Phys · infectious
Viral Hepatitis — Treatment and Surveillance (HBV, HCV, HDV)
Also known as hepatitis B · hepatitis C · hepatitis D · hepatitis E · HBV · HCV · HDV · chronic hepatitis B · tenofovir · entecavir · sofosbuvir · direct-acting antivirals · DAA · SVR · HBsAg · HCC surveillance · HBV reactivation
Consultant-physician-depth guide to chronic viral hepatitis from the infectious-diseases side — HBV serology interpretation, the four phases and treatment thresholds, tenofovir versus entecavir, reactivation prophylaxis in immunosuppression, HCC surveillance, HCV test-and-cure with pangenotypic DAAs, HDV and HEV, vaccination and pregnancy — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Viral Hepatitis — Treatment and Surveillance
The answer first
Chronic viral hepatitis is a topic of three disciplines at once: serology (what do the markers mean), antiviral therapy (who do I treat, with what, for how long), and surveillance (whose liver cancer risk outlives their virus). For the broad virological survey of all five hepatotropic viruses — HAV through HEV — see the hepatic companion topic; this page owns the infectious-diseases depth: interpreting serology, deciding and monitoring treatment, preventing reactivation, and curing HCV [1] [18]. Four rules carry most of the exam:
- Read the serology as a pattern, never as single markers. HBsAg tells you the virus is present; anti-HBc tells you there has been real infection; anti-HBs tells you immunity. The combination is the diagnosis — and vaccine immunity is isolated anti-HBs, never anti-HBc [1].
- Treat immune-active HBV; monitor immune-tolerant HBV; treat all cirrhosis with detectable DNA. The decision hinges on ALT, HBV DNA and fibrosis stage — not on how the patient feels. First-line therapy is tenofovir or entecavir, chosen for their high resistance barrier, and for most patients it is indefinite suppression, not cure [1] [2].
- Every immunosuppressed patient gets screened before, not rescued after. HBsAg and anti-HBc before chemotherapy, anti-CD20 antibodies, HSCT or high-dose steroids — reactivation is common, occasionally fulminant, and almost entirely preventable with prophylactic antivirals [9] [10].
- HCV is now a cure. Test with RNA, treat essentially everyone with a pangenotypic DAA for 8–12 weeks, and confirm SVR12. But cure is not the end of the story: cirrhosis keeps its HCC surveillance for life [16] [18].
Reading HBV serology — the grid examiners demand
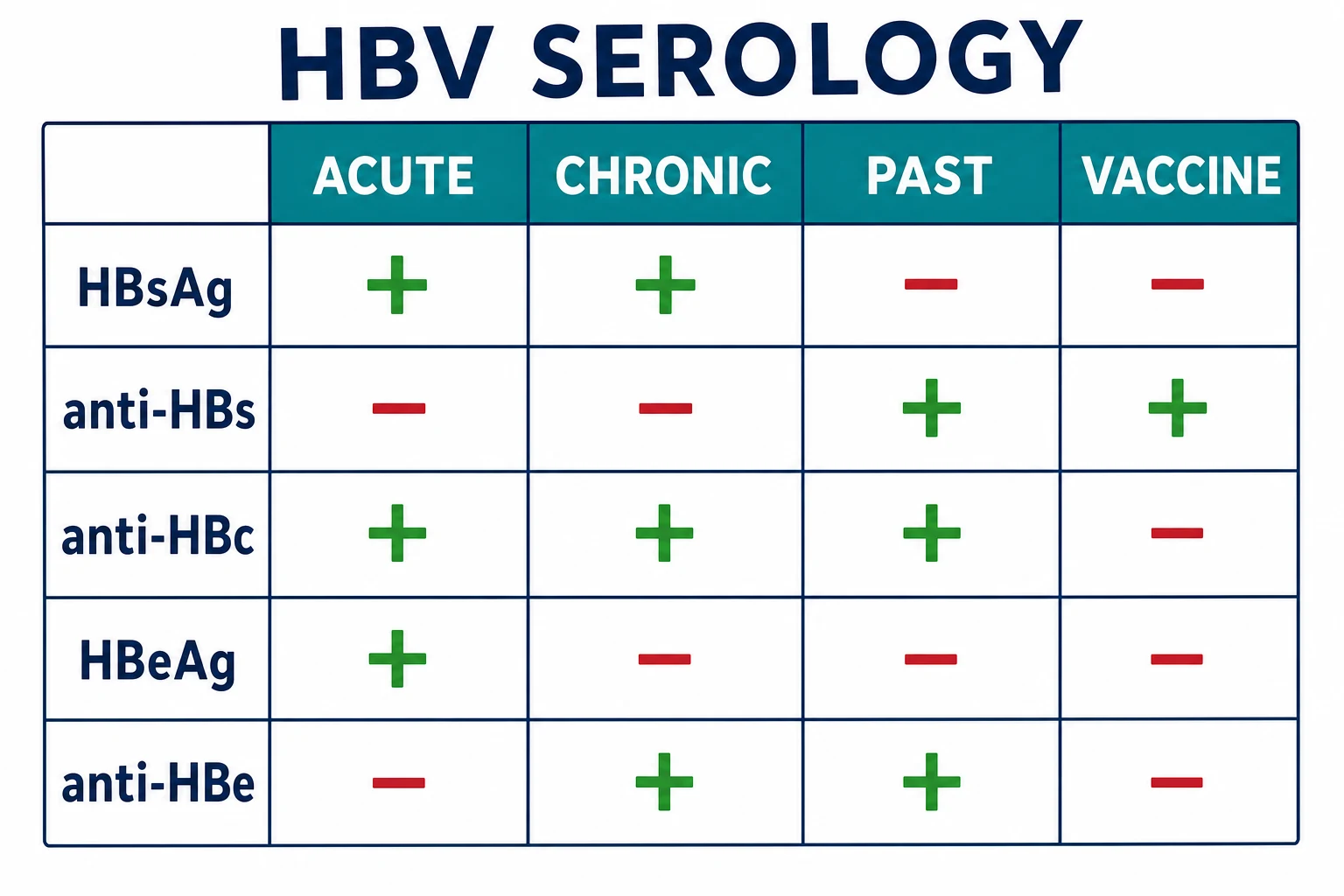
Serology questions are free marks if you think in patterns. The logic: HBsAg is the viral surface coat in the blood — its presence means current infection. Anti-HBc (total, including IgG) appears only after real, whole-virus infection — it is the scar of having met the virus, and it persists for life. Anti-HBs is the neutralising antibody — immunity, from recovery or from vaccine. HBeAg and anti-HBe track replicative activity within chronic infection [1] [3].
