Phys · infectious
Tuberculosis
Also known as TB · pulmonary tuberculosis · extrapulmonary tuberculosis · tuberculosis disease · reactivation tuberculosis · post-primary tuberculosis · scrofula · Pott disease · tuberculous meningitis · miliary tuberculosis · MDR-TB · XDR-TB · latent tuberculosis infection · LTBI
Consultant-physician-depth guide to tuberculosis — pathogenesis of Mycobacterium tuberculosis infection, primary versus reactivation disease, pulmonary and extrapulmonary TB, latent TB infection diagnosis and treatment, the RIPE regimen, drug-resistant TB (MDR/XDR and the BPaL regimen), and infection control — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Tuberculosis
Opening statement
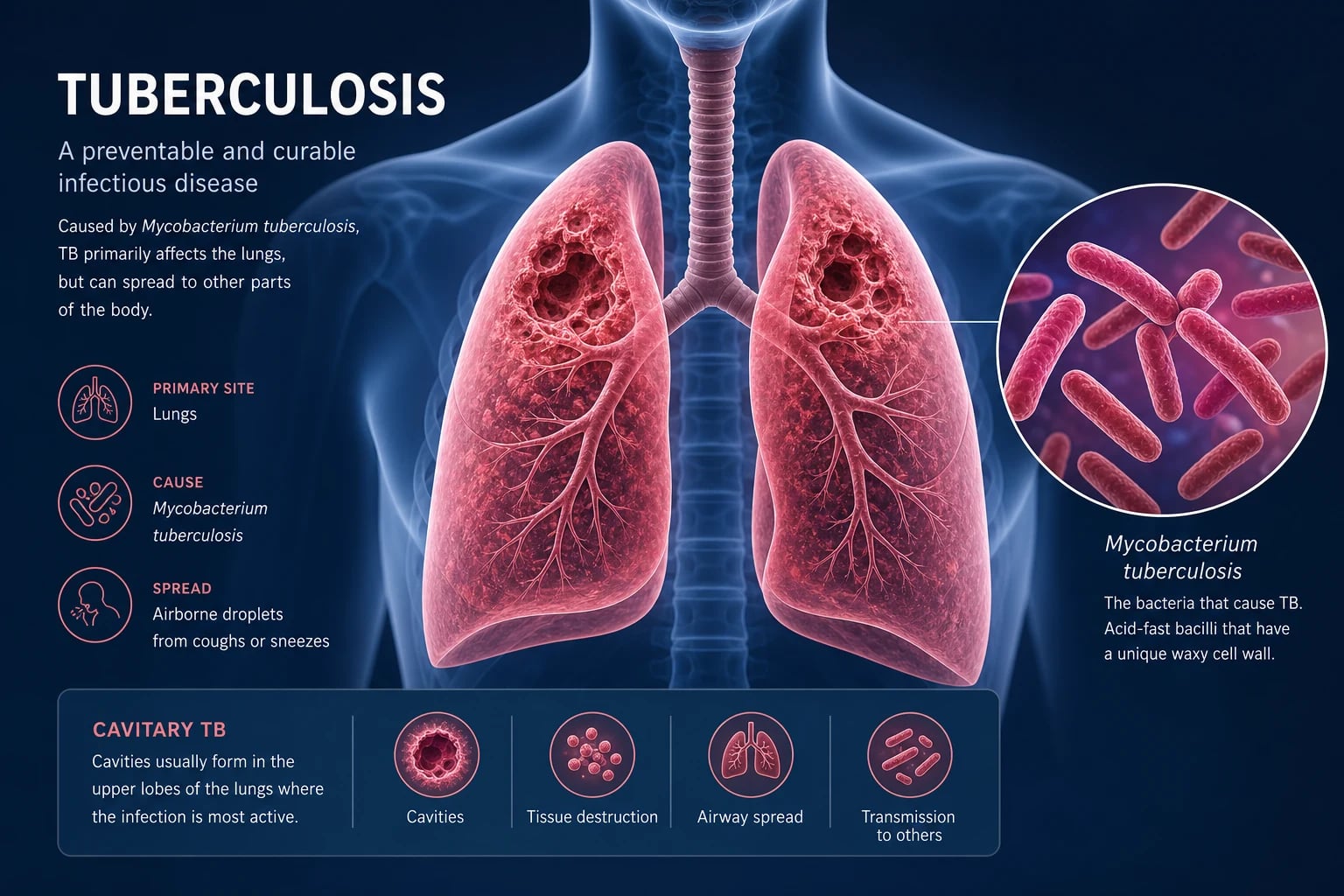
Tuberculosis is a chronic granulomatous infection caused by Mycobacterium tuberculosis complex. It kills more people than any other single infectious agent — approximately 1.25 million in 2023 alone — and is the leading killer of people living with HIV. For the registrar it behaves like three diseases in one body: a droplet-spread pulmonary infection demanding airborne isolation, a multisystem granulomatous disease that can seed any organ, and a latent infection that can reactivate decades later under immunosuppression. The decisive moves are simple and the same in every case — isolate the patient, prove the organism (smear plus nucleic acid amplification plus culture), ask about HIV and drug resistance before choosing a regimen, and complete a full six-month course under observation. [1]
Three examiner facts anchor every TB question. First, rifampicin resistance detected on GeneXpert changes the regimen before culture returns — never start standard RIPE therapy in a rifampicin-resistant case. Second, rifampicin is one of the most potent enzyme inducers in clinical medicine; it lowers the level of the oral contraceptive pill, warfarin, DOACs, corticosteroids, anticonvulsants and many antiretrovirals, and an unexpected loss of efficacy of a concomitant drug in a TB patient is usually rifampicin until proven otherwise. Third, ethambutol optic neuritis is irreversible if the drug is continued — test colour vision at baseline and educate every patient to stop and report visual change. [1]
Epidemiology and the WHO End TB strategy
Tuberculosis is a disease of inequity. The WHO reported an estimated 10.8 million new TB cases and 1.25 million deaths in 2023, with over 80 per cent occurring in 30 high-burden countries (India, Indonesia, China, the Philippines, Pakistan). Eight countries account for two-thirds of global cases. In Australia and New Zealand the annual incidence is low — under 7 per 100,000 — but case rates in Aboriginal and Torres Strait Islander communities, in people born in high-burden countries, and in close contacts of infectious cases are many-fold higher. In the United Kingdom incidence is around 8 per 100,000, concentrated in London and in foreign-born residents. Examiners expect you to know that TB is a notifiable disease in all three regions and that risk-stratified screening of migrants is standard practice. [1]
The WHO End TB strategy (2016 to 2035) sets three high-burden milestones for 2025 and targets for 2030 and 2035:
- A 90 per cent reduction in TB deaths and an 80 per cent reduction in TB incidence by 2030, and 95 per cent and 90 per cent respectively by 2035.
