positive chronic HBV. [2] Marcellin (2008) — Tenofovir superior to adefovir for HBV DNA suppression in both HBeAg-positive and HBeAg-negative chronic hepatitis B. [3] Lai (2006) — Entecavir versus lamivudine for HBeAg-negative chronic HBV; potent suppression with low resistance. [4] Terrault / AASLD (2018) — Hepatitis B guidance on prevention, diagnosis, treatment and the four phases of chronic infection. [5] Pan (2016) — Tenofovir from 30 to 32 weeks in HBeAg-positive high-viraemic mothers reduces perinatal HBV transmission. [6] Feld / ASTRAL-1 (2015) — Sofosbuvir/velpatasvir 12 weeks achieves SVR12 in 99 percent across HCV genotypes 1, 2, 4, 5 and 6. [7] Zeuzem / ENDURANCE-1 (2018) — Glecaprevir/pibrentasvir 8 weeks achieves SVR above 99 percent in genotype 1 without cirrhosis. [8] Wedemeyer / MYR301 (2023) — Bulevirtide 2 to 10 mg daily for 48 weeks reduces HDV RNA and normalises ALT in chronic hepatitis D. [9] Kamar (2014) — Ribavirin monotherapy for chronic HEV in transplant recipients; 95 percent clearance at end of therapy, 78 percent SVR. [10] Marrero / AASLD (2018) — HCC practice guidance: surveillance, LI-RADS diagnostic cascade, and staging-driven treatment.
AASLD 2018 Hepatitis B Guidance and HCC Practice Guidance; EASL 2017 Clinical Practice Guidelines on hepatitis B and hepatitis C; GESA viral hepatitis guidelines; WHO Global Hepatitis Programme and 2030 elimination targets. [1]
References
- [1]Lau GKK, Piratvisuth T, Luo KX, et al. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B N Engl J Med, 2005.PMID 15987917
- [2]Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B N Engl J Med, 2008.PMID 19052126
- [3]Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B N Engl J Med, 2006.PMID 16525138
- [4]Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance Hepatology, 2018.PMID 29405329
- [5]Pan CQ, Duan Z, Dai E, et al. Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load N Engl J Med, 2016.PMID 27305192
- [6]Feld JJ, Jacobson IM, Hezode C, et al. Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection N Engl J Med, 2015.PMID 26571066
- [7]Zeuzem S, Foster GR, Wang S, et al. Glecaprevir-Pibrentasvir for 8 or 12 Weeks in HCV Genotype 1 or 3 Infection N Engl J Med, 2018.PMID 29365309
- [8]Wedemeyer H, Aleman S, Brunetto MR, et al. A Phase 3, Randomized Trial of Bulevirtide in Chronic Hepatitis D N Engl J Med, 2023.PMID 37345876
- [9]Kamar N, Izopet J, Tripon S, et al. Ribavirin for chronic hepatitis E virus infection in transplant recipients N Engl J Med, 2014.PMID 24645943
- [10]Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases Hepatology, 2018.PMID 29624699