Phys · neurological
Meningitis and Encephalitis
Also known as bacterial meningitis · viral meningitis · herpes simplex encephalitis · HSV encephalitis · tuberculous meningitis · cryptococcal meningitis · autoimmune encephalitis · anti-NMDAR encephalitis · meningococcal disease · aseptic meningitis
Consultant-physician-depth guide to central nervous system infections — bacterial meningitis empiric therapy and corticosteroid timing, HSV encephalitis and aciclovir, tuberculous and cryptococcal meningitis, and autoimmune encephalitis — for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Meningitis and Encephalitis
The answer first
Central nervous system infection is a time-critical medical emergency. The single decision that determines outcome is: start empiric antibiotics and antivirals the moment you suspect the diagnosis, before lumbar puncture, before CT, before any delay. A patient with suspected bacterial meningitis who waits for a CT scan before antibiotics has a measurably worse outcome [2].
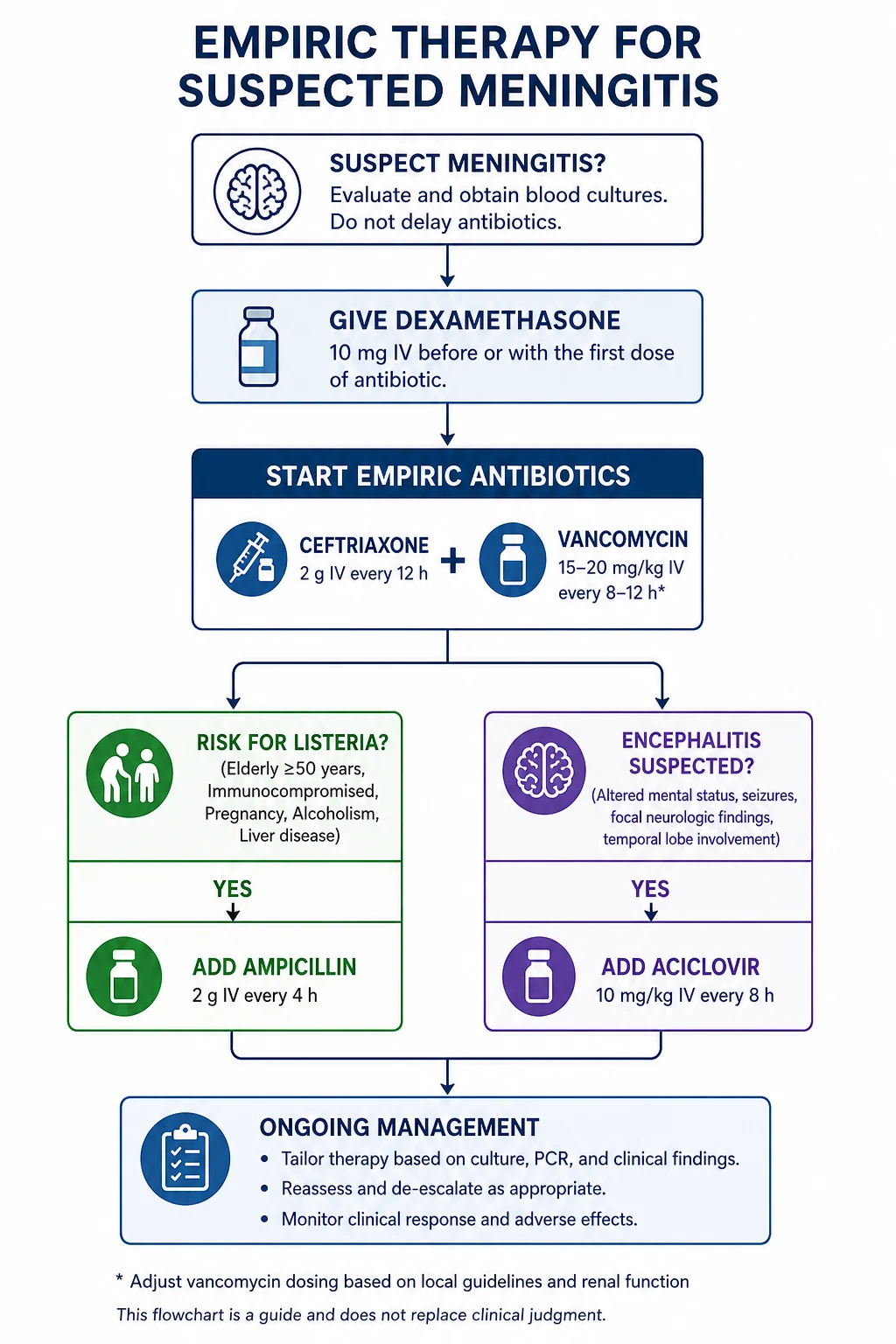
The empiric regimen for a community-acquired CNS infection in an immunocompetent adult is: [1]
- Ceftriaxone 2 g IV every 12 hours plus vancomycin (covering penicillin-resistant pneumococcus and meningococcus)
- Add ampicillin 2 g IV every 4 hours if the patient is over 50, pregnant, alcoholic, or immunocompromised (covers Listeria monocytogenes)
- Aciclovir 10 mg/kg IV every 8 hours if encephalitis is possible (fever with altered mental status, seizures, or focal neurology)
- Dexamethasone 10 mg IV every 6 hours given before or with the first antibiotic dose if bacterial meningitis is suspected — especially pneumococcal [1]
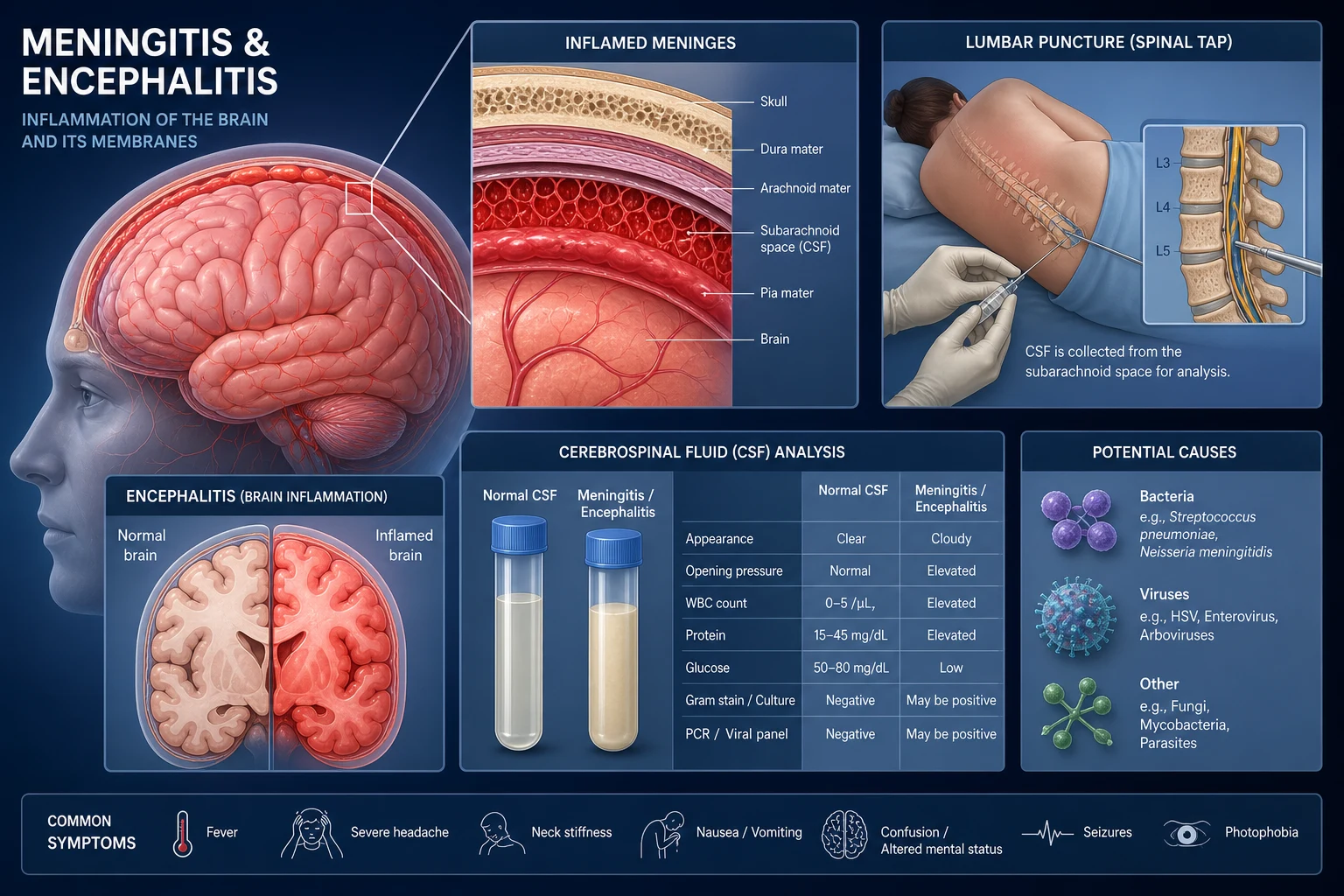
Meningitis (inflammation of the meninges) presents with fever, headache, and neck stiffness. Encephalitis (inflammation of the brain parenchyma) presents with fever plus altered mental status, seizures, or focal neurological deficits. The distinction matters because the empiric therapy and the differential are different. Many patients have meningoencephalitis — overlap of both. [1]
Classification
CNS infections are classified first by anatomical compartment (meninges vs parenchyma), then by aetiology (bacterial, viral, fungal, tuberculous, parasitic, autoimmune). [1]
Meningitis vs encephalitis — the clinical discriminator
| Feature | Meningitis | Encephalitis |
|---|---|---|
| Pathology | Inflammation of meninges | Inflammation of brain parenchyma |
| Hallmark | Fever, headache, neck stiffness | Fever + altered mental status, seizures, focal neurology |
| GCS | Usually preserved (unless severe) | Reduced — confusion, drowsiness, coma |
| Classic pathogen (bacterial) | Pneumococcus, meningococcus | (Rarely bacterial) |
| Classic pathogen (viral) | Enterovirus | HSV, VZV |
| First-line empiric therapy | Ceftriaxone + vancomycin + dexamethasone | Aciclovir (plus bacterial cover) |
DWE high-yield: The classical triad of bacterial meningitis — fever, neck stiffness, and altered mental status — is present in only about 44 to 50 per cent of cases. Fever alone is present in approximately 95 per cent. Absence of all three has a negative predictive value of 99 per cent — meaning if the patient has no fever, no neck stiffness, and a normal GCS, bacterial meningitis is effectively excluded [2].
