Phys · infectious
Healthcare-Associated Infections
Also known as healthcare-associated infection · HAI · hospital-acquired infection · nosocomial infection · catheter-related bloodstream infection · CRBSI · central line-associated bloodstream infection · CLABSI · ventilator-associated pneumonia · VAP · catheter-associated urinary tract infection · CAUTI · surgical site infection · SSI · Clostridioides difficile · C. difficile · care bundle · central line bundle · ventilator bundle · WHO Five Moments · differential time to positivity · antibiotic lock therapy · MRSA · VRE · ESBL · CRE · fidaxomicin · bezlotoxumab · subglottic secretion drainage
Consultant-physician-depth guide to healthcare-associated infections (HAI) — the five major device-associated infection types (CRBSI/CLABSI, VAP, CAUTI, SSI, CDI), their clinical presentation, diagnosis, management and prevention, together with multi-drug resistant organisms (MRSA, VRE, ESBL, CRE), WHO Five Moments for Hand Hygiene, and evidence-based infection control bundles. Covers paired blood cultures and differential time to positivity for CRBSI, the ventilator bundle for VAP, the central line insertion checklist (Pronovost), surgical prophylaxis timing for SSI, the two-step C. difficile diagnostic algorithm with fidaxomicin first-line therapy, and the stewardship principles that prevent all HAIs. Structured for FRACP DWE MCQ, DCE long case and DCE short case, with MRCP and ABIM overlays.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Healthcare-Associated Infections

The one-minute consultant answer
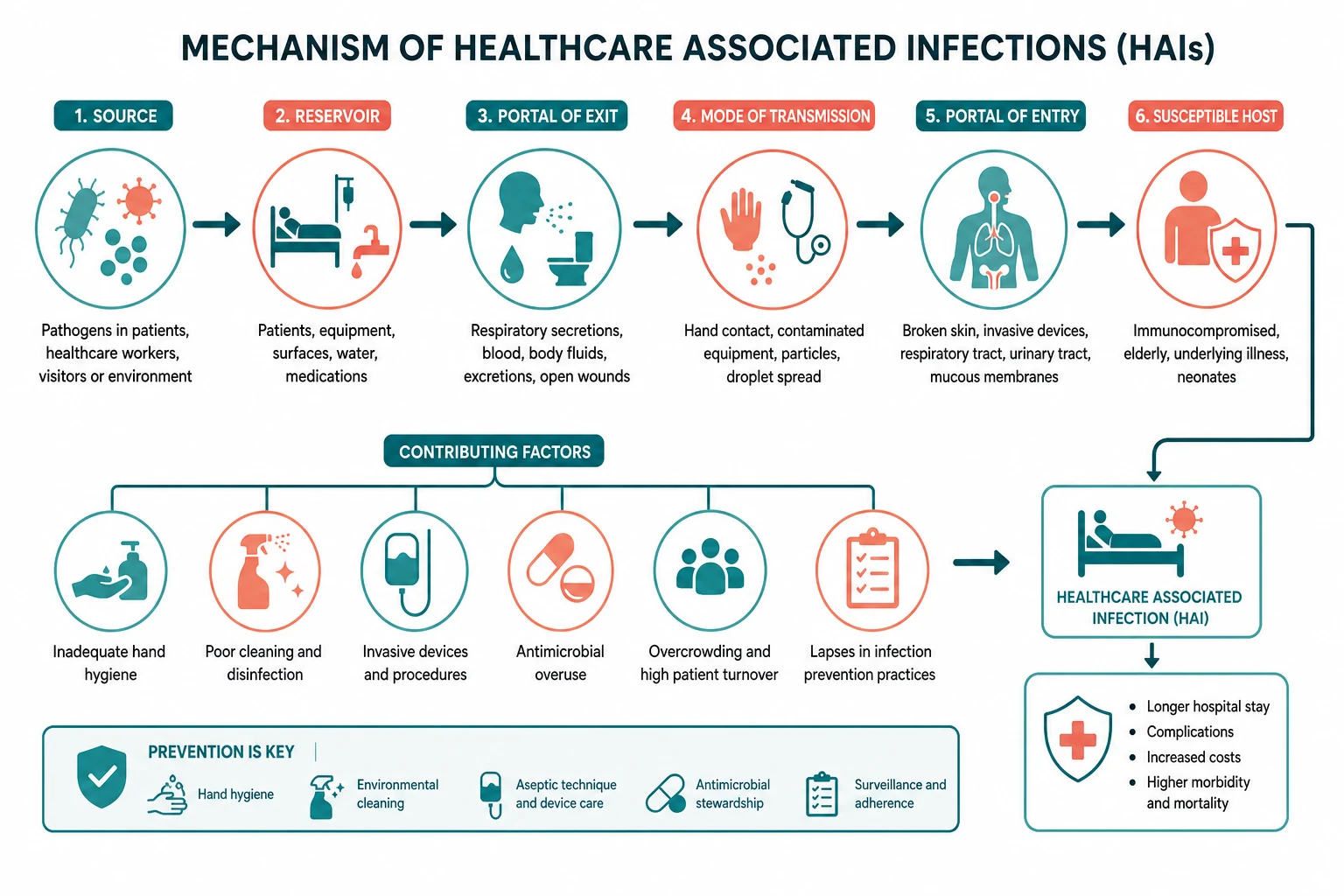
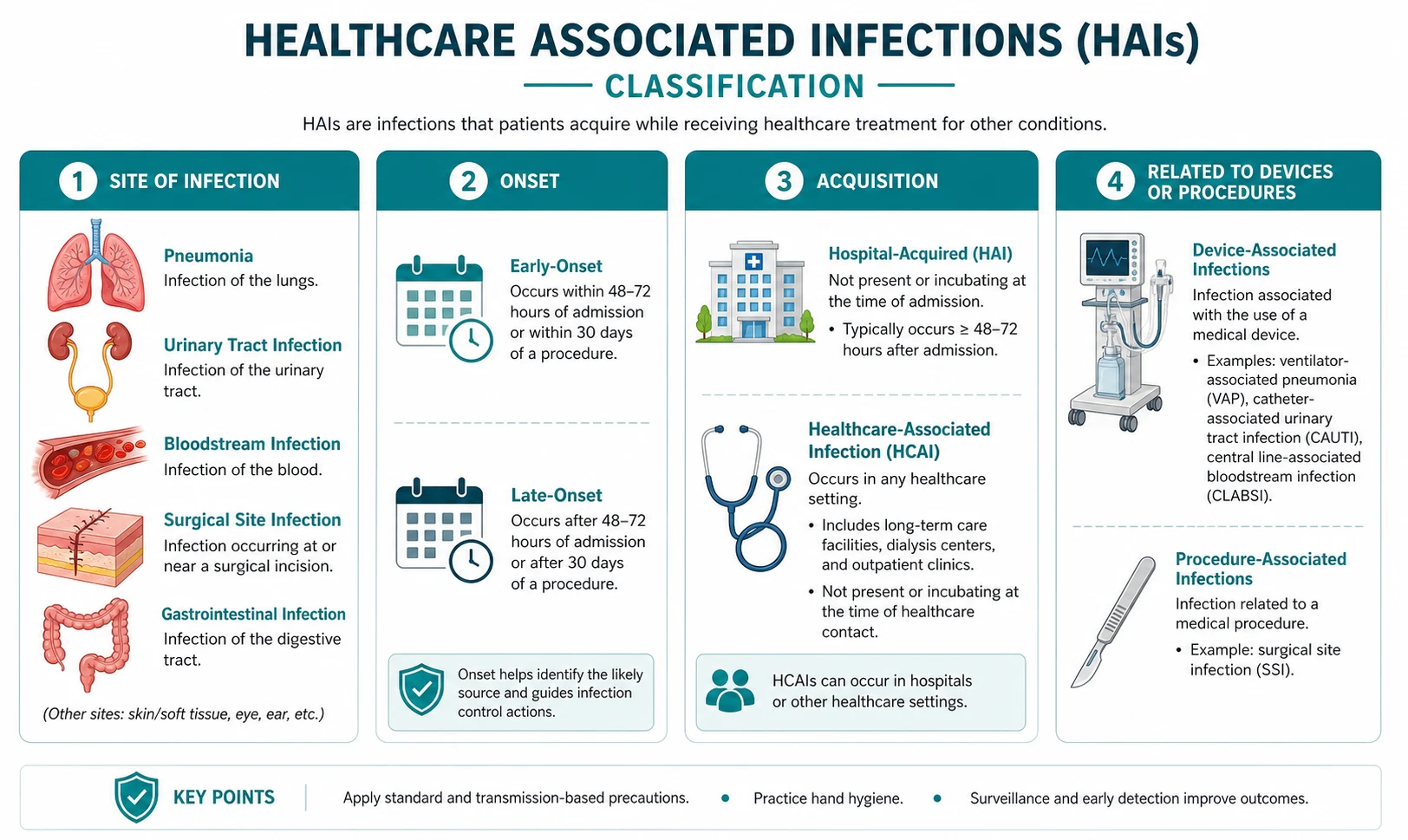
A healthcare-associated infection (HAI) is an infection that was not present or incubating at the time of admission — operationally, one that develops 48 hours or more after admission, or within 30 days of a procedure (90 days if an implant was placed), or within 48 hours of discharge. The five device-associated HAIs that dominate clinical practice and exam questioning are catheter-related bloodstream infection (CRBSI, also called CLABSI), ventilator-associated pneumonia (VAP), catheter-associated urinary tract infection (CAUTI), surgical site infection (SSI), and Clostridioides difficile infection (CDI). Each has a defined clinical syndrome, a defined diagnostic strategy, a defined management pathway, and — critically — a defined evidence-based prevention bundle. The prevention of HAI is a systems activity: hand hygiene, care bundles, antimicrobial stewardship and device minimisation are the four pillars, and the physician's role is to implement them reliably and to remove devices promptly [1] [2].
