Phys · infectious
Infections in the Immunocompromised Host
Also known as febrile neutropenia · neutropenic sepsis · neutropenic fever protocol · opportunistic infection · immunocompromised host · infection in the cancer patient · transplant infection timeline · post-transplant lymphoproliferative disorder · overwhelming post-splenectomy infection · OPSI · invasive aspergillosis · CMV disease · hepatitis B reactivation · anti-TNF tuberculosis
Consultant-physician-depth guide to the febrile immunocompromised patient — the central principle that the TYPE of immune defect predicts the organism, empiric therapy, and prophylaxis. Covers neutropenic fever (post-chemotherapy, AML induction) with the door-to-antibiotic protocol and piperacillin-tazobactam, the IDSA threshold of temperature above 38.3 single or above 38 sustained with neutrophils below 0.5, and G-CSF prophylaxis. Cellular immunodeficiency (HIV CD4-based; transplant 0 to 1 month nosocomial, 1 to 6 months opportunistic, above 6 months community) with PCP, Toxoplasma, Cryptococcus, HSV, VZV, CMV, MAC. Humoral immunodeficiency (myeloma, CLL, splenectomy) with encapsulated bacteria and vaccination. The solid organ transplant infection timeline, biologic therapy infections (anti-TNF and TB, rituximab and HBV, alemtuzumab and CMV), prophylaxis strategies (co-trimoxazole for PCP, valganciclovir for CMV D+/R-, fluconazole in high-risk neutropenia), and vaccination including avoidance of live vaccines — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Infections in the Immunocompromised Host

The one-minute consultant answer
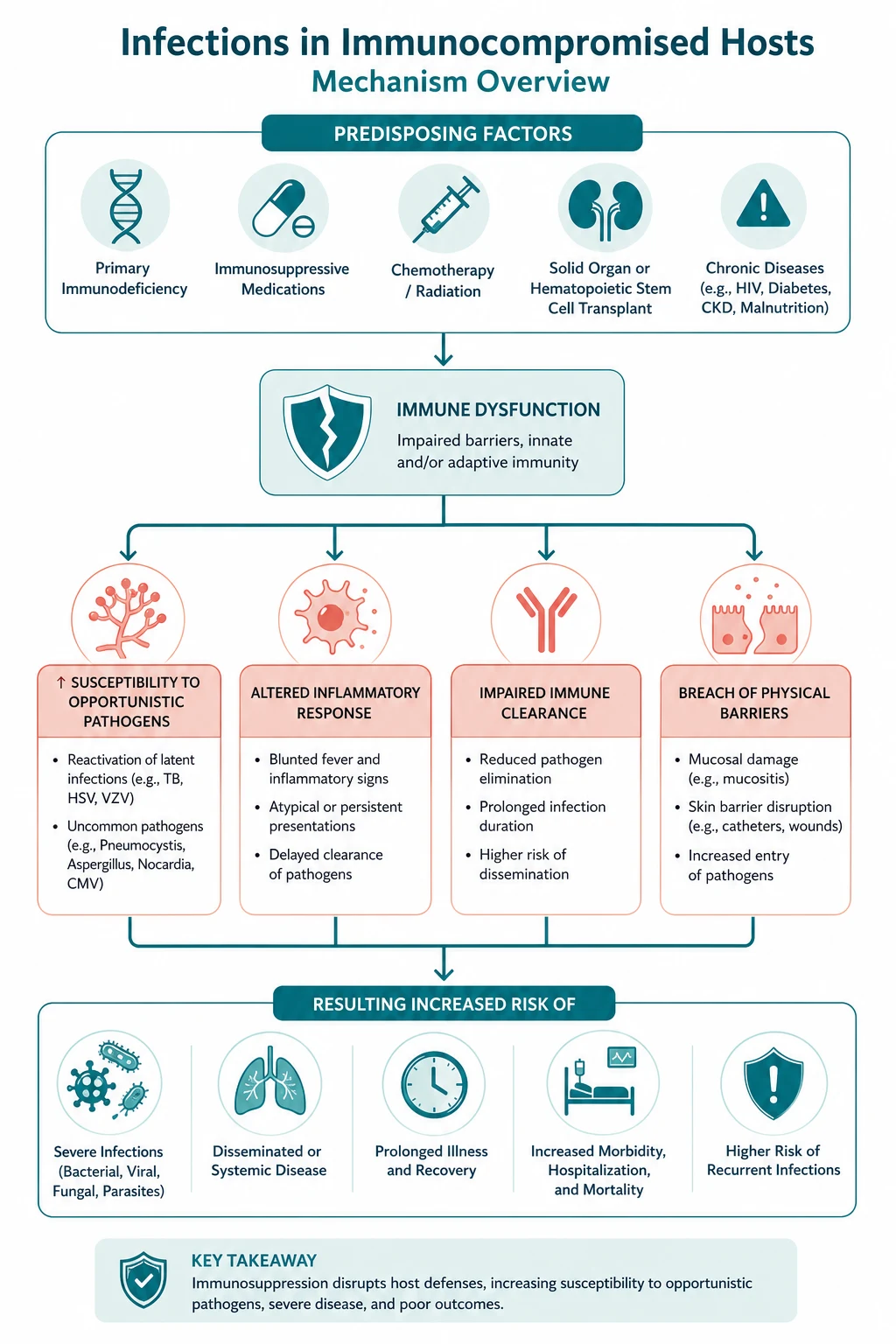
A fever in an immunocompromised patient is a different disease from a fever in a normal host, because the type of immune defect predicts the organism, the empiric therapy, and the prophylaxis. The single most important question at the bedside is therefore what is the type of immunodeficiency? — and the answer divides every patient into one of five buckets that drive the rest of the encounter. [1]
Neutropenia (most often post-chemotherapy, classically AML induction, when neutrophils fall below 0.5) is a medical emergency: febrile neutropenia is defined as a single temperature above 38.3 degrees or a sustained temperature above 38 for over one hour in a patient with a neutrophil count below 0.5, and the door-to-antibiotic time must be within one hour [1]. The empiric regimen is an antipseudomonal beta-lactam — piperacillin-tazobactam 4.5 g IV in the ANZ setting — given immediately after blood cultures, because Pseudomonas aeruginosa bacteraemia can kill within hours and the empiric cover must include it from the first dose. A Cochrane review of 71 trials confirmed that beta-lactam monotherapy is as effective as beta-lactam plus aminoglycoside combination with less toxicity [2], and another Cochrane review established that routine G-CSF does not reduce mortality in established febrile neutropenia [3].
Cellular immunodeficiency (HIV by CD4 count; transplant by time since engraftment) opens the door to the opportunistic organisms: PCP, Toxoplasma, Cryptococcus, CMV, HSV, VZV, MAC, and the endemic fungi. Humoral immunodeficiency (multiple myeloma, CLL, splenectomy) is the home of the encapsulated bacteria — S. pneumoniae, H. influenzae, N. meningitidis — and overwhelming post-splenectomy infection (OPSI), which is prevented by vaccination, prophylactic penicillin, and a standby-antibiotic plan. Solid organ transplant follows a timeline — month 0 to 1: donor-derived, nosocomial, wound; months 1 to 6: opportunistic (CMV, BK, PCP, Aspergillus, EBV); beyond 6 months: community-acquired. And biologic therapy has its own signature: anti-TNF reactivates TB (median 12 weeks, often extrapulmonary) [7]; rituximab reactivates HBV even from resolved infection (which is why every patient must be screened with HBsAg and anti-HBc and given prophylactic entecavir or tenofovir) [5].
