Phys · neurological
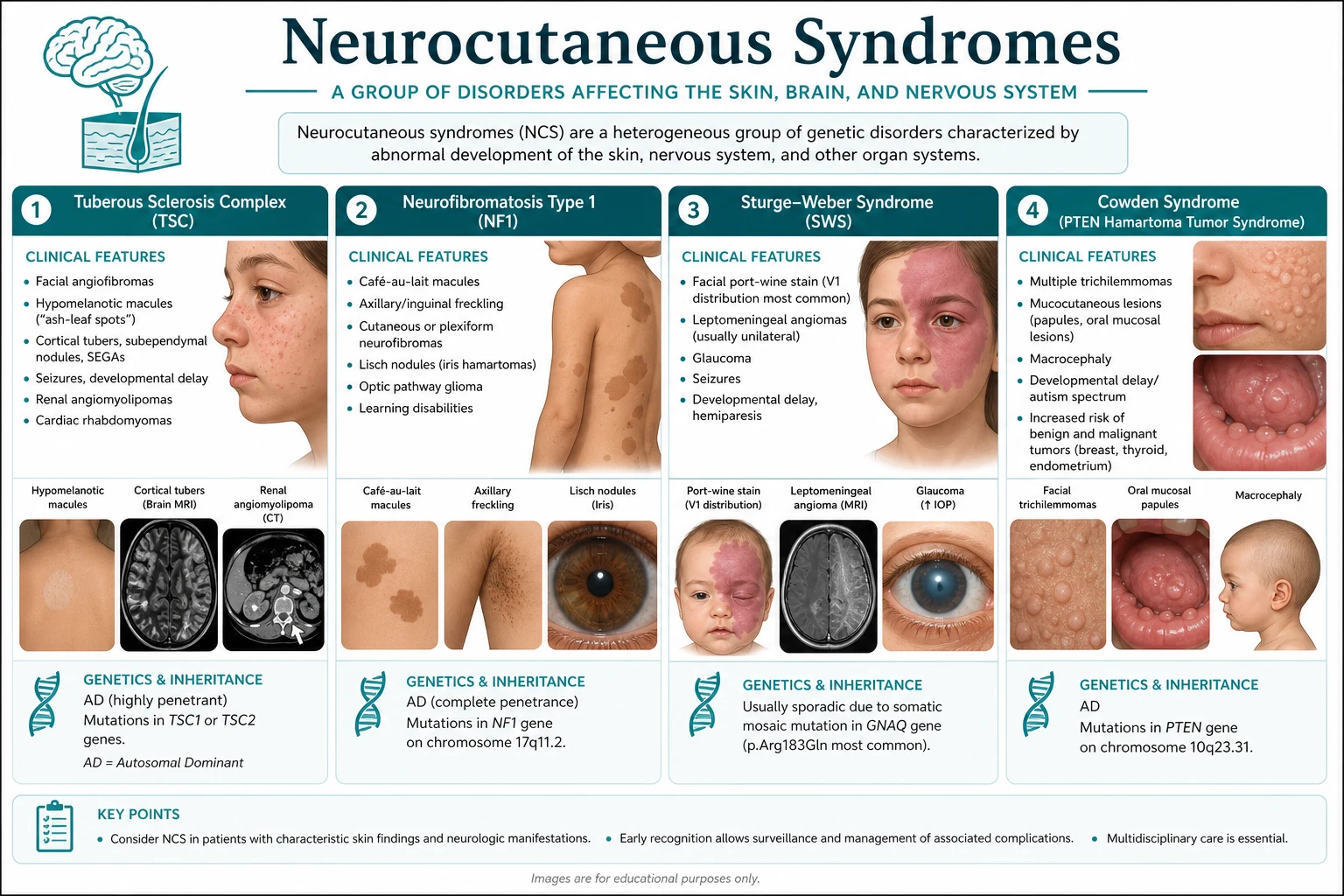
Neurocutaneous Syndromes
Also known as Neurocutaneous Syndromes · neurocutaneous syndromes
Consultant-physician depth guide to Neurocutaneous Syndromes for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
Neurocutaneous Syndromes is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
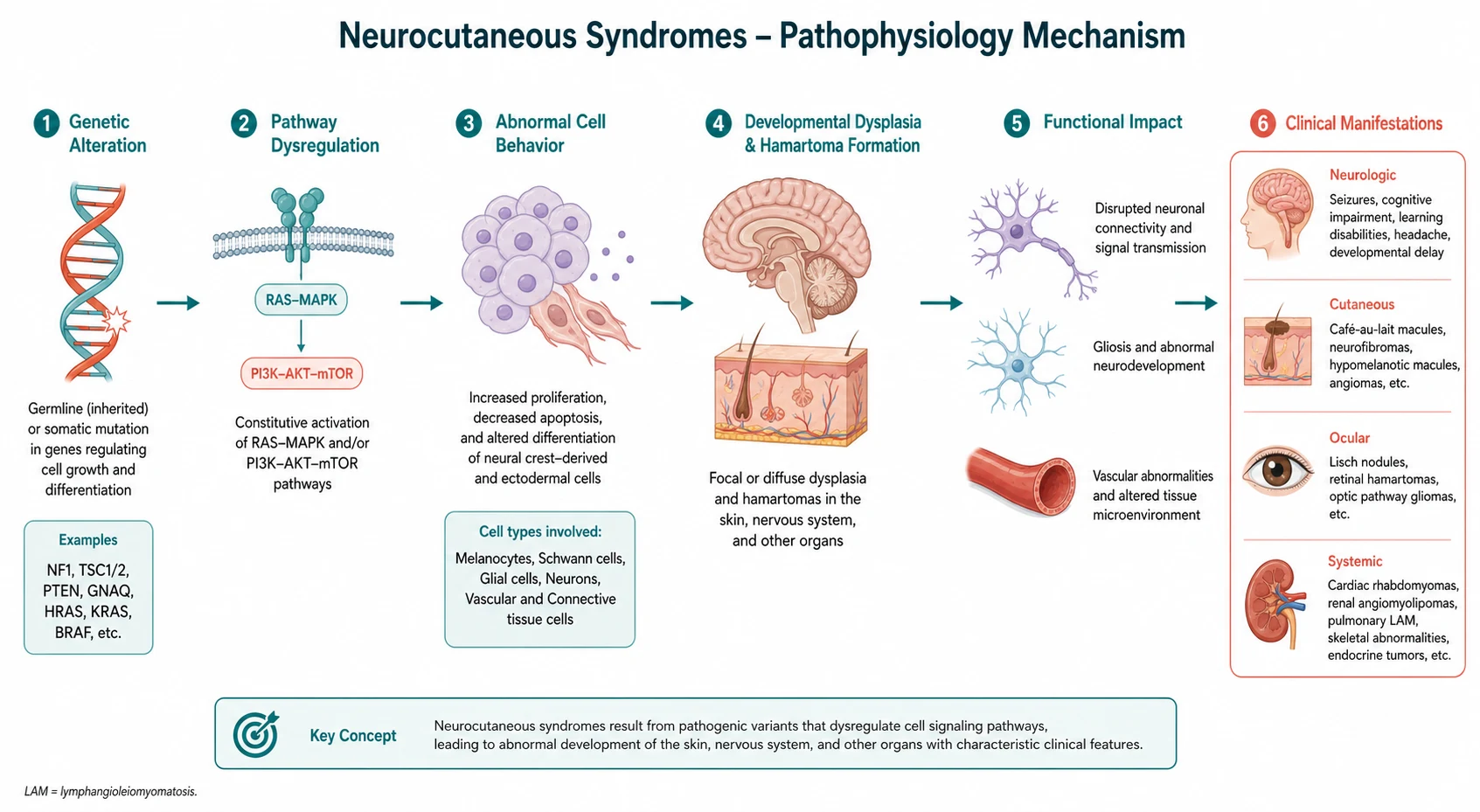
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
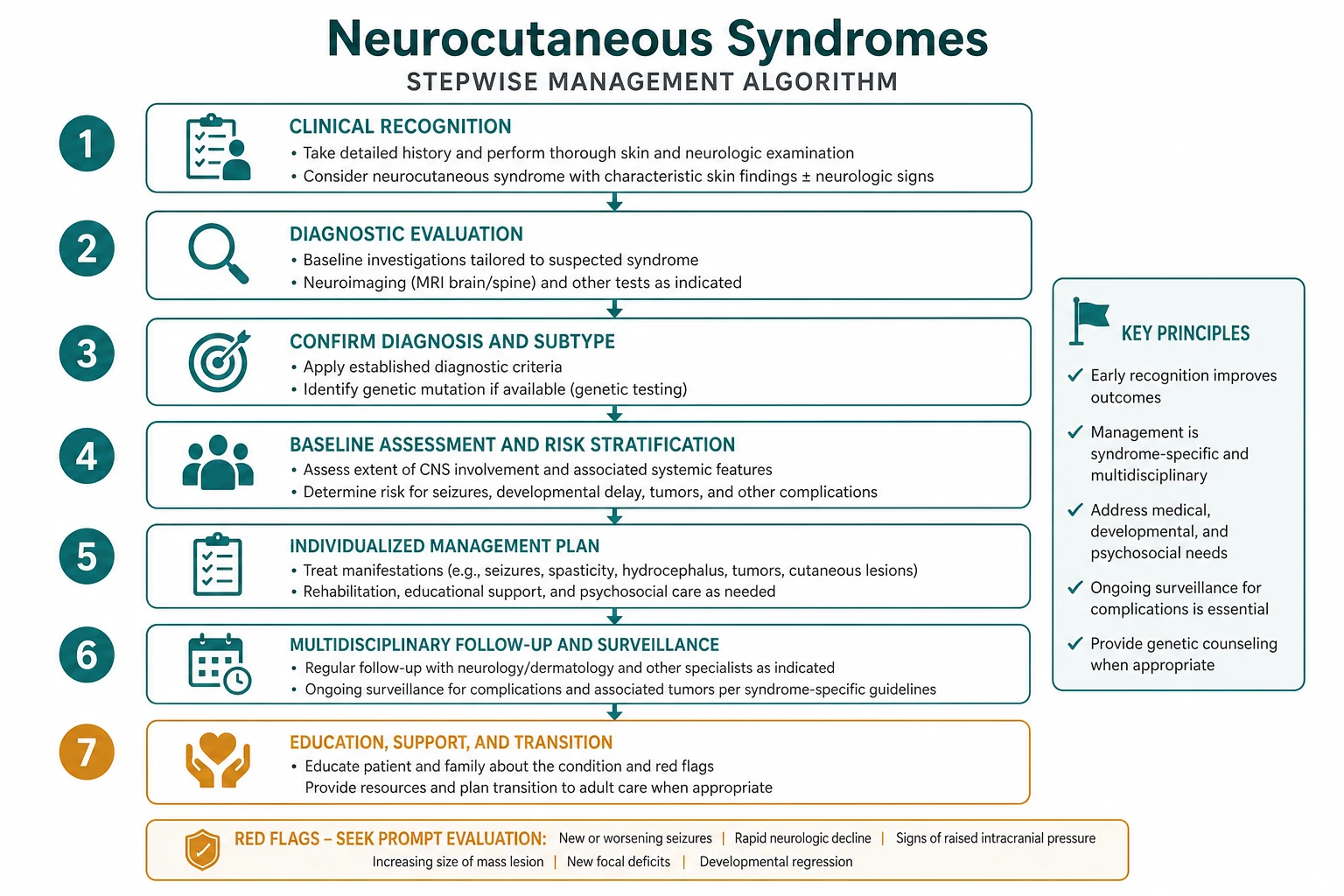
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]
Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Neurocutaneous Syndromes to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Zhang S, Yang G Neurofibromin in bone disease: Mechanisms and therapeutic implications (Review) Int J Mol Med, 2026.PMID 42464674
- [2]Calonge Q, Hanin A, Dade M, Bailly L, et al. Epilepsy and disability in adults with tuberous sclerosis complex: a 16-year retrospective analysis J Neurol, 2026.PMID 42458074