Aetiological classification of meningitis
| Category | Key pathogens | CSF clue |
|---|---|---|
| Acute bacterial | S. pneumoniae, N. meningitidis, L. monocytogenes | Neutrophilic pleocytosis, low glucose, high protein |
| Acute viral ("aseptic") | Enterovirus, HSV-2, VZV | Lymphocytic pleocytosis, normal glucose |
| Chronic (subacute) | M. tuberculosis, Cryptococcus, Borrelia | Lymphocytic pleocytosis, very low glucose, very high protein |
| Fungal | Cryptococcus, Coccidioides, Histoplasma | Lymphocytic, low glucose, high protein, India ink / antigen positive |
Pathophysiology
Bacterial meningitis — how organisms reach the meninges
Bacteria reach the subarachnoid space by one of three routes: [1]
- Haematogenous spread — colonisation of the nasopharynx (pneumococcus, meningococcus) followed by invasion across the blood-brain barrier. This is the most common route.
- Direct extension — from sinusitis, otitis media, mastoiditis, or dental infection, particularly with anatomical defects.
- Post-traumatic or post-surgical — skull fracture with CSF leak, neurosurgery, or indwelling CSF shunt. Think S. aureus, coagulase-negative staphylococci, and gram-negative organisms in shunt infections. [1]
Once in the subarachnoid space, bacteria multiply rapidly because CSF has low levels of complement and immunoglobulin. Bacterial cell wall components (teichoic acid, endotoxin) trigger a massive inflammatory cascade — TNF-alpha, IL-1, IL-6 — recruiting neutrophils. The resulting subarachnoid exudate causes meningeal irritation (neck stiffness, photophobia), impairs CSF flow (hydrocephalus), and damages the pia-arachnoid barrier. The inflammation extends into the cortex (cerebritis), into cranial nerves (deafness, ophthalmoplegia), and into blood vessel walls (vasculitis, cortical vein thrombosis, stroke). [1]
This inflammation is why dexamethasone works — it suppresses the inflammatory cascade that causes neurological damage, particularly in pneumococcal meningitis. The benefit is greatest when the steroid is given before the antibiotic kills the bacteria and releases a burst of inflammatory cell wall products [1][4].
HSV encephalitis — why the temporal lobe
Herpes simplex virus type 1 reaches the brain by retgrade axonal transport along the olfactory and trigeminal nerves, which terminate in the temporal lobes. This neurotropic route explains the characteristic bilateral but asymmetric temporal lobe involvement. The virus causes haemorrhagic necrosis of the temporal cortex — visible on MRI as T2/FLAIR hyperintensity in the temporal lobes, often with areas of haemorrhage. [1]
The reason HSV encephalitis is the most important viral encephalitis is not that it is the most common (enteroviruses are more common overall) — it is that HSV encephalitis is treatable and untreated it kills or maims. Untreated HSV encephalitis has a mortality of over 70 per cent. With aciclovir, mortality falls to approximately 20 to 30 per cent [6].
Tuberculous meningitis — the basal exudate
M. tuberculosis reaches the meninges via haematogenous spread, forming Rich foci — small caseating granulomas in the cortex or meninges. When a Rich focus ruptures into the subarachnoid space, it releases bacilli and triggers a basal exudate — thick, gelatinous inflammatory material that accumulates at the base of the brain, around the circle of Willis. This basal location explains the three clinical hallmarks of TB meningitis: [1]
- Cranial nerve palsies (especially CN III, VI, VII) — the exudate engulfs the cranial nerves at the skull base
- Communicating hydrocephalus — the exudate blocks CSF reabsorption at the arachnoid granulations
- Cerebral infarction — the exudate causes a vasculitis of the arteries of the circle of Willis, producing lacunar and territorial strokes (often in the basal ganglia/internal capsule) [1]
Cryptococcal meningitis — the capsule and raised pressure
Cryptococcus neoformans reaches the brain haematogenously and accumulates in the Virchow-Robin (perivascular) spaces, where it forms mucoid cysts. The thick polysaccharide capsule means the organism is poorly opsonised, so it proliferates in the CSF and in the perivascular spaces, producing a very high organism burden and a characteristically high CSF opening pressure. The raised pressure is the dominant cause of morbidity — headache, visual loss, and death from herniation. This is why management of cryptococcal meningitis is not just antifungal therapy — it is repeated therapeutic LP or shunting to reduce pressure [13].
Common organisms by age and risk group
The single most important step in selecting empiric therapy is matching the antibiotic to the likely organism, which depends on age and immune status. [1]
| Age / risk group | Most common organisms | Empiric antibiotic addition |
|---|---|---|
| Under 1 month | Group B strep, E. coli, Listeria | Ampicillin + cefotaxime + aminoglycoside |
| 1 month to 2 years | Pneumococcus, meningococcus, H. influenzae | Ceftriaxone + vancomycin |
| 2 to 50 years (immunocompetent) | Pneumococcus, meningococcus | Ceftriaxone + vancomycin |
| Over 50 years | Pneumococcus, meningococcus, Listeria | Add ampicillin |
| Alcohol use disorder | Pneumococcus, Listeria | Add ampicillin |
| Immunocompromised (HIV, transplant, chemotherapy, anti-TNF) | Listeria, pneumococcus, Cryptococcus, gram-negatives | Add ampicillin; consider cryptococcus in HIV |
| Pregnant | Listeria, pneumococcus, group B strep | Add ampicillin |
| CSF shunt / post-neurosurgery | S. aureus, coagulase-negative staph, gram-negatives | Vancomycin + ceftazidime (not ceftriaxone — ceftazidime covers pseudomonas) |
DWE high-yield trap: The most commonly tested empiric therapy question gives a patient over 50 years old (or immunocompromised) with suspected meningitis. The answer is ceftriaxone + vancomycin + ampicillin + dexamethasone. Forgetting the ampicillin (Listeria cover) is the single most common error. Listeria is intrinsically resistant to all cephalosporins — ceftriaxone alone will not treat it. [1]
Clinical presentation
Bacterial meningitis — the presentation to recognise in 10 seconds
The presentation is acute (hours to 1 to 2 days). The four cardinal features, in approximate frequency: [1]
- Fever — present in approximately 95 per cent (but may be absent in the elderly or immunocompromised)
- Headache — present in approximately 80 to 90 per cent; typically severe, generalized, throbbing
- Neck stiffness — present in approximately 70 to 80 per cent; assess for nuchal rigidity (inability to flex chin to chest) and Kernig and Brudzinski signs. These signs are insensitive — their absence does not exclude meningitis
- Altered mental status — confusion, drowsiness, or reduced GCS; present in approximately 70 per cent; a marker of severity and a predictor of poor outcome [1]
Other features: photophobia, nausea and vomiting, seizures (approximately 15 to 30 per cent, usually a sign of severe disease or cortical involvement), and focal neurological deficits (cranial nerve palsies, hemiparesis — suggesting vasculitis, cortical vein thrombosis, or cerebral oedema). [1]
Clinical pearl: The classical triad of fever, neck stiffness, and altered mental status is present in only about half of patients. But if all three are absent, bacterial meningitis is excluded with approximately 99 per cent certainty [2]. In practice, a patient with fever and new headache or new confusion deserves investigation.
