Phys · neurological
Stroke
Also known as cerebrovascular accident · CVA · ischaemic stroke · haemorrhagic stroke · intracerebral haemorrhage · cerebral infarction · transient ischaemic attack · TIA · brain attack · minor stroke
Consultant-physician-depth guide to acute stroke — classification, pathophysiology of the ischaemic penumbra, vascular territory localisation, IV thrombolysis and mechanical thrombectomy protocols, and integrated secondary prevention for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Stroke
The answer first
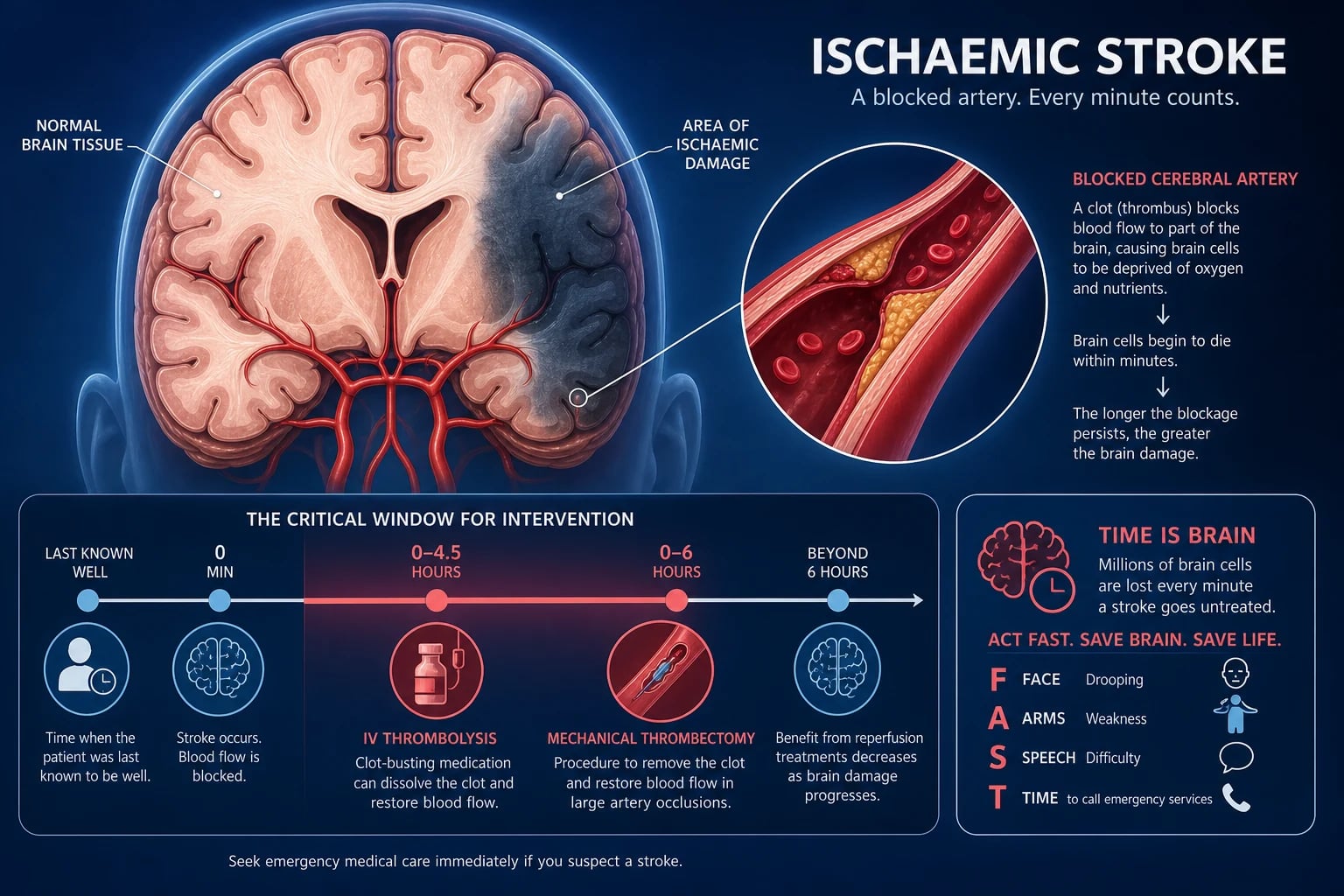
Stroke is a syndrome of sudden onset neurological deficit caused by disruption of cerebral blood flow. It is a medical emergency where every minute of delay kills approximately 1.9 million neurons. The two questions that determine everything are: when was the patient last known well? and is there a large vessel occlusion? [1]
Acute ischaemic stroke (85% of all strokes) is potentially reversible with reperfusion therapy: [1]
- IV thrombolysis — alteplase (or tenecteplase) within 4.5 hours of last-known-well. Earlier is better; the benefit curve is steep in the first 90 minutes and flattens toward 4.5 hours.
- Mechanical thrombectomy — for large vessel occlusion (internal carotid artery terminus, M1 middle cerebral artery, basilar artery) within 6 hours of onset, or up to 24 hours with imaging evidence of salvageable penumbra (DAWN/DEFUSE-3 criteria). [1]
The organising principle is "time is brain." Every minute of delayed reperfusion means less salvageable tissue. The non-contrast CT may be normal in the first hours — a normal CT does not exclude acute stroke; it excludes haemorrhage. [1]
Classification
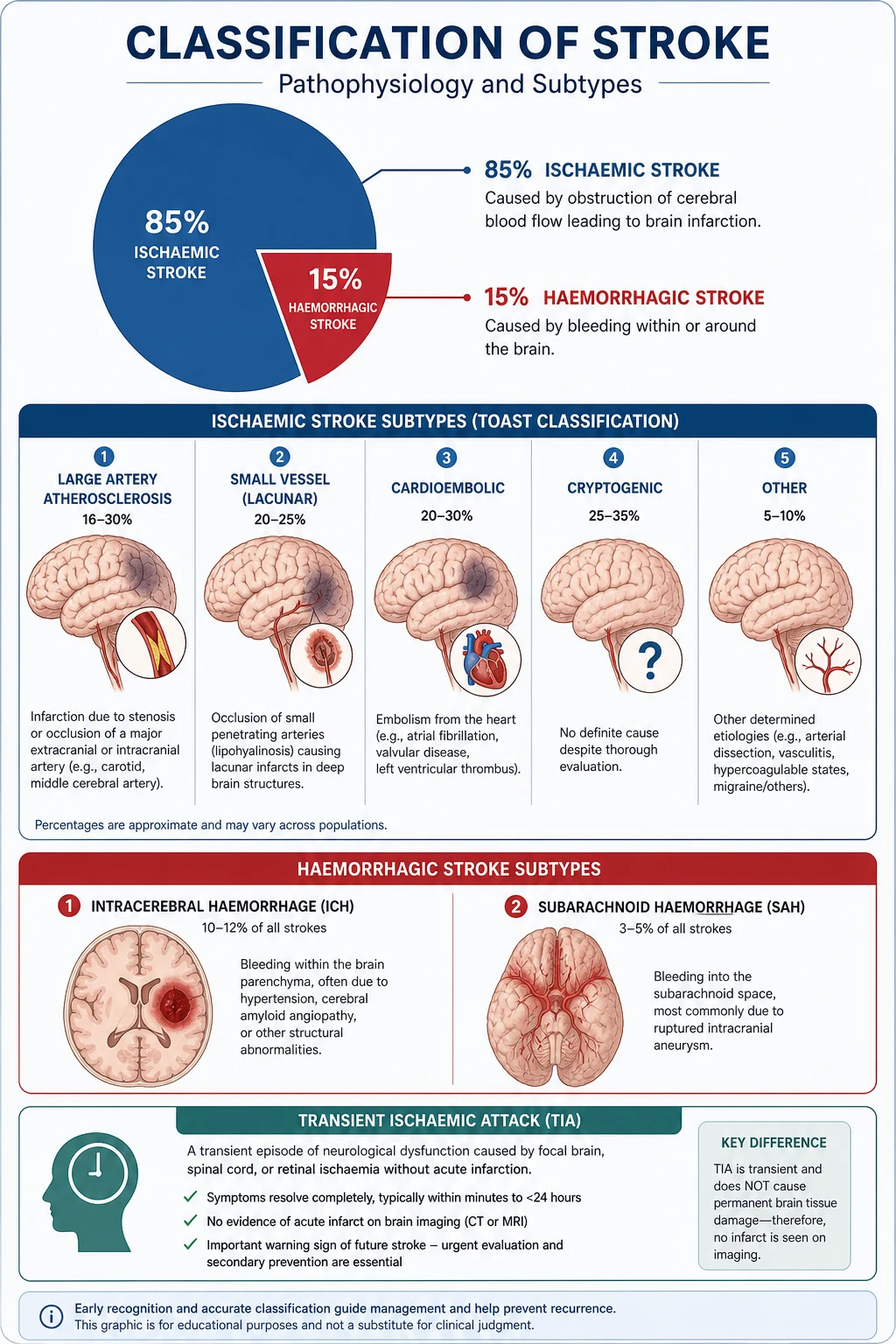
Stroke is classified first by pathology (ischaemic vs haemorrhagic), then by aetiology (the TOAST classification for ischaemic stroke). [1]
Pathological classification
| Type | Proportion | Mechanism | Key imaging |
|---|---|---|---|
| Ischaemic stroke | ~85% | Arterial occlusion — thrombotic or embolic | Non-contrast CT: may be normal early; hypodensity develops over hours. DWI-MRI: hyperintense within minutes |
| Intracerebral haemorrhage (ICH) | ~10-15% | Rupture of small intracerebral vessels (hypertensive vasculopathy, cerebral amyloid angiopathy) | Non-contrast CT: hyperdense area, mass effect |
| Subarachnoid haemorrhage | ~5% | Ruptured saccular aneurysm in 85% | Non-contrast CT: hyperdense sulci/cisterns; LP if CT negative and suspicion high |
Transient ischaemic attack (TIA) — the tissue-based definition
The old definition of TIA required symptom resolution within 24 hours. The modern tissue-based definition replaces this: TIA is a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischaemia without acute infarction on imaging. The 24-hour rule is abandoned because approximately one-third of clinically defined TIAs show infarction on MRI — they are strokes, not TIAs. [1]
This matters because TIA is a warning shot: the 90-day stroke risk after TIA is approximately 10-15% (highest in the first 48 hours). Every TIA demands urgent investigation and secondary prevention, not reassurance. [1]
TOAST classification (ischaemic stroke aetiology)
| Subtype | Proportion | Examples | Investigation priority |
|---|---|---|---|
| Large artery atherosclerosis | ~20% | Carotid stenosis, intracranial atherosclerosis | Carotid Doppler/CTA, CTA head/neck |
| Cardioembolism | ~20% | Atrial fibrillation, prosthetic valve, recent MI, endocarditis | ECG, telemetry/Holter, echocardiogram |
| Small vessel occlusion (lacunar) | ~25% | Hypertensive lipohyalinosis, microatheroma | MRI (small subcortical lesions under 15 mm) |
| Other determined cause | ~5% | Dissection, vasculitis, thrombophilia, drug use | Targeted — CTA neck for dissection, autoimmune screen |
| Undetermined (cryptogenic) | ~30% | No cause identified despite workup | Prolonged cardiac monitoring (implantable loop recorder) |
DWE high-yield: A common MCQ asks which TOAST subtype is most common. The answer is cryptogenic (~30%) or small vessel (~25%), depending on the population studied. But the most commonly tested in management questions is cardioembolic — because anticoagulation (not antiplatelets) is the correct secondary prevention. [1]
Pathophysiology
The ischaemic penumbra — the concept that drives all acute therapy
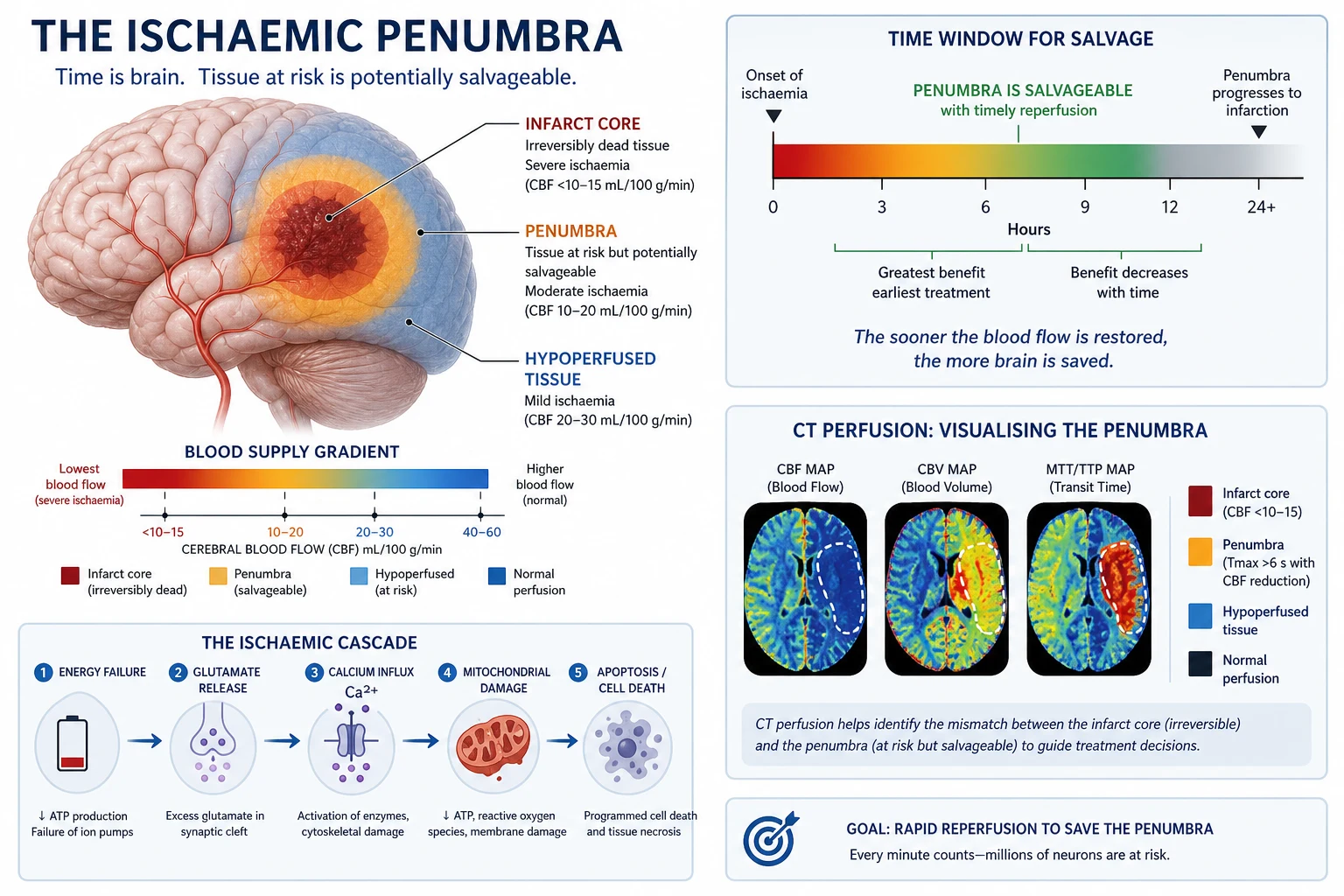
When a cerebral artery occludes, blood flow drops in its territory. The tissue in the centre of the territory — the infarct core — dies within minutes because cerebral blood flow falls below 10 mL/100g/min. Cells here are irreversibly injured; no therapy can save them. [1]
Surrounding the core is the ischaemic penumbra — tissue where flow is reduced (10-20 mL/100g/min) but not critically. These neurons are electrically silent (hence the neurological deficit) but metabolically viable. They are collateral-dependent and will die over hours if perfusion is not restored. [1]
This is why time matters: the penumbra is salvageable, but it shrinks progressively. The penumbra-to-core ratio is approximately 1.0:1.0 at 6 hours (half the threatened tissue is still salvageable). After 6 hours, the rate of penumbra loss accelerates, and without imaging-guided selection, most tissue is irreversibly infarcted. [1]