- No affected family facing catastrophic costs due to TB by 2020. [1]
The world missed the 2020 milestones badly — COVID-19 reversed years of progress by disrupting case detection and treatment. The 2023 figures show partial recovery, but drug-resistant TB remains a threat: only about two in five of the estimated MDR/RR-TB cases were diagnosed and enrolled on treatment. Know these numbers because they appear as MCQ stems and as context in long cases on migrant health and public health. [1]
The three highest-yield risk factors for reactivation of latent TB infection, in order, are HIV infection (the strongest single risk, with up to 10 per cent annual risk if untreated), recent TB infection within two years (especially infants and young adults), and fibrotic radiographic changes consistent with untreated prior TB. Immunosuppression from anti-TNF therapy, solid organ or haematopoietic transplant, silicosis, chronic kidney disease, diabetes, smoking and alcohol use disorder each increase risk several-fold (Getahun et al, 2015, PMID 26017823). [1]
Pathophysiology — primary infection, latency and reactivation
Transmission
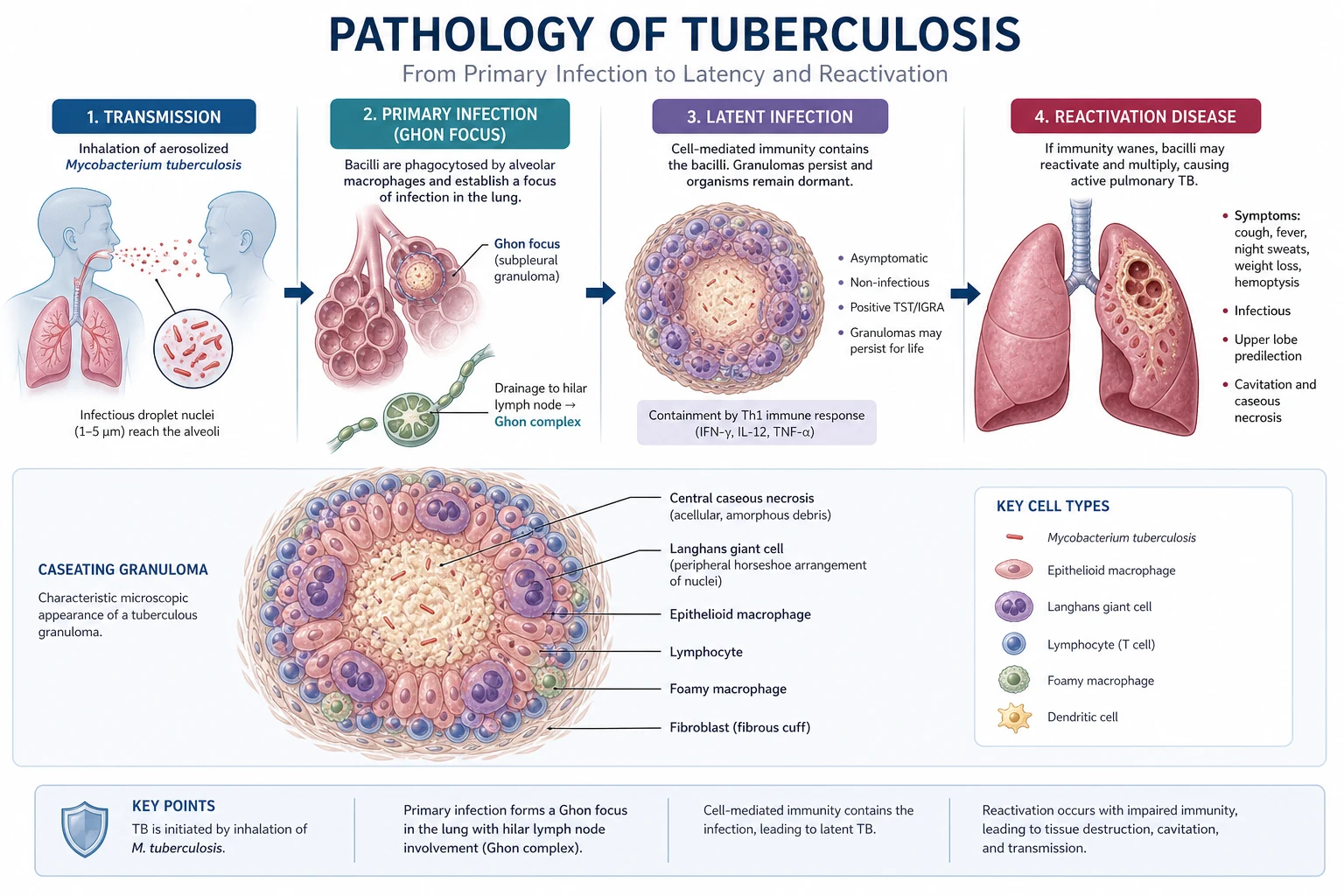
M. tuberculosis is an aerobic, non-motile, non-spore-forming bacillus with a waxy cell wall rich in mycolic acid — the basis for acid-fastness on Ziehl-Neelsen staining. It is spread almost exclusively by the airborne route in droplet nuclei under 5 micrometres generated by coughing, singing or forceful expiration of a person with pulmonary or laryngeal TB. These nuclei remain airborne for hours and reach the terminal alveoli, where they are phagocytosed by alveolar macrophages. Transmission is determined by contagiousness of the source (smear-positive cavitary disease is most contagious), duration and closeness of exposure, and shared air space ventilation. Fomites and the digestive route are essentially irrelevant for M. tuberculosis (the exception is M. bovis from unpasteurised milk). Droplet nuclei, not droplets, are the unit of transmission — this is why the protection is an N95/P2 respirator in a negative-pressure room, not a surgical mask. [1]
Primary infection and the Ghon focus
Inhaled bacilli reach the subpleural upper lower lobe or lower upper lobe — the regions of highest ventilation — and are ingested by alveolar macrophages. The macrophage cannot kill M. tuberculosis because the organism blocks phagolysosome fusion (the mycolic acid cell wall and the secreted antigen EsxA/ESAT-6 disrupt the endosomal pathway). The bacilli multiply intracellularly, the infected macrophage dies, and the bacilli are taken up by recruited macrophages and carried to the draining hilar and mediastinal lymph nodes. The resulting combination — a subpleural granuloma (the Ghon focus) plus enlarged draining hilar nodes — is the Ghon (or primary) complex. In more than 90 per cent of immunocompetent adults the cell-mediated immune response (CD4+ Th1 cells activating macrophages via interferon-gamma) controls the infection within weeks. The Ghon focus then calcifies over months to years; when a calcified Ghon focus is accompanied by a calcified draining lymph node it is called a Ranke complex. [1]
Most primary infections are subclinical. A minority develop primary progressive TB (especially children under 5, the elderly, and the immunosuppressed), presenting as progressive primary pneumonia, pleural effusion, or, rarely, disseminated (miliary) TB or tuberculous meningitis. [1]
Latent tuberculosis infection
Latent TB infection (LTBI) is a state of persistent immune response to M. tuberculosis antigens without clinical, radiographic or microbiological evidence of active disease. Viable bacilli persist in a dormant state inside macrophages within calcified granulomas. The patient is well, is not infectious, and has a normal chest radiograph. LTBI is inferred from a positive tuberculin skin test or interferon-gamma release assay. The lifetime risk of reactivation in an untreated immunocompetent adult is about 5 to 10 per cent, with roughly half of that risk in the first two years after infection. [1]
Post-primary (reactivation) TB
Post-primary TB arises either from endogenous reactivation of latent bacilli or, less commonly, from exogenous reinfection. Reactivation occurs preferentially in the upper lobes because of the high oxygen tension that favours aerobic M. tuberculosis growth. The pathological hallmark is caseating granuloma — a central area of necrotic, cheese-like material surrounded by epithelioid macrophages, Langhans giant cells and lymphocytes. As caseation liquifies and communicates with a bronchus, the necrotic contents are expectorated, leaving a thick-walled cavity — the radiological hallmark of post-primary TB and the source of the heavy bacillary load that makes these patients so infectious. [1]
Why this matters clinically
The pathophysiology tells you five things you will use at the bedside. Airborne spread demands a negative-pressure room, not a side room. The waxy cell wall explains why treatment must be prolonged — the bacillus divides only every 18 to 24 hours and persists in a poorly penetrable granuloma. The high-oxygen upper lobe preference explains the radiographic pattern. The dormant state explains why two drugs (isoniazid and rifampicin) are needed to kill both rapidly dividing bacilli and the slow, persisting sub-population — the principle of sterilising activity that shortens therapy to six months. And the immune (granulomatous) response explains the paradoxical immune reconstitution inflammatory syndrome (IRIS) when ART is started in HIV-TB co-infection. [1]
Pulmonary TB — the clinical presentation
The classic tetrad
Pulmonary TB accounts for about 80 per cent of cases in adults. The classic tetrad is chronic cough, haemoptysis, constitutional symptoms, and weight loss — but the order and prominence of each varies. The cough is persistent, initially dry, later productive of mucopurulent or blood-streaked sputum. Haemoptysis may be minimal (streaks) or, in cavitary disease with erosion into a bronchial artery, massive and life-threatening. Constitutional symptoms are fever (often low-grade and evening), drenching night sweats, fatigue and anorexia. Weight loss can be striking — "consumption" — and cachexia is a feature of advanced disease. The clinical trap is that TB can present as any one of these in isolation: a chronic cough alone in a smoker, an iron-deficiency picture from chronic GI blood loss, an incidental upper-lobe infiltrate on a pre-operative chest radiograph, or a unifocal cervical lymph node. [1]
