Phys · infectious
Tuberculosis
Also known as TB · pulmonary tuberculosis · extrapulmonary tuberculosis · latent tuberculosis infection · LTBI · reactivation tuberculosis · post-primary tuberculosis · tuberculous meningitis · Pott disease · scrofula · miliary tuberculosis · MDR-TB · pre-XDR-TB · XDR-TB · RIPE therapy
Consultant-physician-depth guide to tuberculosis as an infectious disease — latent versus active infection and who to screen, the diagnostic hierarchy from Xpert Ultra to culture, first-line RIPE therapy with drug-level toxicities, MDR/pre-XDR/XDR definitions and all-oral bedaquiline regimens, TB-HIV co-management and IRIS, and the public-health obligations of notification, contact tracing and BCG — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Tuberculosis
The answer first
Tuberculosis is three clinical problems wearing one name, and almost every exam question and every hard ward decision is really asking which of the three you are dealing with [3]:
- Infection or disease? A person with immune sensitisation to M. tuberculosis — a positive IGRA or tuberculin skin test — who has no symptoms, no radiological activity and no detectable organisms is latently infected: well, non-infectious, and a candidate for preventive therapy. The same person with a chronic cough, apical infiltrates and bacilli in sputum has active disease: infectious, notifiable, and needing four drugs. No blood test can tell these two states apart — only clinical assessment plus microbiology can [3] [19].
- Drug-susceptible or resistant? Every confirmed case starts with a molecular test that simultaneously detects M. tuberculosis and rifampicin resistance, because the regimen chosen on day one determines whether you cure the patient or amplify resistance [6] [1].
- Individual patient or public-health event? Active pulmonary TB obliges you to notify, isolate while infectious, and trace contacts. The consultation is not finished when the prescription is written [1].
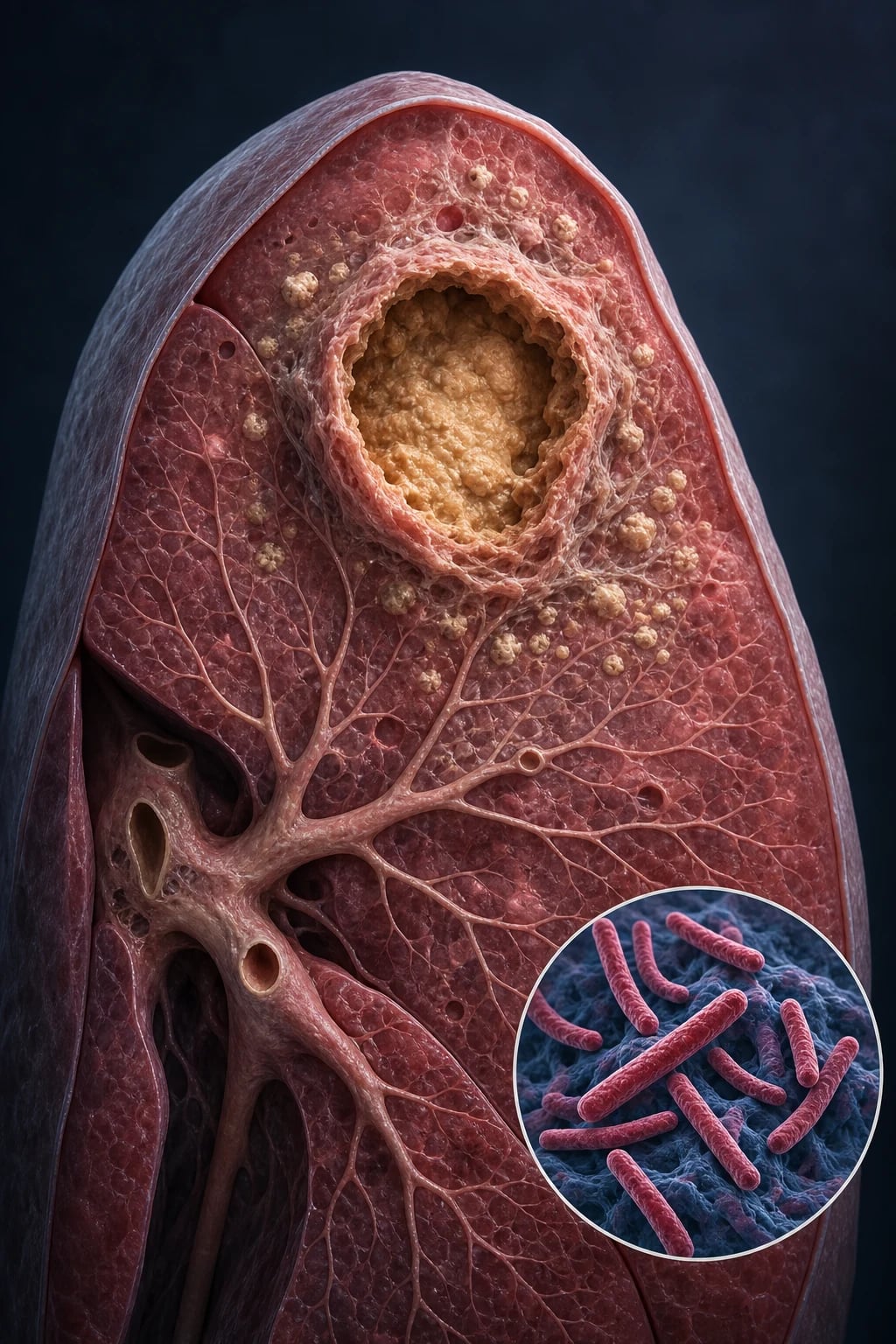
Transmission and containment — the two-minute pathophysiology
M. tuberculosis travels in airborne droplet nuclei generated by coughing, singing and speaking from a person with pulmonary or laryngeal disease; the bacilli reach the terminal alveoli, are engulfed by alveolar macrophages, and either are killed, proliferate into primary disease, or are walled into granulomas where they persist in a metabolically dormant state for decades [3]. The granuloma is therefore both the success and the failure of host immunity — it contains the bacillus, and it stores it. Reactivation happens when the containment cell-mediated response weakens: HIV, TNF blockade, transplantation, high-dose steroids, silicosis, end-stage kidney disease, diabetes and simply age [3] [20].