DCE viva trap: When asked "why does thrombolysis work within 4.5 hours but not after?" the answer is: thrombolysis restores flow to the penumbra before it dies. Beyond 4.5 hours, the risk of haemorrhagic transformation (reperfusion into dead, leaky vessels) outweighs the diminishing salvageable tissue. The DAWN/DEFUSE-3 trials extended the window for thrombectomy — not thrombolysis — because mechanical reperfusion can be guided by imaging that shows surviving penumbra. [1]
The ischaemic cascade (cellular level)
- Energy failure — ATP depletion within seconds of ischaemia
- Ion pump failure — Na+/K+ ATPase fails; intracellular Na+ and water accumulation causes cytotoxic oedema
- Glutamate excitotoxicity — presynaptic glutamate release, NMDA/AMPA receptor activation, massive calcium influx
- Calcium-mediated injury — protease activation, mitochondrial damage, free radical generation
- Inflammatory cascade — microglial activation, cytokine release, blood-brain barrier breakdown (vasogenic oedema follows)
- Apoptosis and necrosis — delayed cell death continues for days [1]
Lacunar infarction
Small vessel disease produces lacunar strokes — small (less than 15 mm) subcortical infarcts in the basal ganglia, thalamus, internal capsule, or pons. The mechanism is lipohyalinosis (degeneration of small penetrating arteries from chronic hypertension) or microatheroma at the origin of the penetrating vessel. Because these are end-artery territories without collateral supply, there is no penumbra to salvage — which is why lacunar strokes generally do not benefit from thrombolysis as dramatically as large vessel strokes, though thrombolysis is still given if within the window and criteria are met. [1]
Vascular territories and clinical presentation
The ability to localise a stroke to a vascular territory from the bedside is a core DCE short-case skill. Examiners will test whether you can distinguish anterior from posterior circulation, and cortical from subcortical patterns. [1]
Middle cerebral artery (MCA) — the most common stroke territory
| Territory | Deficit pattern |
|---|---|
| Complete MCA (M1 occlusion) | Contralateral hemiplegia (face and arm worse than leg), contralateral hemisensory loss, contralateral homonymous hemianopia, conjugate eye deviation toward the lesion. Dominant hemisphere: global aphasia. Non-dominant: neglect |
| Superior division (M2) | Contralateral face and arm weakness greater than leg. Dominant: Broca (expressive) aphasia |
| Inferior division | Contralateral homonymous hemianopia. Dominant: Wernicke (receptive) aphasia. Non-dominant: neglect, behavioural change |
| Lenticulostriate perforators (lacunar) | Pure motor hemiparesis (face, arm, leg equally affected), no cortical signs |
Key discriminators: The face-arm-leg gradient (face and arm worse than leg) points to MCA, because the leg motor cortex (paracentral lobule) is supplied by the ACA. If all three are equally affected with no cortical signs, think lacunar (internal capsule). [1]
Anterior cerebral artery (ACA)
- Contralateral leg weakness greater than arm (the reverse of MCA)
- Urinary incontinence (medial frontal lobe)
- Abulia, apathy, grasp reflex
- Relatively uncommon as an isolated stroke [1]
Posterior cerebral artery (PCA)
- Contralateral homonymous hemianopia (often with macular sparing, due to collateral supply to occipital pole from MCA)
- Contralateral hemisensory loss (thalamus involvement in proximal PCA)
- If dominant: alexia without agraphia (can write but cannot read — left occipital + splenium of corpus callosum)
- Memory impairment (medial temporal lobe involvement) [1]
Vertebrobasilar (posterior circulation)
Posterior circulation stroke is the most commonly missed because symptoms can be vague and non-lateralising. Always think of it when the presentation includes: [1]
- Crossed signs (e.g. ipsilateral cranial nerve palsy with contralateral limb deficit) — pathognomonic of brainstem stroke
- Diplopia, vertigo, dysarthria, dysphagia (brainstem/cerebellar)
- Bilateral or alternating weakness/sensory loss
- Drop attacks (sudden loss of postural tone without LOC)
- Homonymous hemianopia (occipital lobe)
- Coma or locked-in syndrome (basilar artery occlusion) [1]
| Brainstem syndrome | Classic features |
|---|---|
| Wallenberg (lateral medullary) | Ipsilateral facial sensory loss, ipsilateral Horner syndrome, ipsilateral ataxia, contralateral body sensory loss, vertigo, dysphagia, hiccups. PICA territory — most common brainstem stroke |
| Weber (midbrain) | Ipsilateral CN III palsy + contralateral hemiparesis |
| Locked-in syndrome (pontine) | Quadriplegia, aphonia, preserved consciousness (vertical eye movements only) — basilar artery occlusion |
DWE high-yield: The single most tested brainstem stroke is Wallenberg syndrome (lateral medullary). Know the pattern: ipsilateral face (spinal trigeminal tract) + contralateral body (spinothalamic tract) sensory loss, ipsilateral Horner, ipsilateral ataxia (inferior cerebellar peduncle). It is usually caused by PICA or vertebral artery occlusion — it is a vertebral/basilar problem, not carotid. [1]
Lacunar syndromes (pure subcortical)
| Syndrome | Presentation |
|---|---|