The core principle is that devices cause infections, and the safest device is the one that is not there. Every central venous catheter, urinary catheter, and endotracheal tube carries a daily risk of infection, and the single most effective prevention measure for all three is daily review of necessity with prompt removal. When the device cannot be removed, evidence-based care bundles reduce the infection risk substantially — the central line bundle reduced CLABSI rates by up to 66 per cent in the landmark Pronovost Michigan ICU study [1], and the ventilator bundle reduces VAP by approximately 40 per cent in meta-analytic data [4]. These bundles are not a menu of suggestions — they are a set of measures that, when delivered together and reliably, transform the safety of invasive devices.
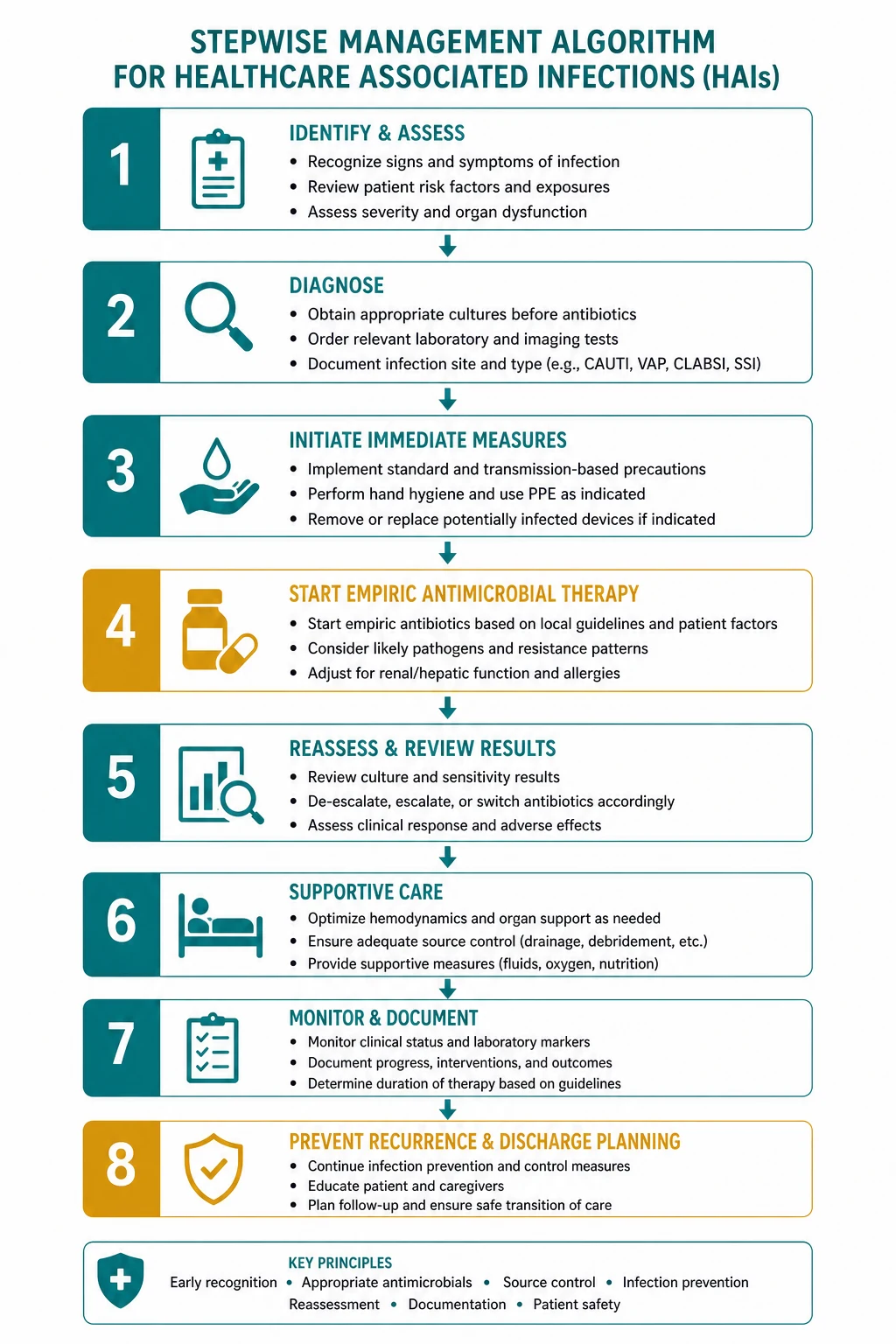
For the physician managing a suspected HAI at the bedside, the approach is: first, identify the likely source (line, lungs, urine, wound, or colon); second, obtain appropriate cultures BEFORE starting or changing antibiotics; third, start empiric therapy calibrated to the likely organism and the local antibiogram; and fourth, de-escalate at 48 hours based on culture results. This connects directly to antimicrobial stewardship (see the dedicated topic): every HAI prevented is one fewer antibiotic course, one fewer selection pressure for resistance, and one fewer risk of CDI [8]. The exam will test you on the specific diagnostic criteria (especially paired blood cultures and differential time to positivity for CRBSI), the bundle components (especially the central line and ventilator bundles), the severity-stratified CDI therapy (especially the fidaxomicin-versus-vancomycin decision), and the distinction between asymptomatic bacteriuria and CAUTI (treating the former is a classic MCQ error).
