Phys · infectious
HIV and AIDS
Also known as human immunodeficiency virus · HIV infection · acquired immunodeficiency syndrome · AIDS · advanced HIV disease
Consultant-physician-depth guide to HIV infection and AIDS — viral lifecycle and CD4 depletion, natural history from acute seroconversion to advanced immunodeficiency, 4th-generation diagnostic strategy, antiretroviral therapy classes and first-line regimens (tenofovir/emtricitabine/dolutegravir or bictegravir), the START trial and Treat-All, opportunistic infections by CD4 threshold, prophylaxis, IRIS, AIDS-defining malignancies, pregnancy and U equals U, PrEP and PEP, drug interactions, and chronic comorbidities — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
HIV and AIDS


The one-minute consultant answer
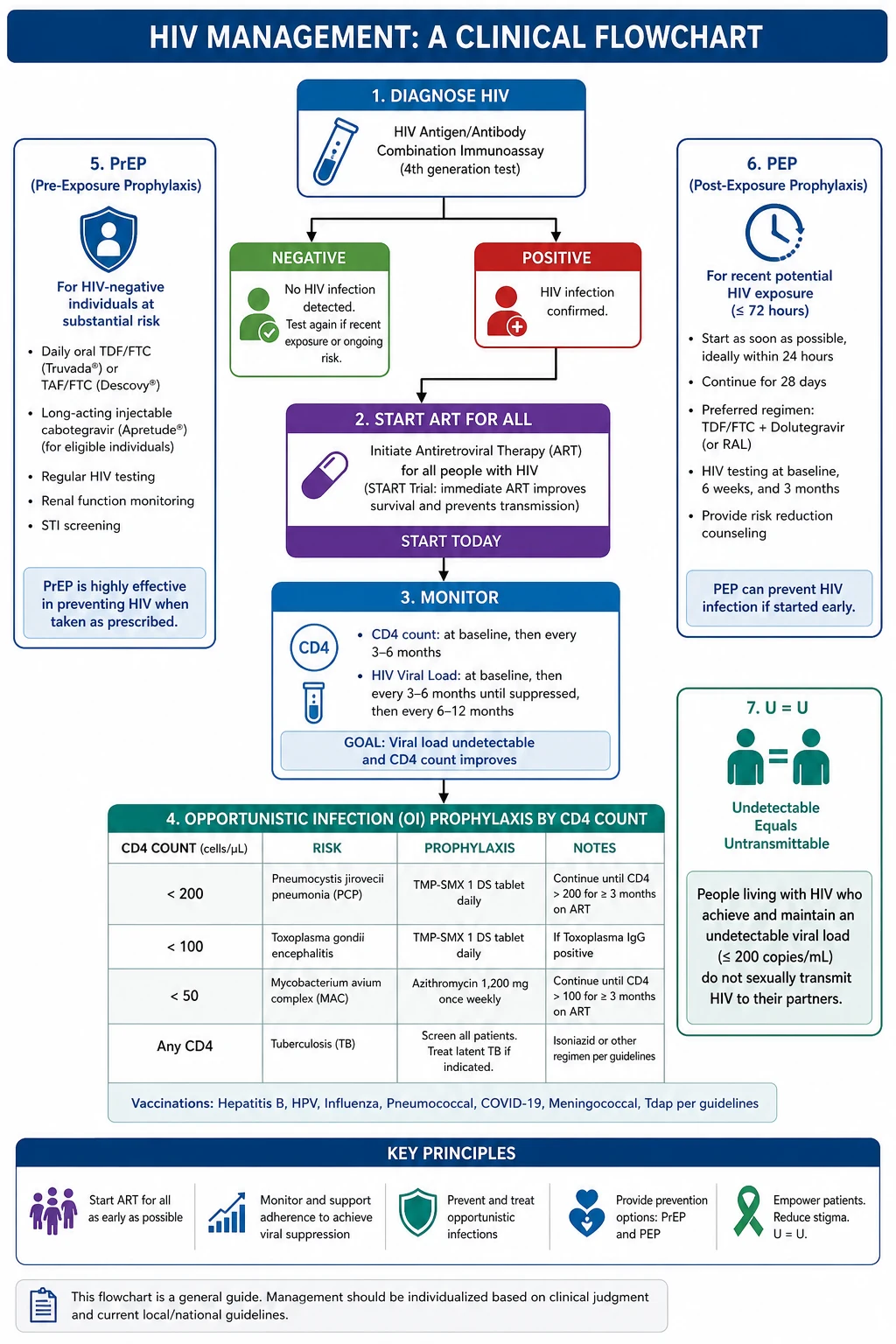
HIV is a retrovirus (HIV-1 is responsible for the global pandemic; HIV-2 is confined mainly to West Africa and runs a more indolent course) that infects and progressively depletes CD4-positive T-lymphocytes, producing a state of progressive cell-mediated immunodeficiency whose end stage is AIDS. The transforming principle of modern management is that antiretroviral therapy (ART) should be started in every person living with HIV regardless of CD4 count — a strategy validated by the START trial, which showed that immediate ART in asymptomatic patients with CD4 above 500 reduced serious AIDS and non-AIDS events by 57 per cent compared with deferring until CD4 fell below 350 [1]. Standard first-line therapy is a single-tablet regimen of tenofovir plus emtricitabine plus an integrase strand transfer inhibitor (dolutegravir or bictegravir), taken once daily, that achieves viral suppression (HIV RNA below 50 copies per millilitre) in over 90 per cent of patients within 12 to 24 weeks [7].
Once viral load is undetectable, the risk of sexual transmission is effectively zero — the principle of Undetectable equals Untransmittable (U equals U), confirmed by the PARTNER and PARTNER2 studies, which recorded zero phylogenetically linked transmissions across tens of thousands of condomless sex acts [3][4]. The physician's job is therefore fourfold: diagnose (4th-generation combination antigen/antibody test plus HIV RNA viral load), treat (start ART immediately, achieve and maintain viral suppression), prevent opportunistic infections by CD4 threshold (co-trimoxazole below 200; azithromycin below 50), and manage the long-term comorbidities of a now-chronic disease (cardiovascular disease, bone disease, renal disease, malignancy, neurocognitive impairment). Treatment interruption is harmful and must not be attempted [9].