Between a quarter and a third of humanity carries latent infection, roughly 9–10 million people develop active disease each year, and untreated smear-positive disease kills about half its victims — which is why TB, a curable disease, remains among the leading infectious causes of death worldwide [3].
Classification: the spectrum from dormant focus to disseminated disease
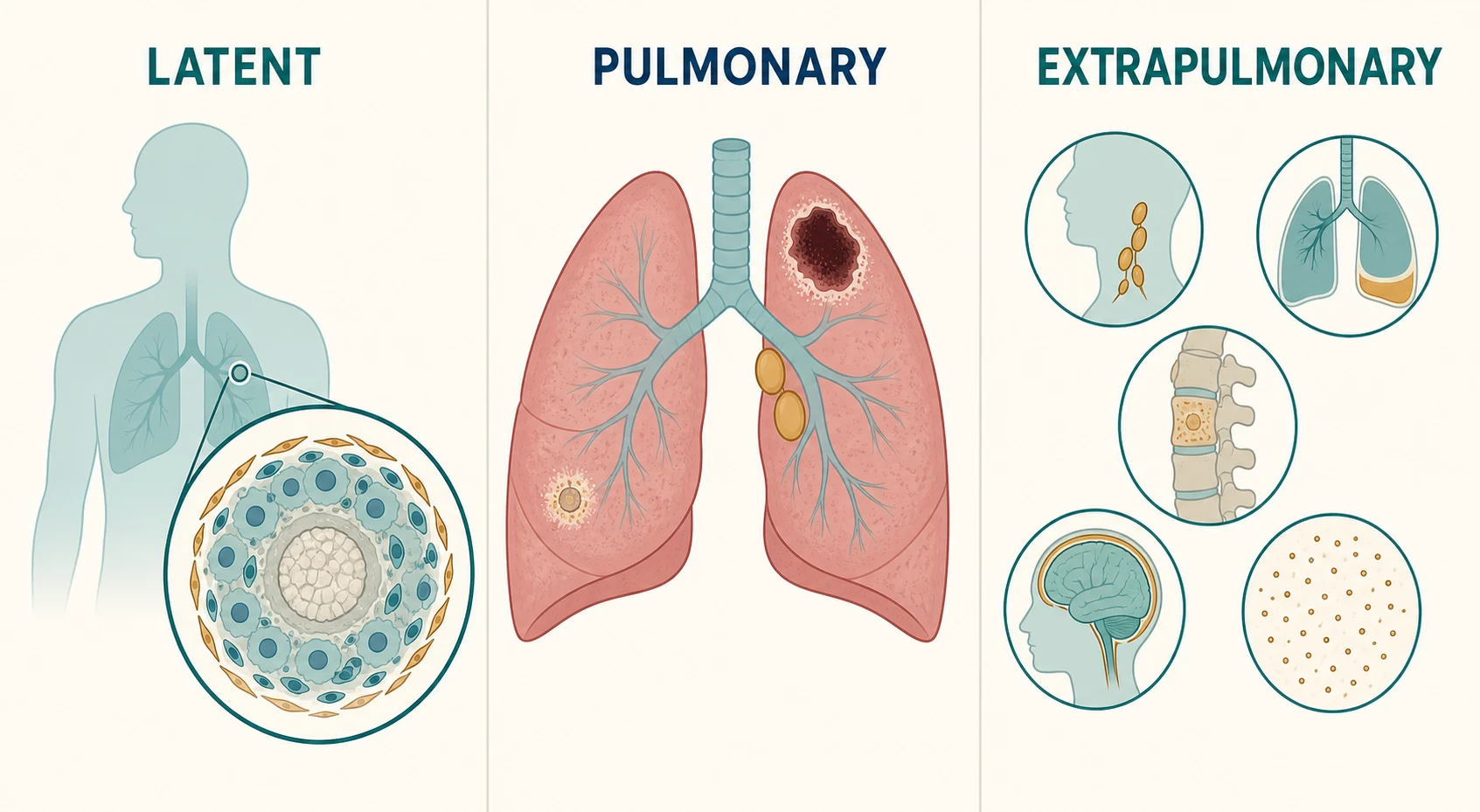
About 5–10 per cent of latently infected, immunocompetent adults will develop active disease over a lifetime, with half of that risk concentrated in the first two years after infection. Everything else is containment holding [3].
