Phys · infectious
Bloodstream Infections and Infective Endocarditis
Also known as bacteraemia · bloodstream infection · BSI · infective endocarditis · IE · SAB · Staphylococcus aureus bacteraemia · CRBSI · line infection · line sepsis · culture-negative endocarditis · endovascular infection
Consultant-physician-depth guide to bacteraemia and infective endocarditis from the infectious-diseases side — blood culture technique, source control and catheter-related BSI, the modified Duke criteria applied, organism-by-context microbiology, empirical and definitive antimicrobial strategy with durations and the POET oral step-down, surgical triggers, and the S. aureus bacteraemia rule — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Bloodstream Infections and Infective Endocarditis
The answer first
A positive blood culture is not a result — it is a decision. Three rules carry most of the DWE marks and most of the ward safety [6]:
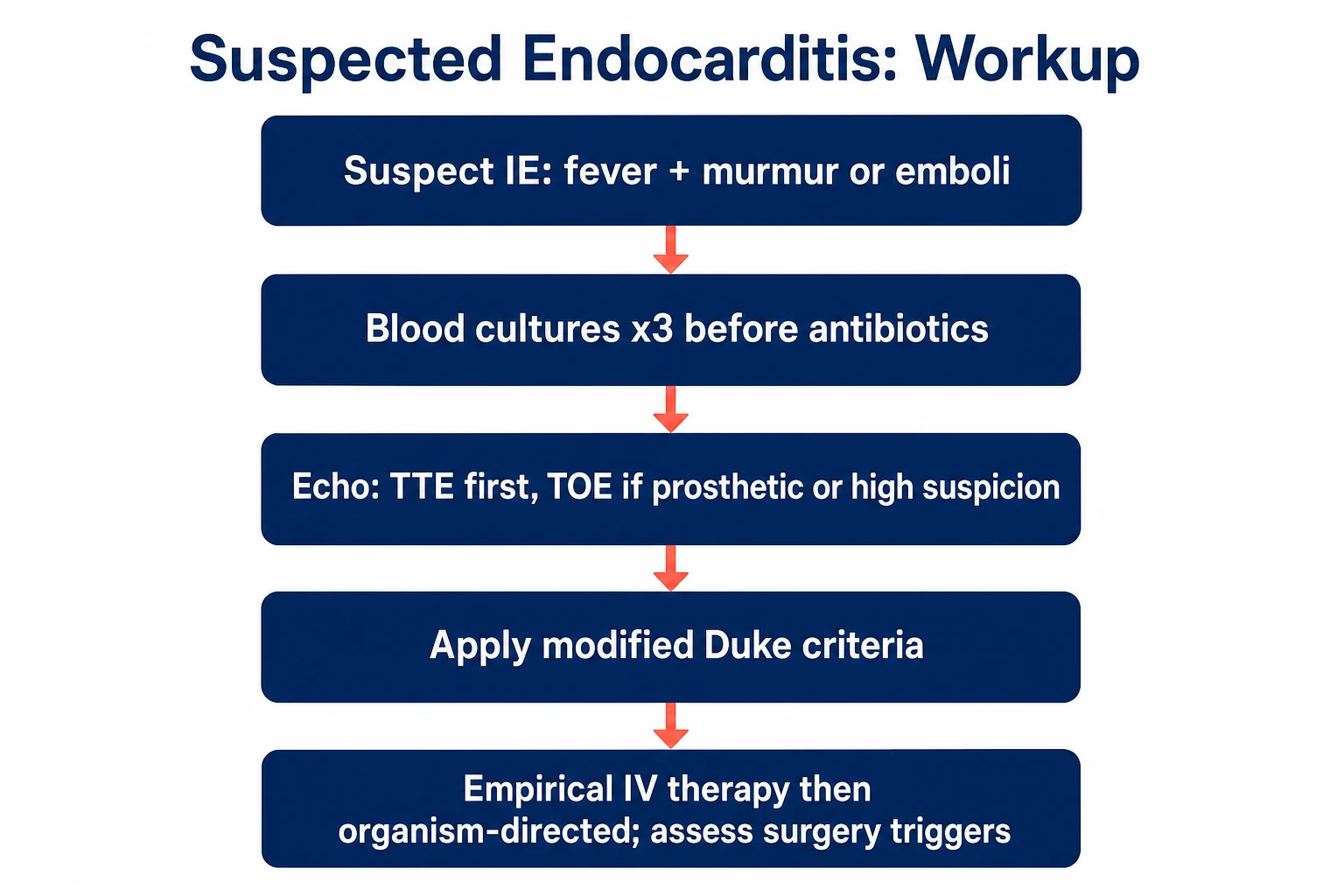
- Cultures before antibiotics, always. Three sets from separate venepuncture sites, with adequate volume, drawn before the first dose whenever the clinical situation allows even a few minutes. Every dose of antibiotic given before cultures erodes the diagnostic yield you will be arguing about for the next fortnight [4].
- S. aureus in the blood is never a contaminant and never minor. It demands repeat cultures to document clearance, an echocardiogram in most patients, an infectious diseases consult, and a hunt for metastatic foci — and it is never short-coursed until endocarditis and seeding have been excluded [6] [7].
- Endocarditis is diagnosed by criteria and treated for weeks, not days. Apply the modified Duke criteria explicitly, image early (TTE, then TOE when there is a prosthetic valve, a device or high suspicion), give organism-directed intravenous therapy for four to six weeks, and know the three surgical triggers — heart failure, uncontrolled infection, and prevention of embolism [1] [2].
A note on scope: this topic owns the infectious-diseases framing — bloodstream infection, cultures, source control, antimicrobial strategy and duration. The structural valve detail and surgical technique of endocarditis live in the cardiovascular infective endocarditis topic; the two are designed to be read together [2].
The bloodstream infection framework
A bloodstream infection (BSI) is viable microorganisms in the blood — transient (dental work, brushing teeth), intermittent (an abscess discharging), or continuous (endovascular infection, the highest-risk pattern). BSIs are among the commonest severe infections in hospital practice, their incidence rises with every device and line we insert, and S. aureus bacteraemia in particular still kills roughly one in five patients despite modern therapy [6] [18].
