Phys · neurological
Spinal Cord Disease
Also known as spinal cord compression · myelopathy · malignant spinal cord compression · MSCC · cord syndrome · Brown-Sequard syndrome · anterior cord syndrome · central cord syndrome · syringomyelia · transverse myelitis · subacute combined degeneration · cauda equina syndrome
Consultant-physician-depth guide to spinal cord anatomy, the cord syndromes (complete transection, anterior cord, Brown-Sequard, central cord, posterior column), malignant spinal cord compression with the Patchell criteria, cauda equina syndrome, syringomyelia, transverse myelitis and B12 deficiency subacute combined degeneration — for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Spinal Cord Disease

The answer first
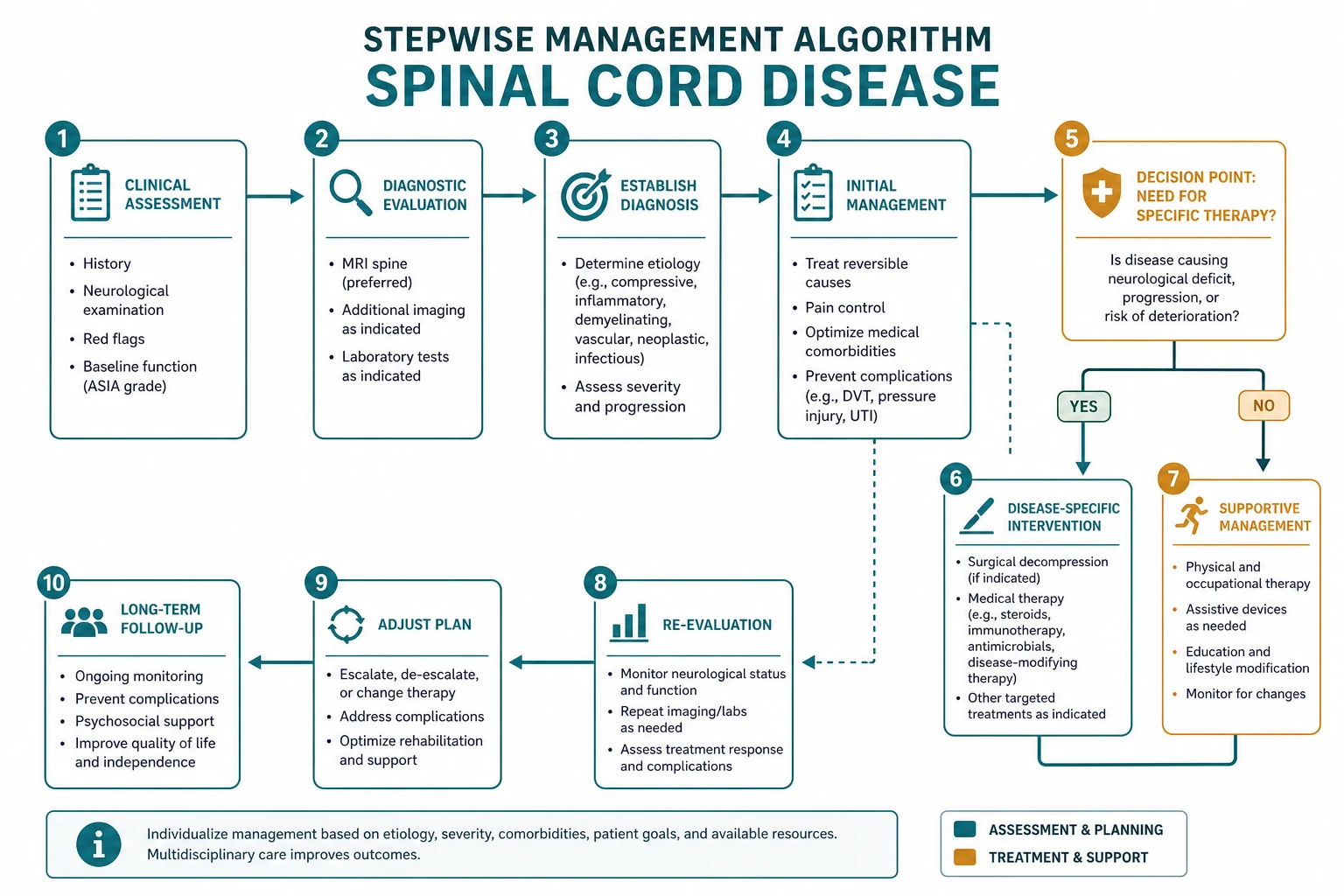
Spinal cord disease is an anatomical diagnosis. The examination alone tells you where the lesion is before any scan. The two questions that determine everything are: where is the level? and is it compressive or not? [1]
The emergencies are three:
- Malignant spinal cord compression (MSCC) — the most common cause in adults. Back pain plus any limb deficit is compression until proven otherwise. Give dexamethasone 16 mg and arrange emergency MRI whole spine within 24 hours.
- Cauda equina syndrome — bilateral leg pain, saddle anaesthesia, sphincter disturbance. Emergency MRI and surgical decompression within 24 to 48 hours.
