Phys · oncological
Breast Cancer (Physician Perspective)
Also known as breast cancer · breast carcinoma · invasive ductal carcinoma · invasive lobular carcinoma · ductal carcinoma in situ · DCIS · lobular carcinoma in situ · LCIS · triple-negative breast cancer · TNBC · HER2-positive breast cancer · hormone receptor positive breast cancer · ER positive breast cancer · BRCA1 · BRCA2 · trastuzumab · Herceptin · tamoxifen · aromatase inhibitor · anastrozole · letrozole · exemestane · pembrolizumab · olaparib · sentinel lymph node biopsy · breast-conserving surgery
Consultant-physician guide to breast cancer — the most common cancer in women worldwide and the second leading cause of cancer death. Organised around the receptor subtype framework (ER/PR, HER2, triple-negative) that drives every systemic therapy decision. Covers epidemiology and risk factors (BRCA1/2, PALB2, reproductive and lifestyle factors), BreastScreen Australia screening and high-risk MRI surveillance, pathology (DCIS, LCIS, invasive ductal and lobular), TNM staging, surgical principles (breast-conserving therapy, sentinel node biopsy), adjuvant and neoadjuvant systemic therapy (endocrine — tamoxifen and aromatase inhibitors with ovarian suppression; HER2-targeted — trastuzumab, pertuzumab, T-DM1; immunotherapy — pembrolizumab for triple-negative; PARP inhibition — olaparib for BRCA), metastatic management by site, treatment complications (cardiotoxicity, osteoporosis, endometrial cancer, lymphoedema), and hereditary risk reduction (BRCA — bilateral mastectomy and salpingo-oophorectomy).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Breast Cancer (Physician Perspective)

The answer first
Breast cancer is the most commonly diagnosed cancer in women worldwide and the second leading cause of cancer death in women. In Australia, a woman has a 1 in 8 lifetime risk of developing breast cancer. Its central importance to a physician is that it is screenable, treatable, and increasingly survivable — over 90 percent five-year survival for localised disease — and the entire field turns on one idea: the receptor subtype determines the systemic therapy [1].
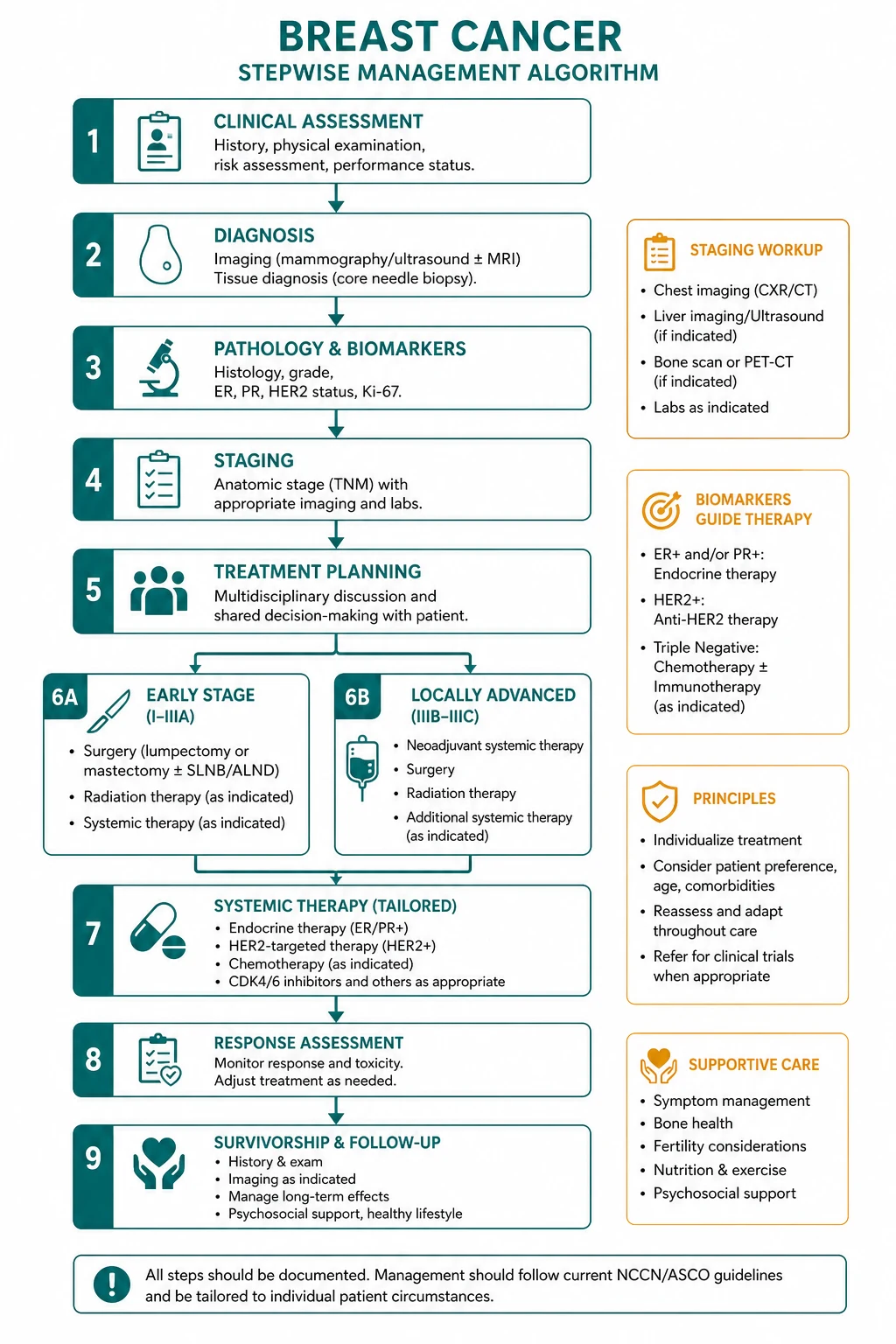