| Pure motor hemiparesis | Contralateral face, arm, leg weakness — equal, no cortical signs. Posterior limb internal capsule or pons |
| Pure sensory stroke | Contralateral hemisensory loss, no motor deficit. Thalamus (VPL/VPM) |
| Ataxic hemiparesis | Contralateral weakness + ipsilateral ataxia out of proportion to weakness. Internal capsule or pons |
| Clumsy hand-dysarthria | Dysarthria, facial weakness, clumsy hand, dysphagia. Pons |
DCE short-case trap: The cardinal feature distinguishing a lacunar stroke from a cortical stroke is the absence of cortical signs (no aphasia, neglect, visual field defect, or eye deviation). If the patient has hemiparesis and aphasia, it is not lacunar — it is MCA territory. This distinction is critical because lacunar strokes do not require carotid imaging (the mechanism is small vessel, not large artery). [1]
NIH Stroke Scale (NIHSS)
The NIHSS quantifies stroke severity and is used for eligibility, communication, and outcome prediction. You should be able to score the key components. [1]
| NIHSS range | Severity | Approximate thrombolysis / thrombectomy implications |
|---|---|---|
| 0 | No deficit | Not stroke (reconsider diagnosis) |
| 1-4 | Minor | Thrombolysis if eligible; DAPT for minor stroke/TIA |
| 5-15 | Moderate | Thrombolysis; assess for large vessel occlusion |
| 16-20 | Moderate-severe | Thrombolysis + high suspicion for thrombectomy-eligible LVO |
| 21-42 | Severe | Thrombolysis + urgent CTA for thrombectomy assessment |
Key scoring principles:
- Score what you actually observe, not what you think should be there
- Record the first response, not the best
- A score of 0 in a patient with a witnessed deficit should prompt reconsideration of the diagnosis (migraine aura, seizure with Todd's paresis, hypoglycaemia)
- NIHSS does not capture all deficits well — particularly posterior circulation strokes (visual fields, ataxia, cranial nerves are under-weighted). A basilar occlusion may have a "low" NIHSS but be life-threatening [1]
DCE trap: Examiners will ask for the patient's NIHSS. The most commonly tested components are: level of consciousness (1A-C), gaze (2), visual fields (3), facial palsy (4), motor arms (5), motor legs (6), limb ataxia (7), sensory (8), best language (9), dysarthria (10), extinction/neglect (11). State the score and the one or two components that drive it. [1]
Differential diagnosis of acute focal neurological deficit
| Mimic | Discriminating features |
|---|---|
| Hypoglycaemia | Check finger-prick glucose immediately — mimics stroke perfectly. Always check glucose before thrombolysis |
| Seizure with Todd's paresis | History of seizure activity; deficit resolves over minutes to hours; may have EEG changes |
| Migraine aura (hemiplegic) | Gradual spread of symptoms over minutes; positive visual phenomena; preceding or concurrent headache; young patient; history of migraine |
| Subdural haematoma | Gradual onset, fluctuating symptoms, history of head trauma or falls (especially elderly/anticoagulated) |
| CNS infection | Abscess, encephalitis; fever, systemic signs, progressive course |
| Functional neurological disorder | Internal inconsistency, give-way weakness, non-anatomical sensory loss. Diagnosis of exclusion in the acute setting |
| Brain tumour | Gradual onset, possible history of systemic malignancy; imaging shows mass effect but not restricted diffusion |
DWE trap: The most dangerous mimic is hypoglycaemia. A glucose check is mandatory in the acute stroke pathway before any imaging. Thrombolysing a hypoglycaemic patient is a catastrophic error. The second most tested mimic is Todd's paresis — a post-ictal deficit. If there was seizure activity, the deficit may resolve spontaneously; however, if uncertainty persists and the patient meets thrombolysis criteria, treat — the risk of withholding therapy outweighs the risk of treating a mimic. [1]
Investigations
Acute (door-to-needle pathway)
| Investigation | Purpose | Timing |
|---|---|---|
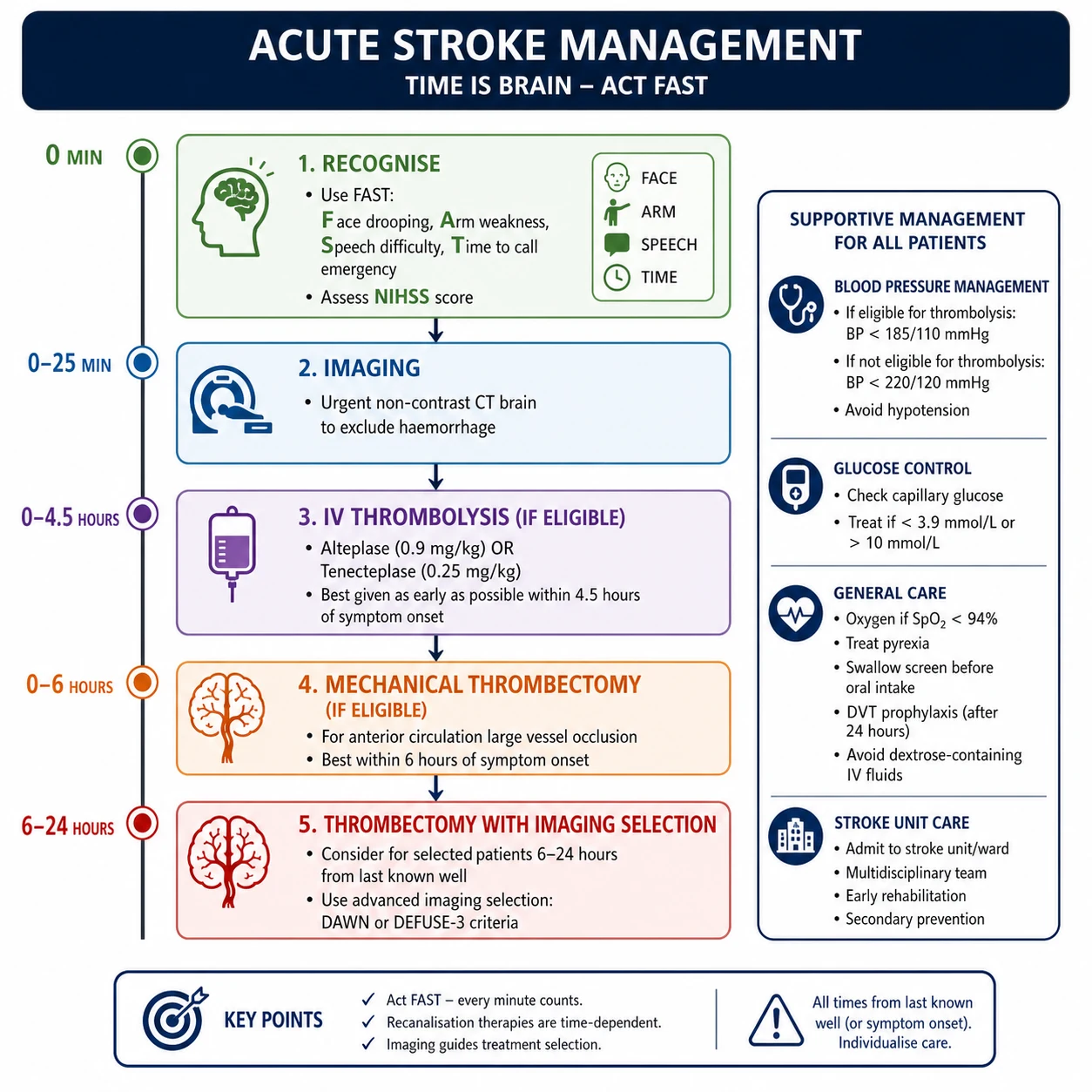
| Non-contrast CT brain | Exclude haemorrhage; identify early ischaemic signs | Immediate — door to CT under 25 minutes |
| CT angiogram (head and neck) | Identify large vessel occlusion for thrombectomy assessment | Concurrent or immediately after CT |
| CT perfusion | Core/penumbra mismatch for extended window (6-24 hr) thrombectomy | If LVO present and beyond 6 hours |
| Finger-prick glucose | Exclude hypoglycaemia | Before thrombolysis — mandatory |
| ECG | Detect AF, prior MI | On arrival |
| Bloods | FBC, coagulation (INR must be under 1.7 for thrombolysis), U&E, troponin, blood glucose | Before thrombolysis — but do not delay if clinical eligibility is clear |
Early ischaemic signs on non-contrast CT (within 6 hours):
- Hyperdense MCA sign (thrombus in the M1 segment)
- Loss of grey-white matter differentiation in the insular ribbon or basal ganglia
- Effacement of cortical sulci
- The ASPECTS score (10-point system) quantifies early ischaemic change — a score below 6 suggests established infarction with poor prognosis for reperfusion benefit [1]
MRI in acute stroke
Diffusion-weighted imaging (DWI) is the most sensitive modality for acute ischaemia, showing hyperintensity within minutes of onset. It detects infarcts that are invisible on CT, including small subcortical and posterior circulation strokes. MRI with DWI is essential for: [1]
