Phys · neurological
Headache — Systematic Approach
Also known as migraine · tension-type headache · cluster headache · giant cell arteritis · temporal arteritis · idiopathic intracranial hypertension · pseudotumour cerebri · trigeminal neuralgia · medication-overuse headache · thunderclap headache · subarachnoid haemorrhage
Consultant-physician-depth guide to the systematic approach to headache — primary headaches (migraine, tension-type, cluster, trigeminal autonomic cephalalgias), secondary headaches, the SNNOOP10 red-flag screen, giant cell arteritis, idiopathic intracranial hypertension, trigeminal neuralgia, and medication-overuse headache — for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Headache — Systematic Approach
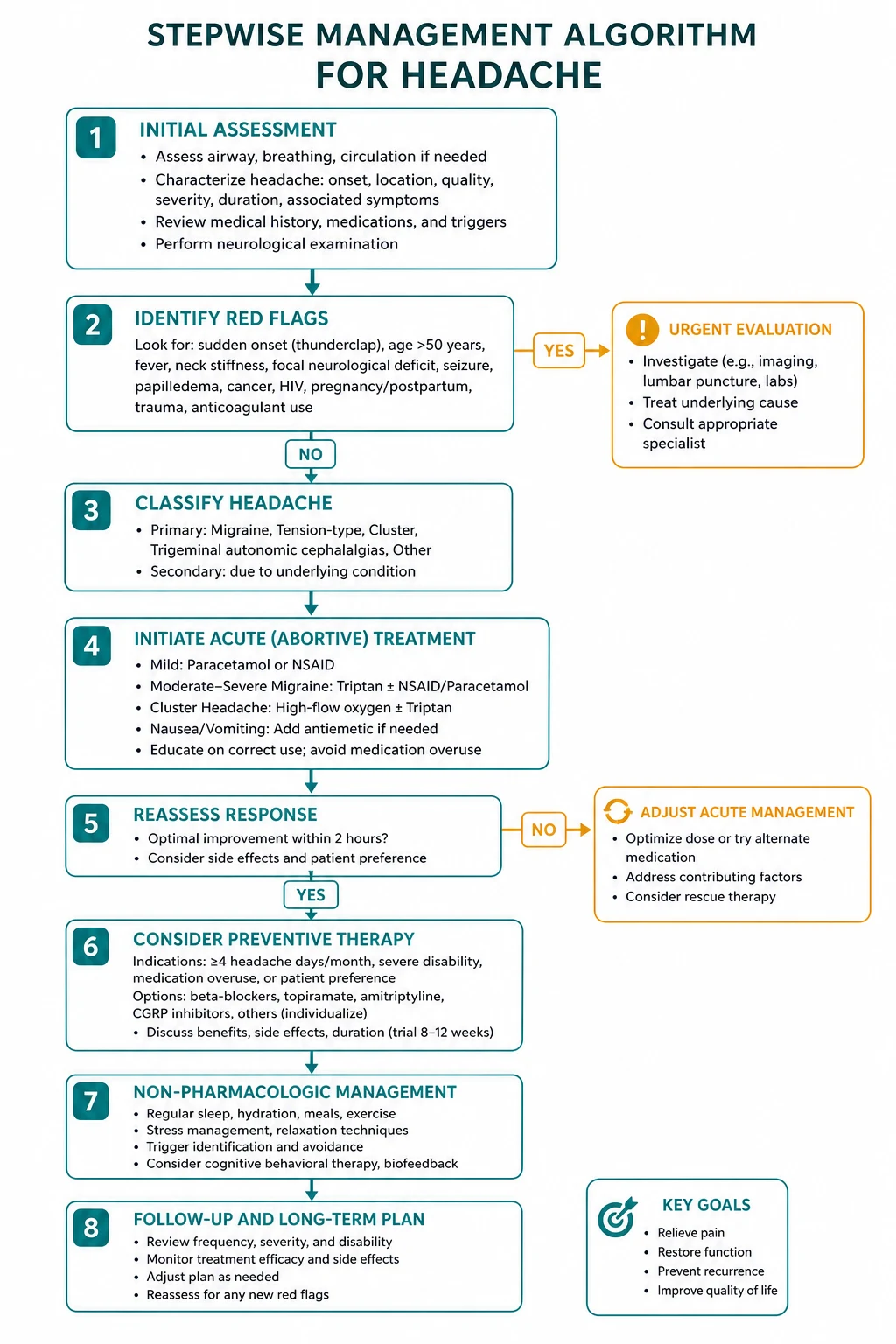

The answer first
Headache is one of the most common presentations in clinical medicine. The single decision that determines safety is: is this a primary or a secondary headache? Primary headaches (migraine, tension-type, cluster) account for approximately 90 per cent of presentations and are diagnosed on characteristic clinical patterns. Secondary headaches (subarachnoid haemorrhage, giant cell arteritis, raised intracranial pressure, infection, mass lesion) account for only 10 per cent but carry the morbidity and mortality [2].
The tool that separates the safe primary headache from the dangerous secondary one is the SNNOOP10 mnemonic — a systematic red-flag screen that you apply to every headache patient before you commit to a primary headache diagnosis [2]. If any red flag is present, you investigate with neuroimaging or targeted blood tests before labelling the headache as primary. If the screen is negative and the pattern matches a primary headache syndrome, you can manage with confidence and avoid unnecessary imaging.
