Phys · neurological
Transient Ischaemic Attack and Carotid Disease
Also known as TIA · mini-stroke · carotid stenosis · ABCD2 · dual antiplatelet therapy · CEA · carotid stenting · NASCET
Consultant-physician guide to TIA and symptomatic carotid disease — tissue-based definition, urgent risk stratification, dual antiplatelet therapy after high-risk TIA or minor stroke, carotid imaging and revascularisation thresholds, and secondary prevention — structured for FRACP DWE and DCE.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
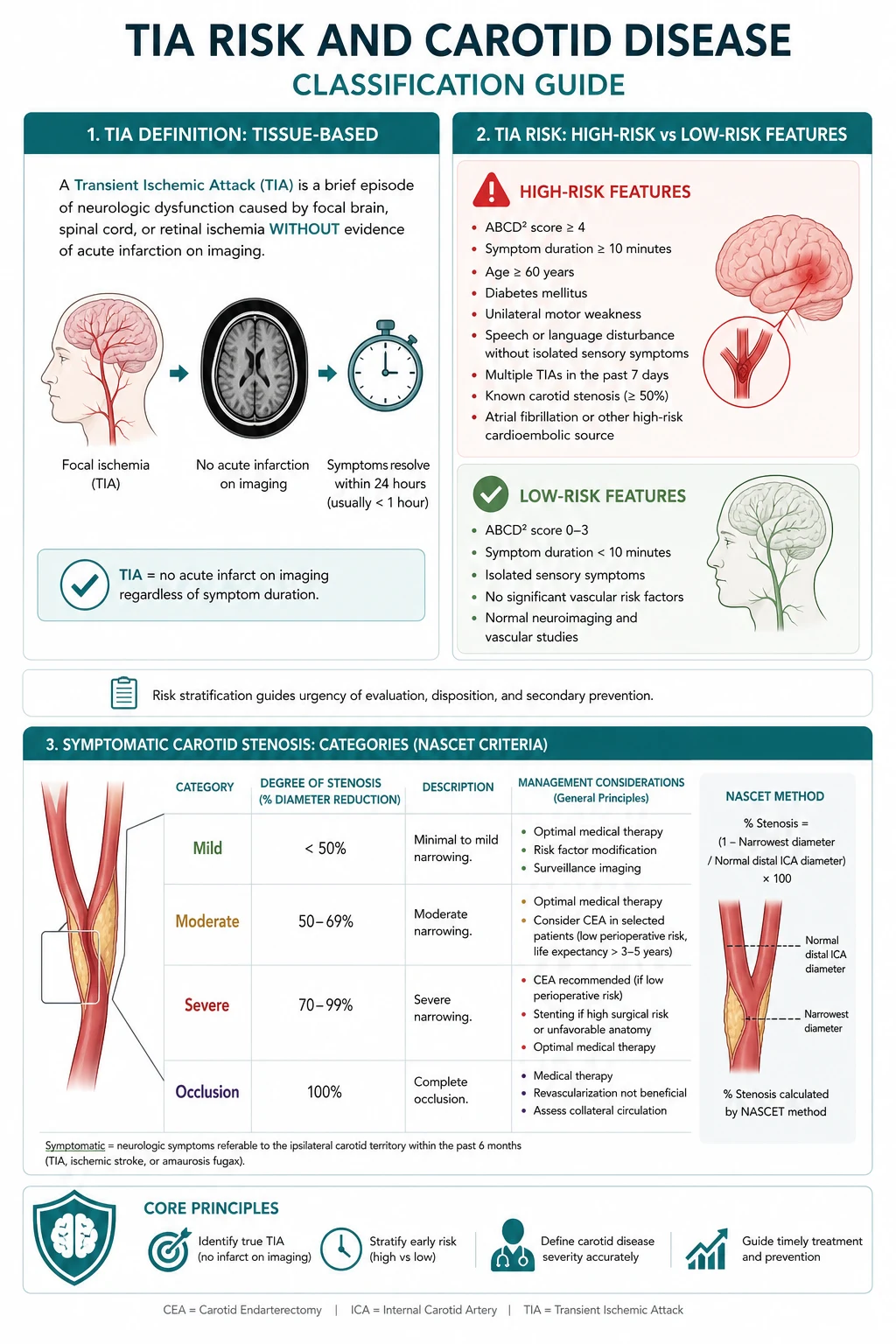
A TIA is a brief episode of neurological dysfunction caused by focal brain, spinal cord or retinal ischaemia without acute infarction on tissue-based definition. [10] The clinical job is not to reassure because the deficit resolved. The job is to prevent the next event in the hours and days when risk is highest. [1] [5]
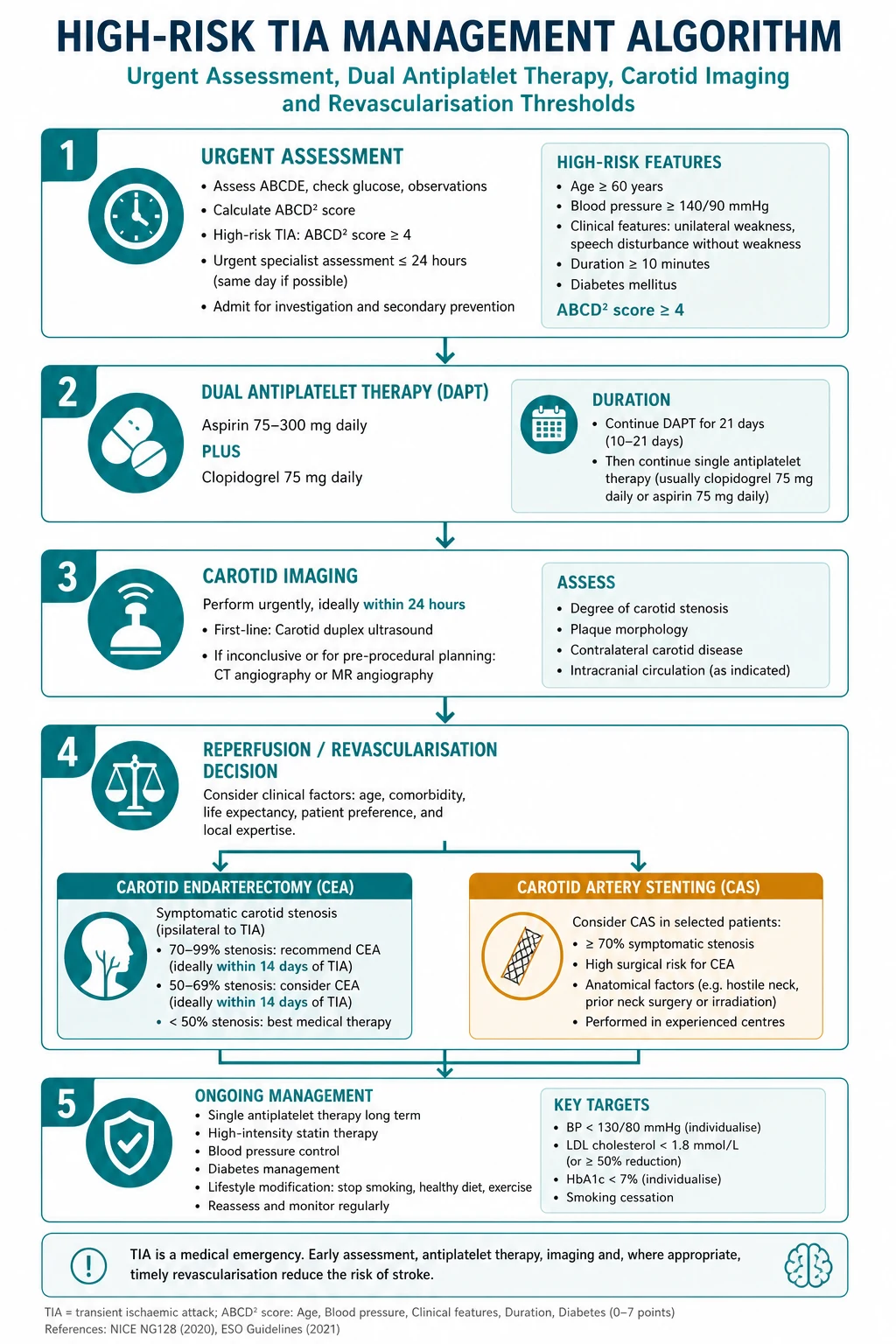
For high-risk TIA or minor non-cardioembolic ischaemic stroke, short dual antiplatelet therapy with aspirin plus clopidogrel reduces early recurrence when started promptly and stopped after a short course. [2] [3] Urgent specialised assessment, same-admission or same-day vascular imaging, and rapid treatment of carotid stenosis and risk factors cut stroke rates in the EXPRESS model of care. [5] [6]
For symptomatic extracranial carotid stenosis of high grade, carotid endarterectomy reduces recurrent ipsilateral stroke when performed with acceptable perioperative risk; stenting is an alternative in selected anatomy and risk profiles. [9] [4]