- Wake-up stroke (symptom onset unknown — DWI/FLAIR mismatch guides thrombolysis)
- TIA confirmation (DWI positive means it was a stroke, not TIA)
- Posterior circulation stroke (CT is often falsely negative)
- Differentiating acute from chronic infarcts (DWI normalises over 7-10 days; chronic infarcts are not DWI-bright) [1]
Aetiological workup (after the acute phase)
| Investigation | Target |
|---|---|
| Carotid Doppler or CTA neck | Symptomatic carotid stenosis (for CEA decision) |
| Echocardiogram (TTE +/- TOE) | Cardiac source of embolus (thrombus, valve vegetations, PFO, low EF) |
| Prolonged cardiac monitoring (Holter, implantable loop recorder) | Paroxysmal AF (detected in 10-20% of cryptogenic stroke with prolonged monitoring) |
| Lipid panel, HbA1c | Risk factor profiling |
| Thrombophilia screen | Only if young patient, unprovoked, family history, or unusual territory — NOT routine |
| Drug screen (amphetamines, cocaine) | If suspected — especially in young patients with ICH or dissection |
Acute management of ischaemic stroke
The golden rule: time is brain
The target is door-to-needle under 45 minutes for IV thrombolysis. Delays kill tissue. The pathway is: recognition (FAST/BE-FAST) → ambulance notification → ED triage as time-critical → immediate CT → decision → treatment. [1]
IV thrombolysis — alteplase and tenecteplase
Alteplase (recombinant tissue plasminogen activator) is the established agent. Tenecteplase (a genetically modified variant with longer half-life and higher fibrin specificity) is increasingly preferred and has replaced alteplase in many centres based on the AcT trial (non-inferiority) and EXTEND-IA TNK (superior reperfusion before thrombectomy). [1]
| Parameter | Alteplase | Tenecteplase |
|---|---|---|
| Dose | 0.9 mg/kg (max 90 mg); 10% bolus over 1 min, remainder over 60 min | 0.25 mg/kg (max 25 mg) single IV bolus over 5 seconds |
| Administration | Infusion (requires pump setup) | Single bolus (faster, simpler) |
| Evidence | NINDS (0-3 hr) [1], ECASS III (3-4.5 hr) [2], SITS-MOST (real-world safety) [3] | EXTEND-IA TNK, AcT trial — non-inferior or superior |
Thrombolysis eligibility criteria
Inclusion:
- Ischaemic stroke with measurable neurological deficit (NIHSS typically greater than 0)
- Onset (last-known-well) within 4.5 hours
- CT excludes haemorrhage [1]
Key exclusion criteria (absolute — this is the DWE exam list):
- Intracranial haemorrhage on CT (current or prior)
- Significant head trauma or prior stroke in the past 3 months
- Active internal bleeding
- Intracranial or intraspinal surgery in the past 3 months
- Intracranial neoplasm, arteriovenous malformation, or aneurysm
- Platelet count under 100,000
- INR above 1.7 or on oral anticoagulant with elevated INR
- Blood glucose below 2.7 mmol/L (correct first — re-assess after correction) [1]
Additional exclusions in the 3-4.5 hour window (per ECASS III) — the most tested group:
- Age over 80 years
- Prior stroke with diabetes (combined)
- On any oral anticoagulant (regardless of INR)
- NIHSS greater than 25 (very severe stroke — higher haemorrhagic transformation risk) [1]
DWE high-yield trap: A common MCQ gives a patient presenting at 3.5 hours and asks whether they are eligible for thrombolysis. The answer depends on the 3-4.5 hour exclusions. If they are over 80, have prior stroke + diabetes, or are on warfarin/DOAC, they are not eligible in the 3-4.5 hour window even if they would be eligible within 0-3 hours. The 0-3 hour window has fewer exclusions. [1]
Mechanical thrombectomy
Mechanical thrombectomy is the greatest advance in stroke treatment in 25 years. The evidence is unambiguous: for large vessel occlusion (LVO) in the anterior circulation, thrombectomy doubles the rate of functional independence compared to medical therapy alone. [1]
| Window | Selection criteria | Key evidence |
|---|---|---|
| 0-6 hours | LVO (ICA terminus, M1 MCA); no advanced infarct on imaging (ASPECTS above 6 or small core) | MR CLEAN [4], HERMES meta-analysis [5] — number needed to treat for functional independence approximately 2.6 |
| 6-24 hours | LVO with imaging-confirmed target mismatch (small core, large penumbra) on CT perfusion or MRI | DAWN (6-24 hr) [6], DEFUSE-3 (6-16 hr) [7] |
DEFUSE-3 imaging criteria for the 6-16 hour window:
- Ischaemic core volume under 70 mL
- Mismatch ratio at least 1.8
- Mismatch volume at least 15 mL [1]
Thrombectomy is not limited by the thrombolysis window. A patient who is thrombectomy-eligible but beyond 4.5 hours (or has a thrombolysis contraindication) should still receive thrombectomy. Thrombolysis and thrombectomy are complementary, not either/or. [1]
DCE viva answer pattern: When asked "what is the role of thrombectomy in this patient?" the structured answer is: "If there is a large vessel occlusion on CTA and the patient has salvageable penumbra on imaging, thrombectomy is indicated up to 24 hours from last-known-well. The number needed to treat for functional independence is approximately 2.6 in the 0-6 hour window and approximately 3-4 in the extended window. The benefit is greatest with early reperfusion." [1]
