Phys · infectious
Central Nervous System Infections
Also known as meningitis · bacterial meningitis · viral meningitis · encephalitis · HSV encephalitis · brain abscess · cryptococcal meningitis · meningoencephalitis
Consultant-physician-depth guide to meningitis, encephalitis and brain abscess — empirical therapy before imaging, CT-before-LP criteria, CSF interpretation, dexamethasone evidence, HSV aciclovir, and cryptococcal management — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Central Nervous System Infections
The answer first
CNS infection is the specialty where sequence saves lives. Three rules cover almost every scenario you will meet, in exams and on call [1]:
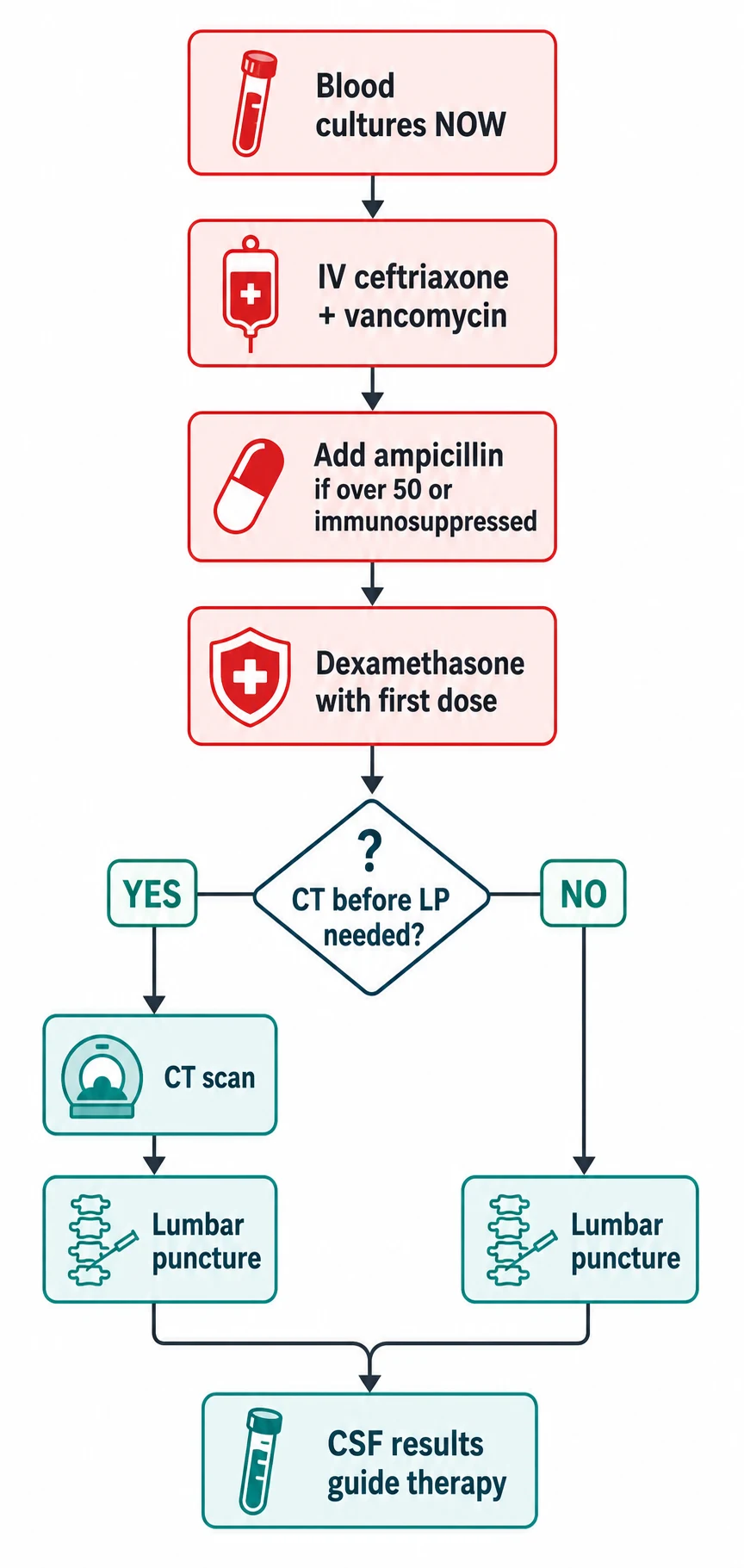
- Antibiotics before imaging, every time. If bacterial meningitis is plausible, take blood cultures and give ceftriaxone (plus vancomycin per local protocol, plus ampicillin if the patient is over 50 or immunosuppressed) immediately. The CT and the LP come after. Every hour of delay worsens outcome [1] [3].
