Phys · infectious
Invasive and Mucocutaneous Fungal Infections
Also known as invasive candidiasis · candidaemia · invasive aspergillosis · cryptococcal meningitis · Pneumocystis pneumonia · PJP · PCP · mucormycosis · zygomycosis · rhinocerebral mucormycosis · histoplasmosis · coccidioidomycosis · Valley fever · blastomycosis · galactomannan · halo sign · echinocandin · voriconazole · amphotericin B · liposomal amphotericin
Consultant-physician-depth guide to fungal infections in the immunocompromised and critically ill host — the central principle that the type of immune defect predicts the fungus, with systematic coverage of candidiasis (mucocutaneous and invasive, including candidaemia risk factors, empiric echinocandin for the unstable patient, and mandatory line removal), invasive pulmonary aspergillosis (halo sign, galactomannan, voriconazole first-line and isavuconazole alternative), cryptococcal meningitis (amphotericin B plus flucytosine induction, fluconazole consolidation, and the manage-raised-ICP principle with serial LPs), the endemic mycoses (Histoplasma, Blastomyces, Coccidioides, Paracoccidioides, Talaromyces), Pneumocystis jirovecii pneumonia (CD4 below 200, co-trimoxazole, adjunctive steroids), and rhinocerebral mucormycosis (ketoacidosis, black necrotic eschar, amphotericin plus debridement) — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Invasive and Mucocutaneous Fungal Infections

The one-minute consultant answer
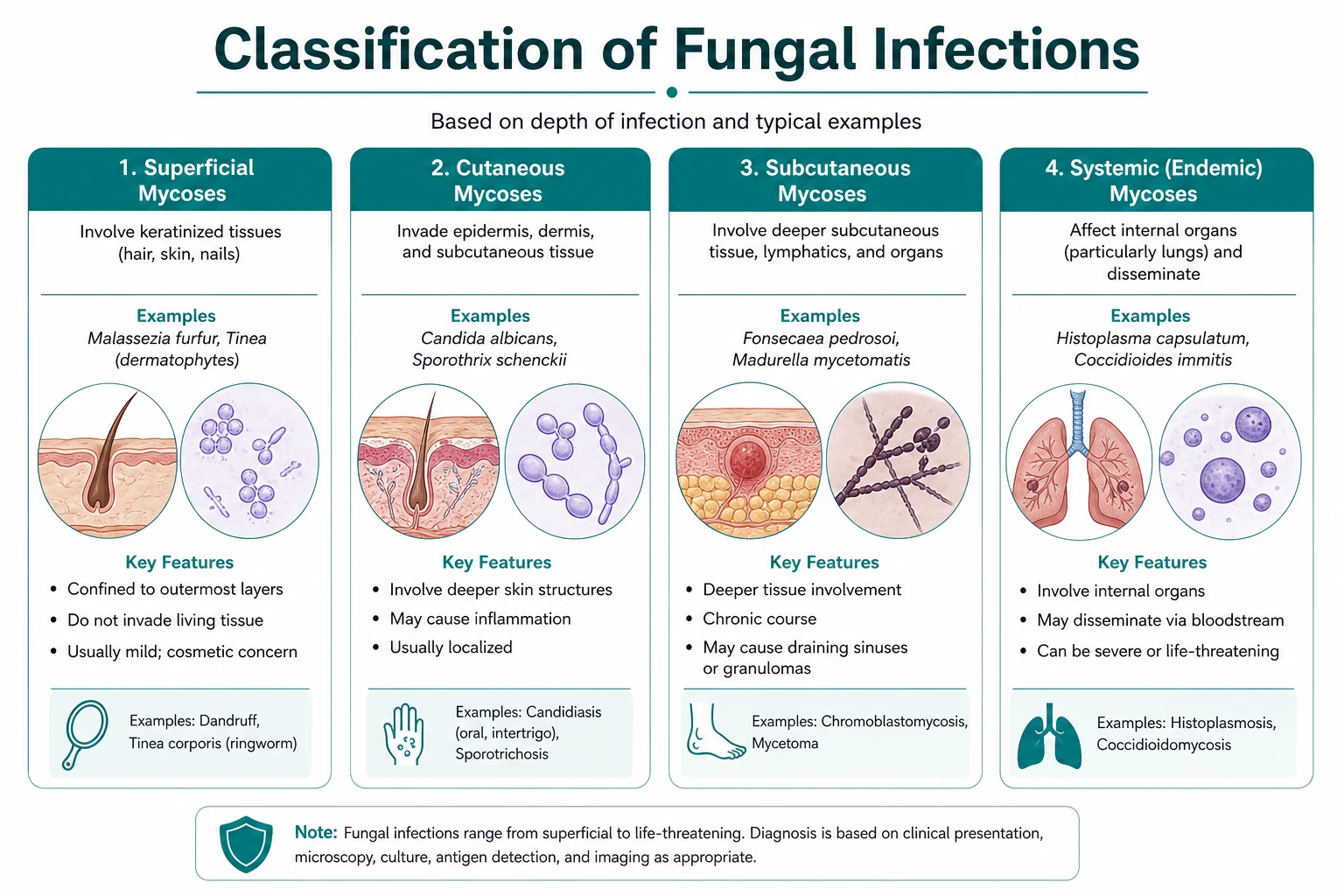
A fungal infection in the immunocompromised or critically ill patient is a different disease from a fungal infection in the normal host, because the type of immune defect predicts the organism, the diagnostic test, the empiric therapy, and the prophylaxis. The single most important question at the bedside is what is the type and depth of immunocompromise? — and the answer divides every patient into one of five categories that drive the rest of the encounter. [1]
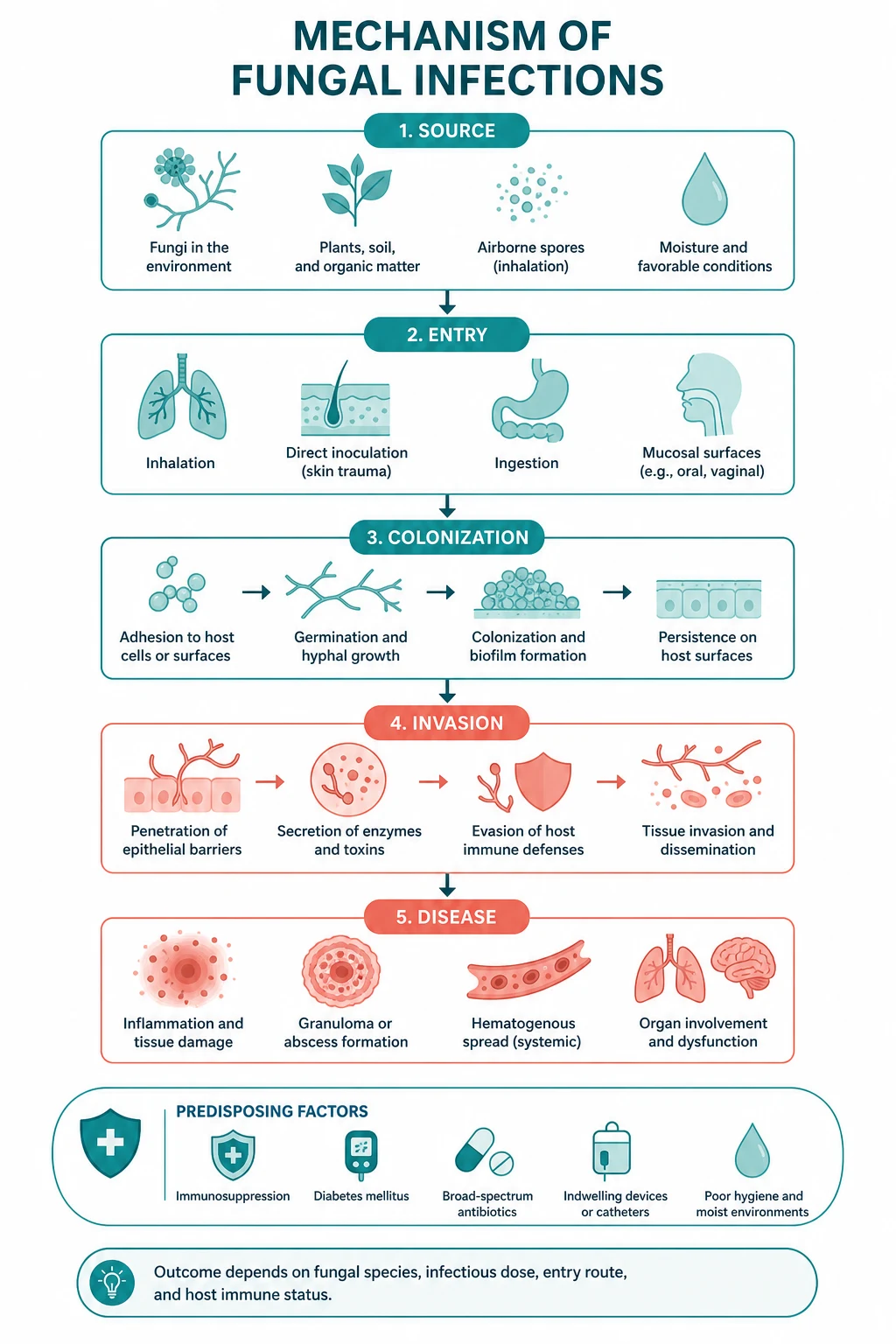