The four emergencies that must never be missed are: [1]
- Subarachnoid haemorrhage — thunderclap headache, CT within 6 hours or LP for xanthochromia
- Giant cell arteritis — age over 50, temporal headache, jaw claudication, raised ESR/CRP, start prednisolone immediately
- Bacterial meningitis — fever, neck stiffness, altered mental status, do not delay antibiotics
- Acute angle-closure glaucoma — painful red eye with halos, measure intraocular pressure [1]
Classification: primary versus secondary
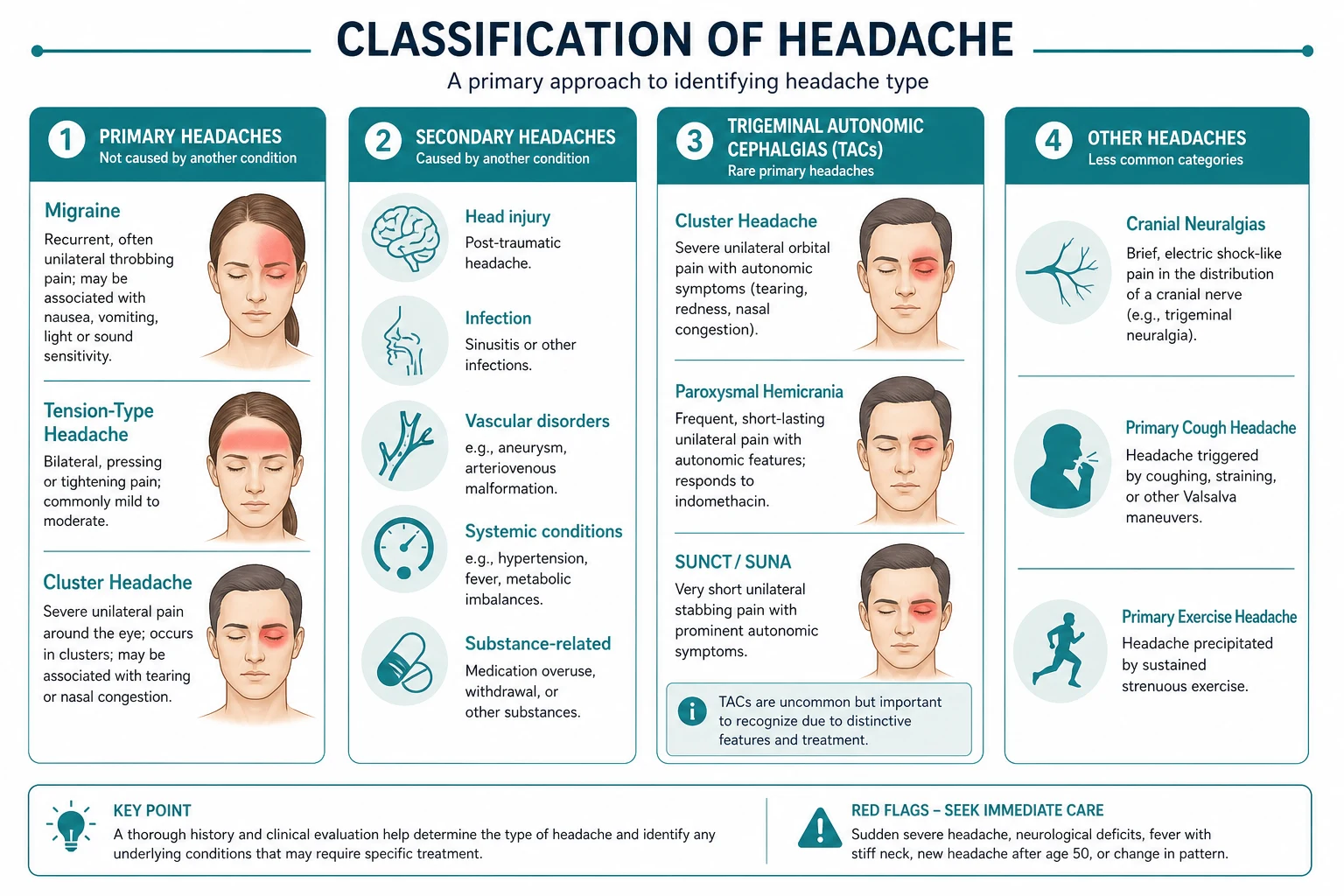
Headache is classified by the International Classification of Headache Disorders, 3rd edition (ICHD-3) into primary and secondary categories [1]. The classification is the global diagnostic standard.

The first question: primary or secondary?
| Category | Examples | Diagnostic principle |
|---|---|---|
| Primary (90 per cent) | Migraine, tension-type, cluster, trigeminal autonomic cephalalgias | Diagnosis by characteristic clinical pattern; normal examination; no red flags |
| Secondary (10 per cent) | SAH, meningitis, GCA, mass lesion, IIH, venous sinus thrombosis, medication overuse | Diagnosis by identifying the underlying cause; red flags drive investigation |
DWE high-yield: The most dangerous cognitive error in headache is assuming a headache is primary without screening for red flags. The SNNOOP10 list is the single highest-yield framework for the exam and for practice. Learn it cold. [1]
The SNNOOP10 red-flag screen
The SNNOOP10 mnemonic was formalised by Do and colleagues in 2019 as a comprehensive screen for secondary headache [2]. Every patient presenting with headache deserves a pass through this list in the history and examination. A single positive item mandates further investigation before a primary headache diagnosis is accepted.
| Letter | Red flag | What it screens for |
|---|---|---|
| S | Systemic symptoms/signs (fever, weight loss, night sweats) | Infection, malignancy, GCA |
| N | Neoplasm history | Brain metastasis |
| N | Neurologic deficit (focal weakness, sensory loss, altered consciousness) | Mass lesion, stroke, SAH, venous sinus thrombosis |
| O | Onset sudden or thunderclap (peak within 1 minute) | Subarachnoid haemorrhage |
| O | Older age (new onset after 50) | Giant cell arteritis, mass lesion |
| P | Pattern change (new or progressive headache, different from usual) | Mass lesion, subdural, GCA |
| P | Positional (worse on standing or lying flat) | Intracranial hypotension, posterior fossa mass |
| P | Precipitated by Valsalva, cough, sneeze, or exertion | Chiari malformation, posterior fossa lesion, venous sinus thrombosis |
| P | Papilloedema | Raised intracranial pressure (mass, IIH, venous sinus thrombosis) |
| P | Progressive headache and atypical presentations | Mass lesion, chronic infection |
| (additional) | Pregnancy or puerperium | Pre-eclampsia, cortical vein thrombosis, IIH |
| (additional) | Painful eye with halos | Acute angle-closure glaucoma |
| (additional) | Post-traumatic | Subdural, traumatic SAH |
| (additional) | Pathology of immune system (HIV, immunosuppression) | Opportunistic infection, lymphoma |
| (additional) | Painkiller overuse (analgesics on 15 or more days/month for 3 months) | Medication-overuse headache |
Clinical pearl: The SNNOOP10 list is highly sensitive but has low specificity — most patients with one red flag will not have a serious secondary cause. But the purpose of the screen is to decide who needs neuroimaging and blood tests, not to diagnose the secondary cause. When in doubt, image. [1]
Migraine