| Pattern | HBsAg | Anti-HBs | Total anti-HBc | IgM anti-HBc | HBeAg / anti-HBe | Interpretation |
|---|---|---|---|---|---|---|
| Acute infection | + | − | + | + (high titre) | HBeAg + | Recent infection; IgM anti-HBc is the discriminator [1] |
| Window period | − | − | + | + | Variable | HBsAg cleared, anti-HBs not yet up — rare but classic |
| Chronic infection | + (beyond 6 months) | − | + | − (or low) | HBeAg + or anti-HBe + | Persistence; HBeAg status defines the phase [3] |
| Resolved (past) infection | − | + | + | − | Usually anti-HBe + | Natural immunity — anti-HBc distinguishes it from vaccine |
| Vaccinated | − | + | − | − | − | Vaccine contains HBsAg only — anti-HBc can never appear [12] |
| Isolated anti-HBc | − | − | + | − | − | Not a diagnosis — a workup (see below) |
HCV serology is simpler but has its own trap: anti-HCV is an exposure marker, not an infection marker. About a quarter of acutely infected people clear HCV spontaneously, so an anti-HCV-positive patient may have current infection, past resolved infection, or a false positive — only HCV RNA distinguishes them, and RNA is therefore the mandatory second step of every positive antibody [18]. The same RNA-first logic applies before treatment, and SVR is judged on RNA, never on antibody, which remains positive for life after cure [19].
The four phases of chronic HBV — natural history as a clinical tool
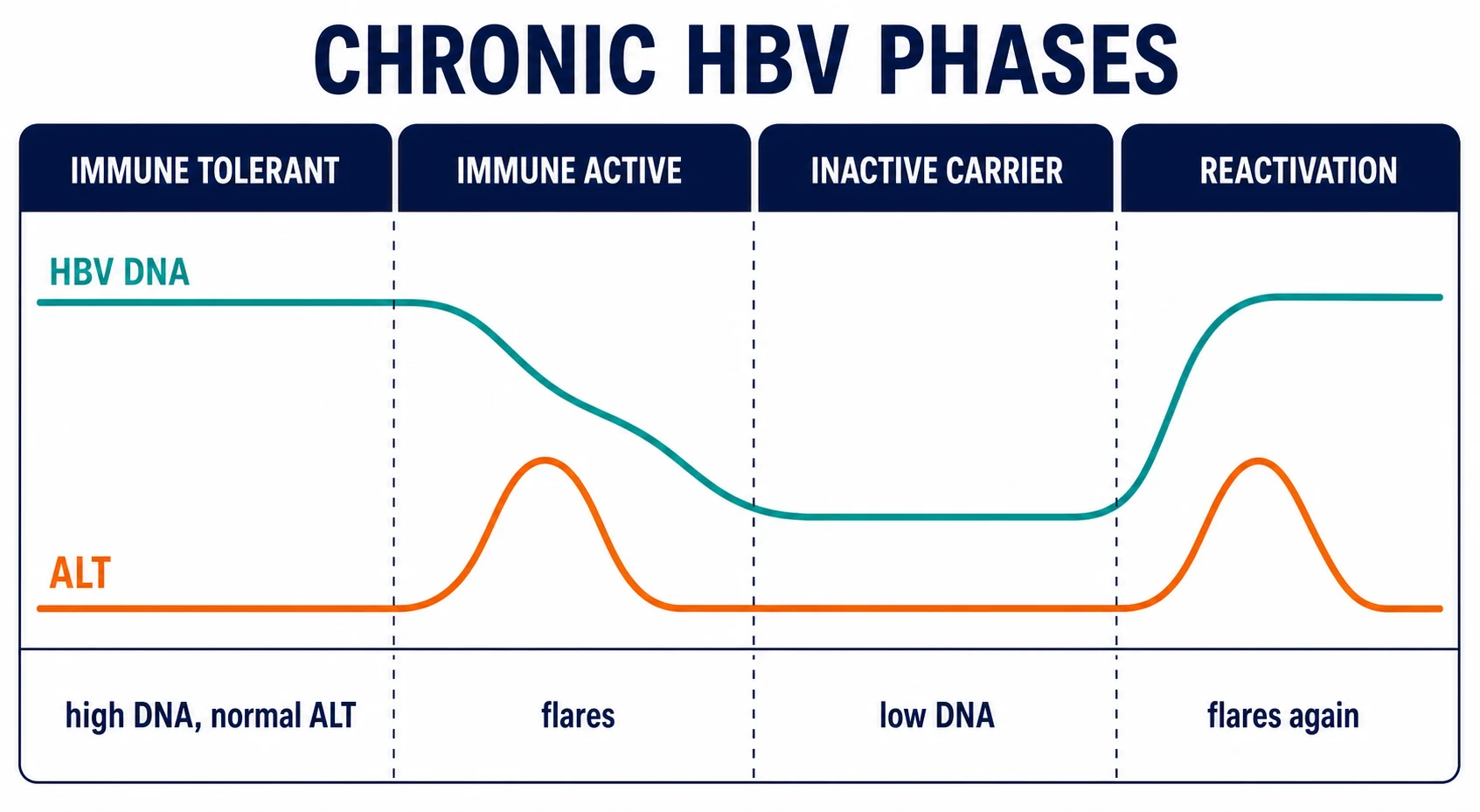
Chronic HBV is not a steady state but a decades-long negotiation between virus and host immunity, and the phase defines the management [3] [2]. Two framing facts first: age at acquisition determines chronicity — perinatal infection becomes chronic in about 90% of cases, adult-acquired in about 5% — which is why the chronic HBV clinic is dominated by people born in endemic regions; and liver injury in HBV is immune-mediated, not cytopathic — the virus does not kill hepatocytes, the immune response to it does, which explains why the highest viral loads coexist with the healthiest livers [3].
| Phase | HBeAg | HBV DNA | ALT | Liver injury | Management posture |
|---|---|---|---|---|---|
| Immune tolerant | + | Very high (often millions of IU/mL) | Normal | Minimal | Monitor — treatment is generally withheld [1] |
| Immune active (HBeAg-positive) | + | High, fluctuating | Elevated, flares | Progressive | Treat when thresholds met [1] |
| Inactive carrier | − (anti-HBe +) | Low (below 2,000 IU/mL) | Normal | Quiescent | Monitor 6–12 monthly; watch for reactivation |