The non-negotiable principles: screen before you suppress (TB before anti-TNF; HBV before rituximab or chemotherapy; strongyloides before steroids in anyone from a tropical area; vaccinations before immunosuppression begins); give prophylaxis that works (co-trimoxazole for PCP; valganciclovir for CMV D+/R-; fluconazole or posaconazole in high-risk neutropenia); and never give a live vaccine to a severely immunosuppressed patient [6].
The central framework — the type of defect predicts the organism
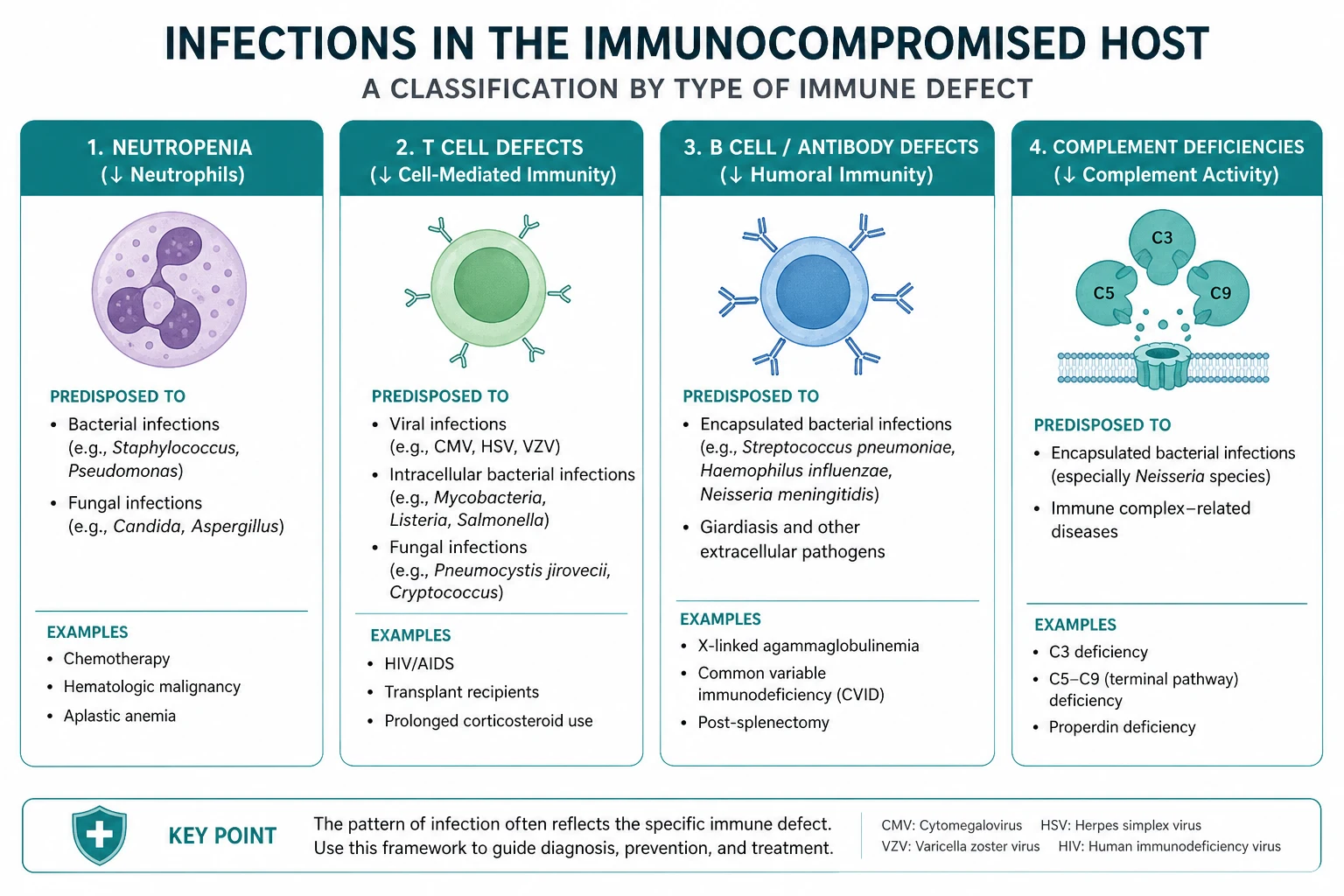

Every immunocompromised patient who arrives with a fever falls into one of five categories. Each category has its own organism list, its own empiric therapy, and its own prophylaxis. Memorise the categories and the rest follows. [1]
| Type of defect | Typical setting | Characteristic organisms | Empiric therapy |
|---|---|---|---|
| Neutropenia (phagocyte defect) | Post-chemotherapy (AML induction), HSCT pre-engraftment, aplastic anaemia | Gram-negative bacilli (Pseudomonas, E. coli, Klebsiella), Gram-positive (coagulase-negative staph, Strep viridans), Candida, Aspergillus | Antipseudomonal beta-lactam (piperacillin-tazobactam); add vancomycin for line infection or sepsis |
| Cellular (T-cell) defect | HIV (by CD4), transplant (months 1 to 6), high-dose steroids, anti-TNF | PCP, Toxoplasma, Cryptococcus, HSV, VZV, CMV, MAC, Listeria, endemic fungi, mycobacteria | Syndrome-directed; reduce immunosuppression; treat the specific organism |
| Humoral (B-cell/complement) defect | Multiple myeloma, CLL, splenectomy, CVID, eculizumab | Encapsulated bacteria (S. pneumoniae, H. influenzae, N. meningitidis), Capnocytophaga, Babesia | Ceftriaxone (cover pneumococcus and meningococcus); add vancomycin if meningitis |
| Solid organ transplant (timeline) | Kidney, liver, heart, lung | Month 0 to 1: nosocomial, donor-derived. Months 1 to 6: CMV, BK, PCP, Aspergillus, EBV. Beyond 6: community | By timeline and syndrome; reduce immunosuppression for opportunistic infection |
| Biologic therapy | Anti-TNF, rituximab, alemtuzumab, tocilizumab | TB (anti-TNF), HBV and PML (rituximab), CMV (alemtuzumab), bowel perforation (tocilizumab) | Stop or reduce the biologic; treat the reactivated organism |
The exam trap: the question stem will name the immune defect (chemotherapy, transplant, anti-TNF, splenectomy, CD4 count) — and the correct answer is the organism or the empiric therapy that matches it. A neutropenic-fever vignette expects an antipseudomonal beta-lactam; an asplenic-fever vignette expects ceftriaxone and a discussion of OPSI; a transplant-month-4 vignette expects CMV. [1]
Neutropenic fever — the protocol that must be automatic

The definition and why it matters
Febrile neutropenia is defined as a single oral temperature above 38.3 degrees Celsius, or a sustained temperature above 38 degrees for over one hour, in a patient with an absolute neutrophil count below 0.5 x 10^9 per litre (or below 1.0 and expected to fall) [1]. The reason the threshold is set so low and the urgency so high is that the neutropenic patient cannot mount a local inflammatory response — the classic signs of infection (induration, exudate, consolidation, infiltrate on chest X-ray) are often absent, and fever may be the only sign of a rapidly progressive bacteraemia.