- Confusion means encephalitis — start aciclovir. Fever with headache alone is meningitis until proven otherwise; fever with altered behaviour, personality change, seizures or dysphasia is encephalitis until proven otherwise, and the treatable cause is HSV. Aciclovir 10 mg/kg TDS IV starts on suspicion, not on PCR confirmation [5].
- The LP is diagnostic, not optional — but respect the two gates. Gate one: CT first if immunosuppression, seizures, papilloedema, focal signs or reduced consciousness (Hasbun criteria). Gate two: measure the opening pressure, because in cryptococcal meningitis the pressure itself kills and serial drainage is treatment [4] [7].
Meningitis, encephalitis or abscess — the discrimination
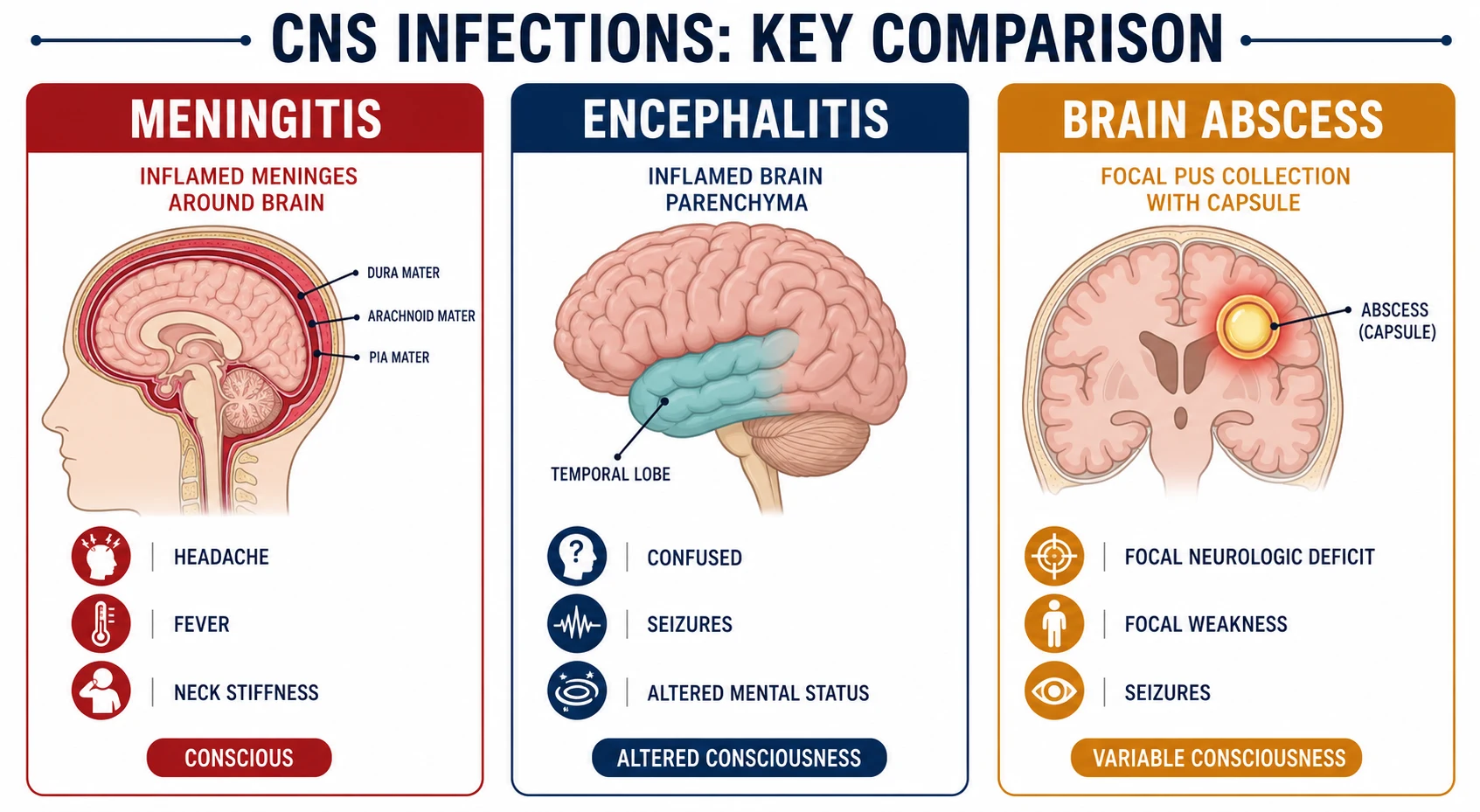
These three share fever and headache. They separate on where the disease sits [1]:
| Meningitis | Encephalitis | Brain abscess | |
|---|---|---|---|
| Site | Meninges [1] | Brain parenchyma [5] | Focal pus collection [9] |
| Consciousness | Preserved early; obtunded late | Altered early — the defining feature | Usually preserved unless raised ICP |
| Focal signs/seizures | Uncommon early | Common (temporal lobe: dysphasia, personality change, olfactory hallucinations) | Common — the presenting feature |
| Pace | Hours to 1–2 days | Days | Subacute, days to weeks |
| Key source | Community respiratory spread | HSV reactivation; autoimmune mimics | Contiguous (sinusitis, otitis, dental) or haematogenous (endocarditis, lung, cyanotic CHD) |
