Phys · infectious
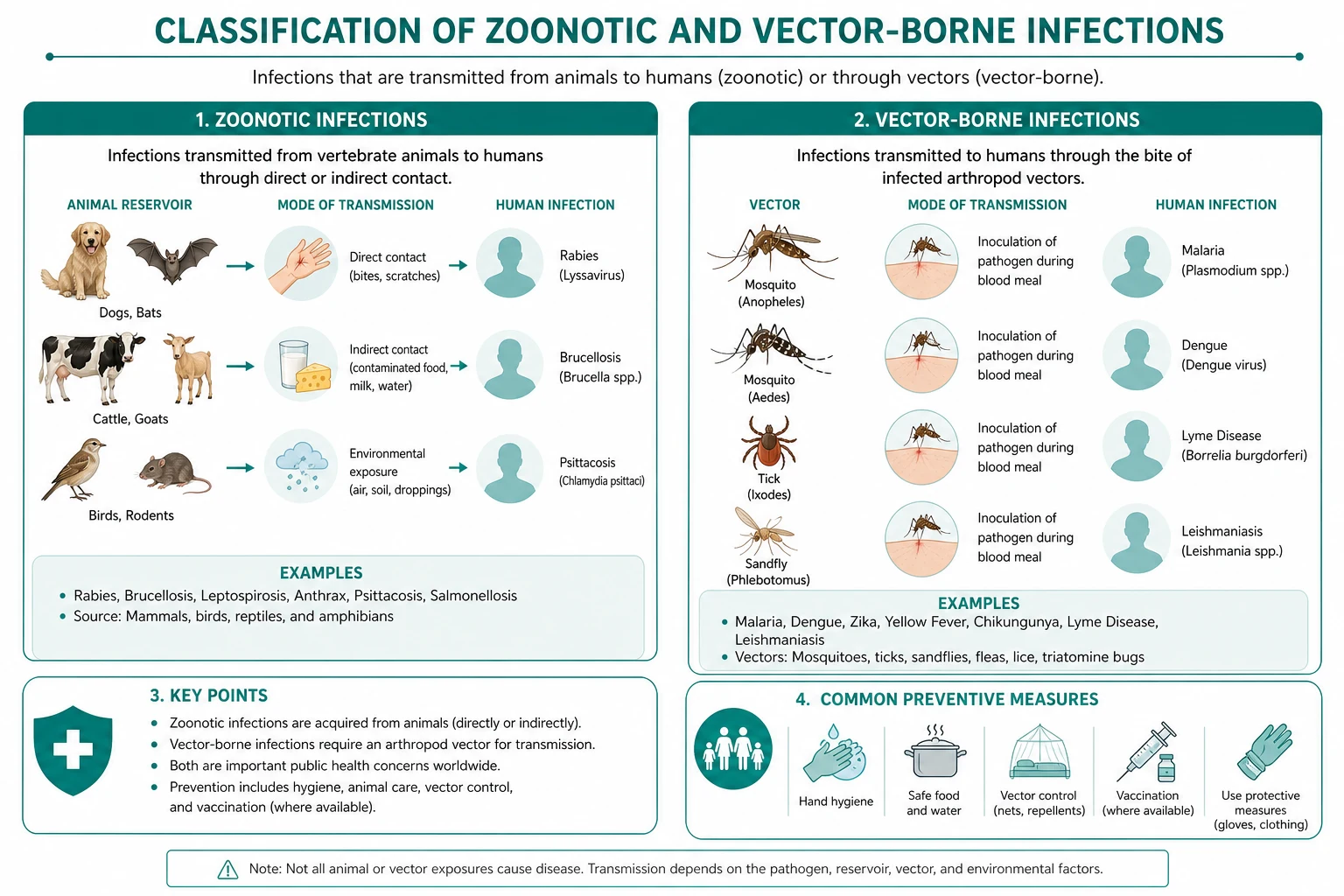
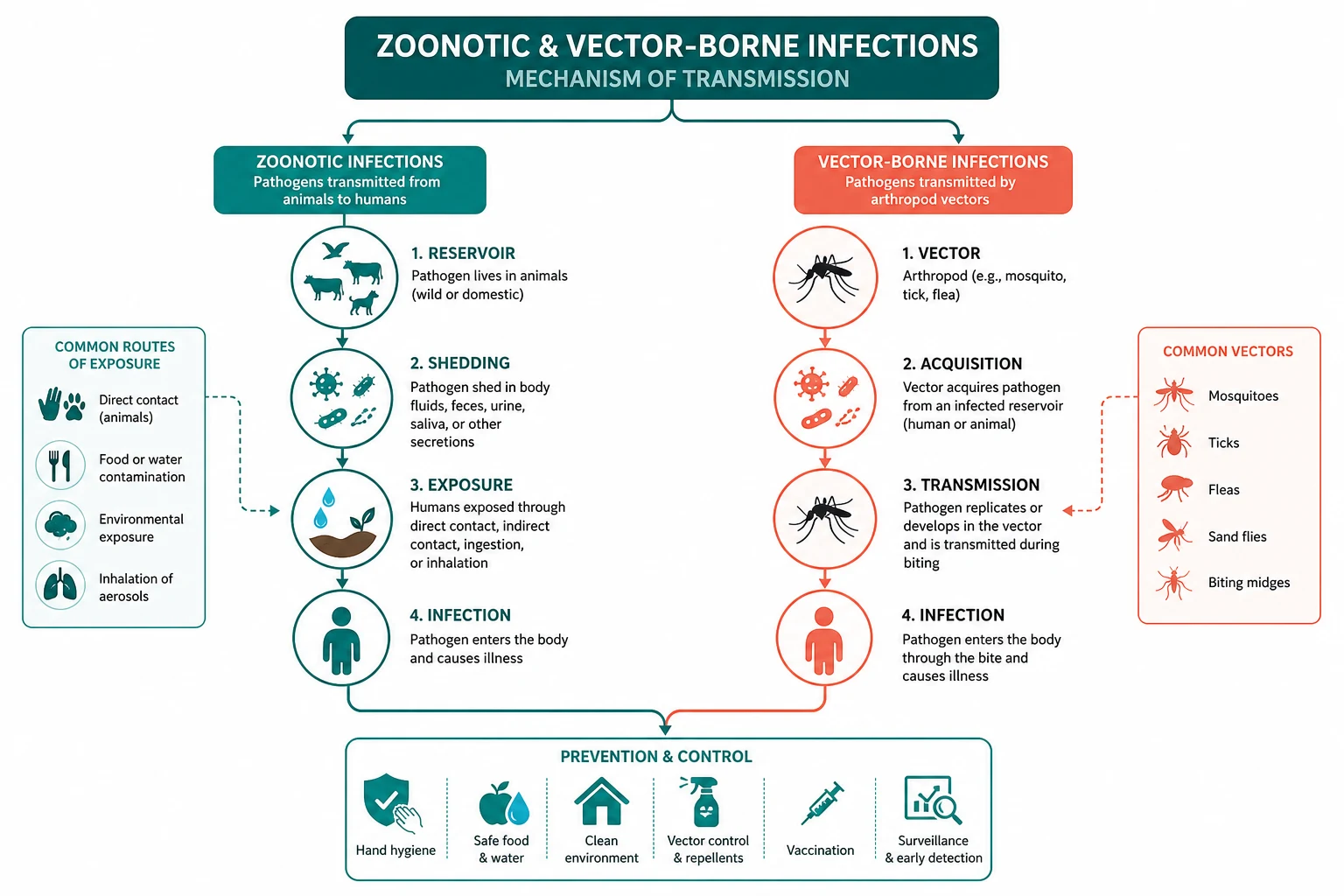
Zoonotic and Vector-Borne Infections
Also known as Q fever · Coxiella burnetii · query fever · leptospirosis · Weil disease · scrub typhus · Orientia tsutsugamushi · Queensland tick typhus · Rickettsia australis · spotted fever · brucellosis · undulant fever · cat-scratch disease · Bartonella henselae · bacillary angiomatosis · toxoplasmosis · Toxoplasma gondii · cerebral toxoplasmosis · hantavirus · hantavirus pulmonary syndrome · Lyme disease · Borrelia burgdorferi · erythema migrans · culture-negative endocarditis · Q-VAX vaccine
Consultant-physician-depth guide to the zoonotic and vector-borne infections relevant to ANZ and global practice — Q fever (Coxiella burnetii, phase I and II serology, doxycycline plus hydroxychloroquine for chronic endocarditis, Q-VAX vaccine), leptospirosis (biphasic illness, Weil disease, conjunctival suffusion, MAT serology, doxycycline and ceftriaxone), scrub typhus (eschar, Orientia tsutsugamushi, doxycycline, endemic in northern Australia), Queensland tick typhus (Rickettsia australis), brucellosis (undulant fever, doxycycline plus rifampicin for 6 weeks), Bartonella (cat-scratch disease, bacillary angiomatosis, culture-negative endocarditis), toxoplasmosis (cerebral toxoplasmosis in HIV, pyrimethamine-sulfadiazine-folinic acid), hantavirus (HFRS, pulmonary syndrome), Lyme disease (NOT endemic in Australia, imported only), and the ANZ-specific arboviruses — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Zoonotic and Vector-Borne Infections


The one-minute consultant answer
A zoonotic infection is suspected when the exposure history points to an animal or vector source — the occupation (abattoir worker, farmer, veterinarian), the recreation (hunting, freshwater swimming, bushwalking in northern Australia), the animal contact (cats, sheep, cattle, goats, rodents), the vector (tick, mite, flea), or the dietary history (unpasteurised dairy, undercooked meat). The single most important diagnostic step is therefore not the blood test but the exposure history — the registrar who takes it well will diagnose a zoonosis the laboratory has never heard of, while the registrar who does not will miss it. Once the exposure is identified, match it to the clinical syndrome — the eschar (scrub typhus, tick typhus), the undulant fever (brucellosis), the culture-negative endocarditis (Q fever, Bartonella), the biphasic illness with jaundice (leptospirosis), the ring-enhancing brain lesions in HIV (toxoplasmosis), the erythema migrans in a returned traveller (Lyme disease). [1]
The treatment decisions that examiners test are few and must be automatic. Acute Q fever gets doxycycline for 14 days; chronic Q fever endocarditis gets doxycycline plus hydroxychloroquine for at least 18 months — the hydroxychloroquine alkalinises the phagolysosome, restoring doxycycline bactericidal activity [1]. Leptospirosis gets doxycycline for mild disease and IV ceftriaxone for severe (Weil) disease [3]. Scrub typhus gets doxycycline, started empirically before serology returns; severe scrub typhus gets combination IV doxycycline plus azithromycin [4]. Brucellosis gets doxycycline plus rifampicin (or streptomycin) for at least 6 weeks — never monotherapy [6]. Cerebral toxoplasmosis gets pyrimethamine plus sulfadiazine plus folinic acid — not folic acid [8]. Lyme disease gets doxycycline or amoxicillin for erythema migrans, ceftriaxone for neuroborreliosis [9].
The ANZ-specific principle that examiners love: Lyme disease is NOT endemic in Australia. All locally-diagnosed "Lyme disease" in Australia is either imported (from the northern hemisphere) or mislabelled. A patient with a rash after a tick bite in Australia has a rickettsial disease (Rickettsia australis, Queensland tick typhus), not Lyme. This is a high-yield discriminator that separates the informed candidate from the one who has not studied the local epidemiology. [1]
The exposure-history framework — the discriminator that drives the differential

The exposure history is the single most powerful discriminator in a suspected zoonotic infection. It converts a non-specific febrile illness into a short, actionable differential. Ask explicitly and document the following five domains: [1]