The IDSA 2011 guideline frames the protocol as a door-to-antibiotic time of within one hour [1]. This is not arbitrary: untreated Pseudomonas bacteraemia in neutropenia has a mortality that climbs hour by hour, and delayed first antibiotic is the single greatest predictor of death. The cultures are taken immediately before the first dose, but the antibiotic is never delayed for the cultures, the count, or any investigation.
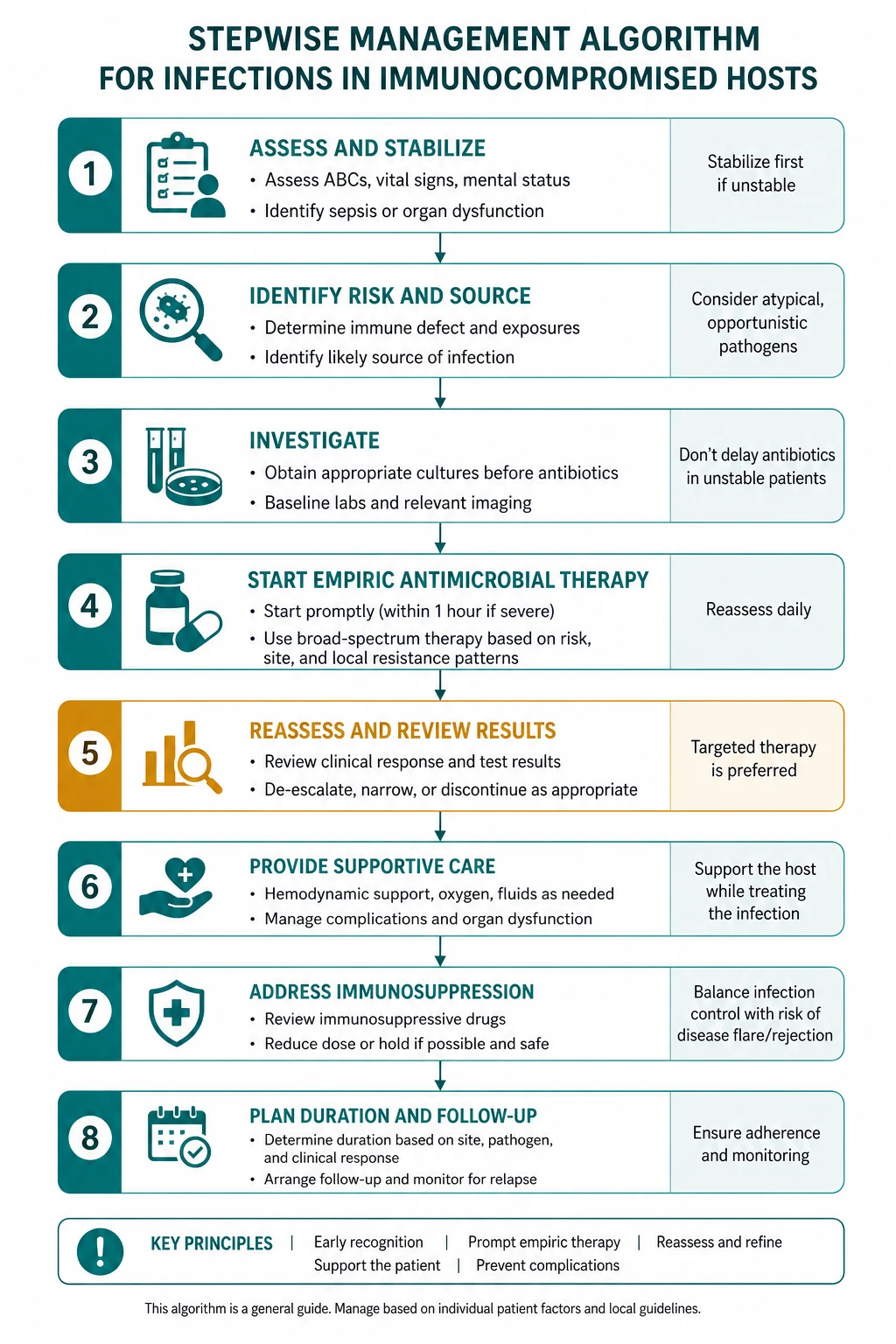
The protocol, step by step
- Recognise it. Any patient on chemotherapy (or with a known low neutrophil count) with a temperature above 38 has febrile neutropenia until proven otherwise. Triage to a resuscitation bay; alert the treating team.
- Resuscitate in parallel. Airway, breathing, circulation. Septic shock gets crystalloid (30 mL/kg), early vasopressors (noradrenaline first-line), and lung-protective ventilation if ARDS develops. Lactate identifies occult hypoperfusion.
- Culture, then dose — within one hour. Two sets of blood cultures: one peripheral, and one from each lumen of the central venous catheter (paired cultures help diagnose catheter-related bloodstream infection by differential time to positivity). Send urinalysis and culture, swab any obvious source (line site, perianal area, mucositis), stool for C. difficile if diarrhoea, and a chest X-ray. Then give the first dose of the empiric antipseudomonal beta-lactam immediately — do not wait for any result.
- The empiric regimen — an antipseudomonal beta-lactam. In ANZ practice the first-line agent is piperacillin-tazobactam 4.5 g intravenously every 6 to 8 hours (extended or continuous infusion in some units). Alternative equivalent agents are cefepime (a fourth-generation cephalosporin with no anaerobic cover — add metronidazole if anaerobes are a concern), or a carbapenem (meropenem) reserved for known ESBL-producing organisms or recent broad-spectrum antibiotic exposure. A Cochrane review of 71 trials established that beta-lactam monotherapy is as effective as the beta-lactam plus aminoglycoside combination, with significantly less nephrotoxicity [2] — the aminoglycoside era for routine empiric febrile neutropenia is over.
- When to add vancomycin (or another Gram-positive agent). Vancomycin is not routine. Add it for: suspected catheter-related infection (erythema, tenderness, or exit-site pus at the line); severe sepsis or septic shock; pneumonia; skin or soft-tissue infection; MRSA colonisation; severe mucositis in a patient on fluoroquinolone prophylaxis (where viridans streptococci are likely and resistant); or a positive blood culture for a Gram-positive organism pending identification [1]. Routine vancomycin increases nephrotoxicity and does not improve outcomes — the trap of "covering everything" is a well-documented source of harm.
- Reassess at 48 to 72 hours. If a pathogen is identified, narrow to the targeted therapy. If the patient is clinically well and cultures are negative, continue the empiric regimen. Persistent fever at day 3 to 5 mandates an antifungal — add liposomal amphotericin B 3 mg/kg daily, an echinocandin (caspofungin, micafungin), or voriconazole or posaconazole — and order a chest CT and a serum galactomannan to look for invasive aspergillosis (see below). The chest X-ray is often normal early in invasive fungal infection; the CT is the test that finds the halo sign.