| Reactivation (HBeAg-negative chronic hepatitis) | − (anti-HBe +) | Rising again (above 2,000 IU/mL) | Elevated | Progressive | Treat — precore/core-promoter variants escape immune control [2] |
The trap is that phases are not a one-way escalator: patients move between immune-active and inactive states, sometimes repeatedly, and a single normal ALT means nothing. "Fluctuating ALT" in an HBeAg-positive patient is the sound of the immune system intermittently attacking infected hepatocytes — it is the signature of immune-active disease and the classic long-case presentation [3].
A precision point for the viva: the inactive carrier label requires serial confirmation — HBeAg negative, anti-HBe positive, DNA persistently below 2,000 IU/mL and ALT normal on repeated testing over at least a year — because HBeAg-negative chronic hepatitis can masquerade as inactivity between flares. One normal ALT does not make a carrier [2].
Who to treat — the HBV treatment thresholds
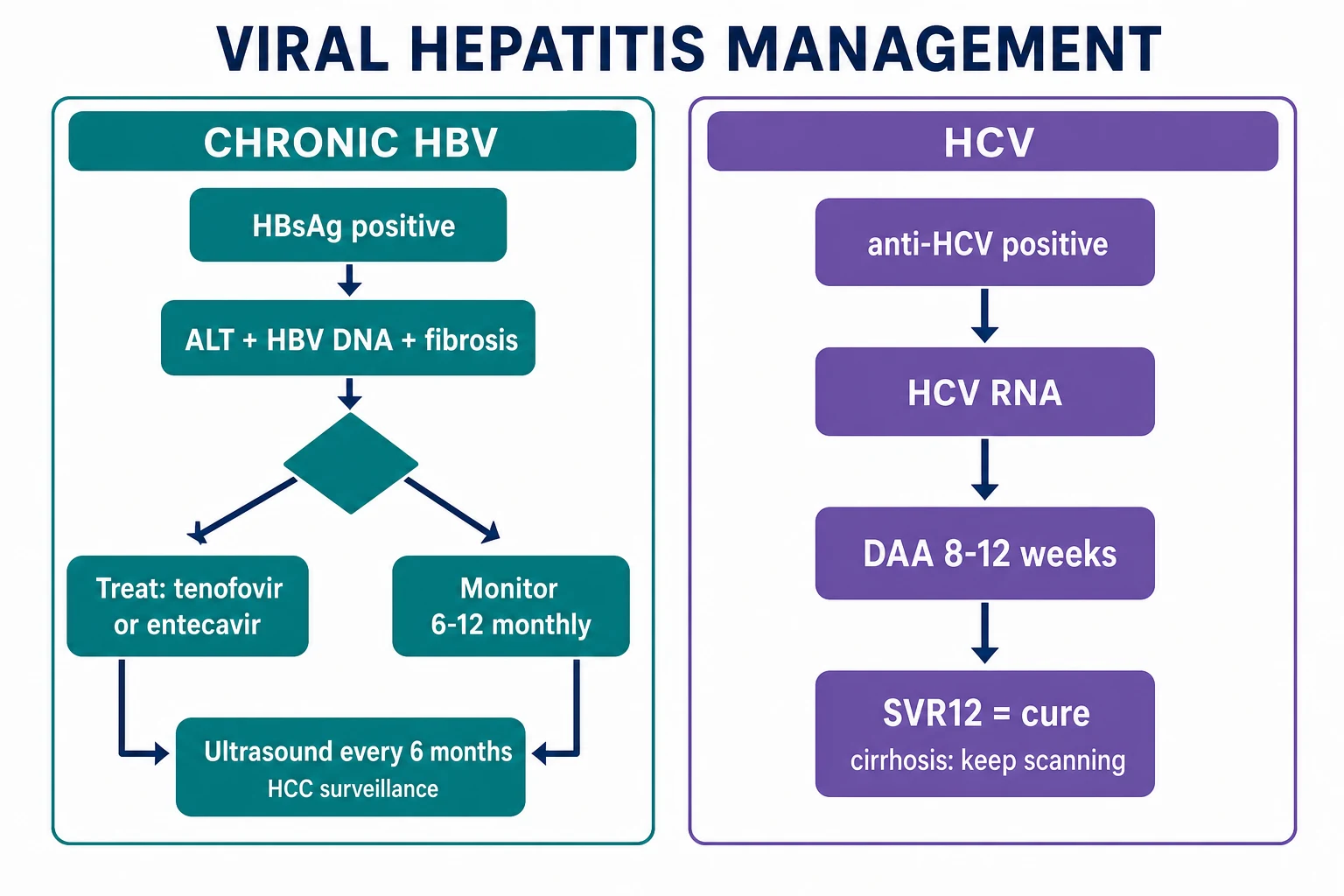
The treatment decision in chronic HBV is made on three axes — ALT, HBV DNA, and fibrosis stage — and the goal is to suppress viral replication before the immune war scars the liver into cirrhosis [1]. The AASLD 2018 guidance anchors the numbers every examiner expects [1]:
AASLD treatment thresholds, committed to memory
The cirrhosis rule overrides everything: any patient with cirrhosis and detectable viraemia should be on antivirals, because suppression reduces decompensation and HCC risk, and long-term tenofovir therapy has been shown to regress fibrosis and even reverse cirrhosis on serial biopsy in the majority of treated patients [1] [8]. EASL is more aggressive still, treating cirrhosis at any detectable DNA and lowering the ALT bar for older patients and those with family histories of HCC [2].
The grey zone is where vivas are won: HBeAg-negative disease with DNA hovering at 2,000–20,000 IU/mL and ALT borderline elevated. Here the fibrosis assessment decides — transient elastography (or APRI/FIB-4 where elastography is unavailable), with biopsy reserved for genuine discordance. Significant fibrosis tips the decision to treatment; the alternative is structured 3-monthly monitoring, not discharge [2].
The treatment-decision sequence for a newly referred HBsAg-positive patient
Confirm chronicity and phase
HBsAg beyond 6 months; HBeAg/anti-HBe; HBV DNA; ALT on at least two occasions
Stage the liver
Transient elastography or APRI/FIB-4; ultrasound for cirrhosis features and baseline HCC screen; AFP per local practice