First, what is the occupation? Abattoir workers and meat processors are at high risk of Q fever (inhalation of Coxiella-laden aerosols from sheep, cattle and goats), brucellosis (from infected animals) and occasionally leptospirosis. Farmers and agricultural workers are at risk of Q fever, leptospirosis (rodent and cattle urine), and brucellosis. Veterinarians and veterinary students are at risk of Q fever, cat-scratch disease (Bartonella henselae), and brucellosis. Sewer workers and those with freshwater occupational exposure are at risk of leptospirosis. Laboratory workers handling C. burnetii are at risk of laboratory-acquired Q fever. [1]
Second, what are the recreational exposures? Bushwalking, camping, and hiking in northern Australia and the Asia-Pacific exposes to scrub typhus (chigger mites in grass and scrub) and Queensland tick typhus (Rickettsia australis from tick bites in coastal eastern Australia). Freshwater swimming, rafting, and wading in the tropics exposes to leptospirosis. Rodent exposure (cleaning sheds, barns, rural cabins) exposes to hantavirus and leptospirosis. Hunting and game meat handling exposes to brucellosis and Q fever. [1]
Third, what is the animal contact? Cats are the reservoir for Bartonella henselae (cat-scratch disease) and Toxoplasma gondii (the cat is the definitive host, shedding oocysts in faeces). Sheep, cattle and goats are the classic reservoirs of Q fever — the organism reaches enormous concentrations in the placenta and birth fluids of parturient animals, and inhalation of a single organism can cause disease. Pigs, cattle, and dogs are reservoirs of leptospirosis. Rodents are reservoirs of leptospirosis and hantavirus. [1]
Fourth, what is the dietary history? Unpasteurised dairy products (milk, cheese) are the classic source of brucellosis (Brucella melitensis from goats and sheep, B. abortus from cattle) and can transmit Q fever and tick-borne encephalitis (from goat milk in endemic areas). Undercooked meat (especially pork, lamb, and venison) transmits toxoplasmosis. [1]
Fifth, what is the travel and vector history? Tick bites in the northern hemisphere expose to Lyme disease (Borrelia burgdorferi via Ixodes ticks) and various spotted fevers. Tick bites in eastern Australia expose to Rickettsia australis (Queensland tick typhus). Chigger bites in the tsutsugamushi triangle (from Japan and Korea through Southeast Asia to northern Australia and Pakistan) expose to scrub typhus. Flea bites transmit murine typhus (Rickettsia typhi) and cat-scratch disease (cat fleas transmit Bartonella henselae between cats). Mosquito bites in Australia transmit Ross River virus, Barmah Forest virus, Murray Valley encephalitis, Japanese encephalitis (in the north) and globally dengue, Zika, chikungunya, yellow fever. [1]
The exam trap: A patient with a tick bite in Australia who develops a rash does NOT have Lyme disease — Lyme is not endemic in Australia. The differential is rickettsial disease (Queensland tick typhus, Flinders Island spotted fever). Lyme disease must be considered only in returned travellers from endemic areas (north-eastern USA, northern and central Europe, parts of Asia). [1]
Q fever — Coxiella burnetii, the phagolysosome pathogen

Q fever is caused by Coxiella burnetii, a small Gram-negative obligate intracellular bacterium with a remarkable ability to survive in the hostile environment of the phagolysosome — the acidic, enzyme-rich compartment where most bacteria are killed. This is not a biological curiosity: it is the key to understanding why chronic Q fever requires a unique treatment regimen. The organism reaches enormous concentrations in the placenta and birth fluids of infected animals (cattle, sheep, goats, and cats), and the infectious dose is extraordinarily low — a single inhaled organism can cause disease. The organism is also remarkably stable in the environment, surviving for months in dust and soil. These properties make Q fever a classic inhalation zoonosis and a significant occupational disease in the meat and livestock industries. [1]
The phase I and phase II concept — the key to serological interpretation
C. burnetii undergoes antigenic phase variation of its lipopolysaccharide (LPS): [1]
- Phase I is the virulent form found in nature and in animals. It has a smooth (complete) LPS. High-titre IgG antibody to phase I antigen indicates chronic infection — a titre above 1:800 (or 1:1024, depending on the laboratory) is diagnostic of chronic Q fever.