- Risk stratify with the MASCC score. The Multinational Association of Supportive Care in Cancer (MASCC) risk index identifies low-risk patients (score at least 21) who may step down to oral antibiotics (ciprofloxacin plus amoxicillin-clavulanate) and even be managed as outpatients with close follow-up. The score weighs burden of illness, absence of hypotension, absence of chronic obstructive airways disease, solid tumour (rather than haematological), no previous fungal infection, no dehydration, outpatient status at onset of fever, and age below 60.
- When to stop. Continue the empiric antibiotics until the patient has been afebrile for at least 48 hours AND the neutrophil count is recovering (above 0.5 and rising). In prolonged neutropenia with a documented infection, treat for the standard course for that organism. Stopping too early risks relapse and selection of resistant organisms.
The role of G-CSF — prophylaxis, not treatment
Granulocyte colony-stimulating factor (G-CSF, filgrastim; or the long-acting pegfilgrastim) accelerates neutrophil recovery, but it has no place in the routine treatment of established febrile neutropenia. A Cochrane review of 14 randomised trials (1,553 participants) found that adding G-CSF to antibiotics did not significantly reduce overall mortality (hazard ratio 0.74, 95 per cent CI 0.47 to 1.16) [3]. Its role is prophylaxis: primary prophylaxis when the expected risk of febrile neutropenia with a regimen is above 20 per cent (some AML induction and aggressive lymphoma regimens, age over 65 with comorbidity), and secondary prophylaxis after a confirmed episode to allow maintenance of dose intensity. Giving G-CSF routinely for an established episode is a recognised exam trap — it does not save lives, and it does not substitute for antibiotics.
The organisms — and the source that gives them away
| Syndrome | Organism | Clue |
|---|---|---|
| Bacteraemia, Gram-negative | Pseudomonas aeruginosa, E. coli, Klebsiella | Ecthyma gangrenosum (Pseudomonas); often no localising sign |
| Bacteraemia, Gram-positive | Coagulase-negative staph, Staph aureus, Strep viridans | Central venous catheter; severe mucositis (viridans) |
| Invasive fungal (prolonged neutropenia above 10 to 14 days) | Aspergillus, Mucorales, Candida | Persistent fever; halo sign on CT (Aspergillus); sinus/cerebral involvement (Mucorales) |
| Enterocolitis | Clostridium septicum, C. difficile, Candida | Right lower quadrant pain and bloody diarrhoea (typhlitis) |
| Reactivation | HSV, VZV | Mucocutaneous lesions in expected dermatomes or perioral distribution |
Invasive aspergillosis — the fungal complication of prolonged neutropenia
When neutropenia is prolonged (typically above 10 to 14 days) and fever persists despite broad-spectrum antibacterials, the leading fear is invasive pulmonary aspergillosis. The pathophysiology is angioinvasion by Aspergillus hyphae: the fungus invades pulmonary vessels, causing thrombosis, infarction, and haemorrhage, which produces two characteristic CT signs. The halo sign — a nodular lesion surrounded by a ground-glass halo of haemorrhage — appears early (within the first week) and is the most sensitive finding. As neutrophils recover, the necrotic lung sequesters, producing the air-crescent sign later. The clinical correlate is pleuritic chest pain, haemoptysis, dry cough, and fever unresponsive to antibiotics. [1]
Diagnosis combines chest CT (halo sign early, air-crescent sign late), serum galactomannan (an Aspergillus cell-wall antigen detected by ELISA; serial monitoring improves sensitivity), bronchoalveolar lavage galactomannan and culture, and histopathology (septate hyphae branching at acute angles, with tissue invasion). Treatment is voriconazole first-line (established by the seminal randomised trial showing survival benefit over amphotericin B deoxycholate) or isavuconazole, with liposomal amphotericin B as an alternative. Reduce immunosuppression where possible; consider surgical resection for localised disease, mould involvement of great vessels, or haemoptysis. Mortality is 50 to 60 per cent despite treatment in the neutropenic and transplant population — which is why prophylaxis with posaconazole or voriconazole in very high-risk AML/MDS and HSCT patients, and early CT at the first sign of persistent fever, are the interventions that change outcome. [1]
Cellular immunodeficiency — HIV by CD4, transplant by timeline
HIV — the CD4 ladder
The CD4 count is the single best predictor of which opportunistic infection an HIV-positive patient is at risk of, and the exam tests it directly: [1]
- CD4 above 500: early HIV. Community infections only.
- CD4 200 to 500: bacterial pneumonia (especially pneumococcal), pulmonary TB, mucocutaneous candidiasis, Kaposi sarcoma, HSV.
- CD4 below 200: Pneumocystis jirovecii pneumonia (PCP) — the opportunistic pneumonia with a dry cough, exertional dyspnoea, bilateral perihilar interstitial infiltrates, a raised lactate dehydrogenase, and a high alveolar-arterial oxygen gradient. Also Toxoplasma gondii encephalitis (ring-enhancing lesions on MRI, headache, focal neurology), Cryptococcus neoformans meningitis (subacute headache, fever, India ink positive CSF, raised opening pressure), Histoplasma and Coccidioides disseminated disease in endemic areas, and CMV disease (retinitis with floaters and visual loss, colitis with diarrhoea, pneumonitis, oesophagitis).
- CD4 below 50: Mycobacterium avium complex (MAC) disseminated disease (fever, weight loss, anaemia, hepatosplenomegaly), CMV retinitis, CNS lymphoma (EBV-driven). [1]
Prophylaxis follows the CD4: co-trimoxazole for PCP when the CD4 is below 200 (or below 250 in some guidelines, or a history of oropharyngeal candidiasis); azithromycin weekly for MAC when the CD4 is below 50. The single most important intervention is antiretroviral therapy — immune restoration reduces the risk of every opportunistic infection, but it can precipitate immune reconstitution inflammatory syndrome (IRIS), a paradoxical worsening as the recovering immune system responds to a latent or partially treated organism. [1]
Cryptococcal meningitis — the manage-raised-ICP principle
Cryptococcal meningitis presents in the cellular-immunodeficiency patient (HIV CD4 below 100, transplant) with subacute headache, fever, and malaise, and the diagnosis is confirmed by CSF India ink (capsule visualisation), cryptococcal antigen (CrAg, in serum and CSF), and CSF culture. The 2010 IDSA guideline established the three-phase regimen: induction with liposomal amphotericin B plus flucytosine for at least two weeks, consolidation with fluconazole for at least eight weeks, then maintenance (fluconazole) until immune restoration [8]. The principle that examiners test hardest is management of raised intracranial pressure: daily therapeutic lumbar punctures to reduce the opening pressure, and a ventricular shunt if the pressure cannot be controlled. Acetazolamide and mannitol have no role. Raised ICP is the single most important determinant of early mortality in cryptococcal meningitis — more than the antifungal choice.