The classification that organises your workup [6]:
- Primary BSI — no identifiable source after history, examination and first-pass investigations. Intravascular by definition: the first suspects are intravascular devices, and the dangerous subset is endocarditis.
- Secondary BSI — spillover from an identified focus (lung, urine, biliary tree, skin, bone, joint). The source dictates both the likely organism and the need for source control: drain the abscess, remove the line, debride the tissue. Antibiotics without source control is the commonest reason bacteraemia persists [6].
- Community-acquired vs healthcare-associated vs hospital-acquired — a second axis that predicts organism ecology and resistance risk, and therefore your empirical choice [18].
And a definition examiners like: bacteraemia is a microbiological finding; sepsis is the dysregulated host response with organ dysfunction. Many bacteraemic patients are not yet septic, and a third of septic patients never have a positive culture — the two concepts overlap but are not interchangeable [6].
Catheter-related BSI (CRBSI). A BSI in a patient with a central line where the catheter is the source. The laboratory signature is the same organism growing from paired catheter-drawn and peripheral cultures, with the catheter set flagging positive at least two hours earlier (differential time to positivity) — which is why, when a line is suspect, you culture through the line and peripherally at the same time [11].
When the line must come out. The IDSA catheter guidelines are explicit enough to be exam-ready: remove the catheter rather than attempt salvage when the organism is S. aureus, Pseudomonas aeruginosa, fungi or mycobacteria, when there is tunnel infection or port abscess, when bacteraemia persists beyond 72 hours of appropriate therapy, or when there is septic thrombosis, endocarditis or metastatic seeding. Salvage with antibiotic lock therapy is defensible mainly for coagulase-negative staphylococci and selected gram-negative bacilli in a stable patient who genuinely needs the access [11].
Blood cultures: the test that decides everything
Get this right and the fortnight is easy; get it wrong and every later decision is built on sand [4]:
- How many sets: at least two, ideally three sets from separate venepuncture sites — not through an existing line unless you are deliberately culturing the line for a CRBSI comparison. A single set gives only a fraction of the yield and leaves contamination uninterpretable; three sets at adequate volume approach full detection and give you the pattern you need — all sets positive with a typical organism means continuous (endovascular) bacteraemia, while one of three sets growing skin flora is usually contamination [4] [5].
- Volume is the variable that matters most. Adult bacteraemia is low-grade — often only a few colony-forming units per millilitre — so each millilitre of blood raises yield more than any other factor. Fill each bottle to its specified volume (roughly 8–10 mL per bottle, 20–30 mL per set) rather than splitting one small draw thinly across sets [4].
- Before antibiotics. Every prior dose cuts yield. If the patient is in septic shock, take cultures and give antibiotics immediately afterwards; if they are stable, cultures come first, even if that means a short delay in the ED [4].
- The timing myth: do not wait for the fever spike. Intravascular infection produces continuous bacteraemia — the organisms are present between rigors, so waiting for the spike delays therapy and adds nothing to yield [4].
- Contamination discipline: alcoholic chlorhexidine skin preparation, no draws through used lines, and a unit contamination rate kept low — the classic contaminants are coagulase-negative staphylococci, Cutibacterium acnes, corynebacteria, Micrococcus and non-anthracis Bacillus. Contaminated cultures are not harmless: they trigger vancomycin, extra cultures, extra days and occasionally an unnecessary six-week endocarditis course [5].
The organism itself tells you the prior probability of truth. Almost always real: S. aureus, Escherichia coli and other enteric gram-negative bacilli, Streptococcus pneumoniae, beta-haemolytic streptococci, Pseudomonas aeruginosa, Candida species — and, in the right host, enterococci. Usually contamination when in a single set: coagulase-negative staphylococci, Cutibacterium, corynebacteria [5].
From bacteraemia to endocarditis
Endocarditis begins with a sterile thrombotic lesion on an injured or inflamed valve — non-bacterial thrombotic endocarditis — which circulating organisms then colonise during a bacteraemic window. That is why the organisms that cause endocarditis are precisely those that adhere to platelet–fibrin matrices (streptococci, staphylococci, enterococci), and why continuous bacteraemia from an intravascular source is the highest-risk state [3].
Clinically, endocarditis is fever plus a mechanism, and the mechanism announces itself through murmurs (new or changing regurgitant murmurs), emboli (stroke, splenic or renal infarcts, limb ischaemia, or septic pulmonary emboli from right-sided disease) and immune phenomena (glomerulonephritis, Osler nodes, Roth spots). The modified Duke criteria simply formalise this structure into a diagnostic instrument [1].
Reading the tempo: acute versus subacute
The tempo is the organism speaking. Acute endocarditis — days to a week or two of high fevers, rigors and rapid deterioration, often on previously normal valves — is S. aureus (and occasionally beta-haemolytic streptococci or pneumococci) until proven otherwise; destruction is fast, abscesses form early, and the window to prevent valve failure and embolism is short [3] [18]. Subacute endocarditis — weeks to months of low-grade fever, malaise, weight loss, anaemia and murmur, on a previously damaged valve — is the viridans streptococci and enterococci, and it is here that the classic immunologic stigmata (Osler nodes, Roth spots, glomerulonephritis) have time to appear [3]. The practical consequence: the sicker the patient, the more your empirical cover must front-load anti-staphylococcal activity, and the less you can afford to wait for culture confirmation before escalating imaging and surgical consultation [2].