Blood pressure management in acute ischaemic stroke
Blood pressure management is the most commonly mismanaged aspect of acute stroke care. The principle is counterintuitive: permissive hypertension maintains collateral perfusion to the penumbra. [1]
| Scenario | Target BP | Rationale |
|---|---|---|
| Before thrombolysis | Below 185/110 mmHg | Reduce haemorrhagic transformation risk during reperfusion |
| After thrombolysis (24 hours) | Below 180/105 mmHg | Maintain for 24 hours post-treatment |
| Not receiving thrombolysis | Permissive — no treatment unless above 220/120 mmHg | Cerebral autoregulation is lost in ischaemia; lowering BP reduces penumbral perfusion |
| Thrombectomy post-procedure | Below 180/105 mmHg | Reperfusion injury and haemorrhagic transformation risk |
Use labetalol (10-20 mg IV over 1-2 minutes, repeat) or nicardipine/clevidipine infusion (titratable). Avoid sublingual nifedipine (unpredictable, rapid drop). Avoid aggressive bolus antihypertensives. [1]
Blood glucose and temperature
- Hypoglycaemia (glucose under 3.3) and hyperglycaemia (glucose above 10) both worsen stroke outcomes. Treat hypoglycaemia immediately. Mild hyperglycaemia in the first 24 hours should be treated with insulin to maintain glucose 4-10 mmol/L (insulin infusion protocols may be used, but avoid hypoglycaemia)
- Fever worsens outcome (each 1 degree C increase doubles poor outcome odds). Maintain normothermia with paracetamol and active cooling if needed. Investigate and treat the cause of fever
- These three — blood pressure, glucose, temperature — are called "neuroprotection basics" and are the foundation of stroke unit care [1]
Stroke unit care
Admitting to a dedicated stroke unit is the single most effective intervention after reperfusion therapy. Organised stroke unit care reduces death and dependency by approximately 20% (one in five patients avoids death or dependency). This is equivalent to the effect of thrombolysis — and applies to all stroke types and severities, including patients not eligible for reperfusion. [1]
The essential components of stroke unit care:
- Co-located, geographically defined unit
- Multidisciplinary team: stroke physician, stroke nurse, physiotherapist, occupational therapist, speech pathologist, dietitian, social worker
- Standardised protocols for monitoring, swallow assessment, DVT prophylaxis, glycaemic/temperature control
- Early mobilisation (unless contraindicated by haemodynamic instability)
- Early discharge planning [1]
Secondary prevention
Secondary prevention after ischaemic stroke or TIA addresses every modifiable risk factor. The guiding principle: every risk factor contributes multiplicatively; treating one is not enough. [1]
Antiplatelet therapy (non-cardioembolic stroke)
| Drug | Evidence | Role |
|---|---|---|
| Aspirin (100-300 mg OD) | IST-2, CAST — modest benefit (2-3% absolute risk reduction for recurrent stroke) | First-line; cheapest |
| Clopidogrel (75 mg OD) | CAPRIE — modestly superior to aspirin in overall vascular events | First-line alternative; preferred in aspirin intolerance |
| Aspirin-dipyridamole (25/200 mg BID) | ESPS-2, ESPRIT — superior to aspirin alone | First-line alternative; equal to clopidogrel per PROFESS [8] |
| Dual antiplatelet therapy (DAPT) | CHANCE [9], POINT — aspirin + clopidogrel for minor stroke (NIHSS under 3) or high-risk TIA for 21-90 days, then single antiplatelet | Short-term DAPT only; long-term DAPT increases bleeding without benefit (SPS3, PROFESS) |
DWE high-yield: The CHANCE and POINT trials established short-term DAPT for minor stroke or high-risk TIA. The regimen is aspirin + clopidogrel started within 24 hours for 21 days (CHANCE) or 90 days (POINT), then de-escalate to clopidogrel monotherapy. This applies ONLY to non-cardioembolic minor stroke/TIA — NOT to moderate-to-severe stroke (where DAPT increases haemorrhagic complications without benefit) and NOT to cardioembolic stroke (where anticoagulation is the correct therapy). [1]
Anticoagulation for cardioembolic stroke (atrial fibrillation)
AF-related stroke is embolic, large, and severe. Anticoagulation is the cornerstone of secondary prevention — antiplatelets are inferior and insufficient. [1]
| Agent | Evidence | Dose |
|---|---|---|
| DOACs (apixaban, dabigatran, rivaroxaban, edoxaban) | RE-LY, ARISTOTLE, ROCKET-AF — non-inferior or superior to warfarin with less intracranial bleeding | Standard doses; dose-adjust for renal function, age, weight (apixaban) |
| Warfarin (INR 2.0-3.0) | Historical standard; still used for mechanical valves, severe MS, antiphospholipid syndrome | INR target 2.5 |
Timing of anticoagulation after stroke: Starting anticoagulation immediately risks haemorrhagic transformation of the infarct. The standard approach (the "1-3-6-12 rule"): [1]
- TIA — start anticoagulation after 1 day
- Minor stroke (NIHSS under 8) — start after 3 days
- Moderate stroke (NIHSS 8-16) — start after 6 days
- Severe stroke (NIHSS above 16) — start after 12 days [1]
These are guidelines, not rigid rules — the principle is to balance stroke recurrence risk (highest in the first days) against haemorrhagic transformation risk (highest in larger infarcts). Repeat imaging before starting anticoagulation if there is uncertainty. [1]