Humoral immunodeficiency and the asplenic patient — the encapsulated bacteria
Patients with B-cell or complement defects — multiple myeloma, CLL, common variable immunodeficiency, complement deficiency, eculizumab therapy, and crucially anatomical or functional asplenia — are uniquely vulnerable to the encapsulated bacteria: Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis, because clearing these organisms requires opsonising antibody and splenic macrophage function. They also carry risk from Capnocytophaga canimorsus (dog bites), Babesia (splenectomy), and Salmonella (sickle cell disease). [1]
Overwhelming post-splenectomy infection (OPSI)
The catastrophic presentation is overwhelming post-splenectomy infection (OPSI): a previously well asplenic patient develops fulminant bacteraemia — most often pneumococcal — with purpura fulminans, Waterhouse-Friderichsen adrenal haemorrhage, disseminated intravascular coagulation, and septic shock, progressing to death within hours despite treatment. Mortality is 50 to 70 per cent even with optimal care. The risk is lifelong, is highest in the first two years after splenectomy and in children and older adults, and the single most important intervention at the bedside of a febrile asplenic patient is empiric ceftriaxone within one hour (add vancomycin if meningitis is possible, for pneumococcal meningitis with possible penicillin resistance). [1]
Prevention — the three-pillar strategy
Preventing OPSI is one of the clearest wins in all of medicine, built on vaccination, prophylactic antibiotics, and patient empowerment. [1]
Vaccination — the asplenic patient needs, ideally at least two weeks before an elective splenectomy (and from 14 days post-op for emergency cases):
- Pneumococcal: conjugate (PCV13 or 15) first, then polysaccharide (PPSV23) at least 8 weeks later; revaccinate PPSV23 at 5 years.
- Haemophilus influenzae type b (Hib).
- Meningococcal ACWY and meningococcal B, with a documented booster plan (every 5 years for ACWY).
- Influenza annually and COVID-19 — these patients do not tolerate respiratory viral infections. [1]
Prophylactic antibiotics — penicillin V 500 mg twice daily (or amoxicillin), lifelong in high-risk groups (age under 16 or over 50, inadequate vaccine response, or a prior invasive infection); the evidence is strongest for children under 16 and for the first two post-splenectomy years. Macrolide prophylaxis is used where penicillin-allergic. [1]
Patient empowerment — a standby dose of amoxicillin (or a clear plan for immediate ceftriaxone), to take at the first sign of fever before reaching hospital; an alert card and medical identification (bracelet); and clear education that any fever is a medical emergency. [1]
The solid organ transplant infection timeline

The post-transplant infection timeline is the single most useful framework for the transplant patient with fever. It works for kidney, liver, heart, and lung — with lung the highest-risk for opportunistic infection. The timeline divides into three phases. [1]
Month 0 to 1 — donor-derived, nosocomial, and wound
In the first month, the patient is essentially a surgical patient with high-acuity nosocomial exposure. The infections are not opportunistic; they reflect the donor, the operation, and the hospital. Think: donor-derived infection (transmitted from the donor organ — HIV, HBV, HCV, West Nile virus, lymphocytic choriomeningitis virus, donor bacteraemia or mycobacteria), nosocomial infection (catheter-related bloodstream infection, ventilator-associated pneumonia, C. difficile, surgical site infection, candiduria), wound and anastomotic complications (bile leak, urinary leak, vascular graft infection), and recurrent native infection (a pre-existing UTI, an aspergilloma, an inadequately treated infection before transplant). [1]
Months 1 to 6 — the opportunistic window
This is the phase of maximal net immunosuppression (induction plus early maintenance immunosuppression) and the home of the classic opportunistic infections. The four to know cold: [1]
- Cytomegalovirus (CMV) — the most important transplant pathogen. Risk is highest in the D+/R- (donor-positive, recipient-negative) mismatch, because the recipient has no pre-existing CMV immunity. Presents as the CMV syndrome (fever, leucopenia, thrombocytopenia, malaise) or as tissue-invasive disease (pneumonitis, especially in lung transplant; colitis with diarrhoea and bleeding; hepatitis; retinitis; nephritis). CMV is itself immunomodulatory — CMV disease increases the risk of bacterial sepsis, invasive fungal infection, EBV-driven post-transplant lymphoproliferative disorder, and acute rejection. Prevention is by either universal prophylaxis with valganciclovir 900 mg daily for 3 to 6 months (longer in lung, and in D+/R-) or pre-emptive therapy guided by weekly quantitative PCR. Treatment of established disease is intravenous ganciclovir 5 mg/kg every 12 hours (or oral valganciclovir 900 mg every 12 hours if gut function allows), with reduction of immunosuppression.
- BK virus nephropathy — particularly after kidney transplant. BK reactivation causes nephropathy that mimics acute rejection (rising creatinine, interstitial inflammation on biopsy), and viruria and viraemia. The trap is treating presumed rejection with intensified immunosuppression, which worsens the BK nephropathy. Management is reduction of immunosuppression; cidofovir and fluoroquinolones have a limited role.
- Pneumocystis jirovecii (PCP) — prevented by co-trimoxazole; a transplant patient with PCP has usually stopped or never started prophylaxis. Presents with dyspnoea, dry cough, fever, and bilateral perihilar infiltrates.
- Invasive aspergillosis — highest in lung transplant; presents with fever, pleuritic chest pain, haemoptysis, and the halo sign on CT. Post-transplant lymphoproliferative disorder (PTLD), driven by Epstein-Barr virus, presents with fever, lymphadenopathy, and extranodal masses (gut, central nervous system, allograft), and is managed by reduction of immunosuppression plus rituximab and chemotherapy as required. [1]
Beyond 6 months — community-acquired dominates
After 6 months, if immunosuppression has been tapered to maintenance levels, the transplant patient develops community-acquired infections like any other host — community-acquired pneumonia, urinary tract infection, influenza, COVID-19 — plus persistent opportunistic infection if the patient is on heavy immunosuppression (chronic rejection, recurrent rejection treatment). Vaccination, particularly annual influenza and pneumococcal, is essential. [1]
Biologic therapy — the agent-specific infection signature
Biologic agents have revolutionised rheumatology, gastroenterology, dermatology, and oncology — and each class carries a characteristic infection signature that the physician must recognise. [1]
Anti-TNF therapy — TB, fungi, and intracellular organisms
Tumour necrosis factor alpha is essential for maintaining the granuloma that contains latent M. tuberculosis. Blocking it disrupts granuloma integrity and liberates dormant bacilli. The seminal report by Keane and colleagues analysed 70 cases of TB reported to the FDA through MedWatch in patients on infliximab: the median time to TB was 12 weeks, and 57 per cent had extrapulmonary disease (17 of them disseminated) [7]. This single paper transformed practice — every patient now has an IGRA (interferon-gamma release assay) and a chest X-ray before the first anti-TNF dose, and latent TB is treated before the biologic is started. The risk differs by class: the monoclonal antibodies (infliximab, adalimumab, certolizumab) carry higher TB reactivation risk than the soluble receptor etanercept. Anti-TNF also increases the risk of endemic mycoses (Histoplasma, Coccidioides), Legionella, and Listeria — all intracellular organisms controlled by cell-mediated immunity.