The trap is that the boundaries blur: severe meningitis causes encephalopathic features, and HSV encephalitis inflames the meninges too. The rule that survives the viva: prominent early alteration of behaviour, personality or language means treat for encephalitis — because the treatable one is HSV and delay costs cortex [5].
Bacterial meningitis — management in order
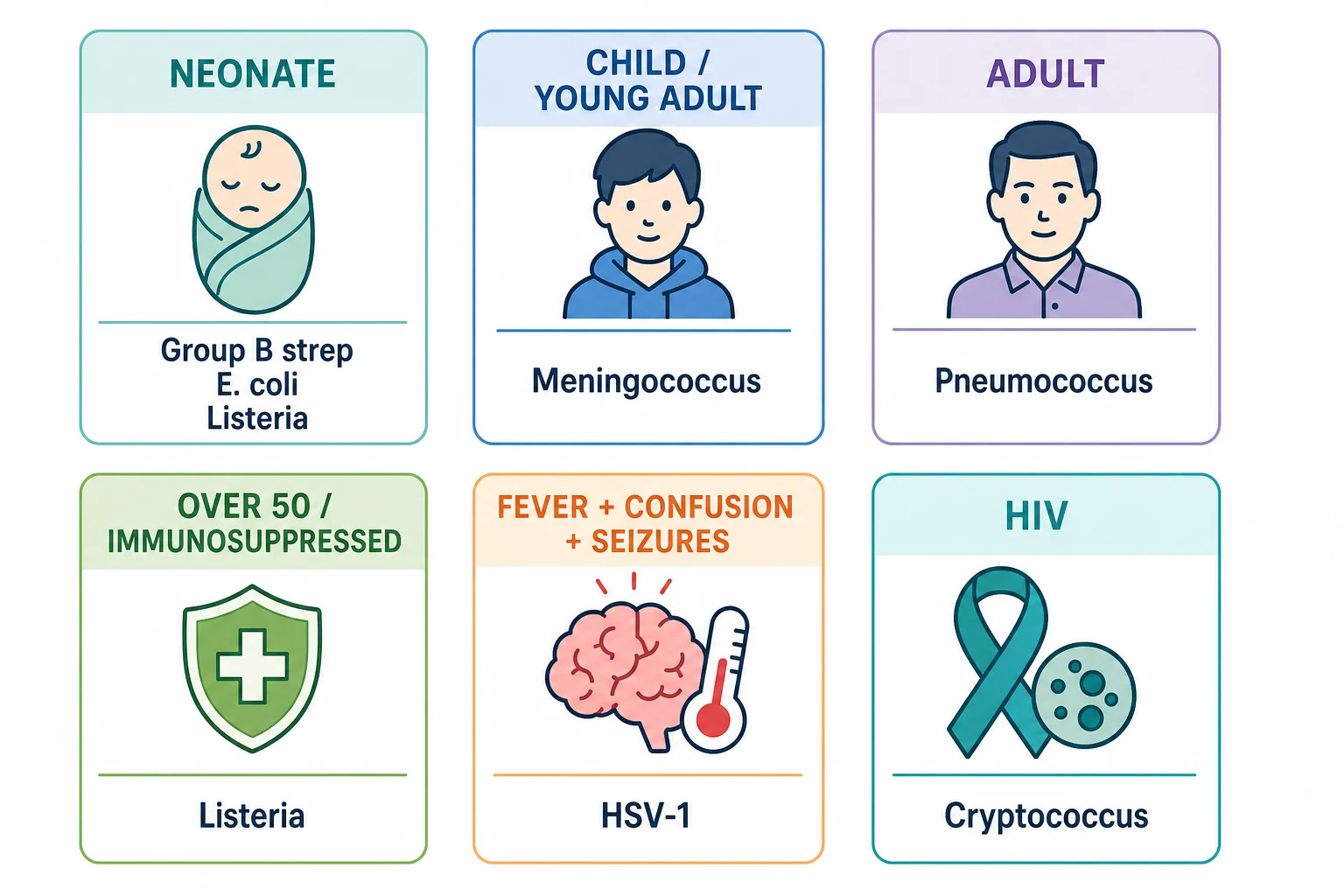
The organism mix shifts with age and immunity, and the empirical regimen follows it [3]:
| Context | Likely pathogens | Empirical regimen (adult) [3] |
|---|---|---|
| 18–50 years, community | Pneumococcus, meningococcus | Ceftriaxone 2 g IV 12-hourly + vancomycin (per local protocol, covers ceftriaxone-resistant pneumococcus) |
| Over 50, or immunosuppressed, pregnant, alcoholic | Above plus Listeria monocytogenes | Add ampicillin 2 g IV 4-hourly (Listeria is intrinsically cephalosporin-resistant) |
Then narrow to the organism: benzylpenicillin for meningococcus, ceftriaxone continued for pneumococcus (duration by susceptibility and course — typically 10–14 days), ampicillin + gentamicin for Listeria (21 days). Therapy is guided by CSF and blood cultures; adjust with your microbiologist [3].
Dexamethasone is the adjunct that actually has trial evidence: 10 mg IV four times daily for 4 days, started with or before the first antibiotic dose, reduced death and unfavourable outcome in community bacterial meningitis — with the benefit concentrated in pneumococcal disease. Starting it after antibiotics have begun removes the rationale; if the organism turns out not to be bacterial, stop it [2].