Definition and why the label still matters
The AHA scientific statement moved TIA from a pure time-based definition (under 24 hours) to a tissue-based definition: a transient episode of neurological dysfunction caused by focal ischaemia without acute infarction. [10] Diffusion-weighted MRI frequently shows infarction in clinically transient events; those patients are reclassified as minor stroke but the prevention pathway is the same high-risk ischaemic pathway. [7]
Operationally, any sudden focal neurological symptom that could be ischaemic — hemiparesis, aphasia, monocular vision loss, dense hemisensory loss — is a cerebrovascular emergency until imaging and work-up say otherwise. [7] [8]
Risk after TIA — front-loaded and modifiable
Early stroke risk after TIA is front-loaded. Clinical scores such as ABCD2 help communicate risk and research stratification, but they are incomplete alone and must not be used to discharge high-risk phenotypes without urgent assessment. [1] Large observational cohorts such as TIAregistry.org show that with rapid modern care, early stroke risk can be substantially lower than historical series — the point is that systems of care change outcomes. [11]
The EXPRESS studies demonstrated that urgent assessment and immediate initiation of secondary prevention after TIA or minor stroke markedly reduced early recurrent stroke compared with a delayed outpatient model. [5] [6] That is the service design lesson examiners want: same-day pathway, not next-available clinic.