Migraine is the second most common primary headache after tension-type headache and is the most common cause of headache severe enough to cause functional impairment. It affects approximately 15 per cent of women and 6 per cent of men, peaking between ages 25 and 55 — the most productive years of life. [1]
ICHD-3 diagnostic criteria for migraine without aura
The ICHD-3 criteria require at least five attacks lasting 4 to 72 hours (untreated or unsuccessfully treated), with the following features [1]:
Criterion B — at least two of:
- Unilateral location
- Pulsating or throbbing quality
- Moderate or severe intensity (inhibits or prohibits daily activities)
- Aggravated by or causing avoidance of routine physical activity (walking, climbing stairs) [1]
Criterion C — at least one of:
- Nausea and/or vomiting
- Photophobia and phonophobia [1]
DWE high-yield discriminator: The mnemonic POUND helps recall the migraine features — Pulsating, One-day duration (4-72h), Unilateral, Nausea, Disabling. Four or five features give a positive likelihood ratio above 24 for migraine versus tension-type headache. [1]
Migraine with aura
Approximately one-third of migraine sufferers experience aura — a fully reversible neurological symptom preceding or accompanying the headache. Aura typically develops gradually over 5 to 20 minutes and lasts less than 60 minutes. The types are: [1]
- Visual aura (most common, 90 per cent) — scintillating scotoma (a jagged, expanding, shimmering visual disturbance), fortification spectra, photopsia
- Sensory aura — positive (tingling) then negative (numbness), spreading slowly over the face and hand
- Motor aura — unilateral weakness (hemiplegic migraine; distinguish from TIA and stroke)
- Brainstem aura (formerly basilar migraine) — vertigo, dysarthria, diplopia, ataxia, bilateral visual symptoms [1]
Clinical pearl — distinguishing migraine aura from TIA: Aura develops gradually over minutes and spreads across cortex (the cortical spreading depression marches at approximately 3 mm/min). TIA is sudden onset and maximal at the start. A visual symptom that expands across the visual field over 15-20 minutes is aura; one that appears instantaneously and fully formed is TIA or stroke. [1]
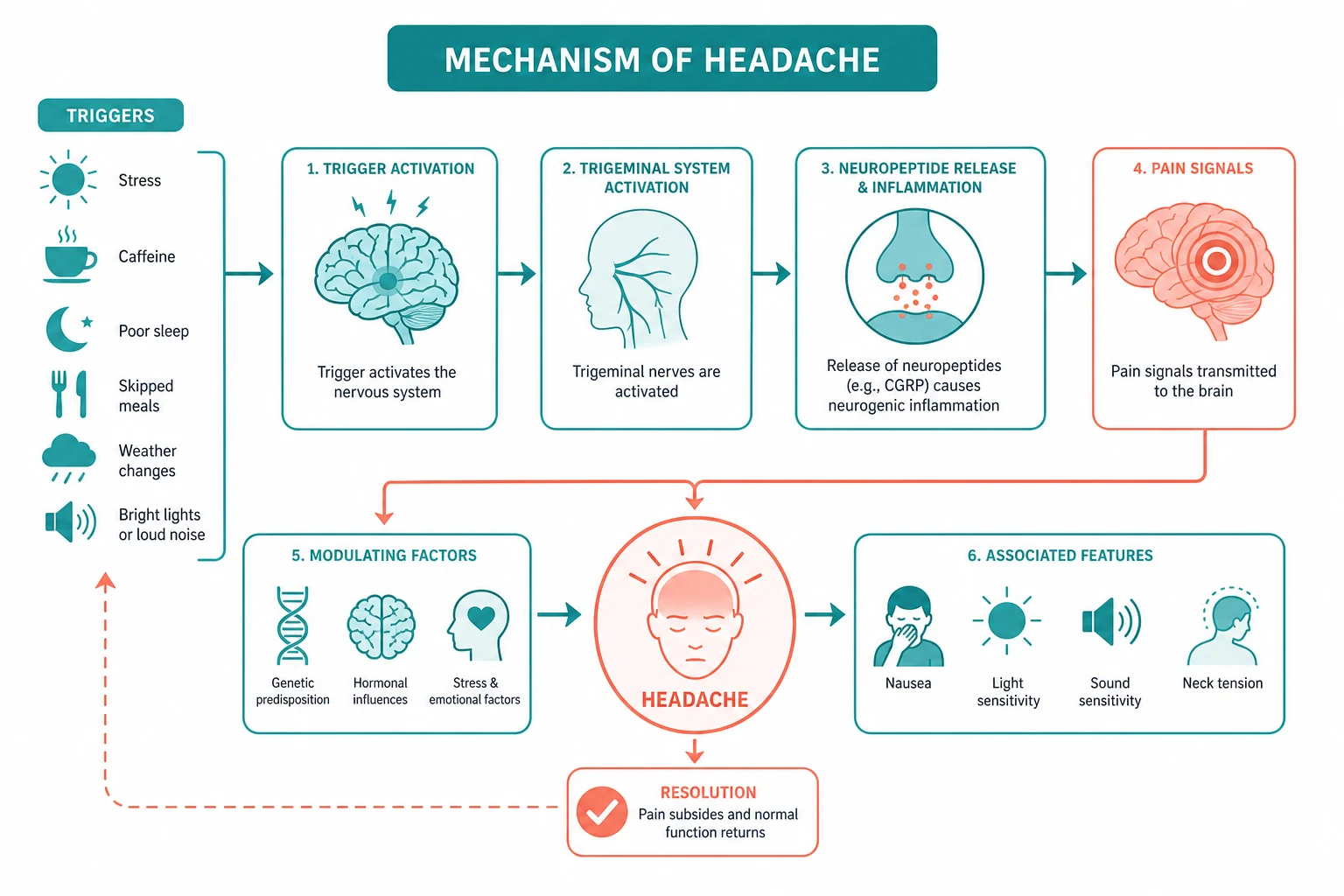
Pathophysiology — why migraine happens
Migraine is a disorder of brain excitability, not simply a vascular phenomenon. The current understanding integrates three mechanisms: [1]
-
Cortical spreading depression — a wave of neuronal depolarisation that spreads across the cortex at approximately 3 mm/min, followed by prolonged suppression of activity. This explains the gradual march of visual aura across the visual field. It also triggers the pain cascade by activating the trigeminovascular system. [1]
-
Trigeminovascular activation — the trigeminal nerve (particularly V1, the ophthalmic division) innervates the meningeal blood vessels. When activated, it releases vasoactive neuropeptides — most importantly calcitonin gene-related peptide (CGRP) — causing vasodilation, neurogenic inflammation, and sensitisation of the pain pathways. This produces the throbbing pain and the worsening with movement. [1]
-
Central sensitisation — repeated activation leads to sensitisation of the trigeminal nucleus caudalis in the brainstem, producing allodynia (pain from normally non-painful stimuli, like brushing hair) and the tendency for migraine to become chronic. [1]
The central role of CGRP is the therapeutic breakthrough: CGRP receptor antagonists (gepants) and CGRP pathway monoclonal antibodies (erenumab, fremanezumab, galcanezumab) are effective for both acute and preventive migraine therapy [4][5].