Pathophysiology — the viral lifecycle and CD4 depletion

Understanding the viral lifecycle is not academic. Every antiretroviral drug is a targeted inhibitor of one of its steps, and knowing the target tells you the mechanism, the resistance pattern, and the interactions. [1]
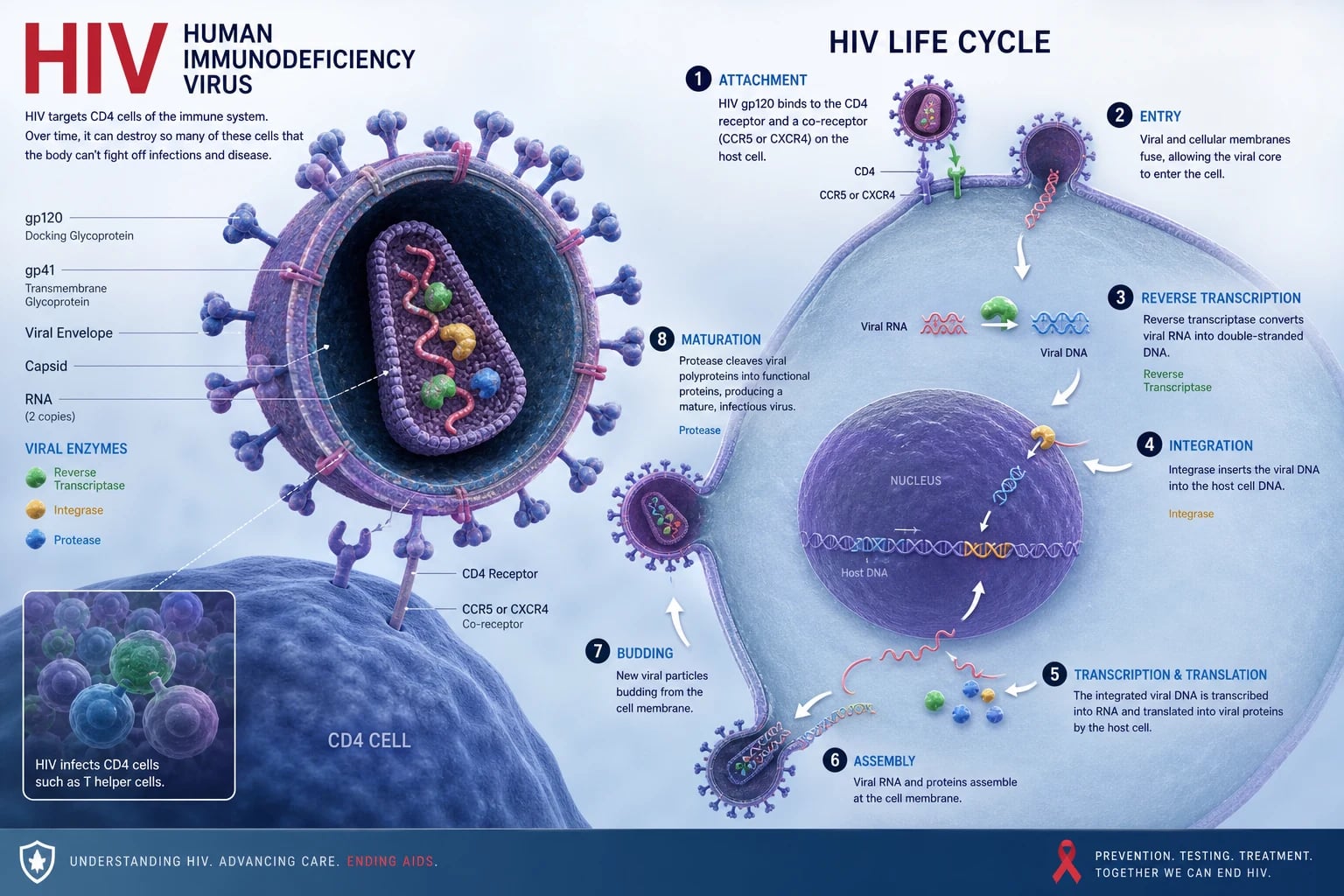
The six steps of the HIV lifecycle
-
Binding and entry. The HIV envelope glycoprotein gp120 binds CD4 on the surface of the T-helper lymphocyte (and macrophages, dendritic cells, and microglial cells). This binding induces a conformational change that exposes a co-receptor binding site. The virus then engages one of two chemokine co-receptors: CCR5 (the dominant co-receptor in early infection, present mainly on macrophages and memory T-cells — hence R5-tropic or M-tropic virus) or CXCR4 (present on naive T-cells — X4-tropic virus, which emerges later and is associated with more rapid CD4 decline). This is clinically important because maraviroc, a CCR5 antagonist, only works against R5-tropic virus — a tropism test is mandatory before use. [1]
-
Fusion. gp41 mediates fusion of the viral envelope with the host cell membrane, allowing the viral core to enter the cytoplasm. Enfuvirtide, a fusion inhibitor, blocks this step (it is an injectable peptide used only in salvage therapy). [1]
-
Reverse transcription. This is the defining act of a retrovirus. The viral reverse transcriptase converts the single-stranded RNA genome into double-stranded DNA. This enzyme is error-prone (no proofreading), generating roughly one mutation per genome per replication cycle — the molecular basis of HIV's extraordinary genetic diversity and its rapid acquisition of drug resistance. Nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) — tenofovir, emtricitabine, lamivudine, abacavir, zidovudine — are nucleoside analogues that terminate the growing DNA chain. Non-nucleoside reverse transcriptase inhibitors (NNRTIs) — efavirenz, nevirapine, rilpivirine, doravirine — bind allosterically to the enzyme and inhibit it non-competitively. [1]
-
Integration. The newly synthesised viral DNA enters the nucleus and is spliced into the host genome by the viral integrase enzyme. Once integrated, the viral DNA (now called a provirus) becomes a permanent part of the host cell's genome — it can remain transcriptionally silent (the latent reservoir) or be actively transcribed. This latent reservoir in resting memory CD4 cells is established within days of infection and is the fundamental reason HIV cannot be cured with current therapy. Integrase strand transfer inhibitors (INSTIs) — dolutegravir, bictegravir, raltegravir, elvitegravir — block this integration step. [1]
-
Translation and assembly. Host cell ribosomes translate viral messenger RNA into large polyprotein precursors. Viral proteins and RNA then assemble at the cell membrane into immature virions that bud outward. [1]
-
Maturation. The viral protease cleaves the polyproteins into functional proteins (capsid, nucleocapsid, enzymes), producing a mature, infectious virion. Protease inhibitors (PIs) — darunavir, atazanavir, lopinavir — block this cleavage step. Most PIs are boosted with ritonavir or cobicistat, which inhibit CYP3A4-mediated metabolism of the PI, raising drug levels — but this same inhibition creates extensive drug interactions. [1]
CD4 depletion — how HIV destroys the immune system
The cardinal pathophysiological event is the progressive loss of CD4-positive T-helper lymphocytes. This is not simply a matter of direct viral killing, though HIV does lyse infected cells. The depletion is multifactorial: [1]
- Direct cytopathic effects — viral replication and budding kill infected cells.
- Apoptosis — both infected and uninfected (bystander) CD4 cells undergo programmed cell death triggered by immune activation and envelope glycoprotein interactions.
- Pyroptosis — abortively infected resting CD4 cells die a highly inflammatory form of programmed cell death, releasing cytokines that drive chronic immune activation.
- Bone marrow and thymic effects — HIV impairs lymphopoiesis, reducing the production of new CD4 cells to replace those lost. [1]
The consequence is a progressive, relentless loss of cell-mediated (Th1-type) immunity. The body loses its ability to mount the delayed-type hypersensitivity and intracellular pathogen defence that depends on CD4 T-cells. The clinical correlate is a predictable ladder of opportunistic infections whose emergence tracks the falling CD4 count (see Opportunistic infections by CD4 count below). [1]
A second hallmark of untreated HIV is chronic immune activation — a state of persistent systemic inflammation driven by microbial translocation (lipopolysaccharide from compromised gut mucosa leaking into the systemic circulation), persistent viral antigen, and co-infections. This immune activation is now understood to be the primary driver of the non-AIDS comorbidities — cardiovascular disease, bone loss, renal disease, neurocognitive impairment, and malignancy — that dominate the clinical picture in the modern ART era. [1]
Natural history — from seroconversion to AIDS
The untreated course of HIV infection proceeds through three phases over a median of 8 to 10 years (highly variable: a minority are rapid progressors who develop AIDS within 3 years; a smaller minority are long-term non-progressors or elite controllers who maintain undetectable viral loads without ART). [1]
Stage 1: Acute HIV infection (seroconversion illness)
Acute infection occurs 2 to 4 weeks after exposure (range 1 to 6 weeks) and lasts 1 to 2 weeks. It is a mononucleosis-like illness caused by the massive initial burst of viral replication — viral load typically exceeds 1 million copies per millilitre and CD4 count transiently drops. It is missed at first presentation in over 50 per cent of cases because it mimics common viral illnesses. [1]
The classic features — the triad of fever, rash, and mucocutaneous ulcers — are the highest-yield discriminator for the exam: [1]
- Fever (present in over 80 per cent)
- Maculopapular rash (erythematous, on the trunk, face, palms and soles — present in 50 to 75 per cent)
- Mucocutaneous ulcers — painful ulcers on the oral mucosa, genitalia, or anus (highly suggestive when present)
- Lymphadenopathy (generalised)
- Pharyngitis (non-exudative)
- Myalgia, arthralgia, fatigue, headache, night sweats
- Aseptic meningitis (headache, photophobia) in a minority — HIV is one of the causes of lymphocytic meningitis in a young adult [1]
The exam trap: A young adult presenting with a glandular fever-like illness, particularly with a rash, mucosal ulcers, or aseptic meningitis, should be tested for acute HIV. Standard antibody tests may be negative during the window period — a HIV RNA viral load or p24 antigen is required. [1]
Stage 2: Clinical latency (chronic HIV infection)