Prolonged neutropenia (post-chemotherapy, AML induction, above 10 to 14 days) opens the door to the angioinvasive moulds — Aspergillus and the Mucorales — because the neutrophil is the primary defence against hyphal organisms. Cellular immunodeficiency (HIV with CD4 below 100 to 200; transplant at 1 to 6 months) is the home of Cryptococcus, the endemic mycoses (Histoplasma, Coccidioides, Talaromyces), and Pneumocystis jirovecii. Broad-spectrum antibiotics, central venous catheters, total parenteral nutrition, and ICU stay together create the substrate for Candida, the most common healthcare-associated fungal pathogen. Diabetic ketoacidosis and iron overload uniquely predispose to Mucorales (Rhizopus), because the acidotic, ketotic, iron-rich environment is the one in which these organisms thrive. And severe immunosuppression with neutropenia or graft-versus-host disease is where mould-active prophylaxis (posaconazole, voriconazole) shifts the epidemiology and where breakthrough infection demands a different empiric approach. [1]
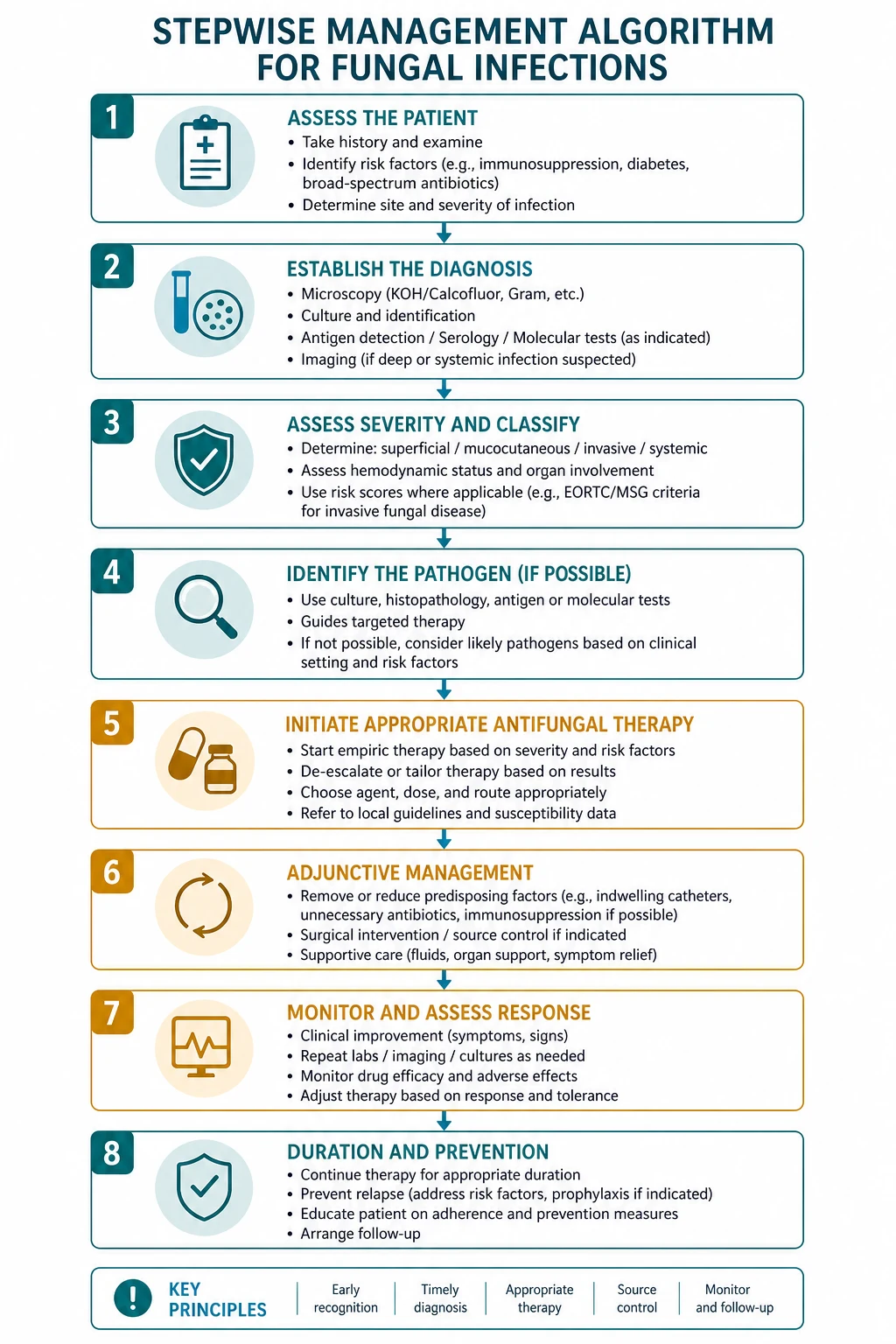
The non-negotiable principles: identify the host, image early, and treat on the basis of the most likely organism — never wait for definitive confirmation in a deteriorating patient. In candidaemia, the echinocandins (caspofungin, micafungin, anidulafungin) are first-line for the unstable or critically ill patient and the central line MUST be removed [1]. In invasive aspergillosis, voriconazole is first-line because the Herbrecht randomised trial showed a survival benefit over amphotericin B deoxycholate [4], and isavuconazole is a non-inferior alternative with a cleaner safety profile [5]. In cryptococcal meningitis the three-phase regimen (amphotericin B plus flucytosine induction, fluconazole consolidation and maintenance) is the framework, but the single most important determinant of early survival is management of raised intracranial pressure with serial therapeutic lumbar punctures [3]. In Pneumocystis pneumonia the treatment is high-dose co-trimoxazole with adjunctive corticosteroids when the PaO2 is below 60 mmHg or the A-a gradient is above 35 mmHg. In mucormycosis the answer is high-dose liposomal amphotericin B plus aggressive surgical debridement — voriconazole and the echinocandins are inactive, and delay is fatal [10].