Rituximab (anti-CD20) — HBV reactivation and PML
Rituximab depletes B-cells for 6 to 12 months, removing the HBsAg-neutralising antibody response that holds HBV in check. HBV reactivation can occur even from resolved infection (HBsAg-negative, anti-HBc-positive) — which is why every patient about to receive rituximab must be screened with HBsAg AND anti-HBc (not just HBsAg), and all at-risk patients (HBsAg-positive or anti-HBc-positive) must receive prophylactic entecavir or tenofovir before, during, and for at least 12 to 18 months after therapy. A systematic review confirmed that preventive antiviral therapy dramatically reduces HBV reactivation and HBV-related hepatic failure [5]. Rituximab also carries a small but serious risk of progressive multifocal leukoencephalopathy (PML) from JC virus, and of enterovirus and parvovirus infection — all consequences of prolonged B-cell depletion.
Alemtuzumab (anti-CD52) — profound and prolonged lymphopenia
Alemtuzumab causes severe and prolonged lymphopenia for months to years, and with it a high risk of CMV reactivation and disease, herpesvirus reactivation, listeriosis, and tuberculosis. CMV monitoring (weekly PCR) and co-trimoxazole prophylaxis are routine. [1]
Tocilizumab (anti-IL-6) — bowel perforation
Tocilizumab, used in rheumatoid arthritis, carries a specific risk of gastrointestinal perforation (particularly with diverticular disease), which can present atypically with minimal pain because the cytokine blockade masks the inflammatory response. [1]
Prophylaxis strategies — the interventions that prevent the worst infections
The right prophylaxis, given to the right patient for the right duration, prevents most of the catastrophic opportunistic infections. The regimen is built on four pillars. [1]
Co-trimoxazole (trimethoprim-sulfamethoxazole) for PCP — one double-strength tablet (960 mg) daily or three times weekly, for at least 6 months after solid organ or haematopoietic transplant (longer in lung or small bowel), and during any course of high-dose corticosteroids (prednisolone above 20 mg for more than 4 weeks) [4]. Co-trimoxazole also covers Toxoplasma, Nocardia, Isospora, Cyclospora, and many urinary pathogens — a broad footprint for a single cheap drug. Dapsone, atovaquone, or inhaled pentamidine are alternatives for the sulfa-allergic or G6PD-deficient.
Valganciclovir for CMV in D+/R- transplants — 900 mg orally daily, for 3 to 6 months in the highest-risk patients (D+/R- kidney, lung, heart-lung, alemtuzumab induction). The alternative strategy is pre-emptive therapy guided by weekly quantitative PCR, treating only when viraemia rises. Bone marrow suppression (leucopenia, thrombocytopenia) is the main toxicity. [1]
Fluconazole, posaconazole, or voriconazole for fungal prophylaxis in high-risk neutropenia — fluconazole for standard-risk HSCT during engraftment; posaconazole or voriconazole for very high-risk AML/MDS induction and for graft-versus-host disease, because they cover moulds (Aspergillus, Mucorales). [1]
Aciclovir or valaciclovir for HSV and VZV — during engraftment and in patients with frequent reactivation; given until immune reconstitution. [1]
Prophylaxis quick-reference — what to give, to whom, for how long
| Indication | Agent and dose | Duration | Notes |
|---|---|---|---|
| PCP after transplant or high-dose steroids | Co-trimoxazole 960 mg (double-strength) daily or three times weekly | At least 6 months post-SOT; lifelong consideration in lung; during steroids above 20 mg prednisolone for over 4 weeks | Covers Toxoplasma, Nocardia, many UTI organisms; dapsone or atovaquone if sulfa-allergic (check G6PD first) |
| HSV/VZV during engraftment | Aciclovir 200 to 400 mg three times daily, or valaciclovir 500 mg twice daily | During neutropenia until immune reconstitution | Reduces mucositis and reactivation in seropositive patients |
| Fungal in high-risk neutropenia (AML/MDS, HSCT, GVHD) | Posaconazole 300 mg daily (after loading) or voriconazole; fluconazole 400 mg daily for standard risk | During neutropenia or GVHD treatment | Posaconazole and voriconazole cover moulds; therapeutic drug monitoring for voriconazole |
| PCP in HIV with CD4 below 200 | Co-trimoxazole 960 mg daily | Until CD4 above 200 for at least 3 months on ART | Also covers Toxoplasma |
| MAC in HIV with CD4 below 50 | Azithromycin 1200 mg weekly | Until CD4 above 100 for at least 3 months on ART | Rule out active MAC first |
| Asplenia | Penicillin V 500 mg twice daily (lifelong in high-risk); standby amoxicillin 1 g at first fever | Lifelong in age under 16 or over 50, or prior invasive infection; otherwise at least 2 years | Plus vaccination (pneumococcal, Hib, meningococcal ACWY and B) |
Vaccination in the immunocompromised host
The 2013 IDSA guideline on vaccination of the immunocompromised host sets the principles [6]:
- Vaccinate before immunosuppression where possible — ideally at least 2 weeks before for inactivated vaccines, and 4 weeks before for live vaccines, so the immune response can develop.
- Inactivated vaccines are safe but may be less immunogenic — the response is blunted by immunosuppression, so timing matters and revaccination or serological confirmation may be required.
- Live vaccines are contraindicated in severe immunosuppression — this includes MMR, varicella (the live vaccine), yellow fever, live attenuated influenza (the intranasal formulation), oral polio, oral typhoid (Ty21a), BCG, and rotavirus (in severe immunodeficiency). The risk is that the attenuated organism causes the actual disease in a host that cannot contain it.
