Phys · infectious
Sepsis and Septic Shock
Also known as sepsis · septic shock · septicaemia · bacteraemia with organ dysfunction · severe sepsis (deprecated) · systemic inflammatory response syndrome (SIRS, historical)
Consultant-physician-depth guide to sepsis and septic shock — Sepsis-3 definitions (SOFA, qSOFA), pathophysiology of the dysregulated host response, Surviving Sepsis Campaign Hour-1 Bundle, vasopressor escalation, fluid responsiveness, source control, supportive care, and special situations (neutropenic sepsis, pregnancy, cirrhosis) — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Sepsis and Septic Shock

The one-minute consultant answer
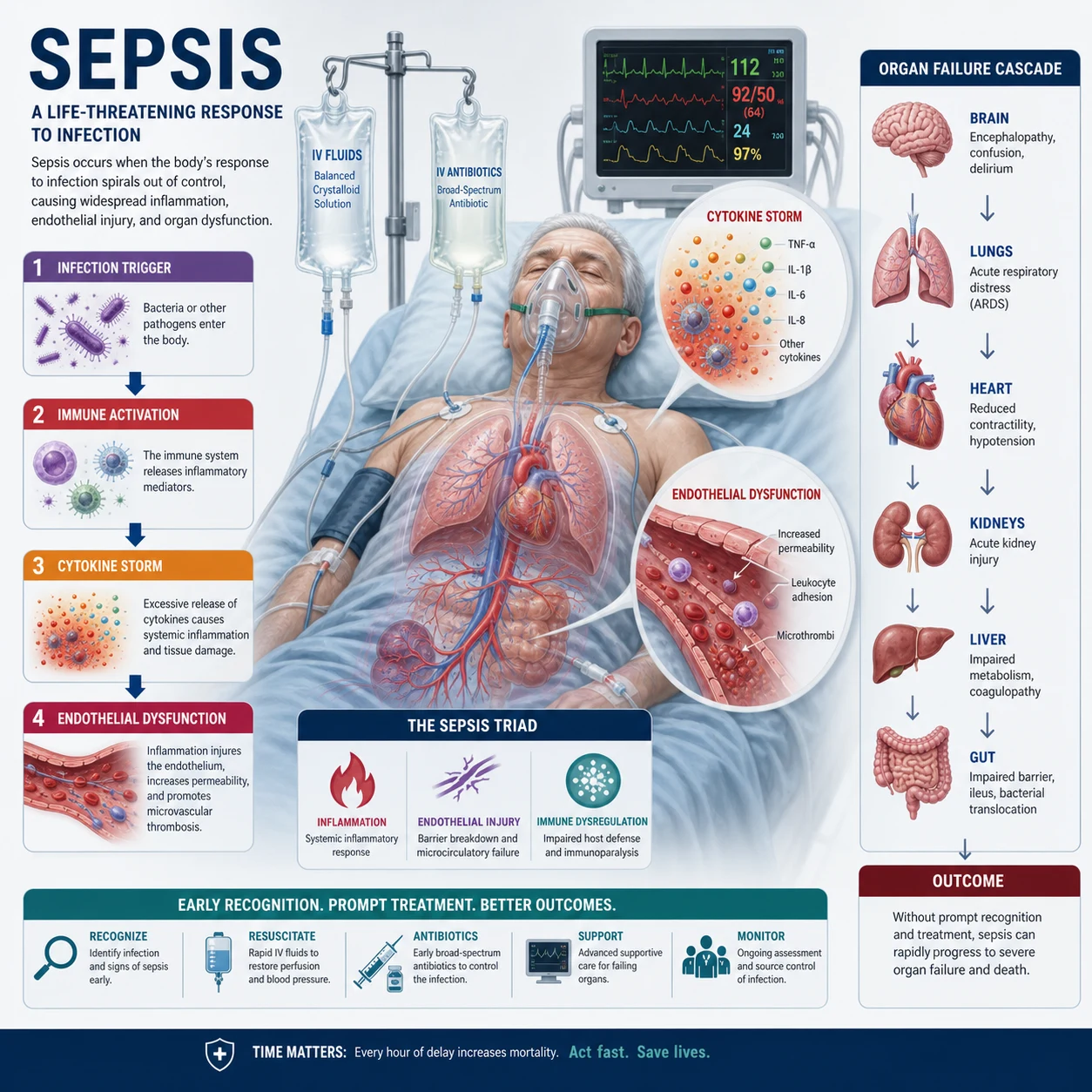
Sepsis is life-threatening organ dysfunction caused by a dysregulated host response to infection [1]. Septic shock is a subset of sepsis with particularly profound circulatory, cellular, and metabolic abnormalities — operationally defined as the need for vasopressors to maintain a mean arterial pressure (MAP) of 65 mmHg or above, plus a serum lactate above 2 mmol/L despite adequate fluid resuscitation [3]. The priority is the Surviving Sepsis Campaign (SSC) Hour-1 Bundle: measure lactate, obtain blood cultures before antibiotics, administer broad-spectrum antibiotics within one hour, give 30 mL/kg crystalloid for hypotension or lactate 4 or above, and start vasopressors for MAP below 65 [4][5]. Every hour of antibiotic delay in septic shock increases mortality [6].
Sepsis-3 Definitions and Severity Staging

What sepsis is — and what it is not
Sepsis-3 retired two older constructs. The term severe sepsis was made redundant because all sepsis is by definition severe (it involves organ dysfunction). SIRS (Systemic Inflammatory Response Syndrome) was discarded as the screening criterion because it is too sensitive (present in many non-infectious conditions — pancreatitis, trauma, burns, surgery) and not specific enough to identify the patients who matter [1].