The central framework — host immunity predicts the fungus

Every patient with suspected invasive fungal infection falls into one of the categories below. Each category has its own organism list, its own diagnostic test, and its own empiric therapy. The exam tests this framework directly — the stem will name the host, and the correct answer is the organism, the test, or the drug that matches it. [1]
| Host category | Characteristic fungi | Key diagnostic test | Empiric therapy |
|---|---|---|---|
| Prolonged neutropenia (post-chemo, AML induction, above 10 to 14 days) | Aspergillus, Mucorales, Candida | Chest CT (halo sign), serum galactomannan | Voriconazole or isavuconazole; add echinocandin if Candida plausible |
| Allogeneic HSCT, graft-versus-host disease | Aspergillus, Mucorales, Candida, Pneumocystis | Chest CT, galactomannan, BAL | Mould-active azole (posaconazole if on prophylaxis breakthrough) |
| Solid organ transplant at 1 to 6 months | Aspergillus, Cryptococcus, Pneumocystis, endemic mycoses | CT, galactomannan, CrAg, induced sputum | Voriconazole; co-trimoxazole for PJP |
| HIV, CD4 below 200 | Pneumocystis, Cryptococcus, Talaromyces, Histoplasma, Coccidioides | CXR/CT, A-a gradient, CrAg, BAL | Co-trimoxazole (PJP); amphotericin plus flucytosine (Cryptococcus) |
| ICU, central line, broad-spectrum antibiotics, TPN | Candida (C. albicans, C. glabrata, C. parapsilosis, C. krusei) | Blood cultures, beta-D-glucan, T2 Candida, fundoscopy | Echinocandin for unstable; fluconazole for stable, no prior azole |
| Diabetic ketoacidosis, iron overload, deferoxamine | Mucorales (Rhizopus, Mucor, Rhizomucor) | Sinus and cerebral CT, tissue biopsy with broad non-septate hyphae | Liposomal amphotericin B 5 to 10 mg/kg/day plus urgent surgical debridement |
| Corticosteroids above 20 mg for more than 4 weeks | Pneumocystis, Candida, Aspergillus, endemic mycoses | Induced sputum or BAL for PJP; chest CT | Co-trimoxazole for suspected PJP |
The exam trap: the question stem will name the host and the risk factor — the correct answer is the organism, the test, or the drug that the host predicts. A neutropenic-and-persistent-fever vignette expects a chest CT, a galactomannan, and a mould-active azole; a DKA-and-facial-pain vignette expects liposomal amphotericin and an ENT surgeon; an ICU-and-central-line vignette expects an echinocandin and line removal. [1]
Candidiasis — from oral thrush to candidaemia

Candida species are the most common cause of fungal infection in hospital practice, and the spectrum runs from trivial mucocutaneous disease to life-threatening disseminated infection. The depth of invasion determines the urgency and the drug. [1]
Mucocutaneous candidiasis — recognising and treating the surface forms
Oral thrush (oropharyngeal candidiasis) presents with white, curdy, adherent plaques on the buccal mucosa, tongue, and palate that scrape off to leave a bleeding erythematous base. It is common in neonates, inhaled corticosteroid users (counsel to rinse and spit after the inhaler), denture wearers, and the immunocompromised (HIV, chemotherapy, broad-spectrum antibiotics). The treatment is topical — oral nystatin suspension or clotrimazole troches — or a short course of oral fluconazole 50 to 100 mg daily for 7 to 14 days for extensive or refractory disease. New-onset thrush in an adult without an obvious cause prompts an HIV test. [1]
Oesophageal candidiasis presents with odynophagia, dysphagia, and retrosternal discomfort, often (but not always) with concurrent oral thrush. The clinical pearl is that oesophageal symptoms in an HIV-positive or neutropenic patient are treated empirically with fluconazole without endoscopy, because the most common cause is Candida and it responds rapidly. Endoscopy is reserved for refractory disease (to distinguish CMV and HSV oesophagitis, which coexist and require different therapy). The treatment is fluconazole 200 to 400 mg daily for 14 to 21 days; an echinocandin or amphotericin is used for refractory or azole-resistant disease. [1]
Vulvovaginal candidiasis presents with pruritus, burning, and a thick white discharge. It is extremely common, usually uncomplicated, and treated with topical azoles (clotrimazole, miconazole) or a single oral dose of fluconazole 150 mg. Complicated vulvovaginal candidiasis (severe symptoms, recurrent above four episodes per year, pregnancy, uncontrolled diabetes, non-albicans species) requires longer or alternative therapy — fluconazole 150 mg every 72 hours for two or three doses, and maintenance weekly for six months in recurrent disease. [1]
Chronic mucocutaneous candidiasis is a syndrome of persistent, recurrent mucocutaneous Candida infection of skin, nails, and mucosa from childhood onward, caused by a T-cell defect (IL-17 or STAT1 pathway). It is rare but important because it signals an underlying immune defect that may also predispose to endocrine autoimmunity (AIRE gene, autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy, APECED). [1]
Invasive candidiasis and candidaemia — the ICU and line-related pathogen
Candidaemia is the presence of Candida in the bloodstream. It is the fourth most common cause of nosocomial bloodstream infection in many ICUs, and it carries an attributable mortality of 15 to 25 per cent. The risk factors are the list every registrar should know by heart: central venous catheter, total parenteral nutrition, broad-spectrum antibiotics, neutropenia, haemodialysis, major abdominal surgery (especially with gastrointestinal perforation or anastomotic leak), prolonged ICU stay, and parenteral nutrition in a neonate. The IDSA candidiasis guideline frames the empiric treatment decision on the clinical stability and the prior exposure to azoles [1].
The empiric treatment decision in candidaemia: [1]
- Stable, non-neutropenic, no prior azole exposure, and in a unit where C. glabrata and C. krusei are uncommon: fluconazole 800 mg loading then 400 mg daily is acceptable. The Candida species must be identified and the susceptibility checked, because C. glabrata is often fluconazole-resistant and C. krusei is intrinsically resistant.
- Unstable (septic shock, ICU), neutropenic, recent azole exposure, or in a unit with significant C. glabrata or C. krusei prevalence: an echinocandin — caspofungin 70 mg loading then 50 mg daily, micafungin 100 mg daily, or anidulafungin 200 mg loading then 100 mg daily — is first-line. The Reboli randomised trial of anidulafungin versus fluconazole showed a higher response rate for anidulafungin, particularly in the more severely ill [7]. The echinocandins are fungicidal against Candida (the azoles are fungistatic), they cover C. glabrata and C. krusei, and they have a clean safety profile with minimal drug interactions.
- Step-down therapy: once the patient has clinically improved, the Candida species is identified and susceptible, and repeat blood cultures are negative, step down to oral fluconazole or voriconazole (the latter for C. krusei) to complete the course.
Source control is non-negotiable: the central venous catheter must be removed. The IDSA guideline is explicit — catheter removal is strongly recommended in non-neutropenic patients with candidaemia, because the catheter is the source or a reservoir in the majority, and leaving it in prolonges bacteraemia/fungaemia and increases metastatic seeding [1]. The duration of therapy is 14 days from the first negative blood culture, provided there is no metastatic focus (endophthalmitis, endocarditis, osteomyelitis, hepatosplenic disease) and the patient has clinically responded.
The dilated fundoscopy is mandatory in every patient with candidaemia. Candidal endophthalmitis — white, fluffy chorioretinal lesions with vitritis — is present in up to 15 per cent of patients with candidaemia, can be sight-threatening, and changes management: prolonged therapy (4 to 6 weeks minimum), intravitreal amphotericin or echinocandin, and vitrectomy in severe disease. Every candidaemic patient gets a dilated fundoscopy by an ophthalmologist within the first week; missing it is a recognised cause of preventable visual loss and a favourite exam discriminator. [1]
Chronic disseminated candidiasis (hepatosplenic candidiasis) presents during neutrophil recovery after intensive chemotherapy, as the returning neutrophils react to Candida that seeded the liver and spleen during the neutropenic episode. The classic presentation is persistent fever, right upper quadrant pain, and raised alkaline phosphatase during neutrophil recovery, with CT showing multiple low-attenuation lesions in the liver and spleen. The treatment is prolonged fluconazole or an echinocandin until the lesions resolve (often months), and it is one of the few situations where amphotericin B is no longer preferred. [1]
The Candida species that matter:
- C. albicans — still the most common overall; usually fluconazole-susceptible.
- C. glabrata — increasing in prevalence, especially in older adults and those with prior azole exposure; often fluconazole-resistant; treat with an echinocandin, step down to high-dose fluconazole or voriconazole only if susceptible.
- C. parapsilosis — associated with central lines and parenteral nutrition; less virulent but has reduced echinocandin susceptibility in some regions — fluconazole may be preferred if susceptible.
- C. krusei — intrinsically fluconazole-resistant; treat with an echinocandin or amphotericin; step down to voriconazole.