- Phase II is the avirulent form that arises after repeated laboratory passage. It has a rough (truncated) LPS. IgM antibody to phase II antigen is the hallmark of acute Q fever. [1]
The single most common exam error is reversing these two. Memorise: phase II IgM equals acute; phase I IgG equals chronic. The serological pattern at baseline and on convalescent testing determines whether the patient has acute disease, chronic infection, or past exposure. [1]
Acute Q fever — the flu-like illness that hides endocarditis
Acute Q fever presents after an incubation period of 2 to 3 weeks (range 1 to 6 weeks) with one of three syndromes: [1]
- A self-limited influenza-like illness (the most common presentation): high fever, severe headache (often retro-orbital), myalgia, arthralgia, and sweats. The fever may be persistent or relapsing.
- Atypical pneumonia: cough, usually non-productive, with patchy infiltrates on chest X-ray. The pneumonia is usually mild and the CXR changes may be out of proportion to the clinical presentation.
- Granulomatous hepatitis: elevated transaminases (typically 2 to 4 times the upper limit of normal), with characteristic doughnut granulomas on liver biopsy (a central lipid vacuole surrounded by a fibrin ring and inflammatory cells). [1]
Less common presentations include myocarditis, pericarditis, meningoencephalitis, orchitis, and a transient maculopapular rash. The illness typically resolves within 1 to 2 weeks but may be prolonged. A proportion of patients develop Q fever fatigue syndrome — a post-infective fatigue syndrome characterised by disabling fatigue, arthralgia, myalgia and night sweats persisting for months to years, without evidence of active infection. [1]
Diagnosis is by serology — immunofluorescence antibody testing for phase I and phase II IgG and IgM. PCR on blood is positive in the first week (before antibodies develop) but becomes negative once seroconversion occurs. Blood cultures are negative — C. burnetii does not grow on routine media, and culture attempts require cell culture and are a biohazard (the laboratory must be notified before any specimen is submitted). [1]
Treatment of acute Q fever is doxycycline 100 mg orally twice daily for 14 days. In pregnancy, doxycycline is contraindicated; co-trimoxazole is used (with folate supplementation) to suppress the infection until delivery, followed by definitive treatment. All patients diagnosed with acute Q fever require serological follow-up — phase I and phase II serology at 3, 6, 12, and 18 months — to detect progression to chronic infection. [1]
Chronic Q fever — the endocarditis that cultures do not find
Chronic Q fever develops in approximately 1 to 5 per cent of patients after acute infection, typically presenting months to years later. The risk is markedly increased in patients with pre-existing valvular heart disease (including prosthetic valves, bicuspid aortic valve, rheumatic valve disease), immunocompromise, and pregnancy. The dominant manifestation is culture-negative endocarditis — classically involving a previously abnormal or prosthetic aortic or mitral valve. [1]
The clinical presentation of Q fever endocarditis is often insidious — low-grade fever, fatigue, weight loss, and the signs of chronic endocarditis (splenomegaly, anaemia, elevated ESR, microscopic haematuria). The classical peripheral stigmata of infective endocarditis (Osler nodes, Janeway lesions) may be absent. Echocardiography may show only small or no vegetations — the infection causes a fibrotic, nodular valvular lesion rather than the typical large friable vegetation of bacterial endocarditis. The modified Duke criteria specifically include Coxiella serology as a major criterion — phase I IgG above 1:800 satisfies the major serological criterion for the diagnosis of infective endocarditis. Any patient with culture-negative endocarditis must have Coxiella serology sent. [1]
Other manifestations of chronic Q fever include vascular infection (infected aneurysms, vascular graft infection), osteomyelitis, hepatitis, and chronic pulmonary infection. Pregnancy-associated chronic Q fever can cause placentitis, miscarriage, and stillbirth. [1]
Treatment of chronic Q fever endocarditis is doxycycline 100 mg twice daily plus hydroxychloroquine 200 mg three times daily. The hydroxychloroquine alkalinises the phagolysosome — the acidic environment protects C. burnetii from doxycycline, and raising the pH restores the bactericidal activity of the antibiotic. This combination, pioneered by Raoult and colleagues, achieved a significantly lower relapse rate than doxycycline plus ofloxacin and shortened the treatment duration [1]. The duration is at least 18 months for native valve endocarditis and at least 24 months for prosthetic valve endocarditis. Doxycycline plasma levels should be monitored (target above 5 micrograms per mL), and hydroxychloroquine requires baseline and annual ophthalmic review. Valve surgery is required for heart failure, perivalvular abscess, or prosthetic valve dehiscence, but must be accompanied by prolonged antibiotic therapy before and after surgery.
Q fever vaccine (Q-VAX) — the Australian innovation
The Q-VAX vaccine is a whole-cell, formalin-inactivated vaccine derived from the Henzerling strain of C. burnetii. It is licensed only in Australia and is the only licensed human Q fever vaccine in the world. Its efficacy is high — in abattoir outbreaks, it reduced Q fever incidence by greater than 83 per cent [2]. It is recommended for all at-risk occupational groups: abattoir workers, farmers, shearers, veterinarians, veterinary students, laboratory workers handling C. burnetii, kangaroo and wildlife shooters, and animal-hide workers.
