Phys · infectious
Bone AND Joint Infections
Also known as Bone AND Joint Infections · bone and joint infections
Consultant-physician depth guide to Bone AND Joint Infections for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
Bone AND Joint Infections is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
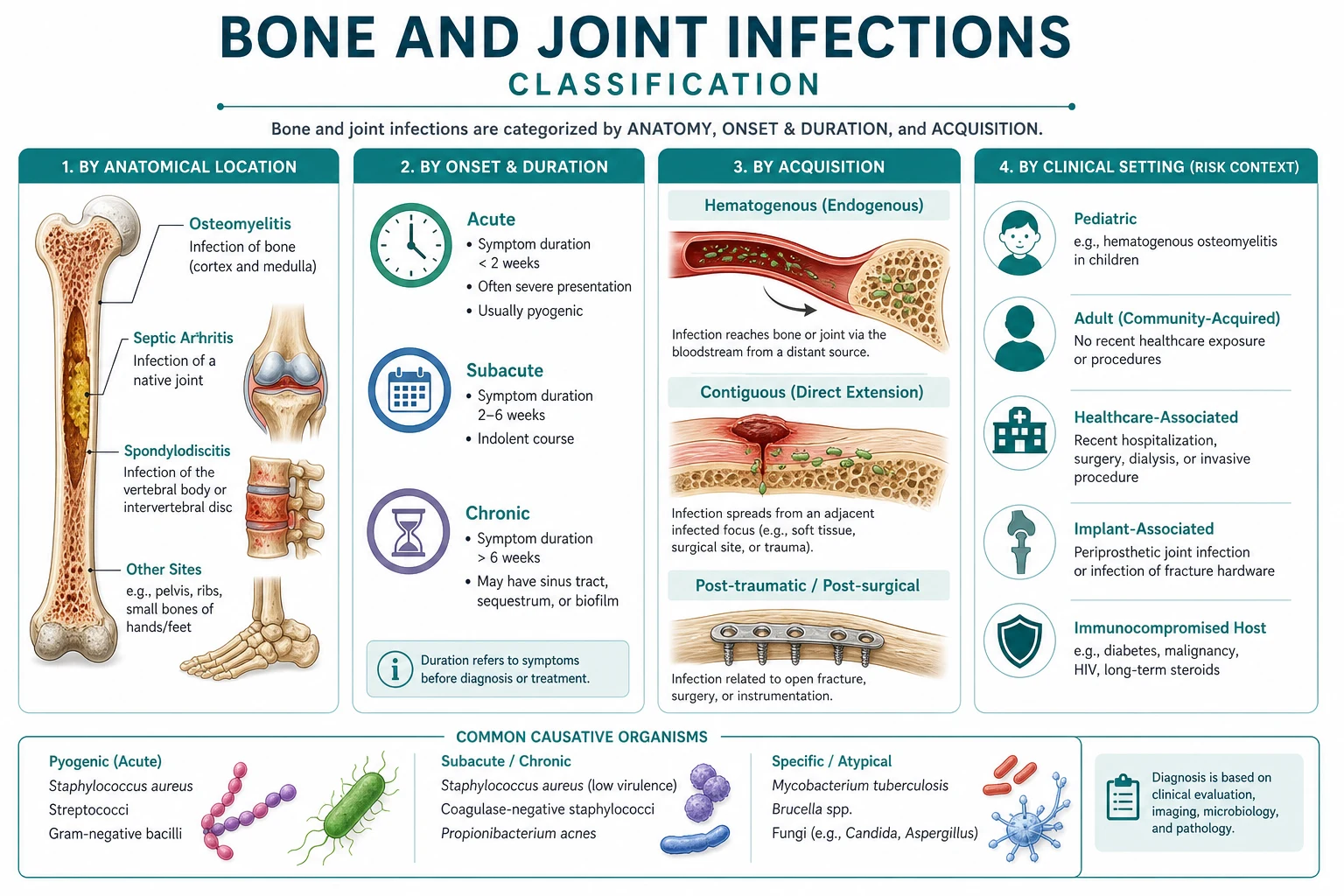
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
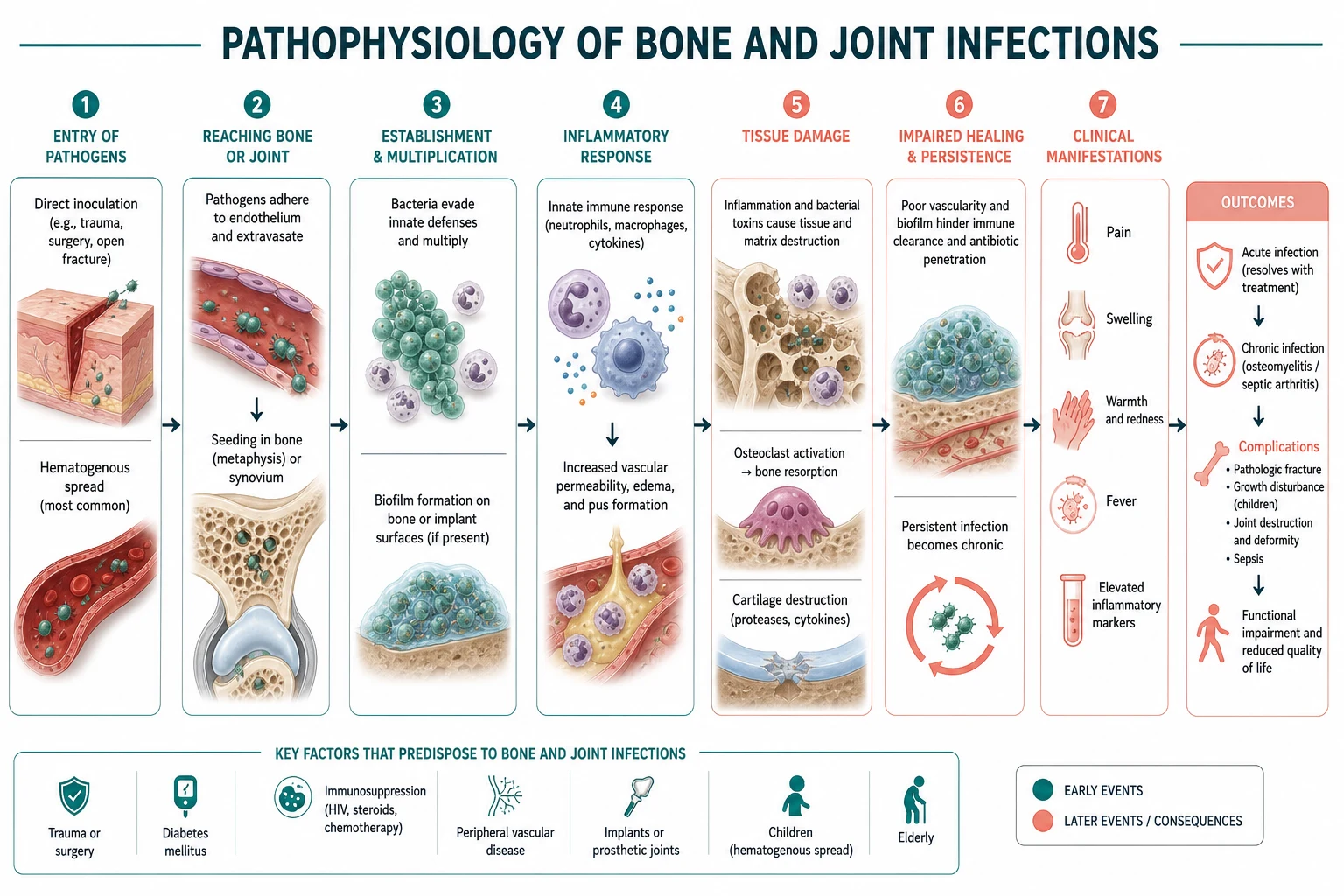
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]

Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Bone AND Joint Infections to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Ren Z, Lan Q, Tian Y, Xu N, et al. Atlantoaxial Rotatory Fixation: Current Challenges and Advances in Diagnosis and Management JB JS Open Access, 2026.PMID 42465621
- [2]Zhu Y, Qin S [Limb reconstruction: connotation, extension, and its core value in modern medicine] Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, 2026.PMID 42464534
- [3]Box MW, Cooper JQ, Stanke J, Domingue GA, et al. Intramedullary nail fixation for tibial plateau fractures: a systematic review of techniques and outcomes OTA Int, 2026.PMID 42459748
- [4]Wang T, Meng Y, Zhang S, Wang Y, et al. Uncovering the cytogenetic hallmarks of resident and expanded natural killer cells from patients with acquired aplastic anemia Sci Rep, 2026.PMID 42448949
- [5]O'Neil JC, Lehman B, Seyler T, Piuzzi N, et al. ID-ing the value: how are orthopaedic infectious disease physicians compensated for their time? A national survey J Bone Jt Infect, 2026.PMID 42312214