- Any acute myelopathy that is progressing — compressive causes must be excluded before inflammatory or vascular causes are treated. [1]
The organising principle is the tract map. Know which tract carries which modality, and you can name the syndrome from the bedside: a sensory level with UMN signs below is a cord lesion; dissociated sensory loss (pain and temperature lost, touch preserved) is a central cord lesion; ipsilateral motor and proprioception loss with contralateral pain and temperature loss is Brown-Sequard. [1]
Spinal cord anatomy — the tract map

The ability to read the cord cross-section like a map is the core DCE short-case skill. Three tracts carry the three clinical modalities. If you know which tract is damaged, you can name the syndrome. [1]
The three principal tracts
| Tract | Location in the cord | What it carries | Where it crosses | Clinical effect of a lesion |
|---|---|---|---|---|
| Corticospinal (lateral) | Lateral column | Motor (voluntary movement) | Medulla (pyramidal decussation) | Ipsilateral UMN weakness below the lesion |
| Spinothalamic | Anterolateral column | Pain and temperature | At the spinal level of entry (1 to 2 segments above) | Contralateral loss of pain and temperature below the lesion |
| Dorsal columns (posterior) | Posterior column | Vibration, proprioception, fine touch | Medulla (internal arcuate fibres) | Ipsilateral loss of vibration and proprioception below the lesion |
The decussation point is the key to lateralising the deficit. The corticospinal tract crosses in the medulla, so a cord lesion produces ipsilateral motor weakness. The spinothalamic tract crosses at the level of entry, so a cord lesion produces contralateral pain and temperature loss. The dorsal columns cross in the medulla, so a cord lesion produces ipsilateral loss of vibration and proprioception. [1]
Blood supply
The cord has a segmental arterial supply with two named longitudinal vessels: [1]
| Artery | Territory supplied | Clinical correlate |
|---|---|---|
| Anterior spinal artery (ASA) | Anterior two-thirds of the cord — corticospinal, spinothalamic, anterior horn (LMN) | Occlusion causes anterior cord syndrome — motor and pain/temperature loss, dorsal columns spared |
| Posterior spinal arteries (PSA, paired) | Posterior one-third — dorsal columns | Occlusion is rare and produces isolated dorsal column loss (vibration and proprioception) |
The ASA is fed by segmental radiculomedullary arteries, the largest being the artery of Adamkiewicz (typically entering at T9 to L2 on the left). This single vessel supplies the lower two-thirds of the cord. Occlusion — classically during aortic surgery, dissection, or atherosclerosis — produces an anterior cord syndrome with sudden paraplegia. [1]
DWE high-yield: The ASA territory includes the corticospinal and spinothalamic tracts but spares the dorsal columns. This is why anterior cord syndrome preserves vibration and proprioception — the dorsal columns have a separate (posterior) blood supply. This is the single most tested vascular anatomy fact in cord disease. [1]
Level localisation — the two-segment offset
A clinical sensory level does not correspond exactly to the vertebral body level. The dorsal root enters the cord at a point that is, on average, one to two segments above the overlying vertebral body in the thoracic spine, and the offset is greater in the cervical and lumbar regions (where the cord segments sit higher than the vertebrae). [1]
This matters clinically: a sensory level at T10 dermatome corresponds to a cord lesion around T10, but the compressive mass is often found at the T11 to T12 vertebral body. When requesting MRI, image at least three segments above and below the clinical level, and preferably the whole spine, to avoid missing the lesion. [1]
Conus medullaris versus cauda equina
The spinal cord ends as the conus medullaris at the L1 to L2 vertebral body level in adults. Below this, the canal contains the cauda equina — the lumbosacral nerve roots. A lesion at or above the conus is a cord (UMN) lesion; a lesion below is a root (LMN) lesion. This anatomical fact is the single most important discriminator in the acute myelopathy. [1]
The cord syndromes — recognition from the bedside

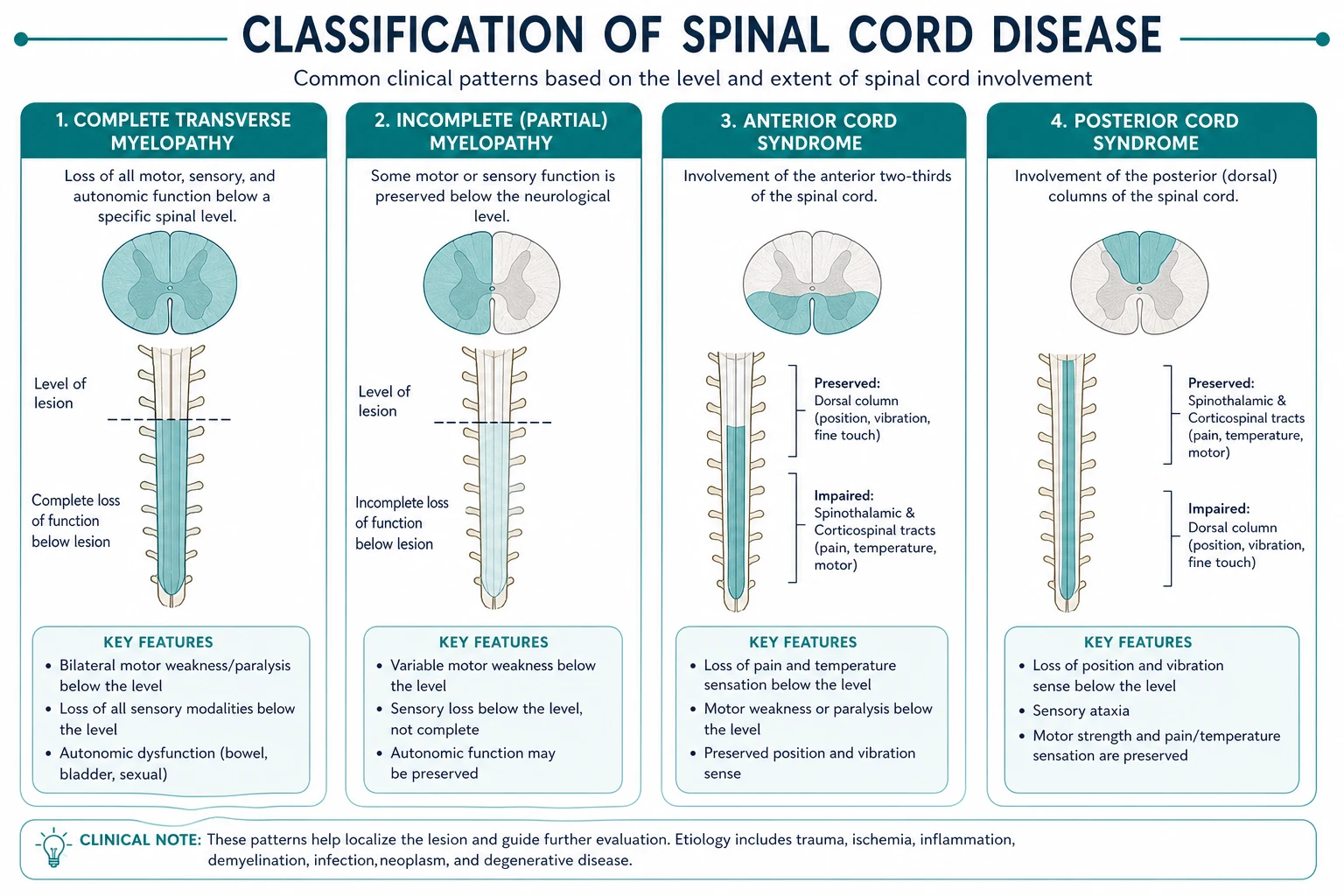
Complete cord transection
A lesion that interrupts all tracts at one level produces: [1]
- Motor: Complete loss of voluntary movement below the level (initially flaccid in spinal shock, then spastic with hyperreflexia and extensor plantar responses as reflex arcs recover over days to weeks).