Screen the stablemates
HDV antibody (every HBsAg-positive patient), HCV antibody, HIV — coinfections change the plan
Decide treat versus monitor
Apply the ALT/DNA/fibrosis thresholds; document the phase assignment and the rationale
Choose the agent and baseline safety tests
Tenofovir (DF or AF) or entecavir; creatinine, phosphate, bone and renal risk review before tenofovir DF
Set the surveillance frame
On-treatment monitoring cadence; HCC surveillance enrolment for cirrhosis and risk groups; vaccination of contacts
Household and sexual contacts of every chronic carrier should be tested and vaccinated if susceptible — the consult is not complete until the family is protected, and in the exam this single sentence signals a physician rather than a prescriber [12].
First-line therapy — tenofovir and entecavir
The modern first-line agents share one property that defines them: a high barrier to resistance. Tenofovir disoproxil fumarate (TDF 300 mg daily), tenofovir alafenamide (TAF 25 mg daily) and entecavir (0.5 mg daily in nucleoside-naive patients) all suppress HBV DNA profoundly, and on-treatment resistance in naive patients is negligible — the exact opposite of lamivudine, whose resistance rate made it obsolete as monotherapy [1] [4].
| Agent | Dose (naive) | Strengths | Watch-points | Choose when |
|---|---|---|---|---|
| TDF (tenofovir disoproxil) | 300 mg daily | Potent; pregnancy data strongest; cheapest | Proximal tubulopathy (Fanconi), bone density loss — check creatinine and phosphate; avoid in CKD and osteoporosis [7] | Pregnancy and most straightforward patients with good renal function |
| TAF (tenofovir alafenamide) | 25 mg daily | Non-inferior efficacy with improved renal and bone safety markers in phase 3 trials [7] | Less long-term pregnancy data than TDF; lipids rise slightly | Renal impairment, bone disease, older patients, long treatment horizon |
| Entecavir | 0.5 mg daily (1 mg daily if lamivudine-experienced) | Potent, well tolerated, no renal signal | Resistance climbs in lamivudine-refractory patients — hence the doubled dose and the preference for tenofovir there [6] | Renal or bone concerns without pregnancy plans; decompensated cirrhosis (with specialist care) |
The evidence behind the choices, in the order examiners quote it [4] [5]:
- Marcellin 2008 (TDF vs adefovir): tenofovir DF produced far higher rates of complete viral suppression than adefovir across HBeAg-positive and -negative disease — the trial that made tenofovir first line [4].