| State | Definition | Infectious? | What it means clinically |
|---|---|---|---|
| Latent TB infection (LTBI) | Immune sensitisation (positive IGRA or TST) with no clinical, radiological or microbiological evidence of disease | No | Well patient; treat to prevent reactivation, especially before immunosuppression [3] |
| Primary pulmonary TB | Disease at first infection — mid-zone infiltrates, hilar or mediastinal lymphadenopathy, sometimes pleural effusion | Yes, if respiratory secretions carry bacilli | The childhood pattern; also seen in recently infected adults from low-incidence settings |
| Reactivation (post-primary) TB | Dormant bacilli escape containment — apical cavitation and upper-lobe fibrosis | Yes — the classic infectious form | The adult pattern; driven by waning cell-mediated immunity [3] |
| Extrapulmonary TB | Disease at any non-lung site — nodes, pleura, CNS, bone, pericardium, abdomen, genitourinary | Not usually (unless concurrent pulmonary disease) | Needs tissue or site-fluid diagnosis; longer therapy for CNS and skeletal disease [1] |
| Miliary TB | Lymphohaematogenous dissemination — millet-seed nodules through lung and organs | Variable | A disease of the immunosuppressed and the very young; often smear-negative and cryptic [2] |
Reactivation risk is not evenly distributed. Untreated HIV is the strongest single driver — up to about 10 per cent per year — followed by recent infection, fibrotic radiographic scars of untreated prior disease, silicosis, transplantation, chronic kidney disease, diabetes, and the iatrogenic immunosuppression physicians control [3] [20].
Latent TB: who to screen, with what, and how to treat
The entire point of latent-TB care is to find the person whose granulomas are about to fail — before they fail [3].
Who to screen. Test people whose future risk justifies preventive therapy: close contacts of infectious cases; migrants and refugees from high-incidence countries, particularly in their first years after arrival; people living with HIV; patients about to start anti-TNF agents, other biologics, high-dose corticosteroids, chemotherapy or transplantation; and people with silicosis, end-stage kidney disease or diabetes where risk accumulates [3] [20].
| Test | What it measures | Strengths | Limitations |
|---|---|---|---|
| IGRA (QuantiFERON-TB Gold Plus, T-SPOT.TB) | T-cell interferon-gamma release to TB-specific antigens (ESAT-6, CFP-10) | No BCG cross-reactivity; single visit; not boosted by repeat testing | Cost and laboratory dependence; indeterminate results in immunosuppression; cannot distinguish latent from active [19] |
| TST (Mantoux) | Delayed-type hypersensitivity to purified protein derivative | Cheap, no laboratory, decades of experience | BCG vaccination can false-positive it; two visits; reader variability; false-negative in severe immunosuppression and overwhelming TB [19] |
Treating latent infection. Four regimens, and the modern direction of travel is short and rifamycin-based [4]:
| Regimen | Duration | Evidence | Practical notes |
|---|---|---|---|
| Rifampicin daily (4R) | 4 months | Non-inferior to 9 months of isoniazid, with better completion and less hepatotoxicity [4] | First choice in most current guidelines |
| Isoniazid + rifapentine weekly (3HP) | 3 months (12 doses) | Non-inferior to 9H with higher completion [5] | Weekly dosing suits observed therapy; flu-like systemic reactions occur |
| Isoniazid + rifampicin daily (3HR) | 3 months | Equivalent efficacy in guideline-concordant trials | Useful where rifapentine is unavailable [3] |
| Isoniazid daily (6H or 9H) | 6–9 months | The historic standard | Reserved for rifamycin contraindication or interactions; add pyridoxine for at-risk patients [3] |
Rifamycin interactions apply even in preventive therapy — reconcile the contraceptive pill, anticoagulants, antiretrovirals and transplant drugs before committing to a rifamycin regimen [1].
Pulmonary TB: the active disease you must not miss
The pulmonary presentation is deliberately unspectacular: a cough that has simply lasted too long. The classic tetrad is subacute cough beyond two to three weeks, fever with drenching night sweats, weight loss, and haemoptysis — read against the epidemiological frame: migration from an endemic country, a known contact, incarceration, homelessness, immunosuppression [2]. The chest X-ray of reactivation disease shows upper-lobe and apical infiltrates, cavitation, volume loss and fibrosis; primary disease shows mid-zone consolidation with hilar nodes; advanced HIV flattens the pattern toward normal films and mid-zone disease [2].
Examination may show cachexia, apical crackles and bronchial breathing, but a normal chest examination never excludes apical disease. The detailed respiratory examination technique and the differential of apical shadowing belong to the companion respiratory-angle tuberculosis topic — here the emphasis is the infectious-disease decision chain that follows suspicion [2].