When is CT required before LP? The Hasbun study gives the criteria: immunocompromise (HIV, transplant, immunosuppressive drugs), history of CNS disease, new seizure in the past week, papilloedema, abnormal level of consciousness, or focal neurological deficit. None of these → LP without CT is safe. Any one of them → CT first (after antibiotics) [4].
The CSF, interpreted
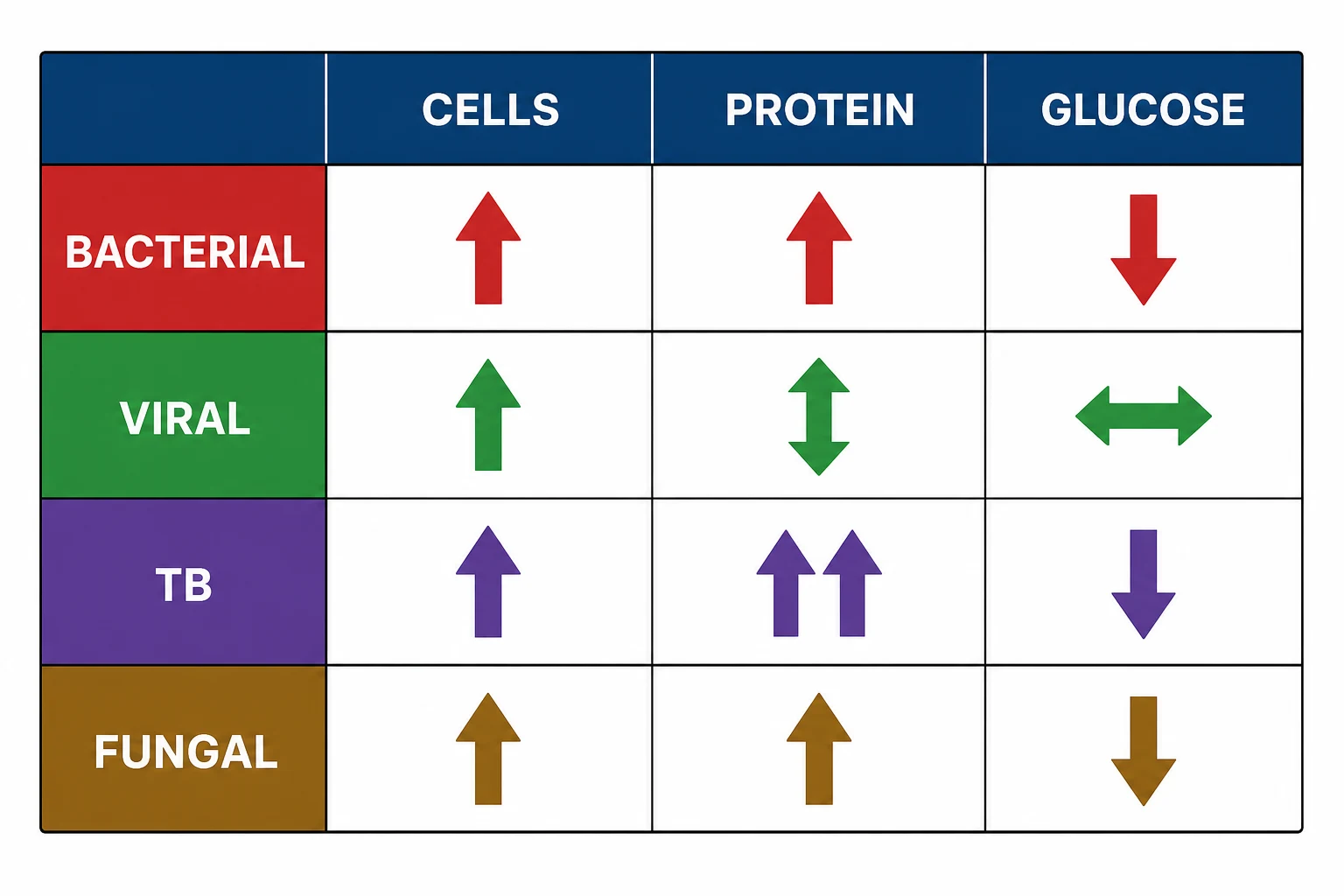
Learn the pattern, not just the numbers — examiners hand you a CSF and watch you reason [1]:
| Cells (dominant) | Protein | Glucose (CSF:serum) | Opening pressure | |
|---|---|---|---|---|
| Bacterial | High, neutrophils | High | Low (below ~0.4) | High |
| Viral | Mild, lymphocytes | Normal to mild rise | Normal | Normal |
| TB | Moderate, lymphocytes | Very high | Low | High [10] |
| Fungal (crypto) | Mild-moderate, lymphocytes (may be near-normal in HIV) | High | Low-normal | Very high [7] |
Three caveats that lose marks when forgotten: early bacterial meningitis can be lymphocyte-predominant; partially treated meningitis shifts toward a viral pattern while glucose stays low; and cryptococcus in advanced HIV can produce an almost normal CSF cell count because the host cannot mount inflammation — the opening pressure and the India ink/antigen test carry the diagnosis there [7].