- Chang 2006 (entecavir vs lamivudine): entecavir beat lamivudine on histological, virological and biochemical endpoints in HBeAg-positive chronic hepatitis — the trial that retired lamivudine [5].
- Sherman 2006 (lamivudine-refractory): entecavir still works after lamivudine failure but with reduced potency and a resistance price — the origin of the 1 mg dose in this group and the modern preference for tenofovir when there is any lamivudine history [6].
- Buti 2016 (TAF vs TDF): tenofovir alafenamide was non-inferior for viral suppression with significantly smaller declines in renal function and bone mineral density — the rationale for TAF in kidneys and bones that matter [7].
Pegylated interferon survives as a finite option — 48 weeks, once weekly — for a narrow band of patients: young, HBeAg-positive, high ALT, low-ish DNA, genotype A or B, who want a defined course and can tolerate the toxicity. The Lau 2005 trial established the peginterferon alfa-2a response benchmark, and the candidacy checklist matters more in the exam than the drug itself [26].
HBV reactivation in immunosuppression — the preventable disaster
The AGA technical review stratifies by agent and serology [9]:
| Risk tier | Examples | HBsAg-positive | HBsAg-negative / anti-HBc-positive (resolved) |
|---|---|---|---|
| High (above 10%) | Anti-CD20 (rituximab, obinutuzumab), anthracyclines, HSCT, high-dose steroids (20 mg or more of prednisolone-equivalent for 4 weeks or more) | Prophylactic antiviral — start before or at cycle 1, continue 6–12 months after (12 months for anti-CD20) | Prophylaxis preferred for anti-CD20; monitor-and-treat is the minimum elsewhere [9] [10] |
| Moderate (1–10%) | TNF inhibitors, many TKIs, moderate-dose steroids, most solid-tumour chemotherapy | Prophylaxis generally recommended | Serial HBsAg/DNA monitoring with pre-emptive therapy is reasonable [9] |
| Low (below 1%) | Methotrexate, azathioprine, low-dose steroids, intra-articular steroids | Monitoring acceptable | Monitoring |
Two physician-level nuances [10]: first, prophylaxis beats pre-emptive rescue in high-risk settings — waiting for the DNA to rise before treating leaves a window in which hepatitis declares; entecavir or tenofovir are the prophylactic agents (never lamivudine, given resistance). Second, the HBsAg-negative, anti-HBc-positive patient is not safe: rituximab in particular can deplete the B-cell compartment that keeps occult virus suppressed, and reactivation of resolved HBV — reverse seroconversion — is well documented, which is why anti-CD20 therapy in this group still earns prophylaxis [10] [13].
HCC surveillance — whose liver cancer risk outlives the virus
Hepatitis B is directly oncogenic — HBV DNA integrates into hepatocyte genomes — so HCC risk exists even without cirrhosis, and it persists, attenuated but real, despite effective antiviral suppression [14]. The evidence that surveillance works is the Zhang randomised trial: six-monthly ultrasound plus AFP in a high-risk Chinese population reduced HCC mortality by 37% through earlier detection [15].
Who enters 6-monthly ultrasound (with or without AFP, per local practice) — the AASLD list, which the DWE expects verbatim [14]:
- All patients with cirrhosis — HBV, HCV (including after SVR), or any cause.
- Non-cirrhotic chronic HBV in defined risk groups: Asian men from about age 40, Asian women from about age 50, people of African ancestry from about age 20, and anyone with a first-degree family history of HCC.
- Patients with advanced (bridging) fibrosis are commonly enrolled by extension, and post-SVR HCV patients with F3 fibrosis are individualised [14] [18].
HCV — test, treat, cure
Hepatitis C has been transformed from an interferon ordeal into one of medicine's cleanest cures, and the physician's job is now logistics and vigilance, not heroics: find the viraemic patient, stage the liver, pick a pangenotypic regimen, and confirm SVR [18].