Sepsis is now defined by organ dysfunction, not by inflammation. This is the critical conceptual shift: the problem in sepsis is not the infection itself, nor the inflammatory response per se, but that the host response has become dysregulated — it has lost its homeostatic balance and is now harming the patient's own tissues. [1]
Operational definitions
Sepsis — Suspected infection plus an acute increase in SOFA score of 2 points or more (from baseline). SOFA (Sequential Organ Failure Assessment) measures six organ systems on a 0-to-4 scale: respiratory (PaO2/FiO2), coagulation (platelets), liver (bilirubin), cardiovascular (MAP and vasopressors), central nervous system (GCS), and renal (creatinine or urine output). A change of 2 or more reflects a mortality risk of approximately 10 per cent or greater [1].
Septic shock — Sepsis requiring vasopressors to maintain MAP 65 mmHg or above, plus serum lactate above 2 mmol/L, despite adequate fluid resuscitation (typically 30 mL/kg crystalloid). The clinical criteria identify a group with hospital mortality exceeding 40 per cent [3].
The key phrase in the septic shock definition is "despite adequate fluid resuscitation." A patient who is hypotensive and lactataemic before fluids has presumed septic shock. A patient who remains so after 30 mL/kg has confirmed septic shock. [1]
qSOFA — the bedside prompt
qSOFA (quick SOFA) is a three-component bedside score designed for use outside the ICU [2]:
| Component | Criterion | Points |
|---|---|---|
| Respiratory rate | 22 breaths/min or above | 1 |
| Altered mentation | GCS below 15 | 1 |
| Systolic blood pressure | 100 mmHg or below | 1 |
A score of 2 or more identifies patients with suspected infection at high risk of poor outcomes. The exam trap: qSOFA is a mortality-prediction prompt, not a diagnostic criterion for sepsis. It prompts the clinician to consider sepsis and initiate the workup. It is not validated for diagnosis, and it has lower sensitivity than SIRS or NEWS2 for identifying sepsis early [4]. In the ANZ setting, NEWS2 (National Early Warning Score) and the Between the Flags deteriorating patient system remain the primary ward-based triggers for clinical review.
Why the definitions matter clinically
The SOFA change of 2 is the operational definition that physicians must apply. In practice, if you suspect infection and the patient has new confusion, raised respiratory rate, hypotension, elevated creatinine, low platelets, or rising bilirubin — they have organ dysfunction. You do not need to calculate the full SOFA score at the bedside; you need to recognise the pattern and act. [1]
Pathophysiology — why sepsis does what it does

Understanding the pathophysiology is not academic. Every management decision — fluids, vasopressors, source control, corticosteroids — flows from understanding the mechanism. [1]
The dysregulated host response
In health, the immune response to infection is proportional and self-limiting: it clears the pathogen and then resolves. In sepsis, this response becomes dysregulated — it is either excessive (hyperinflammatory phase) or suppressed (immunoparalysis), and sometimes both simultaneously in different compartments [1]. The result is that the host response, rather than the pathogen, becomes the primary cause of organ damage.
PAMPs, DAMPs, and pattern recognition
The immune system recognises infection through PAMPs (pathogen-associated molecular patterns) — microbial products like lipopolysaccharide (LPS) from Gram-negative bacteria, lipoteichoic acid from Gram-positives, and flagellin. These bind pattern recognition receptors on immune cells: Toll-like receptors (TLR4 for LPS, TLR2 for Gram-positive products) and NOD-like receptors (NLRs). [1]
Critically, the host response also recognises DAMPs (damage-associated molecular patterns) — the host's own molecules released when tissues are injured: high-mobility group box 1 (HMGB1), mitochondrial DNA (which resembles bacterial DNA), ATP, and S100 proteins. This means that tissue damage from the infection itself further activates the immune system, creating a positive feedback loop that amplifies the inflammatory response. [1]
The cytokine storm and inflammatory amplification
Activation of pattern recognition receptors triggers a cytokine cascade: TNF-alpha and IL-1 (produced within minutes to hours) drive fever, vasodilation, and endothelial activation. IL-6 drives the acute-phase response (CRP synthesis in the liver) and is a useful biomarker. IL-8 recruits neutrophils to sites of infection. [1]
This cytokine storm has three downstream consequences that produce the clinical phenotype: [1]
1. Endothelial dysfunction. The glycocalyx — the carbohydrate-rich layer lining the vascular endothelium — is shed. This exposes the endothelial surface, promotes adhesion of leucocytes and platelets, and increases vascular permeability. The result is capillary leak: protein-rich fluid extravasates into tissues, causing oedema, and intravascular volume is lost despite fluid administration. Nitric oxide production is dysregulated — excessive in the periphery (causing vasodilation and vasoplegia), inadequate in some vascular beds (causing regional ischaemia). [1]
2. Coagulation activation. Tissue factor expression on activated monocytes and endothelial cells triggers the extrinsic coagulation cascade. Simultaneously, anticoagulant pathways are suppressed (antithrombin, protein C, tissue factor pathway inhibitor). Fibrinolysis is inhibited via elevated PAI-1. The result is a procoagulant state that can progress to disseminated intravascular coagulation (DIC) — microvascular thrombosis causing organ ischaemia, combined with consumption of clotting factors and platelets causing bleeding. [1]
3. Mitochondrial dysfunction (cytopathic dysoxia). This is the most important modern concept in sepsis pathophysiology. In septic shock, oxygen delivery to tissues is often adequate (or even supranormal), but cellular oxygen utilisation is impaired. Mitochondria — the cell's energy factories — are damaged by reactive oxygen species, nitric oxide, and inflammatory mediators. ATP production falls, and cells shift to anaerobic metabolism despite adequate oxygen supply. This explains the persistent lactataemia and the failure of supranormal oxygen delivery to improve outcomes. It also explains why aggressive resuscitation to supranormal targets (the Rivers-era approach) does not work — the problem is not oxygen delivery, it is oxygen use [7].