Extrapulmonary TB: one disease, many disguises
Extrapulmonary disease accounts for roughly a fifth of TB notifications in low-incidence countries, and a higher share among migrants and people with HIV. The sites you must be able to present, investigate and treat [2]:
| Site | Signature presentation | Diagnosis | Management nuance |
|---|---|---|---|
| Lymph node (scrofula) | Painless matted cervical nodes, sometimes with sinus formation — the commonest extrapulmonary form | Fine-needle aspiration or excision biopsy for smear, NAAT, culture AND histology (caseating granulomas) | Nodes can paradoxically enlarge on therapy; aspiration is preferred over incision to avoid chronic sinuses [2] |
| Pleural | Subacute unilateral lymphocytic exudate, often in young adults | Pleural fluid (lymphocytic, high adenosine deaminase); pleural biopsy has the highest yield | An immunological reaction to very few bacilli — fluid smear is usually negative [2] |
| CNS — tuberculous meningitis | Subacute meningitis: headache and low-grade fever, then cranial neuropathies, confusion, falling conscious level | Large-volume CSF: lymphocytic pleocytosis, high protein, low glucose; NAAT on CSF; imaging for hydrocephalus and basal exudates | The TB emergency — treat empirically on suspicion and add dexamethasone; delay kills [9] |
| Skeletal (Pott disease) | Insidious back pain with gibbus; disc-space destruction and paravertebral abscess | MRI; CT-guided biopsy for tissue | Prolonged therapy (9–12 months); surgery for instability or cord compression [1] |
| Pericardial | Effusion, tamponade, later constriction | Echocardiography; pericardial fluid or biopsy; empiric treatment in endemic settings | Steroids selective, not routine — see below [10] |
| Miliary / disseminated | Fever, wasting, hepatosplenomegaly, choroidal tubercles; millet-seed CXR pattern | Miliary pattern on CXR or CT; culture any accessible site; often smear-negative | Look hard for CNS involvement; treat as CNS disease if present [2] |
The diagnostic rule for every site: get tissue or site fluid, and split it for mycobacterial culture as well as histology — histology shows caseating granulomas, but only culture yields the organism and its susceptibility profile [2].
Diagnosis: smear, NAAT, culture — three tests, three purposes
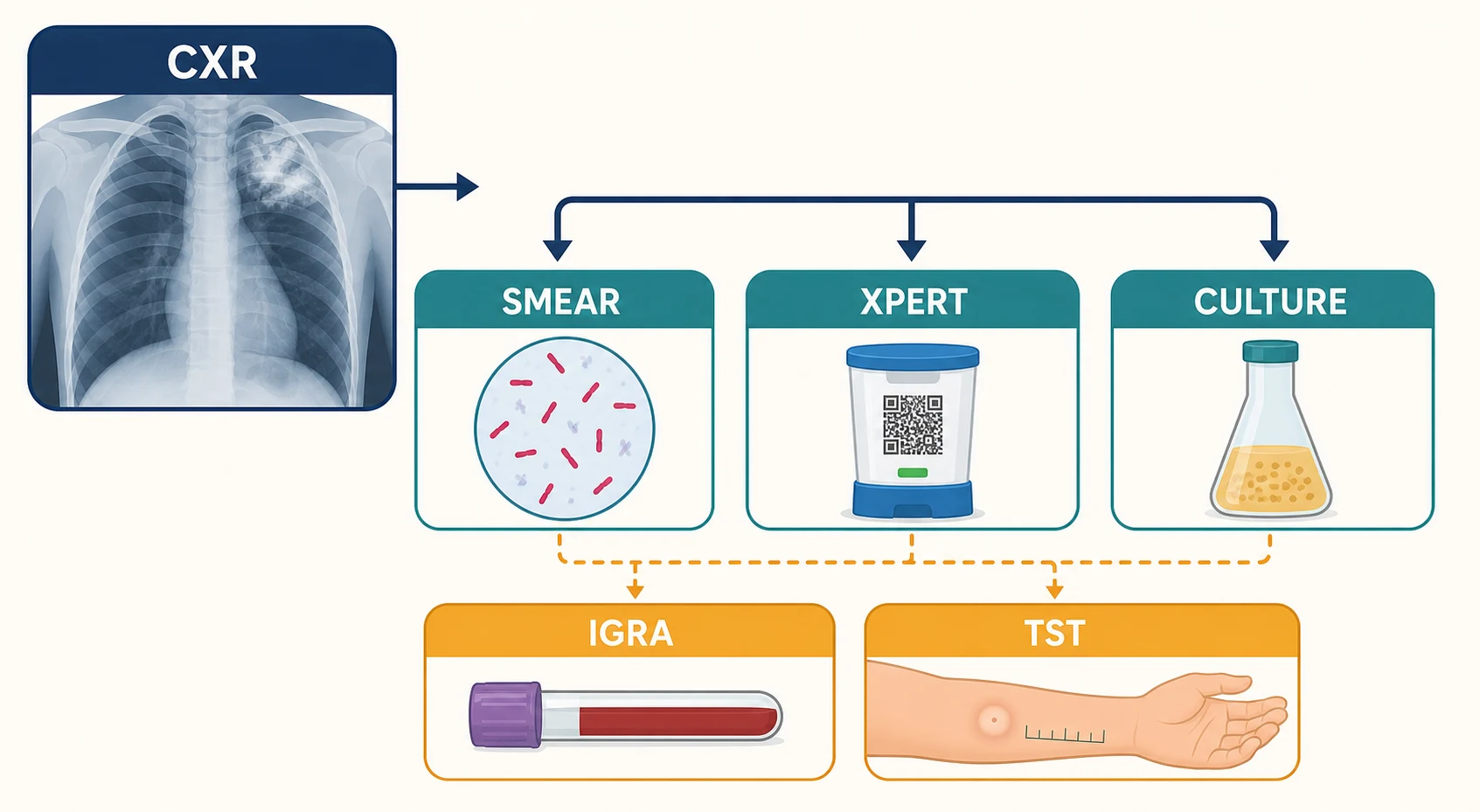
Suspected pulmonary TB triggers a fixed triad on sputum — expectorated, or induced with hypertonic saline when the patient cannot produce it — and the diagnostic guideline is explicit: at least one respiratory specimen should undergo nucleic acid amplification testing, and every patient should have culture, because only culture-backed phenotypic testing defines full drug susceptibility [2]. When sputum cannot be obtained and suspicion is high, bronchoscopy with washings or lavage is the next step — post-bronchoscopy sputum is a bonus sample worth collecting [2].