The modified Duke criteria, applied
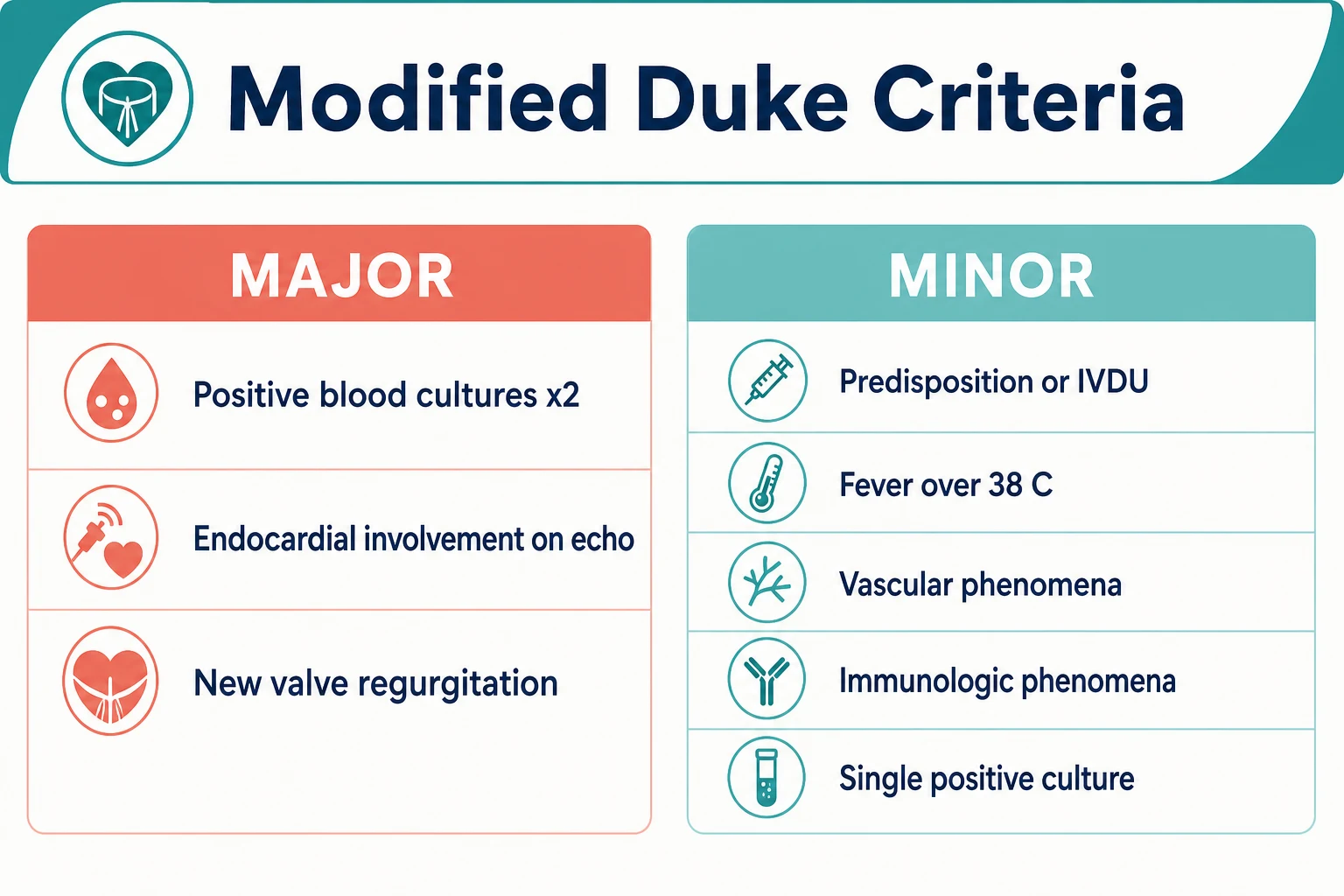
The 2023 Duke–ISCVID update modernised the criteria — molecular diagnostics and advanced imaging entered the major criteria — while preserving the architecture examiners expect you to recite [1]:
| Major criteria | What counts |
|---|---|
| Positive blood cultures | Typical endocarditis organisms (viridans streptococci, Streptococcus gallolyticus, HACEK group, S. aureus, enterococci) from two or more separate sets; or persistently positive cultures with an organism consistent with endocarditis; or a single positive culture or phase I serology for Coxiella burnetii [1] |
| Imaging evidence of endocardial involvement | Vegetation, abscess, pseudoaneurysm, fistula, leaflet perforation or valve aneurysm on echocardiography or cardiac CT; new partial dehiscence of a prosthetic valve; abnormal periprosthetic uptake on ¹⁸F-FDG PET/CT or radiolabelled leucocyte SPECT/CT (new in 2023) [1] |
| New valvular regurgitation | A new regurgitant murmur, or echocardiographic worsening of pre-existing regurgitation — stenosis alone does not qualify [1] |
| Minor criteria | What counts |
|---|---|
| Predisposition | Predisposing cardiac condition, prosthetic material, or injecting drug use |
| Fever | Temperature above 38.0 °C |
| Vascular phenomena | Arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial haemorrhage, conjunctival haemorrhage, Janeway lesions |
| Immunologic phenomena | Glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor |
| Microbiological evidence | Positive cultures that do not meet major criteria (for example, a single set with a typical organism) [1] |
Then the verdict, which you must state without hesitating: definite endocarditis is two major criteria, or one major plus three minor, or five minor; possible is one major plus one minor, or three minor; rejected is a firm alternative diagnosis, resolution of the syndrome with four or fewer days of antibiotics, or no pathological evidence at surgery or autopsy [1].