Immunoparalysis — the late and dangerous phase
In the subacute phase (days 3 to 7), many septic patients develop immunoparalysis: a state of immune suppression characterised by reduced monocyte HLA-DR expression, increased anti-inflammatory cytokines (IL-10, TGF-beta), and T-cell exhaustion (lymphocyte apoptosis). This phase predisposes to secondary nosocomial infections — ventilator-associated pneumonia, catheter-related bloodstream infections, fungal infections — which are major causes of late mortality in sepsis. This is why immunomodulatory therapies that further suppress the immune system (like high-dose steroids outside specific indications) can be harmful. [1]
Sources of Sepsis
Knowing the source determines the empiric antibiotic choice and the source control strategy. The common sources, in order of frequency, are: [1]
| Source | Typical organisms | Empiric cover considerations |
|---|---|---|
| Respiratory (most common) | S. pneumoniae, H. influenzae, Legionella, S. aureus | Community-onset: ceftriaxone plus azithromycin. Nosocomial: piperacillin-tazobactam plus vancomycin |
| Urinary tract | E. coli, Klebsiella, Enterococcus, Proteus | Gentamicin or ampicillin plus gentamicin; adjust for local resistance |
| Abdominal | Enteric Gram-negatives, anaerobes (Bacteroides), enterococci | Piperacillin-tazobactam or ceftriaxone plus metronidazole |
| Skin and soft tissue | S. aureus (including MRSA), S. pyogenes, Clostridium | Flucloxacillin or cefazolin; add vancomycin if MRSA risk or necrotising fasciitis |
| Central nervous system | S. pneumoniae, N. meningitidis, Listeria (if risk) | Ceftriaxone plus vancomycin; add ampicillin if Listeria risk |
| Line-related / catheter | Coagulase-negative staphylococci, S. aureus, Gram-negatives, Candida | Vancomycin; consider antifungal if candidal risk; remove the line |
The source is not identified in approximately 20 to 30 per cent of sepsis cases despite thorough investigation. This does not change the urgency of empiric therapy. [1]
The Surviving Sepsis Campaign Hour-1 Bundle
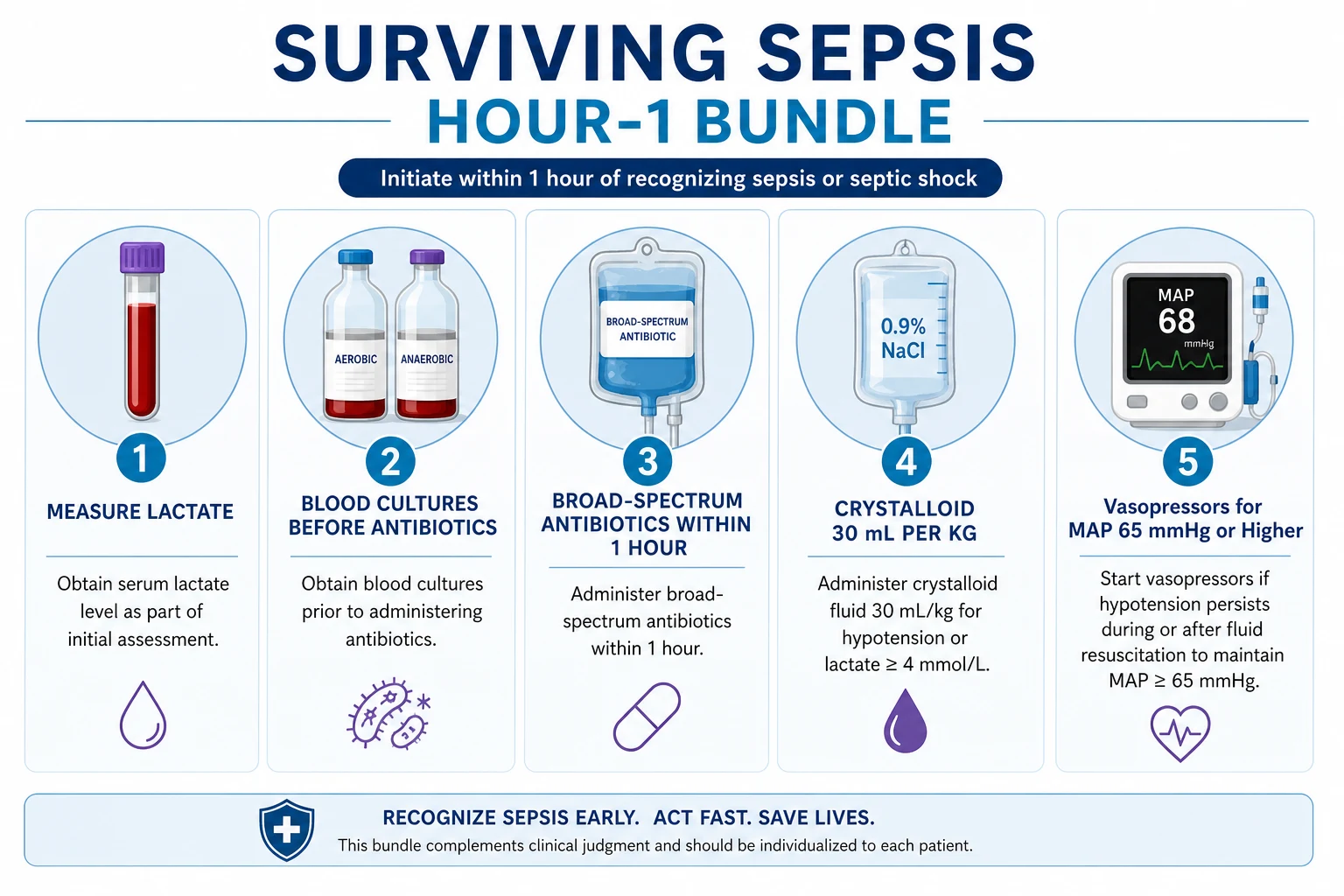
The SSC 2021 guidelines consolidated the previous 3-hour and 6-hour bundles into a single Hour-1 Bundle — the idea is that all five actions should begin immediately upon recognition of sepsis or septic shock, not be spread over hours [4][5].