Examination
Physical signs are often sparse and non-specific. Look for cachexia, low-grade fever, tachycardia and, in advanced disease, clubbing. Chest examination may reveal apical crackles, signs of consolidation, or signs of pleural effusion. Always examine the cervical and supraclavicular lymph nodes (scrofula) and the abdomen (hepatosplenomegaly in miliary disease). Look for signs of HIV — oral candidiasis, generalised lymphadenopathy, hairy leucoplakia — because HIV-TB co-infection changes the management immediately. [1]
The chest radiograph
The chest radiograph distinguishes primary from post-primary disease and drives the diagnostic work-up: [1]
| Pattern | Suggests | Appearance |
|---|---|---|
| Upper lobe apical infiltrate | Post-primary TB | Patchy or nodular opacity in the apical or posterior segment of the upper lobe |
| Cavity with surrounding infiltrate | Post-primary, highly infectious | Thick-walled cavity, often apical, with surrounding fibronodular change |
| Pleural effusion (unilateral) | Primary TB or post-primary | Usually unilateral, straw-coloured, exudative, lymphocyte-predominant |
| Hilar or mediastinal lymphadenopathy | Primary TB (especially children, HIV) | Bulky nodes; in adults raises concern for lymphoma or malignancy |
| Miliary (1 to 3 mm nodules diffusely) | Disseminated TB | Fine "snowstorm" nodules throughout both lungs |
| Lower lobe infiltrate | Atypical in adults; consider HIV with low CD4 | May mimic bacterial pneumonia |
| Fibronodular calcification | Healed prior TB (Ranke complex) | Apical fibrosis with volume loss; not active unless changing |
The single most important radiographic discriminator for an examiner is the upper lobe predominance of post-primary TB. Cavitary disease is the radiographic correlate of high bacillary load and infectivity. HIV co-infection with low CD4 counts produces atypical radiographs — lower lobe infiltrates, diffuse infiltrates, intrathoracic lymphadenopathy, and absence of cavitation — so a normal or atypical chest radiograph does NOT exclude TB in an HIV-positive patient. [1]
Diagnosis of pulmonary TB — three tests, three purposes
The ATS/IDSA/CDC diagnostic guideline (Lewinsohn et al, 2017, PMID 28052967) and the WHO define three laboratory tests with three different purposes. Every suspected pulmonary TB patient gets all three: a smear for speed and infectivity, a nucleic acid amplification test for same-day diagnosis and rifampicin resistance, and culture for confirmation, full drug susceptibility testing and the gold-standard diagnosis. [1]
1. Sputum smear — AFB microscopy (Ziehl-Neelsen or auramine)
Sputum is stained with carbol-fuchsin (Ziehl-Neelsen, light microscopy) or auramine-rhodamine (fluorescence microscopy) to identify acid-fast bacilli. The sensitivity is roughly 50 to 60 per cent of all culture-confirmed cases and is proportional to bacillary load — smear positivity requires approximately 5,000 to 10,000 bacilli per millilitre of sputum. Smear positivity therefore identifies the most infectious patients. Smear does not distinguish M. tuberculosis from non-tuberculous mycobacteria (NTM), and it is negative in paucibacillary disease (HIV, extrapulmonary TB, early infection). Two to three serial early-morning sputums are collected to maximise yield. [1]
2. Nucleic acid amplification testing — GeneXpert MTB/RIF and Xpert Ultra
The Xpert MTB/RIF assay (Boehme et al, 2010, PMID 20825313) is a cartridge-based, automated, real-time PCR that simultaneously detects M. tuberculosis complex DNA and the most common mutations in the rpoB gene conferring rifampicin resistance. It delivers a result within two hours. Performance: sensitivity of about 98 per cent in smear-positive and 70 to 80 per cent in smear-negative disease, with specificity greater than 99 per cent. The newer Xpert MTB/RIF Ultra improves sensitivity in paucibacillary disease (down to about 16 bacilli per millilitre) at the cost of a small loss of specificity, with "trace" calls requiring clinical correlation. Every suspected pulmonary TB sample gets an Xpert on the first specimen — this is the single most important change in TB diagnostics in the last 20 years because it gives a same-day diagnosis with resistance information, allowing rational regimen choice from day one. [1]
The clinical rule: a smear-positive, Xpert-positive patient has infectious pulmonary TB and goes into airborne isolation; an Xpert-detected rifampicin resistance must not be treated with standard RIPE — refer to an MDR-TB service and await full phenotypic susceptibility. [1]
3. Mycobacterial culture — the gold standard
Culture remains the gold standard for diagnosis and the only method that allows full phenotypic drug susceptibility testing. Two culture systems are used in parallel:
- Solid culture — Lowenstein-Jensen (LJ) egg-based medium with malachite green. Slow — visible colonies at 2 to 8 weeks. Largely superseded for primary isolation but still useful for NTM speciation.
- Liquid culture — mycobacterial growth indicator tube (MGIT, BACTEC) using a fluorescence-quenching oxygen sensor. Faster — positivity typically at 1 to 3 weeks — and more sensitive than solid culture. WHO and CDC recommend liquid culture as the primary method. [1]
Once growth is detected, the organism is identified by molecular probe (line-probe assay or MPT64 antigen) and full phenotypic and molecular susceptibility testing to first- and second-line drugs is performed. A negative culture at 8 weeks (MGIT plus LJ) excludes culture-confirmed TB but not paucibacillary disease — the diagnosis of TB can be made on clinical and radiographic grounds if the pre-test probability is high. [1]
Additional investigations
- Line-probe assays (LPA) — GenoType MTBdrplus and MTBdrs1 — detect resistance to rifampicin, isoniazid, fluoroquinolones and second-line injectables from smear-positive sputum or culture in 1 to 2 days. Useful for rapidly characterising MDR-TB.
- Whole genome sequencing — increasingly used in high-income settings for transmission investigation, precise resistance prediction, and ruling in or out recent transmission.
- Interferon-gamma release assays (IGRA) and tuberculin skin test (TST) — tests for latent infection only; they are NOT diagnostic of active disease. See the LTBI section below.
- Bronchoscopy with washings, bronchoalveolar lavage or transbronchial biopsy is useful for smear-negative patients in whom sputum cannot be obtained or is repeatedly negative, and for suspected endobronchial TB.