After seroconversion, the immune system partially controls the virus and the patient enters a clinically latent phase that lasts a median of 8 years. "Latent" is a misnomer — there is no true virological latency. HIV replicates at a rate of approximately 10 billion virions per day, producing and destroying approximately 10 billion CD4 cells per day. The patient is infectious throughout this period. Viral load reaches a relatively stable plateau (the set point) — a higher set point predicts faster progression. [1]
Clinically, the patient may be asymptomatic, or may have:
- Persistent generalised lymphadenopathy
- Oral candidiasis (a sign of early immunodeficiency, appearing at CD4 around 300 to 500)
- Oral hairy leucoplakia (white corrugated lesions on the lateral tongue, caused by EBV — pathognomonic but not premalignant)
- Recurrent herpes zoster (shingles in a young person is a red flag for HIV)
- Recurrent oral or vulvovaginal candidiasis
- Idiopathic thrombocytopenic purpura (ITP — HIV is a classic cause) [1]
Stage 3: AIDS (advanced HIV disease)
AIDS is defined by the onset of AIDS-defining illnesses or a CD4 count below 200 cells per microlitre. Without ART, median survival from an AIDS diagnosis is 12 to 18 months. The clinical picture is dominated by opportunistic infections and malignancies whose type is predictable from the CD4 count (see below). [1]
Diagnosis — the modern testing algorithm
The 4th-generation combination antigen/antibody test
The recommended initial test is a laboratory-based 4th-generation HIV combination antigen/antibody immunoassay, which detects both HIV-1/HIV-2 antibodies and the p24 antigen (a core protein detectable before antibodies develop). The inclusion of p24 closes the diagnostic window to approximately 2 to 6 weeks after exposure (compared with 3 to 12 weeks for antibody-only 3rd-generation tests). [1]
| Test | What it detects | Window period | Role |
|---|---|---|---|
| 4th-gen Ag/Ab combo | p24 antigen + HIV-1/2 antibody | 2 to 6 weeks | First-line screening test |
| HIV-1/HIV-2 differentiation immunoassay | Antibody type | After reactive screening | Confirms and types (HIV-1 vs HIV-2) |
| HIV RNA viral load (PCR) | Viral RNA | 1 to 2 weeks | Diagnosis of acute infection; monitoring response to ART |
| Rapid point-of-care test | Antibody (some p24) | 4 to 12 weeks | Outreach, community, same-day results |
The diagnostic algorithm: A reactive 4th-generation screening test is followed by a supplementary differentiation assay (to confirm HIV-1 vs HIV-2 and exclude false positives). If acute infection is suspected (high-risk exposure within the window, mononucleosis-like illness) and the screening test is negative or indeterminate, perform a HIV RNA viral load — this is the most sensitive test in the first 1 to 2 weeks, when p24 may not yet be detectable. [1]
The exam trap: A negative antibody test in a patient with a mononucleosis-like illness and high-risk exposure 2 weeks ago does not exclude HIV. The patient is in the window period. Request a HIV RNA viral load. The false-negative window for the 4th-generation test is shorter than for older assays, but it still exists. [1]
The two laboratory monitoring pillars: CD4 count and viral load
Once diagnosed, two laboratory numbers govern every management decision: [1]
CD4 count (cells per microlitre) — the immunological report card. It tells you the current risk of opportunistic infections and guides prophylaxis. It is measured at diagnosis, before ART, and at intervals thereafter. Once a patient is stable on ART with suppressed viral load and CD4 consistently above 200, monitoring can be less frequent. CD4 recovery after ART is variable — most recovery occurs in the first year; some patients have limited immunological recovery (discordant responders — viral suppression without CD4 rise). [1]
HIV RNA viral load (copies per millilitre) — the virological report card. It is the primary measure of treatment efficacy. The target is viral suppression: below 50 copies per millilitre (below the limit of quantification). Viral load is checked at baseline, 2 to 8 weeks after starting ART (to confirm the early response), then every 3 to 6 months. A confirmed viral load above 200 copies per millilitre on ART is virological failure and triggers adherence assessment and resistance testing. [1]
Antiretroviral therapy — mechanism classes
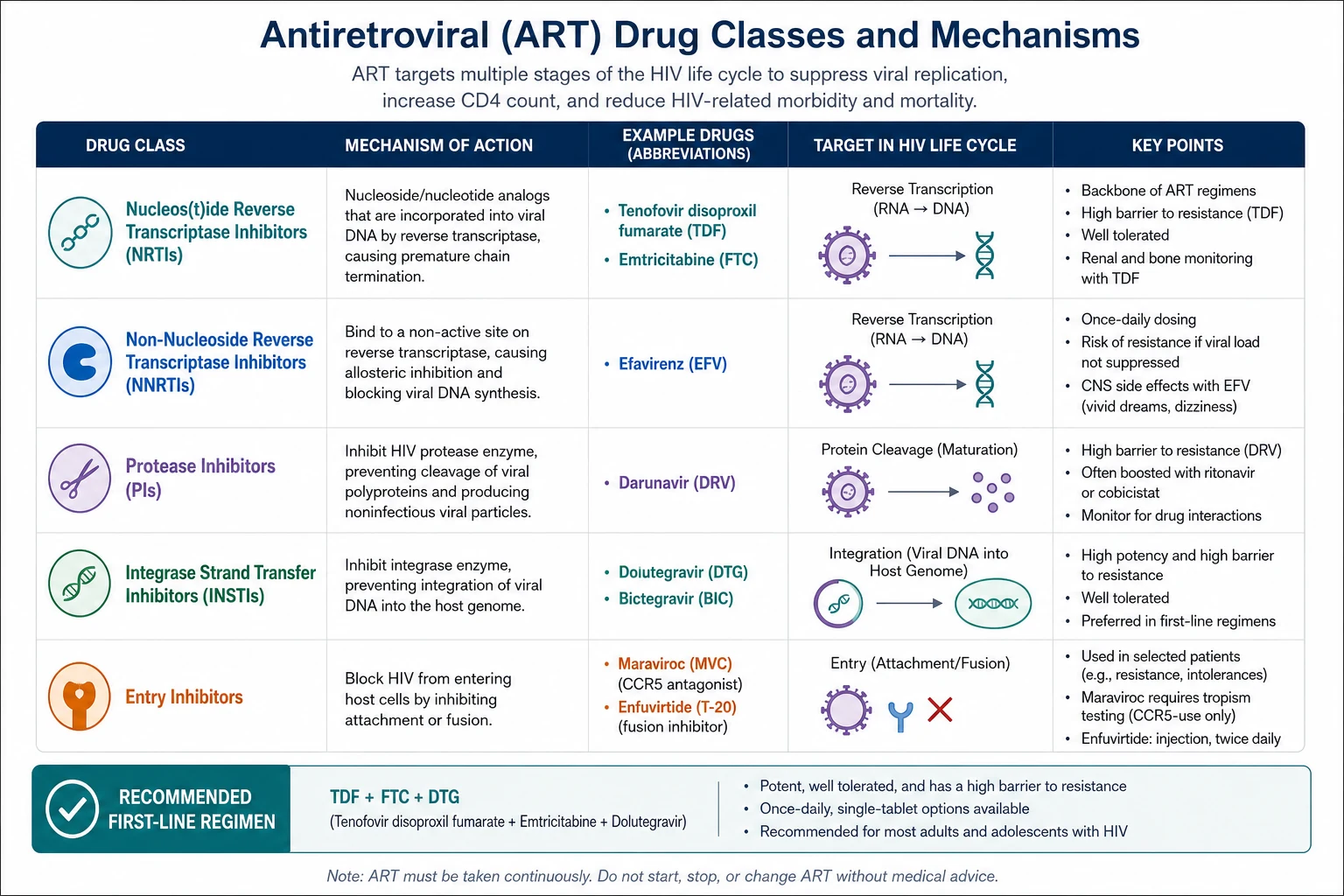
The six drug classes target the six steps of the viral lifecycle. The table maps mechanism to the drugs the examiner expects you to know. [1]
| Class | Mechanism (lifecycle step) | Key drugs | Notable adverse effects and notes |
|---|---|---|---|
| NRTI (nucleoside/nucleotide RT inhibitors) | Chain terminators of reverse transcription (step 3) | Tenofovir (TDF or TAF), emtricitabine (FTC), lamivudine (3TC), abacavir (ABC), zidovudine (AZT) | TDF: renal tubular dysfunction, bone loss. TAF: renal/bone safer. ABC: HLA-B*5701 hypersensitivity — screen before use. AZT: anaemia, mitochondrial toxicity (lipoatrophy) |
| NNRTI (non-nucleoside RT inhibitors) | Allosteric RT inhibition (step 3) | Efavirenz (EFV), nevirapine (NVP), rilpivirine (RPV), doravirine (DOR) | EFV: neuropsychiatric (vivid dreams, depression, suicidality), rash, teratogenic concern (now considered acceptable in pregnancy). NVP: hepatotoxicity, Stevens-Johnson syndrome. Low genetic barrier to resistance |
| INSTI (integrase strand transfer inhibitors) | Block viral DNA integration into host genome (step 4) | Dolutegravir (DTG), bictegravir (BIC), raltegravir (RAL), elvitegravir (EVG) | First-line backbone. High genetic barrier, excellent tolerability. DTG: weight gain, neuropsychiatric (insomnia, depression in a minority), early neural tube defect concern (now reassured — see Pregnancy). Drug interaction with metformin, antacids, polyvalent cations (chelation reduces absorption) |
| PI (protease inhibitors) | Block viral polyprotein cleavage (step 6) | Darunavir (DRV), atazanavir (ATV), lopinavir (LPV) — all boosted with ritonavir or cobicistat | Boosted PIs: extensive CYP3A4 interactions, gastrointestinal effects, lipids, insulin resistance, hepatotoxicity. DRV: rash. ATV: unconjugated hyperbilirubinaemia (benign), nephrolithiasis |
| Entry inhibitors | Block entry/fusion (steps 1 to 2) | Maraviroc (CCR5 antagonist), enfuvirtide (fusion inhibitor, injectable) | Maraviroc: requires tropism testing (only R5-tropic). Enfuvirtide: subcutaneous injections, injection-site reactions — salvage only |
| Capsid inhibitor (newer) | Disrupts capsid function | Lenacapavir (long-acting, subcutaneous every 6 months) | For heavily treatment-experienced patients with multidrug resistance |
The high-yield pharmacology points
- Abacavir hypersensitivity is HLA-B*5701-linked (fever, rash, gastrointestinal, respiratory). Screen HLA-B*5701 before prescribing; if positive, never rechallenge (fatal). This is a classic exam question.
