Phys · infectious
Tropical and Travel-Related Infections
Also known as fever in returning traveller · imported malaria · falciparum malaria · severe malaria · dengue fever · dengue haemorrhagic fever · enteric fever · typhoid fever · scrub typhus · Katayama fever · acute schistosomiasis · Weil disease · leptospirosis · melioidosis · strongyloides hyperinfection · eosinophilia in returning traveller
Consultant-physician-depth guide to the febrile returning traveller — the incubation-period framework that narrows the differential, the rule-out-malaria-first principle, falciparum malaria (thick and thin films, RDT, IV artesunate for severe disease and artemether-lumefantrine for uncomplicated disease), dengue (breakbone fever, plasma leakage, warning signs, fluid-centred supportive care), enteric (typhoid) fever with the step-ladder pattern and ceftriaxone, rickettsial disease (eschar, doxycycline), schistosomiasis (Katayama fever, eosinophilia, praziquantel), leptospirosis (Weil disease), melioidosis in northern Australia (ceftazidime then prolonged oral eradication), the intestinal parasites giardia, amoeba and strongyloides (hyperinfection risk), the eosinophilia workup, and pre-travel advice — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Tropical and Travel-Related Infections



The one-minute consultant answer
A fever in a returning traveller is malaria until proven otherwise — and the single most dangerous mistake in tropical medicine is sending a febrile traveller home after one negative blood film. The GeoSentinel Surveillance Network found that among ill returned travellers presenting with fever, malaria was the most common specific diagnosis (21 per cent), that 26 per cent were hospitalised, and that malaria accounted for a third of the deaths [1]. The framework that drives every decision is therefore: take a precise travel and exposure history, send the minimum investigation set immediately, and rule out falciparum malaria first — because untreated severe falciparum malaria is nearly 100 per cent fatal within 24 to 48 hours.
Two questions change everything. First, where did they go, and when did they return? The incubation period narrows the differential. Fever within one week of return points to arboviruses (dengue, chikungunya), plague or anthrax. Fever one to four weeks after return brings in malaria, typhoid, dengue, rickettsial disease, leptospirosis and schistosomiasis. Fever weeks to months later raises tuberculosis, visceral leishmaniasis, amoebic liver abscess and chronic schistosomiasis. Second, what did they do? Freshwater exposure points to schistosomiasis and leptospirosis; rural Asia or northern Australia in the wet season points to scrub typhus and melioidosis; visiting friends and relatives (VFR travellers, who often take no prophylaxis) is the highest-risk group for falciparum malaria and typhoid. [1]
The treatment decisions that examiners test are few and must be automatic: severe falciparum malaria gets IV artesunate 2.4 mg/kg at 0, 12 and 24 hours then daily — the SEAQUAMAT trial showed a 35 per cent mortality reduction versus quinine in adults [2], and AQUAMAT confirmed a 22.5 per cent reduction in African children [3]. Uncomplicated falciparum malaria gets an oral artemisinin-based combination therapy (ACT) — artemether-lumefantrine, six doses over three days with fatty food. Dengue has no specific antiviral — management is careful fluid-centred supportive care, avoiding NSAIDs and aspirin because of bleeding risk. Typhoid gets ceftriaxone (fluoroquinolones are unreliable because of resistance). Rickettsial disease gets doxycycline — empirically, before serology returns. Schistosomiasis gets praziquantel, leptospirosis gets ceftriaxone or doxycycline, melioidosis gets ceftazidime then a three-month oral eradication phase, and strongyloides gets ivermectin — but only after you have screened for it, because giving corticosteroids to a carrier triggers fatal hyperinfection.
The incubation-period framework — the discriminator that drives the differential
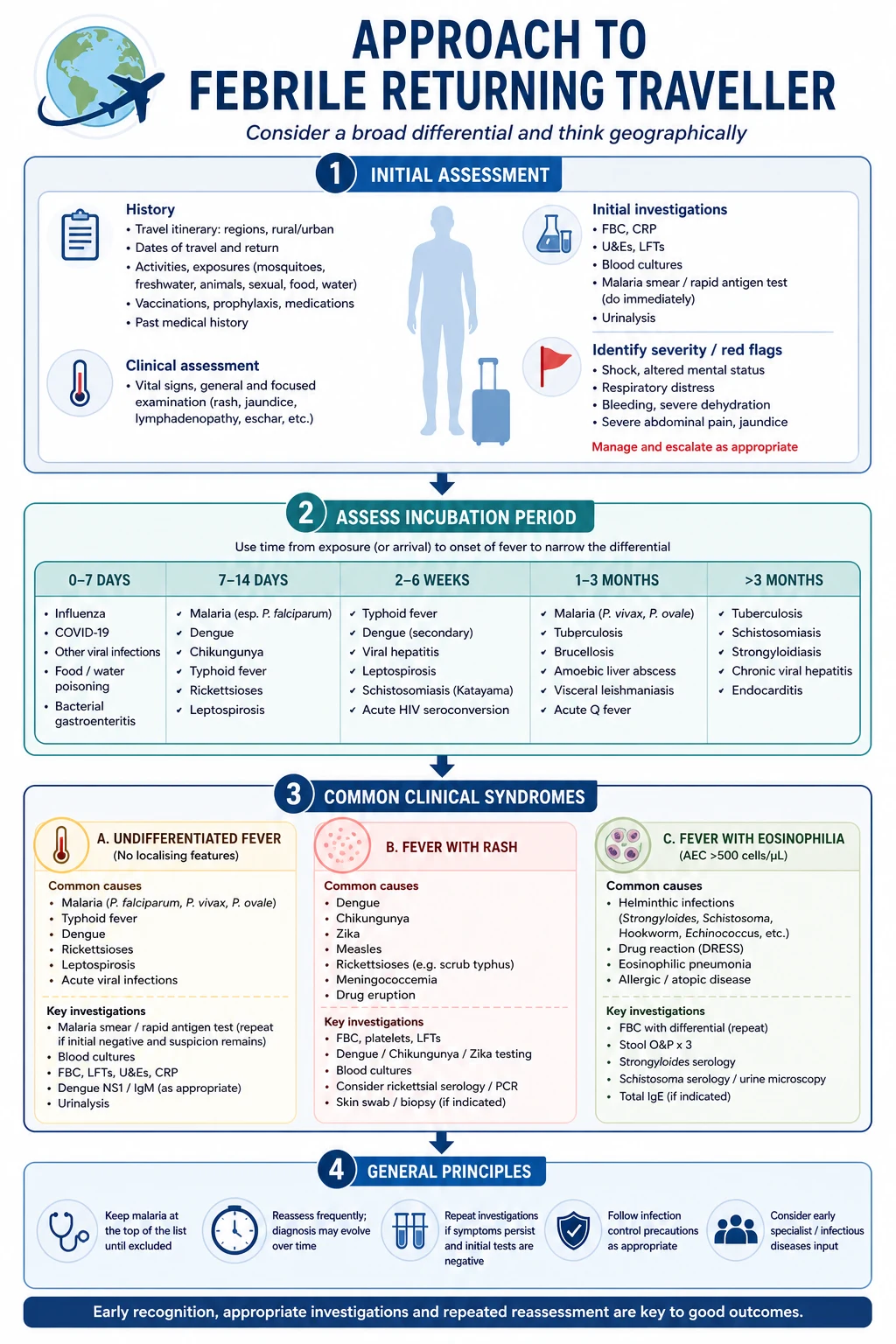
The incubation period is the single most powerful discriminator in a febrile traveller. It turns a bewildering list of tropical infections into a short, actionable one. Memorise three windows. [1]
Under one week from exposure or return. The infection was acquired very recently, which excludes anything with a long latent period. Think: arboviruses (dengue, chikungunya, Zika, yellow fever), plague, anthrax, influenza, and common bacterial infections. Malaria can present this early but is unusual before day 7. [1]
One to four weeks. This is the highest-yield window for exam purposes, and the home of the big four: falciparum malaria, typhoid (enteric fever), dengue, and rickettsial disease (especially scrub typhus). Also leptospirosis, melioidosis, acute schistosomiasis (Katayama fever), viral haemorrhagic fevers (Ebola 2 to 21 days), and viral hepatitis. Most returners who are genuinely unwell fall here. [1]
Weeks to months. Long-incubation infections: tuberculosis, visceral leishmaniasis (kala-azar), chronic schistosomiasis, amoebic liver abscess, brucellosis, Q fever, and the chronic carrier states of typhoid. A fever six months after return is not acute dengue. [1]
The exposure history then refines the list within each window. Ask explicitly and document: [1]
- Freshwater exposure (swimming, wading, rafting in lakes, rivers, streams) — schistosomiasis, leptospirosis.