- [6]Mitrovic S, Delplanque M, Ea HK, Frémond ML, et al. Club Rhumatismes et Inflammation guidelines for anti-interleukin-1 therapy: 2026 update Joint Bone Spine, 2026.PMID 42276158
- [7]Doan HN, Chang MC Comparative Effectiveness of Unstable Versus Stable Resistance Training on Lower Limb Strength, Mobility, and Fear of Falling in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials Am J Phys Med Rehabil, 2026.PMID 42468010
- [8]Liu HW, Tsai TL Virtual Reality-assisted Physiotherapeutic Training for Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis Am J Phys Med Rehabil, 2026.PMID 42468005
- [9]Osborne AK, Brown RD, Sillence E Effects of Social Media Narratives on Affective and Behavioral Responses to Menopause Content: Randomized Online Experimental Study JMIR Form Res, 2026.PMID 42467962
- [10]Pallanza M, Ateschrang A, Boyd A, Conen A, et al. Nationwide, multicentre, prospective periprosthetic joint infection cohort study: study protocol of the Swiss Revision Cohort (REVCO) BMJ Open, 2026.PMID 42463213
- [11]Ng Y, Benedicta S, Hong CC Ankle Arthrodesis After Joint Destruction from Septic Arthritis in a High-Risk Patient Using a Novel Intra-Articular Pinning Technique: A Case Report JBJS Case Connect, 2026.PMID 42462058
- [12]Fonkoué L, Tissingh EK, Marais LC, Malaba M, et al. Management of fracture-related infection in low-resource settings in Africa: recommendations and guidelines from an international expert group J Bone Jt Infect, 2026.PMID 42445811