- Chest CT is not routine but helps characterise pleural disease, adenopathy, miliary nodules, and the complications of cavitation (aspergilloma, bronchiectasis). [1]
Extrapulmonary TB
Extrapulmonary TB occurs in about 20 per cent of immunocompetent cases and in over half of HIV-positive patients. Each site has a typical presentation, a typical diagnostic yield, and a typical exam trap. [1]
Tuberculous lymphadenitis — scrofula
The most common extrapulmonary site. Presents as a painless, slowly enlarging cervical (usually supraclavicular or posterior triangle) lymph node, often unilateral and often in a person born in a high-burden country. As disease progresses, nodes become matted and may develop overlying skin discolouration and a discharging sinus. Diagnosis is by fine-needle aspiration or excision biopsy with histology (caseating granulomas), AFB smear (low sensitivity, 10 to 50 per cent), mycobacterial culture and Xpert. Excision biopsy has the highest yield (over 90 per cent) and is preferred when FNA is non-diagnostic. Treat with standard RIPE for 6 months; surgical excision is reserved for diagnostic uncertainty or non-response. [1]
Tuberculous pleural effusion
Presents as a unilateral pleural effusion, typically a few weeks after primary infection (a form of delayed hypersensitivity reaction to bacilli entering the pleural space). Pleural fluid is an exudate with lymphocyte predominance (greater than 50 per cent lymphocytes), low glucose (often less than 3.3 mmol/L), raised LDH, and a pH typically less than 7.4. AFB smear of pleural fluid is positive in fewer than 10 per cent of cases; culture positivity is about 25 to 50 per cent. The single most useful diagnostic test is closed pleural biopsy with histology (caseating granulomas, positive in 60 to 90 per cent) plus culture; pleural fluid ADA greater than 40 U/L has high sensitivity and is useful in high-prevalence settings. Pleural TB is treated with standard RIPE for 6 months. [1]
Tuberculous meningitis
The most lethal form of TB. Presents subacutely with a prodrome of headache, low-grade fever, malaise and personality change for 2 to 8 weeks, followed by meningism, cranial nerve palsies (especially cranial nerves III, VI, VII), seizures, focal deficits, and progressive depressed consciousness. The British Medical Research Council (BMRC) staging predicts outcome: [1]
| Stage | Features | Mortality |
|---|---|---|
| Stage I | Conscious, no focal signs, no hydrocephalus | Under 10 per cent |
| Stage II | Confused, drowsy, or focal neurological sign | Around 30 per cent |
| Stage III | Comatose, decerebrate or decorticate posturing, or dense paraplegia | Over 50 per cent |
Cerebrospinal fluid shows a lymphocytic pleocytosis (typically 50 to 500 cells per microlitre), raised protein (1 to 5 g/L), and low glucose (less than 2.5 mmol/L or less than 40 per cent of a simultaneous plasma glucose). AFB smear of CSF is positive in fewer than 20 per cent; culture in 50 to 70 per cent; Xpert MTB/RIF has moderate sensitivity (around 60 to 80 per cent) and high specificity for TBM and is the first molecular test to perform on CSF when TBM is suspected. Never delay treatment — if the clinical and CSF picture suggest TBM, start RIPE therapy plus corticosteroids while awaiting results. [1]
Adjunctive intravenous dexamethasone improves survival in adolescents and adults with TBM at all BMRC stages, without clearly reducing severe disability (Thwaites et al, 2004, PMID 15496623). The WHO and CDC recommend corticosteroids for all patients with TBM. The regimen is dexamethasone tapering over 6 to 8 weeks (initial 0.4 mg/kg daily). Antiretroviral therapy in HIV-TBM co-infection should be deferred for at least 4 weeks (and possibly 8 weeks) after starting TB therapy because of the high risk of paradoxical IRIS with neurological deterioration; this is an exception to the usual "ART within 2 weeks" rule for TB in HIV with CD4 under 50. [1]
Skeletal TB — Pott disease (tuberculous spondylitis)
Pott disease typically affects the lower thoracic and upper lumbar spine. The infection begins in the anterior inferior vertebral body, spreads beneath the anterior or posterior longitudinal ligament to the adjacent vertebra, and causes collapse of the intervertebral disc and vertebral body — producing the characteristic gibbus deformity and, with posterior element involvement, spinal cord compression and paraplegia. Presents with chronic back pain, localised tenderness, a cold paraspinal abscess (psoas abscess pointing in the groin), and neurological signs if cord compression. MRI is the imaging modality of choice. Obtain tissue (CT-guided biopsy or open biopsy) for histology, culture and Xpert before starting therapy. Treat medically for at least 9 to 12 months; surgical fixation is indicated for spinal instability, progressive neurological deficit, or failure of medical therapy. Other skeletal sites include the hip, knee, and the digits (tuberculous dactylitis). [1]
Tuberculous pericarditis
Presents with pericardial effusion or constrictive pericarditis in a patient from a high-burden country. The effusion may be large and cause tamponade. Diagnosis is supported by pericardial fluid analysis (exudative, lymphocytic, high ADA) and pericardial biopsy. The WHO and ATS/IDSA/CDC guidelines recommend adjunctive corticosteroids for tuberculous pericarditis to reduce the risk of constrictive pericarditis, although the large IMPI-1 trial did not show a clear mortality benefit. Standard RIPE for 6 months, plus consideration of pericardiocentesis for tamponade and pericardiectomy for established constriction. [1]
Miliary (disseminated) TB
Miliary TB is the haematogenous dissemination of M. tuberculosis throughout the body. It presents with non-specific systemic symptoms — fever, weight loss, anorexia, weakness — and, in advanced disease, with multi-organ involvement (lungs, liver, spleen, bone marrow, meninges, adrenals). The chest radiograph shows the classic fine 1 to 3 mm nodules ("millet seed") throughout both lung fields. Pancytopenia, hyponatraemia from adrenal insufficiency or SIADH, and deranged liver enzymes are common. Fundoscopy may show choroidal tubercles, which are pathognomonic. Diagnosis is by sputum (often smear-negative but culture-positive in over 50 per cent), bronchoscopy, and tissue biopsy (liver, bone marrow). Treatment is standard RIPE for 6 to 9 months, with extension to 9 to 12 months if central nervous system involvement. Add corticosteroids if meningitis coexists. [1]
Gastrointestinal and abdominal TB
GI TB can affect any part of the gut but favours the ileo-caecal region (which mimics Crohn disease). Presents with abdominal pain, weight loss, altered bowel habit, a palpable mass, or obstruction. Ascitic TB presents with a lymphocyte-rich exudative ascites; diagnostic paracentesis shows ADA elevated and culture positivity is moderate; laparoscopy with peritoneal biopsy is the most sensitive test. Always distinguish TB from Crohn disease — wrong treatment (corticosteroids for presumed Crohn) can disseminate TB. [1]
Latent tuberculosis infection — diagnosis and treatment
Tests for latent infection
Neither test diagnoses active disease — they detect a cell-mediated immune response to M. tuberculosis antigens. A diagnosis of LTBI requires a positive test plus exclusion of active TB by chest radiograph and symptom screen. [1]
Tuberculin skin test (Mantoux): 5 tuberculin units of purified protein derivative (PPD) injected intradermally into the volar forearm; read as induration (not erythema) at 48 to 72 hours. Interpretation depends on pre-test probability:
- 5 mm or more is positive in HIV, recent contacts, fibrotic radiographic changes, immunosuppression, organ transplant.
- 10 mm or more is positive in recent arrivals from high-burden countries, injecting drug users, residents and employees of high-risk congregate settings, children under 4, and patients with silicosis, diabetes, chronic renal failure, or on immunosuppressive therapy.
- 15 mm or more is positive in people with no known risk factors. [1]
A BCG vaccine in the past can cause false-positive TST, especially within 10 years of vaccination and most prominently in those vaccinated after infancy. The TST can also be falsely negative in HIV, malnutrition, immunosuppression, disseminated TB, and recent infection (the window period of 8 to 10 weeks). [1]
Interferon-gamma release assays (IGRA): QuantiFERON-TB Gold Plus (whole-blood ELISA measuring interferon-gamma) and T-SPOT.TB (ELISpot counting interferon-gamma-secreting T cells). Both use M. tuberculosis-specific antigens (ESAT-6, CFP-10, TB7.7) that are not present in BCG or most environmental mycobacteria, so they are not affected by prior BCG vaccination. IGRA requires a single blood sample, has no boosting effect, and is generally preferred for BCG-vaccinated adults and for two-step testing in healthcare workers. Sensitivity is similar to TST; in active TB, IGRA sensitivity is around 80 per cent (higher for T-SPOT.TB than QuantiFERON), with specificity around 95 per cent. The UK PREDICT TB cohort showed that IGRAs and the TST all have poor positive predictive value for progression to active TB (Abubakar et al, 2018, PMID 30174209) — the positive predictive value of any single test is only 2 to 3 per cent — so testing should be reserved for people at genuine risk of progression. [1]
Who should be tested
The principle is to test only those in whom you will act on a positive result. The high-yield groups are:
- People living with HIV
- Close contacts of infectious pulmonary TB
- People newly arrived from high-burden countries (within 5 years of arrival in some guidelines)
- Patients about to start anti-TNF therapy, other biologics, or significant immunosuppression (transplant, chemotherapy)
- Patients with end-stage renal failure, silicosis
- Healthcare workers and laboratory staff
- Children under 5 who are contacts of infectious cases [1]
Treatment of latent TB infection
Before treating LTBI, exclude active TB with a chest radiograph, symptom screen and, if any suspicion, sputum for Xpert and culture. Starting single-drug LTBI therapy in a patient with active TB risks treatment failure and acquired resistance. [1]
The WHO and CDC recommend the following regimens, listed in order of preference in high-income settings:
- Rifampicin for 4 months (600 mg daily) — preferred regimen in many high-income settings including the UK NICE and increasingly ANZ. The Menzies RCT (Menzies et al, 2018, PMID 30067931) demonstrated non-inferior efficacy to 9 months of isoniazid with significantly less hepatotoxicity and higher completion rates. [1]- Isoniazid plus rifapentine for 3 months (3HP) — weekly rifapentine plus isoniazid for 12 doses. Now also available daily for 3 months. Equivalent efficacy to 9 months of isoniazid with less hepatotoxicity and shorter duration.