- Tenofovir disoproxil fumarate (TDF) causes renal proximal tubular dysfunction (Fanconi-like syndrome) and reduces bone mineral density. Tenofovir alafenamide (TAF) achieves lower plasma levels and is safer for kidney and bone — preferred in CKD and osteoporosis.
- Boosted protease inhibitors (ritonavir- or cobicistat-boosted darunavir, atazanavir) are potent CYP3A4 inhibitors. This is the single most important drug-interaction class in HIV. They interact with statins (simvastatin is contraindicated — rhabdomyolysis risk), anticoagulants (rivaroxaban), corticosteroids (inhaled fluticasone levels skyrocket — Cushing syndrome), and many anti-infectives and cardiovascular drugs.
- Efavirenz causes neuropsychiatric effects — vivid dreams, insomnia, depression, suicidality — and is now avoided as first-line where alternatives exist. It was a cornerstone of early ART, but INSTIs have replaced it.
- Dolutegravir and other INSTIs are now first-line worldwide (WHO recommends DTG-based regimens for all adults and adolescents). Their advantages: high genetic barrier (resistance is rare), excellent tolerability, once-daily dosing, and high efficacy. The main newer concerns are weight gain (INSTIs and TAF are associated with more weight gain than older regimens) and a small risk of neuropsychiatric side effects (insomnia, mood changes). [1]
First-line ART and the START trial
The first-line regimen
The global consensus first-line regimen for treatment-naive adults is a single-tablet regimen (STR) combining two NRTIs with one INSTI: [1]
- Tenofovir (TDF or TAF) + emtricitabine (FTC) + dolutegravir (DTG) — or the co-formulated single tablet. This is the WHO-preferred first-line worldwide.
- Tenofovir + emtricitabine + bictegravir (BIC) — a co-formulated single tablet. Bictegravir has a profile similar to dolutegravir and is not available as a standalone (only co-formulated). [1]
Alternative backbones when tenofovir is contraindicated (significant renal disease): abacavir + lamivudine + dolutegravir (after confirming HLA-B*5701 negative). This was the regimen studied in the SINGLE trial, which demonstrated dolutegravir superiority over efavirenz-based therapy at week 48 (88 per cent versus 81 per cent suppression) [7].
The goal of therapy is durable viral suppression (HIV RNA below 50 copies per millilitre), CD4 recovery, and prevention of disease progression, transmission, and drug resistance. [1]
The START trial — Treat All, regardless of CD4
The START trial (Strategic Timing of AntiRetroviral Treatment) definitively answered the question that had dominated HIV medicine for two decades: when to start. It randomised 4,685 asymptomatic ART-naive adults with CD4 above 500 to immediate ART versus deferred ART (until CD4 fell below 350 or an AIDS-defining illness developed) [1].
The trial was stopped early by the data safety monitoring board because of clear benefit. The primary composite endpoint (serious AIDS events, serious non-AIDS events, or death) was reduced by 57 per cent with immediate ART (hazard ratio 0.43; 95 per cent CI 0.30 to 0.62). The benefit was driven by reductions in both AIDS events (tuberculosis, Kaposi sarcoma, lymphoma) and non-AIDS events (cancer, cardiovascular disease). [1]
START, together with the TEMPRANO trial (conducted in Cote d'Ivoire, which showed early ART reduced severe illness or death by 44 per cent and confirmed the benefit of isoniazid preventive therapy) [6], established the Treat All policy now endorsed by WHO, DHHS, BHIVA, and EACS: start ART in everyone living with HIV, on the day of diagnosis if possible, regardless of CD4 count or clinical stage.
The corollary: treatment interruption is harmful
The SMART trial tested the opposite strategy — CD4-guided treatment interruption (stop ART when CD4 is above 350, restart when it drops below 250) [9]. It was stopped early because the interruption arm had significantly higher rates of opportunistic disease and death (hazard ratio 2.6), and also higher rates of major cardiovascular, renal, and hepatic events (hazard ratio 1.7). The message: once started, ART is for life.
Monitoring the response to ART
- Viral load at 2 to 8 weeks (expect a drop of at least 1 log; most patients reach below 50 by 12 to 24 weeks), then every 3 to 6 months.
- CD4 count at intervals. Once CD4 is above 200 and stable with viral suppression, monitoring can be annual. If CD4 is below 200, continue opportunistic infection prophylaxis until CD4 recovers.
- Resistance testing (genotype) at baseline and at virological failure. [1]
Virological failure — the management algorithm
A confirmed viral load above 200 copies per millilitre on ART is virological failure. The steps: [1]
- Check adherence first. Non-adherence is by far the most common cause. A sensitive, non-judgemental conversation is essential.
- Drug levels (therapeutic drug monitoring) if available and appropriate.
- Resistance testing (genotype) — but this must be done while the patient is still taking the failing regimen, because resistant strains may be overgrown by wild-type virus once drugs are stopped.
- Never add a single new drug to a failing regimen — this monotherapy selects for resistance to the new agent.