Meningococcal disease — the rash that changes everything
N. meningitidis can cause meningitis, septicaemia (meningococcaemia), or both. The petechial or purpuric rash is the hallmark of meningococcal septicaemia and appears in approximately 50 to 60 per cent of cases. The rash: [1]
- Begins as small petechiae (1 to 2 mm) that may be mistaken for flea bites
- Progresses to larger purpuric lesions (ecchymoses) in fulminant disease
- Has an irregular shape and does not blanch with pressure (test with a glass tumbler)
- May appear anywhere but favours the trunk, extremities, and mucous membranes [1]
A patient with fever and a rapidly evolving petechial or purpuric rash has meningococcal septicaemia until proven otherwise. This is the one scenario where the response must be immediate: [1]
- Draw blood cultures (do not delay more than a few minutes)
- Give ceftriaxone 2 g IV immediately — within 30 minutes of presentation
- Admit to ICU — meningococcal septicaemia causes fulminant septic shock, DIC, adrenal haemorrhage (Waterhouse-Friderichsen syndrome), and multi-organ failure within hours [1]
DWE trap: Meningococcal septicaemia with a purpuric rash and shock is one of the highest-yield scenarios. The key is that the rash does not blanch. Other causes of non-blanching rash include viral exanthems, idiopathic thrombocytopenic purpura, Henoch-Schonlein purpura, and leukaemia — but in the context of fever and rapid progression, treat as meningococcal. [1]
Viral meningitis — the milder cousin
Viral meningitis is more common than bacterial meningitis but is usually self-limiting. The presentation is similar to bacterial meningitis (fever, headache, neck stiffness) but milder — the patient is typically alert, without significant altered mental status, and without focal neurology. The distinction from bacterial meningitis is made on CSF analysis (see below). Enteroviruses (echovirus, coxsackievirus) are the most common cause, particularly in summer and autumn. HSV-2 can cause meningitis (Mollaret meningitis — recurrent aseptic meningitis) without encephalitis. [1]
Viral encephalitis — the presentation that demands aciclovir
Encephalitis should be suspected in any patient with fever plus altered mental status, new seizures, or focal neurological signs. The key clinical features are: [1]
- Fever — usually present
- Altered mental status — confusion, drowsiness, personality change, coma. This is the key discriminator from viral meningitis
- Seizures — focal or generalized; may be non-convulsive (suspect if the patient is not improving as expected or has a fluctuating GCS)
- Focal neurological deficits — aphasia, hemiparesis, cranial nerve palsies
- Behavioural and psychiatric disturbance — particularly prominent in HSV (temporal lobe) and anti-NMDAR encephalitis [1]
Tuberculous meningitis — the subacute presentation
TB meningitis is subacute — developing over days to weeks, not hours. The classic three stages: [1]
- Stage 1: Vague prodrome — malaise, low-grade fever, headache, irritability, for 1 to 3 weeks. Often misdiagnosed as a viral illness
- Stage 2: Meningeal signs emerge — headache, neck stiffness, cranial nerve palsies, confusion, drowsiness
- Stage 3: Severe disease — coma, seizures, hemiplegia (from vasculitic stroke), decerebrate posturing [1]
By the time a patient reaches stage 3, mortality is over 50 per cent even with treatment. The diagnostic challenge is to recognise TB meningitis in stage 1, when the symptoms are non-specific. The clinical clues are: endemic exposure, subacute timeframe, night sweats, weight loss, known TB contact, and a CSF picture of lymphocytic pleocytosis with very low glucose and high protein [12].
Cryptococcal meningitis — the immunocompromised presentation
Cryptococcal meningitis occurs almost exclusively in immunocompromised patients — HIV with CD4 under 100, transplant recipients on immunosuppression, and those on anti-TNF therapy or high-dose corticosteroids. The presentation is subacute to chronic (weeks): [1]
- Headache (often the dominant symptom)
- Fever (may be low-grade or absent)
- Raised intracranial pressure — severe headache, nausea, visual disturbance, papilloedema, cranial nerve palsies
- Less commonly: altered mental status, seizures, skin lesions (molluscum-like cryptococcomas) [1]
Clinical pearl: In any HIV-positive or transplant patient with headache, check the opening pressure at lumbar puncture. A markedly raised opening pressure (above 25 cm of water) in the context of a cryptococcal antigen-positive CSF mandates aggressive pressure management — repeated therapeutic LP, shunt, or acetazolamide — alongside antifungal therapy [13].
Autoimmune encephalitis — the mimic that needs immunotherapy
Autoimmune encephalitis is not an infection — it is an antibody-mediated inflammation of the brain. But it presents like infectious encephalitis (fever, confusion, seizures) and must be considered in the differential of any encephalitis patient who is HSV-PCR negative or who is not improving on aciclovir [10].
Anti-NMDA receptor encephalitis is the most common form. It classically affects young women and has a characteristic multi-phase presentation [11][14]:
- Prodrome — viral-like illness (fever, headache, fatigue) for 1 to 2 weeks
- Psychiatric phase — anxiety, psychosis, hallucinations, bizarre behaviour, agitation. Often admitted to psychiatry initially
- Neurological phase — seizures, dyskinesias (orofacial and limb), speech disturbance (mutism, echolalia), autonomic instability (cardiac arrhythmia, hypoventilation), catatonia, reduced consciousness
- Recovery phase — protracted, often requiring months of ICU and rehabilitation [1]
The exam trap: a young woman with new-onset psychosis, seizures, and orofacial dyskinesia has anti-NMDAR encephalitis until proven otherwise. Screen for an ovarian teratoma (the common associated tumour) with pelvic ultrasound and MRI, because removal of the teratoma improves outcome [14].
Anti-LGI1 encephalitis affects older men, presents with faciobrachial dystonic seizures (brief, frequent, stereotyped arm and face movements) and hyponatraemia (SIADH from the antibody), and is strongly associated with limbic encephalitis on MRI. [1]
Anti-CASPR2 encephalitis presents with neuromyotonia, cognitive impairment, and autonomic instability (Morvan syndrome). [1]
Differential diagnosis
The differential of fever with headache and/or altered mental status is broad. The key is to separate meningitis/encephalitis from mimics, and to separate the aetiologies within CNS infection. [1]
| Diagnosis | Discriminating features |
|---|---|
| Subarachnoid haemorrhage | Thunderclap headache (maximal in seconds); CT shows blood in sulci; xanthochromia on LP if CT normal |
| Brain abscess | Subacute fever, headache, focal neurology; ring-enhancing lesion on contrast CT/MRI |
| Viral meningitis (aseptic) | Mild course, alert, no focal neurology; CSF lymphocytic with normal glucose |
| HSV encephalitis | Fever + confusion + temporal lobe signs; CSF RBCs, MRI temporal signal, EEG PLEDs |
| TB meningitis | Subacute, basal features, very low CSF glucose, high protein; chest X-ray may be normal |
| Cryptococcal meningitis | HIV/immunocompromised, raised CSF opening pressure, India ink and CrAg positive |
| Autoimmune encephalitis | Subacute, psychiatric features, normal glucose, autoimmune Ab panel; often young female (NMDAR) |
| Cerebral malaria | Travel to endemic area, parasites on blood film, cyclical fever |
| Tick-borne disease | Lyme, rickettsia; endemic exposure, rash (erythema migrans, eschar) |
| Drug-induced / toxic encephalopathy | No fever, drug history, normal CSF |
| Septic encephalopathy | Systemic sepsis with delirium, usually normal CSF |
DWE trap: The most dangerous mimic is subarachnoid haemorrhage. A patient with meningism and a normal CT may still have SAH — check the CSF for xanthochromia (yellow discolouration from bilirubin, a breakdown product of RBCs). Xanthochromia is present from 12 hours to 2 weeks after SAH and distinguishes a true bleed from a traumatic LP tap. [1]
Investigations
The diagnostic sequence — and when to image first
The standard diagnostic sequence for suspected CNS infection is: blood cultures, then lumbar puncture, then start or continue therapy. However, not every patient should have an immediate LP. Certain features mandate a CT scan before LP because of the risk of cerebral herniation from raised intracranial pressure or a mass lesion. [1]
Indications for CT before LP (the "red flags"): [1]
| Red flag | Rationale |
|---|---|
| Immunocompromised (HIV, transplant, chemotherapy) | Risk of mass lesion (toxoplasmosis, lymphoma, abscess) |
| New-onset seizures | Suggests parenchymal involvement or mass |
| GCS below 12 or rapidly deteriorating | Risk of raised ICP or herniation |
| Focal neurological deficit | Suggests mass lesion or focal oedema |
| Papilloedema on fundoscopy | Raised ICP |
| Extremes of age (infants, elderly) or diagnostic uncertainty | Increased risk of space-occupying lesion |
Critical rule: CT before LP does NOT mean antibiotics before LP. If there is any clinical suspicion of bacterial meningitis, start empiric antibiotics immediately (ideally after blood cultures), then do the CT, then do the LP. The antibiotics will not significantly alter the CSF for several hours, and a delay in therapy costs lives [5].