| Test | Turnaround | What it gives you | What it misses |
|---|---|---|---|
| AFB smear (auramine or Ziehl–Neelsen) | Hours | Speed and infectiousness — smear-positive patients carry the heaviest bacillary load | Sensitivity: misses around half of culture-positive pulmonary cases; cannot separate TB from non-tuberculous mycobacteria [2] |
| NAAT — Xpert MTB/RIF and Xpert Ultra | Hours | Simultaneous detection of M. tuberculosis and rifampicin resistance (rpoB) — the pivotal first test [6] | Ultra 'trace' calls can reflect dead bacilli in previously treated patients; rifampicin-resistance calls in low-prevalence settings still warrant confirmation [7] |
| Mycobacterial culture (liquid, then solid) | 1–6 weeks | The gold standard — confirms viability, species, and full phenotypic drug susceptibility | Slow; never a reason to withhold treatment from a high-probability patient [2] |
Xpert MTB/RIF transformed diagnosis in 2010 by delivering near-complete detection in smear-positive disease — and about three quarters of smear-negative cases on a single test — plus a rifampicin-resistance answer in one cartridge run [6]. The Ultra generation added sensitivity exactly where the original was weakest — smear-negative, HIV-associated, childhood and extrapulmonary disease — at a small cost in specificity among previously treated patients, where it can detect residual DNA from dead bacilli [7]. Molecular resistance results should still be backed by phenotypic susceptibility testing, and genomic sequencing is increasingly the reference method for the full resistance profile [2].
Urine lipoarabinomannan (LF-LAM) earns its place in one niche: hospitalised patients with advanced HIV. A point-of-care urine LAM strategy reduced mortality in a multicentre randomised trial of HIV-positive inpatients, and it is recommended for seriously ill inpatients with HIV and for those with CD4 counts below about 100 cells/µL — precisely the group whose sputum is hardest to obtain and whose smears are most often negative [8].
For tuberculous meningitis the same logic applies with the stakes raised: send a large CSF volume for NAAT and culture, image the brain for hydrocephalus, and never let a negative early result stop empiric therapy in a compatible syndrome — yield is imperfect and delay is lethal [9].
First-line therapy: 2HRZE then 4HR — and why it is built that way
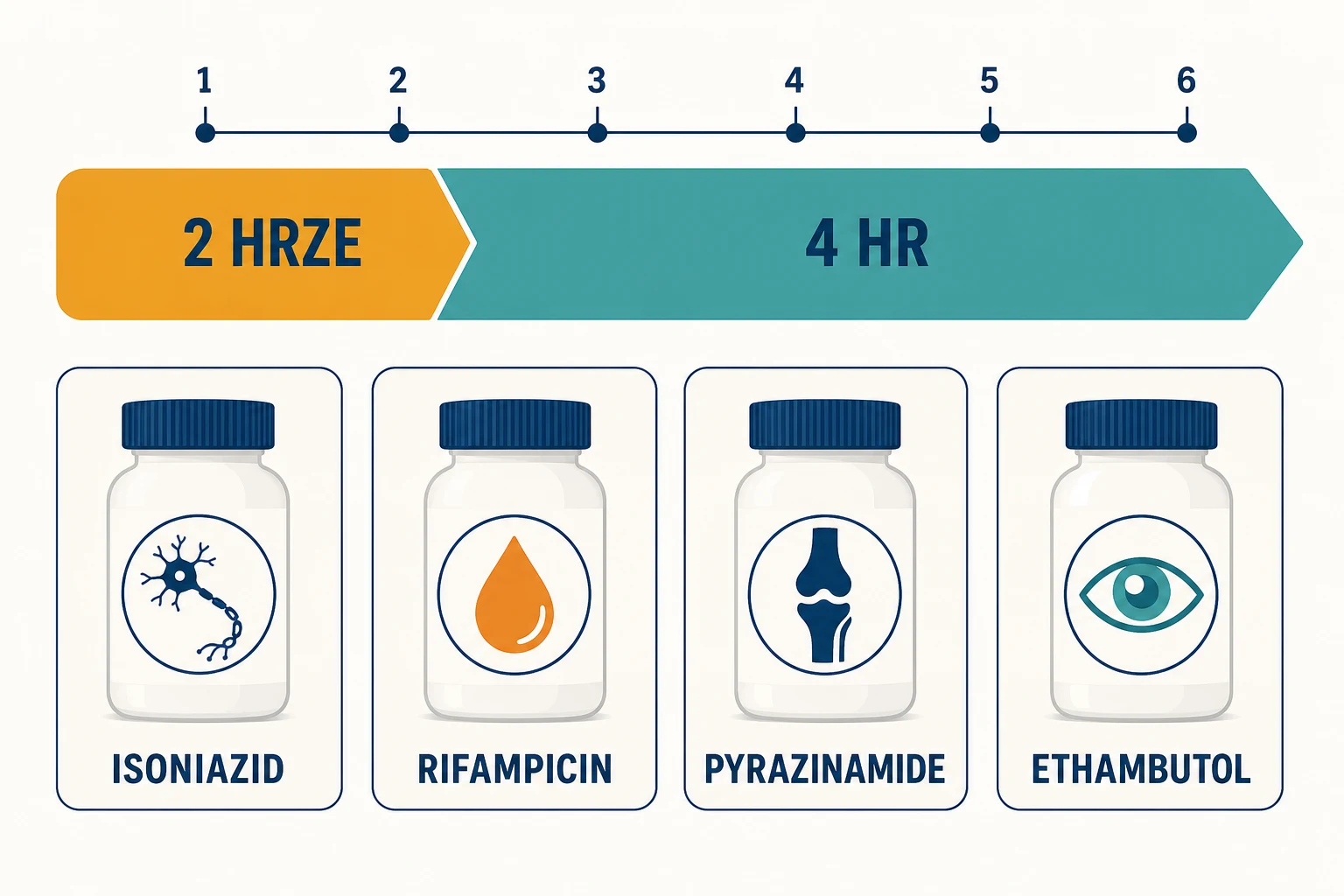
The standard regimen is an engineering solution to a microbiological problem. Within a lesion there are rapidly dividing bacilli (killed by isoniazid), semi-dormant persisters in acidic caseous foci (killed by pyrazinamide) and slowly metabolising bacilli (sterilised by rifampicin). Spontaneous resistance mutations to any single drug exist in every large bacillary population, so monotherapy selects resistance within weeks — four drugs in the intensive phase prevent selection, and two drugs for four further months sterilise the persisters [1].