- Construct a new regimen with at least two (ideally three) fully active drugs, guided by resistance testing and treatment history. This usually involves switching drug classes (e.g., adding a boosted PI or a second INSTI with a new NRTI backbone). [1]
Opportunistic infections by CD4 count
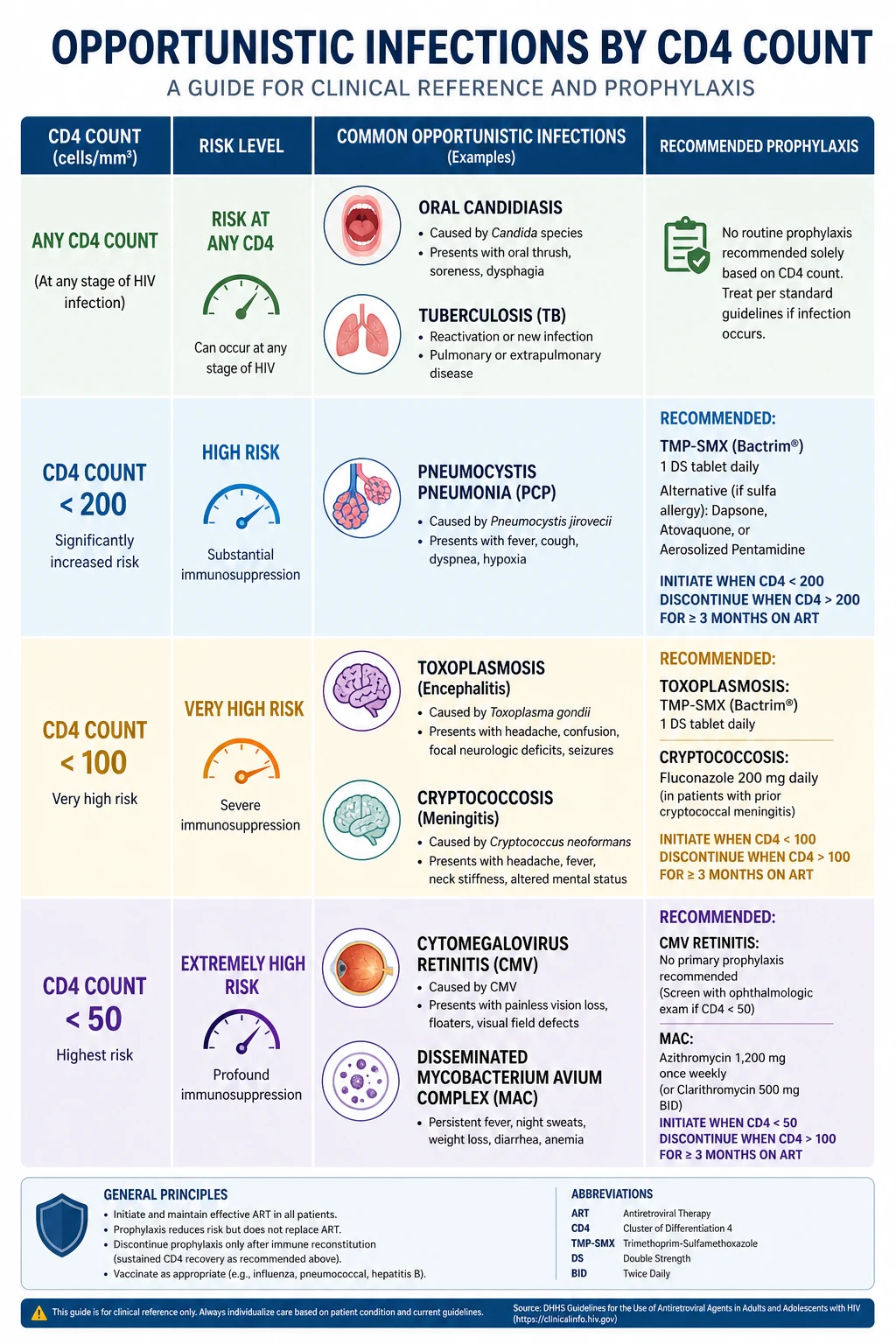
The single highest-yield framework in HIV medicine is the CD4-threshold ladder of opportunistic infections. The CD4 count predicts which infections a patient is at risk for, and this drives prophylaxis decisions. [1]
| CD4 count (cells per microlitre) | Opportunistic infections to expect | Notes |
|---|---|---|
| Any CD4 (including early infection) | Oral candidiasis, tuberculosis, recurrent bacterial pneumonia, herpes zoster, ITP | TB can occur at any CD4; it is the leading cause of death in HIV globally |
| Below 500 | Oral hairy leucoplakia, cervical dysplasia, anal dysplasia | Early immunodeficiency signs |
| Below 200 | Pneumocystis jirovecii pneumonia (PCP), oesophageal candidiasis, disseminated histoplasmosis, cryptococcal antigenaemia | PCP is the classic AIDS-defining pneumonia. Co-trimoxazole prophylaxis starts here |
| Below 100 | Toxoplasma gondii encephalitis, cryptococcal meningitis, microsporidiosis | Ring-enhancing brain lesions = toxoplasmosis until proven otherwise |
| Below 50 | Cytomegalovirus (CMV) retinitis, disseminated Mycobacterium avium complex (MAC), progressive multifocal leucoencephalopathy (PML, JC virus) | Azithromycin prophylaxis for MAC starts here. CMV retinitis is a sight-threatening emergency |
Pneumocystis jirovecii pneumonia (PCP)
PCP is the archetype AIDS-defining illness and the most common cause of pneumonia in patients with CD4 below 200. The clinical triad is subacute dyspnoea, dry cough, and fever over days to weeks. The classic radiographic finding is bilateral interstitial or ground-glass infiltrates, though the chest X-ray can be normal early. A key feature is desaturation on exertion — a drop in oxygen saturation with walking — out of proportion to the examination findings. Elevated serum lactate dehydrogenase (LDH) is a supportive but non-specific marker. [1]
Diagnosis is by demonstration of the organism in induced sputum or bronchoalveolar lavage (with immunofluorescence or PCR). [1]
Treatment is high-dose co-trimoxazole (trimethoprim-sulfamethoxazole at 15 to 20 mg/kg/day trimethoprim component, in 4 divided doses) for 21 days. Corticosteroids (prednisolone 40 mg twice daily, tapering) are added when the PaO2 is below 70 mmHg on room air or the alveolar-arterial gradient is elevated — they reduce mortality in moderate-to-severe PCP by reducing the inflammatory response to dying organisms. [1]
Toxoplasma gondii encephalitis
Toxoplasmic encephalitis occurs with CD4 below 100 and presents with subacute headache, fever, focal neurological deficits, or seizures. Imaging shows multiple ring-enhancing lesions, typically in the basal ganglia and corticomedullary junction. Serum toxoplasma IgG is positive in nearly all cases (reactivation of latent infection). [1]
Treatment is sulfadiazine plus pyrimethamine plus leucovorin for at least 6 weeks. Clinical and radiographic improvement within 2 weeks supports the diagnosis (and is the basis of the empiric-therapy approach). If there is no improvement, consider CNS lymphoma (the key differential — see below). Prophylaxis is co-trimoxazole (which covers both PCP and toxoplasma). [1]
Cryptococcal meningitis
Cryptococcal meningitis (Cryptococcus neoformans) occurs with CD4 below 100 and presents with subacute meningitis — headache, fever, malaise, sometimes altered mentation — that can evolve over weeks. Meningeal signs are often subtle or absent. A defining feature is a very high cerebrospinal fluid (CSF) cryptococcal antigen titre and elevated CSF opening pressure, which drives management. [1]
Diagnosis: CSF cryptococcal antigen (sensitivity over 99 per cent), India ink stain (positive in about 60 per cent), and culture. Serum cryptococcal antigen is also a sensitive screening test. [1]
Treatment is a three-phase strategy (per WHO and IDSA guidelines): induction with amphotericin B (deoxycholate or liposomal) plus flucytosine for at least 2 weeks; consolidation with high-dose fluconazole for 8 weeks; maintenance with fluconazole until immune reconstitution (CD4 above 100 for at least 6 months on ART). Therapeutic lumbar punctures to reduce intracranial pressure are critical — elevated pressure is a major determinant of mortality. [1]
CMV retinitis
CMV retinitis occurs with CD4 below 50 and is the most common sight-threatening opportunistic infection in AIDS. It presents with visual floaters, blurred vision, scotomata, or visual loss. Fundoscopy shows yellow-white retinal infiltrates with haemorrhage along vascular arcades — the classic "pizza pie" or "cottage cheese and ketchup" appearance. Diagnosis is clinical (fundoscopy). Treatment is valganciclovir (oral) or ganciclovir (intravenous), with immediate ophthalmology involvement. CMV disease can also cause colitis, oesophagitis, pneumonitis, and polyradiculopathy. [1]
Disseminated Mycobacterium avium complex (MAC)
Disseminated MAC occurs with CD4 below 50 and presents with fever, night sweats, weight loss, diarrhoea, abdominal pain, and anaemia (a high MCV anaemia is characteristic). It reflects disseminated infection of the reticuloendothelial system. Diagnosis is by blood cultures (mycobacterial) or tissue biopsy. Treatment is multi-drug therapy — typically a macrolide (azithromycin or clarithromycin) plus ethambutol, with rifabutin added in some cases. Prophylaxis is azithromycin 1200 mg once weekly for CD4 below 50. [1]
The brain lesion differential — toxoplasmosis versus lymphoma
When a patient with advanced HIV presents with a cerebral space-occupying lesion, the two leading diagnoses are toxoplasmosis and primary CNS lymphoma (EBV-associated). The discriminating features: [1]
| Feature | Toxoplasmosis | Primary CNS lymphoma |
|---|---|---|
| Number of lesions | Multiple (usually) | Often single (but can be multiple) |
| Location | Basal ganglia, corticomedullary junction | Periventricular, deep white matter |
| Ring enhancement | Multiple ring-enhancing | Often solid or ring-enhancing; subependymal spread |
| Toxoplasma IgG | Positive (in nearly all) | Can be positive or negative |
| Thallium SPECT / FDG-PET | Negative (no uptake) | Positive (avid uptake) |
| CSF EBV DNA PCR | Negative | Positive (highly suggestive) |
| Response to empiric toxo therapy | Improves within 2 weeks | No response |
The standard approach: if the patient has multiple ring-enhancing lesions and positive toxoplasma serology, start empiric anti-toxoplasma therapy and reassess at 2 weeks. Improvement confirms the diagnosis. No improvement, or a single lesion with negative serology, prompts brain biopsy or a trial of whole-brain radiotherapy for lymphoma. [1]
Opportunistic infection prophylaxis
Prophylaxis is the single most evidence-based and cost-effective intervention in advanced HIV. The thresholds are fixed and must be memorised. [1]
| CD4 threshold | Infection | Prophylaxis |
|---|---|---|
| Below 200 | Pneumocystis jirovecii pneumonia (and toxoplasmosis, if seropositive) | Co-trimoxazole 960 mg (one double-strength tablet) once daily |
| Below 50 | Disseminated Mycobacterium avium complex | Azithromycin 1200 mg once weekly (clarithromycin 500 mg twice daily as alternative) |
| Below 50 | CMV retinitis (if CMV seropositive) | No universal primary prophylaxis recommended — monitor with ophthalmology; valganciclovir in selected cases |
Co-trimoxazole is the workhorse. At one double-strength tablet daily it covers PCP, toxoplasmosis, and many bacterial respiratory infections. Prophylaxis can be discontinued once the CD4 count is above 200 for at least 3 months on ART (immune reconstitution to a safe threshold). [1]
In areas of high TB burden (including much of the ANZ tropical region and Asia-Pacific), isoniazid preventive therapy (IPT) after excluding active TB reduces TB disease — validated in the TEMPRANO trial [6].