Lumbar puncture — what to measure and send
The LP is the single most useful investigation in suspected CNS infection. Send at least three to four bottles plus a glucose sample: [1]
| Bottle / test | Purpose |
|---|---|
| Bottle 1 — Cell count and differential | Neutrophils (bacterial) vs lymphocytes (viral, TB, fungal); RBCs (haemorrhagic — HSV, SAH, traumatic) |
| Bottle 2 — Glucose and protein | CSF glucose compared to simultaneous serum glucose; ratio under 0.4 suggests bacterial/TB/fungal |
| Bottle 3 — Gram stain and culture | Identify organism; sensitivity takes 48 to 72 hours |
| Bottle 4 — Molecular and special tests | Meningitis/encephalitis multiplex PCR panel (HSV-1/2, VZV, enterovirus, parechovirus, S. pneumoniae, N. meningitidis, H. influenzae, L. monocytogenes, C. neoformans); TB PCR (Xpert MTB/RIF); cryptococcal antigen; cytology |
Always measure and record the opening pressure (normal under 20 cm of water in adults; raised above 25). A raised opening pressure in cryptococcal meningitis drives management. [1]
CSF interpretation — the four-pattern table
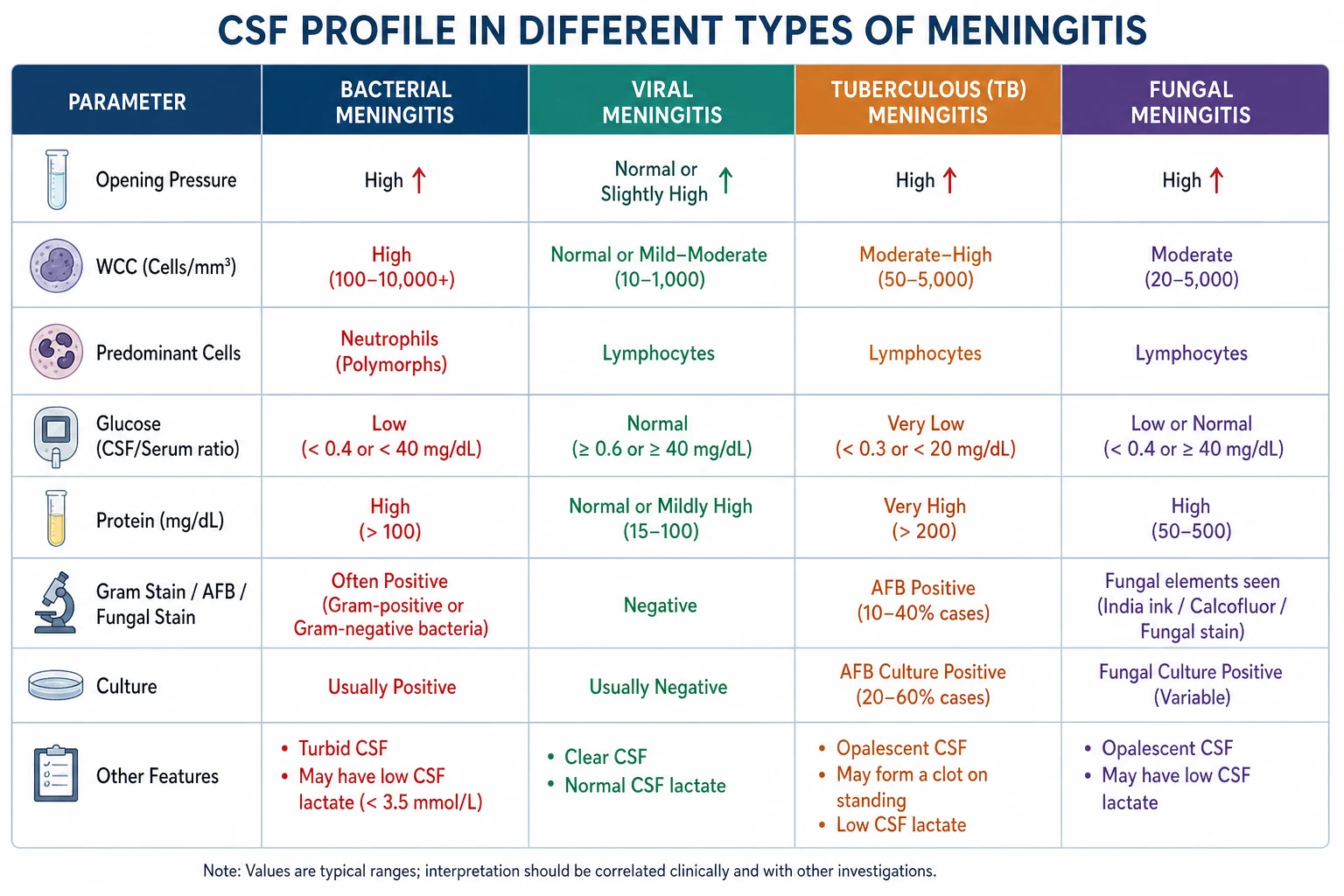
The following table is the single most tested diagnostic pattern in physician exams. Know it cold. [1]
| Parameter | Bacterial | Viral | Tuberculous | Cryptococcal (fungal) |
|---|---|---|---|---|
| Opening pressure | Raised (often above 25 cm) | Normal to mildly raised | Raised | Often markedly raised (above 25) |
| White cells | Markedly raised (100 to 10,000) | Raised (10 to 1,000) | Raised (50 to 500) | Raised (20 to 500) |
| Predominant cell | Neutrophils | Lymphocytes | Lymphocytes (early may be neutrophilic) | Lymphocytes |
| CSF glucose | Markedly reduced (under 2.2 mmol/L or ratio under 0.4) | Normal | Very low (often under 1.0) | Low (under 2.2) |
| Gram stain | Often positive | Negative | Negative (auramine positive for AFB) | India ink positive (60 per cent); mucicarmine |
| Special test | Bacterial PCR, culture | Viral multiplex PCR | TB PCR (Xpert), AFB culture (weeks) | Cryptococcal antigen (CrAg) — highly sensitive |
| RBCs | May be present | HSV — may be haemorrhagic | Variable | Variable |
DWE high-yield: The CSF pattern with neutrophilic pleocytosis, very low glucose, and high protein is bacterial meningitis until proven otherwise. The pattern with lymphocytic pleocytosis, very low glucose, and very high protein is TB or fungal. The pattern with lymphocytic pleocytosis, normal glucose, and mild protein elevation is viral meningitis. The exception: early bacterial meningitis (first few hours) can be lymphocytic, and partially-treated bacterial meningitis can look viral. Listeria meningitis can have a monocytic predominance. [1]
Partially-treated meningitis — the CSF trap
If a patient has received antibiotics before LP (e.g., from a GP), the CSF may show:
- Fewer or no organisms on Gram stain
- Lower cell count
- A shift from neutrophilic to lymphocytic predominance
- Culture may be negative [1]
Do not be falsely reassured. A CSF with elevated protein, low glucose, and pleocytosis after antibiotics is still bacterial meningitis until proven otherwise. PCR panels (which detect DNA, not viable organisms) are particularly valuable here. [1]
HSV PCR — the test that transformed HSV diagnosis
CSF HSV PCR has a sensitivity of approximately 96 to 98 per cent and specificity of approximately 94 per cent when compared to brain biopsy — the old gold standard [7]. PCR has replaced brain biopsy as the diagnostic standard for HSV encephalitis.