The non-negotiable rule: Q-VAX must never be given without prior pre-vaccination screening. Individuals with pre-existing immunity (from a previous Q fever infection) develop severe local and systemic reactions if vaccinated — including large, painful injection-site reactions, prolonged fever, and systemic illness. Screening consists of both serology (Coxiella antibody testing) and skin testing (intradermal injection of diluted Q fever antigen, read at 7 days). The vaccine is contraindicated if either test is positive, and it is also contraindicated in pregnancy and in immunosuppression. [1]
The National Q Fever Management Program, implemented in Australia in 2001, was the world's first comprehensive Q fever vaccination programme for at-risk occupational groups. Vaccine failures do occur but are uncommon [10].
Leptospirosis — Weil disease and the biphasic course
Leptospirosis is a zoonotic spirochaetal infection caused by Leptospira species, acquired through contact with water or soil contaminated by the urine of infected animals — rodents, cattle, pigs, dogs, and horses. The organism penetrates intact mucous membranes (especially the conjunctiva) and abraded skin. Classic exposures are freshwater swimming or wading, farming, dairy work, sewer work, and flooding — the disease is particularly common in the wet tropics (including Queensland and the Pacific Islands) and in adventure travellers. [1]
Clinical presentation — the biphasic illness
Leptospirosis has a characteristic biphasic course, reflecting the transition from the leptospiraemic (infective) phase to the immune phase: [1]
The leptospiraemic phase (first week): sudden onset of high fever, severe headache (often frontal or retro-orbital), intense myalgia (especially in the calf muscles — a classic complaint), and conjunctival suffusion — the diffuse redness of the conjunctivae without purulent discharge, which is the single most specific bedside sign. The patient may also have nausea, vomiting, abdominal pain, and a pretibial rash. The fever settles after 4 to 7 days. [1]
The immune phase (second week): the fever may recur (the biphasic temperature curve), and the immune-mediated manifestations appear — aseptic meningitis (lymphocytic CSF pleocytosis), uveitis (which can recur months to years later), and a macular, maculopapular, or petechial rash. [1]
Severe leptospirosis (Weil disease) develops in approximately 5 to 10 per cent of cases and is the life-threatening form: jaundice (from hepatocellular dysfunction — the bilirubin is disproportionately elevated relative to transaminases, which are typically only mildly raised), acute kidney injury (tubulointerstitial nephritis, often with a non-oliguric pattern initially), and haemorrhage (petechiae, purpura, epistaxis, gastrointestinal bleeding, and the feared severe pulmonary haemorrhage syndrome, which is the major cause of death). Thrombocytopenia is common. A Jarisch-Herxheimer reaction (transient fever, rigors, hypotension) may occur after the first dose of antibiotic, particularly with penicillin. [1]
Diagnosis
IgM ELISA is the usual screening test, but IgM may be negative in the first week. The microscopic agglutination test (MAT) is the gold standard — it uses live leptospiral antigens and can identify the serovar, but it requires a reference laboratory and a panel of serovars. Because antibody rises only in the immune phase, a single early negative serology does not exclude leptospirosis — take an acute sample (first week) and a convalescent sample (2 weeks later) to demonstrate a fourfold or greater rise in titre. PCR on blood is useful in the first week (the leptospiraemic phase), and PCR on urine becomes positive in the second week and remains positive for weeks. Blood cultures are positive in the first week but require special media (Ellinghausen-McCullough-Johnson-Harris medium) and prolonged incubation (up to 4 months). [1]
Management
- Mild disease: doxycycline 100 mg orally twice daily for 7 days (alternatives: amoxicillin, or azithromycin in pregnancy).
- Severe disease (Weil disease): IV ceftriaxone 2 g daily for 7 days (alternatives: IV benzylpenicillin 1.5 million units every 6 hours) [3]. The systematic review evidence shows that antibiotics reduce the time to defervescence, but the evidence for a mortality benefit is limited. Supportive care is equally critical — renal replacement therapy for AKI, blood product support for haemorrhage, and ventilation for the severe pulmonary haemorrhage syndrome.
The exam trap: the jaundice of Weil disease is not primarily haemolytic and not primarily obstructive — it is hepatocellular dysfunction with disproportionate bilirubin elevation relative to the modest transaminase rise. A bilirubin of 300 with ALT of 80 should prompt the search for leptospirosis, not viral hepatitis. [1]
Rickettsial infections — the eschar and doxycycline

Rickettsial diseases are caused by obligate intracellular Gram-negative bacteria that multiply in endothelial cells, causing a vasculitis — this pathophysiology explains the clinical features: the rash (endothelial damage in skin capillaries), the eschar (necrosis at the inoculation site), the thrombocytopenia and hyponatraemia (capillary leak), and the multi-organ involvement. Three groups matter in ANZ practice: [1]
Scrub typhus — Orientia tsutsugamushi
Scrub typhus is the most important rickettsial disease in the ANZ and Asia-Pacific region. It is caused by Orientia tsutsugamushi (formerly classified in the Rickettsia genus, now separated based on genetic and structural differences) and transmitted by the larval stage of trombiculid mites (chiggers), especially Leptotrombidium deliense. The disease is endemic in the "tsutsugamushi triangle" — an area from Japan and Korea in the north, through Southeast Asia and Indonesia, to northern Australia and Pakistan in the west. In Australia, it occurs in Far North Queensland (especially between Ingham and Cooktown), the Northern Territory (Litchfield National Park and surroundings), and the Torres Strait Islands [5].
The classic presentation is fever, headache, myalgia, and an eschar — a black-crusted necrotic lesion with a surrounding red halo at the site of the chigger bite, classically found in warm, moist areas where clothing fits tightly (groin, axilla, popliteal fossa, scrotum, under the breasts, under a belt or bra strap). Regional lymphadenopathy and a maculopapular rash (which may involve the palms and soles) are common. However, the eschar is not universally present — its absence does not exclude scrub typhus. Hepatosplenomegaly and conjunctival injection may occur. [1]
Severe scrub typhus causes multi-organ dysfunction syndrome — ARDS, meningoencephalitis (with CSF lymphocytic pleocytosis and elevated protein), AKI, myocarditis, DIC, and shock. Untreated, the mortality is up to 30 per cent. The INTREST trial (2023) established that combination IV doxycycline plus azithromycin was superior to either alone for severe scrub typhus, with a composite outcome (death at day 28, persistent complications at day 7, or persistent fever at day 5) of 33 per cent with combination versus 47 per cent with doxycycline and 48 per cent with azithromycin monotherapy [4].