Differentials that steal the diagnosis
Not every transient neurological spell is a TIA. Key mimics: [7]
- Migraine aura (positive phenomena, slower march, younger patient, headache association)
- Focal seizure with Todd paresis (positive motor features, post-ictal state)
- Syncope or hypoperfusion (global rather than focal)
- Peripheral vestibulopathy (isolated vertigo without other brainstem signs is usually not TIA)
- Functional or metabolic disturbance [7]
Cortical features (aphasia, neglect, monocular vision loss) raise the pre-test probability of ischaemia. Pure sensory or isolated dizziness without other signs needs careful scrutiny, not automatic TIA labelling. [7]
Pathophysiology in one line that changes management
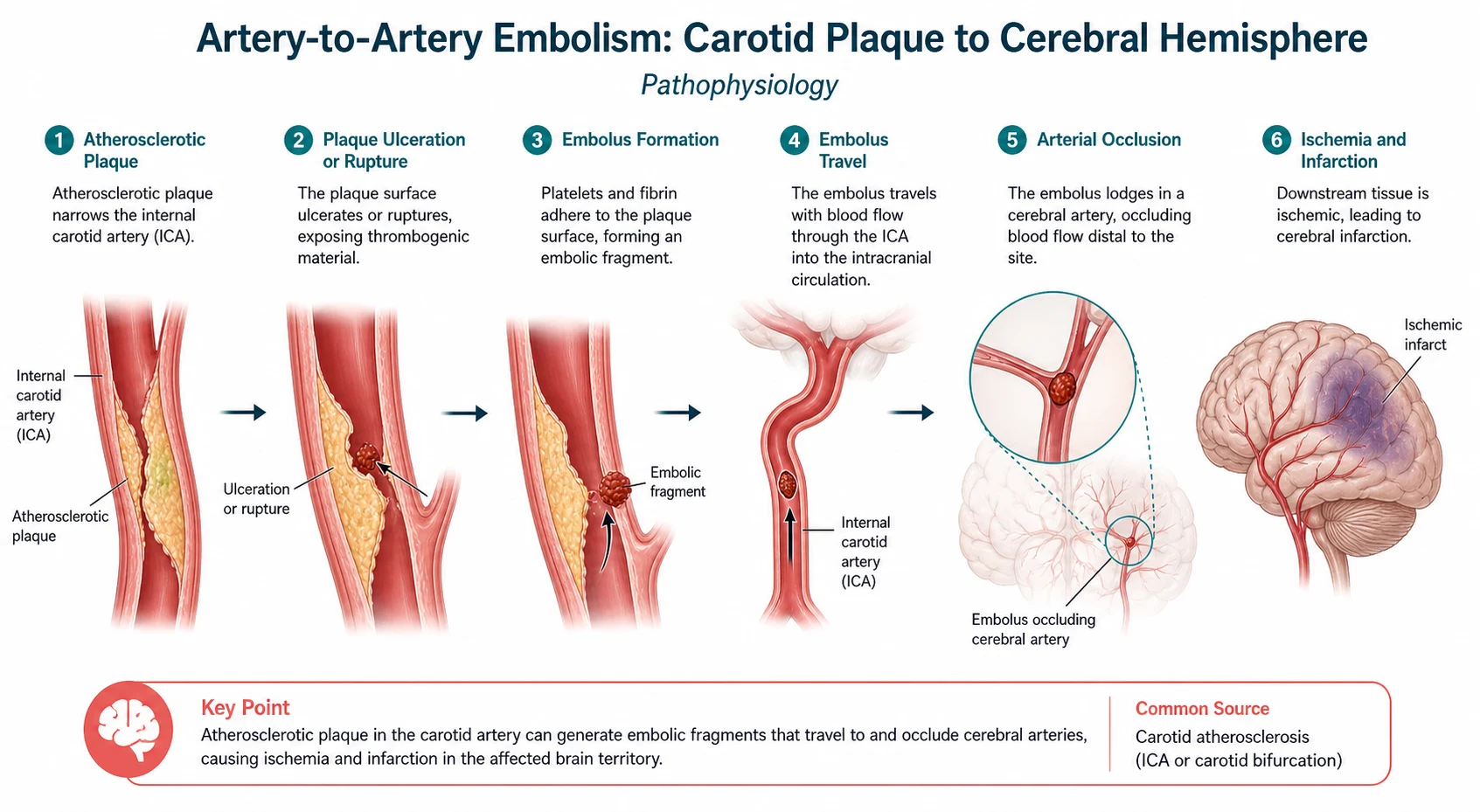
Most non-cardioembolic TIAs related to carotid disease are artery-to-artery embolism from unstable plaque or local hypoperfusion across a critical stenosis. That is why antiplatelet therapy, plaque stabilisation (statin, BP control) and timely revascularisation of high-grade symptomatic stenosis reduce early recurrence. [9] [8]
Cardioembolism (especially atrial fibrillation) is a different pathway: it needs rhythm monitoring and anticoagulation decisions, not dual antiplatelet therapy as the long-term answer. Always branch the work-up: large-artery, cardioembolism, small-vessel, other, undetermined. [8]