Critical caveat: HSV PCR can be false negative in the first 24 to 48 hours of illness because viral load in CSF is initially low. If the clinical picture strongly suggests HSV encephalitis (temporal lobe signal on MRI, PLEDs on EEG) but the first PCR is negative, repeat the PCR at 3 to 7 days and continue aciclovir while waiting. Stopping aciclovir based on a single early negative PCR is a catastrophic error [8].
Neuroimaging — MRI vs CT
| Modality | Role |
|---|---|
| Non-contrast CT | First-line before LP to exclude mass lesion, hydrocephalus, haemorrhage. May be normal in early meningitis |
| Contrast MRI | Most sensitive for meningeal enhancement (pial/arachnoid), cerebritis, abscess, and the characteristic temporal lobe changes of HSV encephalitis |
| MRI in HSV encephalitis | T2/FLAIR hyperintensity in temporal lobes (often bilateral, asymmetric), with restricted diffusion and sometimes haemorrhage. May be normal in first 48 hours |
| MRI in TB meningitis | Basal exudate enhancement, hydrocephalus, tuberculomas, infarcts in basal ganglia |
| MRI in cryptococcal meningitis | Dilated Virchow-Robin spaces ("gelatinous pseudocysts") in basal ganglia; may show cryptococcomas |
EEG in encephalitis
EEG is recommended for all patients with encephalitis [8]. It serves two purposes:
- To detect non-convulsive seizures — common in encephalitis and a cause of persistent coma
- To identify characteristic patterns — periodic lateralised epileptiform discharges (PLEDs) over a temporal lobe are highly suggestive of HSV encephalitis (though not pathognomonic) [1]
In anti-NMDAR encephalitis, the EEG characteristically shows "extreme delta brush" — a pattern of diffuse delta waves with superimposed fast (beta) activity — although this is present in only about 30 per cent of cases [10].
Blood tests
| Test | Purpose |
|---|---|
| Blood cultures | Essential — positive in approximately 50 to 75 per cent of bacterial meningitis; may identify organism even if CSF culture is negative |
| FBC, CRP, lactate | Severity and systemic involvement; thrombocytopenia in meningococcaemia |
| Coagulation | DIC in meningococcal septicaemia |
| U&E, LFTs | Baseline; SIADH common; hyponatraemia |
| Glucose | Compare to CSF glucose |
| HIV test | Essential in any chronic or atypical meningitis; cryptococcal and TB risk |
| Cryptococcal antigen (serum and CSF) | If HIV-positive or immunocompromised |
| Meningococcal and pneumococcal PCR (blood) | If antibiotics given before cultures |
Empiric management of suspected bacterial meningitis
The time-critical pathway
The sequence for a patient presenting with suspected community-acquired bacterial meningitis: [1]
- Recognise — fever + headache + neck stiffness or altered mental status
- Resuscitate — ABC; IV access; oxygen if hypoxic or comatose
- Blood cultures (two sets) — do not delay more than a few minutes
- Start empiric antibiotics immediately — do NOT wait for CT or LP
- Give dexamethasone 10 mg IV before or with the first antibiotic dose if bacterial meningitis suspected (especially pneumococcal) [1]
- If red flags present (immunocompromised, new seizures, GCS under 12, focal neurology, papilloedema) — CT before LP, but antibiotics already started
- Lumbar puncture — unless contraindicated; send for cell count, glucose, protein, Gram stain, culture, multiplex PCR
- De-escalate therapy when organism and sensitivities available
Empiric antibiotic regimens by age and risk
| Patient group | Empiric regimen |
|---|---|
| Immunocompetent adult, 2 to 50 years | Ceftriaxone 2 g IV 12-hourly + vancomycin (15 to 20 mg/kg 12-hourly; target trough 15 to 20) |
| CSF shunt or post-neurosurgery | Vancomycin + ceftazidime 2 g IV 8-hourly (covers pseudomonas; ceftriaxone does not) |
| Severe penicillin allergy | Vancomycin + meropenem 2 g IV 8-hourly (covers Listeria and most bacteria); consult ID |
| Suspected encephalitis (any of the above) | Add aciclovir 10 mg/kg IV 8-hourly until HSV PCR negative |
DWE high-yield trap: The most commonly tested empiric therapy error is failing to add ampicillin for Listeria cover in a patient over 50, an alcoholic, or an immunocompromised patient. Listeria monocytogenes is intrinsically resistant to all cephalosporins — ceftriaxone alone will not treat it. Ampicillin (or penicillin, or trimethoprim-sulfamethoxazole) is required. [1]
Dexamethasone — the what, when, and for whom
Dexamethasone 10 mg IV every 6 hours for 4 days is adjunctive therapy in suspected bacterial meningitis. The landmark trial by de Gans and van de Beek (2002) showed that dexamethasone given before or with the first antibiotic dose reduced unfavourable outcomes (from 25 to 15 per cent overall) and was most effective in pneumococcal meningitis (unfavourable outcomes reduced from 52 to 26 per cent; mortality reduced from 34 to 14 per cent) [1]. The 2015 Cochrane review confirmed benefit in high-income countries, particularly for hearing loss and neurological sequelae [4].
Key rules for dexamethasone:
- Give it before or with the first antibiotic dose — this is when the benefit accrues. Giving it later (after antibiotics) is too late because the inflammatory burst from bacterial lysis has already occurred
- Continue for 4 days if the organism is S. pneumoniae. If the organism is N. meningitidis or the diagnosis is not bacterial meningitis, stop the dexamethasone
- Do not give dexamethasone if you have already given antibiotics more than 1 to 2 hours ago — there is no benefit and it may mask other diagnoses [1]
DCE viva answer pattern: "I would give dexamethasone 10 mg IV immediately, before the first dose of ceftriaxone, because the de Gans trial showed that the benefit is greatest when the steroid is given before antibiotic-induced bacterial lysis triggers the inflammatory cascade. I would continue it for 4 days if the Gram stain or culture confirms pneumococcal meningitis, and stop it otherwise." [1]
Aciclovir in suspected encephalitis — the default is to give it
Aciclovir 10 mg/kg IV every 8 hours (dose-adjusted for renal function) should be started empirically in any patient with suspected encephalitis — fever with altered mental status, seizures, or focal neurology — and continued until HSV PCR is negative. The rationale: [1]
- Untreated HSV encephalitis has a mortality of over 70 per cent
- Aciclovir reduces mortality to approximately 20 to 30 per cent [6]
- The HSV PCR may be negative in the first 24 to 48 hours, so a single negative PCR does not exclude HSV
- Aciclovir is safe and relatively inexpensive — the risk of treating a patient who does not have HSV is far lower than the risk of not treating one who does
Duration: If HSV PCR is negative at 3 to 7 days, stop aciclovir. If HSV PCR is positive, continue for 14 to 21 days [8].