Numbers that carry marks
Organisms by context
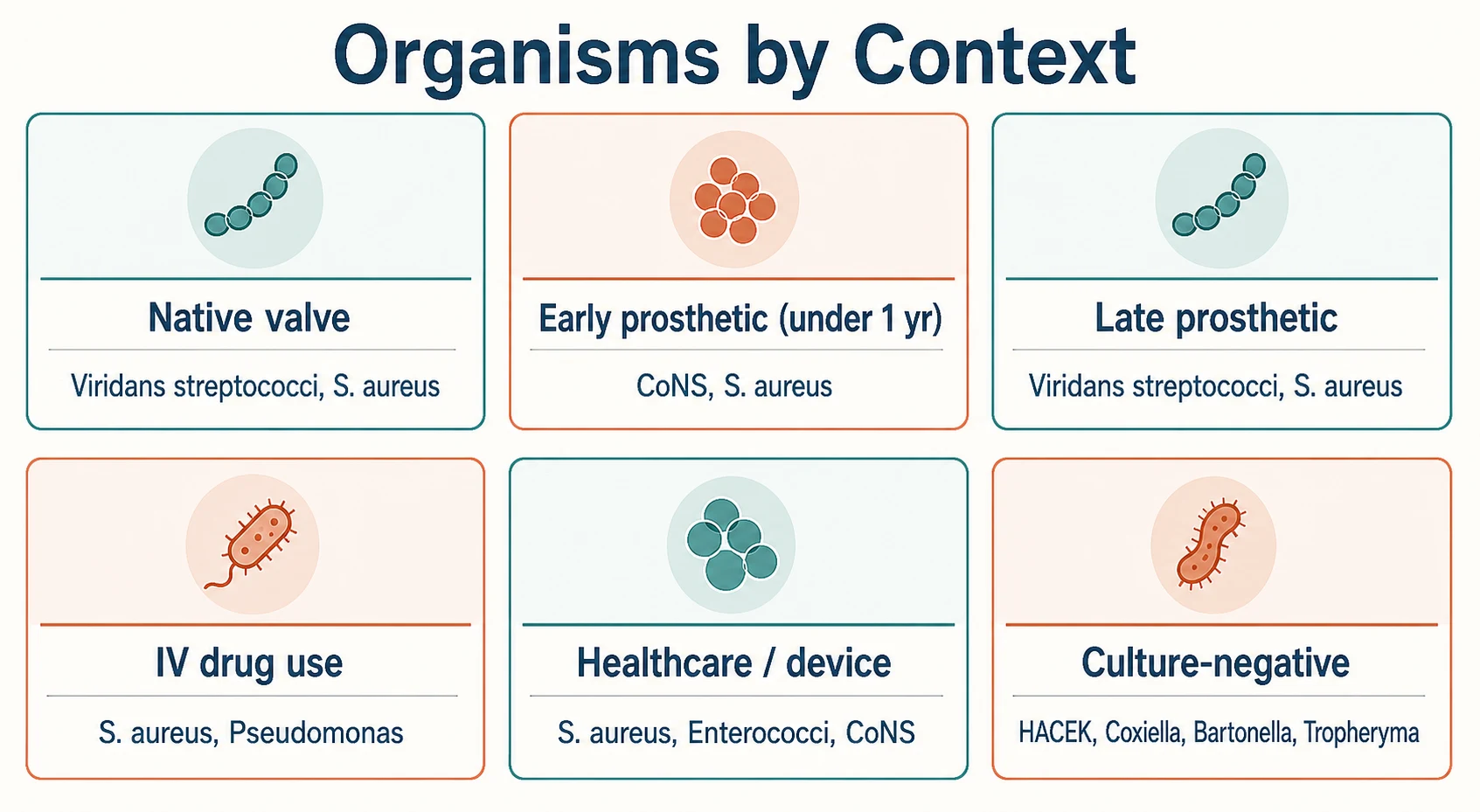
The organism shortlist is written by the clinical context. Examiners expect the table cold [3] [18]:
| Context | Likely organisms | The pearl that earns marks |
|---|---|---|
| Native valve, community | Viridans-group streptococci, S. aureus, enterococci, Streptococcus gallolyticus | S. gallolyticus (formerly S. bovis) endocarditis means colonoscopy — it is a marker of colonic neoplasia [3] |
| Prosthetic valve, early (first year) | Coagulase-negative staphylococci, S. aureus, gram-negative bacilli, fungi | Perioperative seeding; high rates of abscess and dehiscence; low threshold for PET/CT [1] |
| Prosthetic valve, late | Viridans streptococci, S. aureus, enterococci | Microbiology converges on the native-valve pattern |
| Injecting drug use | S. aureus (dominant, usually tricuspid), Pseudomonas, polymicrobial, Candida | Right-sided disease with septic pulmonary emboli; always test for HIV, HBV and HCV [3] |
| Healthcare-associated / haemodialysis | S. aureus, enterococci, coagulase-negative staphylococci | Line- and access-related; organism ecology follows the ward and the device [18] |
| CIED (pacemaker/ICD) infection | S. aureus, coagulase-negative staphylococci | Pocket infection or lead endocarditis; treatment is complete system removal, not antibiotics alone [19] |
| HACEK | Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella | Fastidious gram-negatives of the oropharynx; slow-growing, historically culture-negative; large vegetations and frequent emboli; usually ceftriaxone-susceptible [22] |
| Culture-negative | Coxiella burnetii, Bartonella species, Tropheryma whipplei, fungi | Prior antibiotics are the commonest cause; then think zoonoses and fastidious organisms [20] |
A few organisms deserve their own lines. S. aureus is the acute, destructive pathogen: it attacks normal valves, seeds metastatic foci, and dominates IVDU and healthcare disease. Viridans streptococci are the classic subacute organism of damaged native valves, seeded from the mouth. Enterococci (mostly E. faecalis) affect older patients with gastrointestinal or genitourinary portals and dictate combination therapy. Candida endocarditis — TPN, ICU, IVDU, prosthetic material — carries the worst prognosis and almost always requires surgery [3] [18].
Imaging strategy: TTE, TOE, and the new modalities
Because imaging is a major Duke criterion, the echo strategy is part of the diagnosis, not a downstream nicety [1] [2]:
- TTE first — rapid, safe, quantifies valve function, and detects most large vegetations. Sensitivity is only around 70% for native-valve vegetations, so a negative TTE never excludes endocarditis when suspicion is real [2].
- TOE when there is a prosthetic valve or intracardiac device, high clinical suspicion with a negative or inadequate TTE, S. aureus bacteraemia with risk features, or a preoperative search for periannular extension. TOE sensitivity exceeds 90% for vegetations and is far superior for abscesses [2].