The HAI landscape — the five major types and their prevention

Why this matters
HAIs are the most common complication of hospitalisation. They affect approximately 1 in 10 hospitalised patients in developed countries, prolong hospital stay by an average of 4 to 10 days, increase mortality, and cost healthcare systems billions annually. More importantly for the physician, they are largely preventable — the evidence base for prevention is stronger than for almost any other area of inpatient medicine, and the gap between best practice and actual practice is a quality-of-care problem, not a knowledge problem. [1]
The five device-associated HAIs have a common logic: a device breaches a normal defence barrier (skin for a central line, mucosa for a urinary catheter, the airway for an endotracheal tube, the skin again for a surgical wound, and the colonic microbiome for antibiotic-associated CDI), bacteria colonise the device or the disrupted barrier, and biofilm formation makes the infection difficult to eradicate without removing the device or restoring the disrupted barrier. [1]
The five types at a glance
CRBSI / CLABSI — a bloodstream infection attributable to a central venous catheter. It is defined by paired blood cultures (one peripheral, one drawn through the central line) with the same organism grown from both, and either a differential time to positivity above 120 minutes (the central line culture turns positive first, indicating the line is the source) or a positive semi-quantitative catheter tip culture (Maki roll-plate with above 15 colony-forming units). Common organisms are coagulase-negative staphylococci (the commonest and the most likely to be a contaminant), Staphylococcus aureus (the most virulent — mandates echocardiography and prolonged therapy), enterococci, Gram-negative bacilli (especially Klebsiella, E. coli, Enterobacter, Serratia — these organisms indicate a high bacterial burden at the hub), and Candida (especially in patients on total parenteral nutrition, broad-spectrum antibiotics, or with haematological malignancy). The central line bundle — hand hygiene, full barrier precautions at insertion, chlorhexidine skin preparation, avoidance of the femoral site, and daily review of necessity — reduced CLABSI by up to 66 per cent in the Pronovost study of 103 Michigan ICUs [1].
VAP — pneumonia developing 48 hours or more after the initiation of mechanical ventilation. It arises from microaspiration of oropharyngeal secretions around the endotracheal tube cuff and from biofilm within the tube itself. The common organisms are late-onset VAP organisms: Pseudomonas aeruginosa, Acinetobacter baumannii, MRSA, Klebsiella pneumoniae, and other Enterobacteriaceae. Early-onset VAP (within 4 days) is more likely to be caused by community organisms (Streptococcus pneumoniae, Haemophilus influenzae, methicillin-sensitive S. aureus). The ventilator bundle — head of bed elevation 30 to 45 degrees, daily sedation interruption with spontaneous breathing trial, peptic ulcer prophylaxis where indicated, DVT prophylaxis, oral chlorhexidine, and subglottic secretion drainage — reduces VAP incidence by approximately 40 per cent [4] [5].
CAUTI — the most common HAI, with risk increasing linearly with catheter duration (bacteriuria develops in approximately 3 to 7 per cent of catheterised patients per day). The common organisms are E. coli, Enterococcus, Pseudomonas, Klebsiella, Proteus, and Candida. The critical distinction is between symptomatic CAUTI (new or worsening fever, rigors, altered mental status, malaise, lethargy, flank pain, CVA tenderness, acute haematuria, pelvic discomfort, or suprapubic pain, with a urine culture meeting criteria — above 10 cubed CFU/mL of no more than 2 species) and catheter-associated asymptomatic bacteriuria (positive culture without signs or symptoms), which does not require treatment except in pregnancy and before urological procedures [6] [13]. Prevention centres on avoiding catheterisation and removing the catheter as soon as possible.
SSI — infection occurring within 30 days of a procedure (or within 90 days if an implant was placed). SSIs are classified as superficial incisional (skin and subcutaneous tissue, within 30 days), deep incisional (fascial and muscle layers, within 30 days or 90 days with implant), and organ or space (any part of the body deeper than the fascia opened during the procedure, within 30 days or 90 days with implant). Risk factors include diabetes (poorly controlled), obesity, smoking, prolonged preoperative hospital stay, prolonged operative time, immunosuppression, hypothermia, and failure to give appropriate prophylactic antibiotics at the right time. Prevention rests on the surgical bundle: prophylactic antibiotics within 60 minutes of incision (120 minutes for vancomycin and fluoroquinolones due to longer infusion times), appropriate agent and weight-based dose, normothermia, glycaemic control, hair clipping rather than shaving, and limited duration of prophylaxis (discontinue within 24 hours, or 48 hours for cardiac surgery) [7].
CDI — antibiotic-associated colitis caused by Clostridioides difficile, a spore-forming Gram-positive anaerobic bacillus. It is covered in detail in the antimicrobial stewardship topic; here the key points are the connection to HAI (it is the HAI most directly linked to antibiotic prescribing, and its prevention is primarily a stewardship activity) and the severity-stratified management: fidaxomicin 200 mg twice daily for 10 days is first-line for an initial non-severe or severe (non-fulminant) episode (2021 IDSA/SHEA focused update) [9]; oral vancomycin 125 mg four times daily is an acceptable alternative; fulminant CDI (hypotension, ileus, toxic megacolon) requires oral vancomycin 500 mg four times daily PLUS intravenous metronidazole 500 mg every 8 hours [8].
Catheter-related bloodstream infection (CRBSI / CLABSI)

The clinical problem
A patient with a central venous catheter develops fever, rigors, or signs of sepsis — sometimes with exit-site purulence, tunnel-tract erythema, or pocket infection (for tunnelled lines such as Hickman or Port-a-Cath). The question is: is the line the source, or is this bacteraemia from elsewhere (a pneumonia, a UTI, an intra-abdominal source)? [1]
Pathophysiology
The central venous catheter breaches the skin barrier and provides a foreign body surface on which bacteria form a biofilm — a structured community of bacteria encased in an extracellular polymeric matrix that is relatively resistant to both host defences and antibiotics. Bacteria reach the catheter by two main routes: the extraluminal route (migration from the skin exit site along the external catheter surface into the bloodstream — the dominant route for short-term, non-tunnelled catheters), and the intraluminal route (contamination of the catheter hub during access, followed by migration along the internal lumen — the dominant route for long-term tunnelled catheters) [2] [3].
The organisms reflect these routes and the patient population: coagulase-negative staphylococci (Staphylococcus epidermidis and related species — skin commensals, the commonest CRBSI organism, and the one most likely to represent contamination), Staphylococcus aureus (the most virulent — 10 to 20 per cent of cases but associated with higher mortality, metastatic infection, and the need for prolonged therapy), enterococci (E. faecalis, E. faecium — often VRE in healthcare settings), Gram-negative bacilli (Klebsiella, E. coli, Enterobacter, Serratia, Pseudomonas — these organisms suggest heavy hub contamination or an intra-abdominal source), and Candida species (especially C. albicans and C. glabrata, in patients on broad-spectrum antibiotics, total parenteral nutrition, or with haematological malignancy) [3].
Diagnosis
The diagnosis requires paired blood cultures — one peripheral and one drawn through the central venous catheter — both sent before starting antibiotics [3]. The key diagnostic criteria are:
- The same organism grows from both cultures (if only the line culture is positive, it may be a contaminant).
- Differential time to positivity (DTP) above 120 minutes: if the culture drawn through the central line turns positive more than 2 hours before the peripheral culture, this strongly supports the catheter as the source (sensitivity above 80 per cent, specificity above 90 per cent). The rationale is that a higher bacterial inoculum is present in the blood drawn through the infected line, so it reaches the detection threshold sooner.