- Isoniazid for 6 to 9 months (6H or 9H) — the traditional regimen; effective but longer and associated with higher hepatotoxicity, neuropathy and poor completion. Pyridoxine 25 mg daily is co-administered in pregnancy, HIV, chronic kidney disease, diabetes, alcohol use disorder and malnutrition to prevent peripheral neuropathy.
- Isoniazid plus rifampicin for 3 to 4 months (3HR) — widely used in children and in some adult programmes. [1]
In pregnancy, LTBI treatment is usually deferred until 2 to 3 months postpartum unless the infection is recent or the woman is highly immunosuppressed, in which case isoniazid with pyridoxine is considered safe. Rifampicin in pregnancy is safe but rifapentine data are more limited. [1]
Active TB treatment — the RIPE regimen
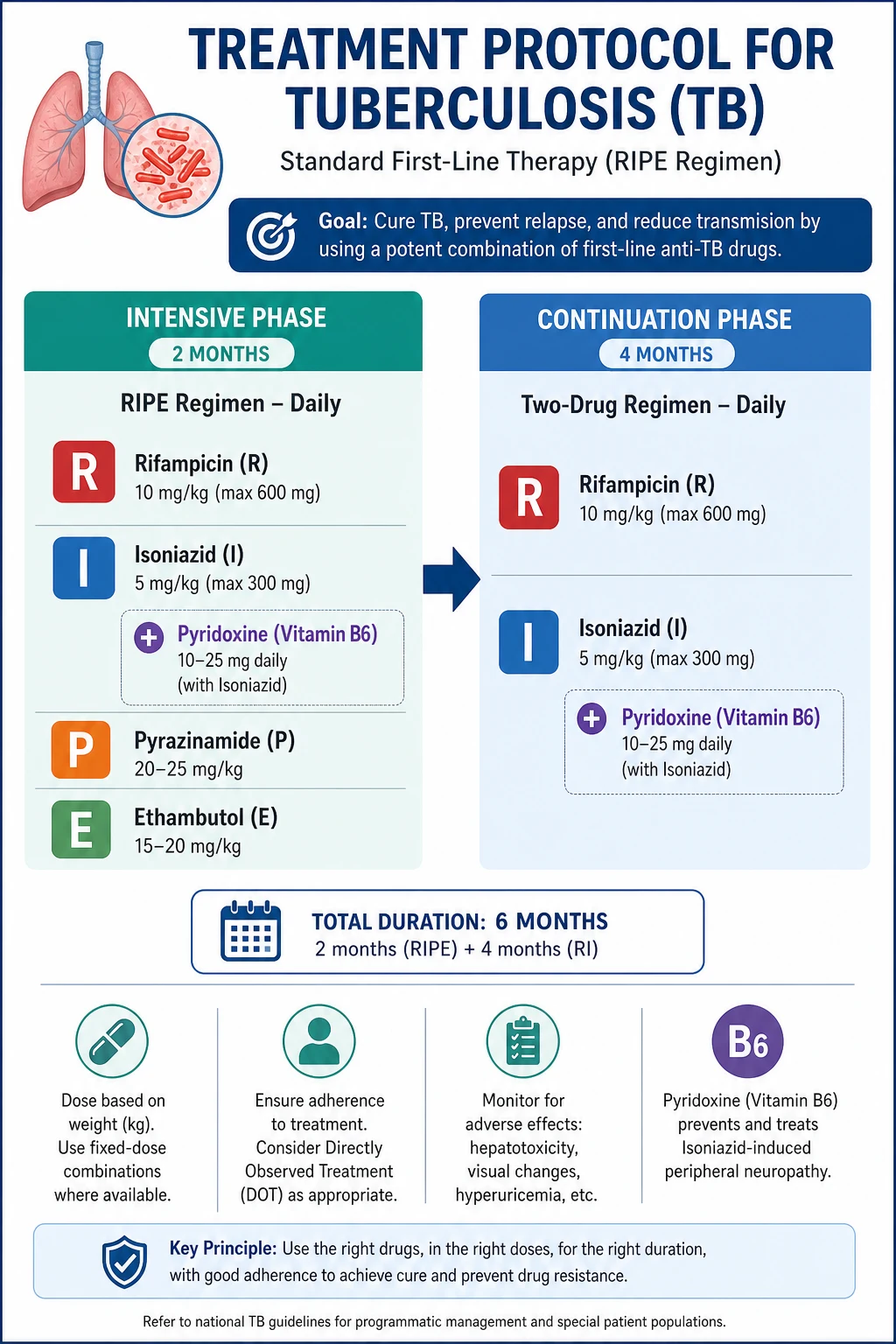
The treatment of drug-susceptible pulmonary TB in adults is the RIPE regimen (also written HRZE): rifampicin, isoniazid, pyrazinamide and ethambutol daily for the intensive phase of 2 months, followed by rifampicin plus isoniazid for the continuation phase of 4 months, for a total of 6 months (Nahid et al, 2016, PMID 27516382). [1]
Phase 1 — intensive phase (8 weeks)
| Drug | Adult daily dose | Role | Target | [1]|---|---|---|---| | Rifampicin | 10 mg/kg (max 600 mg) orally | Bactericidal, sterilising | Rapidly dividing AND slowly metabolising bacilli | | Isoniazid | 5 mg/kg (max 300 mg) orally | Bactericidal, early kill | Rapidly dividing bacilli | | Pyrazinamide | 20 to 25 mg/kg (max 2 g) orally | Sterilising (acidic environment of granuloma) | Intracellular, slowly replicating bacilli | | Ethambutol | 15 to 20 mg/kg orally | Bacteriostatic | Added to cover possible INH resistance until susceptibilities return | [1]
The four drugs together achieve three pharmacodynamic goals: rapid early bactericidal killing (isoniazid), sterilisation of semi-dormant bacilli (rifampicin and pyrazinamide), and protection of the regimen against the emergence of resistance in the first weeks (ethambutol, and the principle of multiple active drugs). The sterilising activity of pyrazinamide and rifampicin is the key insight that allows a 6-month course — without pyrazinamide the regimen must be extended to 9 months. [1]
Phase 2 — continuation phase (16 weeks)
Continue rifampicin and isoniazid daily for a further 4 months. Pyrazinamide and ethambutol are stopped after the intensive phase because their sterilising and resistance-protecting roles are fulfilled and because their toxicity (especially hepatotoxicity from pyrazinamide and optic neuritis from ethambutol) is dose- and duration-dependent. [1]
When to extend therapy
Extend treatment to 9 months for: cavitary pulmonary TB with a positive 2-month sputum culture (a marker of slow response), central nervous system TB (9 to 12 months), bone and joint TB (9 to 12 months), miliary TB with CNS involvement (9 to 12 months), and pericardial TB (6 months but often extended). HIV co-infection does NOT in itself require extension provided the patient is on ART and responding. [1]
Directly observed therapy (DOT)
WHO recommends DOT as part of patient-centred care, with treatment support tailored to the patient. In ANZ, DOT is offered selectively (homelessness, substance use, prior non-adherence, high risk of treatment failure or MDR-TB) rather than universally. Video-observed therapy (VOT) is an increasingly used alternative. [1]
Monitoring during therapy
- Baseline liver function tests, renal function, full blood count, hepatitis B and C and HIV serology, visual acuity and colour vision (Ishihara plates) before ethambutol.