- Rural or agricultural Asia, or the Top End of Australia in the wet season — scrub typhus, melioidosis.
- Mosquito exposure without prophylaxis — malaria, dengue, chikungunya, Japanese encephalitis.
- Tick or mite exposure — rickettsial disease (eschar is the clue).
- Animal exposure — leptospirosis (rodents, livestock), Q fever (livestock), brucellosis (unpasteurised dairy).
- Visiting friends and relatives (VFR travel) — highest-risk group for falciparum malaria and typhoid, because they rarely take prophylaxis and assume immunity they no longer have.
- Sexual exposure, injecting drug use, medical procedures abroad — HIV, viral hepatitis. [1]
The exam trap: A traveller returning from sub-Saharan Africa with fever at two weeks is falciparum malaria until proven otherwise, regardless of prophylaxis taken — prophylaxis reduces but never eliminates the risk, and adherence is frequently imperfect. [1]
Malaria — falciparum is the killer
The life cycle in one paragraph (and why it matters)
A female Anopheles mosquito injects sporozoites during a blood meal. Sporozoites travel to the liver and infect hepatocytes, where they multiply (hepatic schizogony, asymptomatic). After one to two weeks, merozoites are released into the bloodstream, where they infect erythrocytes and multiply inside them (erythrocytic schizogony) — this is what causes the clinical illness. Rupture of infected erythrocytes releases more merozoites (and triggers the fever), and a small fraction differentiate into gametocytes, which infect the next mosquito. Two clinical points follow. First, only the erythrocytic stage causes disease — so drugs acting on the liver (primaquine, tafenoquine) do not treat acute illness but prevent relapse. Second, Plasmodium vivax and P. ovale form hypnozoites — dormant liver stages that can reactivate months to years later, causing relapse unless eradicated with primaquine. [1]
Why P. falciparum is the dangerous species
Five species infect humans: falciparum, vivax, ovale, malariae, and knowlesi (the last is a monkey parasite in Southeast Asia that can be as severe as falciparum). P. falciparum is the killer for three reasons: [1]
- High parasitaemia — falciparum can infect any percentage of erythrocytes; the others are limited to young cells (vivax, ovale) or low parasitaemia (malariae).
- Cytoadherence and sequestration — falciparum-infected erythrocytes express a protein (PfEMP1) on their surface that sticks them to the endothelium of capillaries and venules, especially in the brain, kidney, placenta and gut. This sequestration takes the infected cells out of the peripheral circulation (which is why a thin film can underestimate parasitaemia) and causes microvascular obstruction, endothelial activation, and organ dysfunction.
- Rossetting — infected erythrocytes bind uninfected erythrocytes around them, worsening obstruction. [1]
The clinical correlate is the syndrome of severe falciparum malaria: cerebral malaria, severe anaemia, metabolic acidosis, ARDS, renal failure, hypoglycaemia, and DIC. [1]
Clinical presentation
The classic textbook description is cyclical fever with rigors matching synchronous rupture of erythrocytes — the tertian (every 48 hours) or quartan (every 72 hours) pattern. This pattern is unreliable in practice and especially in falciparum infection, where fever is often continuous or irregular. Do not wait for cyclical fever to make the diagnosis. The reliable features are: fever, chills, headache, myalgia, malaise, and often gastrointestinal symptoms (nausea, vomiting, diarrhoea, abdominal pain). A traveller returning from an endemic area with any of these has malaria until excluded. [1]
Diagnosis — thick film for sensitivity, thin film for species and quantification
The thick blood film is the more sensitive test — the red cells are lysed, concentrating parasites by 20- to 40-fold, so a parasitaemia as low as 10 to 50 parasites per microlitre can be detected. The thin blood film preserves red cell morphology and allows species identification (falciparum has ring forms, often multiple rings per cell, and banana-shaped gametocytes; vivax has enlarged, stippled infected cells and amoeboid trophozoites) and quantification of parasitaemia (percentage of infected erythrocytes), which drives severity assessment and treatment monitoring. [1]
The rule that must never be broken: a single negative film does not exclude malaria. Parasitaemia is cyclical, and in early or partially immune infection the burden can be below the detection threshold of one film. Repeat thick and thin films every 12 to 24 hours for at least three sets over 48 to 72 hours before accepting that malaria is excluded. This is the single most common and most dangerous error in tropical medicine. [1]