The single organising principle: breast cancer management is driven by the TNM stage and the receptor profile (ER, PR, HER2). Know the receptors and the stage and you know the treatment. Surgery and radiotherapy address the locoregional disease; endocrine therapy, chemotherapy, HER2-targeted therapy, immunotherapy, and PARP inhibition address the systemic risk [3][5][8].
The treatment ladder, by subtype and stage: [1]
- DCIS (stage 0) — surgery (WLE or mastectomy) plus radiotherapy after WLE; endocrine therapy for ER-positive DCIS is considered.
- Early-stage ER-positive, HER2-negative — surgery, then adjuvant endocrine therapy (tamoxifen if premenopausal, aromatase inhibitor if postmenopausal, ovarian function suppression for high-risk); chemotherapy guided by genomic assays (Oncotype DX) in node-negative disease [3][4][12].
- HER2-positive — surgery, then chemotherapy plus trastuzumab for 1 year; neoadjuvant TCHP for tumours over 2 cm or node-positive; T-DM1 for residual disease [5][7].
- Triple-negative — neoadjuvant pembrolizumab plus chemotherapy (KEYNOTE-522), then adjuvant pembrolizumab; olaparib for germline BRCA carriers [8][9].
- Metastatic — systemic therapy guided by receptor subtype; bone-targeted therapy (bisphosphonates or denosumab) for bone disease; palliative radiotherapy for symptomatic sites.
DWE high-yield: The answer to almost every breast cancer management question is "determine the receptor status (ER, PR, HER2) and the stage." ER-positive gets endocrine therapy (tamoxifen if premenopausal, AI if postmenopausal, add OFS if high-risk premenopausal). HER2-positive gets trastuzumab for 1 year. Triple-negative gets pembrolizumab plus chemotherapy neoadjuvantly. BRCA-mutated HER2-negative gets olaparib. Never give an AI to a premenopausal woman without ovarian suppression [3][4][8][9].
Epidemiology and risk factors
Breast cancer is the most commonly diagnosed cancer in women worldwide, with approximately 2.3 million new cases and 670 000 deaths in 2022 [1]. In Australia, the lifetime risk is 1 in 8 for a woman, and the age-standardised incidence is among the highest in the world, reflecting reproductive patterns (late first pregnancy, nulliparity, fewer births), hormone use, and the established screening programme.