The test-and-treat pathway
Screen
Anti-HCV in anyone with a risk history (injecting drug use ever, transfusions before the early 1990s, endemic-country birth, incarceration, dialysis, HIV) — and increasingly as once-off universal screening
Confirm viraemia
HCV RNA — antibody alone cannot distinguish current from cleared infection
Stage and screen
Fibrosis assessment (elastography/APRI), HBV and HIV coinfection screen, renal function, pregnancy status, medication review for interactions
Treat
Pangenotypic DAA — sofosbuvir/velpatasvir 12 weeks, or glecaprevir/pibrentasvir 8 weeks if non-cirrhotic — specialist input for decompensated cirrhosis, post-transplant or prior DAA failure
Prove cure
HCV RNA at 12 weeks post-treatment — SVR12
Set the aftercare
Cirrhosis: continue 6-monthly HCC ultrasound for life; counsel on reinfection for ongoing risk; address alcohol and metabolic cofactors
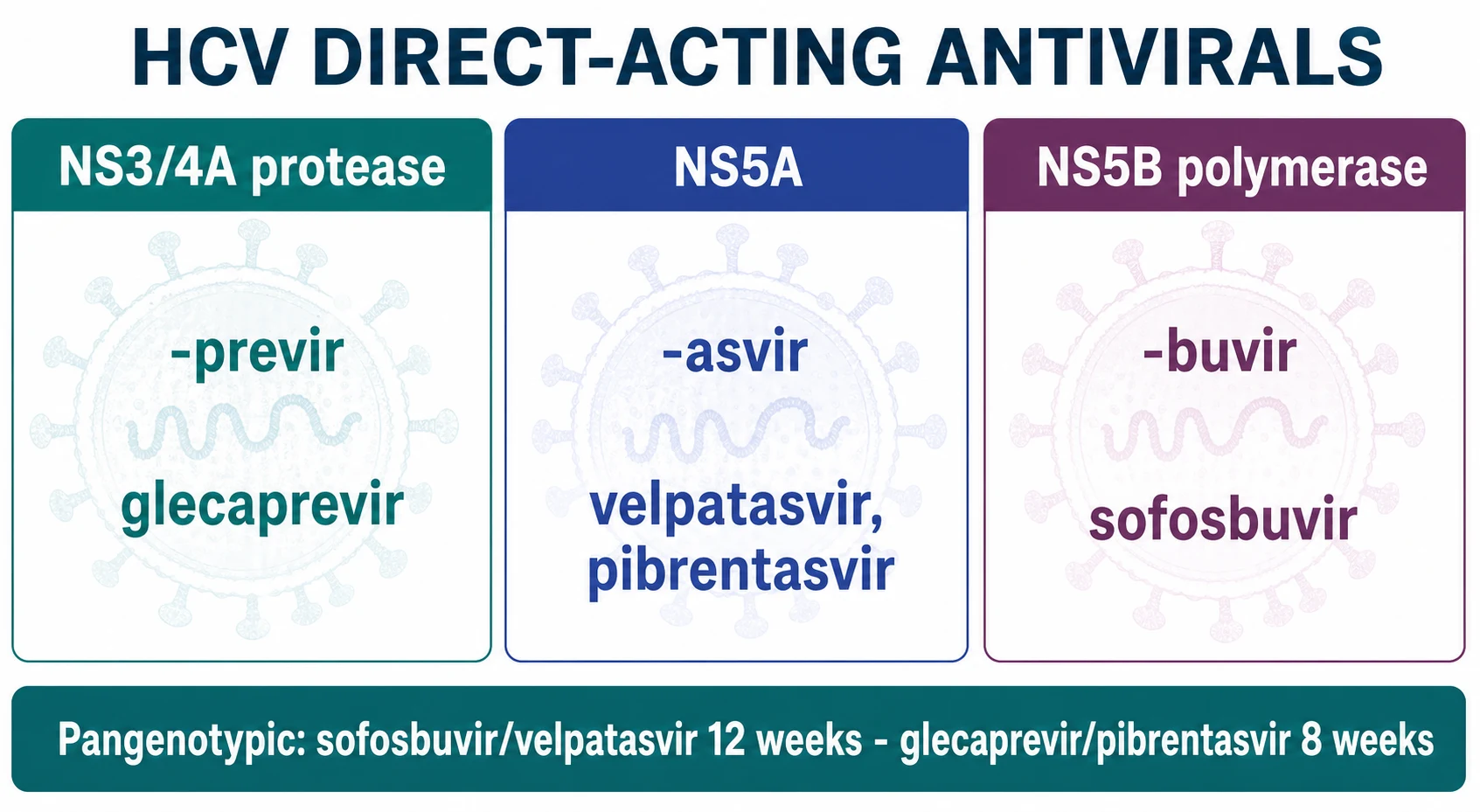
The two pangenotypic workhorses, with their pivotal trials [16] [17]:
| Regimen | Classes combined | Duration (treatment-naive) | Pivotal evidence | Notes |
|---|---|---|---|---|
| Sofosbuvir/velpatasvir | NS5B polymerase inhibitor (-buvir) + NS5A inhibitor (-asvir) | 12 weeks with or without compensated cirrhosis | ASTRAL-1: SVR12 of 99% across genotypes 1, 2, 4, 5, 6 [16] | Velpatasvir absorption falls with acid suppression — mind PPIs; avoid with strong P-gp inducers |
| Glecaprevir/pibrentasvir | NS3/4A protease inhibitor (-previr) + NS5A inhibitor | 8 weeks if non-cirrhotic; 12 weeks if compensated cirrhosis | ENDURANCE trials: SVR12 rates in the high 90s with the shortened course [17] | Contraindicated with strong CYP3A inducers and in decompensated cirrhosis (protease inhibitor class); taken with food |
The remaining subtleties, at guideline depth [18]: decompensated cirrhosis excludes protease-inhibitor regimens (glecaprevir/pibrentasvir is contraindicated) — sofosbuvir/velpatasvir for 24 weeks, or with ribavirin for 12 weeks, under specialist care; prior DAA failure earns retreatment with sofosbuvir/velpatasvir/voxilaprevir; people who inject drugs should be treated without a sobriety precondition — treatment-as-prevention is the backbone of elimination; and HBV coinfection screening precedes DAAs because HCV treatment can unmask HBV replication [18].