Aciclovir cautions:
- Nephrotoxicity — aciclovir crystallises in renal tubules. Ensure adequate hydration and monitor creatinine. Dose-adjust for renal function
- Neurotoxicity — tremor, confusion, lethargy; may mimic encephalitis. Consider if patient deteriorates on aciclovir [1]
Targeted therapy by organism
Once the organism is identified, de-escalate to targeted therapy. Know the durations. [1]
| Organism | Targeted therapy | Duration |
|---|---|---|
| S. pneumoniae (penicillin-sensitive) | Benzylpenicillin 2.4 g IV 4-hourly or ceftriaxone 2 g IV 12-hourly | 10 to 14 days |
| N. meningitidis | Ceftriaxone 2 g IV 12-hourly (or benzylpenicillin if sensitive) | 7 days |
| L. monocytogenes | Ampicillin 2 g IV 4-hourly (+/- gentamicin for first week) | 21 days (at least) |
| Group B strep | Benzylpenicillin or ampicillin | 14 to 21 days |
| Gram-negative (non-pseudomonas) | Ceftriaxone | 7 to 14 days |
| Pseudomonas | Ceftazidime or cefepime | 21 days |
| MSSA | Flucloxacillin or nafcillin | 14 to 28 days |
| MRSA | Vancomycin | 14 to 28 days |
Chemoprophylaxis and public health
Meningococcal disease — chemoprophylaxis for contacts
Meningococcal disease is spread by respiratory droplets and is contagious. Close contacts of a confirmed case require chemoprophylaxis to eradicate nasopharyngeal carriage and prevent secondary cases. [1]
Who needs prophylaxis (high-risk contacts):
- Household contacts — the highest risk group; risk is 500 to 1000 times baseline in the first few days
- Kissing contacts
- Healthcare workers who performed mouth-to-mouth resuscitation or had direct exposure to respiratory secretions without appropriate PPE
- Index case — the patient themselves should receive chemoprophylaxis before discharge (if treated with ceftriaxone, this is already covered; if treated with penicillin only, give prophylaxis) [1]
Who does NOT need prophylaxis:
- Casual contacts (school classmates, work colleagues without close exposure)
- Healthcare workers who used standard precautions [1]
Prophylaxis regimens: [1]
| Drug | Dose | Notes |
|---|---|---|
| Ciprofloxacin | 500 mg orally as a single dose (adults); 250 mg if bodyweight under 35 kg | Preferred in ANZ/UK — single dose, well tolerated. Not in pregnancy or children where alternatives exist |
| Rifampicin | 600 mg orally every 12 hours for 2 days (adults); 5 mg/kg (under 1 month), 10 mg/kg (1 to 12 months), 20 mg/kg (over 1 month) every 12 hours for 2 days | Traditional agent; induces hepatic enzymes (reduces OCP, warfarin effectiveness); stains contact lenses orange |
| Ceftriaxone | 250 mg IM single dose (adults); 125 mg if under 12 years | Preferred in pregnancy (no teratogenic risk) |
DWE high-yield: Chemoprophylaxis should be given as soon as possible (ideally within 24 hours of the index case's diagnosis) to all high-risk contacts. Notify public health immediately — meningococcal disease is a notifiable disease in Australia, New Zealand, the UK, and most jurisdictions. [1]
Pneumococcal and Hib prophylaxis
Chemoprophylaxis is not routinely recommended for contacts of pneumococcal or Hib meningitis (the risk of secondary cases is much lower than meningococcus). The exception is unvaccinated young children exposed to Hib — they may need rifampicin prophylaxis. [1]
Vaccines — prevention
The dramatic decline in bacterial meningitis over the past 30 years is largely due to vaccination. [1]
| Vaccine | Target organism | Schedule (ANZ) |
|---|---|---|
| Conjugated pneumococcal (PCV13) | S. pneumoniae (13 serotypes) | Part of childhood schedule; recommended in adults over 65 and immunocompromised |
| Meningococcal ACWY conjugate | N. meningitidis serogroups A, C, W, Y | Childhood + adolescent; travellers (Hajj, sub-Saharan Africa "meningitis belt"); asplenia, complement deficiency |
| Meningococcal B (4CMenB / Bexsero) | N. meningitidis serogroup B (the most common in ANZ) | At-risk groups; some funded programmes for infants and adolescents |
| Hib conjugate | H. influenzae type b | Part of childhood schedule (6 weeks, 4 months, 12 months in ANZ) |
| BCG (TB) | M. tuberculosis (variable efficacy against meningitis) | At-risk neonates in some countries; not routine in Australia |
Clinical pearl: Patients with asplenia, complement deficiency (C5-C9), or on eculizumab (anti-C5 monoclonal, used in paroxysmal nocturnal haemoglobinuria and atypical HUS) are at markedly increased risk of meningococcal disease. These patients must receive both MenACWY and MenB vaccines, be educated about the risk, and carry emergency antibiotics (e.g., amoxicillin 3 g PO stat) for immediate self-treatment at first sign of fever. [1]
Tuberculous meningitis — management
TB meningitis is the most severe form of extrapulmonary TB, with untreated mortality approaching 100 per cent. The diagnostic challenge is that the CSF AFB smear is positive in only 10 to 20 per cent of cases, and culture takes 2 to 6 weeks. Xpert MTB/RIF (a rapid PCR that detects M. tuberculosis DNA and rifampicin resistance in 2 hours) has improved early diagnosis but has moderate sensitivity (approximately 60 to 80 per cent) — a negative Xpert does not exclude TB meningitis [12].
Empiric anti-TB therapy should be started on clinical suspicion (subacute presentation, characteristic CSF, high-risk exposure) — do not wait for culture confirmation. The standard regimen: [1]
- Intensive phase (2 months): Isoniazid, rifampicin, pyrazinamide, ethambutol (all four)
- Continuation phase (7 to 10 months): Isoniazid + rifampicin
- Total duration: 9 to 12 months [1]
Adjunctive corticosteroids: The Thwaites trial (2004) showed that dexamethasone reduced mortality in TB meningitis (relative risk of death 0.69) without significantly improving severe disability among survivors [12]. Dexamethasone is now standard for TB meningitis, tapered over 6 to 8 weeks. The regimen (for adults, Grade II/III disease): dexamethasone 0.4 mg/kg/day, tapering weekly.
Additional considerations:
- Pyridoxine (vitamin B6) with isoniazid to prevent peripheral neuropathy
- Monitor LFTs — rifampicin, isoniazid, and pyrazinamide are all hepatotoxic
- Manage raised ICP and hydrocephalus — may require shunt or repeated LP
- Drug resistance — if MDR-TB suspected (prior TB treatment, contact with MDR-TB, or rifampicin resistance on Xpert), involve a TB specialist and adjust regimen [1]
Cryptococcal meningitis — management
Management of cryptococcal meningitis has three pillars: antifungal therapy, intracranial pressure control, and management of immune reconstitution [13].
Antifungal therapy — three phases
| Phase | Therapy | Duration |
|---|---|---|
| Induction (sterilise CSF) | Liposomal amphotericin B 3 to 4 mg/kg IV daily + flucytosine 25 mg/kg 6-hourly orally | 2 weeks (HIV); 4 to 6 weeks (non-HIV) |
| Consolidation | Fluconazole 400 to 800 mg orally daily | 8 weeks |
| Maintenance (suppression) | Fluconazole 200 mg orally daily | Until immune reconstitution (CD4 above 100 for 6 months in HIV) or 6 to 12 months (transplant) |
Key points:
- The combination of amphotericin + flucytosine is fungicidal and clears CSF faster than amphotericin alone
- Monitor flucytosine levels — toxicity (bone marrow suppression) is dose-related; keep trough under 40 mg/L
- Liposomal amphotericin is preferred over amphotericin deoxycholate for lower nephrotoxicity; pre-hydrate and monitor creatinine, potassium, and magnesium [1]
Intracranial pressure control — the often-missed pillar
Raised intracranial pressure is the dominant cause of morbidity and mortality in cryptococcal meningitis. Measure opening pressure at every LP. If raised (above 25 cm of water): [1]
- Daily therapeutic LP — drain CSF to reduce pressure to under 20 cm or by 50 per cent
- If daily LPs are inadequate, consider lumbar drain or ventriculoperitoneal shunt
- Acetazolamide has limited efficacy and is not routinely recommended
- Mannitol and hypertonic saline for acute decompensation [1]
Immune reconstitution inflammatory syndrome (IRIS)
In HIV-positive patients starting antiretroviral therapy (ART), or transplant patients reducing immunosuppression, the recovering immune system can mount an intense inflammatory response to cryptococcal antigens — IRIS. This presents as worsening meningitis symptoms, raised CSF white cells (often neutrophilic), and raised pressure, despite sterile CSF cultures. Management: corticosteroids (short course) and continue ART (do not stop unless severe). [1]
Autoimmune encephalitis — management
The Graus 2016 diagnostic criteria define autoimmune encephalitis as possible, probable, or definite, allowing early immunotherapy before antibody results return (which can take weeks) [10].