- C. auris — the emerging, often multidrug-resistant nosocomial pathogen that colonises skin and survives on surfaces, causes outbreaks in ICUs, and demands strict infection control. Identify it promptly and involve infection control and public health. [1]
Invasive aspergillosis — the mould of prolonged neutropenia and transplant

Invasive pulmonary aspergillosis is the feared complication of prolonged neutropenia (classically above 10 to 14 days) and of allogeneic HSCT, particularly with graft-versus-host disease and high-dose corticosteroids. Aspergillus (predominantly A. fumigatus) is an angioinvasive mould: it invades pulmonary vessels, causing thrombosis, infarction, and haemorrhage, and the pathophysiology explains the clinical, radiological, and prognostic features. [1]
The presentation — and why it is missed
The clinical presentation is fever, dry cough, pleuritic chest pain, and haemoptysis, often with fever that has persisted beyond 3 to 5 days of broad-spectrum antibacterials. The trap is that the chest X-ray is often normal or near-normal early — the radiological findings lag behind the clinical disease. Any neutropenic or transplant patient with persistent fever, new respiratory symptoms, or a new pulmonary nodule on imaging has invasive aspergillosis until proven otherwise, and the test that finds it is the high-resolution chest CT, not the chest X-ray. [1]
The CT signs — halo and air-crescent
The two radiological signs of angioinvasive aspergillosis are time-dependent and reflect the underlying pathology: [1]
- The halo sign — a pulmonary nodule surrounded by a ground-glass halo of surrounding haemorrhage — appears early, within the first week, and is the most sensitive early finding. It reflects haemorrhagic infarction around a focus of angioinvasive fungal growth.
- The air-crescent sign — a crescent of air surrounding a sequestered area of necrotic lung — appears later, typically 2 to 3 weeks in, and corresponds to neutrophil recovery and separation of the necrotic core from the surrounding viable parenchyma. Its appearance is a sign of ** marrow recovery and a somewhat better prognosis**, but it is not the early finding you are looking for. [1]
The critical differential is mucormycosis, which can produce a reverse halo sign (the atoll sign) — a focal rounded area of ground-glass opacity surrounded by a ring of consolidation. The reverse halo, especially with multiple lesions and rapid progression and sinus involvement, should raise the concern of Mucorales rather than Aspergillus, and the antifungal must change accordingly. [1]
Diagnosis — galactomannan, beta-D-glucan, and biopsy
Diagnosis combines imaging, antigen detection, and histopathology. The serum galactomannan assay detects an Aspergillus cell-wall polysaccharide released during hyphal growth; a single positive (optical density index above 0.5) or two consecutive positives support invasive disease, and serial monitoring improves sensitivity. The sensitivity is highest in neutropenia and HSCT (above 70 per cent) and much lower in solid organ transplant and in patients on mould-active prophylaxis (because prophylaxis suppresses antigen release). False positives occur with piperacillin-tazobactam (historically, though no longer with current formulations in most regions), Plasma-Lyte and other fluids containing gluconate, and some foods. The bronchoalveolar lavage galactomannan is more sensitive than serum in the non-neutropenic patient and is the test to send when bronchoscopy is performed. [1]
Serum (1,3)-beta-D-glucan is a broad fungal marker (positive in Candida, Aspergillus, and Pneumocystis, but not Cryptococcus or Mucorales) and is supportive but not specific — it is a rule-in adjunct, not a standalone diagnostic. False positives occur with haemodialysis, immunoglobulin, and certain surgical gauze. [1]
The gold standard is tissue diagnosis — percutaneous or bronchoscopic biopsy showing septate hyphae branching at acute angles with tissue invasion, and culture confirming Aspergillus. Biopsy is not always feasible in thrombocytopenic or critically ill patients, which is why the EORTC/MSG criteria allow a probable diagnosis on the basis of a host factor (neutropenia, transplant, steroids) plus a clinical feature (imaging) plus a mycological evidence (galactomannan). [1]
Treatment — voriconazole first-line, isavuconazole alternative
The treatment of invasive pulmonary aspergillosis is voriconazole as first-line therapy. The Herbrecht randomised trial established this in 2002: voriconazole versus amphotericin B deoxycholate for primary therapy showed a higher response rate (52.8 per cent vs 31.6 per cent) and a survival benefit (70.8 per cent vs 57.9 per cent at 12 weeks) for voriconazole [4]. Voriconazole is loaded at 6 mg/kg every 12 hours for two doses, then 4 mg/kg every 12 hours intravenously, transitioning to oral 200 to 300 mg every 12 hours once the patient can absorb (excellent oral bioavailability above 90 per cent). It requires therapeutic drug monitoring (target trough 1 to 5.5 mg/L) because of its nonlinear pharmacokinetics, CYP2C19 polymorphism, and wide inter-patient variability; both subtherapeutic (treatment failure) and supratherapeutic (hepatotoxicity, encephalopathy, visual disturbance) levels are common. The visual disturbance — transient bright lights, altered colour perception — is characteristic, common (above 20 per cent), usually reversible, and important to counsel about.
Isavuconazole is a non-inferior alternative, established by the SECURE randomised non-inferiority trial of isavuconazole versus voriconazole for invasive mould disease [5]. It has a cleaner safety profile (fewer visual and hepatotoxic adverse events, fewer drug interactions), predictable linear pharmacokinetics that do not require routine therapeutic drug monitoring, a loading dose built into the first 48 hours (200 mg every 8 hours for six doses, then 200 mg daily), and — uniquely among the triazoles — it shortens the QT interval rather than prolonging it, which is a potential advantage in patients on QT-prolonging polypharmacy. The trade-off is cost and that the mortality non-inferiority was met but not surpassed.
Liposomal amphotericin B (3 to 5 mg/kg/day) is an alternative for patients who cannot tolerate or fail a triazole, and it has a role in pregnancy (voriconazole is teratogenic). Combination therapy (triazole plus echinocandin) is sometimes used in refractory disease but is not routine first-line. [1]
Reduce the immunosuppression where possible. The single most important adjunct to antifungal therapy is immune recovery — reducing steroids, tapering calcineurin inhibitors where the transplant team permits, and supporting neutrophil recovery with G-CSF in selected patients. In haematology, recovery of the neutrophil count is the strongest predictor of survival from invasive aspergillosis. [1]
Treatment duration is a minimum of 6 to 12 weeks, guided by clinical and radiological response, galactomannan clearance, and immune reconstitution. Secondary prophylaxis with a mould-active azole continues through subsequent chemotherapy cycles and through HSCT. [1]
Chronic and allergic forms of aspergillosis
Not all Aspergillus disease is invasive. Allergic bronchopulmonary aspergillosis (ABPA) is a hypersensitivity reaction to colonising Aspergillus in patients with asthma or cystic fibrosis, presenting with wheeze, eosinophilia, raised IgE (above 1000 IU/mL), and proximal bronchiectasis; treat with corticosteroids and an antifungal (itraconazole or voriconazole) to reduce the fungal burden. Aspergilloma (fungal ball) is a saprophytic colony in a pre-existing cavity (often old TB), presenting with haemoptysis; treat with surgical resection for significant haemoptysis, sometimes with antifungals or bronchial artery embolisation as a bridge. Chronic pulmonary aspergillosis is a slowly progressive cavitary infection in patients with underlying lung disease, treated with prolonged oral triazole therapy. [1]
Cryptococcosis — the manage-raised-ICP principle
Cryptococcus neoformans is an encapsulated yeast acquired by inhalation from soil contaminated with pigeon droppings. It causes disease almost exclusively in the setting of cellular immunodeficiency — HIV with CD4 below 100, solid organ transplant, idiopathic CD4 lymphopenia, and high-dose corticosteroids — though C. gattii (found in tropical and subtropical regions, including parts of Australia and the Pacific Northwest) causes disease in apparently immunocompetent hosts. [1]
Cryptococcal meningitis — the indolent presentation
Cryptococcal meningitis presents with subacute onset of headache, fever, malaise, and altered mental state over days to weeks. The classic teaching is that the onset is indolent and the patient looks better than the CSF suggests — the inflammatory response is often muted in the immunocompromised host. Raised intracranial pressure is the single most important determinant of early mortality: the cryptococcal capsule and the fungal burden obstruct CSF outflow at the arachnoid villi, producing a markedly raised opening pressure that causes headache, vomiting, reduced consciousness, cranial nerve palsies (especially VI), and blindness from optic nerve compression. Skin lesions (molluscum-like papules, cellulitis, ulcers) and pulmonary involvement may accompany the meningitis and are a clue to disseminated disease. [1]
The CSF — India ink, CrAg, and opening pressure
The diagnostic lumbar puncture in cryptococcal meningitis yields several key results:
- Opening pressure — measure it and record it. It is elevated (above 25 cm of water) in the majority of HIV-positive patients with cryptococcal meningitis, and it dictates management.