Element 1: Measure lactate
Obtain a venous or arterial lactate immediately. A lactate above 2 mmol/L indicates tissue hypoperfusion (type A lactic acidosis). A lactate of 4 mmol/L or above is a trigger for aggressive resuscitation. Serial lactate measurements (every 2 to 4 hours) guide the resuscitation: a lactate clearance of 10 per cent or more per hour is the target. Failure to clear lactate despite adequate resuscitation suggests ongoing tissue hypoperfusion, cytopathic dysoxia, or an uncontrolled source. [1]
Lactate caveats: Beta-agonists (salbutamol) and elevated epinephrine drive aerobic lactate production independent of tissue hypoxia. Liver dysfunction impairs lactate clearance. Metformin causes type B lactic acidosis (not tissue hypoxia). Thiamine deficiency, mitochondrial toxins (cyanide, carbon monoxide), and malignancy (Warburg effect) can all elevate lactate. Interpret the lactate in clinical context. [1]
Element 2: Obtain blood cultures before antibiotics
Draw two sets of blood cultures (aerobic and anaerobic, from two separate sites, 20 to 30 mL per bottle total) before administering antibiotics. This increases the yield of organism identification and allows de-escalation. [1]
The critical caveat: Blood cultures should be obtained before antibiotics only if they can be drawn without delaying antibiotic administration beyond 45 minutes. If the patient is in septic shock, do not delay antibiotics for cultures. Antibiotics kill organisms and reduce culture yield after the first dose, but the priority is treating the patient, not obtaining a perfect microbiological specimen [6].
Element 3: Administer broad-spectrum antibiotics within one hour
This is the single most time-sensitive intervention in sepsis. The Seymour et al. New York State study showed that each hour of delay in antibiotic administration in septic shock was associated with increased mortality — the odds of death rose by approximately 4 per cent per hour of delay [6].
Empiric antibiotic principles: [1]
- Cover the likely source — tailor to the suspected site of infection (see the source table above).
- Cover the resistance risk — MRSA risk (recent hospitalisation, healthcare exposure, dialysis, known colonisation): add vancomycin. Pseudomonas risk (nosocomial, structural lung disease, neutropenia, burns): use an anti-pseudomonal beta-lactam (piperacillin-tazobactam, ceftazidime, cefepime, meropenem).
- Dose aggressively — give a loading dose. For example, piperacillin-tazobactam 4.5 g IV, vancomycin 25 to 30 mg/kg IV (loading dose based on actual body weight), ceftriaxone 2 g IV.
- Reassess daily — de-escalate to narrow-spectrum once culture and sensitivity results are available (typically within 48 to 72 hours). This is antimicrobial stewardship.
- Duration — 7 to 10 days is typical for most sepsis. Shorter courses (5 to 7 days) are adequate for many patients with good clinical response and source control. Procalcitonin can guide early cessation. [1]
Element 4: Crystalloid 30 mL/kg for hypotension or lactate 4 or above [1]
Give 30 mL/kg of balanced crystalloid (Hartmann's, Plasmalyte, or Ringer's lactate) within the first 3 hours for patients with hypotension (SBP below 90 or MAP below 65) or lactate 4 mmol/L or above [4]. For a 70 kg patient, this is approximately 2.1 litres.
Why balanced crystalloids, not normal saline? The SSC 2021 guidelines recommend balanced crystalloids over normal saline (weak recommendation). Normal saline causes hyperchloraemic metabolic acidosis (each litre of saline contains 154 mmol/L of chloride), which can worsen renal vasoconstriction and increase the risk of AKI. The SALT-ED and SMART trials demonstrated improved kidney outcomes with balanced crystalloids. [1]
The fluid trap: 30 mL/kg is a starting dose, not a target. Some patients need more (ongoing hypotension, evidence of fluid responsiveness); some need less (heart failure, already volume-overloaded). Ongoing fluid therapy must be guided by dynamic assessment of fluid responsiveness (see below). The ARISE, ProCESS, and ProMISe trials showed that protocolised, aggressive, early goal-directed therapy (EGDT) targeting supranormal central venous oxygen saturation (ScvO2) did not improve outcomes compared to usual care — meaning that more is not better [7].
Risks of fluid overload: Pulmonary oedema, ARDS, abdominal compartment syndrome, tissue oedema impairing oxygen diffusion, and dilutional coagulopathy. The lungs and gut are the sentinel organs for fluid overload. [1]
Element 5: Vasopressors for MAP below 65
If the patient remains hypotensive (MAP below 65 mmHg) despite fluid resuscitation, start a vasopressor. The target MAP is 65 mmHg. Higher targets (75 to 85 mmHg) do not improve outcomes, even in chronic hypertensives [4].