Criteria for possible autoimmune encephalitis (all three):
- Subacute onset (under 3 months) of working memory deficits, altered mental status, or psychiatric symptoms
- At least one of: new focal CNS findings, seizures not explained by prior epilepsy, CSF pleocytosis, or MRI features of inflammation
- Reasonable exclusion of alternative causes [1]
Management:
- First-line immunotherapy: Methylprednisolone 1 g IV daily for 3 to 5 days, +/- IV immunoglobulin (0.4 g/kg/day for 5 days) and/or plasma exchange (5 sessions)
- Second-line (if no response in 1 to 2 weeks): Rituximab (anti-CD20) and/or cyclophosphamide
- Tumour search and removal: Anti-NMDAR — search for ovarian teratoma (pelvic ultrasound, MRI). Anti-LGI1, anti-CASPR2, anti-Hu, anti-Yo — search for small cell lung cancer, breast cancer, thymoma. Removal of the associated tumour dramatically improves outcome [14]
- Supportive care — ICU for autonomic instability, hypoventilation, and seizures (often refractory)
DCE viva pattern: "In a patient with suspected encephalitis who is not improving on aciclovir after 48 hours, I would broaden the differential to include autoimmune encephalitis. I would send a panel of neuronal surface and intracellular antibodies (CSF and serum), screen for an occult tumour (CT chest/abdomen/pelvis, pelvic ultrasound/MRI for ovarian teratoma), and start empiric immunotherapy with high-dose methylprednisolone while awaiting results. The Graus 2016 criteria allow a clinical diagnosis of probable autoimmune encephalitis without waiting for antibody results." [1]
Complications
Cerebral oedema and raised intracranial pressure
Inflammatory cerebral oedema (cytotoxic and vasogenic) develops within hours of severe bacterial meningitis. Signs: deteriorating GCS, bradycardia with hypertension (Cushing reflex), pupillary changes, and respiratory irregularity. Management: head elevation to 30 degrees, hypertonic saline or mannitol, intubation and ventilation with sedation, and in refractory cases, decompressive craniectomy. [1]
Seizures
Seizures occur in approximately 15 to 30 per cent of bacterial meningitis and are more common in HSV encephalitis and TB meningitis (especially with infarction). They may be focal or generalised and may be non-convulsive (suspect if GCS is lower than expected or if there is delayed recovery). Treat with standard antiseizure medication (levetiracetam, valproate, phenytoin). Non-convulsive status epilepticus requires EEG confirmation and continuous infusion therapy (midazolam, propofol). [1]
SIADH and hyponatraemia
The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is common in bacterial meningitis (and TB meningitis in particular), causing hyponatraemia. Monitor sodium daily. Avoid hypo-osmolar fluids. Treat significant hyponatraemia (sodium under 125 mmol/L) with hypertonic saline or fluid restriction. Correct sodium no faster than 8 mmol/L in 24 hours to avoid osmotic demyelination. [1]
Sensorineural hearing loss
Hearing loss occurs in approximately 10 to 30 per cent of bacterial meningitis survivors — from inflammation of the cochlea and eighth cranial nerve. It is most common with pneumococcal meningitis. Dexamethasone reduces the risk [4]. All survivors of bacterial meningitis should have formal audiometry before discharge and at 6 weeks.
Cognitive impairment and behavioural change
Cognitive impairment — affecting memory, attention, and executive function — is common after severe meningitis and encephalitis, particularly HSV. Neuropsychological assessment at 3 to 6 months. Behavioural disturbance (impulsivity, aggression, apathy) may persist for months and require psychological and psychiatric support. [1]
Cortical vein and dural sinus thrombosis
Meningeal inflammation can extend into cortical veins and dural sinuses, causing venous sinus thrombosis — presenting with seizures, focal neurology, or haemorrhagic infarction. Diagnose with MR or CT venography. Anticoagulate (even with haemorrhagic infarction, the evidence favours anticoagulation). [1]
Cranial nerve palsies
CN III, IV, VI (ophthalmoplegia), CN VII (facial palsy), and CN VIII (hearing loss) may be affected by basilar meningitis (TB, cryptococcal, bacterial). Many recover with treatment of the underlying infection. [1]
Hydrocephalus
Obstructive (from basal exudate in TB meningitis) or communicating (from impaired CSF reabsorption) hydrocephalus may require external ventricular drain or shunt. Suspect if GCS is worsening with normal imaging of parenchyma — a shunt series or CT may show dilated ventricles. [1]
Prognosis
| Condition | Mortality | Major morbidity |
|---|---|---|
| Pneumococcal meningitis | 20 to 30 per cent | Hearing loss, cognitive impairment, seizures |
| Meningococcal meningitis (with septicaemia) | 10 to 15 per cent (higher in septicaemia) | Amputations, skin scarring, hearing loss, renal failure |
| Meningococcal meningitis (meningitis alone) | Under 5 per cent | Hearing loss |
| Listeria meningitis | 20 to 30 per cent (higher in immunocompromised) | Cognitive impairment, seizures |
| HSV encephalitis (treated) | 20 to 30 per cent | Cognitive impairment (especially memory), seizures, behavioural change |
| HSV encephalitis (untreated) | Over 70 per cent | Severe disability in survivors |
| Tuberculous meningitis | 10 to 30 per cent (stage-dependent) | Stroke, cranial nerve palsies, hydrocephalus, cognitive impairment |
| Cryptococcal meningitis (HIV) | 10 to 20 per cent (treated) | Visual loss, cognitive impairment |
| Anti-NMDAR encephalitis | Under 10 per cent (with treatment) | Cognitive impairment, persistent seizures, psychiatric disturbance |
Predictors of poor outcome in bacterial meningitis: age over 60, reduced GCS at presentation, seizures within 24 hours, hypotension, pneumococcal aetiology, low CSF white cell count (paradoxically — reflects poor immune response or overwhelming infection), and delay in antibiotic administration [2].
DCE long-case approach
Opening statement (SASPOP)
"Mr Williams is a 68-year-old retired engineer who presents with a 2-day history of fever, severe headache, and progressive confusion. He was brought to the emergency department by his wife after he became unresponsive this morning. [1]
He has a background of type 2 diabetes, chronic lymphocytic leukaemia (on rituximab), and a mechanical aortic valve (on warfarin). [1]
His main problems are:
- Acute community-acquired bacterial meningitis, likely pneumococcal, in an immunocompromised patient — immediate empiric therapy required
- Reduced GCS (12) requiring CT before LP — antibiotics must not be delayed
- Listeria risk (immunocompromised, over 50) — empiric therapy must include ampicillin
- Anticoagulation (warfarin) — complicates LP and warrants reversal strategy
- Immunocompromise from rituximab — broader empiric cover and low threshold for cryptococcal testing
- Risk of complications — SIADH, seizures, hearing loss, cognitive impairment [1]
My immediate plan is to start ceftriaxone, vancomycin, ampicillin, and dexamethasone, obtain blood cultures, perform CT then LP, add aciclovir given his encephalopathic presentation, and involve the intensive care team." [1]
Integrated management plan
Present in three phases: [1]
- Immediate (minutes): Airway and breathing (oxygen, intubation if GCS under 8 or unable to protect airway). IV access. Blood cultures x2. Empiric therapy immediately — ceftriaxone 2 g IV + vancomycin + ampicillin 2 g IV (Listeria cover for immunocompromised) + dexamethasone 10 mg IV before antibiotics + aciclovir 10 mg/kg IV (encephalopathic). Check glucose (exclude hypoglycaemia as mimic). Send cryptococcal antigen (immunocompromised).
- First hour: CT head before LP (immunocompromised, GCS under 12). Address warfarin — if INR above 1.4, give vitamin K and consider prothrombin complex concentrate to permit LP. Admit to ICU for monitoring.
- Definitive (hours to days): LP and CSF analysis. De-escalate antibiotics based on Gram stain, culture, PCR. Add vancomycin + ceftazidime if shunt or post-neurosurgery. Continue dexamethasone for 4 days if pneumococcal. Screen for and manage complications: daily sodium (SIADH), audiometry, EEG if seizures or not improving, MRI if focal neurology. Public health notification if meningococcal. Vaccination advice and immunisation review. [1]
DCE examiner probing questions to anticipate:
- "Why ampicillin?" — Listeria cover; cephalosporins do not cover Listeria.
- "He is on warfarin. How do you manage his LP?" — Reverse with vitamin K and PCC if INR above 1.4; delay LP if possible but do not delay antibiotics.
- "His CSF shows lymphocytic pleocytosis with low glucose. What is your differential?" — TB, fungal, partially-treated bacterial, Listeria, viral. Send TB PCR, cryptococcal antigen, repeat CSF.
- "His cryptococcal antigen is positive. What changes?" — Add liposomal amphotericin + flucytosine, manage raised ICP with therapeutic LP, involve ID. [1]
DCE short-case approach: neurological examination in suspected CNS infection
Instruction: "Examine this patient's neurological system." [1]
Systematic routine (general, mental state, cranial nerves, motor, sensory, coordination, gait, neck)
- End of bed: Observe the level of alertness, posture, abnormal movements, respiratory pattern. Note any photophobia, neck retraction, or signs of sepsis (cool peripheries, mottled skin).