- Semi-quantitative catheter tip culture (Maki roll-plate method): if the catheter is removed, rolling the tip across an agar plate and finding more than 15 colony-forming units supports colonisation of the external catheter surface. A quantitative sonication method (above 10 cubed CFU/mL) is an alternative. [1]
A single positive blood culture drawn through the central line is NOT diagnostic of CRBSI — it may be a contaminant (especially coagulase-negative staphylococci), or it may reflect bacteraemia from another source with the line culture sampling contaminated blood. The paired culture strategy is essential, and failing to send a peripheral culture is a common and serious error. [1]
If there is exit-site purulence, a swab and culture of the discharge is useful, but the paired blood cultures remain the diagnostic test. Tunnel-tract infection (erythema, tenderness, or induration along the subcutaneous track of a tunnelled catheter, more than 2 cm from the exit site) and pocket infection (purulent fluid in the subcutaneous pocket of an implanted port) are clinical diagnoses and almost always require catheter removal. [1]
Management
The management of CRBSI has five elements [3]:
-
Obtain cultures before starting antibiotics — paired peripheral and central blood cultures, plus (if the line is removed) a semi-quantitative tip culture. This is non-negotiable: without cultures, de-escalation is impossible. [1]
-
Empiric antibiotics — the choice depends on severity and risk factors. For an unstable patient, vancomycin 1.5 g IV every 12 hours (covering MRSA and coagulase-negative staphylococci) plus an anti-pseudomonal agent (piperacillin-tazobactam 4.5 g every 6 to 8 hours, or cefepime 2 g every 8 hours) to cover Gram-negatives. If Candida is suspected (TPN, prolonged broad-spectrum antibiotics, haematological malignancy), add an echinocandin (caspofungin 70 mg loading then 50 mg daily, or micafungin 100 mg daily). [1]
-
Decide on line removal versus salvage — the default is to remove the line, but for certain low-virulence organisms (coagulase-negative staphylococci, Enterococcus in a stable patient) in a patient where line replacement is difficult (e.g., limited venous access), antibiotic lock therapy (instilling a high concentration of antibiotic into the catheter lumen for hours or days, in addition to systemic therapy) may allow salvage. Line salvage is NOT appropriate for S. aureus, Pseudomonas, or Candida — these organisms form resilient biofilms, carry a high risk of metastatic infection, and mandate line removal. [1]
-
Targeted therapy based on the organism — de-escalate to the narrowest effective agent based on culture and sensitivity results. For coagulase-negative staphylococci, vancomycin for 7 to 14 days (if uncomplicated). For S. aureus, a beta-lactam (flucloxacillin 2 g IV every 4 to 6 hours for MSSA, or vancomycin for MRSA) for a minimum of 14 days after the first negative blood culture, with echocardiography to exclude endocarditis. For enterococci, ampicillin (if susceptible) or vancomycin. For Gram-negatives, a targeted agent based on sensitivity. For Candida, an echinocandin with transition to fluconazole after clinical response, for 14 days after the first negative culture. [1]
-
Repeat blood cultures — repeat every 48 to 72 hours until clearance. Persistent bacteraemia beyond 72 hours despite appropriate therapy and line removal should prompt a search for metastatic infection (endocarditis, septic thrombophlebitis, vertebral osteomyelitis) with echocardiography, imaging, and consideration of prolonged therapy (4 to 6 weeks) [3].
Prevention — the central line insertion bundle
The five-component central line insertion bundle demonstrated by Pronovost and colleagues in the Michigan ICU study reduced CLABSI rates by up to 66 per cent across 103 ICUs [1]:
- Hand hygiene before the procedure (WHO Five Moments — Moment 1, before touching the patient, and Moment 2, before a clean or aseptic procedure).
- Full barrier precautions at insertion — sterile gown, sterile gloves, cap, and a full-body sterile drape (not just a small drape), for the operator and all assistants.
- Chlorhexidine skin preparation — 2 per cent chlorhexidine in 70 per cent alcohol, applied with friction and allowed to dry completely before puncture.
- Avoid the femoral site in adults — the femoral vein carries the highest infection risk (and bleeding risk) because of the density of skin flora in the groin and the difficulty of maintaining a sterile dressing. The preferred sites are the subclavian vein (lowest infection rate, but small risk of pneumothorax) and the internal jugular vein (moderate infection risk, no pneumothorax risk but higher risk under ultrasound guidance). In children, the femoral site is more acceptable.
- Daily review of necessity with prompt removal — every central line should have a documented daily indication, and the line should be removed as soon as it is no longer needed. This is the single most effective prevention measure. [1]
Additional measures include chlorhexidine-impregnated sponge dressings (reduced CRBSI in high-risk patients), antimicrobial-impregnated catheters (minocycline-rifampicin or chlorhexidine-silver sulfadiazine coating, for catheters expected to remain in situ for more than 5 to 7 days), aseptic technique for hub access (scrub the hub with chlorhexidine or alcohol before every access), and dedicated central-line insertion carts with all supplies in one place [2].
Ventilator-associated pneumonia (VAP)
The clinical problem
A patient intubated and ventilated for more than 48 hours develops a new or progressive infiltrate on chest X-ray, plus fever (above 38 degrees), leucocytosis or leucopenia, and purulent respiratory secretions. This combination suggests VAP, but the diagnosis is imperfect — every component is non-specific in the ICU, and the chest X-ray can show atelectasis, pulmonary oedema, ARDS, or chemical pneumonitis from aspiration rather than infection. [1]
Pathophysiology
The endotracheal tube bypasses the upper airway's natural defence (the cough reflex and the mucociliary escalator) and provides a direct conduit for bacteria to reach the lower respiratory tract. Bacteria enter by three routes: microaspiration of oropharyngeal secretions pooling above the endotracheal tube cuff and leaking past it (the dominant route), biofilm within the endotracheal tube itself (bacteria adhere to the tube surface and are shed into the lower airway), and haematogenous spread (rare) [4].
The causative organisms depend on the timing of VAP: early-onset VAP (within 4 days of intubation) is more likely caused by community-type organisms — Streptococcus pneumoniae, Haemophilus influenzae, methicillin-sensitive S. aureus, Moraxella catarrhalis — reflecting the patient's oropharyngeal flora at the time of intubation. Late-onset VAP (after 4 days) is more likely caused by healthcare-associated, often multidrug-resistant organisms — Pseudomonas aeruginosa, Acinetobacter baumannii, MRSA, Klebsiella pneumoniae, other Enterobacteriaceae, and Stenotrophomonas maltophilia — reflecting colonisation of the oropharynx and stomach by hospital organisms over time. This distinction drives the empiric antibiotic choice: early-onset VAP can be treated with a narrower regimen (e.g., ceftriaxone), while late-onset VAP requires broad anti-pseudomonal and anti-MRSA cover until cultures return. [1]
Diagnosis
The diagnosis of VAP requires the combination of: [1]
- A new or progressive infiltrate on chest imaging (X-ray or CT), AND
- At least two of the following: fever above 38 degrees or hypothermia below 36 degrees; leucocytosis (above 12 x 10 to the 9 per litre) or leucopenia (below 4 x 10 to the 9 per litre); purulent respiratory secretions (neutrophil count above 25 per low-power field on Gram stain). [1]
This definition has imperfect specificity. The Clinical Pulmonary Infection Score (CPIS) — combining temperature, blood count, oxygenation (PaO2 over FiO2 ratio), chest X-ray findings, and tracheal secretions — improves specificity, with a CPIS above 6 supporting the diagnosis, but it is not used routinely. The key principle is to send lower respiratory tract samples (endotracheal aspirate, bronchoalveolar lavage, or protected specimen brush) BEFORE starting or changing antibiotics — without cultures, de-escalation is impossible [4].