- Sensory: Complete loss of all modalities below the level. A sharp sensory level is the cardinal sign.
- Sphincter: Urinary retention, constipation, loss of anal tone. [1]
Causes: severe trauma, large compressive mass, transverse myelitis (complete form), cord infarction. Acutely, the patient may be in spinal shock — flaccid paralysis, areflexia, atonic bladder, paralytic ileus — which can mask the UMN nature of the lesion. Do not be reassured by areflexia in an acute cord injury; the reflexes will return. [1]
Anterior cord syndrome (ASA occlusion)
| Feature | Finding |
|---|---|
| Motor (corticospinal) | Bilateral UMN weakness below the lesion |
| Pain and temperature (spinothalamic) | Bilateral loss below the lesion |
| Vibration and proprioception (dorsal columns) | Preserved — the dorsal columns have a separate posterior arterial supply |
| Level sign | Acute back pain at the level (radicular) |
| Cause | Aortic surgery, dissection, atherosclerosis, vasculitis, fibrocartilaginous embolism |
This is the cord syndrome with the worst prognosis for recovery because the mechanism is infarction (irreversible neuronal death), not compression or inflammation. The preservation of dorsal column modalities is the bedside discriminator — test vibration at the sternum and proprioception at the toes. [1]
DCE short-case trap: When examining a patient with an anterior cord syndrome, the examiner will ask "what is preserved?" The answer is vibration and proprioception (dorsal columns). This single finding excludes a complete transection and points to a vascular (ASA territory) cause. State it clearly. [1]
Brown-Sequard syndrome (hemisection)
A lesion affecting one half of the cord produces the classic dissociated pattern: [1]
- Ipsilateral motor weakness (corticospinal tract, already crossed in the medulla)
- Ipsilateral loss of vibration and proprioception (dorsal columns, already crossed)
- Contralateral loss of pain and temperature (spinothalamic tract, crosses at the level of entry, so fibres from the opposite side have already crossed and are damaged) [1]
The lesion is on the side of the motor and dorsal column loss. Pure Brown-Sequard is rare — most lesions are incomplete (Brown-Sequard-plus), but the ipsilateral UMN and contralateral pain-temperature dissociation is the recognisable pattern. [1]
Causes: penetrating trauma (stab wound), unilateral compressive mass, demyelination (MS plaque), radiation myelopathy. It carries the best prognosis of the incomplete cord syndromes because one side of the cord retains some motor and sensory function. [1]
Central cord syndrome
A lesion in the centre of the cord — typically a syrinx (cavitation) or a hyperextension injury in an older patient with cervical spondylosis — first disrupts the decussating spinothalamic fibres as they cross in the anterior white commissure. Because these fibres are arranged sacral-outside, cervical-inside (the cervical fibres cross most centrally), the earliest loss is in a cape-like distribution across the shoulders and arms — "suspended" sensory loss that does not extend to the legs. [1]
This produces dissociated sensory loss — pain and temperature are lost, but light touch and proprioception are preserved (they travel in the dorsal columns, which are not crossed in the commissure). As the syrinx expands, it can encroach on the anterior horn cells (LMN weakness and atrophy at the level) and the corticospinal tracts (UMN weakness below). [1]
Causes: syringomyelia (associated with Chiari I malformation in around half of cases), traumatic central cord injury, intrinsic cord tumour (ependymoma, astrocytoma). [1]
Posterior column disease (subacute combined degeneration)
Selective damage to the dorsal columns and lateral corticospinal tracts produces: [1]
- Loss of vibration and proprioception (dorsal columns) — positive Romberg, pseudoathetosis, a high-stepping stomping gait
- UMN weakness (lateral corticospinal tract) — spastic paraparesis, hyperreflexia, extensor plantar responses
- Preserved pain and temperature (spinothalamic tract is intact)
- Often a superimposed peripheral neuropathy (loss of ankle jerks despite brisk knee jerks — the "mixed UMN and LMN" picture) [1]
The classic cause is vitamin B12 deficiency (subacute combined degeneration, SCD), but identical pathology occurs with copper deficiency and nitrous oxide abuse. The two clinical clues are a positive Romberg (loss of proprioception) and a macrocytic anaemia on the blood film. [1]
Malignant spinal cord compression

Epidemiology and mechanism
Malignant spinal cord compression (MSCC) affects around 5 to 10 percent of patients with advanced cancer. It is the most common non-traumatic cause of cord compression in adults. The tumours that most commonly metastasise to bone are the "BLT and Kosher Pickle" — Breast, Lung, Thyroid, Kidney, Prostate — plus myeloma and lymphoma. Breast, prostate and lung together account for over half of all MSCC cases. [1]
The mechanism is usually haematogenous spread to the vertebral body, followed by expansion into the epidural space and compression of the cord and its venous plexus. Venous congestion and cord oedema follow, and if untreated, cord infarction produces irreversible paralysis. This is why early decompression (with steroids and surgery or radiotherapy) reverses oedema but not infarction — the window is short. [1]