- CSF India ink — visualises the yeast capsule as a clear halo against the ink; sensitivity is 60 to 80 per cent in HIV (high fungal burden) and lower in non-HIV.
- CSF and serum cryptococcal antigen (CrAg) — above 95 per cent sensitive; a positive serum CrAg in the right host is sufficient to treat empirically. The serum CrAg titre is useful for diagnosis and for monitoring (a rising titre suggests relapse).
- CSF culture — grows the organism, confirms the diagnosis, and allows susceptibility testing.
- CSF cell count, glucose, and protein — often show a lymphocytic pleocytosis with low glucose and elevated protein, but in profound immunosuppression the cell count may be deceptively low. [1]
Treatment — the three-phase regimen and the AMBITION and ACTA evidence
The IDSA 2010 guideline established the three-phase regimen for cryptococcal meningitis [3], and the AMBITION-cm and ACTA trials have refined and simplified it [6], [8].
Induction (at least 2 weeks):
- Liposomal amphotericin B 3 to 4 mg/kg/day intravenously PLUS flucytosine 25 mg/kg orally every 6 hours (100 mg/kg/day). The addition of flucytosine to amphotericin B sterilises the CSF faster and improves survival; flucytosine is never used alone (rapid resistance emergence) and requires renal dose adjustment and blood level monitoring (keep the 2-hour post-dose level below 100 mg/L to avoid bone-marrow suppression).
- The AMBITION-cm trial (2022) demonstrated that a single high-dose liposomal amphotericin B 10 mg/kg on day 1, combined with 14 days of flucytosine and fluconazole (1200 mg/day), was non-inferior to the standard 7-day amphotericin B deoxycholate plus flucytosine regimen for HIV-associated cryptococcal meningitis, with fewer adverse events [6]. This regimen is now endorsed by WHO and is transforming induction in resource-limited settings.
- The ACTA trial (2018) showed that 1 week of amphotericin B plus flucytosine was as effective as 2 weeks, and that fluconazole plus flucytosine was a reasonable oral alternative to amphotericin-based induction [8].
Consolidation (at least 8 weeks):
- Fluconazole 400 to 800 mg/day orally (or 12 mg/kg/day), after a successful induction, until CSF cultures are negative. [1]
Maintenance (until immune restoration):
- Fluconazole 200 mg/day until immune reconstitution. In HIV, this is until the CD4 is above 100 to 200 for at least 6 months on antiretroviral therapy; in transplant, it is typically for 6 to 12 months after the completion of consolidation, individualised to the level of immunosuppression. [1]
The single most important principle in cryptococcal meningitis is the management of raised intracranial pressure. The IDSA guideline is explicit: if the opening pressure is above 25 cm of water, perform daily therapeutic lumbar punctures to drain CSF and reduce the pressure to below 20 cm of water (or by 50 per cent). A ventricular shunt is placed if the pressure cannot be controlled by serial LPs. Acetazolamide, mannitol, and corticosteroids have no role in managing cryptococcal raised ICP — mannitol and acetazolamide were shown not to help, and corticosteroids worsen outcomes in HIV-associated cryptococcal meningitis. Raised ICP, not the choice of antifungal, is the single biggest determinant of early mortality. [1]
Immune reconstitution inflammatory syndrome (IRIS) is a paradoxical clinical worsening that occurs when immune function recovers — typically 1 to 6 weeks after starting antiretrovirals (in HIV) or reducing immunosuppression (in transplant). The management is to continue the antifungal and the antiretroviral, exclude progressive infection or drug resistance, and use corticosteroids only for severe or life-threatening IRIS (such as cerebral oedema with mass effect). The diagnosis is one of exclusion — rule out treatment failure first. [1]
Endemic mycoses — geography and exposure predict the organism
The endemic mycoses are dimorphic fungi — they grow as moulds in the environment (at ambient temperature) and as yeasts in tissue (at body temperature) — and each has a characteristic geographic distribution that predicts the diagnosis from the travel history alone. They are under-recognised causes of pneumonia, disseminated infection, and meningitis in the immunocompromised and the returned traveller. [1]
Histoplasma capsulatum is endemic to the Mississippi and Ohio River valleys of the United States and to parts of Central and South America. The environmental reservoir is soil enriched by bat guano and bird droppings (chickens, starlings, blackbirds); outbreaks follow cave exploration, demolition, and farming. Most infections are asymptomatic or a self-limited flu-like pneumonia. Acute pulmonary histoplasmosis presents with fever, cough, and hilar lymphadenopathy; chronic cavitary histoplasmosis mimics TB in older adults with emphysema; and disseminated histoplasmosis (in HIV with low CD4, transplant, steroids) presents with fever, hepatosplenomegaly, pancytopenia, mucocutaneous ulcers, and adrenal involvement (Addisonian crisis). Diagnosis is by urine and serum Histoplasma antigen (most sensitive in disseminated disease), serology (complement fixation and immunodiffusion), and culture. Treatment of moderate to severe disease is liposomal amphotericin B then itraconazole for 12 months (longer in immunocompromised). An important ANZ pearl: disseminated histoplasmosis in a returning traveller is a great mimicker — the pancytopenia and hepatosplenomegaly can mimic visceral leishmaniasis, miliary TB, or lymphoma. [1]
Blastomyces is endemic to the Mississippi and Ohio River valleys, the Great Lakes, and the St Lawrence Seaway, and is associated with moist soil and decaying wood. It causes pulmonary infection (often with verrucous or ulcerative skin lesions — a helpful discriminator), osteomyelitis, and disseminated disease. Treatment is itraconazole for mild to moderate; amphotericin for severe or disseminated. [1]
Coccidioides (causing Valley fever) is endemic to the desert south-western United States (San Joaquin Valley, Arizona, New Mexico, West Texas) and to parts of Mexico and Central and South America. The environmental reservoir is arid soil; infection follows dust exposure (construction, farming, dust storms). Most infections are asymptomatic or a self-limited pneumonia with erythema nodosum. Disseminated disease (skin, bone, joints, meningitis) occurs in the immunocompromised, in pregnancy, and in those of Filipino or African ancestry (genetic susceptibility). Coccidioidal meningitis is a chronic basilar meningitis that requires lifelong oral triazole therapy (fluconazole) because it relapses when stopped — one of the few fungal infections with a lifelong maintenance requirement. [1]
Paracoccidioides is endemic to Latin America (Brazil, Colombia, Venezuela, Argentina) and is acquired by inhalation of soil. It causes chronic pulmonary disease and mucocutaneous (mulberry-like ulcerative) lesions, more often in men. The classic histopathology is the mariner's wheel (pilot wheel) — multiple daughter buds around a central mother cell. Treatment is itraconazole or sulfamethoxazole-trimethoprim for prolonged courses. [1]
Talaromyces (Penicillium) marneffei is endemic to South-East Asia (Thailand, Vietnam, southern China, Myanmar) and southern Taiwan and is the third most common opportunistic infection in advanced HIV in this region (after TB and cryptococcosis). The classic presentation is fever, weight loss, anaemia, and a generalised papular skin eruption with central umbilication (mimicking molluscum contagiosum) in an HIV-positive patient from or travelling in the region. Diagnosis is by culture, microscopy of skin scrapings or bone marrow aspirate (dividing yeast cells by septation), and antigen testing. Treatment is amphotericin B induction then itraconazole consolidation and maintenance. This is a critical differential for the returned immunocompromised traveller from South-East Asia. [1]
Pneumocystis jirovecii pneumonia (PJP) — hypoxia disproportionate to the radiology
Pneumocystis jirovecii (formerly Pneumocystis carinii, hence the older abbreviation PCP) is a fungus that behaves like an opportunistic protozoon and causes a life-threatening pneumonia in the setting of cellular immunodeficiency. The risk categories are:
- HIV with CD4 below 200 (or a CD4 percentage below 14, or a history of oropharyngeal candidiasis, or unexplained fever above 2 weeks) — PJP is the most common AIDS-defining opportunistic infection in many settings.
- Solid organ or haematopoietic transplant — especially in the first 6 months or with augmented immunosuppression for rejection or graft-versus-host disease.
- Corticosteroid therapy above 20 mg prednisolone equivalent for more than 4 weeks — the classic non-HIV setting.