Acute migraine management
Treat at the onset of the headache, not when it is severe. The earlier the treatment, the more effective. The hierarchy: [1]
| Severity | First-line | Alternative |
|---|---|---|
| Mild-moderate | Paracetamol 1 g PO, or ibuprofen 400-600 mg PO, or naproxen 500 mg PO, with an antiemetic (metoclopramide 10 mg or prochlorperazine) | Aspirin 900 mg PO with metoclopramide |
| Moderate-severe | Triptan (sumatriptan 50-100 mg PO, rizatriptan 10 mg PO wafer, eletriptan 40 mg PO, zolmitriptan 2.5-5 mg PO) | CGRP antagonist (ubrogepant, rimegepant); combination of triptan plus NSAID |
| Severe with vomiting | Sumatriptan 6 mg SC, or zolmitriptan 5 mg intranasal, or prochlorperazine 10 mg IV with an NSAID | Dihydroergotamine 1 mg IV or IM (avoid with triptan) |
DWE high-yield trap — triptan contraindications: Triptans cause vasoconstriction and are contraindicated in ischaemic heart disease, prior stroke or TIA, uncontrolled hypertension, and pregnancy. Do not combine with ergotamine. In a patient with migraine and vascular disease, use a CGRP antagonist (ubrogepant, rimegepant) or high-dose NSAID plus antiemetic instead. [1]
Migraine preventive therapy
Start a preventive when:
- Migraine occurs on 4 or more days per month, or
- Attacks cause significant disability despite optimal acute therapy, or
- Acute therapy is contraindicated or ineffective (e.g., triptan contraindicated in a patient with ischaemic heart disease) [1]
The AAN/AHS evidence-based guideline (Silberstein 2012) established Level A efficacy for propranolol, timolol, metoprolol, topiramate, valproate, and divalproex [3]. Amitriptyline and candesartan are also widely used with good evidence.
| Drug | Starting dose | Target dose | Key adverse effects |
|---|---|---|---|
| Propranolol | 20-40 mg twice daily | 40-80 mg twice daily (up to 160 mg) | Fatigue, bradycardia, exercise intolerance, depression |
| Amitriptyline | 10-25 mg nocte | 25-75 mg nocte | Sedation, dry mouth, weight gain, constipation |
| Valproate | 200 mg twice daily | 500 mg twice daily | Weight gain, tremor, hair loss, hepatotoxicity; teratogenic — avoid in women of childbearing potential |
| Candesartan | 4-8 mg daily | 8-16 mg daily | Hypotension, dizziness, hyperkalaemia |
CGRP monoclonal antibodies — the modern preventive class, added after the 2012 guideline. Indicated when oral preventives are ineffective, contraindicated, or poorly tolerated. They are administered by subcutaneous injection and have minimal systemic side effects: [1]
- Erenumab — 70-140 mg SC monthly (CGRP receptor antagonist; STRIVE trial showed significant reduction in monthly migraine days) [4]
- Fremanezumab — 225 mg SC monthly or 675 mg SC quarterly (ligand antibody; HALO-CM trial for chronic migraine) [5]
- Galcanezumab — 120 mg SC monthly after 240 mg loading dose
Communication point: The CGRP monoclonal antibodies have transformed migraine prevention for patients who have failed multiple oral drugs. They target a specific pain chemical (CGRP) released during migraine, are well tolerated (main side effect is injection-site reaction and constipation), and do not have the cognitive, weight, or cardiovascular effects of the oral preventives. The barrier in ANZ is cost and PBS restriction (typically requiring failure of three oral preventives). [1]
Migraine in women and the oral contraceptive pill
Migraine with aura is an independent risk factor for ischaemic stroke. The mechanism is thought to be endothelial dysfunction and a prothrombotic state associated with the cortical spreading depression. [1]
- Migraine with aura: Oestrogen-containing combined oral contraceptives are contraindicated (UKMEC 4). Use progestogen-only methods (POP, implant, injectable, IUS).
- Migraine without aura: Combined oral contraceptives may be used with caution if there are no other stroke risk factors (UKMEC 2-3). Review vascular risk factors and avoid in smokers over 35. [1]
Tension-type headache
Tension-type headache (TTH) is the most common primary headache, but patients rarely present to a doctor for it because it is mild and non-disabling. When they do, it is because the frequency has increased or they fear a serious cause. [1]
ICHD-3 criteria for tension-type headache
At least 10 episodes lasting 30 minutes to 7 days, with:
- Bilateral location
- Pressing or tightening (non-pulsating) quality
- Mild or moderate intensity
- Not aggravated by routine physical activity
- No nausea or vomiting (anorexia may occur)
- No more than one of photophobia or phonophobia [1]
The contrast with migraine is the key: tension-type headache is bilateral, non-pulsating, mild-to-moderate, has no nausea, and does not worsen with movement. Migraine is unilateral, throbbing, moderate-to-severe, with nausea and both photo- and phonophobia. [1]
Management
- Acute: Paracetamol 1 g or NSAIDs (ibuprofen 400 mg, naproxen 500 mg). Avoid opioids and codeine — they drive medication-overuse headache.