Semiquantitative BAL culture results guide the diagnosis: above 10 to the 4 CFU/mL on BAL, or above 10 to the 3 CFU/mL on protected specimen brush, supports a diagnosis of VAP. Lower counts in a patient with radiographic and clinical changes suggest colonisation or an alternative diagnosis. [1]
Management
-
Send lower respiratory tract cultures BEFORE starting or changing antibiotics — endotracheal aspirate or BAL. [1]
-
Empiric therapy — calibrated to the risk of MDR organisms. For patients with no risk factors for MDR organisms (early-onset VAP, no recent antibiotics, no recent hospitalisation), ceftriaxone 2 g IV daily, or moxifloxacin 400 mg IV daily, or ampicillin-sulbactam. For patients WITH risk factors for MDR organisms (late-onset VAP, recent broad-spectrum antibiotics, recent ICU or hospitalisation, structural lung disease), two anti-pseudomonal agents (piperacillin-tazobactam 4.5 g every 6 hours PLUS amikacin or gentamicin, or cefepime 2 g every 8 hours) PLUS vancomycin 1.5 g every 12 hours or linezolid 600 mg every 12 hours for MRSA cover. [1]
-
De-escalate at 48 hours — once culture and sensitivity return, narrow to the narrowest effective agent. Stop the aminoglycoside (nephrotoxic) and the MRSA cover (if no MRSA) at 3 to 5 days if the organism is sensitive. Duration of therapy is typically 7 days for uncomplicated VAP with good clinical response, with clinical assessment (fever, white cell count, oxygenation, radiographic improvement) guiding the endpoint [4].
-
Source control — there is no device to remove (the endotracheal tube is needed for ventilation), but daily assessment for readiness to extubate (sedation interruption with spontaneous breathing trial) minimises the duration of ventilation and therefore the VAP risk. [1]
Prevention — the ventilator bundle
The ventilator bundle reduces VAP by approximately 40 per cent in meta-analytic data [4]. Its components are:
- Head of bed elevation 30 to 45 degrees (unless contraindicated) — this reduces the reflux of gastric contents and the microaspiration of oropharyngeal secretions.
- Daily sedation interruption with a spontaneous breathing trial (the "wake up and breathe" protocol) — this reduces the duration of mechanical ventilation (each additional day of ventilation increases VAP risk) and allows early identification of patients ready for extubation. [1]3. Peptic ulcer prophylaxis with a proton pump inhibitor or H2-receptor antagonist for patients at high risk of stress ulcer bleeding (mechanically ventilated for more than 48 hours, coagulopathy, recent GI bleed) — the rationale is that preventing stress ulcer bleeding prevents the gastric pH rise that promotes gastric bacterial colonisation, but this component is increasingly debated given the association between PPI use and CDI.
- DVT prophylaxis — subcutaneous heparin or mechanical compression — as part of the overall ICU care bundle (this does not prevent VAP per se but is included in the original IHI bundle to reduce overall ICU morbidity and mortality).
- Oral chlorhexidine mouthwash or gel (0.12 per cent or 0.2 per cent, every 8 to 12 hours) — reduces oropharyngeal bacterial load and microaspiration. (Note: the 2022 SHEA/IDSA Compendium made this a conditional recommendation with reduced emphasis, as some recent trials have shown less benefit than earlier studies.)
- Subglottic secretion drainage — using endotracheal tubes with a dedicated suction port above the cuff to continuously remove the pooled secretions that leak past the cuff. The Muscedere meta-analysis of 13 randomised trials showed a pooled relative risk of 0.55 for VAP, with reductions in duration of ventilation and ICU stay [5].
- Avoidance of unnecessary reintubation — reintubation carries a high risk of VAP.
Catheter-associated urinary tract infection (CAUTI)
The clinical problem
A patient with a urinary catheter develops fever, rigors, flank pain, suprapubic tenderness, or acute haematuria, and the urine culture is positive. The question is: is this a true CAUTI requiring antibiotics, or asymptomatic bacteriuria that should not be treated? [1]
Pathophysiology
The urinary catheter breaches the urethral defence barrier and provides a surface for bacterial biofilm formation. Bacteria reach the bladder by two routes: the extraluminal route (bacteria ascending along the outside of the catheter from the perineum — the dominant route in women) and the intraluminal route (bacteria ascending along the inside of the catheter from a contaminated drainage bag or a breach in the closed drainage system — the dominant route in men) [6]. Bacteriuria develops in 3 to 7 per cent of catheterised patients per day, and after 30 days virtually all catheterised patients are bacteriuric. The organisms are E. coli (the commonest), Enterococcus, Pseudomonas, Klebsiella, Proteus, Providencia, Morganella, and Candida, often in polymicrobial biofilm.
The critical distinction: CAUTI versus asymptomatic bacteriuria
This distinction is the single highest-yield exam point in the entire HAI topic, and the single most common antibiotic-prescribing error on the ward [6] [13].
Catheter-associated asymptomatic bacteriuria (CA-ASB) is defined as a positive urine culture (above 10 to the 5 CFU/mL of at least one organism) in a catheterised patient without signs or symptoms of UTI. It is common, it is not an infection in the clinical sense, and it does NOT require antibiotic treatment — except in two specific situations: pregnancy (risk of pyelonephritis and adverse pregnancy outcomes) and before urological procedures (risk of bacteraemia from the procedure). In all other situations — including elderly patients, patients with indwelling catheters, patients post-surgery, and patients with positive cultures at catheter removal — treating CA-ASB does not improve outcomes and increases resistance, C. difficile, and adverse drug reactions [13].
CAUTI is defined as signs or symptoms compatible with UTI (new or worsening fever, rigors, altered mental status, malaise, lethargy with no other identified cause, flank pain, costovertebral angle tenderness, acute haematuria, pelvic discomfort, or suprapubic pain) with a urine culture above 10 cubed CFU/mL of no more than 2 species of microorganisms [6]. Note the lower threshold (10 cubed rather than the traditional 10 to the 5) for catheterised patients, reflecting the biofilm effect.
Management
- Remove or change the catheter if it has been in situ for more than 7 days — the biofilm on a long-standing catheter means the catheter itself is colonised, and treating through it is unlikely to succeed.
- Culture the urine — preferably from a freshly inserted catheter or a clean-catch specimen if the catheter has been removed.
- Antibiotics — for symptomatic CAUTI, treat with a targeted agent based on culture results, for 5 to 7 days for uncomplicated lower UTI (or 7 to 14 days if upper tract signs or bacteraemia). Empirically, while awaiting cultures, use trimethoprim-sulfamethoxazole (if local E. coli resistance is below 20 per cent), nitrofurantoin (for lower UTI only, not effective for bacteraemia), or amoxicillin-clavulanate. For unwell patients with upper tract signs or sepsis, use an intravenous agent with Gram-negative cover (ceftriaxone, gentamicin, or piperacillin-tazobactam) [6].
Prevention
The prevention strategy is simple in principle and challenging in practice [6]:
- Avoid catheterisation — use catheters only for appropriate indications (acute urinary retention, accurate monitoring in critically ill patients, selected perioperative patients, end-of-life comfort, and management of sacral or perineal wounds in incontinent patients). Inappropriate indications include routine catheterisation of all admitted patients, catheterisation for incontinence in a patient who can be managed with pads or scheduled toileting, and catheterisation for convenience.
- Remove the catheter as soon as possible — implement catheter reminder systems, automatic stop orders, and daily review of necessity. Nurse-driven protocols for catheter removal (removing the catheter unless a physician documents a reason to continue) reduce catheter days and CAUTI rates.
- Use a closed drainage system with aseptic technique — maintain the drainage bag below the level of the bladder, prevent reflux of urine from the bag, and avoid disconnecting the system.