- [3]Zeppieri M, D'Esposito F, Gagliano C, Battista M, et al. Looking at Optic Nerve Sheath Meningiomas Through Genetics-From Clinic to Bench and Back Again Front Biosci (Schol Ed), 2026.PMID 42411653
- [4]Erdem S, Amparore D, Re C, Verep S, et al. What should the urologist know on the management of kidney cancer in patients with Von Hippel-Lindau syndrome? Recommendations of the European Association of Urology (EAU) Young Academic Urologists (YAU) Renal Cancer Working Group World J Urol, 2026.PMID 42373875
- [5]Pawlak KM, Jagielski M, Papanikolaou IS, Hong W, et al. Pancreatic cystic lesions in hereditary syndromes: Diagnostic role of endoscopic ultrasound Best Pract Res Clin Gastroenterol, 2026.PMID 42167859
- [6]Miranda M, Ferreira C, Fernandes M, Lopes F, et al. Hereditary renal cell carcinoma surveillance protocols: a review of the literature and proposed recommendations Fam Cancer, 2026.PMID 41518461
- [7]Xi Y, Yao T, Zhang C, Zhuang T Effectiveness of safety care and clinical nursing pathway in patients undergoing cardiovascular intervention: a randomized controlled trial Perioper Med (Lond), 2026.PMID 42469924