- Mental state and GCS: Document GCS precisely (eye, verbal, motor). Assess orientation, attention (serial 7s), and higher cognitive function. Note confusion or behavioural change.
- Neck: Test for neck stiffness (passive flexion — inability to touch chin to chest), Kernig sign (with hip flexed 90 degrees, attempt to extend knee — resistance or pain indicates meningeal irritation), and Brudzinski sign (flexion of neck causes involuntary hip and knee flexion).
- Cranial nerves: Document any cranial nerve palsies (CN III, IV, VI, VII, VIII). Check fundoscopy for papilloedema (raised ICP). Test hearing (whisper test — hearing loss post-meningitis).
- Motor: Tone, power (MRC scale), reflexes, plantar responses. Look for focal weakness (vasculitic stroke in TB or bacterial meningitis).
- Sensory: Pinprick, light touch, vibration, joint position. Focal sensory loss suggests stroke or abscess.
- Coordination: Finger-nose, heel-shin, rapid alternating movements. Ataxia suggests cerebellar involvement or vestibular neuritis (varicella, Lyme).
- Gait: If able to walk — assess for ataxia (cerebellar, vestibular, or sensory). [1]
Presentation template
"I examined Mrs Patel's neurological system. She is drowsy but rousable, GCS 13 (E3, V4, M6). She has marked neck stiffness with a positive Kernig sign. On fundoscopy there is no papilloedema. [1]
Cranial nerve examination reveals a left VI nerve palsy. Motor examination shows normal tone and power 5/5 in all four limbs, with symmetric reflexes and downgoing plantars. Sensation is intact. Coordination and gait could not be fully assessed due to drowsiness. [1]
These findings — fever, meningism, altered mental status, and a sixth nerve palsy — are consistent with meningoencephalitis. The VI nerve palsy may be a false-localising sign from raised intracranial pressure. I would urgently investigate with blood cultures, CT head, lumbar puncture, and start empiric ceftriaxone, vancomycin, aciclovir, and dexamethasone." [1]
Key DWE MCQ patterns
- Empiric therapy in the over-50 / immunocompromised: Add ampicillin (Listeria cover) to ceftriaxone + vancomycin. The most commonly tested error is omitting ampicillin.
- Dexamethasone timing: Must be before or with the first antibiotic dose. Giving it after antibiotics provides no benefit in pneumococcal meningitis.
- CSF pattern recognition: Neutrophils + low glucose + high protein = bacterial. Lymphocytes + normal glucose = viral. Lymphocytes + very low glucose + very high protein = TB or fungal.
- HSV PCR false negative: Early in disease (first 24 to 48 hours). Repeat at 3 to 7 days if suspicion high. Do not stop aciclovir based on an early negative PCR.
- CT before LP indications: Immunocompromised, new seizures, GCS under 12, focal neurology, papilloedema. But never delay antibiotics for CT.
- Meningococcal chemoprophylaxis: Ciprofloxacin 500 mg PO stat or rifampicin for household and kissing contacts; index case needs prophylaxis if treated with penicillin alone. [1]7. Anti-NMDAR encephalitis: Young woman with new psychiatric symptoms, seizures, and orofacial dyskinesia. Search for ovarian teratoma. Treat with immunotherapy.
- Cryptococcal meningitis opening pressure: Raised pressure (above 25 cm of water) requires therapeutic LP; blindness and death from uncontrolled intracranial hypertension.
- Aciclovir dose in HSV encephalitis: 10 mg/kg IV every 8 hours for 14 to 21 days. Dose-adjust for renal function.
- Lumbar puncture interpretation after antibiotics: May shift to lymphocytic and be culture-negative. PCR (DNA-based) is more useful. [1]
References
[1] de Gans & van de Beek (2002) — Dexamethasone before or with first antibiotic dose in adults with bacterial meningitis; unfavourable outcomes reduced from 25 to 15 per cent overall, and from 52 to 26 per cent in pneumococcal meningitis. [2] van de Beek et al. (2004) — Clinical features and prognostic factors in adults with bacterial meningitis; the classical triad present in only 44 per cent; absence of all three excludes meningitis with 99 per cent NPV. [3] van de Beek et al. (2006) — NEJM review of community-acquired bacterial meningitis in adults; organisms, pathophysiology, management framework. [4] Brouwer et al. (2015) — Cochrane review of corticosteroids in acute bacterial meningitis; benefit confirmed in high-income countries, especially for pneumococcus and for reducing hearing loss. [5] Tunkel et al. (2004) — IDSA practice guidelines for the management of bacterial meningitis; empiric therapy by age and risk, CT-before-LP indications, duration of therapy. [6] Whitley et al. (1986) — Aciclovir vs vidarabine in HSV encephalitis; aciclovir reduced mortality from 54 to 28 per cent; established aciclovir as the treatment of choice. [7] Lakeman & Whitley (1995) — CSF HSV PCR sensitivity 98 per cent, specificity 94 per cent vs brain biopsy; replaced biopsy as the diagnostic standard for HSV encephalitis. [8] Tunkel et al. (2008) — IDSA guidelines for the management of encephalitis; empiric aciclovir for suspected encephalitis; 14 to 21 days for confirmed HSV; EEG for non-convulsive seizures. [9] Venkatesan et al. (2013) — International Encephalitis Consortium consensus; case definitions and diagnostic algorithms for encephalitis. [10] Graus et al. (2016) — Clinical approach to diagnosis of autoimmune encephalitis; possible, probable, and definite criteria; allows early immunotherapy before antibody results. [11] Dalmau et al. (2008) — Anti-NMDA receptor encephalitis case series of 100 patients; clinical features, antibody effects, association with ovarian teratoma. [12] Thwaites et al. (2004) — Dexamethasone in tuberculous meningitis; reduced mortality (relative risk 0.69) without reducing severe disability; standard adjunctive therapy. [13] Perfect et al. (2010) — IDSA guidelines for cryptococcal disease; amphotericin + flucytosine induction, fluconazole consolidation and maintenance, intracranial pressure management. [14] Dalmau et al. (2007) — Paraneoplastic anti-NMDA receptor encephalitis associated with ovarian teratoma; the seminal description of the syndrome.
IDSA Practice Guidelines for Bacterial Meningitis (Tunkel et al., 2004); IDSA Guidelines for the Management of Encephalitis (Tunkel et al., 2008); IDSA Guidelines for Cryptococcal Disease (Perfect et al., 2010); Therapeutic Guidelines Australia — Antibiotic (CNS infections); NICE CKS — Meningitis (bacterial) and meningococcal septicaemia. [1]
References
- [1]de Gans J, van de Beek D Dexamethasone in adults with bacterial meningitis N Engl J Med, 2002.PMID 12432041
- [2]van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M Clinical features and prognostic factors in adults with bacterial meningitis N Engl J Med, 2004.PMID 15509818
- [3]van de Beek D, de Gans J, Tunkel AR, Wijdicks EFM Community-acquired bacterial meningitis in adults N Engl J Med, 2006.PMID 16394301
- [4]Brouwer MC, McIntyre P, Prasad K, van de Beek D Corticosteroids for acute bacterial meningitis Cochrane Database Syst Rev, 2015.PMID 26362566
- [5]Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis Clin Infect Dis, 2004.PMID 15494903
- [6]Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis N Engl J Med, 1986.PMID 3001520
- [7]Lakeman FD, Whitley RJ Diagnosis of herpes simplex encephalitis: application of polymerase chain reaction to cerebrospinal fluid from brain-biopsied patients and correlation with disease. National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group J Infect Dis, 1995.PMID 7706811
- [8]Tunkel AR, Glaser CA, Bloch KC, et al. The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America Clin Infect Dis, 2008.PMID 18582201
- [9]Venkatesan A, Tunkel AR, Bloch KC, et al. Case definitions, diagnostic algorithms, and priorities in encephalitis: consensus statement of the international encephalitis consortium Clin Infect Dis, 2013.PMID 23861361
- [10]Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis Lancet Neurol, 2016.PMID 26906964
- [11]Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies Lancet Neurol, 2008.PMID 18851928
- [12]Thwaites GE, Nguyen DB, Nguyen HD, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults N Engl J Med, 2004.PMID 15496623
- [13]Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america Clin Infect Dis, 2010.PMID 20047480
- [14]Dalmau J, Tuzun E, Wu HY, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma Ann Neurol, 2007.PMID 17262855