Treatment: doxycycline 100 mg orally twice daily for 7 days (or azithromycin 500 mg daily in pregnancy and in severe disease, with combination IV doxycycline plus azithromycin for severe disease per INTREST). The response is usually rapid (defervescence within 24 to 48 hours). [1]
Queensland tick typhus — Rickettsia australis
Rickettsia australis causes Queensland tick typhus (also called Australian spotted fever), endemic in the coastal regions of eastern Australia (Queensland and northern New South Wales). It is transmitted by the bite of the paralysis tick (Ixodes holocyclus) and other Ixodes species. The clinical presentation is similar to scrub typhus — fever, headache, myalgia, eschar at the tick bite site, regional lymphadenopathy, and a maculopapular rash that characteristically involves the palms and soles. The illness is generally milder than scrub typhus but can cause severe disease. Flinders Island spotted fever (Rickettsia honei) occurs on Flinders Island in Bass Strait and in eastern Australia, presenting a similar picture. [1]
Treatment: doxycycline 100 mg orally twice daily for 7 to 10 days, started empirically when the clinical picture is suggestive. [1]
The empiric treatment principle
The non-negotiable rule: start doxycycline empirically for any suspected rickettsial infection — do not wait for serology. Rickettsial serology requires paired acute and convalescent sera (a fourfold or greater rise in titre between acute and convalescent samples is diagnostic), and the result takes weeks. In the acute illness, the antibody titres have not yet risen. The indirect immunofluorescence antibody test (IFA) is the reference method for serological diagnosis; PCR and immunohistochemistry on skin biopsy of the eschar can provide a more rapid diagnosis in reference laboratories. The Weil-Felix test (proteus agglutination) is obsolete and should not be used. [1]
The reasoning is straightforward: untreated rickettsial disease has a significant mortality (up to 30 per cent for scrub typhus), doxycycline is safe and highly effective, and the defervescence within 24 to 48 hours of starting treatment provides retrospective clinical confirmation. A short course of doxycycline carries far less risk than the untreated disease. [1]
Brucellosis — the undulant fever
Brucellosis is caused by Brucella species — small Gram-negative intracellular coccobacilli. The species and their animal reservoirs are: B. melitensis (goats and sheep — the most virulent, acquired from unpasteurised dairy in the Mediterranean, Middle East, and Latin America), B. abortus (cattle — largely controlled in Australia through eradication programmes), B. suis (pigs — occurs in feral pigs in Queensland, a risk for hunters), and B. canis (dogs). Transmission is by ingestion of unpasteurised dairy products, by direct contact with infected animal tissues (occupational exposure in abattoir workers, veterinarians, hunters), or by inhalation of aerosols (a laboratory hazard). [1]
Clinical presentation — the great imitator
Brucellosis presents after an incubation period of 2 to 4 weeks (range 1 week to several months) with insidious onset of undulant fever — the classic temperature pattern is a fever that rises in the afternoon and evening and falls toward morning, persisting for weeks. Constitutional symptoms are prominent: drenching sweats (especially the malodorous sweat classic in brucellosis), fatigue, anorexia, weight loss, headache, arthralgia, and myalgia. Hepatosplenomegaly and lymphadenopathy are common. Focal disease develops in a significant proportion: [1]
- Osteoarticular disease is the most common focal manifestation — sacroiliitis, spondylitis (lumbar most common, with the "Pedro Pons sign" of paravertebral abscess formation), and peripheral arthritis.
- Genitourinary disease — epididymo-orchitis in men (a classic presentation); abortion in animals (Brucella is abortifacient, hence B. abortus), though human abortion is uncommon.
- Endocarditis — the most common cause of brucellosis-related death, usually involving the aortic valve.
- Neurobrucellosis — meningitis, encephalitis, cranial neuropathies, and polyradiculopathy. [1]
Diagnosis
Blood culture is the gold standard but requires prolonged incubation (the organism is slow-growing, and cultures should be held for at least 4 weeks). Importantly, the laboratory must be notified of the suspicion, because Brucella is a hazard group 3 pathogen and laboratory-acquired infection is well documented — culture work should be performed in a biological safety cabinet. Serology is the more commonly used diagnostic tool: the Rose Bengal test is a rapid screening test; the standard tube agglutination test (STAT) with a single titre above 1:160, or a fourfold rise in paired sera, supports the diagnosis. ELISA and immunoblot assays are also available. PCR on blood is increasingly used and has the advantage of species identification. [1]
Management
The principle is combination therapy for a prolonged duration — monotherapy has an unacceptable relapse rate (above 30 per cent): [1]
- Standard regimen: doxycycline 100 mg twice daily plus rifampicin 600 to 900 mg daily for 6 weeks [6].
- Preferred regimen (lower relapse rate): doxycycline 100 mg twice daily for 6 weeks plus streptomycin 1 g IM daily for the first 2 to 3 weeks. The Cochrane review confirmed that aminoglycoside-containing regimens have lower relapse rates than doxycycline plus rifampicin [6].
- Alternatives: doxycycline plus gentamicin (5 mg/kg daily for 7 days) is a practical alternative to streptomycin. TMP-SMX is used in pregnancy and in children (doxycycline and aminoglycosides are avoided). Complicated disease (spondylitis, endocarditis, neurobrucellosis) requires extended therapy (8 to 12 weeks or more) and often triple therapy.
The exam trap: brucellosis relapses because the organism is an intracellular pathogen of the reticuloendothelial system, surviving in macrophages. Relapse is due to inadequate treatment (monotherapy, too short a duration), not antimicrobial resistance. The registrar who treats brucellosis with a single agent for 2 weeks will see the patient return with recurrent fever. [1]
Bartonella — cat-scratch, bacillary angiomatosis, and culture-negative endocarditis
Bartonella henselae is a fastidious Gram-negative bacterium transmitted between cats by the cat flea (Ctenocephalides felis); cats are the reservoir and bacteraemic hosts. Humans acquire infection through cat scratches or bites (and rarely flea bites). The clinical spectrum depends on the immune status of the host: [1]
Cat-scratch disease (immunocompetent host)
The classic presentation is regional lymphadenopathy developing 1 to 3 weeks after a cat scratch, often preceded by a papule or pustule at the inoculation site. The lymphadenitis is typically in the draining lymph node of the scratch site — epitrochlear, axillary, or cervical. The node is tender, may suppurate, and persists for weeks to months. Systemic symptoms (fever, fatigue) are mild or absent in most patients. The disease is usually self-limiting (resolves over weeks to months) and symptomatic treatment suffices for most patients. Azithromycin may be considered for severe or persistent disease, or for patients with systemic symptoms or hepatosplenic involvement. [1]
Atypical presentations include Parinaud oculoglandular syndrome (granulomatous conjunctivitis with preauricular lymphadenopathy — from inoculation into the conjunctiva), neuroretinitis (Leber idiopathic stellate neuroretinitis — causing painless visual loss with a macular star on fundoscopy), encephalopathy, and hepatosplenic disease (granulomatous hepatitis and splenitis with microabscesses, in systemic cat-scratch disease). [1]
Bacillary angiomatosis (immunocompromised host)
In patients with advanced HIV (CD4 typically below 100) or other immunosuppression, B. henselae (and B. quintana) cause bacillary angiomatosis — a vascular proliferative disorder presenting as cutaneous lesions that resemble Kaposi sarcoma (red, purple, or skin-coloured papules, nodules, and angiomatous plaques). Visceral involvement causes peliosis hepatis (blood-filled cystic spaces in the liver) and bacillary splenitis. The histology shows lobular proliferation of capillaries with plump endothelial cells and neutrophilic debris. Treatment is erythromycin or doxycycline for at least 3 months. [1]