Clinical presentation — the cardinal triad
| Feature | Detail |
|---|---|
| Back pain | The earliest and most common symptom (over 95 percent). Often progressive, nocturnal, worse on lying flat — distinguishing it from mechanical back pain. May radiate in a band (radicular) at the level. |
| Sensory level | Numbness below the lesion, often ascending as the compression worsens. A sharp dermatomal level to pinprick is the cardinal sign. |
| Motor weakness | UMN pattern below the lesion — initially the patient notices heaviness, dragging the foot, or falls; later a visible paraparesis. |
| Sphincter disturbance | A late sign — urinary retention, constipation, loss of anal tone. Its presence indicates advanced compression and a worse prognosis. |
DCE long-case trap: Back pain is the presenting symptom in over 95 percent of MSCC cases, often for weeks or months before the neurological deficit appears. Any patient with known cancer and new or worsening back pain must be assessed urgently — do not wait for the neurological deficit. The single best predictor of ambulation after treatment is ambulation at presentation. [1]
Emergency management
The management of suspected MSCC is a neurological emergency — every hour of cord compression reduces the chance of ambulation. The pathway is: [1]
- Recognise: Known cancer (or unexplained weight loss) plus new back pain with any neurological symptom. Examine for a sensory level, UMN signs, and sphincter disturbance.
- Give dexamethasone 16 mg immediately (IV or oral). This reduces cord oedema and buys time for definitive imaging and treatment. The conventional regimen is 16 mg loading, then 8 mg twice daily, tapered after definitive treatment (radiotherapy or surgery). [1]3. Emergency MRI whole spine with gadolinium within 24 hours. MRI is the gold standard. If MRI is contraindicated (pacemaker), CT myelography is the alternative. A plain CT or X-ray does NOT exclude cord compression — it shows bone but not the cord.
- Urgent referral to the spinal surgery, radiation oncology and oncology teams. The decision between surgery and radiotherapy is made on the Patchell criteria (below).
- Analgesia (opioid-based, as the pain is often severe), DVT prophylaxis (immobility is a major risk), gastric protection (PPI with dexamethasone), and glucose monitoring (steroid hyperglycaemia). [1]
DWE high-yield — the dexamethasone dose: The standard MSCC dose is 16 mg loading then 8 mg twice daily. High-dose regimens (96 to 100 mg per day) are no longer recommended because the Vecht 1989 trial (PMID 2771077) showed no additional benefit over the conventional dose, with significantly more toxicity (psychosis, gastric perforation, infection). This is one of the most commonly tested MSCQ facts in cord compression. [1]
Surgery versus radiotherapy — the Patchell criteria
The Patchell 2005 randomised trial (PMID 16112300, published in the Lancet — not NEJM, a common exam misattribution) compared direct decompressive surgery plus radiotherapy against radiotherapy alone in patients with a single area of MSCC. The trial was stopped early at interim analysis because surgery was clearly superior: [1]
- Ambulation: 84 percent in the surgery group vs 57 percent with radiotherapy alone.
- Duration of ambulation: Median 122 days vs 13 days.
- Regaining ambulation: Among non-ambulatory at presentation, 62 percent with surgery vs 19 percent with radiotherapy alone regained walking.
- Survival: Significantly longer in the surgery group (median 126 days vs 100 days). [1]
The Patchell criteria for surgical candidacy are: [1]
| Criterion | Requirement |
|---|---|
| Single compressive site | One level of cord compression (multiple sites favour radiotherapy) |
| Predicted survival | Greater than 3 months |
| Ambulatory or paraparetic | Paraplegia for more than 48 hours is an exclusion (irreversible) |
| Radioresistant tumour | Surgery preferred for renal cell, melanoma, sarcoma; radiotherapy sufficient for small cell lung, lymphoma, myeloma |
| Fit for surgery | Cardiorespiratory and nutritional fitness |
Patients who do not meet the Patchell criteria — multiple sites, poor prognosis, paraplegia more than 48 hours, or radioresponsive tumours — receive palliative radiotherapy (typically 8 Gy single fraction or 20 Gy in 5 fractions) plus continued dexamethasone. [1]
DCE viva answer pattern: When asked "what is the role of surgery in this patient?", the structured answer is: "If this patient has a single compressive site on MRI, an expected survival of more than three months, and is ambulatory or paraparetic for less than 48 hours, they meet the Patchell criteria for direct decompressive surgery followed by radiotherapy, which more than doubles the chance of remaining ambulatory compared to radiotherapy alone. If they have multiple sites, a poor prognosis, or a radioresponsive tumour, I would give radiotherapy and dexamethasone." [1]
Outcomes and prognosis
The single most important prognostic factor is neurological status at presentation:
- Ambulatory at presentation: over 80 percent remain ambulatory with treatment.
- Paraparetic at presentation: around 30 to 60 percent regain ambulation.