Statins
Start high-intensity statin (atorvastatin 80 mg or rosuvastatin 20-40 mg) for all ischaemic stroke/TIA patients regardless of baseline LDL, targeting LDL reduction. The SPARCL trial demonstrated that atorvastatin 80 mg reduced recurrent stroke in patients with recent stroke/TIA. [1]
Blood pressure control
Treat to a target of under 130/80 mmHg (after the acute permissive-hypertension phase has resolved). Any effective agent is acceptable; thiazide-like diuretics, ACE inhibitors, and ARBs are commonly used. The PROGRESS trial (perindopril +/- indapamide) demonstrated a 28% relative risk reduction in recurrent stroke with BP lowering post-stroke. [1]
Carotid endarterectomy (CEA) and stenting
Carotid revascularisation is indicated for symptomatic significant carotid stenosis. The NASCET method of measuring stenosis (using the narrowest luminal diameter compared to the distal internal carotid artery) is standard. [1]
| Degree of symptomatic stenosis (NASCET) | CEA recommendation | Evidence |
|---|---|---|
| 70-99% (severe) | Strongly recommended — NNT approximately 3-6 to prevent one stroke over 2 years | NASCET 1991 [10] |
| 50-69% (moderate) | Recommended in selected patients (men, hemispheric symptoms, recent onset) — NNT approximately 15 | NASCET 1998 [10] |
| Under 50% | No benefit from surgery — medical therapy only | NASCET 1998 |
| Complete occlusion (100%) | No benefit from CEA — medical therapy (collateral-dependent) | — |
Timing: CEA should be performed as early as possible, ideally within 2 weeks of the qualifying event. The benefit halves if performed after 2 weeks and is negligible after 12 weeks. This is because the highest recurrence risk is in the first days. [1]
Carotid artery stenting (CAS) is an alternative for patients who are not surgical candidates or have restenosis after prior CEA. It carries a slightly higher peri-procedural stroke risk in older patients but is preferred in selected younger patients with favourable anatomy. [1]
DCE long-case trap: When presenting a patient with recent stroke, always state: "The carotid Doppler shows [X]% stenosis ipsilateral to the infarct. Given the symptomatic stenosis of [70-99%], this patient should be referred for carotid endarterectomy ideally within 2 weeks. The procedural risk (stroke/death) should be below 6% at the treating centre." The examiner will test whether you know the timing (within 2 weeks) and the degree threshold (50-69% moderate, 70-99% severe). [1]
Haemorrhagic stroke
Intracerebral haemorrhage (ICH)
Spontaneous ICH accounts for approximately 10-15% of all strokes but has a disproportionate mortality (30-50% at 30 days). The two most common causes are hypertensive vasculopathy (affecting deep structures — basal ganglia, thalamus, pons, cerebellum) and cerebral amyloid angiopathy (affecting lobar regions in elderly patients). [1]
Management principles: [1]
| Priority | Target | Approach |
|---|---|---|
| Blood pressure | Systolic under 140 mmHg (INTERACT2, ATACH-2) | IV labetalol or nicardipine infusion; rapid but controlled reduction |
| Surgical evacuation | Cerebellar haemorrhage over 3 cm or with brainstem compression/hydrocephalus | Urgent neurosurgical evacuation — life-saving. Supratentorial haemorrhage: surgery generally does not improve outcome except in selected lobar haemorrhages (STICH II) |
| ICP management | Maintain CPP above 60 mmHg | Elevate head of bed 30 degrees, sedation, osmotic therapy (mannitol or hypertonic saline) |
| Seizure prophylaxis | Not routine; treat if seizures occur | Levetiracetam or valproate |
DWE high-yield: The most important intervention in ICH on anticoagulants is immediate reversal. Do not wait for repeat coagulation tests in a patient with known warfarin use and ICH — give PCC (faster than FFP) and vitamin K immediately. For DOAC-related ICH, use the specific reversal agent. Time is critical: ongoing haematoma expansion worsens outcome. [1]
Subarachnoid haemorrhage (SAH)
SAH presents with a thunderclap headache — "worst headache of my life" — reaching maximum intensity within seconds to minutes. Neck stiffness, photophobia, nausea, vomiting, and transient or persistent loss of consciousness may follow. Always ask: was the headache instantaneous? [1]
Management cascade:
- Diagnose: Non-contrast CT (sensitivity approximately 100% within 6 hours but declines to ~95% by 24 hours). If CT negative and clinical suspicion high, perform lumbar puncture (look for xanthochromia and non-clearing RBCs across sequential bottles) after at least 12 hours from onset
- Secure the aneurysm: Endovascular coiling (preferred if feasible) or surgical clipping, ideally within 24 hours
- Nimodipine 60 mg every 4 hours for 21 days — reduces delayed cerebral ischaemia from vasospasm (improves outcome)
- Monitor for complications: Vasospasm (days 4-14), hydrocephalus (external ventricular drain), rebleeding, hyponatraemia (cerebral salt wasting) [1]
Complications and post-stroke care
Swallow assessment
Aspiration pneumonia is a leading cause of post-stroke mortality. Every stroke patient must be kept nil by mouth until a formal swallow assessment is completed. [1]
- Bedside swallow screen (water swallow test) within 4 hours of admission by trained nursing staff