HDV — the parasite of hepatitis B
Hepatitis delta virus is a defective RNA virus that requires HBsAg to assemble and spread — it exists only in HBsAg-positive hosts, which makes every HBsAg-positive patient a candidate and every HDV diagnosis an HBV diagnosis first [20]. Two clinical patterns: coinfection (HBV and HDV acquired together, usually self-limited but with a higher fulminant rate than HBV alone) and superinfection (HDV landing on established chronic HBV — the dangerous one, with rapid progression to cirrhosis) [20].
The physician-level facts [20]:
- Screen every HBsAg-positive patient with anti-HDV at least once — and repeat when hepatitis is disproportionate to HBV DNA, when ALT flares in a suppressed patient, or with endemic exposure (Mediterranean, Middle East, Central Asia, parts of Africa and South America). Confirm with HDV RNA.
- Chronic HDV is the most aggressive chronic viral hepatitis — faster to cirrhosis and HCC than HBV alone — and suppressing HBV with nucleos(t)ides does nothing to HDV itself [20].
- Bulevirtide, an entry inhibitor blocking the NTCP receptor the viruses share, is the first specific therapy: the phase 3 trial showed combined virological and biochemical response at 48 weeks in about half of patients on 2 mg daily versus almost none untreated [21]. Availability varies by jurisdiction — in Australia and many regions it remains specialist-access or trial-based.
- Pegylated interferon for 48 weeks was the previous backbone; the HIDIT-1 trial showed sustained HDV RNA suppression in roughly a quarter of treated patients, with late relapses — it remains an option where bulevirtide is unavailable [22].
- Management belongs with a viral-hepatitis service; transplant-free survival, not eradication, is the realistic near-term goal [20].
HEV — two diseases in one virus
Hepatitis E is usually a self-limited acute hepatitis from contaminated water or undercooked pork and game, but it wears two faces the exam loves [23]:
- In pregnancy, genotype 1 HEV can produce fulminant hepatic failure with maternal mortality reported around a fifth of cases in endemic series — the reason jaundice in a pregnant traveller is an emergency, and a classic DWE discriminator against the benign "acute hepatitis, supportive care" answer [23].
- In the immunosuppressed — classically solid-organ transplant recipients — genotype 3 HEV becomes chronic: persistent RNA, quietly rising transaminases, and progressive fibrosis. The treatment sequence is evidence-based: first reduce immunosuppression where possible, then ribavirin; in the Kamar series of transplant recipients, about three-quarters achieved sustained clearance with a ribavirin course [24].
Prevention — vaccination, exposure management, elimination
Hepatitis B is vaccine-preventable, and the physician-level content is in the details [12]:
- Standard schedule is three doses (0, 1, 6 months) of recombinant vaccine; healthcare workers, dialysis patients, immunosuppressed patients and household contacts of carriers need post-vaccination anti-HBs testing — a level of 10 IU/L or more is protective [12].
- Non-responders (anti-HBs below 10 IU/L after a complete series): give a second complete series — about half respond — and consider higher-dose or adjuvanted formulations in dialysis and immunocompromised patients; document the status explicitly for occupational health [12].
- Post-exposure prophylaxis: a susceptible person with a needlestick or sexual exposure from an HBsAg-positive source gets HBIG plus the first vaccine dose, ideally within 24 hours; a non-responder with a completed second series gets HBIG. Know that the exposed healthcare worker question is answered with serology of BOTH parties, not guesswork [12].
- There is no HCV vaccine — prevention is harm reduction (needle-syringe programs, opioid agonist therapy), screening of risk groups, and treatment-as-prevention, the pillars of the WHO 2030 elimination targets that Australia has committed to [18].
Pregnancy — protecting the next generation
Chronic HBV in pregnancy is a two-part problem: the mother's liver, and the baby's lifetime risk. Without intervention, mothers with high-level viraemia transmit perinatally at high rates — and perinatal infection is precisely the kind that becomes chronic in about 90% of cases [11] [3].
The prevention sequence for an HBsAg-positive mother
Quantify in pregnancy
HBV DNA in the second trimester; ALT and fibrosis context; continue any pre-existing tenofovir (safe in pregnancy and breastfeeding)
Treat high viraemia
DNA above 200,000 IU/mL: start tenofovir DF in the third trimester (from about week 28–32) to slash transmission risk — the Pan trial showed markedly reduced mother-to-child transmission versus standard care
Immunise the neonate
HBIG plus the first vaccine dose within 12 hours of birth, then complete the series — over 90% protective even without maternal antivirals
Confirm the baby
Post-vaccination serology at 9–12 months: HBsAg and anti-HBs
Post-partum decisions
Tenofovir given purely for transmission prevention may be stopped after delivery with flare monitoring; breastfeeding on tenofovir is supported
HCV in pregnancy is different again: DAAs are not yet routine in pregnancy, so the plan is screen, quantify, defer treatment to post-partum, and test the infant (antibody testing is unhelpful before 18 months because of transplacental antibody — use RNA if early diagnosis is needed) [18].