- Repeat echo in 5–7 days if suspicion persists and early studies are negative — vegetations and abscesses declare themselves over time [2].
- ¹⁸F-FDG PET/CT and leucocyte SPECT/CT earned major-criterion status in the 2023 Duke update for prosthetic valves and devices, exactly where echo struggles most [1].
For S. aureus bacteraemia specifically, a validated criteria set helps decide who needs transoesophageal imaging: persistent bacteraemia, community acquisition, haemodialysis dependence and intracardiac devices all push toward mandatory TOE [24].
Empirical antimicrobial therapy
Empirical therapy starts after the cultures, covers what the context dictates, and is de-escalated the moment the organism and susceptibilities return. The governing principle, with the standing caveat that local antibiograms and current Therapeutic Guidelines or equivalent always trump a textbook table [2] [3]:
| Scenario | A defensible empirical choice | Rationale |
|---|---|---|
| Native valve, indolent presentation | Amoxicillin/ampicillin-based cover; add anti-staphylococcal cover if acutely unwell | Streptococci and enterococci dominate indolent native disease [3] |
| Native valve, acutely ill or septic | Vancomycin plus ceftriaxone (or the local anti-staphylococcal plus gram-negative equivalent) | Must cover S. aureus including MRSA until susceptibilities return [3] |
| Prosthetic valve | Vancomycin plus an anti-pseudomonal beta-lactam, with or without gentamicin and rifampicin per local protocol | Early prosthetic disease spans CoNS, S. aureus and gram-negatives [2] |
| MRSA plausible (healthcare, dialysis, IVDU) | Vancomycin (AUC-guided dosing) as the empirical backbone | De-escalate to a beta-lactam the moment MSSA is proven — see below [12] |
Two practical additions. First, take a real allergy history: a documented anaphylactic penicillin allergy changes the backbone (vancomycin or daptomycin), but a vague "rash as a child" should not deny the patient the beta-lactam that treats MSSA best. Second, think about logistics early: once the patient is stable on an organism-directed regimen, outpatient parenteral antimicrobial therapy (OPAT) with a once-daily agent such as ceftriaxone, or a PICC-delivered continuous infusion, is how a six-week course actually gets delivered [3] [9].
Definitive therapy and duration
Once the organism and susceptibilities return, therapy becomes organism-directed, intravenous, and counted from the first negative blood culture [3]:
| Organism and setting | Regimen (representative) | Duration |
|---|---|---|
| MSSA, native valve | Flucloxacillin 2 g IV 4–6 hourly (cefazolin if non-severe penicillin allergy) | 4–6 weeks [3] |
| MRSA | Vancomycin (AUC-guided) or daptomycin | 6 weeks [3] |
| Viridans streptococci, fully penicillin-susceptible | Benzylpenicillin, or ceftriaxone 2 g IV daily; a 2-week course combined with gentamicin is an option in selected low-risk patients | 4 weeks (native valve) [3] |
| Enterococcus faecalis | Ampicillin 2 g IV 4-hourly plus ceftriaxone — now preferred over ampicillin plus gentamicin because efficacy is equivalent and nephrotoxicity is avoided | 4–6 weeks [14] |
| Prosthetic valve (any organism) | Organism-directed, with guideline-specified additions (rifampicin and an initial aminoglycoside for staphylococcal prosthetic disease) | 6 weeks minimum [2] |
| HACEK group | Ceftriaxone 2 g IV daily (ampicillin if susceptible) | 4 weeks [22] |
| Selected uncomplicated right-sided MSSA (IVDU) | Anti-staphylococcal beta-lactam; a 2-week course is a guideline option when there is no left-sided disease, no metastatic focus, no renal failure and rapid response | 2 weeks, strictly selected [3] |
The gentamicin controversy. Synergistic aminoglycoside was once reflex for staphylococcal and enterococcal endocarditis; the tide has turned. Initial low-dose gentamicin in S. aureus bacteraemia and endocarditis is measurably nephrotoxic without improving outcomes, and guidelines have progressively restricted it — it is no longer routine for native-valve staphylococcal disease, and for enterococci the ampicillin–ceftriaxone double beta-lactam has taken over wherever renal function is a concern [23] [14] [2].
The POET trial and oral step-down. POET randomised stable patients with left-sided endocarditis (streptococci, E. faecalis, S. aureus or coagulase-negative staphylococci) who had completed at least 10 days of intravenous therapy (or at least one week after valve surgery), were afebrile and clinically responding, and had a TOE excluding abscess or valve deterioration: switching them to a two-drug oral regimen was non-inferior to completing the full course intravenously. The selection criteria are the exam content — stable, left-sided, responding, echo-clean. POET does not license early oral therapy for the septic, the abscessed or the actively embolising patient [9].
For contrast, uncomplicated gram-negative bacteraemia without endocarditis can be treated for seven days as safely as fourteen — useful context for how duration thinking has shortened everywhere except endovascular infection [10].
Right-sided disease and the IVDU patient
Right-sided (usually tricuspid) endocarditis is a different disease from its left-sided counterpart: it dominates in people who inject drugs, S. aureus causes the great majority, and its emboli go to the lung — so the presentation is fever with cough, pleuritic pain and cavitating nodules on CT rather than stroke and splenic infarcts [3] [18]. Prognosis is better, valve surgery is needed far less often, and strictly selected uncomplicated MSSA tricuspid disease can be treated with two weeks of intravenous therapy (no left-sided involvement, no metastatic foci, no renal failure, no immunosuppression, rapid response) [3]. The ward craft matters as much as the pharmacology: test for HIV and viral hepatitis, involve addiction medicine while the patient is admitted, start opioid agonist therapy where appropriate, and plan venous access deliberately — PICC decisions in active injecting drug use are a governance question, and the discharge conversation should include harm reduction as genuine endocarditis prevention [2] [6].