| Drug | Daily dose | Mechanism | Signature toxicities and monitoring |
|---|---|---|---|
| Isoniazid (H) | 5 mg/kg (maximum 300 mg) | Inhibits mycolic acid synthesis (InhA) | Hepatitis; peripheral neuropathy — give pyridoxine 10 mg daily to at-risk patients (pregnancy, diabetes, CKD, HIV, malnutrition, alcohol use) [1] |
| Rifampicin (R) | 10 mg/kg (maximum 600 mg) | Inhibits DNA-dependent RNA polymerase | Potent CYP3A4 and P-glycoprotein induction — reconcile every interacting drug; orange urine, tears and sweat (warn patients); hepatitis; thrombocytopenia [1] |
| Pyrazinamide (Z) | 25 mg/kg | Sterilises persisters in acidic foci | The most hepatotoxic of the four; hyperuricaemia with arthralgia and gout flares [1] |
| Ethambutol (E) | 15 mg/kg | Inhibits arabinosyl transferase — cell-wall arabinogalactan | Optic neuritis, dose-related; red-green colour blindness precedes acuity loss; baseline testing, then monthly monitoring when renal impairment, longer courses, diabetes or higher doses raise risk [1] |
The architecture of first-line therapy
A 4-month regimen of rifapentine with moxifloxacin was non-inferior to standard 6-month therapy in the Study 31 trial and is now a legitimate option for drug-susceptible pulmonary TB in eligible patients — know the trial name and the concept even where local uptake is still catching up [18]. Two extensions matter at the other end: extend the continuation phase to seven months (nine total) when cavitation coexists with a positive culture at two months, and prolong therapy for CNS and skeletal disease [1].
Monitoring a patient through six months of therapy
Baseline
LFTs, bilirubin, creatinine, platelets; HIV, hepatitis B and C serology; visual acuity and Ishihara colour testing; weight for dosing
Monthly clinical review
Symptoms, adherence, adverse effects; ask specifically about visual change on ethambutol and neuropathic symptoms on isoniazid
Targeted bloods
LFTs only if baseline abnormal, symptoms, or risk factors — routine monthly biochemistry is not required for low-risk patients
Sputum at 2 months
Smear and culture at the end of the intensive phase; a positive culture at two months flags relapse risk and prompts review of adherence and susceptibility
End of treatment
Clinical and radiological response; document completion — no routine test-of-cure culture in a well patient
Adherence is a treatment component, not a personality assessment. Six months is a long course, and the support package matters as much as the prescription: directly observed or video-observed therapy where indicated, a named case manager through the TB service, reminder systems, and honest management of adverse effects before they become reasons to stop. The continuation phase is where adherence quietly fails — the two-month sputum result is often where you find out [1].
Drug-resistant TB: definitions first, then the all-oral revolution
Suspect resistance before you can prove it: prior TB treatment (especially interrupted or relapsed), a known resistant source case, migration from a high-MDR-incidence region, and failure of smear or culture to convert by two months. The Xpert rifampicin-resistance call is usually your first warning, and it must change practice the same day — do not start or continue standard RIPE while you confirm; refer to the MDR service [1] [6].
Treatment of rifampicin-resistant TB has been rebuilt around bedaquiline (an ATP synthase inhibitor), pretomanid (a nitroimidazole) and linezolid, replacing the old 18–20-month injectable-containing regimens [14]:
| Evidence base | Regimen | Population | Headline result |
|---|---|---|---|
| Nix-TB (2020) | BPaL — bedaquiline, pretomanid, linezolid, 6 months | Highly drug-resistant disease (XDR, or treatment-intolerant/non-responsive MDR) | About 90 per cent favourable outcome — at the cost of heavy linezolid toxicity at 1200 mg daily [14] |
| ZeNix (2022) | BPaL with linezolid dose and duration ranging | As Nix-TB | Linezolid 600 mg daily for 26 weeks preserved efficacy with less myelosuppression and neuropathy [15] |
| TB-PRACTECAL (2022) | BPaLM — BPaL plus moxifloxacin, 24 weeks | Rifampicin-resistant TB broadly | Superior to standard care (about 89 versus 52 per cent favourable) with fewer severe adverse events — the basis of the WHO 6-month recommendation [16] |
| STREAM (2019) | 9–11-month standardised regimen | MDR-TB without second-line resistance | Non-inferior to the long conventional regimen — still an option where bedaquiline or pretomanid access is limited [17] |
At consultant level you are not expected to prescribe these regimens unsupervised — MDR-TB belongs to specialist units — but you are expected to define MDR, pre-XDR and XDR precisely, name BPaLM and BPaL with their trials, and know the signature toxicities: bedaquiline and moxifloxacin prolong the QT interval; linezolid causes myelosuppression, peripheral neuropathy and optic neuropathy; pretomanid is hepatotoxic [15] [16].