Rapid diagnostic tests (RDTs) detect parasite antigens and are useful where microscopy is unavailable. HRP-2 (histidine-rich protein 2) is highly sensitive for falciparum but persists for weeks after treatment (so a positive RDT does not mean active infection in a recently treated patient), and HRP-2 gene deletions in some falciparum strains (especially in South America and the Horn of Africa) cause false negatives. pLDH-based tests allow some species differentiation. RDTs do not quantify parasitaemia, so microscopy remains essential for severity assessment and monitoring. [1]
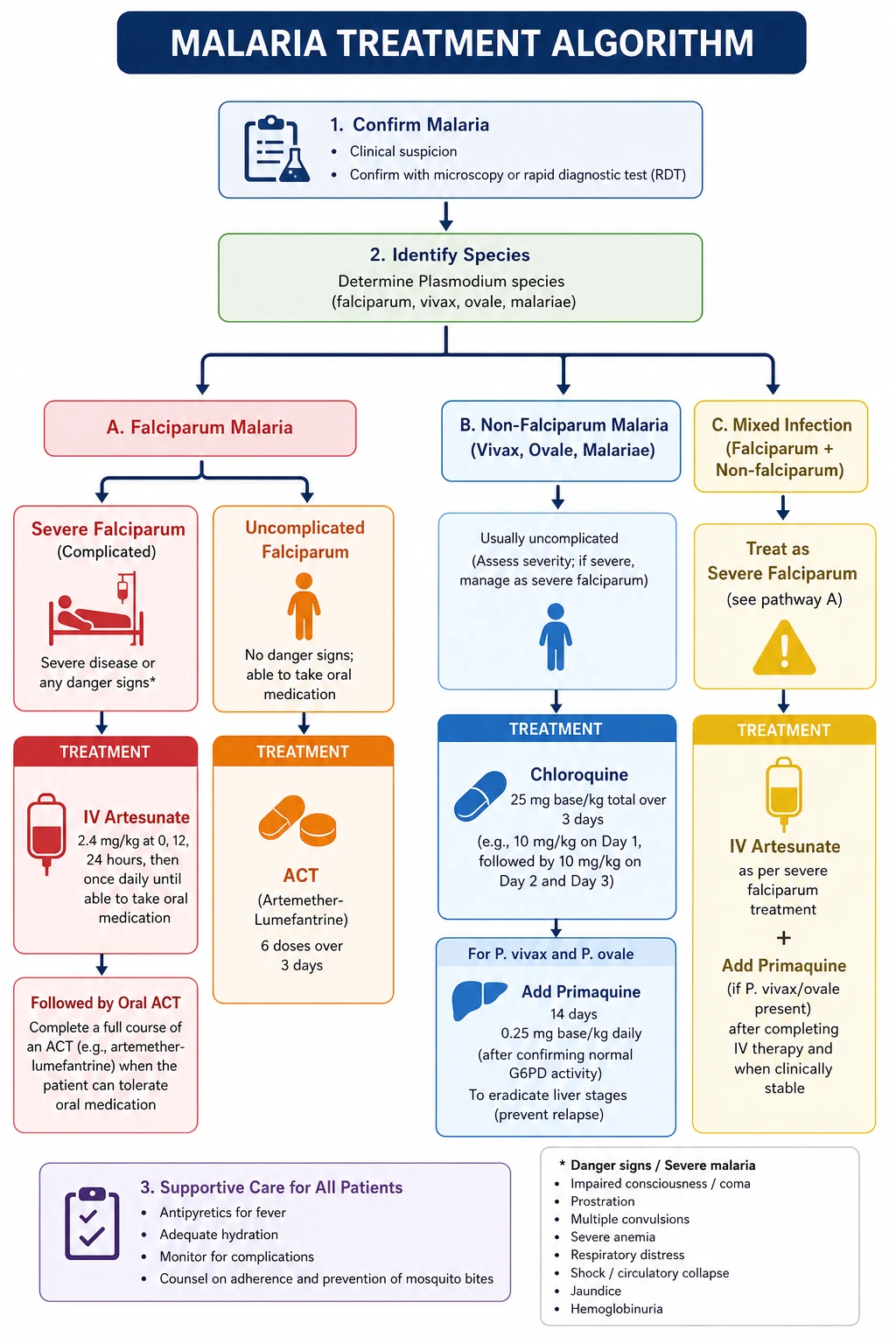
Severe falciparum malaria — recognise it and give artesunate immediately
Severe malaria is defined by any WHO severity criterion. The exam-relevant ones are: impaired consciousness (GCS below 11, or multiple seizures), prostration (inability to sit or stand), respiratory distress (acidotic breathing or ARDS), jaundice (bilirubin above 50 micromol/L), hyperparasitaemia (above 2 per cent in non-immune, above 10 per cent in semi-immune), metabolic acidosis (bicarbonate below 15 mmol/L or lactate above 5), renal impairment (creatinine above 265 micromol/L or oliguria), hypoglycaemia (below 2.2 mmol/L), and important bleeding or DIC. [1]
Treatment of severe falciparum malaria is IV artesunate 2.4 mg/kg at 0, 12, and 24 hours, then daily until oral therapy is tolerated, then a full course of oral ACT. The SEAQUAMAT trial established IV artesunate as superior to IV quinine in adults — mortality was 15 per cent with artesunate versus 22 per cent with quinine, a 34.7 per cent relative reduction [2]. AQUAMAT confirmed the benefit in African children, with a 22.5 per cent mortality reduction [3]. Artesunate is also simpler (no loading-dose calculation, no cardiac monitoring) and safer (quinine causes hypoglycaemia from insulin stimulation, especially in pregnancy, and is cardiotoxic). IV artesunate should be given immediately severe malaria is recognised — do not wait for the parasitaemia to climb.
Post-artesunate delayed haemolysis (PADH) — the trap after recovery
A specific complication of artesunate must be anticipated: post-artesunate delayed haemolysis (PADH), occurring 1 to 4 weeks after treatment. The mechanism is the pitting response — the spleen expels the dead parasite from the infected erythrocyte, returning the once-infected "pitted" cell to the circulation with a shortened lifespan; these cells then haemolyse a week or more later. Jauréguiberry and colleagues showed that among non-transfused travellers treated with artesunate for severe malaria, 22 per cent developed delayed haemolysis, predictable from the early concentration of once-infected erythrocytes [4]. The practical implication: monitor haemoglobin weekly for four weeks after artesunate in any non-immune traveller treated for severe malaria.
Uncomplicated falciparum malaria — oral ACT
Uncomplicated falciparum malaria (no severity criteria, able to take oral medication, low parasitaemia) is treated with an artemisinin-based combination therapy (ACT). The combination partners a fast-clearing artemisinin derivative (short half-life, reduces the parasite burden rapidly) with a longer half-living partner drug (eliminates the residual parasites and prevents resistance). The standard is artemether-lumefantrine, six doses over three days at 0, 8, 24, 36, 48 and 60 hours, taken with fatty food because lumefantrine absorption is fat-dependent (a common reason for treatment failure is taking it fasting). Alternative ACTs include artesunate-amodiaquine, dihydroartemisinin-piperaquine (watch for QT prolongation), and artesunate-pyronaridine. [1]
Non-falciparum malaria — chloroquine plus primaquine for radical cure
P. vivax, P. ovale, P. malariae and P. knowlesi are generally less severe but still require treatment. For chloroquine-sensitive strains, give chloroquine (total 25 mg base/kg over three days). Crucially, P. vivax and P. ovale require primaquine (0.25 to 0.5 mg/kg daily for 14 days) — or the single-dose tafenoquine — to eradicate the hypnozoite liver stage and prevent relapse. Always check G6PD status before primaquine, because it causes life-threatening haemolysis in G6PD-deficient patients. In Papua New Guinea and Indonesia, vivax is chloroquine-resistant and requires an ACT. P. knowlesi (Southeast Asia) can be severe and is treated as falciparum. [1]
Malaria in pregnancy
Malaria in pregnancy is more severe, with higher parasitaemia, hypoglycaemia, pulmonary oedema, and adverse fetal outcomes (miscarriage, stillbirth, low birthweight). IV artesunate is used for severe disease in all trimesters (it is safer than quinine). For uncomplicated falciparum in pregnancy, the ACT of choice depends on trimester — artemether-lumefantrine is now WHO-recommended in all trimesters based on safety data; quinine plus clindamycin is an older alternative. Primaquine and tetracyclines are contraindicated in pregnancy. [1]
Dengue — breakbone fever and the plasma-leakage trap