- Monthly clinical review with symptom enquiry, weight, adherence, and enquiry about drug side effects.
- Liver function tests if baseline abnormal, pregnancy, HIV, alcohol use disorder, hepatitis B or C; or symptoms of hepatitis (nausea, vomiting, abdominal pain, jaundice).
- Repeat sputum smear and culture at 2 months (a positive 2-month culture predicts relapse and mandates extension to 9 months for cavitary disease), and at 5 and 6 months to document bacteriological cure.
- Visual acuity and colour vision monthly while on ethambutol; stop immediately and refer to ophthalmology if any visual change. [1]
Drug side effects — memorise these
| Drug | Key toxicity | Management |
|---|---|---|
| Rifampicin | Hepatitis (usually mild transaminitis), orange discolouration of secretions (benign, warn patients), flu-like syndrome with intermittent dosing, drug interactions (potent hepatic enzyme inducer) | Stop if ALT exceeds 3 times upper limit of normal with symptoms, or 5 times without; check all concomitant drug levels |
| Isoniazid | Hepatitis, peripheral neuropathy (pyridoxine-responsive), drug-induced lupus, CNS effects | Pyridoxine 25 mg daily prophylaxis in high-risk patients; stop and investigate if hepatitis symptoms |
| Pyrazinamide | Hepatitis (often the most hepatotoxic), hyperuricaemia and gout, arthralgia, photosensitivity | Stop for symptomatic hyperuricaemia or significant hepatitis; pyrazinamide is the first drug to withhold in significant transaminitis |
| Ethambutol | Optic neuritis (retrobulbar, dose- and duration-related) — reduced visual acuity, red-green colour blindness, central scotoma; usually reversible if stopped early | Baseline and monthly visual acuity and colour vision; stop immediately and refer if visual change; avoid in young children who cannot report visual symptoms |
The shared hepatotoxicity of isoniazid, rifampicin and pyrazinamide is the single most important adverse effect of the RIPE regimen. The clinical rule: any patient on TB therapy reporting nausea, vomiting, abdominal pain or jaundice must have liver function tests performed urgently and the drugs withheld until results. The usual sequence for reintroduction after drug-induced hepatitis is to restart one drug at a time, beginning with rifampicin, then isoniazid, then pyrazinamide, observing LFTs at each step; if pyrazinamide is the culprit the regimen can be extended to 9 months without it. [1]
Rifampicin — the master drug-interaction trap
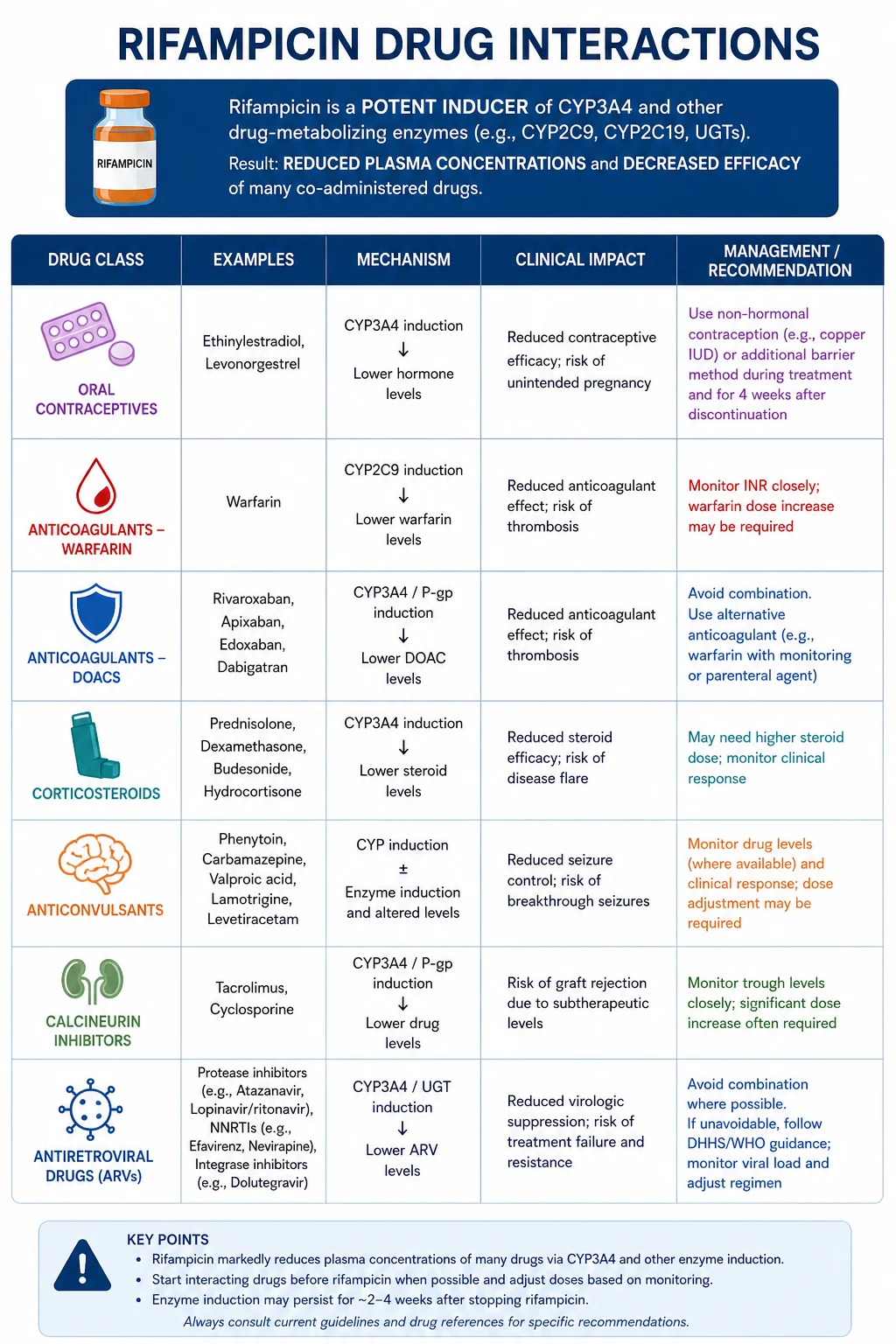
Rifampicin is a potent inducer of hepatic cytochrome P450 enzymes (especially CYP3A4) and the P-glycoprotein efflux transporter. Induction peaks at 1 to 2 weeks and persists for up to 2 weeks after rifampicin is stopped. The consequence is a clinically important reduction in the level of many co-administered drugs. This is the single most tested pharmacological fact about TB. Know the following: [1]
- Oral contraceptive pill — rifampicin reduces OCP efficacy; advise additional barrier contraception throughout therapy.
- Warfarin — rifampicin markedly lowers INR; warfarin dose typically needs to be doubled or tripled.
- DOACs (dabigatran, rivaroxaban, apixaban) — rifampicin reduces DOAC levels and may compromise anticoagulation; switch to warfarin or low-molecular-weight heparin during TB therapy.
- Corticosteroids — rifampicin increases corticosteroid clearance and may precipitate adrenal crisis in patients on long-term replacement; double the hydrocortisone dose.
- Anticonvulsants (phenytoin, valproate, lamotrigine) — reduced levels; monitor levels and clinical seizure control.
- Calcineurin inhibitors (cyclosporin, tacrolimus) — dramatically reduced levels; monitor troughs and adjust.
- Antiretrovirals — rifampicin reduces levels of most protease inhibitors (contraindicated with boosted PIs) and many NNRTIs; use efavirenz-based ART (or rifabutin instead of rifampicin) when co-administering.
- Statins, beta-blockers, digoxin, theophylline, methadone, oral hypoglycaemics — all affected. [1]
Drug-resistant TB — MDR, pre-XDR and XDR
Definitions (WHO, 2021)
- Mono-resistance — resistance to one first-line drug.
- Poly-resistance — resistance to more than one first-line drug, other than both isoniazid and rifampicin.
- Multidrug-resistant TB (MDR-TB) — resistance to at least isoniazid AND rifampicin.