- Formal assessment by speech pathologist if screen failed or patient is high-risk
- If unsafe swallow: NG feeding within 24 hours; consider PEG if prolonged (beyond 2-3 weeks) [1]
DVT prophylaxis
Immobile stroke patients have a 10-50% risk of DVT. Prophylaxis:
- Mechanical: Intermittent pneumatic compression for all immobile patients
- Pharmacological: Low-molecular-weight heparin (enoxaparin 40 mg SC OD) once haemorrhage risk is excluded — typically after 24-48 hours for ischaemic stroke, after a longer period for haemorrhagic stroke. The PREVAIL trial showed enoxaparin reduced VTE vs unfractionated heparin without increasing ICH [1]
Post-stroke seizures
- Early seizures (within 7 days): occur in 2-6% of stroke patients, highest in cortical and haemorrhagic strokes. Treat with antiseizure medication but do NOT routinely prophylax
- Late seizures (after 7 days): higher recurrence risk — these meet the definition of epilepsy. Treat with standard antiseizure medication
- Cortical involvement, haemorrhagic stroke, and large infarct size are the main risk factors [1]
Post-stroke depression
Affects approximately one-third of stroke patients. It impairs recovery, functional outcome, and survival. Screen with a validated tool (PHQ-9, HADS) at 1, 3, and 6 months. Treat with SSRIs (sertraline, citalopram — avoid tricyclics in elderly/cardiac patients). Do not wait — untreated depression impairs rehabilitation participation. [1]
Spasticity and shoulder pain
- Spasticity: Early physiotherapy and stretching. Focal spasticity: botulinum toxin injection. Generalised: baclofen, tizanidine
- Shoulder subluxation and pain: Common in hemiplegic arm. Support with sling/lapboard, avoid traction on the arm during handling and transfers [1]
Rehabilitation
Rehabilitation starts in the acute stroke unit, not after discharge. The principles:
- Early, intensive, task-specific therapy — the greatest gains are in the first 3 months
- Multidisciplinary team approach with goal-setting
- Intensity matters — more therapy time produces better outcomes (within patient tolerance)
- Constraint-induced movement therapy for upper limb recovery in selected patients
- Early supported discharge (ESD) — for mild-moderate stroke patients, returning home with a coordinated community rehab team produces equivalent outcomes to inpatient rehab at lower cost [1]
The modified Rankin Scale (mRS) is the standard outcome measure (0 = no symptoms, 1 = no significant disability, 2 = slight disability, 3 = moderate disability, 4 = moderately severe disability, 5 = severe disability, 6 = death). A mRS of 0-2 is generally defined as "functional independence." [1]
Prognosis
| Outcome | Ischaemic stroke | Haemorrhagic stroke |
|---|---|---|
| 30-day mortality | ~10-15% | ~30-40% (ICH), ~30-50% (SAH) |
| Functional independence (mRS 0-2) at 90 days | ~50% (higher with thrombolysis/thrombectomy) | ~20-30% |
| Recurrence risk (1 year) | ~10% (highest in first 90 days) | Varies by cause |
Key prognostic factors: Age, NIHSS on presentation, infarct volume on imaging, comorbidities (AF, diabetes, CKD), time to reperfusion, and whether reperfusion was achieved. [1]
DCE long-case approach
Opening statement (SASPOP)
"Mrs Chen is a 74-year-old woman who presents with sudden onset right-sided weakness and inability to speak, witnessed by her husband 2 hours ago. She has a background of paroxysmal atrial fibrillation (not on anticoagulation), hypertension, type 2 diabetes, and dyslipidaemia. [1]
Her main problems are:
- Acute left MCA territory ischaemic stroke, NIHSS 14, presenting within the thrombolysis window — immediate IV thrombolysis required
- Paroxysmal atrial fibrillation — not anticoagulated, likely cardioembolic source
- Hypertension (BP 175/95) — will need lowering before thrombolysis (target under 185/110)
- Type 2 diabetes (HbA1c 72) — risk factor and complicating factor
- Dysphagia risk — requires formal swallow assessment before any oral intake
- Secondary prevention planning — anticoagulation timing, statin, BP, glycaemic control [1]
Integrated management plan
Present in three phases: [1]
-
Immediate (minutes): Confirm last-known-well time (within 4.5 hours). Check glucose (exclude hypoglycaemia). Lower BP to under 185/110 if needed. Non-contrast CT to exclude haemorrhage. If ischaemic and criteria met — administer tenecteplase 0.25 mg/kg bolus. CTA head/neck for thrombectomy assessment. [1]
-
Acute (hours to days): Stroke unit admission. BP post-thrombolysis under 180/105 for 24 hours. Glycaemic control 4-10 mmol/L. Normothermia. Swallow assessment. DVT prophylaxis at 24 hours. Repeat imaging at 24 hours before starting antiplatelet or anticoagulation. [1]
-
Long-term: Start high-intensity statin. Anticoagulation for AF after the appropriate interval (moderate stroke — approximately day 6). BP target under 130/80 long-term. Carotid Doppler to exclude concomitant large artery stenosis. Rehabilitation with MDT. Address post-stroke depression screening at 1 month. [1]
DCE examiner probing questions you must anticipate:
- "Why is she not on anticoagulation for her AF?" → Common real-world scenario — patient refusal, perceived bleeding risk, or missed diagnosis. Address the root cause in the plan.