Enterococcal endocarditis: combination is the point
Enterococci are intrinsically tolerant to single-agent beta-lactams, which is why endocarditis — unlike enterococcal bacteraemia from a line — demands combination therapy aimed at bactericidal synergy. The modern default for E. faecalis is ampicillin plus ceftriaxone, which matched ampicillin plus gentamicin for efficacy while avoiding the aminoglycoside nephrotoxicity that older regimens inflicted on an elderly, often renally impaired population [14]. Ask the laboratory about high-level aminoglycoside resistance before committing to any gentamicin-containing plan, and remember that E. faecium — frequently vancomycin-resistant — is a different and much harder problem that belongs to the ID team [3].
Surgery: the three triggers
Valve surgery in active endocarditis is not a failure of antibiotics — it is a defined arm of treatment, and a substantial proportion of patients meet a surgical indication. The three indication groups, each worth marks separately [2] [13]:
- Heart failure — severe acute regurgitation (or obstruction) with heart failure or shock is the strongest indication and the main driver of mortality benefit; operate urgently.
- Uncontrolled infection — periannular abscess or fistula (heralded by new PR prolongation or heart block), persistent bacteraemia beyond about 5–7 days of appropriate therapy, enlarging vegetations, or fungal and multiresistant organisms.
- Prevention of embolism — recurrent emboli with persistent vegetations, or very large vegetations: greater than 10 mm after an embolic event, or greater than 15 mm in isolation on ESC thresholds [2].
The EASE trial randomised patients with left-sided endocarditis, severe valve disease and large vegetations to early surgery versus conventional care: early surgery cut the composite of death and systemic embolism, driven almost entirely by fewer emboli [13]. Timing after a stroke is the classic viva probe: an ischaemic stroke without haemorrhage is not a reason to delay indicated valve surgery, whereas intracranial haemorrhage generally mandates a delay of at least two weeks — and neurological deterioration or a mycotic aneurysm rewrites the plan entirely [2] [3].
CIED infection deserves its own line: the treatment is complete system removal — generator and leads — plus organism-directed antibiotics; antibiotics alone without extraction relapse, and percutaneous extraction is the default where expertise exists [19].
Culture-negative endocarditis
Blood culture-negative endocarditis (BCNE) is endocarditis by imaging or surgical criteria without culture growth, and the first question is always: did antibiotics precede the cultures? Prior antibiotics are the commonest cause; truly fastidious organisms come second [20].
The structured workup, built on the prospective 819-case Marseille experience [20]:
- Re-take the history for epidemiology — livestock or abattoir exposure and unpasteurised dairy (Coxiella burnetii), cats, homelessness and body lice (Bartonella), chronic diarrhoea and weight loss (Tropheryma whipplei), travel and aquatic exposures.
- Serologies — Coxiella phase I IgG (a titre at or above 1:800 is itself a Duke major criterion) and Bartonella serology [20] [1].
- Special microbiology — prolonged-incubation cultures, Bartonella and Tropheryma PCR from blood, and — if surgery happens — valve tissue 16S rRNA PCR, which identifies the organism in the majority of truly culture-negative valves [20].
- Non-infective mimics — marantic (non-bacterial thrombotic) endocarditis in malignancy, Libman–Sacks endocarditis in lupus, atrial myxoma. These are the classic "rejected Duke" endpoints, and they are exactly why the rejected category exists [3] [1].
Complications: the embolic and immunologic twin engines
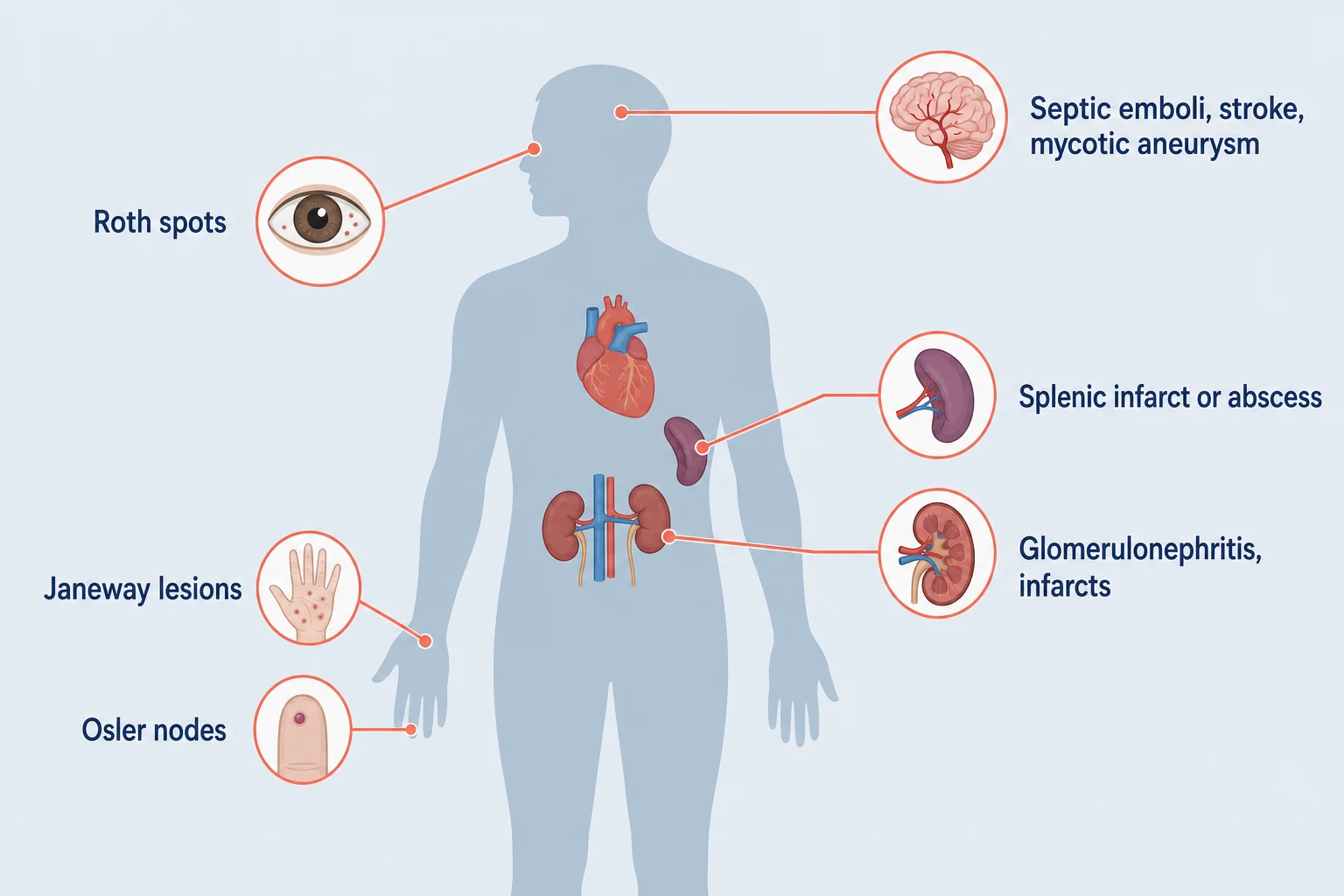
Everything bad in endocarditis travels by one of two routes: bits of vegetation breaking off, or immune complexes depositing [3] [21]:
- Embolic, left-sided: stroke (the most feared — a validated risk calculator weighs S. aureus aetiology, vegetation size and mobility, prior embolism, age and atrial fibrillation), splenic infarct or abscess (left upper quadrant pain, persistent fever), renal infarcts (flank pain, haematuria), limb ischaemia, coronary embolism, and mycotic aneurysms — intracranial ones rupture and kill, so new severe headache or neurological signs mandate cerebrovascular imaging [21] [3].