Acute liver failure — when hepatitis becomes an emergency
Any of the hepatotropic viruses can tip into acute liver failure — coagulopathy (INR 1.5 or more) with hepatic encephalopathy in a patient without pre-existing cirrhosis — and the physician's contribution is recognition and transfer, not disease-specific therapy [25]. The viral patterns worth naming: acute HBV (including reactivation), HEV in pregnancy, HDV superinfection, and HAV in the elderly or those with chronic liver disease. Management is a transplant-centre conversation early: supportive care, N-acetylcysteine as in other aetiologies, cerebral-oedema vigilance, and listing before the window closes — antivirals (entecavir or tenofovir) are given for severe acute HBV, but they do not substitute for transfer [25] [1].
DCE angles — how this topic is examined live
The long case archetype: a 45-year-old, born overseas, with chronic HBV and "fluctuating ALT" referred from a screening program. The examiner's arc runs phase assignment (is this immune-active disease?), the treat-versus-watch defence (quote the ALT/DNA/fibrosis thresholds and own the grey zone), the surveillance frame (is he in the HCC program and is he actually attending?), and the human layer — stigma, family screening, vaccination of the household, adherence to an indefinite therapy for an asymptomatic disease [1] [14]. A second archetype: the cured-HCV patient with cirrhosis, testing whether you understand that SVR ended the virus but not the surveillance [18].
The short case is the abdominal examination for chronic liver disease stigmata — spider naevi, palmar erythema, gynaecomastia, parotid fullness, a firm liver edge, splenomegaly of portal hypertension, ascites — presented toward a synthesis: "chronic liver disease with portal hypertension, in a patient with treated chronic viral hepatitis, currently compensated" [14].
References
- [1]Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance Hepatology, 2018.PMID 29405329
- [2]European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection J Hepatol, 2017.PMID 28427875
- [3]Yim HJ, Lok AS. Natural history of chronic hepatitis B virus infection: what we knew in 1981 and what we know in 2005 Hepatology, 2006.PMID 16447285
- [4]Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B N Engl J Med, 2008.PMID 19052126
- [5]Chang TT, Gish RG, de Man R, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B N Engl J Med, 2006.PMID 16525137
- [6]Sherman M, Yurdaydin C, Sollano J, et al. Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronic hepatitis B Gastroenterology, 2006.PMID 16762627
- [7]Buti M, Gane E, Seto WK, et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of patients with HBeAg-negative chronic hepatitis B virus infection: a randomised, double-blind, phase 3, non-inferiority trial Lancet Gastroenterol Hepatol, 2016.PMID 28404092
- [8]Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study Lancet, 2013.PMID 23234725
- [9]Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy Gastroenterology, 2015.PMID 25447852
- [10]Loomba R, Liang TJ. Hepatitis B Reactivation Associated With Immune Suppressive and Biological Modifier Therapies: Current Concepts, Management Strategies, and Future Directions Gastroenterology, 2017.PMID 28219691
- [11]Pan CQ, Duan Z, Dai E, et al. Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load N Engl J Med, 2016.PMID 27305192
- [12]Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices MMWR Recomm Rep, 2018.PMID 29939980
- [13]Raimondo G, Locarnini S, Pollicino T, et al. Update of the statements on biology and clinical impact of occult hepatitis B virus infection J Hepatol, 2019.PMID 31004683
- [14]Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases Hepatology, 2018.PMID 29624699
- [15]Zhang BH, Yang BH, Tang ZY. Randomized controlled trial of screening for hepatocellular carcinoma J Cancer Res Clin Oncol, 2004.PMID 15042359
- [16]Feld JJ, Jacobson IM, Hezode C, et al. Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection N Engl J Med, 2015.PMID 26571066
- [17]Zeuzem S, Foster GR, Wang S, et al. Glecaprevir-Pibrentasvir for 8 or 12 Weeks in HCV Genotype 1 or 3 Infection N Engl J Med, 2018.PMID 29365309
- [18]European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series(☆) J Hepatol, 2020.PMID 32956768
- [19]Swain MG, Lai MY, Shiffman ML, et al. A sustained virologic response is durable in patients with chronic hepatitis C treated with peginterferon alfa-2a and ribavirin Gastroenterology, 2010.PMID 20637202
- [20]European Association for the Study of the Liver. EASL Clinical Practice Guidelines on hepatitis delta virus J Hepatol, 2023.PMID 37364791
- [21]Wedemeyer H, Aleman S, Brunetto MR, et al. A Phase 3, Randomized Trial of Bulevirtide in Chronic Hepatitis D N Engl J Med, 2023.PMID 37345876
- [22]Wedemeyer H, Yurdaydin C, Dalekos GN, et al. Peginterferon plus adefovir versus either drug alone for hepatitis delta N Engl J Med, 2011.PMID 21268724
- [23]European Association for the Study of the Liver. EASL Clinical Practice Guidelines on hepatitis E virus infection J Hepatol, 2018.PMID 29609832
- [24]Kamar N, Izopet J, Tripon S, et al. Ribavirin for chronic hepatitis E virus infection in transplant recipients N Engl J Med, 2014.PMID 24645943
- [25]Stravitz RT, Lee WM. Acute liver failure Lancet, 2019.PMID 31498101
- [26]Lau GK, Piratvisuth T, Luo KX, et al. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B N Engl J Med, 2005.PMID 15987917