Immune reconstitution inflammatory syndrome (IRIS)
IRIS is a paradoxical worsening of a known opportunistic infection (or the unmasking of a subclinical one) that occurs within weeks of starting ART, as the recovering immune system mounts an inflammatory response against microbial antigens. [1]
There are two patterns: [1]
- Paradoxical IRIS — a known, treated opportunistic infection (e.g., TB, cryptococcal meningitis) worsens after ART is started.
- Unmasking IRIS — a previously undiagnosed opportunistic infection declares itself as the immune system recovers. [1]
Risk factors for IRIS include a very low baseline CD4 count, a high antigen burden (disseminated infection), and early ART initiation in the setting of an untreated opportunistic infection. This creates a clinical tension for the most dangerous infections: TB-associated IRIS and cryptococcal IRIS can be life-threatening. For this reason, in cryptococcal meningitis, ART is deferred for 2 to 4 weeks after starting antifungal therapy (to reduce the antigen burden first). For TB, ART is started within 2 weeks if CD4 is below 50 (the CAMELIA and SAPiT trials showed mortality benefit), but within 8 weeks for higher CD4 counts. [1]
Management of IRIS: the key is recognition. ART is usually continued (do not stop it). The underlying infection is treated definitively. Corticosteroids are used for severe IRIS (particularly TB-IRIS with respiratory compromise or cryptococcal-IRIS with raised intracranial pressure), based on the prednisolone data from the CORTICUS-style IRIS trials. Mild IRIS (lymph node enlargement, fever) is managed with symptomatic treatment and reassurance. [1]
The exam trap: IRIS is not treatment failure, not drug resistance, and not a new infection. It is an inflammatory response to microbial antigen by a recovering immune system. The correct response is to treat the underlying infection, manage inflammation, and continue ART. [1]
HIV-related malignancies
Three malignancies are AIDS-defining: Kaposi sarcoma, non-Hodgkin lymphoma, and invasive cervical cancer. Their incidence has fallen dramatically with ART, but they remain important, especially in late presenters. [1]
Kaposi sarcoma
Kaposi sarcoma is caused by Kaposi sarcoma-associated herpesvirus (KSHV / human herpesvirus 8). It presents with violaceous (purple-brown) cutaneous plaques or nodules on the skin (face, trunk, extremities), oral mucosa (hard palate is classic), and can involve the gastrointestinal tract (bleeding) and lungs (dyspnoea, haemoptysis). The violaceous colour reflects the vascular proliferation. Diagnosis is biopsy. Treatment is ART (immune reconstitution often causes regression) plus, for extensive or visceral disease, chemotherapy (liposomal doxorubicin). [1]
Non-Hodgkin lymphoma
HIV-associated non-Hodgkin lymphoma is typically a high-grade B-cell lymphoma (diffuse large B-cell or Burkitt). It can be systemic or primary CNS lymphoma (EBV-associated). The risk is markedly elevated with low CD4 counts. Presentation depends on site — systemic symptoms (fever, sweats, weight loss), lymphadenopathy, extranodal masses, or neurological symptoms (CNS lymphoma). Treatment is ART plus R-CHOP or equivalent chemotherapy regimens (modified for immunocompetence), with CNS-directed therapy for primary CNS lymphoma. [1]
Cervical cancer
HIV is associated with persistent high-risk HPV infection and accelerated cervical intraepithelial neoplasia progression. Invasive cervical cancer is AIDS-defining. This underscores the importance of cervical screening (and increasingly anal screening) in people living with HIV. HPV vaccination is recommended. [1]
With effective ART, the incidence of all three AIDS-defining malignancies falls substantially — but non-AIDS-defining cancers (lung, liver, anal, Hodgkin lymphoma) become relatively more important in the ageing HIV population and are now a leading cause of death. [1]
HIV in pregnancy — prevention of vertical transmission
The principle that has transformed perinatal HIV is U equals U: when the maternal viral load is undetectable at delivery, the risk of vertical transmission is less than 1 per cent (compared with 15 to 45 per cent without intervention). The strategy has three components: [1]
- Maternal viral suppression throughout pregnancy — ART is started immediately (or continued) with a regimen safe in pregnancy. The goal is an undetectable viral load by the third trimester and especially by delivery.
- Mode of delivery — planned caesarean section at 38 weeks is recommended if the viral load is detectable (above the limit) near delivery. If the viral load is undetectable, vaginal delivery is acceptable (the risk is so low that caesarean adds no benefit).
- Neonatal prophylaxis — the infant receives ART for 2 to 6 weeks (longer if maternal viral load was high). Exclusive formula feeding (replacement feeding) eliminates breast-milk transmission where safe and affordable. Where formula feeding is not safe, ART during breastfeeding suppresses transmission risk to very low levels. [1]
The dolutegravir pregnancy question
In 2018, a preliminary signal from the Tsepamo study in Botswana raised concern that dolutegravir at conception was associated with neural tube defects (initial prevalence 0.94 per cent) [10]. This caused global guideline caution. However, with more data, the estimated prevalence fell to 0.10 to 0.30 per cent — a small or non-significant excess over background. By 2022, updated surveillance found no statistically significant association. WHO now recommends dolutegravir-based regimens for all adults and adolescents, including women of childbearing potential, weighing the substantial benefits (high efficacy, high barrier to resistance) against the now-reassuring safety data. Counselling about the (small) risk and the option of alternative regimens remains good practice, but dolutegravir is no longer avoided in women who might conceive.
U equals U — treatment as prevention
The PARTNER study (serodifferent couples, predominantly heterosexual, some MSM) [3] and PARTNER2 (exclusively gay male serodifferent couples) [4] together followed couples in which the HIV-positive partner was on suppressive ART (viral load below 200 copies per millilitre). Across over 126,000 acts of condomless sex, there were zero phylogenetically linked HIV transmissions. The upper bound of the 95 per cent confidence interval for the transmission risk was effectively zero.