Vasopressor Strategy and Haemodynamic Management
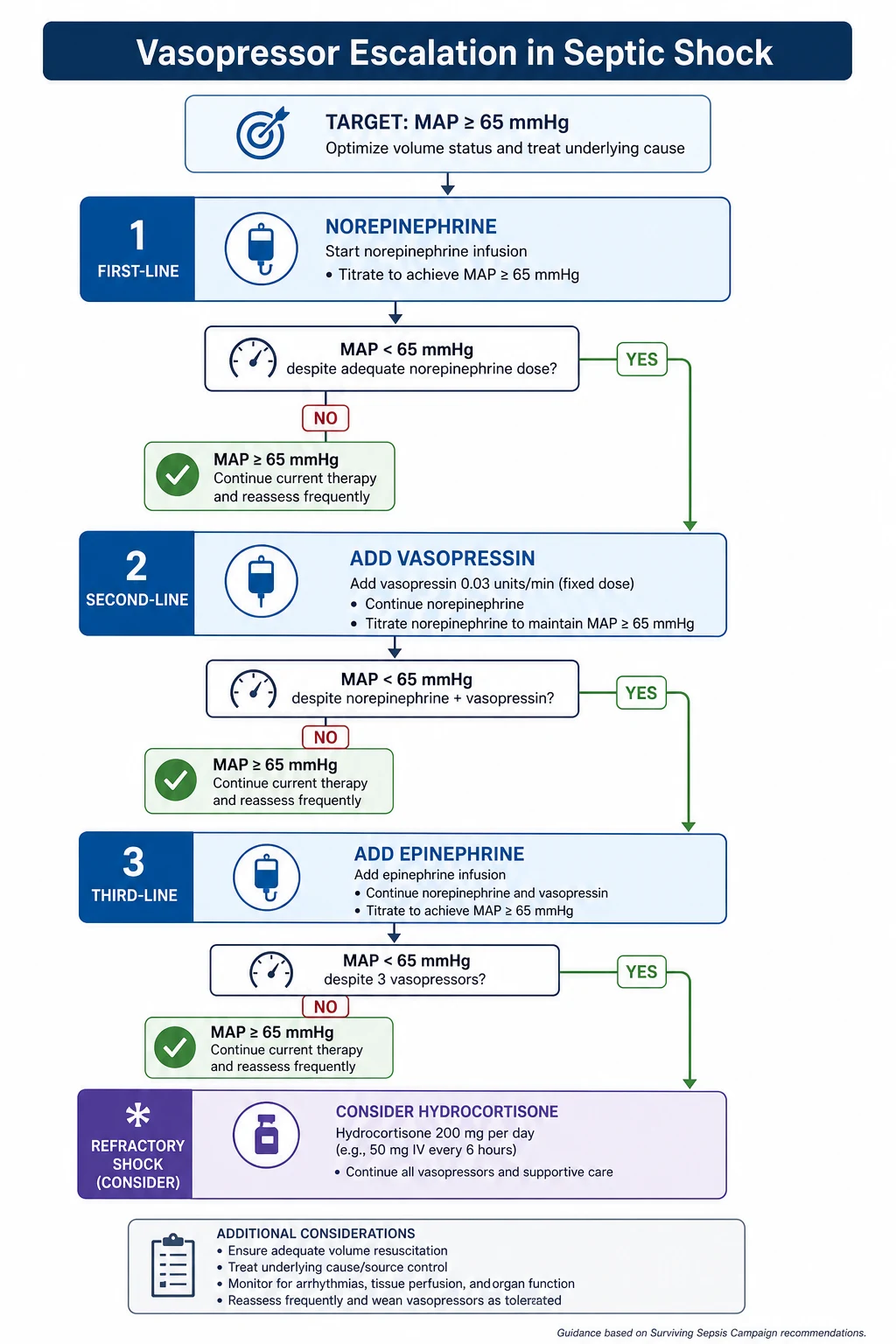
First-line: Norepinephrine
Norepinephrine is the first-line vasopressor for septic shock [4]. It is a pure alpha-adrenergic agonist (with modest beta-1 activity) that increases systemic vascular resistance without significantly increasing heart rate or myocardial oxygen demand. Starting dose: 0.05 to 0.1 microgram/kg/min, titrated to MAP 65 mmHg or above. It should be given through a central venous catheter (though a large-bore peripheral cannula is acceptable for short-term use while central access is obtained, with the risk of extravasation managed by having phentolamine available).
Second-line: Vasopressin
Vasopressin is added when norepinephrine alone does not achieve the target MAP, or when norepinephrine doses are rising (typically above 0.25 to 0.5 microgram/kg/min). It is given at a fixed dose of 0.03 U/min (not titrated — higher doses cause ischaemia). Vasopressin acts via V1 receptors to cause vasoconstriction and is relatively deficient in septic shock (the vasopressin axis is suppressed). The VANISH trial showed that early vasopressin did not improve kidney-failure-free days compared to norepinephrine, but it does allow norepinephrine dose reduction [4].
Third-line: Epinephrine
Epinephrine is the third-line agent if MAP remains below target despite norepinephrine plus vasopressin. Starting dose: 0.05 to 0.1 microgram/kg/min, titrated. Epinephrine has both alpha and beta activity — it increases cardiac output (beta-1) and systemic vascular resistance (alpha). Caution: Epinephrine increases lactate production via beta-2 stimulation of skeletal muscle (aerobic glycolysis), which can make lactate monitoring unreliable as a resuscitation endpoint [4].
Corticosteroids in refractory septic shock
Hydrocortisone 200 mg/day (as a continuous infusion or 50 mg IV every 6 hours) is recommended for patients with refractory septic shock — defined as ongoing vasopressor requirement despite adequate fluid resuscitation and escalating vasopressor doses [4].