- Do not routinely change catheters — catheter changing does not prevent infection and should be reserved for clinical indications (blockage, leakage, bypassing). [1]
Surgical site infection (SSI)
The clinical problem
A patient who underwent surgery develops increasing pain, erythema, swelling, warmth, or purulent discharge at the incision site, with or without systemic signs (fever, tachycardia, rising white cell count). The SSI may be superficial (skin and subcutaneous tissue), deep (fascia and muscle), or organ or space (any structure opened or manipulated during the procedure, such as the peritoneal cavity, the pleural space, or a joint). [1]
Risk factors
The modifiable and non-modifiable risk factors for SSI [7]:
- Patient factors: diabetes (especially poorly controlled — HbA1c above 8 per cent or perioperative blood glucose above 10 mmol/L), obesity (BMI above 30 or above 35), smoking, malnutrition, immunosuppression (corticosteroids, chemotherapy), older age.
- Preoperative factors: prolonged preoperative hospital stay (colonisation with hospital organisms), shaving the surgical site with a razor (nicks in the skin become foci for infection — clipping is preferred), failure to use a preoperative antiseptic wash.
- Operative factors: prolonged operative time (infection risk increases with each additional hour), inappropriate or poorly timed antibiotic prophylaxis (the most modifiable factor), perioperative hypothermia (core temperature below 36 degrees impairs tissue oxygenation and immune function), perioperative hyperglycaemia (impairs neutrophil function), poor surgical technique (excessive electrocautery, dead space, haematoma), and inadequate sterile technique. [1]
Prevention — the surgical bundle
The surgical bundle is built on the principle that prophylactic antibiotics must be in the tissue at the time of incision, and that maintaining tissue oxygenation, normothermia, and normoglycaemia supports the host defence [7]:
-
Prophylactic antibiotics within 60 minutes before incision (within 120 minutes for vancomycin and fluoroquinolones, which require longer infusion times) — this is the single most evidence-based SSI prevention measure. The antibiotic must achieve a tissue concentration above the MIC of likely organisms at the time of incision. Late administration (after incision) is equivalent to no prophylaxis. [1]
-
Appropriate agent — cefazolin 2 g IV (3 g for patients above 120 kg) is the standard for most clean and clean-contaminated procedures (covers MSSA and streptococci). Add metronidazole 500 mg IV for colorectal and gynaecological procedures (anaerobic cover). Use vancomycin 15 mg/kg IV for MRSA-colonised patients, known beta-lactam allergy, or procedures where MRSA is a concern (cardiac, orthopaedic implant). [1]
-
Re-dosing for prolonged surgery or major blood loss — re-dose at two half-lives of the drug (cefazolin every 4 hours during prolonged surgery) or after blood loss above 1.5 litres. [1]
-
Discontinue prophylaxis within 24 hours (48 hours for cardiac surgery) — prolonged prophylaxis does not prevent SSI and increases resistance and C. difficile. This is a stewardship priority. [1]
-
Normothermia — maintain core temperature above 36 degrees Celsius using forced-air warming, warmed intravenous fluids, and increased ambient operating theatre temperature. [1]
-
Glycaemic control — for diabetic patients and cardiac surgery patients, maintain blood glucose below 10 to 11 mmol/L (180 to 200 mg/dL) in the perioperative period. Tighter control is not clearly beneficial and risks hypoglycaemia. [1]
-
Hair clipping, not shaving — clip hair with electric clippers immediately before surgery; do not use a razor. [1]
-
Preoperative skin preparation — 2 per cent chlorhexidine in 70 per cent alcohol (preferred) or povidone-iodine, applied to the surgical site and allowed to dry. [1]
Management
- Open the wound — for superficial and deep incisional SSI, opening the incision, draining any collection, and debriding necrotic tissue is the primary treatment. Most SSIs can be managed with wound care alone if there is no significant cellulitis or systemic toxicity.
- Culture — wound swab or aspirate of purulent material, to guide targeted therapy.
- Antibiotics — for SSIs with significant cellulitis (spreading erythema beyond 5 cm from the wound), systemic signs (fever, tachycardia, rising white cell count), or deep or organ-space infection. Empirically, cefazolin 2 g IV every 8 hours (or flucloxacillin 2 g IV every 6 hours) for clean-wound organisms; add metronidazole 500 mg IV every 8 hours for colorectal and gynaecological SSI; vancomycin 1.5 g IV every 12 hours for MRSA. De-escalate based on culture.
- Imaging — CT or ultrasound to identify deep collections or organ-space infection requiring drainage.
- Surgical debridement — for necrotising infection, deep space infection, or fascial dehiscence. [1]
Clostridioides difficile infection (CDI)

CDI is covered in detail in the antimicrobial stewardship topic. Here we focus on the HAI perspective and the exam-critical points. [1]
The connection to HAI
CDI is the HAI most directly linked to antibiotic prescribing. The pathogenesis is antibiotic-induced disruption of the normal colonic microbiome, which removes the competitive barrier (colonisation resistance) and allows C. difficile spores (ingested from the environment or present asymptomatically) to germinate, proliferate, and release toxins A and B that cause colonic inflammation, fluid secretion, and mucosal damage. The antibiotics most strongly associated with CDI are clindamycin, second- and third-generation cephalosporins, fluoroquinolones, and broad-spectrum penicillins — but ANY antibiotic can precipitate it [8] [14].
The NAP1/BI/027 hypervirulent strain (identified in the Quebec outbreak of 2002 to 2005 by Loo and colleagues [14]) carries a deletion in the tcdC gene (a negative regulator of toxin production), produces binary toxin, and is fluoroquinolone-resistant — features that drove its emergence and its association with severe, fulminant, and recurrent disease.
Diagnosis — the two-step algorithm
The recommended diagnostic approach is a two-step algorithm [8]:
- Glutamate dehydrogenase (GDH) — a sensitive screening test for the presence of C. difficile (detects a metabolic enzyme common to all strains). GDH-negative effectively rules out CDI. GDH-positive does not confirm it (it detects colonisation, not toxin production).
- Toxin enzyme immunoassay (EIA) — if GDH-positive, test for toxins A and B. Toxin-positive confirms CDI. Toxin-negative in a GDH-positive sample is indeterminate — either the patient is colonised without active toxin production (treatment not needed), or the toxin level is below the EIA detection threshold (treatment may be needed). [1]
An alternative is nucleic acid amplification testing (NAAT/PCR) for the toxin genes — highly sensitive and specific, but it detects the gene, not the toxin, so it may overdiagnose colonisation as active disease. The optimal strategy is GDH plus toxin EIA, with NAAT as a reflex test for GDH-positive, toxin-negative samples in patients with high clinical suspicion. [1]
A single GDH-positive but toxin-negative stool does NOT confirm CDI and should not be treated without clinical correlation — this is a common MCQ trap. [1]
Management — severity-stratified therapy
The 2018 IDSA/SHEA guideline, updated by the 2021 focused update [9], stratifies therapy by severity:
- Initial non-severe CDI (WBC below 15, creatinine below 1.5 times baseline) — fidaxomicin 200 mg orally twice daily for 10 days is the preferred first-line agent (2021 update), based on its lower recurrence rate compared to vancomycin [9] [11]. Oral vancomycin 125 mg four times daily for 10 days is an acceptable alternative. Metronidazole is no longer first-line for any adult CDI.
- Initial severe CDI (WBC 15 or above, or creatinine 1.5 times baseline or above) — fidaxomicin 200 mg twice daily for 10 days, OR oral vancomycin 125 mg four times daily for 10 days.
- Fulminant CDI (hypotension, shock, ileus, toxic megacolon) — oral vancomycin 500 mg four times daily PLUS intravenous metronidazole 500 mg every 8 hours, with a vancomycin rectal retention enema if ileus is present, and urgent surgical review for toxic megacolon or perforation [8].