This evidence, combined with the earlier HPTN 052 trial (which showed a 96 per cent reduction in transmission with early ART in serodiscordant couples) [2], established the consensus statement endorsed by WHO, CDC, UNAIDS, BHIVA, and ASHM: Undetectable equals Untransmittable (U equals U). A person living with HIV who maintains an undetectable viral load on ART cannot transmit HIV through sexual contact.
The clinical and psychosocial impact is profound: it removes the fear and stigma of infectiousness, supports ART adherence (a powerful motivation), and underpins the public health strategy of treatment as prevention (TasP). [1]
Pre-exposure and post-exposure prophylaxis
Pre-exposure prophylaxis (PrEP)
PrEP is the use of antiretrovirals by HIV-negative people at high risk of acquisition, to prevent infection. The landmark trial, iPrEx, showed that daily oral tenofovir disoproxil fumarate plus emtricitabine (TDF/FTC) reduced HIV acquisition by 44 per cent overall in men who have sex with men — but protection was strongly adherence-dependent, approaching 90 per cent or more in those with detectable drug levels [5]. Subsequent trials (PROUD, Partners PrEP, TDF2) confirmed high efficacy across populations.
Current PrEP practice:
- Daily oral TDF/FTC is the standard regimen (on-demand "2-1-1" dosing is an alternative for MSM, based on the IPERGAY trial). [1]- TAF/FTC is an alternative (renal/bone safer).
- Long-acting injectable cabotegravir (every 2 months) is a newer option (HPTN 083/084 showed superiority to daily oral PrEP).
- Indicated for people at ongoing high risk: condomless sex with HIV-positive or unknown-status partners, bacterial STI in past 6 months, people who inject drugs with sharing equipment, and serodiscordant couples attempting conception.
- Requires quarterly follow-up: HIV testing (to avoid starting PrEP during acute HIV, which selects resistance), renal monitoring (tenofovir), STI screening, and adherence support. [1]
The exam trap: Do not start PrEP during acute HIV infection. A person with acute HIV given only two drugs (TDF/FTC) is on inadequate therapy and will develop resistance. Always confirm HIV-negative status immediately before prescribing. [1]
Post-exposure prophylaxis (PEP)
PEP is ART given after a potential exposure to prevent establishment of infection. It must be started as soon as possible — ideally within 2 hours, and no later than 72 hours after exposure. The rationale is to extinguish the virus during the eclipse phase before it establishes the latent reservoir. [1]
Indications: occupational exposure (needlestick, mucous membrane splash) and non-occupational exposure (sexual assault, condom break, shared injecting equipment), following a risk assessment of the source and exposure type. [1]
Regimen: a 28-day course of a three-drug regimen — typically tenofovir + emtricitabine + dolutegravir (or raltegravir). Baseline HIV, hepatitis B and C, and liver/renal testing is performed; follow-up HIV testing at 4 to 6 weeks and 3 months. Hepatitis B vaccination status is checked and boosted if needed. [1]
Drug interactions — the CYP3A4 minefield
Drug interactions are among the most common causes of ART toxicity and failure in the modern era. The dominant offenders are the boosted protease inhibitors (ritonavir- and cobicistat-boosted darunavir, atazanavir, lopinavir), which are potent CYP3A4 inhibitors. [1]
| Interacting drug | Effect with boosted PI / cobicistat | Action |
|---|---|---|
| Simvastatin, lovastatin | Skyrocket levels — rhabdomyolysis | Contraindicated — use pravastatin or rosuvastatin (cautiously) |
| Inhaled or intranasal fluticasone, budesonide | Markedly elevated — iatrogenic Cushing syndrome, adrenal suppression | Avoid; use beclomethasone or fluticasone propionate with caution, or switch ART |
| Rivaroxaban, dabigatran | Increased anticoagulant effect — bleeding | Avoid or reduce dose; prefer alternatives |
| Rifampicin | Potent CYP3A4 inducer — drops PI levels to subtherapeutic — treatment failure | Contraindicated with PIs; use rifabutin (a weaker inducer) for TB co-treatment |
| Metformin | Dolutegravir inhibits renal tubular secretion — metformin levels rise | Monitor; reduce metformin dose |
| Antacids, calcium, iron supplements | Polyvalent cations chelate INSTIs (dolutegravir, bictegravir) — reduce absorption | Dose INSTI 2 hours before or 6 hours after polyvalent cation-containing products |
| Warfarin | Variable — monitor INR closely | Monitor |
| Macrolides (clarithromycin, erythromycin) | QT prolongation, elevated levels | Prefer azithromycin |
The exam principle: When a patient on a boosted PI presents with new symptoms, always consider a drug interaction before a new diagnosis. The most classic vignettes are Cushing syndrome from inhaled fluticasone and rhabdomyolysis from simvastatin. Always run an interaction checker (such as the Liverpool HIV drug interactions tool) before adding any drug to an ART regimen. [1]
Comorbidities of chronic HIV
With effective ART, people living with HIV now have a near-normal life expectancy. The clinical focus has shifted to the non-AIDS comorbidities that are driven by chronic inflammation, immune activation, drug effects, and the ageing of the cohort. These comorbidities are exactly what a DCE long-case examiner will probe. [1]
Cardiovascular disease
People living with HIV have an approximately 1.5 to 2-fold increased risk of cardiovascular disease (myocardial cardial infarction, stroke) compared with uninfected controls, even after controlling for traditional risk factors. This is driven by chronic inflammation, endothelial dysfunction, and dyslipidaemia. Some antiretrovirals contribute: the D:A:D study found that abacavir and didanosine were associated with an increased risk of myocardial infarction [8] (the abacavir signal remains debated but influenced prescribing). Boosted PIs worsen lipids and insulin resistance.
Management: aggressive cardiovascular risk factor modification — statin therapy (the REPRIEVE trial showed pitavastatin reduced major adverse cardiovascular events in HIV), blood pressure control, smoking cessation (smoking is the single biggest modifiable risk factor in this population), diabetes management. Avoid abacavir in patients with high cardiovascular risk where alternatives exist. Use the ASCVD risk calculator but consider HIV as an amplifier. [1]
Bone disease
People living with HIV have lower bone mineral density and higher fracture risk. Contributing factors: chronic inflammation, vitamin D deficiency, low body weight, and tenofovir disoproxil fumarate (TDF), which causes bone loss. TAF and INSTI-based switches are preferred in osteoporosis. DEXA scanning is recommended for older patients and those with risk factors. Standard osteoporosis treatment (bisphosphonates, vitamin D, calcium) applies. [1]
Renal disease
HIV-associated nephropathy (HIVAN, a collapsing focal segmental glomerulosclerosis seen predominantly in people of African descent) was a major cause of ESRD before ART; it is now uncommon with early treatment. TDF causes proximal tubular dysfunction (a Fanconi-like syndrome with phosphaturia and glycosuria). Patients with CKD should receive TAF instead of TDF and have renal function and phosphate monitored. Hypertension and diabetes (common comorbidities) drive most CKD in the modern era. [1]
Neurocognitive impairment
HIV-associated neurocognitive disorder (HAND) ranges from asymptomatic neurocognitive impairment to mild neurocognitive disorder to HIV-associated dementia (the severe form, now rare with ART). The milder forms persist in 20 to 50 per cent of treated patients and affect attention, executive function, and processing speed (subcortical pattern). The mechanism is chronic neuroinflammation. Screening (e.g., the International HIV Dementia Scale or MoCA) and managing reversible contributors (depression, substance use, cardiovascular risk) are the mainstay. CSF viral escape (detectable virus in CSF despite plasma suppression) is a rarer cause of neurological decline. [1]
Metabolic and body composition changes
Weight gain on INSTI-based and TAF-based regimens is increasingly recognised — it may be a "return to health" effect but can be substantial. Dyslipidaemia, insulin resistance, and lipoatrophy/lipohypertrophy (the latter now rare since older thymidine analogues and PIs were phased out) require monitoring and management. [1]
The integrated management algorithm
The consultation follows a fixed structure that mirrors what the examiner expects: [1]
- Confirm the diagnosis — reactive 4th-generation Ag/Ab test, supplementary differentiation assay. If acute infection suspected, HIV RNA.
- Baseline assessment — CD4 count, HIV RNA viral load, genotype resistance test, full blood count, renal and liver function, lipids, glucose, hepatitis B and C serology, syphilis, chlamydia and gonorrhoea screening, tuberculosis screening (interferon-gamma release assay or symptom screen), cervical/anal cytology, pregnancy test in women, cardiovascular risk assessment, mental health and substance use screening, vaccination status (hepatitis A and B, pneumococcal, influenza, COVID-19).