The evidence is nuanced. The Annane 2002 trial showed a survival benefit in non-responders to the ACTH stimulation test [10], but the CORTICUS trial (2008) showed no mortality benefit overall, though it did show faster shock reversal [9]. The APROCCHSS trial (2018) found that hydrocortisone plus fludrocortisone reduced 90-day mortality in patients with septic shock on vasopressors [8]. The SSC 2021 guideline recommends hydrocortisone for adults with septic shock requiring ongoing vasopressor therapy (weak recommendation, low-quality evidence).
When to start steroids: When the patient is on moderate-to-high dose vasopressors (norepinephrine equivalent of 0.25 microgram/kg/min or above) and not achieving MAP target despite adequate fluids and two vasopressors. When to stop: Wean as the patient improves — do not stop abruptly (risk of rebound hypotension). Note: The ACTH stimulation test is no longer recommended to guide steroid therapy. [1]
Adjunctive therapies NOT recommended
Vitamin C, thiamine, and hydrocortisone ("HAT" or "metabolic resuscitation" cocktail): The SSC 2021 guideline recommends against high-dose vitamin C monotherapy and suggests against the combination. The ACTS trial (Moskowitz 2020) showed no benefit on SOFA score or outcomes [11]. The VITAMINS trial similarly showed no mortality benefit. This is an exam favourite — the answer is that the combination does not work.
Fluid Responsiveness — the right way to give fluids
After the initial 30 mL/kg, further fluid boluses should be guided by whether the heart can increase stroke volume in response to a fluid challenge. This is the principle of fluid responsiveness: the patient is fluid-responsive if both ventricles are operating on the steep portion of the Frank-Starling curve (preload-dependent). Giving fluid to a patient who is on the flat portion of the curve will increase venous pressure and cause oedema without improving cardiac output. [1]
Dynamic tests of fluid responsiveness
Passive leg raise (PLR) — The best bedside test. Lift the patient's legs to 45 degrees (transferring approximately 300 mL of venous blood from the legs to the thorax). Measure the response: a 10 per cent or greater increase in stroke volume (measured by echocardiography, arterial pulse contour analysis, or end-tidal CO2) indicates fluid responsiveness. PLR is reversible, self-contained, and does not require fluids [4].
Stroke volume variation (SVV) and pulse pressure variation (PPV) — In mechanically ventilated patients with a regular cardiac rhythm and closed chest, a PPV above 12 to 13 per cent or SVV above 10 per cent predicts fluid responsiveness. These are invalid in atrial fibrillation, spontaneous breathing, open chest, right heart failure, and low tidal volume ventilation. [1]
End-tidal CO2 (EtCO2) changes after PLR or fluid challenge — A 5 per cent or greater rise in EtCO2 after PLR is a surrogate for increased cardiac output (more pulmonary blood flow delivers more CO2 to the lungs). [1]
Static parameters — why they are unreliable
Central venous pressure (CVP) and inferior vena cava diameter are poor predictors of fluid responsiveness. CVP is influenced by vascular tone, intrathoracic pressure, right ventricular compliance, and tricuspid regurgitation. The SSC 2021 guideline recommends against using CVP alone to guide fluid therapy [4]. The IVC collapsibility index (greater than 50 per cent collapse on inspiration suggesting volume responsiveness) is better than CVP but still has significant limitations.
Source Control
Source control is the physical intervention to eliminate or reduce the source of infection and restore anatomy to promote recovery. It is as important as antibiotics and should be achieved as soon as practically possible [4].
| Modality | Examples |
|---|---|
| Drainage | Percutaneous drainage of abscess (radiology-guided), chest drain for empyema, ERCP for cholangitis |
| Debridement | Surgical debridement of necrotising fasciitis, peritoneal lavage for perforated viscus |
| Device removal | Removal of infected central venous catheter, urinary catheter change, removal of infected prosthetic material |
Timing: Source control should be achieved within 6 to 12 hours of recognition when feasible. Delayed source control is associated with increased mortality. For necrotising soft tissue infection, source control (surgical debridement) must happen within hours — this is a surgical emergency. [1]
The principle: No amount of antibiotics or vasopressors will overcome an undrained abscess or a necrotic infection. If the patient is not improving despite appropriate antibiotics and resuscitation, the question is always: have we missed a source? [1]
Supportive Care in the ICU
Lung-protective ventilation for sepsis-associated ARDS
Approximately 30 to 40 per cent of patients with septic shock develop ARDS. The standard of care is lung-protective ventilation:
- Tidal volume: 6 mL/kg predicted body weight (PBW, not actual body weight) [1]- Plateau pressure: below 30 cm of water
- PEEP: titrated to maintain oxygenation (FiO2/PEEP ladder)
- Permissive hypercapnia: accept a pH above 7.20 to avoid injurious tidal volumes
- Prone positioning for moderate-to-severe ARDS (PaO2/FiO2 below 150) for 16 hours per day
- Neuromuscular blockade (cisatracurium) for 48 hours in severe ARDS
- Conservative fluid strategy after the initial resuscitation — avoid positive fluid balance [1]
Renal replacement therapy
Approximately 20 to 30 per cent of patients with septic shock develop AKI requiring renal replacement therapy (RRT). Indications: refractory hyperkalaemia (K above 6.5 mmol/L not responding to medical therapy), refractory metabolic acidosis (pH below 7.15), volume overload unresponsive to diuretics, and uraemic complications. Continuous renal replacement therapy (CRRT) or sustained low-efficiency dialysis (SLED) is generally preferred over intermittent haemodialysis in haemodynamically unstable patients. [1]
Glycaemic control
Target blood glucose: 140 to 180 mg/dL (7.8 to 10.0 mmol/L) [4]. The NICE-SUGAR trial showed that intensive insulin therapy (target 81 to 108 mg/dL) increased hypoglycaemia and mortality compared to a target of 140 to 180 mg/dL. Hypoglycaemia is dangerous and easily missed in sedated patients. Use an insulin infusion protocol with hourly glucose monitoring initially.