- Preventive (chronic TTH, more than 15 days/month): Amitriptyline 10-75 mg nocte is first-line. Start low and titrate. Mirtazapine and topiramate are alternatives. [1]
DWE trap: A patient describing "band-like pressure around the head" with mild-moderate daily headache has tension-type headache, not migraine. The distinction matters because the preventive and acute therapy differ, and because chronic tension-type headache is the setting where medication-overuse headache most easily develops. [1]
Cluster headache
Cluster headache is the most severe of the primary headaches — patients describe the pain as worse than renal colic, childbirth, or amputation. The suicide risk in untreated cluster headache is significant, which is why rapid diagnosis and effective acute therapy are critical. [1]
ICHD-3 criteria for cluster headache
Severe or very severe unilateral orbital, supraorbital, and/or temporal pain lasting 15 to 180 minutes (untreated), with at least one of the following ipsilateral autonomic features:
- Conjunctival injection and/or lacrimation
- Nasal congestion and/or rhinorrhoea
- Eyelid oedema
- Forehead and facial sweating
- Miosis and/or ptosis (partial Horner syndrome)
- A sense of restlessness or agitation [1]
Frequency: Every other day to 8 per day. Attacks occur in bouts (clusters) lasting weeks to months, separated by remission periods — hence the name. The circadian and circannual periodicity (attacks at the same time each day, often at night, and bouts in the same season each year) is a hallmark pointing to hypothalamic involvement. [1]
Pathophysiology — the hypothalamus
Unlike migraine, cluster headache does not involve cortical spreading depression. The posterior hypothalamus is activated during attacks (demonstrated on functional MRI), explaining the characteristic circadian periodicity. The trigeminovascular system is activated (as in migraine), producing the severe unilateral pain. The ipsilateral autonomic features arise from activation of the superior salivatory nucleus-parasympathetic pathway through the greater petrosal nerve, causing lacrimation, nasal congestion, and conjunctival injection. [1]
Acute management
Cluster attacks peak within 5-10 minutes and last 15-180 minutes. Oral therapy is useless — it is too slow. The two effective acute treatments are: [1]
- 100 per cent oxygen at 12-15 L/min via a non-rebreather mask for 15 minutes. This is effective in approximately 78 per cent of patients within 15 minutes (versus 20 per cent with placebo) and has no systemic side effects [6]. The mechanism is thought to be cerebral vasoconstriction and suppression of the trigeminovascular cascade.
- Subcutaneous sumatriptan 6 mg. Rapid onset; effective within 10-15 minutes. Intranasal zolmitriptan 5 mg is an alternative. Remember triptan contraindications (ischaemic heart disease — a problem in the middle-aged male cluster patient who often has cardiovascular risk factors).
Preventive therapy
During a bout, start a preventive immediately to shorten the cluster and reduce attack frequency: [1]
| Drug | Dose | Notes |
|---|---|---|
| Verapamil (first-line) | 240-960 mg daily in divided doses | ECG before starting and with each dose increase (risk of AV block); the only preventive shown to be effective in randomised trials for cluster |
| Topiramate | 50-200 mg daily | Useful adjunct |
| CGRP monoclonal antibody (galcanezumab) | 300 mg SC monthly at bout onset | Emerging evidence for episodic cluster |
Transitional therapy: Oral prednisolone 1 mg/kg (maximum 60 mg) daily for 5 days, tapering over 2-3 weeks, provides bridge coverage while verapamil takes effect. Greater occipital nerve injection with corticosteroid and local anaesthetic is another transitional option. [1]
DWE high-yield: The classic cluster headache vignette is a 35-year-old man who wakes at 2 am with excruciating right-sided orbital pain, a watering right eye, and a blocked right nostril, pacing the room (restlessness distinguishes cluster from migraine, where the patient lies still in a dark room). The acute treatment is 100 per cent oxygen at 12-15 L/min via non-rebreather mask or subcutaneous sumatriptan 6 mg. [1]
Giant cell arteritis (temporal arteritis)
Giant cell arteritis is a rheumatological emergency. It is a granulomatous vasculitis of medium and large arteries, predominantly the extracranial branches of the carotid artery. Untreated, it causes irreversible blindness from anterior ischaemic optic neuropathy — and that blindness can occur within hours to days of the first symptom. [1]
Who gets it
GCA occurs almost exclusively in patients over 50 (median age 76). It is more common in women, in Northern European populations, and in patients with polymyalgia rheumatica (PMR). Approximately 40-50 per cent of patients with GCA have PMR, and 15-20 per cent of patients with PMR develop GCA. [1]
Clinical features
| Feature | Frequency | Clinical note |
|---|---|---|
| New headache (usually temporal) | 70-80 per cent | The headache is often the presenting complaint; may be occipital if the occipital artery is involved |
| Scalp tenderness | 70 per cent | Pain on combing hair or lying on a pillow |
| Jaw claudication | 50 per cent | The most specific symptom — pain in the masseter on prolonged chewing, relieved by rest; indicates external carotid involvement |
| Visual disturbance | 25-50 per cent | amaurosis fugax, diplopia, or permanent visual loss; the most feared complication |
| Polymyalgia rheumatica | 40-50 per cent | Proximal limb girdle stiffness and aching |
| Constitutional symptoms | 40 per cent | Fever, malaise, weight loss, night sweats — GCA is a cause of fever of unknown origin in the elderly |
Examination
- Palpate the temporal arteries for thickening, tenderness, and diminished or absent pulse.
- Examine for signs of PMR — difficulty raising the arms, proximal muscle tenderness (but no true weakness).
- Fundoscopy may show a pale, swollen disc (anterior ischaemic optic neuropathy) in a patient with visual loss.
- Listen for bruits over the carotids, subclavian, and brachial arteries — large-vessel GCA can cause limb claudication and bruits. [1]
Investigation
| Test | Finding | Notes |
|---|---|---|
| ESR | Markedly elevated, usually above 50 mm/h | Can be normal in up to 15 per cent of biopsy-proven cases — a normal ESR does NOT exclude GCA |
| CRP | Markedly elevated, usually above 20 mg/L | More sensitive than ESR; check both |
| Temporal artery ultrasound | Halo sign (dark ring around the vessel lumen from oedema in the vessel wall) | Increasingly used as first-line imaging; rapid and non-invasive |
| Temporal artery biopsy | Granulomatous arteritis with multinucleated giant cells | Gold standard but has skip lesions (sensitivity approximately 77 per cent; a negative biopsy does NOT exclude GCA) |
| FDG-PET or MRA of large vessels | Uptake or wall thickening in the aorta and subclavian arteries | For suspected large-vessel GCA |
DWE high-yield trap: The most commonly tested error in GCA is delaying steroids while waiting for the ESR result, the biopsy, or a rheumatology consult. Start prednisolone immediately on clinical suspicion. Vision lost to GCA does not recover. The biopsy can be arranged within the next 2 weeks and will remain positive during early steroid therapy. [1]
Management
- No visual symptoms: Prednisolone 40-60 mg PO daily, immediately. Do not wait for biopsy. Arrange temporal artery ultrasound and biopsy within 2 weeks. [1]- Visual symptoms or threatened vision: Admit and give IV methylprednisolone 500 mg-1 g daily for 3 days, then oral prednisolone 60-80 mg daily. This is the one situation where IV is preferred over oral — to maximise the chance of preserving remaining vision and protecting the contralateral eye.