- [8]Marks FJ, Walters SJ, Sutton L, Jacques RM What statistical methods are more appropriate for predicting recruitment at the design stage of a randomised controlled trial? Trials, 2026.PMID 42469922
- [9]Hajiaqaei M, Mohammadi A Transcranial random noise stimulation (tRNS) over the left dorsolateral prefrontal cortex ameliorates emotion dysregulation and executive function: a single-blind, randomized, sham-controlled clinical trial BMC Psychol, 2026.PMID 42469906
- [10]Suaste V, Presterud R, Wennerström AB, Wang HL, et al. Transcriptional Profiling Shows Dampening of Interferon Gene Signatures by NAD(+) Augmentation in Ataxia-Telangiectasia Int J Mol Sci, 2026.PMID 42449929
- [11]Panvino F, Paparella R, Urciuolo G, Galosi S, et al. Pharmacological Treatment of Cerebellar Ataxia in Pediatric Ataxia-Telangiectasia: A Systematic Review Eur J Neurol, 2026.PMID 42387837
- [12]Martakis K, Bremova-Ertl T, Bolton C, Foltan T, et al. Safety and efficacy of levacetylleucine in ataxia-telangiectasia: a phase 3, randomised, double-blind, placebo-controlled crossover trial Lancet Neurol, 2026.PMID 42309084