Urgent assessment package
History: exact onset, duration, residual symptoms, stereotyped recurrence, AF history, neck trauma, migraine, seizure clues, medications (antiplatelets, anticoagulants), bleeding risk. [7]
Examination: full neurological exam, heart rhythm and murmurs, bilateral BP, carotid bruits (supportive only), fundoscopy if monocular symptoms. [7]
Investigations (same day or admission):
- Non-contrast CT brain if hyperacute stroke pathway still live; MRI with DWI when available for tissue definition. [10]
- Vascular imaging of the extracranial carotids urgently — duplex, CTA or MRA depending on local pathway — because revascularisation benefit is time-sensitive after symptoms. [7] [9]
- ECG and prolonged rhythm monitoring for AF when mechanism is unclear. [8]
- Labs: glucose, lipids, FBC, coagulation, renal function. [8]
Dual antiplatelet therapy after high-risk TIA or minor stroke
CHANCE and POINT showed that aspirin plus clopidogrel started early after high-risk TIA or minor non-cardioembolic ischaemic stroke reduces early recurrent stroke compared with aspirin alone. [2] [3] The benefit is early; bleeding rises if dual therapy is prolonged unnecessarily. In practice:
- Confirm non-cardioembolic mechanism pathway (not an AF patient who needs anticoagulation).
- Load and continue short dual therapy per trial-aligned local protocol, then step down to single antiplatelet.
- Avoid stacking with full anticoagulation.