- Embolic, right-sided: septic pulmonary emboli — cough, pleuritic pain and cavitating nodules on CT — the signature of IVDU tricuspid disease [3].
- Immunologic: immune-complex glomerulonephritis (haematuria, low complement, rising creatinine), Osler nodes (tender pulp nodules), Roth spots (retinal haemorrhages with pale centres) and a positive rheumatoid factor — all subacute features, all minor Duke criteria [1].
- Cardiac structural: valve destruction with acute severe regurgitation, periannular abscess (new PR prolongation or bundle branch block), fistula formation, and the heart failure that drives surgical urgency [2].
- Metastatic seeding from S. aureus: vertebral osteomyelitis and epidural abscess (back pain with bacteraemia is an MRI decision, not an analgesic decision), septic arthritis, psoas and visceral abscesses [6] [18].
The S. aureus bacteraemia rule
S. aureus bacteraemia (SAB) is the highest-stakes routine problem in hospital infection practice, and it has its own discipline [6] [18]:
The complicated-SAB identifiers from Fowler's derivation cohort are worth reciting: positive follow-up blood cultures at 48–96 hours, persistent fever at 72 hours, community acquisition, and skin findings suggesting acute systemic infection — each independently predicted endocarditis or deep-seated infection [8].
Persistent and relapsing bacteraemia. Bacteraemia that persists beyond 48–72 hours of appropriate therapy, or that relapses after a course finishes, is not a pharmacology problem — it is an anatomy problem. The discipline is to re-interrogate every potential focus systematically: the line and any device, the valves (repeat or escalate imaging — a first negative TTE does not end the search), the spine and epidural space (back pain with bacteraemia is an MRI), joints, and solid-organ abscesses in spleen, kidneys, liver and psoas. Relapsing S. aureus after a "completed" course almost always means the course was too short for an unrecognised focus — usually endocarditis or vertebral infection — and the answer is to find and control that focus and then treat to the longer, counted duration, not to cycle through broader antibiotics [6] [8] [18].
The dialysis-catheter SAB deserves a special mention because it is the classic SAQ and long-case scenario: culture through the line and peripherally, remove the catheter (S. aureus is a mandatory-removal organism), establish temporary access, echo, and treat for four weeks when endocarditis or seeding cannot be excluded [11] [6].
Prevention: who actually gets dental prophylaxis
Prophylaxis policy is where ANZ, UK and US guidance visibly diverge, and examiners enjoy it [16] [17]:
- US (AHA 2007) and ANZ practice restrict prophylaxis to the highest-risk hosts: prosthetic cardiac valve or prosthetic material used for valve repair, previous infective endocarditis, unrepaired cyanotic congenital heart disease (or repaired congenital disease with residual defects adjacent to prosthetic material), and cardiac transplant recipients with valvulopathy. For these patients, prophylaxis is given only for dental procedures that manipulate gingival or periapical tissue or perforate the oral mucosa — amoxicillin 2 g orally about an hour before the procedure, with guideline-listed alternatives for penicillin allergy [16].
- UK (NICE 2008) went further and advised against routine prophylaxis for anyone undergoing dental or non-dental procedures. The before-and-after data showed prophylaxis prescribing collapsed after NICE without a statistically significant rise in endocarditis in the initial analysis [17] — but the interrupted time-series out to 2013 showed a significant increase in endocarditis incidence in England, leaving genuine international disagreement about whether NICE went too far [15].
- The defensible exam position: follow the local guideline (in ANZ, the restricted AHA-style list), emphasise oral hygiene and skin/injection-site care as the highest-value prevention for everyone, and in people who inject drugs, invest in harm reduction as endocarditis prevention [16] [15].
The DCE long-case angle
The examiner's favourite long case is endocarditis with embolic complications in a patient whose social world complicates the medical plan — classically a person who injects drugs with tricuspid endocarditis and septic pulmonary emboli, or a mechanical-valve patient with a septic embolic stroke [2] [6].
- Open with the problem list, not the organism: active infection and its source, cardiac structural damage, embolic burden, the anticoagulation question, the substance-use and social determinants, and the six-week treatment logistics (venous access, OPAT suitability, adherence, housing) [6].
- For mechanical valve plus embolic stroke, state the dilemma plainly: continuing anticoagulation risks haemorrhagic transformation of a septic infarct; stopping it risks valve thrombosis. A defensible position is to pause anticoagulation briefly after a significant septic cerebral embolus, image the brain, and restart once haemorrhage is excluded — with the multidisciplinary team, not the registrar alone, owning the decision [3] [2].