- Other T-cell depleting therapies — anti-CD52 (alemtuzumab), anti-TNF, purine analogues (fludarabine, cladribine), and malignancies with cell-mediated immune defects (Hodgkin lymphoma). [1]
The presentation — and why it is missed
The presentation in HIV is classically insidious over days to weeks — a dry cough, exertional dyspnoea, low-grade fever, and malaise. The cardinal feature is hypoxia disproportionate to the chest X-ray — the patient is breathless and desaturating on exertion, but the CXR may show only subtle bilateral perihilar interstitial infiltrates or look near-normal. The A-a gradient is markedly elevated (above 35 mmHg, often much higher), reflecting impaired gas transfer from the foamy alveolar exudate. The non-HIV PJP presentation is often more acute (over days) and more inflammatory, because the neutrophil response is preserved. [1]
The CXR in established disease shows bilateral, symmetrical, perihilar, interstitial infiltrates progressing to alveolar consolidation, often with pneumothorax or pneumatocele formation (cystic changes). Pneumothorax in an HIV-positive patient is PJP until proven otherwise. The chest CT is more sensitive and shows the classic ground-glass attenuation pattern. [1]
Diagnosis — induced sputum or BAL with immunofluorescence or PCR
The diagnosis is confirmed by identifying the organism in respiratory secretions. Induced sputum (after nebulised hypertonic saline, collected by a physiotherapist) is the least invasive test and is reasonably sensitive in HIV (high organism burden). Bronchoalveolar lavage is more sensitive and is the test of choice if induced sputum is negative or unavailable, or in non-HIV PJP (lower organism burden, higher yield from BAL). Immunofluorescent monoclonal antibody staining (which visualises the cysts) and PCR are the most sensitive laboratory methods; silver stain and toluidine blue O are older alternatives. Serum (1,3)-beta-D-glucan is elevated in PJP and is a supportive marker (it is not specific — it is also positive in Candida and Aspergillus); serum LDH is characteristically elevated. Empiric therapy on the basis of a compatible clinical and radiological picture is reasonable when the patient is too unstable for bronchoscopy — the bronchoscopy can be done once the patient stabilises. [1]
Treatment — co-trimoxazole and adjunctive steroids
Co-trimoxazole (trimethoprim-sulfamethoxazole) is the treatment of choice for PJP of any severity. The regimen for moderate to severe disease is 15 to 20 mg/kg/day of the trimethoprim component in divided doses every 6 to 8 hours intravenously for 21 days (for a 70 kg adult: 4 to 5 double-strength 960 mg tablets orally four times daily for mild disease, or intravenous for severe). The treatment course is 21 days, longer than most pneumonias because the organism clears slowly. [1]
Adjunctive corticosteroids are indicated when the PJP is moderate to severe — defined as a room air PaO2 below 60 mmHg (below 70 mmHg by some guidelines) or an A-a oxygen gradient above 35 mmHg. A Cochrane review confirmed that adjunctive corticosteroids reduce mortality in HIV-associated PJP with moderate to severe disease [9]. The steroid must be started within 72 hours of the first dose of co-trimoxazole to obtain the benefit. The classic regimen is prednisolone 40 mg twice daily for 5 days, then 40 mg daily for 5 days, then 20 mg daily for 11 days (or an equivalent hydrocortisone or methylprednisolone IV regimen). The mechanism is suppression of the inflammatory response to the organisms killed by co-trimoxazole — early in treatment, the dying organisms provoke a brisk alveolitis that worsens gas exchange.
Alternatives for sulfa-allergic or treatment-failing patients:
- Primaquine plus clindamycin — the most effective alternative for moderate to severe disease.
- Atovaquone — oral, for mild to moderate disease only.
- Pentamidine isethionate — intravenous, for severe disease; significant adverse effects (pancreatitis, nephrotoxicity, hypoglycaemia, hyperglycaemia, arrhythmia). Inhaled pentamidine is used only for prophylaxis, not treatment.
- Trimetrexate — a dihydrofolate reductase inhibitor, used historically for salvage. [1]
If the patient deteriorates despite 5 to 7 days of co-trimoxazole, switch to primaquine plus clindamycin and reassess — treatment failure in HIV usually reflects severe disease rather than resistant organism, and adjunctive steroids should be reviewed. [1]
Prophylaxis. Co-trimoxazole 960 mg daily (or three times weekly) is the prophylactic regimen of choice for HIV (CD4 below 200), for transplant recipients (at least 6 months post-SOT, longer in lung and small bowel, 6 months post-engraftment for HSCT), and during high-dose corticosteroids (above 20 mg prednisolone for more than 4 weeks). Dapsone, atovaquone, and inhaled pentamidine are alternatives for the sulfa-allergic or G6PD-deficient (dapsone is contraindicated in G6PD deficiency). [1]
Mucormycosis — the emergency of ketoacidosis and immunosuppression
Mucormycosis (formerly zygomycosis) is an aggressive, angioinvasive infection caused by the Mucorales — Rhizopus, Mucor, Rhizomucor, Cunninghamella, Apophysomyces, and Lichtheimia. The pathophysiology is rapid angioinvasion with vascular thrombosis, tissue infarction, and necrosis — and it progresses to death within days if untreated. The mortality is above 50 per cent despite optimal therapy, and delay is the single greatest predictor of death. [1]
The risk factors — and why they matter
The risk categories for mucormycosis are distinct from aspergillosis and reflect the unique biology of Mucorales:
- Diabetic ketoacidosis or poorly controlled diabetes — the single most common risk factor globally. The acidotic, ketotic environment disables transferrin's iron-sequestration function, liberating free iron that the organism uses for rapid growth; ketone bodies are a preferred carbon source. The COVID-19 pandemic saw a surge of COVID-associated mucormycosis (CAM), particularly in India, driven by the combination of diabetic ketoacidosis and high-dose corticosteroids for COVID pneumonia.
- Haematological malignancy, neutropenia, and graft-versus-host disease after HSCT.
- Solid organ transplant — particularly with high-dose steroids for rejection.
- Iron overload and deferoxamine (desferrioxamine) chelation therapy — deferoxamine acts as a siderophore for the Mucorales, paradoxically enhancing their growth; the newer chelators (deferasirox) do not carry this risk.
- Injection drug use — a distinct route for disseminated disease.
- Prolonged corticosteroid therapy and severe immunosuppression. [1]
A critical exam point: prior voriconazole or echinocandin exposure is a risk factor for mucormycosis, because these agents have no activity against Mucorales and so select for it — breakthrough mould infection on voriconazole prophylaxis in a high-risk host is mucormycosis until proven otherwise. [1]
Rhinocerebral mucormycosis — the surgical emergency
The most dramatic presentation is rhinocerebral mucormycosis — the angioinvasive infection that begins in the paranasal sinuses, spreads to the orbit, and invades the brain via the cavernous sinus and internal carotid artery. The presentation in a diabetic ketoacidotic patient is facial or sinus pain, nasal congestion, black or blood-tinged nasal discharge, fever, and swelling of the eyelid. The pathognomonic sign is the black necrotic eschar on the palate, turbinate, or nasal mucosa — tissue infarction made visible at the mucosal surface. Cranial nerve palsies (especially the abducens and oculomotor nerves from cavernous sinus involvement), visual loss, and reduced consciousness indicate intracranial extension and a grim prognosis. [1]
The diagnostic approach is urgent CT or MRI of the sinuses, orbits, and brain (showing sinus opacification, bony destruction, orbital cellulitis, cavernous sinus thrombosis, cerebral infarction), and urgent tissue biopsy with histopathology showing broad, non-septate (or sparsely septate), ribbon-like hyphae branching at right angles — the morphology that distinguishes Mucorales from the septate acute-angle-branching Aspergillus. Urgent surgical assessment by ENT and ophthalmology is part of the initial management, not a referral for the next day. [1]
Treatment — amphotericin, surgery, and reverse the immunosuppression
The ECMM global guideline for mucormycosis (2019) is the current reference [10]. Treatment rests on three simultaneous pillars:
- High-dose liposomal amphotericin B — 5 to 10 mg/kg/day intravenously (the higher dose for cerebral or extensive disease). Liposomal is preferred over amphotericin B deoxycholate because of the better toxicity profile at these high doses. The treatment continues for several weeks until there is clinical and radiological stability, then a step-down to isavuconazole or posaconazole (the only triazoles with activity against Mucorales — voriconazole, fluconazole, and the echinocandins have no activity).