- First recurrence — fidaxomicin 200 mg twice daily for 10 days, or a tapered and pulsed vancomycin course.
- Second or subsequent recurrence — fidaxomicin, tapered and pulsed vancomycin, or faecal microbiota transplantation (94 per cent cure after one or two infusions in the van Nood trial [12]).
- Recurrence prevention — bezlotoxumab (a single 10 mg/kg IV infusion of a monoclonal antibody against toxin B), given WITH antibiotic therapy, reduced 12-week recurrence from 26.6 to 16.5 per cent in the MODIFY trials, with the greatest benefit in high-risk patients (age above 65, severe episode, prior recurrence, immunocompromised) [10]. Note the FDA warning for heart failure exacerbation.
Infection control for CDI
CDI infection control differs from other HAIs in one critical respect: alcohol-based hand rub does NOT kill C. difficile spores — soap and water hand washing is required after every contact with a CDI patient. Other measures: single-room isolation with contact precautions, dedicated equipment, environmental cleaning with a sporicidal agent (hypochlorite bleach at 1000 to 5000 ppm), and surveillance for ward clusters (an outbreak warrants environmental investigation and enhanced cleaning) [8].
Multi-drug resistant organisms (MDROs)
The key MDROs in the hospital, their mechanisms of resistance, and their first-line agents are covered in the antimicrobial stewardship topic. Here we focus on the infection control prevention strategy: [1]
MRSA (methicillin-resistant Staphylococcus aureus)
MRSA carries the mecA gene encoding PBP2a (an altered penicillin-binding protein with low affinity for beta-lactams). Prevention: active surveillance (nasal swabs on admission to high-risk areas — ICU, transplant, dialysis, orthopaedic implant units), contact isolation for known or newly identified carriers, decolonisation (mupirocin nasal ointment twice daily for 5 days plus chlorhexidine body wash) for preoperative patients or during outbreaks, and hand hygiene. MRSA bacteraemia is a reportable quality metric in most healthcare systems. [1]
VRE (vancomycin-resistant enterococci)
VRE carry vanA or vanB genes encoding D-alanyl-D-lactate (which has low affinity for vancomycin). Prevention: contact isolation, active surveillance (rectal or stool swab), hand hygiene, and antimicrobial stewardship (restricting vancomycin and cephalosporins, which select for VRE). [1]
ESBL Enterobacteriaceae
ESBL producers (E. coli, Klebsiella) carry extended-spectrum beta-lactamases that hydrolyse penicillins, cephalosporins, and aztreonam. They are treated with carbapenems (meropenem, ertapenem). Prevention: contact isolation, active surveillance in high-risk settings, and antimicrobial stewardship. [1]
CRE (carbapenem-resistant Enterobacteriaceae)
CRE carry carbapenemases (KPC, NDM, OXA-48, VIM, IMP) that hydrolyse all beta-lactams including carbapenems. They carry mortality of 40 to 50 per cent in bacteraemia. Prevention: strict contact isolation, active surveillance (rectal swabs) for patients with epidemiological risk factors (recent hospitalisation overseas, transfer from a facility with known CRE, known prior colonisation), cohorting of CRE-positive patients with dedicated nursing staff during outbreaks, and molecular typing to identify cross-transmission. [1]
The unifying prevention principle
All MDRO prevention rests on the same foundation: hand hygiene, contact precautions, active surveillance, environmental cleaning, antimicrobial stewardship, and institutional commitment. The single most effective measure is hand hygiene — the WHO Five Moments framework is the global standard, and adherence is measurable and improvable. [1]
Hand hygiene — the WHO Five Moments
The WHO Five Moments for Hand Hygiene is the global standard for hand hygiene in healthcare, developed to translate the evidence on hand hygiene effectiveness into a simple, memorable framework applicable to every patient encounter: [1]
- Before touching a patient — protects the patient from the healthcare worker's flora.
- Before a clean or aseptic procedure — protects the patient from the healthcare worker's flora entering a sterile site (catheter insertion, wound care, injection, line access).
- After body fluid exposure risk — protects the healthcare worker and the environment from patient-derived organisms. This moment occurs after any contact with blood, body fluids, secretions, excretions, mucous membranes, non-intact skin, or wound dressings.
- After touching a patient — protects the healthcare worker and the environment from patient-derived organisms on intact skin.
- After touching patient surroundings — protects the healthcare worker and the environment from organisms on surfaces, equipment, and items in the patient's environment (bed rails, monitors, IV poles, charts). [1]
Alcohol-based hand rub is the preferred agent for Moments 1, 2, 4, and 5 — it is faster (20 to 30 seconds versus 40 to 60 seconds for soap and water), more effective against most organisms, less irritating to skin, and does not require a sink. Soap and water is required after visible soiling, after contact with spore-forming organisms (C. difficile, Bacillus anthracis), and after using the toilet. Alcohol-based hand rub does NOT kill spores — this is a critical distinction for CDI [8].
Infection control bundles and checklists — why they work
The evidence that care bundles reduce HAI is among the strongest in all of inpatient medicine. The Pronovost Michigan study is the landmark: a prospective cohort study of 103 ICUs implementing the five-component central line bundle reduced CLABSI rates from a median of 2.7 to 0 per 1000 catheter-days at 3 months, with a sustained reduction of up to 66 per cent at 18 months [1]. Similar reductions have been demonstrated for VAP, CAUTI, and SSI with their respective bundles.
The bundle concept — a small, straightforward set of evidence-based practices (typically 3 to 6 elements) that, when performed collectively and reliably, improve outcomes — works because of synergistic effect (components address different stages of pathogenesis), standardisation (every patient receives every evidence-based intervention every time), team culture and empowerment (the "stop the line" principle empowers nurses to halt a procedure if a bundle element is missed), and measurement with feedback (adherence rates are tracked and reported back to the team) [4].
The institutional infection control programme
Beyond individual bundles, a comprehensive institutional HAI prevention programme includes [2]: surveillance (measuring HAI rates by type, ward, and device, with benchmarking against the CDC NHSN standard); a hand hygiene programme (education, alcohol-based hand rub at every point of care, observation and feedback of adherence targeting above 80 per cent); PPE with training on donning and doffing technique; isolation (single-room contact, droplet, or airborne precautions as indicated); environmental cleaning and disinfection of patient rooms, shared equipment, and high-touch surfaces with quality monitoring; sterilisation and disinfection of reusable medical equipment; antimicrobial stewardship (reducing selection pressure for MDROs and CDI); and a defined outbreak response plan (environmental sampling, molecular typing, enhanced cleaning, cohorting, and communication).