Risk factors
| Risk factor | Mechanism / magnitude |
|---|---|
| Female sex | Breast cancer is 100 times more common in women than in men |
| Age | Risk increases throughout life; most cases occur after age 50 |
| Family history | One first-degree relative roughly doubles risk; the risk is higher the younger the relative was at diagnosis |
| BRCA1 / BRCA2 mutations | BRCA1: 60 to 70 percent lifetime breast risk, often triple-negative; BRCA2: 50 to 60 percent, often ER-positive; both increase ovarian cancer risk |
| Other inherited genes | PALB2 (30 to 60 percent lifetime risk), TP53 (Li-Fraumeni syndrome), CHEK2 (moderate risk), CDH1 (lobular) |
| Early menarche (before 12) | Longer lifetime oestrogen exposure |
| Late menopause (after 55) | Longer lifetime oestrogen exposure |
| Nulliparity or late first pregnancy (after 30) | Pregnancy differentiates breast epithelium and is protective; nulliparity removes this protection |
| Hormone replacement therapy | Combined oestrogen-progestogen HRT increases risk; risk falls after stopping |
| Combined oral contraceptive pill | Small transient increase in risk |
| Alcohol | Dose-dependent risk increase; there is no safe lower limit |
| Obesity (postmenopausal) | Peripheral aromatisation of androgens to oestrogens in adipose tissue |
| Radiation exposure | Chest irradiation before age 30 (e.g. mantle radiotherapy for Hodgkin lymphoma) significantly increases risk |
| Prior breast biopsy with atypia | Atypical ductal or lobular hyperplasia increases risk 4- to 5-fold |
| Dense breast tissue | Independent risk factor and reduces mammographic sensitivity |
DWE trap: A family history of breast cancer does not automatically mean a BRCA mutation. Only about 5 to 10 percent of breast cancers are hereditary. The red flags that increase the likelihood of a hereditary syndrome are: early onset (under 40), triple-negative histology (under 60), bilateral disease, male breast cancer, ovarian cancer in the family, Ashkenazi Jewish ancestry, and multiple affected relatives across generations. [1]
Pathology — in situ and invasive disease
Ductal carcinoma in situ (DCIS)
DCIS is a non-invasive malignancy — malignant epithelial cells proliferate within the ductal basement membrane without breaching it into the surrounding stroma. It is a non-obligate precursor to invasive ductal carcinoma: if untreated, some (not all) DCIS will progress to invasive cancer over 10 to 30 years. DCIS presents most commonly as microcalcifications on screening mammography and is confirmed on core biopsy. [1]
The management of DCIS is surgical — wide local excision with clear margins (if feasible) or mastectomy (for extensive or multicentric disease). Radiotherapy after breast-conserving surgery reduces local recurrence, as demonstrated by the EBCTCG meta-analysis [2]. Endocrine therapy (tamoxifen) for ER-positive DCIS is considered to reduce ipsilateral and contralateral recurrence, though its role is less established than in invasive disease.