- For IVDU, be visibly non-judgemental: treat the infection completely, involve addiction medicine early, start opioid agonist therapy in hospital, plan venous access deliberately (PICC decisions are a governance question, not a reflex), and frame any future valve-surgery candidacy as a multidisciplinary decision made with the patient, because recurrence risk is real [2] [6].
The DCE short-case angle
"Examine this patient for signs of infective endocarditis" is a systematic-routine station. The sequence that looks effortless [1] [3]:
- Hands — splinter haemorrhages, Janeway lesions (non-tender palmar or plantar macules), Osler nodes (tender pulp nodules), clubbing, and the dialysis fistula or injection marks that point to the source.
- Eyes and mouth — conjunctival petechiae, Roth spots on fundoscopy (say that you would examine the fundi), dental state, palatal petechiae.
- Precordium — inspect for sternotomy and CIED scars, then auscultate for regurgitant murmurs (aortic and mitral), prosthetic valve sounds, and signs of heart failure.
- Abdomen and urine — splenomegaly, and a urine dipstick for haematuria from glomerulonephritis.
- Close the loop — ask for the temperature chart, the blood culture results and the echocardiogram [1] [3].
Present with Duke language: "This patient has peripheral stigmata of endocarditis, a new early diastolic murmur and splenomegaly — findings that satisfy vascular and immunologic minor criteria and mandate blood cultures and echocardiography" [1].
Exam traps, collected
References
- [1]Fowler VG, Durack DT, Selton-Suty C, et al. The 2023 Duke-International Society for Cardiovascular Infectious Diseases Criteria for Infective Endocarditis: Updating the Modified Duke Criteria Clin Infect Dis, 2023.PMID 37138445
- [2]Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis Eur Heart J, 2023.PMID 37622656
- [3]Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association Circulation, 2015.PMID 26373316
- [4]Lee A, Mirrett S, Reller LB, et al. Detection of bloodstream infections in adults: how many blood cultures are needed? J Clin Microbiol, 2007.PMID 17881544
- [5]Doern GV, Carroll KC, Diekema DJ, et al. Practical Guidance for Clinical Microbiology Laboratories: A Comprehensive Update on the Problem of Blood Culture Contamination and a Discussion of Methods for Addressing the Problem Clin Microbiol Rev, 2019.PMID 31666280
- [6]Holland TL, Arnold C, Fowler VG Jr. Clinical management of Staphylococcus aureus bacteremia: a review JAMA, 2014.PMID 25268440
- [7]Bai AD, Showler A, Burry L, et al. Impact of Infectious Disease Consultation on Quality of Care, Mortality, and Length of Stay in Staphylococcus aureus Bacteremia: Results From a Large Multicenter Cohort Study Clin Infect Dis, 2015.PMID 25701854
- [8]Fowler VG Jr, Olsen MK, Corey GR, et al. Clinical identifiers of complicated Staphylococcus aureus bacteremia Arch Intern Med, 2003.PMID 14504120
- [9]Iversen K, Ihlemann N, Gill SU, et al. Partial Oral versus Intravenous Antibiotic Treatment of Endocarditis N Engl J Med, 2019.PMID 30152252
- [10]Yahav D, Franceschini E, Koppel F, et al. Seven Versus 14 Days of Antibiotic Therapy for Uncomplicated Gram-negative Bacteremia: A Noninferiority Randomized Controlled Trial Clin Infect Dis, 2019.PMID 30535100
- [11]Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America Clin Infect Dis, 2009.PMID 19489710
- [12]McDanel JS, Perencevich EN, Diekema DJ, et al. Comparative effectiveness of beta-lactams versus vancomycin for treatment of methicillin-susceptible Staphylococcus aureus bloodstream infections among 122 hospitals Clin Infect Dis, 2015.PMID 25900170
- [13]Kang DH, Kim YJ, Kim SH, et al. Early surgery versus conventional treatment for infective endocarditis N Engl J Med, 2012.PMID 22738096
- [14]Fernández-Hidalgo N, Almirante B, Gavaldà J, et al. Ampicillin plus ceftriaxone is as effective as ampicillin plus gentamicin for treating enterococcus faecalis infective endocarditis Clin Infect Dis, 2013.PMID 23392394
- [15]Dayer MJ, Jones S, Prendergast B, et al. Incidence of infective endocarditis in England, 2000-13: a secular trend, interrupted time-series analysis Lancet, 2015.PMID 25467569
- [16]Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group Circulation, 2007.PMID 17446442
- [17]Thornhill MH, Dayer MJ, Forde JM, et al. Impact of the NICE guideline recommending cessation of antibiotic prophylaxis for prevention of infective endocarditis: before and after study BMJ, 2011.PMID 21540258
- [18]Tong SY, Davis JS, Eichenberger E, et al. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management Clin Microbiol Rev, 2015.PMID 26016486
- [19]Blomström-Lundqvist C, Traykov V, Erba PA, et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) Europace, 2020.PMID 31702000
- [20]Fournier PE, Thuny F, Richet H, et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases Clin Infect Dis, 2010.PMID 20540619
- [21]Hubert S, Thuny F, Resseguier N, et al. Prediction of symptomatic embolism in infective endocarditis: construction and validation of a risk calculator in a multicenter cohort J Am Coll Cardiol, 2013.PMID 23906859
- [22]Sharara SL, Tayyar R, Kanafani ZA, et al. HACEK endocarditis: a review Expert Rev Anti Infect Ther, 2016.PMID 27124204
- [23]Cosgrove SE, Vigliani GA, Fowler VG Jr, et al. Initial low-dose gentamicin for Staphylococcus aureus bacteremia and endocarditis is nephrotoxic Clin Infect Dis, 2009.PMID 19207079
- [24]Kaasch AJ, Fowler VG Jr, Rieg S, et al. Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia Clin Infect Dis, 2011.PMID 21653295