Dengue is the most common arboviral infection in returning travellers, transmitted by Aedes mosquitoes (mainly A. aegypti) that bite during the day. It is caused by four serotypes (DEN-1 to DEN-4); infection with one serotype gives lifelong immunity to that serotype but not the others, and a second infection with a different serotype carries a higher risk of severe dengue through antibody-dependent enhancement. [1]
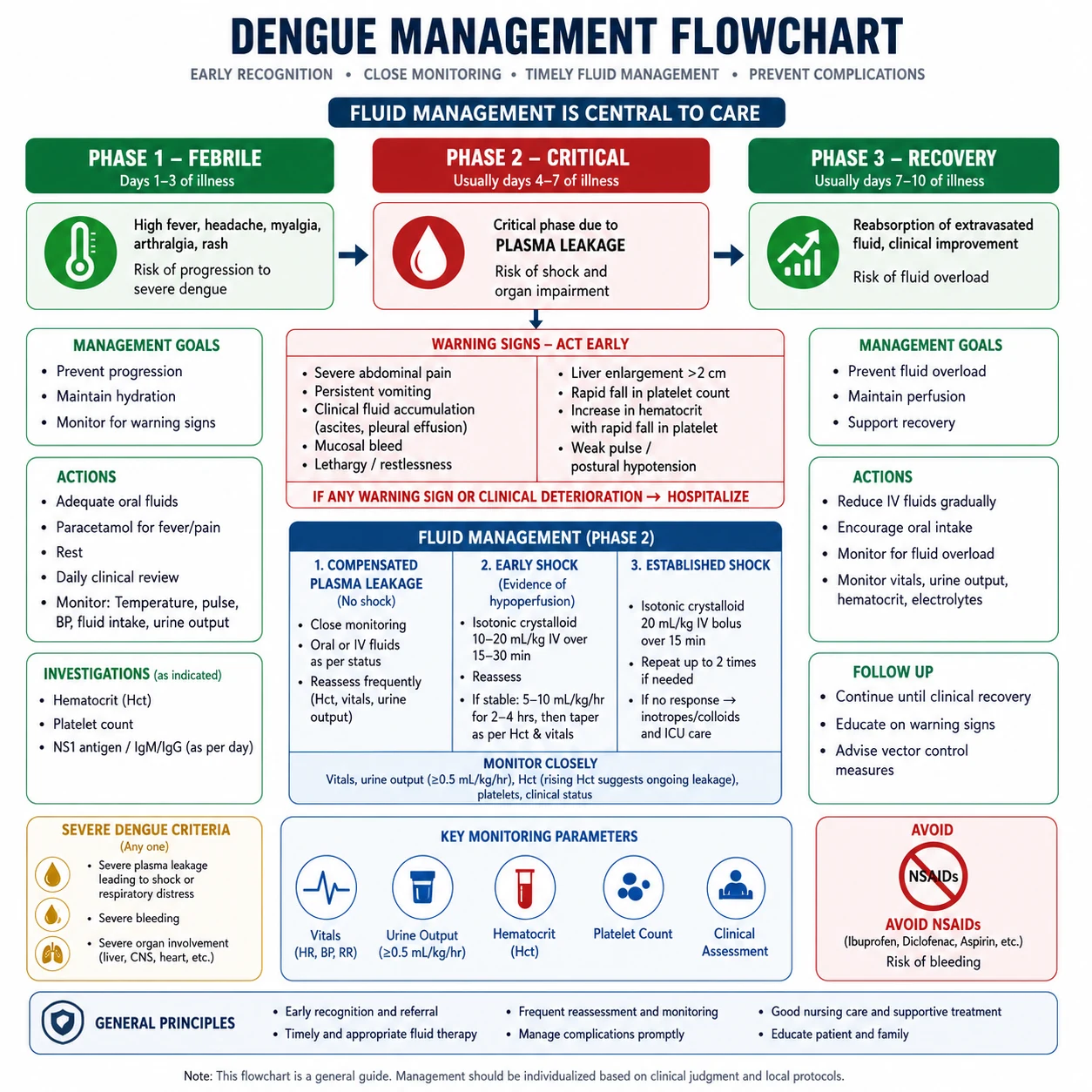
Clinical presentation and the three phases
Dengue has a characteristic three-phase course that drives every management decision [5]:
-
Febrile phase (days 1 to 3) — sudden high fever (often 39 to 40 degrees), severe headache, retro-orbital pain (pain behind the eyes, a classic discriminator), myalgia and arthralgia so severe it earns the name breakbone fever, a maculopapular rash in many patients, mild haemorrhagic manifestations (petechiae, easy bruising, epistaxis), and leucopenia with thrombocytopenia. [1]
-
Critical phase (days 3 to 7, around defervescence) — as the fever settles, a subset of patients develop plasma leakage: increased capillary permeability causes fluid to shift into the third space, producing haemoconcentration (rising haematocrit), hypoalbuminaemia, pleural effusions and ascites. This is the dangerous window. The defervescence of fever is not recovery — it is the moment of maximum risk. [1]
-
Recovery phase (days 7 to 10) — capillary leak resolves, the haematocrit falls as fluid returns to the intravascular space, platelets recover, and the patient clinically improves. [1]
Warning signs — the trigger to escalate
The WHO warning signs identify the patient about to enter the critical phase and dictate admission for close monitoring and fluid management: [1]
- Abdominal pain or tenderness
- Persistent vomiting (more than twice in a day, or inability to tolerate oral fluids)
- Clinical fluid accumulation (pleural effusion, ascites)
- Mucosal bleeding (gum bleeding, epistaxis, menorrhagia, haematemesis, melaena)
- Lethargy or restlessness
- Hepatomegaly (more than 2 cm)
- Rising haematocrit with a falling platelet count — the laboratory signature of impending plasma leakage. [1]
Narrow pulse pressure (20 mmHg or below) is a bedside sign of impending dengue shock. [1]
Severe dengue — dengue shock syndrome and severe bleeding
Severe dengue is defined by one of: severe plasma leakage leading to shock (dengue shock syndrome) or fluid accumulation with respiratory distress, severe bleeding, or severe organ impairment (AST or ALT above 1000, impaired consciousness, myocarditis). Untreated dengue shock has a mortality above 20 per cent; with good supportive care it falls below 1 per cent. [1]
Management — fluid is everything
There is no specific antiviral for dengue. Management is supportive and the single most important intervention is careful fluid management during the critical phase — the goal is to maintain effective intravascular volume during the period of capillary leak without causing fluid overload when the leak resolves. [1]
- Febrile phase: oral fluids, paracetamol for fever. Never give aspirin or NSAIDs — the combination of thrombocytopenia and platelet dysfunction risks severe bleeding.
- Critical phase with warning signs: admit, monitor haematocrit, platelet count, urine output and vital signs every few hours. Give isotonic crystalloid (Hartmann or normal saline) at 5 to 10 mL/kg/hour, titrated to haematocrit and urine output.
- Dengue shock: cautious isotonic crystalloid bolus (10 to 20 mL/kg over one hour), then titrate. If shock persists, add colloid and consider ICU. Over-resuscitation is the major iatrogenic harm — it causes pulmonary oedema when the capillary leak resolves.
- Recovery phase: taper intravenous fluid as the haematocrit stabilises and urine output improves. This is the second classic trap — continuing full-rate fluid into the recovery phase causes pulmonary oedema. [1]
Diagnosis
NS1 antigen is detectable in the first one to five days (febrile phase) and is the test of choice early. After day 5, IgM and IgG serology becomes positive (IgM indicates recent infection; IgG high titre with IgM suggests secondary infection). A positive NS1 in the febrile phase confirms dengue. Monitor with daily full blood count for the platelet trend and haematocrit (the plasma-leakage marker). [1]
Enteric (typhoid) fever — the step-ladder pattern
Typhoid fever is caused by Salmonella Typhi (and paratyphoid by S. Paratyphi A, B and C), transmitted by the faecal-oral route through contaminated food or water. It remains a major global burden, with an estimated 14.3 million cases and 136,000 deaths in 2017 [6]. Travellers to South Asia (especially India, Pakistan, Bangladesh) are at highest risk; the rise of extensively drug-resistant (XDR) S. Typhi in Pakistan — resistant to first-line agents, fluoroquinolones, and third-generation cephalosporins — has reshaped empiric therapy.