Lobular carcinoma in situ (LCIS)
LCIS is not cancer — it is a risk marker indicating increased bilateral breast cancer risk (approximately 1 to 2 percent per year, 25 to 30 percent over 15 to 20 years). It is characterised by small, uniform cells filling the acini without stromal invasion. LCIS is typically ER-positive, is often incidental on biopsy for another lesion, and is managed with close surveillance and risk-reducing endocrine therapy (tamoxifen) rather than excision. The key exam point: LCIS is a marker, DCIS is a cancer (in situ). [1]
Invasive ductal carcinoma (no special type)
Invasive ductal carcinoma is the commonest histology, accounting for 70 to 75 percent of invasive breast cancers. It arises from ductal epithelium, breaches the basement membrane, and invades the surrounding stroma. It presents as a hard, irregular, fixed mass and may cause skin dimpling, nipple retraction, or axillary lymphadenopathy. Grading (Elston-Ellis: tubule formation, nuclear pleomorphism, mitotic count) provides prognostic information. [1]
Invasive lobular carcinoma
Invasive lobular carcinoma accounts for 10 to 15 percent of invasive breast cancers. It is defined by loss of E-cadherin (CDH1 gene on chromosome 16q), a cell adhesion molecule. The histological hallmark is the single-file infiltration pattern — discohesive cells infiltrating the stroma in linear strands, producing a diffusely thickened breast rather than a discrete mass. Clinically and radiologically, lobular carcinoma is more difficult to detect — it often eludes mammography due to its diffuse growth pattern, and MRI is more sensitive. Lobular carcinoma has a higher rate of bilaterality (up to 20 percent synchronous or metachronous) and tends to metastasise to unusual sites (peritoneum, retroperitoneum, gastrointestinal tract, ovary, meninges). [1]
Receptor subtypes — the organising framework
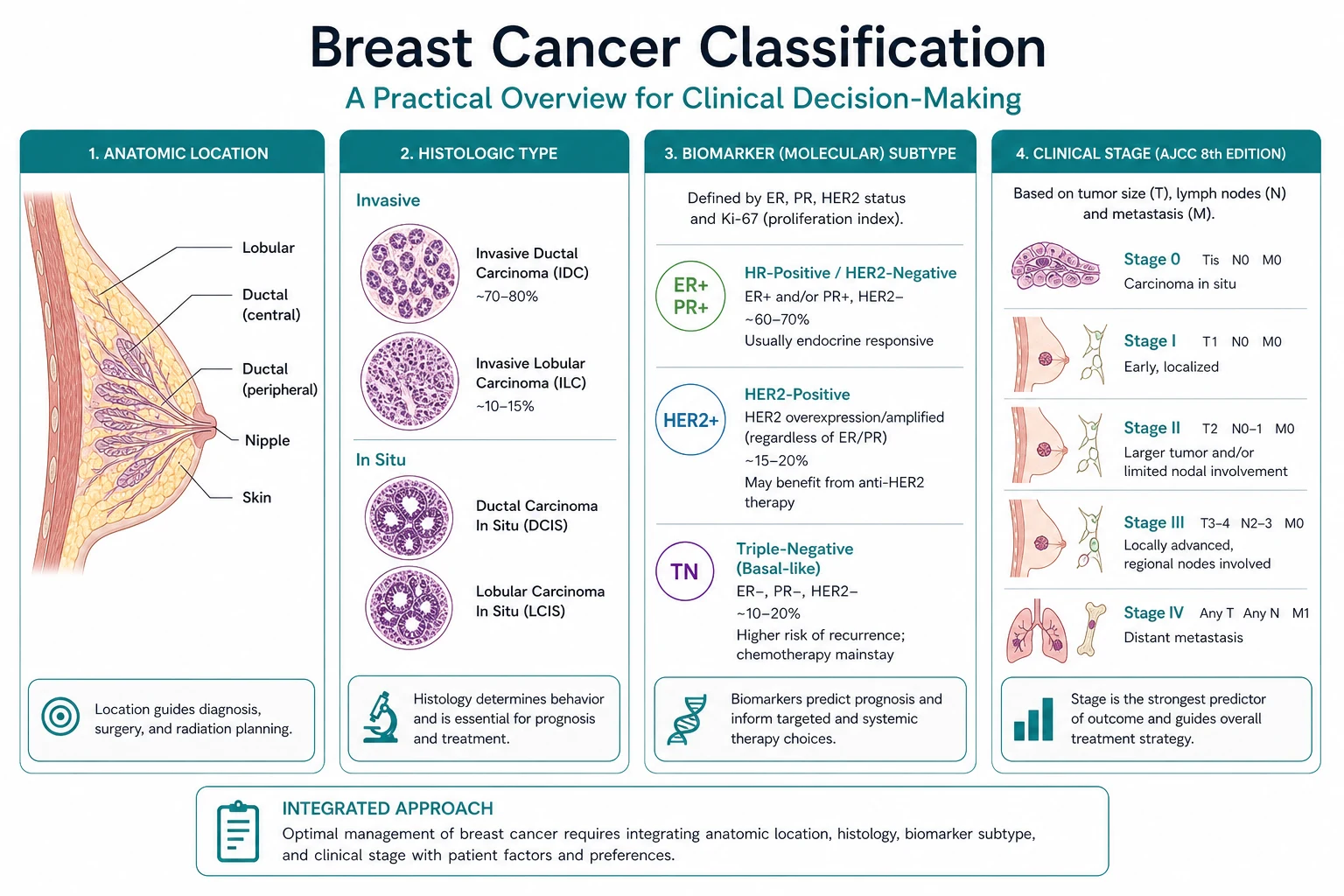
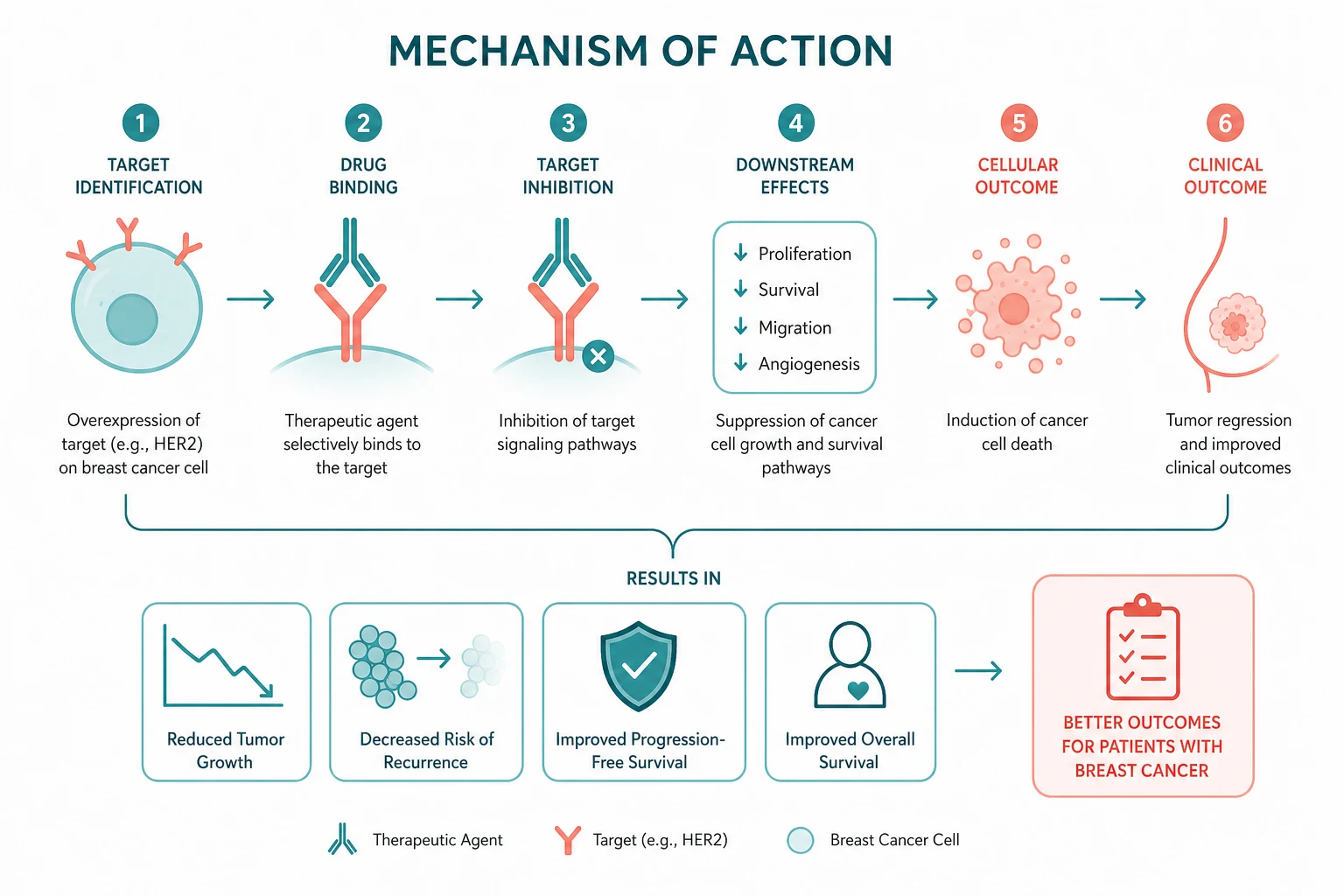
The receptor profile — oestrogen receptor (ER), progesterone receptor (PR), and HER2 — is determined by immunohistochemistry on the core biopsy and is the single most important determinant of systemic therapy. Breast cancers are classified into four intrinsic subtypes that drive treatment decisions [3][5][8].