Always send: cell count and differential, protein, glucose with a paired serum glucose, Gram stain and culture, and the PCR relevant to context (HSV when encephalitic, meningococcal/pneumococcal PCR when pre-treated, cryptococcal antigen when immunocompromised) [7].
Encephalitis — treat HSV before you prove it
HSV-1 encephalitis is the one sporadic encephalitis with effective therapy, so it owns the default position: every encephalopathic febrile patient gets empirical aciclovir 10 mg/kg IV three times daily (ideal body weight, renal-adjusted) while the workup proceeds. The vidarabine-versus-aciclovir trial established acyclovir as life-saving, and outcome tracks directly with how early it starts [5].
The diagnostic pattern to name aloud: temporal lobe disease — personality change, olfactory or gustatory hallucinations, dysphasia, complex partial seizures — with MRI FLAIR temporal hyperintensity (may be normal in the first 48 hours) and HSV PCR on the CSF. Treat for 14–21 days and repeat the PCR before stopping if suspicion is high: a negative early PCR does not exclude HSV, and premature cessation relapses [5].
Brain abscess — focal, not diffuse
A brain abscess announces itself like a tumour that runs a fever: subacute headache, focal deficit, sometimes seizures, with fever present in only about half. Sources matter for both organisms and management: contiguous spread (sinusitis → frontal lobe; otitis → temporal lobe/cerebellum; dental → frontal) and haematogenous spread (endocarditis, pulmonary infections, cyanotic congenital heart disease — often multiple, at the grey-white junction) [9].