Clinical presentation
The textbook description, which examiners love, is: [1]
- Step-ladder fever — the temperature rises in a stepwise fashion over the first week, settling into a continuous high fever (unlike the abrupt onset of malaria or dengue).
- Relative bradycardia (Faget sign) — the pulse is slower than expected for the degree of fever (normally, fever raises the pulse by about 10 beats per minute per degree Celsius; in typhoid this pulse-temperature dissociation is a classic but imperfect sign).
- Rose spots — faint salmon-pink macules, 2 to 4 mm, blanching, on the upper abdomen and lower chest, appearing in the second week. They are easy to miss in dark skin.
- Splenomegaly and dry cough (the cough often misleads clinicians toward a respiratory diagnosis early on).
- Abdominal pain, with constipation more than diarrhoea in the early phase (a counter-intuitive point — typhoid is a constipation illness early, not the watery diarrhoea of a typical gastroenteritis).
- A coated tongue ("typhoid tongue") and relative leucopenia with a left shift. [1]
Untreated, the illness lasts four weeks and follows a characteristic course: the fever rises in week one, plateaus in week two (when rose spots and splenomegaly are maximal), and in the third or fourth week the Peyer patch ulcers in the terminal ileum may perforate or bleed — the life-threatening complications. [1]
Diagnosis
Blood culture is the gold standard and is most sensitive (70 to 90 per cent) in the first week of illness — this is a key teaching point: take blood cultures early. Sensitivity falls as the illness progresses. Stool and urine cultures become positive later. Bone marrow culture is the most sensitive of all (85 to 95 per cent) and is useful if the patient has already taken antibiotics. The Widal test (agglutination antibodies) is unreliable — it has poor sensitivity and specificity, varies by region, and should not be relied upon for diagnosis. NAAT (PCR) is increasingly available. [1]
Management
Empiric therapy has changed because of resistance. Historically, fluoroquinolones (ciprofloxacin) were first-line, but high rates of fluoroquinolone resistance (especially from South Asia — the nalidixic-acid-resistant strains that have poor response to ciprofloxacin) have made them unreliable for empiric use. [1]
- Uncomplicated typhoid: azithromycin 500 mg daily for 5 to 7 days (oral or IV) — effective against most strains including many XDR.
- Severe typhoid: ceftriaxone 2 g IV daily for 10 to 14 days.
- XDR typhoid (resistant to ceftriaxone): azithromycin or carbapenem (meropenem) for severe disease. [1]
Do not switch antibiotics prematurely if the fever has not settled by day 3 — ceftriaxone takes 3 to 7 days to defervesce typhoid, and a slow response in an otherwise improving patient is expected. This is a classic exam trap. [1]
Complications
The two life-threatening complications occur in the third to fourth week: [1]
- Intestinal perforation — at a Peyer patch ulcer in the terminal ileum. Presents with sudden severe abdominal pain, rigidity, and signs of peritonitis. Surgical emergency — emergency laparotomy with repair, plus IV ceftriaxone and metronidazole to cover the peritonitis.
- Gastrointestinal haemorrhage — from erosion into a vessel in an ulcer. [1]
Less common complications include encephalopathy ("typhoid state"), cholecystitis, osteomyelitis, and the chronic carrier state (gallbladder colonisation, especially with gallstones) — treated with prolonged ciprofloxacin or cholecystectomy. [1]
Rickettsial disease — the eschar and doxycycline
Rickettsial diseases are obligate intracellular bacteria transmitted by ticks, mites and fleas. Three groups matter in travellers: the spotted fever group (African tick bite fever, Mediterranean spotted fever), the typhus group (epidemic and endemic typhus), and scrub typhus — the most important in the ANZ and Asia-Pacific region, caused by Orientia tsutsugamushi and transmitted by the larval stage of trombiculid mites ("chiggers"). [1]
Scrub typhus — the eschar is pathognomonic
The classic presentation is fever, headache, myalgia, and an eschar — a black-crusted necrotic lesion with a surrounding red halo at the site of the mite bite, often in the genital, axillary or popliteal area where clothing fits tightly. Regional lymphadenopathy and a maculopapular rash (which may involve the palms and soles) are common. The illness is acquired in rural or agricultural Asia (the "tsutsugamushi triangle" from Japan to northern Australia to Pakistan), especially in the wet season. [1]
Severe scrub typhus causes multi-organ dysfunction — ARDS, meningoencephalitis, AKI, myocarditis and DIC — and can be fatal. The INTREST trial (2023) established that combination IV doxycycline plus azithromycin was superior to either alone for severe scrub typhus, with a composite outcome (death at day 28, persistent complications at day 7, or persistent fever at day 5) of 33 per cent with combination versus 47 per cent with doxycycline and 48 per cent with azithromycin monotherapy [7].
Management
- Uncomplicated scrub typhus: doxycycline 100 mg twice daily for 7 days. The response is usually dramatic (defervescence within 24 to 48 hours).
- Severe scrub typhus: IV doxycycline plus azithromycin (per INTREST).
- Pregnancy and children under 8: doxycycline is relatively contraindicated, but in life-threatening rickettsial disease the benefit outweighs the dental risk; otherwise use azithromycin. [1]
The exam principle: in a febrile traveller with an eschar, start doxycycline empirically — do not wait for serology, which requires paired acute and convalescent titres and is unhelpful in the acute illness. [1]
Other rickettsial diseases
African tick bite fever (Rickettsia africae, sub-Saharan Africa) often produces multiple eschars (because the vector ticks feed in clusters) and a milder illness. Mediterranean spotted fever (R. conorii, the "tache noire" eschar) occurs around the Mediterranean. All respond to doxycycline. Always examine the whole skin, including scalp, genitals, popliteal fossae and interdigital webs, for an eschar. [1]
Schistosomiasis — Katayama fever and eosinophilia
Schistosomiasis is acquired when cercariae in freshwater (lakes, rivers, streams) penetrate the skin during swimming or wading. The species differ by geography and target organ: S. mansoni (Africa, Caribbean, South America — gut and liver), S. haematobium (Africa and the Middle East — bladder, causing haematuria and bladder cancer), and S. japonicum (East Asia — gut and liver, the most aggressive). The freshwater exposure history is the key — a single swim in Lake Malawi or the Nile is a classic vignette. [1]
Katayama fever (acute schistosomiasis)
Two to eight weeks after exposure, some patients develop Katayama fever — a systemic hypersensitivity reaction to the massive egg deposition, presenting with fever, urticarial rash, dry cough, diarrhoea, and hepatosplenomegaly, with marked eosinophilia. This is an immune-complex phenomenon, analogous to serum sickness. The diagnosis is clinical plus serology (stool and urine microscopy for ova are often negative at this early stage because egg production has not yet begun). [1]
Chronic schistosomiasis
Months to years after infection, chronic disease reflects the organ of egg deposition: periportal (pipestem) fibrosis and portal hypertension (S. mansoni and S. japonicum — the haematemesis of oesophageal varices is a classic late presentation), and bladder cancer and obstructive uropathy (S. haematobium). Neuroschistosomiasis — ectopic egg deposition in the spinal cord causing acute transverse myelitis — is a rare but devastating complication. [1]
Diagnosis
- Serology is the most sensitive test in travellers (a single exposure often produces a detectable antibody response), and is the first-line test in returned travellers.