- Aggressive, repeated surgical debridement — the cornerstone. Mucormycosis is a disease where antifungals alone cannot clear infected, infarcted tissue because the angioinvasion has cut off the blood supply to the area; only surgery can remove the necrotic, organism-laden tissue. The surgery is often disfiguring (palate, orbit, sinuses) and must be repeated until clear margins are achieved. This is the hardest conversation with the patient and family, and it is non-negotiable.
- Rapid reversal of the underlying immunosuppression — correct the diabetic ketoacidosis aggressively, reduce or stop corticosteroids where possible, and reduce transplant immunosuppression in consultation with the transplant team. Recovery of metabolic and immune function is as important as the antifungal. [1]
Salvage and adjunctive therapy. Isavuconazole and delayed-release posaconazole are recommended as salvage or step-down therapy [10]. High-dose deferasirox (iron chelation) was investigated as an adjunctive therapy on the rationale of iron withdrawal, but a randomised trial showed harm and it is no longer recommended. Hyperbaric oxygen has theoretical benefit (enhancing neutrophil function and reducing tissue hypoxia in infarcted areas) but limited evidence; it is used in selected centres.
Antifungal agents — class by class
A working knowledge of the antifungal classes is essential because the empiric choice depends on the suspected organism, the patient's stability, the drug's spectrum, and the drug's toxicity and interactions. The classes below cover the antifungals a physician uses. [1]
Azoles — the largest class, with the most interactions
The azoles inhibit lanosterol 14-alpha-demethylase, depleting ergosterol and disrupting the fungal cell membrane. They are divided into the imidazoles (topical, e.g. clotrimazole, miconazole, ketoconazole — the last is now essentially obsolete systemically because of hepatotoxicity and adrenal suppression) and the triazoles (the systemic agents). [1]
Fluconazole — excellent bioavailability, good CSF penetration, covers most Candida (except C. krusei, and often C. glabrata) and Cryptococcus; no mould activity. Use for oesophageal candidiasis, candidal vaginitis, candidaemia in the stable patient, cryptococcal consolidation and maintenance, and coccidioidal meningitis. Standard dose 200 to 400 mg daily (up to 800 to 1200 mg for severe or meningitis). Minimal CYP interactions relative to the other triazoles. Prolongs the QT interval. [1]
Voriconazole — the first-line for invasive aspergillosis and most invasive mould disease (except Mucorales). Excellent bioavailability, good CSF penetration, requires therapeutic drug monitoring. Major CYP2C19 and CYP3A4 substrate and inhibitor — significant interactions with tacrolimus, sirolimus, cyclosporin, warfarin, statins, and many others. Adverse effects: transient visual disturbance (the classic bright-lights and colour-perception effect), hepatotoxicity, photosensitivity (and a concerning signal for squamous cell carcinoma of the skin with prolonged use), and periostitis (fluoride in the molecule). Contraindicated in pregnancy. [1]
Posaconazole — the broadest-spectrum triazole, covering Aspergillus, Mucorales, Candida, and the endemic mycoses. Used for mould prophylaxis in very high-risk neutropenia and graft-versus-host disease, and for mucormycosis treatment (as step-down or salvage). The delayed-release tablet and intravenous formulation achieve much higher and more reliable levels than the original oral suspension; therapeutic drug monitoring is recommended. Significant CYP3A4 inhibition (interactions with calcineurin inhibitors). [1]
Isavuconazole — the newest triazole; covers Aspergillus and Mucorales (the only triazole with reliable activity against both). Established by the SECURE trial as non-inferior to voriconazole for invasive mould disease [5]. Predictable linear pharmacokinetics (no routine drug monitoring required), loading dose built into the first 48 hours, fewer drug interactions than voriconazole, fewer visual adverse events, and — uniquely — it shortens the QT interval (so avoid in familial short QT syndrome, but a potential advantage over other azoles in patients on QT-prolonging polypharmacy). An excellent alternative to voriconazole, especially where drug interactions are a concern.
Itraconazole — used for the endemic mycoses (Histoplasma, Blastomyces, Sporothrix, Paracoccidioides), for allergic bronchopulmonary aspergillosis, and for mild chronic pulmonary aspergillosis. Oral solution (better absorption than the capsule, which requires food and gastric acidity); requires level monitoring; negative inotrope effect (can precipitate heart failure). [1]
Echinocandins — the fungicidal Candida class
The echinocandins inhibit beta-(1,3)-D-glucan synthase, depleting the fungal cell wall (a structure absent in mammalian cells, hence the clean toxicity profile). They are fungicidal against Candida (the azoles are fungistatic) and have modest activity against Aspergillus (fungistatic, used as adjunct in refractory disease) and no activity against Cryptococcus, Mucorales, or the endemic mycoses. They have minimal drug interactions and minimal toxicity. The three agents are clinically interchangeable for invasive candidiasis: [1]
- Caspofungin — 70 mg loading then 50 mg daily intravenously (dose-reduce in hepatic impairment).
- Micafungin — 100 mg daily intravenously (no loading dose; 150 mg daily for Candida endocarditis).
- Anidulafungin — 200 mg loading then 100 mg daily intravenously. [1]
The echinocandins are first-line for candidaemia in the unstable, neutropenic, or critically ill patient and in the patient with recent azole exposure, and for oesophageal candidiasis refractory to fluconazole. They do not reach the urine or the CSF in useful concentrations, so they are not appropriate for candidal urinary tract infection or meningitis. [1]
Polyenes — amphotericin B, deoxycholate and liposomal
Amphotericin B binds to ergosterol in the fungal cell membrane, forming pores that leak cellular contents and kill the organism. It is the broadest-spectrum antifungal — active against most pathogenic fungi including Aspergillus, Candida, Cryptococcus, the endemic mycoses, and the Mucorales — and it remains the drug of choice (or the backbone of combination therapy) for severe cryptococcal meningitis, visceral leishmaniasis, and mucormycosis. [1]
Amphotericin B deoxycholate — the original formulation; effective but with substantial toxicity (acute infusion reactions of fever, rigors, hypotension; nephrotoxicity from afferent arteriolar vasoconstriction and tubular injury; renal potassium and magnesium wasting; anaemia from erythropoietin suppression). The test dose and premedication (paracetamol, antihistamine, hydrocortisone) and the saline loading (500 mL normal saline before the infusion to reduce nephrotoxicity) are traditional measures. [1]
Liposomal amphotericin B (AmBisome) — the lipid formulation in which amphotericin is encapsulated in liposomes; it delivers the drug preferentially to the fungus-rich tissues and reticuloendothelial system and markedly reduces nephrotoxicity and infusion reactions. The standard dose is 3 mg/kg/day (3 to 4 for cryptococcal meningitis, 5 to 10 for mucormycosis). Liposomal is the preferred formulation for most indications in the developed world because of the better toxicity profile at higher doses. [1]
Flucytosine (5-fluorocytosine) — the adjunct for cryptococcal meningitis
Flucytosine is converted by fungal cytosine deaminase to 5-fluorouracil, which inhibits fungal DNA synthesis. It is only used in combination with amphotericin B for cryptococcal meningitis (it accelerates CSF sterilisation and improves survival) and is never used as monotherapy because of rapid resistance emergence. The dose is 25 mg/kg orally every 6 hours (100 mg/kg/day), dose-adjusted for renal function, with peak serum levels monitored (2-hour post-dose, target below 100 mg/L) to avoid the principal toxicity of bone-marrow suppression (leucopenia, thrombocytopenia, anaemia) and colitis. The ANZ pearl: flucytosine is often unavailable or unaffordable in resource-limited settings, which is part of the rationale for the AMBITION single-dose regimen. [1]
Prophylaxis strategies — preventing the catastrophic infections
The right prophylaxis, given to the right patient for the right duration, prevents most of the catastrophic fungal infections. The strategy is built on the host. [1]
| Host / setting | Prophylaxis | Duration |
|---|---|---|
| Prolonged neutropenia (AML induction, MDS, high-risk chemotherapy) | Posaconazole (preferred, covers moulds including Mucorales) or fluconazole | During neutropenia |