Luminal A (ER-positive, HER2-negative)
The commonest and most favourable subtype. ER strongly positive, PR positive, low Ki-67 (under 20 percent), low grade. Treatment: surgery, then adjuvant endocrine therapy (tamoxifen or aromatase inhibitor for 5 to 10 years). Chemotherapy is reserved for high-risk features (large tumour, node-positive, high Oncotype DX score) [3][12].
Luminal B (ER-positive, HER2-positive or high Ki-67)
ER-positive but either HER2-positive or with high proliferation (Ki-67 over 20 percent). More aggressive than luminal A but still endocrine-responsive. Treatment: endocrine therapy plus HER2-targeted therapy (if HER2-positive) and often chemotherapy. [1]
HER2-enriched (ER-negative, HER2-positive)
Driven by ERBB2 gene amplification on chromosome 17q, causing overexpression of the HER2 receptor. Historically the most aggressive subtype, now dramatically improved by HER2-targeted therapy. Treatment: chemotherapy plus trastuzumab for 1 year, with pertuzumab added in neoadjuvant and metastatic settings, and T-DM1 for residual disease [5][6][7].
Triple-negative / basal-like (ER-negative, PR-negative, HER2-negative)
The most aggressive subtype, accounting for 10 to 15 percent of breast cancers. Lacks all three receptors, so endocrine therapy and trastuzumab are ineffective. Tends to occur in younger women and is strongly associated with BRCA1 mutations. Treatment: neoadjuvant pembrolizumab plus platinum-taxane chemotherapy (KEYNOTE-522), then adjuvant pembrolizumab; olaparib for germline BRCA carriers [8][9].
DWE high-yield — test ER, PR, and HER2 on every new breast cancer. The receptor profile is non-negotiable and determines the entire systemic strategy. HER2 testing uses immunohistochemistry (3+ is positive, 0 is negative, 2+ is equivocal and requires in situ hybridisation for amplification). Missing a HER2-positive tumour denies the patient the single most transformative targeted therapy in oncology. Missing a triple-negative tumour denies immunotherapy and BRCA testing [5][8].
Screening — finding cancer before it is palpable
Screening works because mammography can detect breast cancer at a pre-clinical stage, when treatment is most effective. The EBCTCG meta-analysis of 17 trials involving over 10 800 women demonstrated that radiotherapy after breast-conserving surgery halved the 10-year recurrence rate and reduced 15-year breast cancer mortality by about a sixth, underscoring the importance of early detection [2].
BreastScreen Australia
BreastScreen Australia offers biennial screening mammography to asymptomatic women aged 50 to 74 at average risk. This age range is targeted because breast cancer incidence rises sharply after 50, mammographic sensitivity increases as the breast involutes (becomes fattier), and the benefit-to-harm ratio is most favourable. Women aged 40 to 49 and over 74 may also screen but are not actively invited, as the evidence for benefit is weaker in these groups. [1]
High-risk screening (BRCA carriers)
Women with a BRCA1 or BRCA2 mutation require enhanced surveillance that goes beyond the standard programme: [1]
- Annual breast MRI from age 30 to 50 (MRI is more sensitive in dense young breasts and does not use ionising radiation).
- Annual mammography from age 40 (often alternating with MRI at 6-monthly intervals).