- Paraplegic at presentation: under 10 percent regain ambulation. [1]
This is why early recognition matters — the loss of ambulation is often irreversible. Median survival after MSCC is 3 to 6 months for most solid tumours, but patients with breast, prostate or myeloma can survive for years, justifying aggressive treatment. [1]
Cauda equina syndrome
Cauda equina syndrome (CES) is the acute compression of the lumbosacral nerve roots below the conus medullaris (below L1 to L2 vertebral level). It is a surgical emergency — delay produces permanent bladder, bowel and sexual dysfunction. [1]
Clinical presentation
The cardinal features are: [1]
| Feature | Detail |
|---|---|
| Severe low back pain | Often bilateral sciatica — distinguishes from unilateral disc protrusion |
| Saddle anaesthesia | Numbness in the perianal, perineal and genital regions (S2 to S4 dermatomes). Ask: "Can you feel the toilet paper when you wipe?" |
| Bladder dysfunction | Painless urinary retention (the classic sign) — but a post-void residual on bladder scan is more sensitive. Overflow incontinence is a late sign. |
| Bowel dysfunction | Faecal incontinence or loss of rectal fullness sensation |
| Motor and reflex | LMN weakness in the legs (the roots are LMN), absent ankle jerks, and in severe cases flaccid paralysis |
DWE high-yield trap: CES produces lower motor neuron signs (flaccid weakness, absent reflexes, no extensor plantar) because the lesion is in the nerve roots, below the cord. A conus medullaris lesion (at T12 to L1) produces a mixed UMN and LMN pattern — UMN leg signs with sacral sensory loss and sphincter dysfunction. The imaging and urgency are the same, but the clinical signs distinguish them. [1]
Management
- Emergency MRI whole spine (or at least lumbosacral spine) within hours.
- Urinary catheterisation for retention (prevents bladder overdistension injury).
- Urgent surgical decompression, ideally within 24 to 48 hours of the onset of sphincter disturbance. Delays beyond 48 hours are associated with a significantly higher rate of permanent sphincter dysfunction.
- Analgesia, DVT prophylaxis, and postoperative rehabilitation. [1]
The most common cause is a large central lumbar disc herniation (L4 to L5 or L5 to S1), but other causes include tumour (schwannoma, metastasis), spinal epidural abscess, haematoma (anticoagulation), and trauma. The prognosis is best when surgery is performed within 24 to 48 hours of the onset of sphincter symptoms. [1]
Syringomyelia
Syringomyelia is a fluid-filled cavitation (syrinx) within the spinal cord, most often cervical. Around half of cases are associated with a Chiari I malformation (cerebellar tonsil descent through the foramen magnum), which obstructs CSF flow at the craniocervical junction and drives CSF into the cord substance. Other causes include trauma, meningitis, arachnoiditis, and intrinsic cord tumours. [1]
Clinical presentation
The syrinx begins centrally and expands outward, first compressing the decussating spinothalamic fibres in the anterior white commissure. This produces the classic dissociated sensory loss: [1]
- Loss of pain and temperature in a cape-like or suspended distribution across the shoulders and arms (the crossing cervical fibres are most central and affected first). The patient notices painless burns or injuries to the hands.
- Preserved light touch and proprioception (dorsal columns are not crossed in the commissure).
- As the syrinx expands: LMN weakness and atrophy at the level (anterior horn cells), and UMN weakness below (corticospinal tracts).
- Associated features: scoliosis, Charcot joints (neuropathic arthropathy from the painless injuries), and in Chiari-associated cases, suboccipital headache worsened by cough or straining. [1]
DWE high-yield: The hallmark of syringomyelia is dissociated sensory loss — pain and temperature lost, touch preserved — in a cape-like or suspended distribution. This is because the crossing spinothalamic fibres in the anterior commissure are damaged while the dorsal columns (uncrossed at that level) are spared. The diagnosis is confirmed by MRI cervical spine (and posterior fossa, to identify Chiari). [1]
Management
- MRI cervical and thoracic spine, plus posterior fossa to identify the syrinx and any associated Chiari malformation.
- Conservative monitoring for asymptomatic or minimally symptomatic syrinxes — many remain stable for years.
- Surgical decompression (posterior fossa decompression for Chiari I, or syringosubarachnoid shunt for isolated syrinx) for progressive neurological deficit. The goal is to restore CSF flow and prevent further expansion. [1]
Transverse myelitis
Transverse myelitis is an inflammatory disorder of the spinal cord producing a band-like sensory level and bilateral motor and autonomic dysfunction below the lesion. It can affect any level but is most common in the thoracic cord. The onset is typically acute to subacute — hours to days — and the inflammation can be: [1]
- Idiopathic (the most common category after workup)
- Multiple sclerosis — especially a partial (not complete) transverse myelitis, often cervical, with brain MRI lesions
- Neuromyelitis optica spectrum disorder (NMOSD) — typically a longitudinally extensive transverse myelitis (LETM) spanning 3 or more vertebral segments, AQP4-IgG positive
- MOG antibody-associated disease (MOGAD) — also LETM, often with optic neuritis, MOG-IgG positive
- ADEM (acute disseminated encephalomyelitis) — post-infectious, typically in children
- Systemic autoimmune — systemic lupus, Sjogren, sarcoid, Behcet
- Infectious/post-infectious — viral myelitis (HSV, VZV, enterovirus), Lyme, syphilis, TB, schistosomiasis [1]
Diagnostic criteria
The Transverse Myelitis Consortium Working Group (2002, PMID 12236201) diagnostic criteria for idiopathic acute transverse myelitis are: [1]
- Bilateral spinal cord dysfunction (sensory, motor, or autonomic)
- A clearly defined sensory level
- Progression to nadir between 4 hours and 21 days from onset
- Evidence of inflammation — CSF pleocytosis or elevated IgG index, OR a gadolinium-enhancing cord lesion on MRI
- Exclusion of a compressive cause (MRI is mandatory) and of radiation, vascular, and neoplastic causes [1]
DCE viva trap: The MRI must exclude a compressive lesion before a lumbar puncture is performed. Performing an LP in a patient with an undiagnosed compressive cord lesion risks neurological deterioration. The sequence is always: clinical exam, MRI, then CSF. [1]
NMOSD — the key differential
Neuromyelitis optica spectrum disorder (NMOSD) is the most important diagnosis to exclude in a patient with transverse myelitis. The 2015 International Consensus Diagnostic Criteria (PMID 26092914) require, for AQP4-IgG-positive NMOSD, at least one core clinical characteristic (optic neuritis, acute myelitis — typically LETM, area postrema syndrome with hiccups and vomiting, brainstem syndrome) plus a positive AQP4-IgG test. The antibody test is essential because NMOSD is treated differently from MS (rituximab, eculizumab, satralizumab; beta-interferon can worsen it). [1]
| Feature | MS myelitis | NMOSD myelitis |
|---|---|---|
| Cord lesion length | Short (less than 2 segments), peripheral, asymmetrical | Longitudinally extensive (greater than 3 segments), central |
| Antibody | None | AQP4-IgG positive |
| Brain MRI | Typical periventricular, juxtacortical, infratentorial lesions | Often normal or atypical |
| Optic neuritis | Unilateral, mild | Bilateral, severe, with recovery poor |
Management
- IV methylprednisolone 1 g daily for 3 to 5 days as first-line for any acute transverse myelitis. This reduces inflammation and speeds recovery. [1]- Plasma exchange (5 sessions over 1 to 2 weeks) if there is no response to steroids by 5 to 7 days — especially in NMOSD and severe idiopathic cases.