Culture-negative endocarditis
Bartonella species (B. quintana and B. henselae) are a leading cause of culture-negative endocarditis, particularly in homeless or alcoholic patients (B. quintana, transmitted by the human body louse) and in cat owners (B. henselae). The organism is fastidious and does not grow on routine blood cultures. Diagnosis requires serology (IgG by immunofluorescence, titre above 1:800 is suggestive) or PCR on resected valve tissue. Treatment is doxycycline plus gentamicin (or ceftriaxone) for at least 4 weeks, with valve replacement often required. Any patient with culture-negative endocarditis must have Bartonella serology sent alongside Coxiella serology. [1]
Toxoplasmosis — the cat, the meat, and the brain
Toxoplasma gondii is an obligate intracellular protozoan parasite. The cat is the definitive host — cats shed oocysts in their faeces, which sporulate and become infective in the environment. Humans acquire infection by ingesting oocysts (from cat litter, soil, or contaminated food) or tissue cysts (in undercooked meat — especially pork, lamb, and venison). The parasite disseminates haematogenously and forms tissue cysts (containing bradyzoites) in brain, skeletal muscle, cardiac muscle, and eye — these persist for the life of the host and are held in check by cell-mediated immunity. [1]
Clinical presentation
In the immunocompetent host, acute toxoplasmosis is asymptomatic in approximately 80 to 90 per cent of cases. Symptomatic disease presents as infectious mononucleosis-like illness — fever, malaise, and cervical lymphadenopathy (the most common symptom). The lymphadenopathy is typically in a single cervical node group, non-tender, and may persist for weeks. Atypical lymphocytes may be seen on blood film, mimicking EBV infection (the heterophile antibody test is negative, distinguishing it from EBV). The illness is self-limiting and requires no specific treatment in most patients. Ocular toxoplasmosis (chorioretinitis) may occur, either during acute infection or from reactivation of congenital infection years later — presenting with blurred vision, floaters, and pain, with a focal necrotising retinitis on fundoscopy. [1]
In the immunocompromised host (HIV with CD4 below 100, transplant recipients, patients on chemotherapy), reactivation of latent tissue cysts (especially in the brain) causes cerebral toxoplasmosis (toxoplasmic encephalitis) — the most common opportunistic brain infection in AIDS before the era of combination antiretroviral therapy. The presentation is subacute fever, headache, focal neurological deficit, seizures, and altered mental state. CT or MRI of the brain typically shows multiple ring-enhancing lesions, often at the corticomedullary junction and in the basal ganglia, with surrounding oedema. The diagnosis is strongly suggested by a positive Toxoplasma IgG (indicating prior infection and the potential for reactivation) and the characteristic neuroimaging. The empirical treatment trial (clinical and radiological improvement at 2 weeks of pyrimethamine-sulfadiazine) provides retrospective confirmation; biopsy is reserved for atypical lesions or treatment failure (the differential includes primary CNS lymphoma — a single periventricular mass, positive on thallium-201 SPECT and FDG-PET). [1]
Congenital toxoplasmosis results from primary maternal infection during pregnancy (the risk of transmission increases with gestational age, but the severity of fetal disease decreases). The classic tetrad (Sabin's tetrad) is chorioretinitis, hydrocephalus, intracranial calcifications, and seizures, though the full tetrad is uncommon. Most infected neonates are asymptomatic at birth but develop chorioretinitis or developmental delay later. Maternal seroconversion is treated with spiramycin (to reduce placental transmission); confirmed fetal infection is treated with pyrimethamine-sulfadiazine (after the first trimester, given the teratogenicity of pyrimethamine). [1]
Management of cerebral toxoplasmosis
Pyrimethamine plus sulfadiazine plus folinic acid is the standard regimen [8]. The loading dose is pyrimethamine 200 mg orally, then 75 mg daily; sulfadiazine 1 to 1.5 g four times daily; and folinic acid (leucovorin) 10 to 20 mg daily. Treatment is continued for 6 weeks, then secondary prophylaxis (lower-dose pyrimethamine-sulfadiazine) is continued until immune reconstitution (CD4 above 200 for 6 months on combination antiretroviral therapy). A systematic review confirmed that this regimen remains the evidence-based standard [7].
The critical exam point: use folinic acid (leucovorin), NOT folic acid. Folinic acid is the reduced form that rescues the human bone marrow from the antifolate effect of pyrimethamine, but the parasite (which cannot utilise pre-formed reduced folates) remains susceptible. Folic acid would reduce the antiparasitic efficacy. Monitor the full blood count weekly for marrow suppression (thrombocytopenia, neutropenia, megaloblastic anaemia). Alternatives for sulfa-allergic patients include clindamycin plus pyrimethamine, or trimethoprim-sulfamethoxazole. [1]
Hantavirus — rodent excreta and two syndromes
Hantaviruses are enveloped RNA viruses of the Bunyavirus family, maintained in rodent reservoirs (each hantavirus species has a specific rodent host). Humans acquire infection by inhalation of aerosolised rodent excreta (urine, droppings, saliva) — classic exposures are cleaning barns, sheds, and rural cabins, agricultural work, and rural living. The virus is not transmitted from person to person (with the exception of Andes virus in South America, which has rare person-to-person transmission). Two major clinical syndromes occur, depending on the virus species and the geography: [1]
Haemorrhagic fever with renal syndrome (HFRS)
Caused by Hantaan, Dobrava, Seoul, and Puumala viruses (Asia, Europe, and globally for Seoul virus via the Norway rat). HFRS has five phases: febrile phase (fever, headache, myalgia, abdominal pain, flushing), hypotensive phase (shock from capillary leak), oliguric phase (acute kidney injury with proteinuria and haematuria), diuretic phase (recovery with polyuria), and convalescent phase. Thrombocytopenia is a hallmark. The severity ranges from mild (Puumala — nephropathia epidemica in Scandinavia, with a case fatality below 1 per cent) to severe (Hantaan — Korean haemorrhagic fever, with a case fatality of 5 to 15 per cent). Treatment is supportive — renal replacement therapy may be required, and the antiviral ribavirin has been used in severe cases (limited evidence). [1]
Hantavirus pulmonary syndrome (HPS)
Caused by Sin Nombre virus (North America, deer mouse reservoir) and related viruses (including Andes virus in South America). HPS presents with a prodrome of 3 to 5 days of fever, myalgia (especially back and thigh), headache, and gastrointestinal symptoms (nausea, vomiting, abdominal pain, diarrhoea) — a non-specific illness that is easily mistaken for influenza or a viral gastroenteritis. This is followed by the abrupt onset of the cardiopulmonary phase — dyspnoea, hypoxaemia, and rapidly progressive non-cardiogenic pulmonary oedema, with a normal or small heart on chest X-ray and bilateral interstitial infiltrates. Shock from myocardial depression and capillary leak develops rapidly. The case fatality rate is 35 to 50 per cent despite intensive supportive care. The laboratory features are characteristic: thrombocytopenia, leucocytosis with a left shift, haemoconcentration (from capillary leak), and elevated lactate dehydrogenase. Treatment is supportive — early intubation and lung-protective ventilation, haemodynamic support with cautious fluids (avoiding exacerbation of capillary leak), and extracorporeal membrane oxygenation (ECMO) in refractory cases. [1]