- Vaccinate household contacts — to provide indirect (cocoon) protection; household contacts should also avoid the live intranasal influenza vaccine if the immunocompromised person is severely immunosuppressed. [1]
The specific vaccines the immunocompromised patient needs, in addition to standard age-based schedules: annual inactivated influenza (patient and household); pneumococcal (PCV then PPSV23) for asplenia, transplant, nephrotic syndrome, myeloma, CLL; hepatitis B for all patients on dialysis or before anti-CD20 therapy; meningococcal ACWY and B for asplenia and complement deficiency; recombinant zoster (Shingrix), which is inactivated and safe, for patients above 50 and for immunosuppressed adults above 19. [1]
Syndrome-based investigations — the immunocompromised patient with a localising problem
Most immunocompromised patients do not present as a clean "type of defect" vignette; they present with a syndrome. The investigation is then driven by the syndrome, refined by the immune defect. Four syndromes dominate. [1]
Pulmonary infiltrates in the immunocompromised host. The chest X-ray is often unhelpful (insensitive early); the high-resolution CT chest is the first test. The pattern drives the differential: bilateral perihilar ground-glass suggests PCP (confirm with induced sputum or bronchoalveolar lavage; serum beta-D-glucan is supportive, LDH is raised, and the alveolar-arterial oxygen gradient is high); nodules with a halo suggest invasive aspergillosis (serum and BAL galactomannan; biopsy shows septate acute-angle branching hyphae); reverse halo (the atoll sign) suggests Mucorales (urgent sinus and cerebral imaging; tissue biopsy with broad non-septate ribbon-like hyphae); consolidation suggests bacterial pneumonia (sputum, blood cultures, urinary antigens). Add CMV PCR in the transplant patient (CMV pneumonitis), serum and urinary Histoplasma antigen in endemic areas, Nocardia cultures (hold longer), and bronchoalveolar lavage if the patient is deteriorating or the diagnosis is unclear. [1]
Central nervous system infection. MRI brain before lumbar puncture if there is any focal deficit, immunocompromise, or reduced consciousness. Ring-enhancing lesions in an HIV patient with CD4 below 100 are Toxoplasma gondii encephalitis (confirm with Toxoplasma IgG; treat empirically with sulfadiazine plus pyrimethamine and folinic acid; the response at two weeks is diagnostic). A subacute lymphocytic meningitis with a positive cryptococcal antigen is Cryptococcus (CSF India ink, antigen, culture; measure and manage opening pressure). Rhombencephalitis (brainstem encephalitis) is Listeria monocytogenes — treat with IV ampicillin (or co-trimoxazole if penicillin-allergic). Progressive white-matter lesions on MRI in a patient on rituximab or natalizumab are progressive multifocal leukoencephalopathy (PML) from JC virus (CSF JC virus PCR). And fever, headache, and a confusional state in the transplant patient raises EBV-driven post-transplant lymphoproliferative disorder (PTLD) involving the central nervous system — quantitate EBV viral load. [1]
Diarrhoea in the transplant or HIV patient. The differential is broad: CMV colitis (diarrhoea, bleeding, colonoscopic ulceration with viral inclusions on biopsy), Clostridioides difficile (toxin assay), Cryptosporidium, Microsporidium, Cyclospora, Isospora (stool microscopy with special stains), Giardia, Adenovirus, and in the transplant patient graft-versus-host disease (which mimics infection and is worsened by empiric immunosuppression reduction rather than antibiotics). Send stool for culture, C. difficile toxin, microscopy for ova cysts and parasites (with acid-fast stain), and multiplex molecular testing; colonoscopy and biopsy if persistent or bloody. [1]
Central venous catheter infection. The paired-culture principle: draw blood cultures from each lumen of the catheter and from a peripheral vein simultaneously. A catheter-drawn culture that turns positive at least 2 hours before the peripheral culture (differential time to positivity) localises the infection to the line. Coagulase-negative staphylococci are the most common; Staphylococcus aureus, Pseudomonas aeruginosa, Candida, and atypical mycobacteria (Mycobacterium fortuitum, chelonae, abscessus) mandate line removal. Tunnel infection, port abscess, septic emboli, or endocarditis also mandate removal. The line can stay for uncomplicated coagulase-negative staphylococcal bacteraemia treated with antibiotics (often antibiotic lock therapy), but the threshold to remove is low. [1]
Neutropenic enterocolitis (typhlitis) — the right lower quadrant in profound neutropenia
Neutropenic enterocolitis, also called typhlitis (from the Greek for caecum), is a transmural inflammation of the caecum and often the terminal ileum that occurs in profound neutropenia, typically after intensive AML induction or HSCT conditioning. The pathophysiology is mucosal damage from chemotherapy combined with neutropenia, allowing bacterial translocation across the damaged bowel wall, with relative sparing of the rectum. The presentation is fever with right lower quadrant abdominal pain, often with diarrhoea (frequently bloody), abdominal distension, and signs of peritonitis if perforation has occurred. The diagnosis is clinical plus CT abdomen showing bowel wall thickening of the caecum and ascending colon (greater than 4 mm), often with surrounding fat stranding and sometimes pneumatosis. [1]
Management is supportive: bowel rest with nasogastric decompression, broad-spectrum antibiotics covering Gram-negatives and anaerobes (piperacillin-tazobactam plus metronidazole, or meropenem), intravenous fluids and electrolyte correction, and G-CSF in selected high-risk patients (though the evidence is limited). Surgery is reserved for frank perforation, uncontrolled bleeding, or clinical deterioration despite maximal medical therapy. The mortality is significant (10 to 50 per cent), driven by perforation, sepsis, and the underlying malignancy. The key trap is operating too early — most cases settle with medical management — or too late — missing the perforation. [1]
Immune reconstitution inflammatory syndrome (IRIS)
IRIS is a paradoxical clinical worsening that occurs when immune function recovers in a patient treated for an opportunistic infection. It is most familiar in HIV (after starting antiretroviral therapy), in transplant (after reduction of immunosuppression), and in the post-neutropenia recovery phase. The mechanism is the recovering immune system mounting an exuberant inflammatory response to a latent or partially treated organism. [1]
In HIV, IRIS most commonly involves Mycobacterium avium complex, Mycobacterium tuberculosis, Cryptococcus, and CMV — presenting as fever, lymphadenitis, abscess formation, or worsening infiltrates days to weeks after starting antiretrovirals. In transplant, reduction of immunosuppression for a treated opportunistic infection can unmask CMV, BK, or hepatitis. The diagnosis is one of exclusion — rule out progressive infection, drug resistance, a new infection, or drug reaction before attributing the worsening to IRIS. [1]
Management is continuation of treatment of the underlying opportunistic infection (do not stop the antimicrobial), continuation of the antiretroviral or the reduced immunosuppression (do not abandon the immune recovery), and corticosteroids only for severe or life-threatening inflammation — for example, IRIS involving the central nervous system, the airway, or causing respiratory failure. The trap is misdiagnosing IRIS as treatment failure and escalating antimicrobials unnecessarily, or misdiagnosing true progressive infection as IRIS and withholding treatment. [1]
The haematopoietic stem cell transplant phases — beyond the solid organ timeline
The HSCT recipient has a distinct infection timeline that reflects the depth and timing of immune reconstitution, and which differs from the solid organ transplant timeline in important ways. [1]
Pre-engraftment (days 0 to 30): the patient is profoundly neutropenic and mucositis is common. The organisms are those of febrile neutropenia — Gram-negative bacilli (Pseudomonas), Gram-positive cocci (viridans streptococci from mucositis, coagulase-negative staph from lines), Candida, and Aspergillus from prolonged neutropenia, and HSV reactivation. Prophylaxis during this phase is fluoroquinolone (ciprofloxacin or levofloxacin) for Gram-negative cover, aciclovir for HSV, and fluconazole or posaconazole for fungal cover. [1]
Early post-engraftment (days 30 to 100): neutrophils recover but T-cell and B-cell immunity are profoundly impaired (especially after allogeneic transplant). The dominant pathogens are the opportunistic viruses — CMV (the single most important), adenovirus, human herpesvirus 6, EBV (driving PTLD) — and PCP. Co-trimoxazole for PCP begins once the patient engrafts; CMV is monitored by weekly PCR with pre-emptive ganciclovir or foscarnet. [1]
Late post-engraftment (beyond day 100): T-cell immunity slowly recovers, but patients remain at risk of VZV reactivation (shingles, often disseminated, for up to two years), encapsulated bacterial infection (functional hyposplenism, especially after chronic graft-versus-host disease), PCP if co-trimoxazole is stopped too early, and chronic viral infection (chronic HBV, HCV, BK). Vaccination restarts from 6 months (inactivated) and from 24 months (live vaccines, only if immune reconstitution is documented and immunosuppression is minimal). [1]
Donor-derived infection — the often-missed first-month diagnosis
Donor-derived infection is the diagnosis that is missed because the recipient's symptoms are attributed to the operation or to rejection. Organ donors are screened for the standard blood-borne viruses (HIV, HBV, HCV) and for bacteraemia, but screening is imperfect, and several high-consequence pathogens can be transmitted and are not routinely tested for. The list to hold in mind for an unexplained infection in the first month: West Nile virus (encephalitis, from a viraemic donor in an endemic area), lymphocytic choriomeningitis virus (LCMV, from rodents — a devastating meningoencephalitis in the cluster of transplant recipients), Trypanosoma cruzi (Chagas disease, from Latin American donors), Strongyloides (hyperinfection, from donors from endemic areas), Mycobacterium tuberculosis (the donor's latent TB transmitted with the allograft), Toxoplasma (especially in heart transplant, where the recipient is often D+/R-), and donor bacteraemia or candidemia at the time of procurement. The principle is that any unexplained infection in the first month after transplant should prompt a conversation with the organ procurement organisation and the transplant infectious diseases team about the donor's history and screening — and a consideration of the other recipients of organs from the same donor. [1]
Regional guideline deltas
| Aspect | ANZ (eTG, ASID) | UK (NICE, BIA, BCSH) | US (IDSA, CDC, NCCN) |
|---|---|---|---|
| Empiric febrile neutropenia | Piperacillin-tazobactam first-line | Piperacillin-tazobactam (Tazocin) first-line | Cefepime, piperacillin-tazobactam, or carbapenem equivalent |
| G-CSF | Prophylaxis in high-risk regimens; not routine treatment | Same | Same (ASCO/IDSA alignment) |
| PCP prophylaxis | Co-trimoxazole for at least 6 months post-transplant | Co-trimoxazole; alternatives dapsone/atovaquone | Co-trimoxazole; inhaled pentamidine in select |
| HBV before rituximab | Entecavir or tenofovir for HBsAg+ and anti-HBc+ | Entecavir or tenofovir; lamivudine avoided (resistance) | Entecavir or tenofovir preferred over lamivudine |
| Live vaccine avoidance | MMR, VZV, yellow fever, oral polio, BCG, Ty21a avoided | Same | Same (CDC immunization schedule) |
High-yield exam discriminators
- Door-to-antibiotic within one hour in febrile neutropenia — temperature above 38.3 single or above 38 sustained, neutrophils below 0.5; cultures immediately before the dose; never delay for results.