TB and HIV: two infections, one calendar
HIV is the strongest single reactivation risk, and TB remains a leading killer of people with advanced HIV — the co-infected patient is where timing decisions carry mortality [3].
When to start ART. The evidence is unusually clear. In SAPiT, integrating ART into TB therapy rather than waiting for its completion substantially reduced mortality, and CAMELIA showed that in profoundly immunosuppressed patients (median CD4 around 25 cells/µL) starting ART at two weeks rather than eight weeks improved survival [11] [12]. The working rule: CD4 below 50 — start ART within two weeks of starting TB therapy; CD4 50 or above — by eight weeks. The one exception is tuberculous meningitis, where immediate ART in a randomised trial produced more severe adverse events without survival benefit — defer ART to around eight weeks and give corticosteroids [22] [9].
Which regimen. Rifampicin's enzyme induction collides with boosted protease inhibitors and cobicistat — use rifabutin, a weaker inducer, when a protease-inhibitor regimen must continue, or build ART around an integrase inhibitor with adjusted dosing; efavirenz-based ART was the historical default precisely because it tolerates rifampicin [1].
IRIS. Paradoxical TB-IRIS — fever, enlarging nodes and worsening infiltrates days to weeks after ART starts in a patient who was improving on TB therapy — is a diagnosis of exclusion: adherence, drug resistance and other opportunistic infections must be ruled out first. Most cases are managed by continuing both therapies, and a randomised trial supports prednisone for moderate-to-severe paradoxical TB-IRIS [13].
Adjunctive corticosteroids: proven in two sites, tempting everywhere
Tuberculous meningitis: dexamethasone, tapered over about six to eight weeks, reduced death in a landmark randomised trial of adolescents and adults and is standard of care alongside antituberculous therapy — start it with the antibiotics rather than waiting for microbiological confirmation [9].
Tuberculous pericarditis: the IMPI trial gives the nuanced answer examiners want — prednisolone did not significantly reduce the composite of death, tamponade or constriction overall, although it did reduce constriction and hospitalisation, and it increased HIV-associated malignancy. Steroids in pericardial TB are therefore selective — large effusion, high inflammatory burden, early constriction — never automatic [10].
For ordinary pulmonary TB, steroids have no routine role; reserve them for the two proven sites and for paradoxical TB-IRIS [9] [13].
Special populations you will be asked about
Pregnancy. Standard RIPE is safe in pregnancy and treatment should not be deferred; pair isoniazid with pyridoxine. Streptomycin is contraindicated because of fetal ototoxicity, and preventive therapy for latent infection is usually postponed until after delivery unless risk is high. The newborn of an infectious mother needs specialist assessment, and often preventive therapy until the mother is non-infectious [1].
Chronic kidney disease. Ethambutol and pyrazinamide are renally cleared — in significant renal impairment they are given three times weekly rather than daily (after dialysis on dialysis days), with ethambutol ocular monitoring tightened. Isoniazid and rifampicin need no dose adjustment, and pyridoxine is mandatory [1].
Diabetes. Diabetes multiplies TB risk several-fold, worsens treatment outcomes and complicates glycaemic control during illness — and rifampicin induction destabilises oral hypoglycaemics. Screen diabetic TB patients closely and expect to escalate glucose therapy during treatment [3].
The pre-immunosuppression patient. Within its first years of use, infliximab was linked to reactivation TB — often disseminated, often within months of the first dose — the lesson that created modern pre-biologic screening. Before anti-TNF agents, other biologics, transplantation or prolonged high-dose steroids: take a risk history, image the chest, and test with IGRA or TST; treat latent infection first, and where immunosuppression is urgent, start it after at least a month of preventive therapy is on board [20] [3].
Public health: the part of the job description nobody writes down
Active TB is a notifiable disease in every Australian jurisdiction — laboratory and clinician both notify — and notification triggers the machinery: case management by the TB service, observed therapy where indicated, and contact investigation [1].
Contact tracing works in concentric circles: household and other close shared-air contacts first, then casual contacts only when the index case is highly infectious or contacts are vulnerable. A contact evaluation is a symptom screen, chest X-ray and IGRA or TST; young children and immunosuppressed contacts are prioritised, and children under five with evidence of infection but no disease receive preventive therapy once active disease has been excluded [3].
Airborne infection control: suspected or confirmed smear-positive pulmonary TB means a negative-pressure room and fit-tested P2/N95 respirators for staff; isolation is typically lifted after about two weeks of effective therapy with clinical response and a falling smear grade [1].
BCG is a neonatal vaccine for high-incidence settings and selected at-risk infants in low-incidence countries: meta-analysis of randomised trials shows solid protection against TB disease, strongest against the disseminated and meningeal forms that kill young children. Two exam-critical corollaries: BCG can make the TST false-positive — especially when given after infancy — but it does not affect IGRA; and BCG is contraindicated in significant immunosuppression [21] [19].