- Start ART immediately (Treat All) — first-line tenofovir (TDF or TAF) + emtricitabine + dolutegravir or bictegravir, as a single tablet once daily. Counselling on adherence, side effects, and U equals U. [1]4. Assess opportunistic infection risk — if CD4 below 200, start co-trimoxazole prophylaxis; if below 50, add azithromycin for MAC. Screen for and treat active opportunistic infections before or alongside ART (timing depends on the infection — defer ART 2 to 4 weeks for cryptococcal meningitis).
- Monitor — viral load at 2 to 8 weeks, then every 3 to 6 months; CD4 at intervals; watch for IRIS in the first weeks.
- Manage comorbidities — cardiovascular risk, bone, renal, metabolic, mental health, cancer screening, substance use.
- Prevent onward transmission — achieve and maintain undetectable viral load (U equals U); offer partner testing and PrEP for HIV-negative partners.
- Longitudinal care — lifelong ART, annual review of regimen (interactions, new comorbidities), vaccination, cancer screening, psychosocial support. [1]
High-yield exam discriminators
- Treat All — start ART in every person living with HIV regardless of CD4 count (START trial). Treatment interruption is harmful (SMART trial).
- First-line ART — tenofovir + emtricitabine + dolutegravir or bictegravir (an INSTI), as a single daily tablet. [1]3. U equals U — undetectable viral load means effectively zero sexual transmission (PARTNER, PARTNER2, HPTN 052).
- CD4 thresholds drive prophylaxis — co-trimoxazole below 200 (PCP and toxoplasma); azithromycin below 50 (MAC).
- Acute seroconversion is missed — test for HIV RNA in a mononucleosis-like illness with rash, mucosal ulcers, or aseptic meningitis; antibody tests may be negative.
- 4th-generation Ag/Ab combo is the screening test; the p24 antigen closes the window to 2 to 6 weeks. HIV RNA is the most sensitive test for acute infection.
- Abacavir and HLA-B*5701 — screen before use; never rechallenge a positive patient (fatal hypersensitivity).
- Virological failure — check adherence first, then resistance; never add a single new drug to a failing regimen.
- IRIS is not failure — it is immune recovery; treat the underlying infection and usually continue ART; corticosteroids for severe cases.
- Boosted PIs and CYP3A4 — simvastatin is contraindicated (rhabdomyolysis); inhaled fluticasone causes Cushing syndrome; rifampicin causes treatment failure (use rifabutin).
- Cerebral ring-enhancing lesions in advanced HIV — treat empirically for toxoplasmosis first (if seropositive); no response at 2 weeks or single lesion with negative serology, consider CNS lymphoma.
- Dolutegravir in pregnancy — the Tsepamo neural tube defect signal is now reassured; WHO recommends DTG for women of childbearing potential.
- PrEP — daily TDF/FTC; never start during acute HIV (resistance risk). PEP — within 72 hours, 28-day three-drug course. [1]
Regional guideline deltas
| Aspect | ANZ (ASHM / ASID) | UK (BHIVA / BASHH) | US (DHHS / CDC) |
|---|---|---|---|
| First-line ART | TDF or TAF + FTC + DTG (or BIC) | TAF + FTC + DTG (or BIC) | TAF + FTC + DTG (or BIC) |
| When to start | Immediately, all patients (Treat All) | Immediately, all patients | Immediately, all patients |
| PrEP | Daily or on-demand TDF/FTC (subsidised via PBS) | Daily TDF/FTC or TAF/FTC; on-demand for MSM | Daily TDF/FTC or TAF/FTC; injectable cabotegravir |
| PCP prophylaxis | Co-trimoxazole, CD4 below 200 | Co-trimoxazole, CD4 below 200 | Co-trimoxazole, CD4 below 200 |
| Pregnancy | DTG acceptable with counselling; aim undetectable by delivery | DTG acceptable; undetectable allows vaginal delivery | DTG preferred; undetectable allows vaginal delivery |
In the ANZ setting, ASHM (Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine) publishes the local guidance and PrEP is accessible through the PBS. BHIVA is the UK authority. The DHHS/CDC guidelines are the US standard and are among the most detailed globally. WHO provides the global framework, with particular emphasis on TB-HIV co-management and dolutegravir-based regimens for low- and middle-income settings. [1]
Communication and shared decision-making
HIV diagnosis carries enormous psychosocial weight. The physician must address the medical and the human dimensions: [1]
- At diagnosis: explain that HIV is now a manageable chronic condition with near-normal life expectancy on ART. Address stigma, confidentiality, partner notification (a legal and ethical obligation in most jurisdictions — facilitated, supportive, not punitive), and the immediate support available. Offer to start ART the same day.
- U equals U counselling: this is one of the most powerful messages a clinician can deliver. "If your viral load is undetectable, you will not pass HIV to your sexual partners." This transforms the patient's self-image, relationships, and adherence.
- Adherence: frame ART as a daily, lifelong commitment. Link doses to routines. Address side effects promptly (do not let the patient suffer in silence — switch regimens). Use motivational interviewing. [1]- Comorbidity screening and prevention: the long-term patient is a patient with cardiovascular, bone, renal, metabolic, and cancer risk — manage these proactively, as you would in any chronic disease.
- Reproductive health: women living with HIV can have HIV-negative children. Explain the perinatal strategy and offer pre-conception counselling. Offer PrEP to serodiscordant couples attempting conception.
- End-of-life and advance care planning: in late presenters with advanced disease, or in non-adherent patients with resistant virus, have honest conversations about prognosis, goals, and the role of palliative care alongside disease-directed therapy. [1]
Summary: the HIV consultation in one paragraph
Test for HIV with a 4th-generation combination antigen/antibody assay in every adult at risk and in every patient with a mononucleosis-like illness, and confirm with a differentiation assay and viral load. Start ART immediately with tenofovir plus emtricitabine plus dolutegravir or bictegravir — Treat All, regardless of CD4 count. Target an undetectable viral load (below 50 copies per millilitre), which confers near-normal life expectancy and zero sexual transmission (U equals U). Give co-trimoxazole prophylaxis if CD4 is below 200 and azithromycin if below 50. Watch for IRIS in the first weeks of ART. Manage drug interactions aggressively — boosted protease inhibitors are a CYP3A4 minefield. Address the chronic comorbidities of cardiovascular disease, bone loss, renal disease, neurocognitive impairment, and malignancy with the same rigour applied to any chronic disease. Never interrupt therapy. Offer PrEP to HIV-negative partners and PEP within 72 hours of exposure. Frame HIV as a chronic, manageable condition — because with ART, it is. [1]
References
- [1]INSIGHT START Study Group, Lundgren JD, Babiker AG, Gordin F, et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection N Engl J Med, 2015.PMID 26192873
- [2]Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy N Engl J Med, 2011.PMID 21767103
- [3]Rodger AJ, Cambiano V, Bruun T, et al. Sexual Activity Without Condoms and Risk of HIV Transmission in Serodifferent Couples When the HIV-Positive Partner Is Using Suppressive Antiretroviral Therapy JAMA, 2016.PMID 27404185
- [4]Rodger AJ, Cambiano V, Bruun T, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study Lancet, 2019.PMID 31056293
- [5]Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men N Engl J Med, 2010.PMID 21091279
- [6]TEMPRANO ANRS 12136 Study Group, Danel C, Moh R, et al. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa N Engl J Med, 2015.PMID 26193126
- [7]Walmsley SL, Antela A, Clumeck N, et al. Dolutegravir plus abacavir-lamivudine for the treatment of HIV-1 infection N Engl J Med, 2013.PMID 24195548
- [8]Sabin CA, Worm SW, Weber R, et al. (D:A:D Study) Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaboration Lancet, 2008.PMID 18387667
- [9]Strategies for Management of Antiretroviral Therapy (SMART) Study Group, El-Sadr WM, Lundgren J, et al. CD4+ count-guided interruption of antiretroviral treatment N Engl J Med, 2006.PMID 17135583
- [10]Zash R, Holmes L, Diseko M, et al. Neural-Tube Defects and Antiretroviral Treatment Regimens in Botswana N Engl J Med, 2019.PMID 31329379