- Empiric antipseudomonal beta-lactam (piperacillin-tazobactam) monotherapy is the cornerstone; add vancomycin only for line infection, sepsis, pneumonia, skin or soft-tissue infection, MRSA colonisation, or severe mucositis on fluoroquinolone prophylaxis.
- Persistent fever beyond 3 to 5 days in neutropenia mandates chest CT, galactomannan, and empiric antifungal therapy (liposomal amphotericin B, echinocandin, voriconazole).
- CMV is the most important transplant pathogen — highest risk in D+/R-; presents 1 to 6 months post-transplant; prophylaxis with valganciclovir or pre-emptive PCR-guided therapy.
- HBV screening before rituximab (or chemotherapy) must include HBsAg AND anti-HBc — resolved HBV can reactivate and cause fulminant hepatic failure; prophylactic entecavir or tenofovir prevents it.
- Anti-TNF reactivates TB at a median of 12 weeks, often extrapulmonary or disseminated; IGRA and chest X-ray before the first dose; treat latent TB first.
- Asplenic fever is OPSI until proven otherwise — empiric ceftriaxone within one hour; lifelong penicillin and standby amoxicillin; vaccination with pneumococcal, Hib, and meningococcal ACWY and B.
- Live vaccines (MMR, VZV, yellow fever, live attenuated influenza, oral polio, Ty21a, BCG) are contraindicated in severe immunosuppression — use the inactivated alternatives and vaccinate household contacts.
- G-CSF does not reduce mortality in established febrile neutropenia (Cochrane review of 14 trials) — its role is primary prophylaxis in high-risk regimens.
- Raised intracranial pressure in cryptococcal meningitis is managed with daily therapeutic lumbar punctures (or a ventricular shunt), not acetazolamide or mannitol — and is the main determinant of early mortality. [1]
Communication and shared decision-making
- Before splenectomy: "Your spleen protects you from certain bacteria that cause rapid, life-threatening infection. Without it, a chest infection or sore throat can become overwhelming within hours. So you must carry a standby antibiotic, wear a medical bracelet, and come straight to hospital with any fever — even a mild one. We vaccinate you before the operation to give your immune system time to respond."
- Before anti-TNF therapy: "This medicine can wake up a sleeping tuberculosis infection. I am testing you for it today with a blood test and a chest X-ray. If the test is positive we treat the TB first, before starting the biologic. The risk is small but the consequence is serious, so we never skip the screen."
- Before rituximab: "This medicine can let a virus called hepatitis B come back, even if you had it years ago and cleared it. So I am testing your blood for past hepatitis B today. If the test is positive we give you an antiviral tablet during and after the treatment to keep it asleep."
- A febrile neutropenic emergency to family: "Your husband's white blood cells are very low from the chemotherapy, so he cannot fight infection. The fever means there may already be bacteria in his bloodstream, which is why we are giving the antibiotic through the drip within the hour. We take the cultures first, then we treat — waiting is the one thing we cannot do." [1]
Summary: the immunocompromised host consultation in one paragraph
Identify the type of immune defect — neutropenic, cellular, humoral, transplant phase, or biologic — because the defect predicts the organism, the empiric therapy, and the prophylaxis. In febrile neutropenia give an antipseudomonal beta-lactam (piperacillin-tazobactam) within one hour after blood cultures, add vancomycin only for line infection or sepsis, escalate with an antifungal at 3 to 5 days of persistent fever, and do not give G-CSF routinely. In the transplant patient use the timeline (month 0 to 1 donor and nosocomial, 1 to 6 CMV and opportunistic, beyond 6 community) and prevent CMV with valganciclovir and PCP with co-trimoxazole. Screen every patient before immunosuppression: IGRA for TB before anti-TNF; HBsAg and anti-HBc for HBV before rituximab or chemotherapy; strongyloides serology before steroids in anyone from a tropical area; and vaccinate (pneumococcal, Hib, meningococcal, influenza) before splenectomy and before transplant. In the asplenic patient treat any fever as OPSI with empiric ceftriaxone within one hour, and ensure lifelong penicillin, a standby-antibiotic plan, and an alert card. Never give a live vaccine to a severely immunosuppressed patient, and vaccinate the household contacts instead. [1]
References
- [1]Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america Clin Infect Dis, 2011.PMID 21258094
- [2]Paul M, Dickstein Y, Borok S, Vidal L, Leibovici L Empirical antibiotics targeting gram-positive bacteria for the treatment of febrile neutropenic patients with cancer Cochrane Database Syst Rev, 2017.PMID 28577308
- [3]Mhaskar R, Clark OAC, Lyman G, et al. Colony-stimulating factors for chemotherapy-induced febrile neutropenia Cochrane Database Syst Rev, 2014.PMID 25356786
- [4]Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective Biol Blood Marrow Transplant, 2009.PMID 19747629
- [5]Loomba R, Rowley A, Wesley R, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy Ann Intern Med, 2008.PMID 18378948
- [6]Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host Clin Infect Dis, 2014.PMID 24421306
- [7]Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent N Engl J Med, 2001.PMID 11596589
- [8]Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america Clin Infect Dis, 2010.PMID 20047480