Long-case integration — the multi-device patient
A postoperative or transplant patient with multiple devices (central line, urinary catheter, endotracheal tube, surgical wound) who develops fever on day 5 of admission presents a diagnostic and management challenge that models the DCE long case perfectly. The approach is: [1]
-
Assess severity — vital signs, lactate, organ dysfunction. If septic shock is present, manage as per the sepsis bundle (see sepsis topic) with empiric antibiotics and source control. [1]
-
Generate a differential based on the devices present — the line, the lungs, the urine, the wound, the colon (CDI), and consider non-device sources (drug fever, pulmonary embolism, transfusion reaction, pancreatitis). [1]
-
Obtain cultures before starting or changing antibiotics — paired blood cultures (peripheral plus central) for suspected CRBSI; endotracheal aspirate or BAL for suspected VAP; urine culture for suspected CAUTI; wound swab and imaging for suspected SSI; stool for C. difficile toxin if diarrhoea is present. [1]
-
Start empiric therapy calibrated to the likely source(s) and the patient's risk factors (recent antibiotics, known colonisation, severity). For the multi-device patient, this is often broad (vancomycin plus piperacillin-tazobactam) initially. [1]
-
De-escalate at 48 hours based on culture results and clinical response. This is the stewardship moment — narrowing therapy to the narrowest effective agent, switching from IV to oral when the patient is stable and absorbing, and defining a stop date. [1]
-
Remove devices — every device needs a daily indication, and removal is the single most effective infection prevention and treatment measure. If the line is the source, remove it. If the catheter is the source, remove or change it. If the patient can be extubated, extubate. [1]
-
Communicate and document — the management plan, the stewardship decisions, the infection control measures, and the patient and family discussion. [1]
Short-case examination — bedside assessment of the device-associated infection
The DCE short case may present a patient with a device in situ and ask you to perform a focused examination. The key points: [1]
For suspected CRBSI — examine the catheter exit site for erythema, induration, tenderness, and purulent discharge. For tunnelled lines, palpate the entire subcutaneous track for tenderness, induration, or fluctuance. For implanted ports, examine the pocket for overlying erythema, swelling, or purulent discharge. Examine for signs of systemic sepsis (fever, tachycardia, hypotension) and for signs of metastatic infection (new murmur suggesting endocarditis, spinal tenderness suggesting vertebral osteomyelitis). [1]
For suspected SSI — inspect the wound for erythema (measure the extent of spreading cellulitis from the wound edge), warmth, swelling, purulent discharge (note colour, quantity, and odour), and dehiscence (separation of the wound edges at the skin, fascial, or muscular layers). Palpate for fluctuance (suggesting an underlying collection) and surrounding induration. Assess for systemic signs (fever, tachycardia). Examine for signs of deep or organ-space infection (peritonitis suggesting intra-abdominal collection, joint swelling suggesting septic arthritis). [1]
For suspected CDI — examine for abdominal distension, tenderness (localised or generalised), reduced or absent bowel sounds (suggesting ileus), and signs of peritonism (guarding, rigidity, rebound) suggesting toxic megacolon or perforation. Assess hydration (dry mucous membranes, reduced skin turgor, hypotension, tachycardia) and signs of acute kidney injury. [1]
Exam traps and high-yield discriminators
The top MCQ traps
-
Treating catheter-associated asymptomatic bacteriuria — the single most common MCQ trap in the entire HAI topic. A patient with a urinary catheter, a positive urine culture, but no symptoms does NOT need antibiotics — except in pregnancy and before urological procedures. Treating it drives resistance, C. difficile, and adverse drug reactions [13].
-
Using alcohol-based hand rub for C. difficile — alcohol does not kill spores. Soap and water is required. This is a classic MCQ discriminator. [1]
-
A single positive blood culture from a central line diagnosing CRBSI — without a paired peripheral culture and differential time to positivity, a single positive line culture may be a contaminant. The paired culture strategy is essential. [1]
-
Treating a GDH-positive but toxin-negative stool as CDI — the two-step algorithm requires toxin positivity or NAAT positivity for active disease. GDH positivity alone reflects colonisation. [1]
-
Metronidazole as first-line for CDI — no longer first-line for any adult CDI. Use fidaxomicin or oral vancomycin for non-fulminant disease. [1]
-
Continuing surgical prophylaxis beyond 24 hours — prolonged prophylaxis does not prevent SSI and drives resistance and C. difficile. Stop at 24 hours (48 hours for cardiac surgery). [1]
-
Giving prophylactic antibiotics too late — the antibiotic must be in the tissue at the time of incision. Giving it after incision is equivalent to no prophylaxis. [1]
-
Using daptomycin for MRSA pneumonia — daptomycin is inactivated by pulmonary surfactant and is NEVER used for pneumonia. Use vancomycin or linezolid. [1]
The top DCE long-case traps
-
Not removing the device — leaving a central line, urinary catheter, or endotracheal tube in place when it is no longer needed. Daily review of necessity is the single most effective prevention measure. [1]
-
Not sending cultures before starting antibiotics — without cultures, de-escalation is impossible. This is both a clinical error and a stewardship failure. [1]
-
Not addressing the stewardship dimension — every HAI case deserves a documented review of the antibiotic exposures that contributed to it, and a plan to minimise future exposure. This demonstrates the integrated thinking that distinguishes a passing long-case candidate from a failing one. [1]
-
Not communicating the prevention plan to the patient and the team — a patient who has had an HAI deserves to understand what caused it, what was done about it, and what to do to prevent it in the future. The communication is part of the treatment. [1]
The bottom line for the exam
Healthcare-associated infections are largely preventable, and the prevention strategies are among the most evidence-based in all of medicine. The physician's role is to implement them reliably. Know the five types (CRBSI, VAP, CAUTI, SSI, CDI), their organisms, their diagnostic criteria (especially paired blood cultures and DTP for CRBSI, the two-step CDI algorithm, and the CAUTI versus CA-ASB distinction), their management pathways, and their prevention bundles (central line bundle, ventilator bundle, CAUTI strategy, surgical bundle, and stewardship for CDI). Know the WHO Five Moments for Hand Hygiene and the soap-and-water requirement for C. difficile spores. Know that antimicrobial stewardship and hand hygiene are the unifying prevention principles. And in every case, apply the rule that the safest device is the one that is not there — remove it when you can, and use it only when you must. Apply the central line bundle (hand hygiene, full barrier precautions, chlorhexidine prep, avoid the femoral site, daily review of necessity) for every central line insertion. Apply the ventilator bundle (head of bed elevated, daily sedation interruption, oral chlorhexidine, subglottic secretion drainage) for every ventilated patient. Avoid and remove urinary catheters whenever possible, and never treat asymptomatic bacteriuria. Give the right antibiotic at the right time for surgical prophylaxis, and stop at 24 hours. For CDI, use fidaxomicin first-line for non-fulminant disease and vancomycin plus IV metronidazole for fulminant disease. And in every case, apply the stewardship principle: send cultures before starting antibiotics, start broad when the patient is unstable, and NARROW to the narrowest effective agent at the 48-hour review [1] [8] [9].
References
- [1]Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU N Engl J Med, 2006.PMID 17192537
- [2]O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections Clin Infect Dis, 2011.PMID 21460264
- [3]Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America Clin Infect Dis, 2009.PMID 19489710
- [4]Li Y, Zhou J, Wang J, et al. Prevention of ventilator-associated pneumonia through care bundles: A systematic review and meta-analysis J Intensive Med, 2023.PMID 38028633
- [5]Muscedere J, Rewa O, McKechnie K, et al. Subglottic secretion drainage for the prevention of ventilator-associated pneumonia: a systematic review and meta-analysis Crit Care Med, 2011.PMID 21478738
- [6]Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America Clin Infect Dis, 2010.PMID 20175247
- [7]Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery Am J Health Syst Pharm, 2013.PMID 23327981
- [8]McDonald LC, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) Clin Infect Dis, 2018.PMID 29462280
- [9]Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults Clin Infect Dis, 2021.PMID 34164674
- [10]Wilcox MH, Gerding DN, Poxton IR, et al. Bezlotoxumab for Prevention of Recurrent Clostridium difficile Infection N Engl J Med, 2017.PMID 28121498
- [11]Louie TJ, Miller MA, Mullane KM, et al. Fidaxomicin versus vancomycin for Clostridium difficile infection N Engl J Med, 2011.PMID 21288078
- [12]van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal infusion of donor feces for recurrent Clostridium difficile N Engl J Med, 2013.PMID 23323867
- [13]Nicolle LE, Gupta K, Bradley SF, et al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America Clin Infect Dis, 2019.PMID 30895288
- [14]Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality N Engl J Med, 2005.PMID 16322602