- Stool microscopy (S. mansoni, S. japonicum) and urine microscopy (S. haematobium) for ova — sensitivity is low in light infections and negative early in Katayama fever.
- Eosinophilia is a supportive marker (see the eosinophilia workup below). [1]
Management
- Praziquantel 20 mg/kg orally twice, 4 hours apart (a single day of treatment) is the standard for S. mansoni and S. haematobium. For S. japonicum, give 60 mg/kg in three divided doses.
- Katayama fever: add corticosteroids (prednisolone) to suppress the hypersensitivity reaction before or alongside praziquantel — treating the worm load too early can worsen the immune reaction. [1]
Leptospirosis — Weil disease and conjunctival suffusion
Leptospirosis is a spirochaete (Leptospira species) acquired through contact with water or soil contaminated by animal urine — rodents, livestock, dogs. Classic exposures are freshwater swimming, farming, sewage work, and flooding. It is common in the tropics (including Queensland and the Pacific) and in adventure travellers. [1]
Clinical presentation — the biphasic course
Leptospirosis has a characteristic biphasic illness: [1]
- Leptospiraemic phase (first week): fever, severe headache (often retro-orbital), myalgia (especially calf — a classic complaint), and conjunctival suffusion — the redness of the conjunctivae without purulent discharge, which is the single most specific bedside sign. A pretibial rash may occur.
- Immune phase (second week): in a minority, the disease progresses to Weil disease — the severe form characterised by the triad of jaundice, AKI, and haemorrhage. The jaundice is primarily from hepatocellular dysfunction (transaminases are only mildly elevated, distinguishing it from viral hepatitis); the AKI is from tubulointerstitial nephritis; the haemorrhage ranges from petechiae to pulmonary haemorrhage (the major cause of death). Myocarditis and rhabdomyolysis also occur. [1]
Diagnosis
IgM ELISA is the usual screening test, and the microscopic agglutination test (MAT) is the gold standard — but antibody rises only in the immune phase, so take both an acute and a convalescent sample two weeks apart to demonstrate seroconversion. PCR on blood (early) or urine (later) is useful in the acute phase. The illness is often under-recognised because the early phase is non-specific. [1]
Management
- Mild disease: doxycycline 100 mg twice daily for 7 days (or amoxicillin).
- Severe (Weil) disease: IV ceftriaxone or benzylpenicillin.
- A Jarisch-Herxheimer reaction (transient fever, rigors, hypotension from released spirochaetal antigens) may complicate the first dose — anticipate it, but do not withhold antibiotics. Supportive care (renal replacement therapy for AKI, ventilation for pulmonary haemorrhage) is central to managing severe disease. [1]
Melioidosis — the "Vietnam time bomb" in northern Australia
Melioidosis is caused by Burkholderia pseudomallei, an environmental Gram-negative bacillus found in soil and surface water in the tropics. In Australia it is endemic in the Top End of the Northern Territory, and also occurs in northern Queensland, Torres Strait Islands and parts of Southeast Asia (Thailand). The Darwin Prospective Melioidosis Study has defined the epidemiology: it is a disease of the wet season, and the major risk factors are diabetes, hazardous alcohol use, chronic kidney disease, chronic lung disease, and immunosuppression [8]. Acquisition is by percutaneous inoculation (skin abrasions), inhalation (during severe weather events like cyclones), and ingestion.
Clinical presentation
Melioidosis is a great mimicker. The spectrum ranges from asymptomatic seroconversion, through a single skin lesion, to: [1]
- Community-acquired pneumonia — often upper lobe, and can be subacute or chronic, mimicking tuberculosis (cavitation is common).
- Bacteraemia with septic shock — the most lethal presentation, especially in diabetics.
- Skin and soft tissue infection, prostatic abscess (a characteristic visceral site), hepatic and splenic abscesses, osteomyelitis, and septic arthritis.
- Latent reactivation — the organism can persist intracellularly for years and reactivate with immunosuppression (the "Vietnam time bomb", named for Vietnam veterans presenting decades after exposure). [1]
Diagnosis
Blood culture is the cornerstone. Also culture throat swabs, sputum, wound swabs and urine. On Ashdown's selective medium, colonies have a characteristic wrinkled, dry, corrugated colonial morphology. The laboratory must be notified of the suspicion, because B. pseudomallei is a hazard group 3 organism and misidentification (as Pseudomonas or Burkholderia cepacia) is a recognised safety issue. Serology (indirect haemagglutination) is useful for exposure history but not for acute diagnosis. [1]
Management — biphasic, prolonged
The single most important teaching point: melioidosis requires two phases of treatment, and omitting the eradication phase causes relapse in 10 to 20 per cent of cases. [1]
- Intensive phase: IV ceftazidime 2 g every 6 hours (or meropenem 1 g every 8 hours) for at least 14 days (longer — at least 4 weeks — for deep-seated infection, osteomyelitis, abscesses, and neurologic disease). Add trimethoprim-sulfamethoxazole for the intensive phase in some regimes.
- Eradication phase: oral trimethoprim-sulfamethoxazole (weight-based, up to 8/40 mg/kg twice daily) for at least 3 months (some use doxycycline, or amoxicillin-clavulanate in pregnancy and children). [1]
Intestinal parasites — giardia, amoeba, and the strongyloides trap
Giardiasis
Giardia lamblia is the most common parasitic cause of traveller's diarrhoea that persists beyond a week. It presents with foul-smelling, fatty, watery diarrhoea, bloating, flatulence, and eructation, often without fever or blood (afebrile, non-bloody, persistent — the "beaver fever" of freshwater exposure). Diagnosis is by stool microscopy for cysts or antigen testing (more sensitive); repeat stool samples increase yield because cyst shedding is intermittent. Treatment is metronidazole 400 mg three times daily for 5 to 7 days (or tinidazole as a single dose), or nitazoxanide. [1]
Amoebiasis — Entamoeba histolytica
E. histolytica causes both intestinal amoebiasis (dysentery — bloody, mucoid diarrhoea, lower abdominal pain) and extraintestinal disease, the most important being the amoebic liver abscess. The amoebic liver abscess is a classic exam case: a single right-lobe abscess, in a traveller or migrant, with fever and right-upper-quadrant pain, negative blood cultures, and a well-appearing patient relative to the size of the abscess. The aspirate is the classic "anchovy paste" — thick, reddish-brown, sterile pus. Serology (E. histolytica antibody) is positive, distinguishing it from pyogenic abscess. Treatment is metronidazole 750 mg three times daily for 7 to 10 days (or tinidazole), followed by a luminal agent (paromomycin or diloxanide furoate) to clear gut cysts. Do not confuse E. histolytica with the non-pathogenic E. dispar (which does not cause disease and does not need treatment). [1]
Strongyloides stercoralis — the hyperinfection trap
Strongyloides is the parasite most likely to kill an immunosuppressed patient, and the one every physician must screen for before starting steroids. Its life cycle is unique among human helminths because it can complete an autoinfection cycle entirely within the host: rhabditiform larvae in the gut develop into infective filariform larvae, which penetrate the intestinal mucosa or perianal skin, migrate to the lungs, and re-establish infection — enabling decades of chronic, low-grade infection. The system runs in equilibrium until the host is immunosuppressed, when the autoinfection cycle accelerates catastrophically into hyperinfection. [1]
Chronic strongyloidiasis is often asymptomatic, or causes intermittent abdominal pain, diarrhoea, and larva currens — a rapidly migrating serpiginous urticarial rash, usually perianal or on the trunk. Eosinophilia is present in the majority (76.9 per cent at diagnosis in a systematic review) [9], but may be absent in hyperinfection — a negative eosinophil count does not exclude it.