DVT prophylaxis
All septic patients are at high risk of venous thromboembolism. Give enoxaparin 40 mg subcutaneously daily (or 20 mg daily if creatinine clearance is below 30 mL/min) or unfractionated heparin 5000 units subcutaneously every 8 to 12 hours. Use intermittent pneumatic compression as an adjunct or if anticoagulation is contraindicated. [1]
Stress ulcer prophylaxis
Give a proton pump inhibitor (e.g., pantoprazole 40 mg IV daily) to patients who are mechanically ventilated for more than 48 hours or have coagulopathy (platelets below 50, INR above 1.5, or partial thromboplastin time above twice normal). These are the two strongest risk factors for stress-related mucosal disease [4].
Nutrition
Early enteral nutrition (trophic feeding, 10 to 20 mL/hour, within 24 to 48 hours) is recommended. Parenteral nutrition is reserved for patients who cannot meet nutritional needs enterally after 7 days. Avoid full-calorie enteral feeding in the first week — trophic feeding is safer and outcomes are equivalent [4].
Special Situations
Neutropenic sepsis
Neutropenic sepsis (neutrophil count below 0.5 x 10^9/L or below 1.0 with anticipated fall) is a medical emergency. The IDSA guideline mandates empiric broad-spectrum antibiotics within one hour of presentation [13].
Empiric regimen: Piperacillin-tazobactam 4.5 g IV every 6 to 8 hours (monotherapy in most cases). Add vancomycin (15 to 20 mg/kg every 8 to 12 hours, or by dosing nomogram) if there is suspected catheter-related infection, known MRSA colonisation, severe mucositis, haemodynamic instability, or pneumonia. Add antifungal cover (echinocandin such as caspofungin or liposomal amphotericin B) if the patient has persistent fever after 4 to 7 days of broad-spectrum antibiotics. [1]
Key principles:
- Do not delay antibiotics for cultures — take cultures then treat immediately.
- The patient may be afebrile — neutropenic patients may not mount a fever. Any unwell neutropenic patient is presumed to have neutropenic sepsis.
- Look for the source: central line, perianal area (do NOT perform digital rectal examination), mouth (mucositis), lungs, skin.
- Colony-stimulating factors (G-CSF) are not routinely recommended for acute management. [1]
Sepsis in pregnancy
Sepsis in pregnancy is complicated by the physiological adaptations of pregnancy — tachycardia, increased cardiac output, decreased systemic vascular resistance, mild respiratory alkalosis, and mild leukocytosis — which can mask the signs of sepsis. The most common sources are pyelonephritis, chorioamnionitis, and postpartum wound or uterine infection. [1]
Antibiotics in pregnancy: Most standard sepsis antibiotics are safe — piperacillin-tazobactam, ceftriaxone, clindamycin, gentamicin (short course with therapeutic drug monitoring). Avoid tetracyclines, quinolones (relative), and trimethoprim in the first trimester. Add metronidazole for intra-abdominal or pelvic sources. The fetus is a second patient — consult obstetrics early regarding delivery if chorioamnionitis is the source. [1]
Sepsis in cirrhosis
Cirrhosis is the prototypical immunocompromised state. Cirrhotic patients have impaired reticuloendothelial function, complement deficiency, and gut bacterial translocation. They are at high risk of spontaneous bacterial peritonitis, bacteraemia from gut organisms, and overwhelming infection. They may be afebrile, and their inflammatory markers may be blunted. [1]
Empiric regimen: Third-generation cephalosporin (cefotaxime 2 g IV every 8 hours or ceftriaxone 2 g IV daily) for community-acquired infection. For nosocomial infection, broaden to piperacillin-tazobactam or meropenem. Consider adding MRSA cover (vancomycin) and antifungal cover (especially if on long-term proton pump inhibitor or broad-spectrum antibiotics). Albumin 1.5 g/kg on day 1 and 1 g/kg on day 3 is indicated for spontaneous bacterial peritonitis (reduces renal failure and mortality). [1]
Post-Sepsis Recovery — the survivorship problem
Survival from sepsis is not the end of the story. Sepsis survivors face a constellation of long-term problems collectively termed post-intensive care syndrome (PICS) and, more specifically, post-sepsis syndrome. [1]
Cognitive impairment
The Iwashyna et al. study (2010) using the Health and Retirement Study cohort showed that severe sepsis survivors had a threefold increase in moderate-to-severe cognitive impairment after hospitalisation. This is independent of age and pre-existing cognitive function. The cognitive domains affected are executive function, attention, and processing speed [12]. The mechanism is multifactorial: septic encephalopathy, microvascular thrombosis, neuroinflammation, and prolonged sedation.
Functional decline
Sepsis survivors acquire an average of 1 to 2 new activities of daily living (ADL) dependencies per episode. Up to 30 per cent require new institutional care or increased home assistance. The functional trajectory often does not return to baseline — each sepsis hospitalisation accelerates functional decline. [1]
Psychological sequelae
Post-traumatic stress disorder (PTSD), anxiety, and depression affect 20 to 40 per cent of sepsis survivors. Recall of delusional memories from ICU delirium is a major contributor. ICU diaries, early rehabilitation, and psychological follow-up can mitigate this. [1]
Increased mortality
Sepsis survivors have a 40 per cent 1-year mortality and remain at elevated risk for years. Recurrent infection (especially in the first 90 days) is common, reflecting persistent immune dysfunction. [1]
Management of the sepsis survivor
The SSC 2021 guideline, for the first time, included recommendations for post-ICU follow-up: screening for cognitive impairment, functional assessment, psychological support, and early rehabilitation. In the ANZ context, ICU follow-up clinics and rehabilitation programmes are increasingly available. The physician managing a post-sepsis patient in a DCE long case must address these domains proactively [4].