- Long-term immunotherapy if NMOSD, MS, or MOGAD confirmed — rituximab or mycophenolate for NMOSD, disease-modifying therapy for MS.
- Supportive care — DVT prophylaxis, bladder and bowel management, pressure-area care, early rehabilitation. [1]
Vitamin B12 deficiency and subacute combined degeneration
Pathophysiology
Vitamin B12 (cobalamin) is a cofactor for two enzymes: methionine synthase (folate-dependent DNA synthesis) and methylmalonyl-CoA mutase (fatty acid metabolism). Deficiency impairs myelin synthesis in the dorsal columns and lateral corticospinal tracts, producing subacute combined degeneration (SCD). The term "combined" refers to the combination of dorsal column (posterior) and corticospinal (lateral) tract involvement. [1]
The causes of B12 deficiency are: [1]
| Cause | Mechanism |
|---|---|
| Pernicious anaemia | Autoimmune destruction of gastric parietal cells (loss of intrinsic factor) — the most common cause |
| Terminal ileum disease | Crohn disease, resection, coeliac disease — B12 is absorbed in the terminal ileum |
| Dietary (vegans) | No animal products — the most common cause in young vegans |
| Metformin | Long-term use impairs B12 absorption (a reversible cause) |
| Nitrous oxide abuse | Oxidises the cobalt ion in B12, producing functional deficiency even with normal serum levels |
| Proton pump inhibitors (long-term) | Reduced acid impairs B12 release from food |
Nitrous oxide — the rising cause
Nitrous oxide (recreational "whippets" or "nangs") irreversibly oxidises the cobalt ion in B12 from its active Co(1+) to an inactive state, producing functional B12 deficiency even with a normal serum B12 level. The systematic review by Garakani et al. (2016, PMID 27037733) documented myeloneuropathy and subacute combined degeneration as the most common neurological consequence. This is now one of the most common causes of subacute combined degeneration in young adults — always ask about nitrous oxide use in any young patient with paraesthesia and posterior column signs. [1]
Clinical presentation of SCD
The presentation is insidious and progressive: [1]
- Early: Paraesthesia in the hands and feet (often symmetrical), loss of vibration and proprioception, a positive Romberg (unsteadiness worse with eyes closed), and a high-stepping stomping gait.
- Motor: UMN weakness in the legs (spastic paraparesis, hyperreflexia, extensor plantar), often mixed with LMN signs from the accompanying peripheral neuropathy (absent ankle jerks despite brisk knee jerks — the "mixed UMN/LMN" picture that is a DCE classic).
- Cognitive/psychiatric: Irritability, memory impairment, depression, and rarely psychosis ("megaloblastic madness").
- Haematological: Macrocytic anaemia (often with hypersegmented neutrophils on the blood film) — but neurological disease can occur without anaemia, so do not be reassured by a normal haemoglobin. [1]
DCE long-case trap: The Healton et al. (1991, PMID 1648656) series showed that neurological symptoms can precede anaemia in a significant proportion of patients with B12 deficiency. A normal haemoglobin does NOT exclude subacute combined degeneration. Check the serum B12, methylmalonic acid and homocysteine in any patient with unexplained posterior column signs. [1]
Investigations
- Serum B12 — low (typically under 150 pmol/L), but a normal or low-normal B12 does NOT exclude deficiency.
- Methylmalonic acid (MMA) and homocysteine — elevated in true deficiency; these are the most sensitive markers, especially when the serum B12 is borderline or normal (as in nitrous oxide-related functional deficiency).
- FBC and blood film — macrocytic anaemia with hypersegmented neutrophils (over 5 lobes).
- Folate — check concurrently; combined deficiency is common.
- Intrinsic factor antibodies — positive in pernicious anaemia.
- MRI cervical and thoracic spine — T2 hyperintensity in the dorsal columns (the classic "inverted V" sign in nitrous oxide myelopathy).
- Identify the cause — dietary history, metformin, nitrous oxide, terminal ileum disease, autoimmune screen for pernicious anaemia. [1]
Treatment
- Intramuscular hydroxocobalamin 1000 micrograms on alternate days for 2 weeks (or until no further neurological improvement), then 1000 micrograms every 2 to 3 months lifelong for pernicious anaemia or irreversible malabsorption.
- Oral cyanocobalamin may suffice for dietary deficiency in vegans.
- Identify and remove the cause — stop nitrous oxide, review metformin, investigate malabsorption, dietary advice for vegans.