- Counsel on bleeding signs and drug interactions (including omeprazole–clopidogrel debates in local formulary guidance). [2] [3] [8]
ESO and AHA secondary prevention documents place this short dual therapy strategy in the modern high-risk TIA/minor stroke toolbox alongside risk-factor control. [7] [8]
Carotid revascularisation — symptomatic thresholds
NASCET established that carotid endarterectomy benefits patients with recent symptomatic high-grade stenosis when perioperative risk is acceptable. [9] Benefit is greatest soon after the index event and in higher-grade stenosis. Moderate symptomatic stenosis needs individualised decision-making; near-occlusion and chronic total occlusion are different conversations. [9] [8]
CREST compared stenting with endarterectomy and found similar composite outcomes with different periprocedural stroke/MI trade-offs; age and anatomy influence modality choice. [4] The physician role is to:
- Confirm the stenosis is symptomatic (same-side TIA/stroke in the relevant territory).
- Quantify stenosis with quality imaging.
- Refer urgently to a high-volume vascular/stroke team.
- Optimise medical therapy immediately regardless of procedure. [4] [8] [9]
Asymptomatic carotid disease is a separate evidence base and must not be treated with symptomatic thresholds by reflex. [8]
Secondary prevention bundle (every patient)
- Antiplatelet (or anticoagulation if AF/cardioembolic)
- High-intensity statin
- Blood pressure target individualised but treated aggressively after the acute phase
- Diabetes optimisation
- Smoking cessation
- Lifestyle, sleep apnoea consideration, driving advice per local authority rules
- Education on 000/911 recurrence symptoms [8]
The bundle is not optional paperwork — EXPRESS-type gains came from immediate implementation, not delayed GP letters alone. [5] [6]
DCE long-case angles
Classic long case: recent TIA, diabetes and hypertension, carotid bruit or known stenosis, polypharmacy, driving concerns, and fear of stroke. Structure: [7]
- Opening statement with mechanism hypothesis
- Problem list: index TIA, carotid disease, vascular risk factors, bleeding risk, social/driving
- Plan: imaging results, DAPT duration, CEA/CAS referral, risk-factor targets, follow-up [7] [8]
DCE short-case angles
- Discuss significance of a carotid bruit (neither rules in nor rules out severe stenosis). [8]
- Demonstrate residual upper motor neuron signs after a recent event. [7]
- Counsel on dual antiplatelet duration and bleeding warning signs. [8]
Exam traps
- Treating resolved deficit as benign.
- Using ABCD2 alone to avoid imaging or specialist review. [1]
- Prolonging dual antiplatelets for months without indication. [2] [3]
- Confusing symptomatic and asymptomatic carotid thresholds. [9]
- Missing AF and leaving the patient on antiplatelets alone long term. [8]
- Delaying carotid referral until "the next clinic" after a hemispheric TIA with 80% stenosis. [5] [9]
References
- [1]Johnston SC, Rothwell PM, Nguyen-Huynh MN, Giles MF, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack Lancet, 2007.PMID 17258668
- [2]Wang Y, Wang Y, Zhao X, Liu L, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack N Engl J Med, 2013.PMID 23803136
- [3]Johnston SC, Easton JD, Farrant M, Barsan W, et al. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA N Engl J Med, 2018.PMID 29766750
- [4]Brott TG, Hobson RW 2nd, Howard G, Roubin GS, et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis N Engl J Med, 2010.PMID 20505173
- [5]Rothwell PM, Giles MF, Chandratheva A, Marquardt L, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison Lancet, 2007.PMID 17928046
- [6]Luengo-Fernandez R, Gray AM, Rothwell PM Effect of urgent treatment for transient ischaemic attack and minor stroke on disability and hospital costs (EXPRESS study): a prospective population-based sequential comparison Lancet Neurol, 2009.PMID 19200786
- [7]Fonseca AC, Merwick Á, Dennis M, Ferrari J, et al. European Stroke Organisation (ESO) guidelines on management of transient ischaemic attack Eur Stroke J, 2021.PMID 34414306
- [8]Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association Stroke, 2021.PMID 34024117
- [9]North American Symptomatic Carotid Endarterectomy Trial Collaborators, Barnett HJM, Taylor DW, Haynes RB, et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis N Engl J Med, 1991.PMID 1852179
- [10]Easton JD, Saver JL, Albers GW, Alberts MJ, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists Stroke, 2009.PMID 19423857
- [11]Amarenco P, Steering Committee Investigators of the TIAregistry.org Risk of Stroke after Transient Ischemic Attack or Minor Stroke N Engl J Med, 2016.PMID 27464211