- Rifampicin-resistant TB (RR-TB) — resistance to rifampicin alone or in combination (managed as MDR-TB because rifampicin resistance is the strongest predictor of treatment failure).
- Pre-XDR-TB — MDR/RR-TB with additional resistance to any fluoroquinolone (levofloxacin or moxifloxacin).
- Extensively drug-resistant TB (XDR-TB) — MDR/RR-TB with resistance to any fluoroquinolone AND at least one additional Group A drug (bedaquiline or linezolid). The 2021 WHO update removed the older "second-line injectable" requirement because injectables are no longer recommended in all-oral regimens. [1]
The shorter MDR-TB regimen
The WHO-endorsed shorter all-oral MDR-TB regimen (9 to 12 months) is based on the STREAM Stage 1 trial (Nunn et al, 2019, PMID 30865791), which demonstrated non-inferiority of a 9 to 11 month regimen versus the 20 month conventionally longer regimen. The current WHO shorter regimen includes bedaquiline (6 months), levofloxacin or moxifloxacin, ethionamide, ethambutol, isoniazid (high-dose), pyrazinamide and clofazimine for 4 to 6 months, then 5 months of fluoroquinolone, clofazimine, ethambutol and pyrazinamide. Eligibility requires no resistance to the shorter regimen components and no previous second-line exposure. [1]
The BPaL and BPaLM regimens
The Nix-TB trial (Conradie et al, 2020, PMID 32130813) established the BPaL regimen — bedaquiline, pretomanid and linezolid for 6 months — for XDR-TB or treatment-intolerant/non-responsive MDR-TB, with favourable outcomes in about 90 per cent of patients. The ZeNix trial refined linezolid dose and duration to reduce myelosuppression and neuropathy. The newer BPaLM regimen (BPaL plus moxifloxacin) is now WHO-recommended for MDR/RR-TB patients without additional fluoroquinolone resistance, offering a 6-month all-oral cure for many MDR-TB patients. [1]
Second-line drugs and Group A agents
The WHO classifies anti-TB drugs into Groups A to C for designing MDR-TB regimens. Group A drugs are the most potent and should all be included in a regimen if possible: levofloxacin or moxifloxacin, bedaquiline, linezolid. Group B includes clofazimine and cycloserine/terizidone. Group C includes ethambutol, delamanid, pyrazinamide, imipenem-cilastatin/meropenem, amikacin (or streptomycin), ethionamide/prothionamide, and para-aminosalicylic acid. The injectable aminoglycosides (amikacin, capreomycin, kanamycin) are no longer first-line for MDR-TB because of ototoxicity and nephrotoxicity; they are reserved as last-resort Group C agents. [1]
Monitoring
All MDR-TB patients need a baseline ECG (bedaquiline and fluoroquinolones prolong QT interval), full blood count (linezolid causes myelosuppression), audiology (if aminoglycosides used), renal function, LFTs and mental health assessment. Treatment is delivered in close liaison with a specialist MDR-TB service and is always individualised to the resistance pattern. [1]
Special situations
TB and HIV
Every patient with TB is tested for HIV, and every patient with HIV is screened for TB at every encounter. HIV is the strongest single risk factor for reactivation and for progression of primary infection. Clinical differences in advanced HIV include atypical radiographs (lower lobe, diffuse, nodal), extrapulmonary and disseminated disease, and high bacillary load with paradoxically negative smears. Management rules: use a rifamycin (rifampicin or rifabutin) throughout; start ART within 2 weeks of TB therapy for patients with CD4 less than 50 cells per microlitre, and by 8 weeks for higher CD4 counts; defer ART for at least 4 weeks in tuberculous meningitis because of IRIS risk; use an efavirenz-based ART regimen with rifampicin or substitute rifabutin with a protease inhibitor; treat TB for the standard 6 months if drug-susceptible. Always treat the patient with an HIV physician and a TB physician together. [1]
TB and TNF inhibitors
Anti-TNF therapy (infliximab, adalimumab, etanercept) increases reactivation risk several-fold. Screen all patients for LTBI with a TST or IGRA and a chest radiograph before starting anti-TNF therapy, and treat LTBI before or concurrent with the biologic. Use isoniazid for 6 to 9 months or rifampicin for 4 months. The same applies before other significant immunosuppression (transplant, chemotherapy, high-dose corticosteroids for more than 2 to 4 weeks, anti-CD20 therapy). [1]
TB in pregnancy
Untreated TB is dangerous to mother and fetus; treat drug-susceptible pulmonary TB in pregnancy with the standard RIPE regimen — all four drugs are considered safe in pregnancy. Pyridoxine is mandatory because of increased neuropathy risk. Streptomycin is avoided (ototoxicity in the fetus). Breastfeeding is safe; the small amounts of anti-TB drugs in breast milk are not clinically significant. [1]
Childhood TB
Children, especially under 5, are more likely to progress rapidly from infection to disease and to develop severe forms (miliary, TBM). Paediatric dosing is weight-based; the continuation phase is 4 months as in adults. Children are often paucibacillary — smear and culture yields are lower — and diagnosis frequently rests on contact history, TST/IGRA and radiograph. Gastric aspirates early morning on 2 to 3 consecutive days, or induced sputum, improve yield. [1]
Infection control, BCG and screening
Airborne isolation
A patient with suspected or confirmed pulmonary or laryngeal TB is placed in a single negative-pressure ventilation room (at least 6 to 12 air changes per hour, air exhausted outside or HEPA-filtered) with the door closed. Healthcare workers and visitors wear a fit-tested particulate respirator (N95, P2 or FFP2/3) — a surgical mask is inadequate protection against droplet nuclei. The patient wears a surgical mask when leaving the room (for procedures or transfer). Airborne precautions are continued until the patient is on effective therapy, clinically improving, and has had three consecutive negative sputum smears (on separate days, including one early morning) — typically 2 to 3 weeks for drug-susceptible disease. Drug-resistant TB may require isolation for the full course if treated as an inpatient. [1]
BCG vaccine
Bacillus Calmette-Guerin is a live attenuated strain of M. bovis. It protects against disseminated and meningeal TB in children (especially under 5) but provides variable and incomplete protection against adult pulmonary TB. In ANZ and the UK, BCG is targeted to neonates at increased risk (Aboriginal and Torres Strait Islander babies, babies with family from high-burden countries, neonates in high-burden communities) and to tuberculin-negative healthcare workers and laboratory staff with high exposure. It is contraindicated in primary immunodeficiency, symptomatic HIV, and pregnancy. Because it can cause a false-positive TST, IGRA is preferred for LTBI screening in BCG-vaccinated people. [1]
Screening
- Migrants — pre-migration chest radiograph or screening in high-burden source countries; post-arrival IGRA or TST in many ANZ and UK programmes, especially for high-yield groups.
- Healthcare workers — baseline IGRA (preferred) or two-step TST; serial testing only in high-risk roles.
- Contacts — concentric (stone-on-stone) contact investigation starting with the highest-exposure close contacts; symptom screen, IGRA or TST (8 to 10 weeks post-exposure), and chest radiograph.
- Immunosuppressed — all patients before anti-TNF, transplant, or significant immunosuppression. [1]
Long-case integration — the TB patient with comorbidity
A classic FRACP long case is a 58-year-old man born in Vietnam, with type 2 diabetes and chronic kidney disease stage 4, presenting with 6 weeks of cough, weight loss, night sweats and haemoptysis. Chest radiograph shows right upper lobe cavity with surrounding infiltrate. Sputum Xpert MTB/RIF positive, rifampicin susceptible. He is on warfarin for atrial fibrillation and a sulfonylurea for diabetes. [1]
The problem list is:
- Drug-susceptible pulmonary TB — start standard RIPE for 6 months; notify public health; airborne isolation until non-infectious.
- Rifampicin-warfarin interaction — anticipate a marked fall in INR; switch to low-molecular-weight heparin during therapy or increase warfarin dose substantially and monitor INR twice weekly.
- Rifampicin-sulfonylurea interaction — monitor glucose; may need dose adjustment or insulin.
- Diabetes control — TB worsens glycaemia; rifampicin affects oral hypoglycaemic metabolism; treat with insulin in the acute phase.