- Never give folate alone — folate can improve the anaemia while allowing irreversible neurological deterioration to continue. Always give B12 with (or before) folate. [1]
DWE high-yield — the folate trap: Giving folate alone to a B12-deficient patient is a catastrophic error because folate can correct the megaloblastic anaemia (by bypassing the methionine synthase block) while the subacute combined degeneration progresses. Always give B12 first or concurrently. This is one of the most commonly tested pharmacology facts in cord disease. [1]
Investigation approach — the systematic workup
The investigation of a patient with a suspected cord lesion follows a clear sequence: [1]
Tier 1 — Emergency (any acute myelopathy)
| Investigation | Purpose |
|---|---|
| MRI whole spine with gadolinium | Exclude compression; identify the level, extent, and enhancement pattern |
| MRI brain (if transverse myelitis suspected) | Identify demyelinating lesions (MS) or area postrema lesions (NMOSD) |
| Bloods — FBC, ESR, CRP, electrolytes, LFTs, glucose | Baseline and systemic disease screening |
| Coagulation | Before any LP or surgery |
Tier 2 — Aetiological (after the level is confirmed)
| Investigation | Target |
|---|---|
| CSF analysis (cell count, protein, glucose, oligoclonal bands, culture, viral PCR) | Inflammation, infection, MS, NMOSD — but ONLY after MRI excludes compression |
| B12, folate, methylmalonic acid, homocysteine | Subacute combined degeneration |
| Copper | Copper deficiency myeloneuropathy (bariatric, zinc excess) |
| Syphilis serology (RPR/TPHA) | Tabes dorsalis, meningovascular syphilis |
| ANA, dsDNA, ENA, ANCA | Systemic autoimmune (lupus, Sjogren, vasculitis) |
| AQP4-IgG and MOG-IgG | NMOSD and MOGAD — if LETM or atypical myelitis |
| ACE, sarcoid screen | Neurosarcoidosis |
| HIV | HIV-related myelopathy and vacuolar myelopathy |
| Nerve conduction studies and EMG | Distinguish UMN cord disease from LMN radiculopathy; identify peripheral neuropathy |
DCE viva answer pattern: When presenting the investigation plan, state the principle: "I would arrange an emergency MRI whole spine with gadolinium to exclude a compressive cause — this is the single most important investigation. Once compression is excluded, I would proceed to CSF analysis and targeted bloods for inflammatory, infectious, and metabolic causes, guided by the clinical picture. In any young adult with an unexplained myelopathy I would test AQP4-IgG and MOG-IgG to exclude NMOSD and MOGAD." [1]
DCE long-case approach
Opening statement (SASPOP)
"Mr Patel is a 64-year-old man who presents with three weeks of progressive lower back pain and three days of difficulty walking, with numbness ascending from his feet to his waist. He has a known history of metastatic prostate cancer, diagnosed two years ago, on androgen deprivation therapy. [1]
On examination he is afebrile, alert and oriented. He has weakness in both legs — power 3 out of 5 in the hips and 2 out of 5 at the ankles — with increased tone, brisk knee and ankle jerks, and extensor plantar responses. There is a sensory level to pinprick at T10. He has a distended bladder on palpation and a post-void residual of 400 mL on bladder scan. The rest of his neurological examination is normal. [1]
His main problems are:
- Acute thoracic malignant spinal cord compression from prostate cancer metastasis — emergency dexamethasone and MRI required
- Metastatic prostate cancer — oncology input for systemic disease control
- Urinary retention — catheterisation required
- Pain management and VTE prophylaxis
- Functional and psychological support for a potentially life-changing diagnosis." [1]
Integrated management plan
Present in three phases: [1]
-
Immediate (minutes to hours): Recognise the syndrome. Give dexamethasone 16 mg immediately. Arrange emergency MRI whole spine with gadolinium within 24 hours. Catheterise for retention. Start opioid analgesia and DVT prophylaxis. Notify the spinal surgery, radiation oncology and oncology teams. [1]
-
Definitive (24 to 72 hours): Apply the Patchell criteria. If a single compressive site with predicted survival greater than 3 months and paraplegia less than 48 hours — direct decompressive surgery followed by radiotherapy. Otherwise — palliative radiotherapy (8 Gy single fraction or 20 Gy in 5 fractions) plus continued dexamethasone, tapering after treatment. [1]
-
Longitudinal: Rehabilitation (physiotherapy, occupational therapy, mobility aids), bladder and bowel management, spasticity control, neuropathic pain management, psychological support, and systemic oncology treatment. Serial MRI to monitor response and detect new sites. [1]
DCE examiner probing questions you must anticipate:
- "Why did you choose surgery (or radiotherapy) for this patient?" → Apply the Patchell criteria explicitly.
- "What is his prognosis for walking?" → Ambulation at presentation is the key predictor — over 80 percent of ambulatory presenters remain ambulatory.
- "What dose of dexamethasone and why?" → 16 mg loading then 8 mg twice daily; the Vecht trial showed high-dose regimens add toxicity without benefit.
- "How will you manage his pain?" → Opioid-based for nociceptive (bone) pain; gabapentin or pregabalin for neuropathic (cord) pain; consider palliative care input. [1]
DCE short-case approach: neurological examination of a cord lesion
Instruction: "Examine this patient's neurological system. They were admitted two weeks ago with progressive leg weakness." [1]
Systematic routine (observe, motor, sensory, coordination, gait)
- General inspection: Observe for posture (spastic posture, wheelchair, catheter bag), wasting, fasciculations, and any surgical scar.
- Cranial nerves: Usually normal in a cord lesion (unless a high cervical lesion or Chiari malformation). A positive test for any cranial nerve sign should prompt consideration of a brainstem or cerebral lesion.
- Motor: Assess tone, power, reflexes and plantar responses in all four limbs. A UMN pattern below the lesion — increased tone, weakness, hyperreflexia, extensor plantar — localises to the cord. LMN signs at the level (anterior horn involvement in central cord) and UMN signs below is the classic pattern.