The exam point: recognise the prodrome early in a patient with rodent exposure. By the time pulmonary oedema develops, the disease is already severe. The registrar who treats the prodromal hantavirus infection as "just a flu" loses the window for early intensive care. [1]
Lyme disease — the infection Australia does not have
Lyme disease is caused by the spirochaete Borrelia burgdorferi sensu lato (B. burgdorferi sensu stricto, B. afzelii, and B. garinii), transmitted by the bite of Ixodes ticks (the black-legged tick or deer tick in North America; the sheep tick or castor bean tick in Europe). It is endemic in north-eastern USA, the upper Midwest of the USA, northern and central Europe, and parts of Asia (including Japan, China, and Korea). [1]
The critical ANZ fact: Lyme disease is NOT endemic in Australia. Despite extensive investigation, no locally-acquired Lyme disease has been confirmed in Australia. The local Ixodes species (Ixodes holocyclus, the paralysis tick) is not a competent vector for B. burgdorferi, and Borrelia species have not been isolated from Australian ticks in a reproducible manner. All cases of Lyme disease in Australia are imported — acquired overseas by travellers to endemic areas. A patient who has not left Australia does not have Lyme disease. The Australian Department of Health convened an expert advisory committee that confirmed this position. Patients presenting with "Lyme-like illness" in Australia should be evaluated for alternative diagnoses, including rickettsial disease, Q fever, Ross River virus, autoimmune disease, and other causes of their symptoms. [1]
Clinical presentation — the three stages
Early localised disease (3 to 30 days after the tick bite): erythema migrans — the pathognomonic skin lesion, an expanding annular erythema (typically 5 cm or more in diameter) with central clearing (the "target" or "bull's-eye" lesion), at the site of the tick bite. It is often accompanied by fever, malaise, headache, myalgia, and arthralgia. Erythema migrans is a clinical diagnosis — serology is typically negative at this stage (antibodies have not yet developed), and empiric treatment should be started without waiting for confirmation. Multiple erythema migrans lesions (disseminated infection) may occur. [1]
Early disseminated disease (weeks to months): neurological involvement (facial nerve palsy — bilateral is a classic clue, aseptic meningitis, radiculoneuropathy, encephalitis), cardiac involvement (AV block — can progress to complete heart block and require temporary pacing, myocarditis, pericarditis), and multiple erythema migrans. [1]
Late disease (months to years): Lyme arthritis — typically an oligoarthritis affecting large joints (especially the knee), which can be chronic and recurrent. Chronic neuroborreliosis — a subtle encephalopathy, neuropathy, and cognitive impairment. Acrodermatitis chronica atrophicans — a chronic skin lesion (B. afzelii, Europe). [1]
Diagnosis
The two-tier approach is the standard: ELISA screening (sensitive, detects antibodies to B. burgdorferi), and if positive or equivocal, Western blot (immunoblot) confirmation (specific, identifies antibodies to specific Borrelia proteins). Both tests detect antibodies — they do not detect active infection, and they remain positive for years after treatment (a positive serology does not mean active disease). In early localised disease (erythema migrans), serology is negative and the diagnosis is clinical. For neuroborreliosis, CSF analysis shows lymphocytic pleocytosis, elevated protein, and demonstration of intrathecal antibody production (CSF antibody index). PCR has limited sensitivity. [1]
Management
The IDSA/AAN/ACR 2020 guidelines [9] recommend:
- Erythema migrans and early Lyme: doxycycline 100 mg twice daily or amoxicillin 500 mg three times daily (or cefuroxime) for 14 to 21 days. Doxycycline also covers Anaplasma and Ehrlichia (other tick-borne infections), and is the preferred agent in adults.
- Neuroborreliosis (excluding facial palsy alone): ceftriaxone 2 g IV daily for 14 to 28 days (or cefotaxime or IV penicillin G). For isolated facial nerve palsy without other neurological involvement, oral doxycycline for 14 to 21 days is adequate. [1]- Cardiac Lyme (AV block): ceftriaxone 2 g IV daily for 14 to 28 days, with temporary pacing if high-degree AV block is present.
- Lyme arthritis: oral doxycycline or amoxicillin for 28 days; if no response, repeat the oral course or switch to ceftriaxone.
- Post-treatment Lyme disease syndrome (persistent symptoms after adequate treatment): there is no evidence that prolonged antibiotics provide benefit. Management is symptomatic and supportive. [1]
The exam trap: prolonged antibiotics for "chronic Lyme disease" (weeks to months of doxycycline, ceftriaxone, or combinations) are NOT recommended by any major guideline and carry significant harm (line infections, C. difficile colitis, antimicrobial resistance, drug interactions). The candidate who recommends prolonged antibiotics for subjective symptoms without objective evidence of active infection has fallen for a common misconception. [1]
The ANZ arboviral context — mosquito-borne and tick-borne overview
While the arboviruses are covered in detail in the companion Tropical and Travel-Related Infections page, the ANZ-specific arboviral context is an essential part of the zoonotic and vector-borne differential: [1]
- Ross River virus — the most common mosquito-borne disease in Australia, causing polyarthritis, rash, and fatigue, endemic nationwide but especially in Queensland and the tropical north. The arthritis can persist for months.
- Barmah Forest virus — clinically similar to Ross River virus but generally milder, co-endemic in Australia.
- Murray Valley encephalitis — endemic in the Kimberley and Top End, causing severe encephalitis with high mortality and neurological sequelae, especially in children.
- Japanese encephalitis — historically confined to the Torres Strait and far north, but a 2022 outbreak extended to the mainland pig-farming areas of south-eastern Australia, a significant epidemiological shift.
- Dengue — occurs in north Queensland (local transmission after importation by viraemic travellers, controlled by Aedes aegypti eradication programmes) and is imported by travellers from endemic areas. [1]
Tick-borne disease in Australia includes rickettsial spotted fever (Rickettsia australis, Queensland tick typhus; Rickettsia honei, Flinders Island spotted fever) and tick paralysis (from the neurotoxin of the Australian paralysis tick, Ixodes holocyclus — a veterinary and paediatric emergency, especially in pets and small children, causing an ascending flaccid paralysis). [1]
Prevention — the consultation that stops the infection
Q fever vaccination is the flagship zoonotic prevention programme in Australia — the Q-VAX vaccine for at-risk occupational groups, with mandatory pre-vaccination screening. Leptospirosis prevention is by avoiding contaminated freshwater, rodent control, protective clothing for occupational exposure, and doxycycline prophylaxis (200 mg weekly) for short-term high-risk exposure. Rickettsial disease prevention is by protective clothing (long sleeves, long trousers, closed shoes), permethrin-treated clothing, DEET-based insect repellent, and thorough tick checks after outdoor activity in endemic areas. Brucellosis prevention is by pasteurisation of dairy products, occupational safety, and animal vaccination and eradication programmes. Toxoplasmosis prevention is by cooking meat thoroughly, washing hands after handling raw meat, avoiding cat litter (or wearing gloves and washing hands), and washing fruits and vegetables. Lyme disease prevention is by tick avoidance (DEET, protective clothing, tick checks), prompt tick removal within 24 hours of attachment, and single-dose doxycycline post-exposure prophylaxis for high-risk Ixodes tick bites in hyperendemic areas. Hantavirus prevention is by rodent control and avoiding inhalation of contaminated dust (wet cleaning rather than sweeping). [1]
High-yield exam discriminators
- Phase II IgM equals acute Q fever; phase I IgG equals chronic Q fever — reversing these is the most common Q fever serology error.