Hyperinfection and disseminated disease occur with corticosteroids (the classic trigger), HTLV-1 infection (strongyloides is driven by a Th2 response, which HTLV-1 suppresses — the opposite of the HIV relationship), malignancy, organ transplantation, and other immunosuppression. Critically, HIV is NOT a major risk factor for hyperinfection (because HIV depletes Th17/Th1 pathways, not the Th2/eosinophil axis that controls strongyloides). The presentation is Gram-negative sepsis — because the migrating filariform larvae carry enteric bacteria out of the gut, causing bacteraemia, meningitis, and pneumonia, often polymicrobial. Mortality exceeds 50 per cent. [1]
Diagnosis: serology (ELISA) is the screening test of choice in travellers and pre-immunosuppression screening; stool microscopy is insensitive (single stool catches only about 30 per cent) unless repeated or concentrated. In hyperinfection, larvae are found in stool, sputum and other body fluids in large numbers. [1]
Management:
- Chronic infection: ivermectin 200 micrograms/kg orally, two doses on consecutive days (more effective than albendazole).
- Hyperinfection: ivermectin daily until stool and sputum are negative, often for 2 weeks or more, then a maintenance course. [1]
The non-negotiable rule: any patient who has ever lived in a tropical or subtropical area (including refugees, migrants, and long-term travellers) must be screened for strongyloides with serology and treated before starting corticosteroids, biologics, chemotherapy, or transplantation. This single practice prevents a substantial proportion of fatal hyperinfection cases. [1]
The eosinophilia workup in a returning traveller
Eosinophilia (absolute eosinophil count above 0.5 x 10^9/L, or above 0.4 by some definitions) in a returned traveller is a powerful clue to helminthic infection, and the pattern of exposure plus the degree of eosinophilia drives the workup. The framework: [1]
First, confirm it is real and persistent. Repeat the full blood count. Exclude non-infectious causes: atopy, drug reaction, connective tissue disease, eosinophilic gastrointestinal disease, and malignancy (especially T-cell lymphoma and the hypereosinophilic syndrome). A drug history is essential. [1]
Second, match the helminth to the exposure. [1]
| Exposure / feature | Likely helminth | Diagnostic test |
|---|---|---|
| Freshwater exposure | Schistosoma species | Serology; stool/urine ova |
| Tropical residence, larva currens | Strongyloides stercoralis | Serology; stool concentration |
| Barefoot exposure (soil) | Hookworm (Necator, Ancylostoma) | Stool ova |
| Skin contact with dog/cat faeces soil | Cutaneous larva migrans (dog/cat hookworm) | Clinical |
| Tropical residence | Filariasis (lymphatic, loa, onchocerca) | Serology; specific blood/skin smears |
| Undercooked meat | Trichinellosis | Serology; muscle biopsy |
| Dog/cat exposure | Toxocariasis (visceral larva migrans) | Serology |
Third, treat the cause. Praziquantel for schistosomiasis, ivermectin for strongyloides, albendazole or mebendazole for hookworm and cutaneous larva migrans, diethylcarbamazine or ivermectin (depending on species) for filariasis. [1]
The exam trap: eosinophilia is not a feature of malaria, dengue, typhoid, leptospirosis or rickettsial disease — if you see eosinophilia in a febrile traveller, think helminth, and specifically schistosomiasis or strongyloides. Conversely, absence of eosinophilia does not exclude strongyloides hyperinfection. [1]
The integrated workup of the febrile returning traveller
The minimum investigation set, sent at first contact for any febrile traveller, is: [1]
- Thick and thin blood films for malaria (the rule-out-malaria-first principle) — repeat every 12 to 24 hours for at least three sets if negative.
- Malaria RDT if microscopy is delayed.
- Full blood count and differential — look for anaemia and thrombocytopenia (malaria, dengue), leucopenia (dengue, typhoid), eosinophilia (helminths), and atypical lymphocytes (viral).
- Urea and electrolytes, liver function tests — renal failure and jaundice indicate severe disease (severe malaria, leptospirosis, typhoid).
- Blood cultures — at least two sets (typhoid, melioidosis, leptospirosis).
- C-reactive protein.
- Dengue NS1 antigen and serology if in the right window.
- Urinalysis.
- Chest X-ray — pneumonia (melioidosis, scrub typhus), ARDS.
- Targeted tests based on exposure: schistosomiasis and strongyloides serology, leptospirosis serology (acute and convalescent), rickettsial serology, amoebic serology and liver imaging if an abscess is suspected. [1]
The viral haemorrhagic fever precaution: if the traveller has fever within 21 days of returning from an Ebola, Lassa or Marburg endemic area, isolate immediately in a negative-pressure room, notify public health, and use full PPE before any investigation including blood sampling. Do not send routine bloods to the standard laboratory without consulting the infectious diseases and public health teams first. [1]
High-yield exam discriminators
- Rule out malaria first — any febrile traveller from an endemic area gets a thick and thin film immediately; a single negative film never excludes malaria, repeat for three sets.
- Severe falciparum malaria gets IV artesunate 2.4 mg/kg — not quinine, not oral therapy. SEAQUAMAT and AQUAMAT proved the mortality benefit. [1]3. Monitor haemoglobin for four weeks after artesunate for post-artesunate delayed haemolysis.
- Dengue: paracetamol only, never aspirin or NSAIDs — thrombocytopenia plus platelet dysfunction is the bleeding risk.
- Dengue critical phase is at defervescence — the settling of fever is not recovery; it is the moment of maximum plasma-leakage risk. Watch the haematocrit and pulse pressure.
- Typhoid: blood culture in week one; ceftriaxone or azithromycin — fluoroquinolones are unreliable due to resistance.
- Typhoid perforation is a surgical emergency in week three — sudden abdominal pain with peritonism.
- Eschar plus fever: doxycycline empirically — do not wait for serology.
- Severe scrub typhus: combination IV doxycycline plus azithromycin (INTREST trial).
- Schistosomiasis: praziquantel; Katayama fever: add corticosteroids.
- Strongyloides: screen with serology and treat with ivermectin before any immunosuppression — hyperinfection is fatal.
- Melioidosis: ceftazidime then 3 months of oral eradication — omitting the eradication phase causes relapse.