- Clinical breast examination every 6 to 12 months. [1]
Mammography alone is inadequate for BRCA carriers, as the dense breast tissue of younger women reduces sensitivity and the cancer risk begins much earlier than the general screening age. Breast MRI surveillance detects cancers at a smaller size and earlier stage in this high-risk group. [1]
When to refer for genetic testing
Germline genetic testing for BRCA1, BRCA2, PALB2, TP53, and CHEK2 should be offered to: [1]
- Any woman diagnosed with breast cancer under age 40.
- Any woman with triple-negative breast cancer under age 60.
- Any woman with bilateral breast cancer.
- Any man with breast cancer.
- Any woman with a family history of breast and ovarian cancer meeting referral criteria (e.g. two breast cancers under 50, breast and ovarian cancer in the family, Ashkenazi Jewish ancestry with a breast cancer diagnosis). [1]
Staging — the TNM system
Breast cancer is staged using the AJCC TNM system (8th edition), which integrates tumour size (T), nodal status (N), and metastasis (M), modified by receptor status and grade. [1]
Tumour (T):
- Tis: in situ (DCIS or LCIS)
- T1: 20 mm or less (T1mi: microinvasion under 1 mm; T1a: up to 5 mm; T1b: 5 to 10 mm; T1c: 10 to 20 mm)
- T2: 21 to 50 mm
- T3: over 50 mm
- T4: extension to chest wall or skin (inflammatory carcinoma is T4d) [1]
Nodes (N):
- N0: no regional node metastasis
- N1: movable ipsilateral axillary nodes (1 to 3)
- N2: fixed or matted ipsilateral axillary nodes, or internal mammary nodes
- N3: infraclavicular or supraclavicular nodes, or extensive axillary and internal mammary involvement [1]
Metastasis (M):
- M0: no distant metastasis
- M1: distant metastasis (bone, lung, liver, brain) [1]
Stage grouping maps TNM to prognostic categories: stage 0 (in situ), stage I (small, node-negative), stage II (larger or limited nodal), stage III (locally advanced), stage IV (metastatic). Five-year survival ranges from over 99 percent for stage I to approximately 30 percent for stage IV. [1]
Management — the physician perspective
Surgery
Surgical management is a shared decision between the breast surgeon and the patient, but the physician must understand the principles to guide adjuvant therapy. [1]
Breast-conserving surgery (BCS): Wide local excision (WLE) removes the tumour with a margin of normal tissue, preserving the breast. BCS must be followed by whole-breast radiotherapy — the EBCTCG meta-analysis showed that omitting radiotherapy after BCS halves the local recurrence rate and increases breast cancer mortality [2]. BCS is equivalent to mastectomy in survival for most early-stage tumours, provided clear margins are achieved and radiotherapy is delivered.
Mastectomy: Removal of the entire breast parenchyma. Indicated for large tumours (relative to breast size), multicentric disease, failure to achieve clear margins with BCS, known BRCA mutation (risk-reducing), or patient preference. Immediate or delayed reconstruction should be discussed. [1]
Sentinel lymph node biopsy (SLNB): The standard axillary staging procedure for clinically node-negative disease. The NSABP B-32 trial established that SLNB is equivalent to axillary lymph node dissection (ALND) for overall survival and regional control in node-negative patients, with significantly less morbidity (lymphoedema, sensory loss, restricted shoulder movement) [10]. A negative sentinel node spares the patient ALND.
Axillary management after a positive sentinel node: The ACOSOG Z0011 trial showed that in women with T1 to T2 tumours and 1 to 2 positive sentinel nodes undergoing BCS with whole-breast radiotherapy, omitting completion ALND does not compromise survival [11]. This is a practice-changing finding that has spared many women the morbidity of full axillary clearance.
Adjuvant systemic therapy
Endocrine therapy for ER-positive disease is the cornerstone of adjuvant treatment for the majority of breast cancers: [1]
- Premenopausal women: Tamoxifen 20 mg daily for 5 to 10 years. Tamoxifen is a SERM that blocks the oestrogen receptor in breast tissue. For higher-risk premenopausal women (node-positive, young age, large tumour), ovarian function suppression (OFS) with a GnRH agonist (goserelin) should be added, combined with either tamoxifen or an aromatase inhibitor (exemestane). The SOFT trial established that OFS plus exemestane is superior to tamoxifen alone in higher-risk premenopausal women who remained premenopausal after chemotherapy [4].