The long case: TB with HIV and social complexity
The archetypal DCE long case is the recently arrived migrant with pulmonary TB, a new HIV diagnosis, and a life that does not pause for a six-month regimen — casual work, shared housing, family overseas, sometimes a visa process, and two stigmatised diagnoses arriving at once. Examiners are scoring whether you move from the regimen to the person: regimen construction with ART timing and interactions, IRIS counselling before it happens, adherence architecture (case manager, observed therapy, practical supports), contact tracing of the share house and workplace, and honest counselling about infectiousness at work and at home. Your management plan should name the public-health unit as part of the treating team, not as an afterthought [11] [1]. The viva companion to this topic walks through that defence in the first person.
The short case: examining for apical disease
The respiratory short case is the patient with treated or suspected TB — cachexia, sometimes a thoracoplasty scar in an older patient, apical crackles and bronchial breathing over upper-lobe fibrosis or a cavity. Present the findings, then the interpretation: "chronic apical changes consistent with prior tuberculosis, with no features to suggest current activity" — and be ready with the differentials of apical cavitation (TB, non-tuberculous mycobacteria, cavitating lung cancer, fungal infection, vasculitis) and with the question every examiner asks next: "how would you determine whether this is active?" The answer: symptoms first, then sputum smear, NAAT and culture, and comparison with old imaging [2].
Exam traps, collected
References
- [1]Nahid P, Dorman SE, Alipanah N, et al. Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis Clin Infect Dis, 2016.PMID 27516382
- [2]Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children Clin Infect Dis, 2017.PMID 28052967
- [3]Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection N Engl J Med, 2015.PMID 26017823
- [4]Menzies D, Adjobimey M, Ruslami R, et al. Four Months of Rifampin or Nine Months of Isoniazid for Latent Tuberculosis in Adults N Engl J Med, 2018.PMID 30067931
- [5]Sterling TR, Villarino ME, Borisov AS, et al. Three months of rifapentine and isoniazid for latent tuberculosis infection N Engl J Med, 2011.PMID 22150035
- [6]Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tuberculosis and rifampin resistance N Engl J Med, 2010.PMID 20825313
- [7]Dorman SE, Schumacher SG, Alland D, et al. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Lancet Infect Dis, 2018.PMID 29198911
- [8]Peter JG, Zijenah LS, Chanda D, et al. Effect on mortality of point-of-care, urine-based lipoarabinomannan testing to guide tuberculosis treatment initiation in HIV-positive hospital inpatients: a pragmatic, parallel-group, multicountry, open-label, randomised controlled trial Lancet, 2016.PMID 26970721
- [9]Thwaites GE, Nguyen DB, Nguyen HD, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults N Engl J Med, 2004.PMID 15496623
- [10]Mayosi BM, Ntsekhe M, Bosch J, et al. Prednisolone and Mycobacterium indicus pranii in tuberculous pericarditis N Engl J Med, 2014.PMID 25178809
- [11]Abdool Karim SS, Naidoo K, Grobler A, et al. Timing of initiation of antiretroviral drugs during tuberculosis therapy N Engl J Med, 2010.PMID 20181971
- [12]Blanc FX, Sok T, Laureillard D, et al. Earlier versus later start of antiretroviral therapy in HIV-infected adults with tuberculosis N Engl J Med, 2011.PMID 22010913
- [13]Meintjes G, Wilkinson RJ, Morroni C, et al. Randomized placebo-controlled trial of prednisone for paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome AIDS, 2010.PMID 20808204
- [14]Conradie F, Diacon AH, Ngubane N, et al. Treatment of Highly Drug-Resistant Pulmonary Tuberculosis N Engl J Med, 2020.PMID 32130813
- [15]Conradie F, Bagdasaryan TR, Borisov S, et al. Bedaquiline-Pretomanid-Linezolid Regimens for Drug-Resistant Tuberculosis N Engl J Med, 2022.PMID 36053506
- [16]Nyang'wa BT, Berry C, Kazounis E, et al. A 24-Week, All-Oral Regimen for Rifampin-Resistant Tuberculosis N Engl J Med, 2022.PMID 36546625
- [17]Nunn AJ, Phillips PPJ, Meredith SK, et al. A Trial of a Shorter Regimen for Rifampin-Resistant Tuberculosis N Engl J Med, 2019.PMID 30865791
- [18]Dorman SE, Nahid P, Kurbatova EV, et al. Four-Month Rifapentine Regimens with or without Moxifloxacin for Tuberculosis N Engl J Med, 2021.PMID 33951360
- [19]Abubakar I, Drobniewski F, Southern J, et al. Prognostic value of interferon-γ release assays and tuberculin skin test in predicting the development of active tuberculosis (UK PREDICT TB): a prospective cohort study Lancet Infect Dis, 2018.PMID 30174209
- [20]Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent N Engl J Med, 2001.PMID 11596589
- [21]Mangtani P, Abubakar I, Ariti C, et al. Protection by BCG vaccine against tuberculosis: a systematic review of randomized controlled trials Clin Infect Dis, 2014.PMID 24336911
- [22]Török ME, Yen NT, Chau TT, et al. Timing of initiation of antiretroviral therapy in human immunodeficiency virus (HIV)--associated tuberculous meningitis Clin Infect Dis, 2011.PMID 21596680