- Eosinophilia in a traveller means helminth — schistosomiasis and strongyloides first; not malaria, dengue, typhoid or leptospirosis. [1]
Regional guideline deltas
| Aspect | ANZ (Therapeutic Guidelines / ASID) | UK (NICE / PHE / BIA) | US (CDC Yellow Book / IDSA) |
|---|---|---|---|
| Malaria treatment | IV artesunate for severe; ACT for uncomplicated | As per WHO; IV artesunate via named-patient | CDC supplies IV artesunate; ACT for uncomplicated |
| Dengue classification | WHO 2009 (warning signs / severe) | WHO 2009 | WHO 2009 |
| Typhoid empiric | Azithromycin or ceftriaxone (high fluoroquinolone resistance from South Asia) | Ceftriaxone then de-escalate | Azithromycin or ceftriaxone |
| Melioidosis | Endemic in the Top End; ceftazidime then 3-month TMP-SMX | Imported; treat per sensitivities | Rare; CDC guidance |
| Scrub typhus | Endemic in northern Australia and Torres Strait; doxycycline | Imported from Asia | Imported; doxycycline |
In the ANZ setting, Therapeutic Guidelines (eTG) and ASID (Australasian Society for Infectious Diseases) publish the local guidance; the Darwin Prospective Melioidosis Study underpins the melioidosis recommendations. The CDC Yellow Book is the global travel-medicine reference. WHO provides the malaria and dengue treatment frameworks. [1]
Pre-travel advice — the consultation that prevents disease
The pre-travel consultation reduces risk through four mechanisms: vaccination, chemoprophylaxis, behavioural advice, and post-exposure planning. [1]
Malaria chemoprophylaxis — the ABCD. Awareness of risk; Bite avoidance (DEET-based insect repellent, permethrin-treated clothing, bed nets — remembering that Aedes mosquitoes bite by day and Anopheles by night); Chemoprophylaxis; and Diagnosis (prompt medical attention if febrile). The three standard agents: [1]
| Agent | Dosing | Key features |
|---|---|---|
| Atovaquone-proguanil | Daily, start 1 to 2 days before travel, continue 7 days after return | Best tolerated, expensive, short post-travel course |
| Doxycycline | Daily, start 1 to 2 days before, continue 4 weeks after return | Cheap, photosensitivity, contraindicated in pregnancy and under 8 years |
| Mefloquine | Weekly, start 1 to 2 weeks before, continue 4 weeks after return | Convenient weekly dosing, neuropsychiatric side effects (anxiety, vivid dreams, psychosis) |
Travel vaccines. Routinely recommended: hepatitis A (very common food-borne risk), typhoid (injectable Vi polysaccharide or oral live Ty21a), yellow fever (live attenuated, required for entry to some countries in sub-Saharan Africa and South America — give at least 10 days before travel; contraindicated in pregnancy, infants under 9 months, and immunosuppression), Japanese encephalitis (for rural Asia travel of more than a month), rabies (pre-exposure for high-risk travellers), and meningococcal ACWY (required for the Hajj, recommended for the sub-Saharan meningitis belt). Typhoid conjugate vaccines have improved immunogenicity in young children and are increasingly used in endemic countries [6]. Give vaccines ideally 4 to 6 weeks before travel — live vaccines must be given on the same day or four weeks apart, and immunity takes time to develop.
Behavioural advice. Food and water safety ("boil it, cook it, peel it, or forget it"); avoid freshwater exposure in endemic areas (schistosomiasis, leptospirosis) — locals saying the water is safe is not reassurance; sun protection; safe sex; and insect avoidance. [1]
Traveller's diarrhoea. Rehydration first; loperamide for symptomatic relief (not in dysentery or fever); antibiotic self-treatment with azithromycin (preferred over fluoroquinolones due to resistance, especially for Southeast Asia); seek medical attention for fever, bloody stool, or persistence beyond 14 days (when parasitic causes such as giardia become likely). [1]
The post-travel screen. For asymptomatic long-term travellers to the tropics, consider screening for tuberculosis (QuantiFERON or tuberculin), schistosomiasis and strongyloides serology, stool microscopy, HIV, and viral hepatitis — and screen for sexually transmitted infections based on exposure history. [1]
Communication and shared decision-making
The febrile traveller is often anxious, has often self-treated or taken incomplete prophylaxis, and may minimise exposures. The physician must communicate urgency without alarm: [1]
- Ruling out malaria: "I need to exclude malaria today because, although uncommon, it can become life-threatening within 24 hours. I am repeating the blood test because a single negative result does not fully exclude it."
- Dengue warning signs: "Your fever will settle over the next day or two, but that is exactly when you are at risk of the leaky-blood-vessel complication. Return immediately if you have abdominal pain, persistent vomiting, bleeding, drowsiness, or you cannot keep fluids down. Avoid ibuprofen and aspirin; paracetamol only."
- Strongyloides before immunosuppression: "I need to test you for a worm called strongyloides because the medication I am about to start could trigger a dangerous reaction if you carry it — and many people who grew up in tropical areas do carry it without knowing. The test is a simple blood test, and the treatment is two tablets."
- Public health and contact tracing: typhoid, dengue and viral haemorrhagic fevers are notifiable. Explain the legal requirement, the purpose of protecting others, and the supportive role of the public health team. [1]
Summary: the tropical medicine consultation in one paragraph
Take a precise travel and exposure history and use the incubation period to narrow the differential. Rule out malaria first — thick and thin films, repeated for three sets, every 12 to 24 hours. Treat severe falciparum malaria with IV artesunate and watch for delayed haemolysis; treat uncomplicated falciparum with oral ACT and non-falciparum with chloroquine plus primaquine (after checking G6PD). Manage dengue with paracetamol only, daily platelet and haematocrit monitoring, and cautious isotonic fluid in the critical phase — never aspirin or NSAIDs. Diagnose typhoid by blood culture in week one and treat with ceftriaxone or azithromycin; watch for perforation in week three. Treat rickettsial disease empirically with doxycycline when you see an eschar; treat severe scrub typhus with combination IV doxycycline plus azithromycin. Treat schistosomiasis with praziquantel (plus corticosteroids for Katayama fever), leptospirosis with ceftriaxone, melioidosis with ceftazidime then a three-month oral eradication phase, and strongyloides with ivermectin — always before immunosuppression. Work up eosinophilia by matching the helminth to the exposure. Give pre-travel advice that combines vaccination, chemoprophylaxis, behavioural change, and a plan for illness abroad. Isolate any suspected viral haemorrhagic fever immediately and call for help. [1]
References
- [1]Wilson ME, Weld LH, Boggild A, et al. Fever in returned travelers: results from the GeoSentinel Surveillance Network Clin Infect Dis, 2007.PMID 17516399
- [2]Dondorp A, Nosten F, Stepniewska K, Day N, White N Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial Lancet, 2005.PMID 16125588
- [3]Dondorp AM, Fanello CI, Hendriksen IC, et al. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial Lancet, 2010.PMID 21062666
- [4]Jaureguiberry S, Ndour PA, Roussel C, et al. Postartesunate delayed hemolysis is a predictable event related to the lifesaving effect of artemisinins Blood, 2014.PMID 24859359
- [5]Simmons CP, Farrar JJ, Nguyen VV, Wills B. Dengue N Engl J Med, 2012.PMID 22494122
- [6]GBD 2017 Typhoid and Paratyphoid Collaborators The global burden of typhoid and paratyphoid fevers: a systematic analysis for the Global Burden of Disease Study 2017 Lancet Infect Dis, 2019.PMID 30792131
- [7]Varghese GM, Dayanand D, Gunasekaran K, et al. Intravenous Doxycycline, Azithromycin, or Both for Severe Scrub Typhus N Engl J Med, 2023.PMID 36856615
- [8]Currie BJ Melioidosis: evolving concepts in epidemiology, pathogenesis, and treatment Semin Respir Crit Care Med, 2015.PMID 25643275
- [9]Buonfrate D, Fittipaldo A, Vlieghe E, Bottieau E Clinical and laboratory features of Strongyloides stercoralis infection at diagnosis and after treatment: a systematic review and meta-analysis Clin Microbiol Infect, 2021.PMID 34325063