- Taper: Reduce prednisolone gradually over 12-18 months, guided by symptoms and ESR/CRP. Start bone protection (calcium, vitamin D, a bisphosphonate) and gastric protection (PPI) at the outset, given the prolonged course.
- Steroid-sparing: Tocilizumab (an IL-6 receptor antagonist) is now licensed for GCA and reduces relapse risk and steroid exposure. Consider for patients who relapse on steroid taper or who develop significant steroid toxicity. [1]
Idiopathic intracranial hypertension
Idiopathic intracranial hypertension (IIH), formerly called pseudotumour cerebri, is raised intracranial pressure of unknown cause in the absence of a mass lesion or hydrocephalus. The classic patient is a young, obese woman of childbearing age. [1]
Clinical features
- Headache — daily, often worse in the morning or on lying flat; the most common presenting symptom [1]- Visual obscurations — transient grey-outs or blurring lasting seconds, often on bending or rising; a warning sign of threatened permanent visual loss
- Pulsatile tinnitus — a whooshing sound synchronous with the pulse, often ipsilateral to the side of the venous sinus stenosis
- Papilloedema — bilateral disc swelling; the hallmark on fundoscopy
- Diplopia — from CN VI palsy (a false localising sign from raised pressure stretching the nerve) [1]
Diagnostic criteria (Friedman 2013)
The revised diagnostic criteria require [8]:
- Signs and symptoms of raised intracranial pressure (papilloedema, headache, visual symptoms)
- Normal neurological examination except for CN VI palsy
- Normal neuroimaging (MRI brain; MRV to exclude venous sinus thrombosis) — no mass, no hydrocephalus
- Normal CSF composition (no cells, normal protein and glucose)
- Elevated lumbar puncture opening pressure above 25 cm of water in adults (above 28 cm in children) in the lateral decubitus position, legs relaxed
Investigation pathway
- MRI brain with MRV — to exclude a mass lesion, hydrocephalus, and venous sinus thrombosis (the key mimic of IIH). Empty sella and flattened posterior globe are supportive radiological signs.
- Lumbar puncture — measuring opening pressure (the critical test); CSF sent for cells, protein, glucose, and culture to confirm normal composition.
- Ophthalmology — formal visual fields (perimetry), optical coherence tomography (OCT) of the optic nerve, and visual acuity to establish baseline and monitor for visual loss. [1]
Management
| Intervention | Mechanism | Dose |
|---|---|---|
| Weight loss | The only disease-modifying intervention; 5-10 per cent weight loss can produce remission | Diet, exercise; bariatric surgery for refractory obesity |
| Acetazolamide | Carbonic anhydrase inhibitor; reduces CSF production | 500 mg twice daily, titrate to 1-4 g daily |
| Topiramate | Reduces CSF production and causes weight loss (unlike acetazolamide which can cause weight loss but also paraesthesia) | 50-200 mg daily |
| Surgical (for progressive visual loss): CSF shunting (lumboperitoneal or ventriculoperitoneal), optic nerve sheath fenestration, venous sinus stenting | Reduces CSF pressure or protects the optic nerve | Referral to neurosurgery or interventional neuroradiology |
Evidence base: The NORDIC IIH Treatment Trial confirmed that acetazolamide, when combined with a weight-reduction diet, produces modest but significant improvement in visual field function, papilloedema grade, and quality of life in patients with mild visual loss [9]. Weight loss remains the definitive therapy.
Monitoring and prognosis
The main risk is permanent visual loss from chronic papilloedema causing optic neuropathy. Every patient needs serial perimetry and OCT. The visual loss can be insidious — patients may not notice constriction of their visual fields until it is severe. The headache can persist even after the pressure is controlled, sometimes as a transformed migraine. [1]
Trigeminal neuralgia
Trigeminal neuralgia (TN) is a severe, paroxysmal facial pain in the distribution of the trigeminal nerve (most commonly V2 and V3, rarely V1). The pain is so characteristic that the diagnosis is clinical. [1]
Classic presentation
- Electric shock or lancinating pain, lasting seconds (never minutes or hours)
- In the distribution of V2 (maxillary) or V3 (mandibular), rarely V1 (ophthalmic)
- Triggered by light touch to a trigger zone — washing the face, shaving, brushing teeth, eating, cold wind, or even talking
- The patient can have hundreds of attacks per day and may become malnourished and dehydrated from fear of eating
- Between attacks, the patient is pain-free (though anxious about the next attack)
- No neurological deficit on examination — if there is sensory loss in the trigeminal distribution, suspect a mass lesion or multiple sclerosis [1]
Pathophysiology
The most widely accepted theory is neurovascular compression of the trigeminal nerve root entry zone by an aberrant vascular loop (usually the superior cerebellar artery). The compression causes focal demyelination and ephaptic (cross-talk) transmission between touch and pain fibres, so that light touch triggers a massive pain discharge. This theory is supported by the finding of vascular loops on thin-slice MRI and by the success of microvascular decompression surgery. [1]
In a young patient (under 40) or bilateral TN, consider multiple sclerosis — a plaque at the root entry zone produces identical symptoms. An MRI brain with contrast is indicated in these atypical presentations. [1]
Management
The AAN/EFNS guideline (Gronseth 2008) established carbamazepine as Level A first-line therapy [10]:
| Drug | Starting dose | Target dose | Key adverse effects |
|---|---|---|---|
| Carbamazepine (first-line) | 100 mg twice daily | 600-1600 mg daily in divided doses | Drowsiness, ataxia, diplopia, hyponatraemia (check sodium at 4-6 weeks), leukopenia, rash (Stevens-Johnson syndrome in HLA-B*1502 positive — screen in Han Chinese/Southeast Asian patients) |
| Lamotrigine (Level C) | 25 mg daily, titrate slowly | 200-400 mg daily | Slow titration to avoid Stevens-Johnson syndrome |
| Baclofen (Level C) | 5 mg three times daily | 10-20 mg three times daily | Sedation, dizziness |
If medical therapy fails, surgical options include microvascular decompression (moving the offending vessel off the nerve — the most durable procedure for classic TN), percutaneous procedures (radiofrequency rhizotomy, glycerol injection, balloon compression), and stereotactic radiosurgery (gamma knife). [1]
Medication-overuse headache
Medication-overuse headache (MOH) is a secondary headache caused by the regular overuse of acute headache medication. It is the most common cause of chronic daily headache and is entirely iatrogenic. The paradox is that the medication the patient takes to relieve the headache transforms it into a daily, chronic headache — and the only treatment is withdrawal of that very medication. [1]
ICHD-3 criteria
Headache occurring on 15 or more days per month in a patient with a pre-existing primary headache disorder, developing as a consequence of regular medication overuse for 3 or more months [1]:
| Medication class | Threshold (days/month) |
|---|---|
| Ergotamine, triptans, opioids, combination analgesics | 10 or more days/month for 3 months |
| Simple analgesics (paracetamol, NSAIDs, aspirin) | 15 or more days/month for 3 months |
| Multiple drug classes (any combination) | 10 or more days/month for 3 months |
The clinical scenario
The typical patient has a history of episodic migraine (or tension-type headache) that has gradually transformed over months to years into a daily or near-daily headache. They take increasing amounts of analgesia — often codeine-containing compounds — believing that the pain is worsening. The analgesia provides transient relief but the headache returns, driving more analgesia. The cycle is self-perpetuating. [1]
Management
- Explain the diagnosis — the most important step. The patient must understand that the medication they believe is helping is actually causing the daily headache. Expect resistance; this is counter-intuitive. [1]2. Withdraw the offending medication — abruptly for triptans, ergots, and simple analgesics; taper over 2-4 weeks for opioids and codeine-containing compounds (to avoid withdrawal symptoms). Warn the patient that the headache will worsen for 1-2 weeks (withdrawal headache) before it improves.