| Allogeneic HSCT, acute or chronic GVHD | Posaconazole or voriconazole (mould-active) | Until engraftment; through GVHD treatment |
| Solid organ transplant (kidney, liver, heart) | Co-trimoxazole for PJP; nystatin or fluconazole for mucocutaneous candidiasis in the first month | PJP: at least 6 months (longer in lung, small bowel) |
| Lung transplant | Voriconazole or posaconazole for Aspergillus prophylaxis; co-trimoxazole for PJP | Often 6 to 12 months (longest of SOT) |
| HIV, CD4 below 200 | Co-trimoxazole for PJP; fluconazole maintenance after cryptococcal meningitis | Until CD4 above 100 to 200 for 6 months on ART |
| Corticosteroids above 20 mg for more than 4 weeks | Co-trimoxazole for PJP | Through the steroid course and beyond |
| Liver transplant, high risk (fulminant failure, retransplant, long operative time, renal failure) | Fluconazole or an echinocandin for the first month (pre-transplant colonisation, high Candida risk) | 4 weeks |
The principle: the prophylaxis matches the predicted risk. Posaconazole or voriconazole for the highest-risk mould settings (prolonged neutropenia, GVHD, lung transplant); fluconazole for the standard-risk Candida settings (standard HSCT engraftment, liver transplant); co-trimoxazole for PJP across the T-cell-deficient settings (HIV, transplant, high-dose steroids). Always screen for HBV, HCV, HIV, CMV, EBV, and strongyloides before transplant or intense immunosuppression, because these infections complicate the fungal prophylaxis plan. [1]
Regional guideline deltas
| Aspect | ANZ (eTG, ASID) | UK (NICE, BIA, BSH) | US (IDSA, CDC/NIH OI) |
|---|---|---|---|
| Empiric antifungal in neutropenic fever | Echinocandin or liposomal amphotericin; mould-active azole if galactomannan positive or halo sign | Echinocandin or liposomal amphotericin; posaconazole or caspofungin if prior azole prophylaxis | Liposomal amphotericin B, echinocandin, or voriconazole per IDSA |
| First-line for invasive aspergillosis | Voriconazole (or isavuconazole) | Voriconazole (or isavuconazole) | Voriconazole (or isavuconazole) per IDSA 2016 |
| Cryptococcal induction | Liposomal amphotericin B plus flucytosine 2 weeks; AMBITION single high-dose regimen increasingly used | Liposomal amphotericin B plus flucytosine 2 weeks | Liposomal amphotericin B plus flucytosine at least 2 weeks (IDSA 2010) |
| Mucormycosis first-line | Liposomal amphotericin 5 to 10 mg/kg/day plus debridement | Liposomal amphotericin plus debridement | Liposomal amphotericin 5 to 10 mg/kg/day plus debridement (ECMM 2019) |
| PJP prophylaxis threshold | CD4 below 200; co-trimoxazole | CD4 below 200; co-trimoxazole | CD4 below 200; co-trimoxazole |
High-yield exam discriminators
- Echinocandin for unstable candidaemia; fluconazole only for stable, non-neutropenic, no prior azole — and always remove the central line and do a fundoscopy.
- Voriconazole first-line for invasive aspergillosis (Herbrecht survival benefit); isavuconazole is the non-inferior alternative with a cleaner profile — liposomal amphotericin is not first-line.
- Liposomal amphotericin B plus flucytosine for cryptococcal meningitis induction; fluconazole for consolidation and maintenance; serial therapeutic LPs for raised ICP — and manage the ICP, which is the biggest determinant of early death.
- High-dose co-trimoxazole for PJP; add adjunctive steroids when PaO2 below 60 or A-a gradient above 35, within 72 hours of starting co-trimoxazole.
- Liposomal amphotericin B 5 to 10 mg/kg/day plus surgical debridement for mucormycosis; voriconazole and the echinocandins are inactive. [1]6. The halo sign is Aspergillus (early); the reverse halo (atoll sign) is Mucorales (early) — and the distinction changes the drug.
- Galactomannan is for Aspergillus; beta-D-glucan is for Candida, Aspergillus, and PJP (but not Cryptococcus or Mucorales); CrAg is for Cryptococcus; India ink is Cryptococcus on microscopy.
- Histopathology is the discriminator between Aspergillus (septate acute-angle hyphae) and Mucorales (broad non-septate ribbon-like right-angle hyphae).
- Isavuconazole shortens the QT; all other triazoles prolong it — a unique pharmacological point and a favourite viva question.
- Coccidioidal meningitis requires lifelong fluconazole; cryptococcal maintenance continues until immune restoration. [1]
Communication and shared decision-making
- Before prolonged antifungal therapy: "This infection will need several months of treatment. The first few weeks will be in hospital with intravenous medication; once you are stable, you will move to tablets that you take at home, and we will monitor your blood tests and the drug levels to make sure the treatment is working and is not causing side effects. The visual effects you might notice with voriconazole — bright lights or altered colours — are common, are not dangerous, and settle when we stop the drug."
- Before surgical debridement for mucormycosis: "This is a rapidly destructive infection. The medication alone cannot reach the dead tissue because the infection has cut off its blood supply, so the surgery is as important as the medication. The surgery will be disfiguring — it may remove tissue from your palate, your nose, or the area around your eye — and it may need to be repeated. I know this is devastating news, and we will support you and your family through it, but without the surgery the infection will progress within days."
- On raised ICP in cryptococcal meningitis: "The infection has caused a build-up of pressure in the brain, which is the most dangerous part of this illness. We will need to drain fluid from your spine every day until the pressure comes down. This is uncomfortable but it is the single most important thing we can do to save your life and your sight." [1]
Summary: the fungal infection consultation in one paragraph
Identify the host — neutropenic, T-cell-deficient, transplant phase, ICU with central lines, or diabetic in ketoacidosis — because the host predicts the organism, the diagnostic test, and the empiric therapy. In candidaemia use an echinocandin for the unstable or critically ill patient (or fluconazole for the stable patient without prior azole exposure), remove the central line, perform a dilated fundoscopy, and treat for 14 days from the first negative culture. In invasive aspergillosis use voriconazole first-line (or isavuconazole), with therapeutic drug monitoring, and reduce immunosuppression; the chest CT finds the halo sign early, and the galactomannan supports the diagnosis. In cryptococcal meningitis use amphotericin B plus flucytosine induction (or the AMBITION single-dose regimen), fluconazole consolidation and maintenance, and manage the raised ICP with serial therapeutic lumbar punctures — the ICP, not the antifungal, is the biggest determinant of early death. In PJP use high-dose co-trimoxazole for 21 days with adjunctive corticosteroids when the PaO2 is below 60 mmHg or the A-a gradient is above 35 mmHg, given within 72 hours. In mucormycosis use high-dose liposomal amphotericin B and aggressive surgical debridement — voriconazole and the echinocandins are inactive, and delay is fatal. Give the right prophylaxis to the right host — posaconazole or voriconazole for the highest-risk mould settings, fluconazole for standard Candida risk, and co-trimoxazole for PJP across the T-cell-deficient settings — and screen before you suppress. [1]
References
- [1]Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America Clin Infect Dis, 2016.PMID 26679628
- [2]Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America Clin Infect Dis, 2016.PMID 27365388
- [3]Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america Clin Infect Dis, 2010.PMID 20047480
- [4]Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med, 2002.PMID 12167683
- [5]Maertens JA, Raad II, Marr KA, et al. Isavuconazole versus voriconazole for primary treatment of invasive mould disease caused by Aspergillus and other filamentous fungi (SECURE): a phase 3, randomised-controlled, non-inferiority trial Lancet, 2016.PMID 26684607
- [6]Jarvis JN, Lawrence DS, Meya DB, et al. Single-Dose Liposomal Amphotericin B Treatment for Cryptococcal Meningitis N Engl J Med, 2022.PMID 35320642
- [7]Reboli AC, Rotstein C, Pappas PG, et al. Anidulafungin versus fluconazole for invasive candidiasis N Engl J Med, 2007.PMID 17568028
- [8]Boulware DR, Rolfes MA, Rajasingham R, et al. Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa N Engl J Med, 2018.PMID 29539274
- [9]Ewald H, Raatz H, Boscacio R, et al. Adjunctive corticosteroids for Pneumocystis jiroveci pneumonia in patients with HIV infection Cochrane Database Syst Rev, 2015.PMID 25835432
- [10]Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium Lancet Infect Dis, 2019.PMID 31699664