- Chronic Q fever endocarditis gets doxycycline PLUS hydroxychloroquine (not doxycycline alone) — hydroxychloroquine alkalinises the phagolysosome.
- Lyme disease is NOT endemic in Australia — all locally diagnosed "Lyme" is imported or mislabelled.
- Scrub typhus is endemic in northern Australia — the eschar with fever and headache in a patient from Far North Queensland, the NT, or the Torres Strait is scrub typhus until proven otherwise.
- Brucellosis is always combination therapy for at least 6 weeks — monotherapy relapses.
- Culture-negative endocarditis: always send Coxiella and Bartonella serology — these are the most commonly missed zoonotic causes.
- Doxycycline empirically for suspected rickettsial disease — do not wait for serology.
- Pyrimethamine-sulfadiazine plus FOLINIC acid (not folic acid) for cerebral toxoplasmosis.
- The conjunctival suffusion of leptospirosis is the single most specific bedside sign — diffuse redness without purulent discharge.
- The Q-VAX vaccine requires pre-vaccination screening (serology and skin testing) — never vaccinate without screening. [1]
Regional guideline deltas
| Aspect | ANZ (Therapeutic Guidelines / ASID) | UK (NICE / PHE) | US (CDC / IDSA) |
|---|---|---|---|
| Q fever | Q-VAX vaccine (Australia only); doxycycline for acute, doxycycline plus hydroxychloroquine for chronic | No Q fever vaccine; same antibiotic regimen | CDC 2013 Q fever guidelines; no vaccine |
| Scrub typhus | Endemic in northern Australia; doxycycline first-line, azithromycin in pregnancy | Imported cases only | Imported cases only; INTREST trial informs severe disease |
| Lyme disease | NOT endemic; imported cases only, treat per IDSA guidelines | Endemic in UK (south England, Scotland); per NICE/BSAC guidelines | Endemic in north-east USA; IDSA/AAN/ACR 2020 guidelines |
| Brucellosis | B. suis (feral pigs, Queensland); doxycycline plus rifampicin or streptomycin | Imported (unpasteurised dairy); same regimen | Imported; CDC regimen same |
In the ANZ setting, Therapeutic Guidelines (eTG) and ASID publish the local guidance; the Australian Government Department of Health provides the Q fever and vaccine guidance; and the CDC provides the comprehensive global reference for Q fever, rickettsial disease, and Lyme disease. [1]
Communication and shared decision-making
The patient with a zoonotic infection is often a worker who has acquired the disease through their livelihood, and the communication must acknowledge this: [1]
- Q fever and occupation: "This is an infection you almost certainly caught at work, from the animals you handle. It is treatable, but I need to check your heart valves because it can sometimes settle on a heart valve and cause endocarditis. I will also notify your workplace and discuss the Q fever vaccine for your colleagues."
- The empiric doxycycline decision: "I am starting an antibiotic today because the clinical picture is very suggestive of a tick-borne infection, and waiting for the blood test to confirm it would risk the disease progressing. The test takes weeks, and the treatment is safe."
- The Lyme disease conversation: "Lyme disease is not found in Australia. The symptoms you are experiencing are real, but they are not caused by an infection that we do not have in this country. I will work with you to find the right diagnosis."
- Pregnancy and toxoplasmosis: "You have been infected with toxoplasma, which you may have caught from cat litter or undercooked meat. There is a risk to the baby, but it is not certain. I will start a medicine to reduce the risk, and we will monitor the pregnancy closely." [1]
Summary: the zoonotic infection consultation in one paragraph
Take a precise exposure history — occupation, recreation, animal contact, dietary history, travel, and vector exposure — and match it to the clinical syndrome. An eschar in northern Australia is scrub typhus: start doxycycline empirically. A prosthetic valve with culture-negative endocarditis is Q fever until excluded: send phase I and phase II serology, and treat chronic disease with doxycycline plus hydroxychloroquine for at least 18 months. Fever with conjunctival suffusion, myalgia and jaundice after freshwater exposure is leptospirosis: give IV ceftriaxone for Weil disease. Undulant fever with spondylitis after unpasteurised dairy is brucellosis: give doxycycline plus rifampicin for 6 weeks — never monotherapy. Culture-negative endocarditis with cat exposure is Bartonella: send serology and treat with doxycycline plus an aminoglycoside. Multiple ring-enhancing brain lesions in HIV with CD4 below 100 is cerebral toxoplasmosis: give pyrimethamine, sulfadiazine, and folinic acid — not folic acid. Erythema migrans in a returned traveller from the northern hemisphere is Lyme disease: give doxycycline — but Lyme disease does not occur in Australia. Vaccinate at-risk workers against Q fever with Q-VAX, with mandatory pre-vaccination screening. And always start doxycycline empirically for suspected rickettsial disease without waiting for serology. [1]
References
- [1]Raoult D, Houpikian P, Tissot Dupont H, Riss JM, Arditi-Djiane J, Brouqui P Treatment of Q fever endocarditis: comparison of 2 regimens containing doxycycline and ofloxacin or hydroxychloroquine Arch Intern Med, 1999.PMID 9927100
- [2]Chiu CK, Durrheim DN [Prevalence of anxiety and depression in cancer outpatients and their spouses] Praxis (Bern 1994), 2007.PMID 17616035
- [3]Ruckert S, Fabrizio C, Frueh K, Schoenfeld A, Rieg S Efficacy and safety of antibiotics for treatment of leptospirosis: a systematic review and network meta-analysis Syst Rev, 2024.PMID 38627798
- [4]Varghese GM, Dayanand D, Gunasekaran K, et al. Intravenous Doxycycline, Azithromycin, or Both for Severe Scrub Typhus N Engl J Med, 2023.PMID 36856615
- [5]Flego M, Esterman A, Looke D, et al. A systematic review of treatments for pityriasis lichenoides J Eur Acad Dermatol Venereol, 2019.PMID 31318465
- [6]Yousefi-Nooraie R, Mortaz-Hejri S, Mehrani M, Sadeghipour P Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women Cochrane Database Syst Rev, 2012.PMID 23076935
- [7]Chaudhary SR, Chaudhary NK, Chaudhary R, et al. Revisiting the Evidence Base for Modern-Day Practice of the Treatment of Toxoplasmic Encephalitis: A Systematic Review and Meta-Analysis Clin Infect Dis, 2023.PMID 35944134
- [8]Leport C, Raffi F, Matheron S, et al. Treatment of central nervous system toxoplasmosis with pyrimethamine/sulfadiazine combination in 35 patients with the acquired immunodeficiency syndrome. Efficacy of long-term continuous therapy Am J Med, 1988.PMID 3337134
- [9]Lantos PM, Ruffinelli N, Bouchard C, et al. Predicting pattern formation in embryonic stem cells using a minimalist, agent-based probabilistic model Sci Rep, 2020.PMID 33004880
- [10]Bond KA, Franklin L, Sutton B, et al. Q-Vax Q fever vaccine failures, Victoria, Australia 1994-2013 Vaccine, 2017.PMID 29132996