- "When will you start anticoagulation?" → Use the 1-3-6-12 rule based on stroke severity. For NIHSS 14, approximately day 6, with repeat CT to exclude haemorrhagic transformation.
- "What is her prognosis?" → NIHSS 14 suggests moderate-severe stroke. Without treatment, approximately 30% chance of functional independence. With thrombolysis within 2 hours, this improves significantly. [1]
DCE short-case approach: neurological examination post-stroke
Instruction: "Examine this patient's neurological system." [1]
Systematic routine (cranial nerves, motor, sensory, coordination, gait)
- General inspection: Observe for facial asymmetry, hemiparetic posture (flexed upper limb, extended lower limb), neglect (patient ignores one side), communication difficulty (aphasia — assess fluency, comprehension, repetition)
- Cranial nerves: Visual fields (homonymous hemianopia — PCA or MCA), pupils and eye movements (gaze palsy, nystagmus), facial symmetry (UMN facial weakness — forehead spared), tongue and palate
- Motor: Tone (spasticity is a late sign; acute stroke is flaccid), power (MRC grade — document the face/arm/leg gradient), reflexes (initially absent or reduced in acute stroke; hyperreflexia and Babinski develop over hours to days)
- Sensory: Pinprick and light touch — document the pattern (hemisensory, crossed). Joint position sense and vibration if suspected posterior column lesion
- Coordination: Finger-nose, heel-shin — cerebellar signs suggest posterior circulation or the cerebellar connections
- Higher cortical function: Language (fluency, comprehension, naming, repetition, reading, writing), neglect (double simultaneous stimulation, line bisection), executive function
- Gait: Hemiparetic gait (circumduction), ataxic gait (cerebellar) [1]
Presentation template
"I examined Mrs Chen's neurological system. She is alert and cooperative but has obvious difficulty with speech production. On cranial nerve examination, there is a right homonymous hemianopia. The patient has a right upper motor neuron facial weakness with forehead sparing. [1]
In the upper limbs, tone is reduced on the right. Power is 3/5 in the right arm and hand, 5/5 on the left. In the lower limbs, power is 4/5 in the right leg, 5/5 on the left. Reflexes are initially reduced on the right with an extensor plantar response on the right. Sensation is reduced to pinprick on the right side of the body. Coordination is limited on the right by weakness but intact on the left. [1]
Her speech is non-fluent with preserved comprehension — consistent with Broca aphasia. She does not demonstrate overt neglect. [1]
In summary, these findings localise to a left middle cerebral artery territory infarct, with right hemiparesis (arm worse than leg), Broca aphasia, and right homonymous hemianopia. The arm-worse-than-leg pattern and the cortical sign of aphasia distinguish this from a lacunar stroke." [1]
Key DWE MCQ patterns
- Thrombolysis eligibility (3-4.5 hr exclusions): A patient at 4 hours — if over 80, prior stroke + diabetes, or on oral anticoagulant, they are not eligible in the 3-4.5 hour window.
- Thrombectomy window: LVO on CTA at 8 hours with perfusion mismatch — eligible for thrombectomy (DAWN/DEFUSE-3). Even at 20 hours if clinical-imaging mismatch.
- Lacunar vs cortical: Hemiparesis with no cortical signs = lacunar. Hemiparesis + aphasia/neglect/visual field defect = cortical (MCA).
- Wallenberg syndrome: Ipsilateral face + contralateral body sensory loss, Horner, ataxia → lateral medullary (PICA/vertebral). Posterior circulation, not carotid.
- DAPT for minor stroke: Aspirin + clopidogrel for 21-90 days (CHANCE/POINT), then de-escalate to single antiplatelet. Only for non-cardioembolic minor stroke/TIA.
- CEA timing: Symptomatic stenosis 70-99% — refer within 2 weeks. The stenosis must be ipsilateral to the symptoms.
- BP post-thrombolysis: Under 180/105 for 24 hours. Pre-thrombolysis: under 185/110.
- ICH on warfarin: Immediate PCC + vitamin K. Do not wait for repeat INR. [1]
References
[1] NINDS rt-PA Stroke Study Group — rt-PA within 3 hours of ischaemic stroke onset; 30% more likely to have minimal/no disability at 3 months. [2] ECASS III (Hacke et al., 2008) — Alteplase in the 3-4.5 hour window; extended the thrombolysis window from 3 to 4.5 hours. [3] SITS-MOST (Wahlgren et al., 2007) — Real-world safety of alteplase within 3 hours in routine practice; symptomatic ICH rate comparable to RCTs. [4] MR CLEAN (Berkhemer et al., 2015) — First positive RCT of intra-arterial thrombectomy within 6 hours of anterior circulation LVO. [5] HERMES (Goyal et al., 2016) — Individual patient data meta-analysis of 5 RCTs; thrombectomy doubles functional independence in LVO within 6 hours (NNT 2.6). [6] DAWN (Nogueira et al., 2018) — Thrombectomy 6-24 hours with clinical-imaging mismatch; 49% vs 13% functional independence. [7] DEFUSE-3 (Albers et al., 2018) — Thrombectomy 6-16 hours with perfusion imaging selection; core under 70 mL, mismatch ratio at least 1.8. [8] PROFESS (Sacco et al., 2008) — Aspirin-dipyridamole vs clopidogrel for secondary prevention; equivalent efficacy and safety. [9] CHANCE (Wang et al., 2013) — Aspirin + clopidogrel for 21 days in minor stroke/TIA; 32% relative risk reduction in recurrent stroke at 90 days vs aspirin alone. [10] NASCET (Barnett et al., 1998) — CEA benefit for symptomatic stenosis 50-69% (moderate, NNT 15) and 70-99% (severe, NNT 3-6).
AHA/ASA Guidelines for Early Management of Acute Ischemic Stroke (2019); ESO Stroke Guidelines; Stroke Foundation of Australia Clinical Guidelines for Stroke Management; NICE NG128. [1]
References
- [1]The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group Tissue plasminogen activator for acute ischemic stroke N Engl J Med, 1995.PMID 7477192
- [2]Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke N Engl J Med, 2008.PMID 18815396
- [3]Wahlgren N, Ahmed N, Davalos A, et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study Lancet, 2007.PMID 17258667
- [4]Berkhemer OA, Fransen PSS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke N Engl J Med, 2015.PMID 25517348
- [5]Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials Lancet, 2016.PMID 26898852
- [6]Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct N Engl J Med, 2018.PMID 29129157
- [7]Albers GW, Marks MP, Kemp S, et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging N Engl J Med, 2018.PMID 29364767
- [8]Sacco RL, Diener HC, Yusuf S, et al. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke N Engl J Med, 2008.PMID 18753638
- [9]Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack N Engl J Med, 2013.PMID 23803136
- [10]Barnett HJM, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators N Engl J Med, 1998.PMID 9811916