High-Yield Exam Discriminators
- qSOFA is not a diagnostic criterion — it is a mortality-prediction prompt. Sepsis is diagnosed by suspected infection plus SOFA change of 2 or more.
- Septic shock requires both criteria — vasopressors for MAP 65 or above AND lactate above 2, despite fluids. One without the other is not septic shock by the Sepsis-3 definition.
- Norepinephrine is first-line — not epinephrine, not dopamine, not phenylephrine. Dopamine causes more arrhythmias and is not recommended [4].
- 30 mL/kg is a starting dose — not a target. Subsequent fluids must be guided by fluid responsiveness.
- Steroids are for refractory shock only — not for all septic shock. The threshold is ongoing vasopressor requirement despite adequate fluids.
- Vitamin C does not work — SSC 2021 recommends against it.
- Blood cultures before antibiotics only if no delay — never delay antibiotics beyond 45 to 60 minutes for cultures.
- MAP target is 65 mmHg — not 70, not 80. Higher targets do not improve outcomes.
- Balanced crystalloids over saline — hyperchloraemic acidosis worsens renal outcomes.
- Source control is non-negotiable — no antibiotic regimen overcomes an undrained abscess.
Regional Guideline Deltas
| Aspect | ANZ (ANZICS / NHMRC) | UK (NICE NG51) | US (SSC 2021) |
|---|---|---|---|
| Screening trigger | NEWS2, Between the Flags | NEWS2 | qSOFA, SIRS |
| Fluids | Balanced crystalloid, 30 mL/kg | Crystalloid, 30 mL/kg in first 3 hours | Balanced crystalloid, 30 mL/kg |
| Corticosteroids | Hydrocortisone for refractory shock | Consider if shock unresponsive to fluids and vasopressors | Hydrocortisone for ongoing vasopressor requirement |
| Antibiotic timing | Within 1 hour for shock | Within 1 hour for high-risk sepsis | Within 1 hour for shock or high-probability sepsis |
NICE NG51 (Sepsis: Recognition, Assessment and Early Management) is the UK primary guideline and uses a risk-stratified approach based on age and physiological parameters. It is more granular than the SSC guidelines for the non-ICU setting. In the ANZ setting, the Australian Commission on Safety and Quality in Health Care has published a national consensus statement on sepsis, and most hospitals have local sepsis pathways. [1]
Communication and Shared Decision-Making
In the acute phase, communication is primarily with the family: explaining what sepsis is, the prognosis, the treatments, and the plan for the next 24 hours. The message should be honest: "your relative has a life-threatening infection, we are treating it aggressively, the next 24 to 48 hours are critical, and the mortality risk is significant." [1]
In the recovery phase (DCE long case territory), the physician must address the post-sepsis trajectory: cognitive and functional recovery, psychological support, prevention of recurrence (vaccination, especially pneumococcal and influenza), and advance care planning. Many sepsis survivors (and their families) are profoundly affected by the experience and benefit from structured follow-up [12].
Summary: the sepsis consultation in one paragraph
Suspect sepsis in any patient with infection and new organ dysfunction. Apply the Hour-1 Bundle immediately: lactate, cultures, antibiotics within one hour, 30 mL/kg crystalloid if hypotensive or lactate 4 or above, norepinephrine for MAP below 65. Assess fluid responsiveness before giving more fluids. Achieve source control as soon as feasible. Add vasopressin and then epinephrine if MAP is not achieved. Start hydrocortisone 200 mg/day for refractory shock. Provide lung-protective ventilation, glycaemic control (140 to 180), DVT and stress ulcer prophylaxis, and early trophic enteral nutrition. De-escalate antibiotics at 48 to 72 hours. Plan for post-sepsis recovery from day one. [1]
References
- [1]Singer M, Deutschman CS, Seymour CW, et al. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA, 2016.PMID 26903336
- [2]Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA, 2016.PMID 26903335
- [3]Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA, 2016.PMID 26903336
- [4]Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021 Intensive Care Med, 2021.PMID 34599691
- [5]Levy MM, Evans LE, Rhodes A The Surviving Sepsis Campaign Bundle: 2018 update Intensive Care Med, 2018.PMID 29675566
- [6]Seymour CW, Gesten F, Prescott HC, et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis N Engl J Med, 2017.PMID 28528569
- [7]ARISE Investigators, ANZICS Clinical Trials Group Goal-directed resuscitation for patients with early septic shock N Engl J Med, 2014.PMID 25272316
- [8]Annane D, Renault A, Brun-Buisson C, et al. Hydrocortisone plus Fludrocortisone for Adults with Septic Shock N Engl J Med, 2018.PMID 29490185
- [9]Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for patients with septic shock N Engl J Med, 2008.PMID 18184957
- [10]Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock JAMA, 2002.PMID 12186604
- [11]Moskowitz A, Huang DT, Hou PC, et al. Effect of Ascorbic Acid, Corticosteroids, and Thiamine on Organ Injury in Septic Shock: The ACTS Randomized Clinical Trial JAMA, 2020.PMID 32809003
- [12]Iwashyna TJ, Ely EW, Smith DM, Langa KM Long-term cognitive impairment and functional disability among survivors of severe sepsis JAMA, 2010.PMID 20978258
- [13]Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america Clin Infect Dis, 2011.PMID 21258094