- Chronic kidney disease — adjust ethambutol and pyrazinamide dosing; nephrology liaison; monitor renal function.
- Hepatitis B and C screening — co-infection increases hepatotoxicity; baseline serology.
- HIV testing — mandatory.
- Smoking cessation, nutrition, social work for housing and adherence support, and contact tracing. [1]
The integrated management plan addresses each problem with a named owner (TB physician, pharmacist, diabetes nurse, social worker) and a defined endpoint. The communication piece includes a culturally sensitive explanation of the diagnosis and the 6-month commitment, the risks of untreated TB to family, and the support structures available. A trainee who presents this problem list, integrates the drug interactions, and addresses the patient perspective will pass the long case comfortably. [1]
Short-case examination — cervical lymphadenopathy and chronic cough
The short-case instruction is "Examine this patient's respiratory system and cervical lymph nodes." The routine is: [1]
- Introduction, consent, exposure, position. Expose the patient to the waist, position at 45 degrees.
- End of bed — cachexia, breathlessness, accessory muscle use, oxygen.
- Hands — clubbing (chronic suppurative disease), peripheral stigmata of TB (rare; cachexia).
- Face and neck — oral candidiasis (HIV), cervical and supraclavicular lymphadenopathy (scrofula — matted, non-tender, often posterior triangle).
- Thorax — inspection for scars; palpation for chest expansion; percussion (dullness over consolidation, effusion); auscultation (apical crackles, bronchial breath sounds, wheeze, effusion signs).
- Back — spinal tenderness (Pott), sacral oedema.
- Abdomen — hepatosplenomegaly (miliary), ascites (abdominal TB). [1]
Presentation template: "Mr Lee is a cachectic 58-year-old man with no respiratory distress. There is finger clubbing and a 2 cm matted, non-tender mass in the right posterior triangle of the neck consistent with scrofula. Examination of the chest reveals reduced right upper lobe expansion, dullness to percussion and bronchial breath sounds with inspiratory crackles at the right apex. The remainder of the examination is unremarkable. My differential diagnosis is pulmonary tuberculosis with associated tuberculous lymphadenitis; I would also consider lung malignancy, atypical infection such as non-tuberculous mycobacterial disease, and lymphoma. My initial investigation is a sputum for AFB smear, GeneXpert MTB/RIF and culture, and a chest radiograph." [1]
Common exam traps and high-yield discriminators
- The Xpert-positive, rifampicin-resistant patient — never start RIPE. Refer to MDR-TB service and await phenotypic susceptibility.
- Ethambutol optic neuritis — baseline and monthly colour vision; stop immediately if visual change; the toxicity is often irreversible if missed.
- Pyridoxine for isoniazid — co-prescribe in pregnancy, HIV, chronic kidney disease, diabetes, alcohol use disorder, malnutrition, and the elderly to prevent peripheral neuropathy.
- Rifampicin and the OCP — additional barrier contraception for the duration of therapy; unplanned pregnancies are common.
- Rifampicin and warfarin/DOACs — anticipate and adjust; an unexpected rise in INR target or loss of anticoagulation is rifampicin.
- TB meningitis and ART — defer ART for at least 4 weeks; the usual "2 weeks" rule does not apply because of IRIS risk.
- TB and HIV with CD4 under 50 — start ART within 2 weeks of TB therapy.
- Three negative smears to leave isolation — on separate days, including one early-morning specimen.
- Cavitary disease with positive 2-month culture — extend treatment to 9 months to prevent relapse.
- LTBI treatment before active TB excluded — always perform a chest radiograph and symptom screen; single-drug therapy for active TB causes resistance.
- IGRA and TST diagnose latent infection, not active disease — a positive IGRA in a patient with active TB requires the full work-up, not LTBI therapy.
- BCG effect on TST — IGRA is preferred in BCG-vaccinated adults. [1]
References
- Nahid P, Dorman SE, Alipanah N, et al. Official ATS/CDC/IDSA Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis. 2016;63(7):e147-e195. PMID: 27516382.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official ATS/IDSA/CDC Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. 2017;64(2):e1-e33. PMID: 28052967.
- Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010;363(11):1005-1015. PMID: 20825313.
- Thwaites GE, Nguyen DB, Nguyen HD, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults. N Engl J Med. 2004;351(17):1741-1751. PMID: 15496623.
- Menzies D, Dion MJ, Rabinovitch B, et al. Adverse events with 4 months of rifampin therapy or 9 months of isoniazid therapy for latent tuberculosis infection. Ann Intern Med. 2008;149(10):689-697. PMID: 19017587.
- Menzies D, Adjobimey M, Ruslami R, et al. Four months of rifampin or nine months of isoniazid for latent tuberculosis in adults. N Engl J Med. 2018;379(5):440-453. PMID: 30067931.
- Conradie F, Diacon AH, Ngubane N, et al. Treatment of highly drug-resistant pulmonary tuberculosis. N Engl J Med. 2020;382(10):893-902. PMID: 32130813.
- Nunn AJ, Phillips PPJ, Meredith SK, et al. A trial of a shorter regimen for rifampin-resistant tuberculosis. N Engl J Med. 2019;380(13):1201-1214. PMID: 30865791.
- Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection. N Engl J Med. 2015;372(22):2127-2135. PMID: 26017823.
- Abubakar I, Drobniewski F, Southern J, et al. Prognostic value of interferon-gamma release assays and tuberculin skin test in predicting the development of active tuberculosis (UK PREDICT TB). Lancet Infect Dis. 2018;18(10):1077-1087. PMID: 30174209.
- Zumla A, George A, Sharma V, et al. WHO's 2013 global report on tuberculosis: successes, threats, and opportunities. Lancet. 2013;382(9907):1765-1767. PMID: 24269294. [1]
References
- [1]Nahid P, Dorman SE, Alipanah N, Barry PM, Brozek JL, Cattamanchi A, et al. Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis Clin Infect Dis, 2016.PMID 27516382
- [2]Lewinsohn DM, Leonard MK, LoBue PA, Cohn DL, Daley CL, Desmond E, et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children Clin Infect Dis, 2017.PMID 28052967
- [3]Boehme CC, Nabeta P, Hillemann D, Nicol MP, Shenai S, Krapp F, et al. Rapid molecular detection of tuberculosis and rifampin resistance N Engl J Med, 2010.PMID 20825313
- [4]Thwaites GE, Nguyen DB, Nguyen HD, Hoang TQ, Do TT, Nguyen TC, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults N Engl J Med, 2004.PMID 15496623
- [5]Menzies D, Dion MJ, Rabinovitch B, Mannix S, Brassard P, Schwartzman K. Adverse events with 4 months of rifampin therapy or 9 months of isoniazid therapy for latent tuberculosis infection: a randomized trial Ann Intern Med, 2008.PMID 19017587
- [6]Menzies D, Adjobimey M, Ruslami R, Trajman A, Sow O, Kim H, et al. Four Months of Rifampin or Nine Months of Isoniazid for Latent Tuberculosis in Adults N Engl J Med, 2018.PMID 30067931
- [7]Conradie F, Diacon AH, Ngubane N, Howell P, Everitt D, Crook AM, et al. Treatment of Highly Drug-Resistant Pulmonary Tuberculosis N Engl J Med, 2020.PMID 32130813
- [8]Nunn AJ, Phillips PPJ, Meredith SK, Chiang CY, Conradie F, Dalai D, et al. A Trial of a Shorter Regimen for Rifampin-Resistant Tuberculosis N Engl J Med, 2019.PMID 30865791
- [9]Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis infection N Engl J Med, 2015.PMID 26017823
- [10]Abubakar I, Drobniewski F, Southern J, Sitch AJ, Jackson C, Lipman M, et al. Prognostic value of interferon-γ release assays and tuberculin skin test in predicting the development of active tuberculosis (UK PREDICT TB): a prospective cohort study Lancet Infect Dis, 2018.PMID 30174209
- [11]Zumla A, George A, Sharma V, et al. WHO's 2013 global report on tuberculosis: successes, threats, and opportunities Lancet, 2013.PMID 24269294