Management has three legs: aspirate for diagnosis (culture and sterility — especially when the organism is unknown, the lesion is sizeable, or the capsule is thin), prolonged IV antibiotics (typically ceftriaxone + metronidazole to cover streptococci and anaerobes, then culture-directed, usually 6–8 weeks), and excision when the abscess is large, mass-effecting, posterior-fossa, or failing to shrink. Steroids only for significant oedema with mass effect — they impair antibiotic penetration and healing [9].
Cryptococcal meningitis in HIV — the pressure is the problem
In advanced HIV, cryptococcus presents indolently: days to weeks of headache, low-grade fever, sometimes little else. Two management facts dominate everything else. First, induction is amphotericin B plus flucytosine — the combination sterilises CSF faster than amphotericin alone; the ACTA trial then showed a single high-dose liposomal amphotericin (10 mg/kg) plus flucytosine and fluconazole is as effective and far less toxic than the week of daily amphotericin it replaced [7] [8].
Second, the opening pressure is a treatment target, not a number. Markedly elevated pressure causes blindness and death; management is serial therapeutic lumbar punctures draining to a normal closing pressure, repeated daily until controlled. This is the answer examiners want when they describe an HIV patient with headache and a CSF pressure you could not record because it overflowed the manometer [7].
ART timing is the third judgement: starting ART too early invites paradoxical IRIS that can be fatal in CNS crypto — defer roughly 4–6 weeks after antifungal initiation, and say that you coordinate this with the HIV team [7].
Meningococcaemia — the rash that outruns the meningitis
Meningococcal disease kills through sepsis more often than through meningitis. The teaching triad is fever, non-blanching purpuric rash (press a glass against it), and rapid deterioration — and the rash can be sparse or absent early. Meningococcaemia without meningitis produces a comparatively bland CSF while the patient is in septic shock; treat as sepsis with immediate ceftriaxone and ICU support, and do not wait for the LP [1].
Public health is part of the management, not an afterthought: meningococcal disease is notifiable, and close contacts (household, kissing, secretion exposure) receive chemoprophylaxis — ciprofloxacin or rifampicin per local guidance — with vaccination for the relevant serogroup in defined risk groups. State this explicitly in the exam; candidates lose marks by treating the patient and forgetting the contacts [3].
Complications and follow-up — where the long case lives
Surviving bacterial meningitis is not the end of the admission. Look for and name the complications: cerebral oedema and herniation (early deaths), seizures, SIADH (fluid management nuance), hydrocephalus, and the signature late complication — sensorineural hearing loss, which is common enough that audiology before or soon after discharge is standard of care. Follow-up also asks why this patient: complement deficiency in recurrent meningococcal disease, asplenia (functional or surgical) in pneumococcal disease — and vaccinates accordingly (pneumococcal, meningococcal, Hib, influenza) [1] [3].
For TB meningitis, remember the steroid parallel: dexamethasone tapered over 6–8 weeks reduces death in tuberculous meningitis, analogous to but distinct from the 4-day bacterial course [10].
Exam traps, collected
References
- [1]van de Beek D, de Gans J, Tunkel AR, Wijdicks EF. Community-acquired bacterial meningitis in adults N Engl J Med, 2006.PMID 16394301
- [2]de Gans J, van de Beek D; European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis N Engl J Med, 2002.PMID 12432041
- [3]Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis Clin Infect Dis, 2004.PMID 15494903
- [4]Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before lumbar puncture in adults with suspected meningitis N Engl J Med, 2001.PMID 11742046
- [5]Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis N Engl J Med, 1986.PMID 3001520
- [6]Dalmau J, Lancaster E, Martinez-Hernandez E, Rosenfeld MR, Balice-Gordon R. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis Lancet Neurol, 2011.PMID 21163445
- [7]Day JN, Chau TT, Wolbers M, et al. Combination antifungal therapy for cryptococcal meningitis N Engl J Med, 2013.PMID 23550668
- [8]Jarvis JN, Lawrence DS, Meya DB, et al. Single-Dose Liposomal Amphotericin B Treatment for Cryptococcal Meningitis N Engl J Med, 2022.PMID 35320642
- [9]Brouwer MC, Tunkel AR, McKhann GM 2nd, van de Beek D. Brain abscess N Engl J Med, 2014.PMID 25075836
- [10]Thwaites GE, Nguyen DB, Nguyen HD, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults N Engl J Med, 2004.PMID 15496623