- Start a preventive — migraine preventive (topiramate, propranolol, CGRP monoclonal antibody) to address the underlying primary headache, which will still be present after withdrawal.
- Provide acute therapy for breakthrough attacks — but limit to 2 days per week, and never the overused drug class.
- Follow up at 4-8 weeks — the headache frequency should decline markedly. If the patient remains headache-free after 2 months off the offending medication, the MOH is resolved. [1]
DWE high-yield trap: The most commonly tested scenario is a patient with a history of migraine who now has daily headache and takes codeine or paracetamol daily. The answer is medication-overuse headache, and the management is withdraw the offending analgesic — not a brain scan, not a new acute drug, not a different preventive. You cannot treat chronic migraine on top of medication overuse. [1]
Thunderclap headache and subarachnoid haemorrhage
A thunderclap headache reaches maximum intensity within 1 minute. This is the single most important red flag in headache medicine. While not every thunderclap headache is a subarachnoid haemorrhage, every thunderclap headache must be investigated as if it were until SAH is excluded. [1]
The Ottawa SAH Rule
Perry and colleagues validated a clinical decision rule with 100 per cent sensitivity for identifying patients with suspected SAH who require investigation [7]. The rule applies to alert patients (GCS 15) presenting with a new, severe, non-traumatic headache peaking within 1 hour. Investigate if any one of the following is present:
- Age 40 years or older
- Neck pain or stiffness
- Witnessed loss of consciousness
- Onset during exertion
- Thunderclap (instantly peaking) headache
- Limited neck flexion on examination [1]
Investigation pathway for suspected SAH
- Non-contrast CT head within 6 hours of onset — sensitivity approaches 100 per cent in the first 6 hours (third-generation CT). This is the first and most important test.
- If CT is negative or performed after 6 hours: Lumbar puncture at 12 hours after onset (to allow xanthochromia to develop). Look for:
- Xanthochromia (yellow discolouration of the CSF supernatant from bilirubin — a breakdown product of haemoglobin that is only produced in vivo, confirming true SAH rather than a traumatic tap)
- Non-clearing red blood cells (RBCs that do not diminish from bottle 1 to bottle 3 or 4, unlike a traumatic tap)
- If CT or LP is positive: CT angiography to identify the aneurysm, then neurosurgical and interventional neuroradiology referral for clipping or coiling. [1]
DWE high-yield trap: A normal CT does not exclude SAH, especially after 6 hours. A lumbar puncture at 12 hours or more for xanthochromia is required. A "traumatic tap" (where the needle hits a blood vessel) can mimic SAH with red cells — but xanthochromia will be absent, and the red cell count will diminish from bottle 1 to bottle 3. Xanthochromia is the critical discriminator. [1]
When is neuroimaging indicated in headache?
Neuroimaging is not indicated for every headache. It is indicated when the SNNOOP10 screen is positive, and in specific clinical scenarios: [1]
| Indication | Imaging modality | Rationale |
|---|---|---|
| Any positive SNNOOP10 red flag | CT or MRI | Exclude secondary cause |
| Thunderclap headache | Non-contrast CT within 6 hours; CTA if positive | SAH |
| New headache after age 50 | MRI (or CT) | GCA, mass lesion, subdural |
| Papilloedema on fundoscopy | MRI brain plus MRV | Mass lesion, IIH, venous sinus thrombosis |
| Positional headache | MRI | Intracranial hypotension, posterior fossa lesion |
| Focal neurological deficit | MRI (with contrast if mass suspected) | Stroke, mass, demyelination |
| Trigeminal neuralgia (atypical: under 40, bilateral, sensory loss) | MRI brain with contrast | MS, mass at cerebellopontine angle |
| Headache with HIV or immunosuppression | MRI with contrast | Toxoplasmosis, lymphoma, cryptococcus |
Clinical pearl: For the vast majority of primary headache patients (migraine, tension-type, cluster), neuroimaging is normal and unnecessary. Ordering a CT or MRI for every headache is not only expensive and wasteful — it occasionally finds an incidental finding that generates anxiety and further unnecessary investigation. The SNNOOP10 screen is the gatekeeper. [1]
The headache examination
Every headache patient requires a focused neurological examination. The examination is designed to find signs of secondary cause. [1]
Fundoscopy (the single most important sign)
Look for papilloedema — disc swelling from raised intracranial pressure. Early papilloedema is subtle: loss of spontaneous venous pulsations (a sign present in 80 per cent of normal individuals), blurring of the disc margins (starting superiorly and inferiorly), and elevation of the disc. Late papilloedema shows haemorrhages and exudates. [1]
Limitation of fundoscopy: Absence of papilloedema does not exclude raised intracranial pressure — it can take days to develop, and the fundus may be normal early. If clinical suspicion is high, image and perform LP with opening pressure regardless of the fundus. [1]
Temporal artery examination (for suspected GCA)
- Palpate both temporal arteries for thickening, tenderness, nodularity, and diminished or absent pulse
- Listen for bruits over the temporal, carotid, subclavian, and brachial arteries
- Test for scalp tenderness (combing the hair, pressing on the occiput) [1]
Full neurological examination
- Cranial nerves — especially CN II (visual acuity, fields, fundus), CN III/IV/VI (eye movements, pupillary response), CN V (sensory in V1, V2, V3, corneal reflex), CN VII (facial symmetry)
- Motor — tone, power, reflexes, plantars (any focal deficit suggests a structural lesion)
- Sensory — pinprick, light touch, joint position (sensory level or hemisensory deficit suggests spinal cord or cortical lesion)
- Coordination and gait — cerebellar signs suggest a posterior fossa lesion
- Neck — stiffness, Kernig and Brudzinski signs (meningitis, SAH)
- Blood pressure — severe hypertension can cause headache; also screen for cardiovascular risk factors before prescribing a triptan [1]
DCE exam integration

How headache is tested in the DWE (MCQ)
The DWE tests headache with vignettes that discriminate primary from secondary, and that test the correct management decision:
- Thunderclap headache: The answer is always CT, then LP for xanthochromia. The distractor is "migraine" or "CTA first."