- Sensory: Test pinprick and temperature (spinothalamic), then vibration and proprioception (dorsal columns), dermatomally from distal to proximal. Mark the sensory level. Compare light touch (often preserved) with pinprick (lost) to identify dissociated sensory loss.
- Coordination: Limited by weakness in the legs, but assess the upper limbs fully. A positive Romberg (loss of proprioception) points to dorsal column disease.
- Gait: If ambulatory, observe for spastic gait (stiff, circumducting), high-stepping gait (foot drop), or a sensory ataxic gait (stomping, worse with eyes closed). [1]
Presentation template
"I examined Mr Patel's neurological system. He is alert and cooperative, seated in a wheelchair with an indwelling urinary catheter. [1]
Cranial nerves are intact. In the upper limbs, tone, power, reflexes and coordination are normal. In the lower limbs, tone is increased. Power is 3 out of 5 in the hips and 2 out of 5 at the ankles and feet, symmetric. Reflexes are pathologically brisk at the knees and ankles, with clonus at both ankles. Both plantar responses are extensor. [1]
Sensation is reduced to pinprick below the T10 dermatome on both sides — a clear sensory level. Vibration sense is absent at the ankles and reduced at the knees. Joint position sense is impaired at the toes. [1]
In summary, these findings — a spastic paraparesis with a T10 sensory level, hyperreflexia, extensor plantar responses, and urinary retention — localise to a thoracic spinal cord lesion at or above the T10 cord segment. The clinical picture is most consistent with malignant spinal cord compression." [1]
Key DWE MCQ patterns
- Cord syndrome identification: Brown-Sequard (ipsilateral motor and proprioception loss, contralateral pain and temperature), anterior cord (motor and pain/temperature loss, dorsal columns preserved), central cord (cape-like dissociated sensory loss). The sensory pattern names the syndrome.
- MSCC initial management: A patient with known cancer and new back pain with leg weakness — the correct first step is dexamethasone 16 mg plus emergency MRI whole spine, not analgesia alone or a CT scan. [1]3. Patchell criteria for surgery: A single compressive site, predicted survival greater than 3 months, paraplegia less than 48 hours. Multiple sites or poor prognosis — radiotherapy.
- B12 and nitrous oxide: A young adult with paraesthesia, positive Romberg, and posterior column signs — check B12 and MMA, and ask about nitrous oxide ("whippet") use. A normal B12 does NOT exclude functional deficiency.
- Cauda equina vs conus: Cauda equina (LMN signs, saddle anaesthesia, below L1) vs conus medullaris (mixed UMN and LMN, sacral sensory loss, T12 to L1).
- LETM and NMOSD: A longitudinally extensive transverse myelitis (greater than 3 segments) — test AQP4-IgG for NMOSD, which requires long-term immunotherapy (rituximab) and is worsened by MS disease-modifying drugs.
- The folate trap: Never give folate alone in suspected B12 deficiency — it can precipitate or worsen subacute combined degeneration.
- ASA vs PSA territory: Anterior cord syndrome spares dorsal columns (separate posterior supply); the bedside test is preserved vibration and proprioception. [1]
References
[1] Patchell et al. (2005, Lancet) — Direct decompressive surgery plus radiotherapy vs radiotherapy alone in MSCC; 84 percent vs 57 percent ambulation; stopped early for benefit. Defines the surgical candidacy criteria. [2] Vecht et al. (1989, Neurology) — Conventional (10 mg load, 16 mg/day) vs high-dose (100 mg load, 96 mg/day) dexamethasone in MSCC; no difference in outcome; high-dose more toxic. Establishes the 16 mg standard. [3] Transverse Myelitis Consortium Working Group (2002, Neurology) — Proposed diagnostic criteria for idiopathic acute transverse myelitis: bilateral cord dysfunction, sensory level, progression to nadir 4 hours to 21 days, inflammatory CSF or MRI, exclusion of compression. [4] Wingerchuk et al. (2015, Neurology) — International consensus diagnostic criteria for NMOSD: AQP4-IgG positive plus one core clinical characteristic (optic neuritis, acute myelitis/LETM, area postrema syndrome, brainstem syndrome). [5] Healton et al. (1991, Medicine) — Neurologic aspects of cobalamin deficiency in 153 episodes; paresthesia and ataxia were often the first signs; neurological disease could precede anaemia; 47 percent complete recovery with treatment. [6] Garakani et al. (2016, Am J Addict) — Systematic review of nitrous oxide abuse: myeloneuropathy and subacute combined degeneration the most common neurological manifestation; low or low-normal B12 with elevated MMA and homocysteine.
NICE Guideline NG75 (Metastatic spinal cord compression in adults); NICE Guideline NG59 (Low back pain and sciatica — cauda equina red flags); NICE Clinical Knowledge Summary on MSCC. [1]
References
- [1]Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial Lancet, 2005.PMID 16112300
- [2]Vecht CJ, Haaxma-Reiche H, van Putten WLJ, et al. Initial bolus of conventional versus high-dose dexamethasone in metastatic spinal cord compression Neurology, 1989.PMID 2771077
- [3]Transverse Myelitis Consortium Working Group Proposed diagnostic criteria and nosology of acute transverse myelitis Neurology, 2002.PMID 12236201
- [4]Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders Neurology, 2015.PMID 26092914
- [5]Healton EB, Savage DG, Brust JCM, Garrett TJ, Lindenbaum J Neurologic aspects of cobalamin deficiency Medicine (Baltimore), 1991.PMID 1648656
- [6]Garakani A, Jaffe RJ, Savla D, et al. Neurologic, psychiatric, and other medical manifestations of nitrous oxide abuse: A systematic review of the case literature Am J Addict, 2016.PMID 27037733