- Cluster headache: The acute answer is 100 per cent oxygen at 12-15 L/min or SC sumatriptan; the preventive is verapamil. The distractor is oral sumatriptan or a beta-blocker.
- Giant cell arteritis: The answer is prednisolone 40-60 mg immediately, do not wait for biopsy. The distractor is "wait for ESR" or "start low-dose aspirin." [1]- Trigeminal neuralgia: The answer is carbamazepine. The distractor is gabapentin, pregabalin, or surgery as first-line.
- Medication-overuse headache: The answer is withdraw the analgesic. The distractor is "increase the preventive" or "switch analgesics."
- Migraine preventive: The answer is propranolol, topiramate, or a CGRP monoclonal antibody. The distractor is a triptan (acute, not preventive) or an opioid. [1]
How headache is tested in the DCE (long case)
A headache long case will typically involve a patient with chronic migraine transformed by medication overuse, complicated by comorbidity (obesity, depression, vascular disease) that limits drug choice. The examiner will probe:
- The problem list (chronic migraine, MOH, medication-induced depression, disability)
- The management plan (analgesia withdrawal, preventive selection, lifestyle, follow-up)
- Why you chose or avoided specific drugs (e.g., avoiding a triptan in ischaemic heart disease; avoiding topiramate in pregnancy; choosing a CGRP monoclonal antibody after failure of three oral preventives)
- How you would investigate (the SNNOOP10 screen, when to image) [1]
How headache is tested in the DCE (short case)
A headache short case may present a patient with papilloedema (IIH), a temporal artery abnormality (GCA), or trigeminal sensory signs. The examiner will ask you to:
- Examine the cranial nerves or fundus systematically
- Present your findings
- Give a differential from the signs
- Discuss the investigation and management [1]
Key exam pitfalls summary
- Never label a thunderclap headache as migraine without excluding SAH with CT and, if needed, LP for xanthochromia.
- Never delay steroids in suspected GCA for biopsy or ESR. Vision lost is vision lost.
- Always screen for medication overuse in a patient with daily headache — it is the most common cause of chronic daily headache and the only treatment is withdrawal. [1]4. Remember that oral therapy is useless in cluster headache — use oxygen or subcutaneous sumatriptan.
- Never prescribe a combined oral contraceptive to a woman with migraine with aura — use progestogen-only methods.
- Remember that a normal ESR does not exclude GCA — treat on clinical suspicion.
- Remember that absence of papilloedema does not exclude raised ICP — image and measure LP opening pressure.
- Carbamazepine is first-line for trigeminal neuralgia — but check sodium at 4-6 weeks for hyponatraemia, and screen HLA-B*1502 in at-risk populations before starting. [1]
Key references
ICHD-3 (Headache Classification Committee, Cephalalgia 2018, PMID 29368949); SNNOOP10 (Do et al., Neurology 2019, PMID 30587518); Silberstein AAN/AHS migraine preventive guideline (Neurology 2012, PMID 22529202); Erenumab STRIVE trial (Goadsby et al., NEJM 2017, PMID 29171821); Fremanezumab HALO-CM (Silberstein et al., NEJM 2017, PMID 29171818); Cluster headache oxygen (Cohen et al., JAMA 2009, PMID 19996400); Ottawa SAH Rule (Perry et al., JAMA 2013, PMID 24065011); Friedman revised IIH criteria (Neurology 2013, PMID 23966248); NORDIC IIH acetazolamide trial (Wall et al., JAMA 2014, PMID 24756514); Gronseth AAN/EFNS trigeminal neuralgia guideline (Neurology 2008, PMID 18716236); ACR/EULAR GCA classification criteria (2022, PMID 36351706); NICE Clinical Guideline CG150 — Headaches in over 12s; British Association for the Study of Headache (BASH) Guidelines. [1]
References
- [1]Headache Classification Committee of the International Headache Society (IHS) Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition Cephalalgia, 2018.PMID 29368949
- [2]Do TP, Remmers A, Schytz HW, et al. Red and orange flags for secondary headaches in clinical practice: SNNOOP10 list Neurology, 2019.PMID 30587518
- [3]Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E Evidence-based guideline update: pharmacologic treatment for episodic migraine prevention in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society Neurology, 2012.PMID 22529202
- [4]Goadsby PJ, Reuter U, Hallstrom Y, et al. A Controlled Trial of Erenumab for Episodic Migraine N Engl J Med, 2017.PMID 29171821
- [5]Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the Preventive Treatment of Chronic Migraine N Engl J Med, 2017.PMID 29171818
- [6]Cohen AS, Burns B, Goadsby PJ High-flow oxygen for treatment of cluster headache: a randomized trial JAMA, 2009.PMID 19996400
- [7]Perry JJ, Stiell IG, Sivilotti MLA, et al. Clinical decision rules to rule out subarachnoid hemorrhage for acute headache JAMA, 2013.PMID 24065011
- [8]Friedman DI, Liu GT, Digre KB Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children Neurology, 2013.PMID 23966248
- [9]Wall M, McDermott MP, Kieburtz KD, et al.; NORDIC Idiopathic Intracranial Hypertension Study Group Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: the idiopathic intracranial hypertension treatment trial JAMA, 2014.PMID 24756514
- [10]Gronseth G, Cruccu G, Alksne J, et al. Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies Neurology, 2008.PMID 18716236
- [11]Ponte C, Grayson PC, Robson JC, et al. 2022 American College of Rheumatology/EULAR classification criteria for giant cell arteritis Ann Rheum Dis, 2022.PMID 36351706