- Postmenopausal women: Aromatase inhibitor (anastrozole, letrozole, or exemestane) for 5 to 10 years. Aromatase inhibitors block peripheral conversion of androgens to oestrogens and are superior to tamoxifen in postmenopausal women, as demonstrated by the ATAC trial [3]. Aromatase inhibitors are ineffective and potentially harmful in premenopausal women unless ovarian function is suppressed.
Endocrine therapy side effects and monitoring:
- Tamoxifen: hot flushes, VTE (2- to 3-fold increased risk), endometrial proliferation and cancer (2- to 3-fold increased risk — investigate any postmenopausal bleeding), and ovarian cysts in premenopausal women.
- Aromatase inhibitors: hot flushes, arthralgia (common, may limit adherence), osteoporosis (baseline DEXA, bisphosphonate or denosumab prophylaxis), and vaginal dryness. [1]
Adjuvant chemotherapy is indicated for high-risk disease: node-positive (especially 4 or more nodes), large tumours (over 5 cm), triple-negative subtype, HER2-positive subtype, or high Oncotype DX recurrence score (over 25 in node-negative ER-positive disease, per TAILORx) [12]. Standard regimens are anthracycline and taxane based (e.g. dose-dense AC followed by paclitaxel, or docetaxel, cyclophosphamide). The principal toxicities are alopecia, myelosuppression, nausea, peripheral neuropathy (taxanes), and cardiotoxicity (anthracyclines).
HER2-targeted therapy for HER2-positive disease: Trastuzumab (monoclonal antibody to the HER2 extracellular domain) for 1 year, added to chemotherapy. The HERA trial established the survival benefit of 1 year of adjuvant trastuzumab after chemotherapy [5]. Two years offered no additional benefit. Baseline and serial echocardiography (every 3 months) is mandatory, as trastuzumab causes reversible LV dysfunction in 2 to 7 percent [5].
Neoadjuvant therapy
Neoadjuvant systemic therapy is given before surgery to downstage the tumour (enabling breast-conserving surgery), to assess treatment response (pathologic complete response is a prognostic marker), and to treat micrometastatic disease earlier. It is now the standard for: [1]
- HER2-positive tumours over 2 cm or node-positive: Docetaxel, carboplatin, trastuzumab, and pertuzumab (TCHP). The pathologic complete response rate is approximately 40 to 60 percent, and patients who achieve pCR have excellent outcomes. Those with residual disease switch to T-DM1 (KATHERINE trial) [7].
- Triple-negative tumours over 2 cm or node-positive: Pembrolizumab plus platinum-taxane chemotherapy (KEYNOTE-522), followed by surgery and adjuvant pembrolizumab. This improved both pCR and event-free survival [8].
Neoadjuvant therapy does not improve survival compared with the same therapy given adjuvantly, but it provides critical information about tumour biology and enables response-adapted escalation (T-DM1 for residual HER2-positive disease) or de-escalation. [1]
HER2-positive metastatic disease
First-line therapy for HER2-positive metastatic breast cancer is pertuzumab, trastuzumab, and docetaxel (the CLEOPATRA regimen), which demonstrated significantly improved progression-free and overall survival compared with trastuzumab and docetaxel alone [6]. After progression, T-DM1 is the standard second-line therapy. Later lines include trastuzumab deruxtecan (T-DXd), lapatinib plus capecitabine, and tucatinib-based regimens (especially for brain metastases).
Triple-negative metastatic disease
For PD-L1-positive triple-negative metastatic breast cancer, pembrolizumab plus chemotherapy (nab-paclitaxel, paclitaxel, or gemcitabine plus carboplatin) is the first-line standard. For PD-L1-negative disease, platinum-based chemotherapy (especially for BRCA carriers, who are platinum-sensitive) is preferred. Sacituzumab govitecan (antibody-drug conjugate targeting Trop-2) is approved for refractory disease. [1]
ER-positive metastatic disease
For ER-positive HER2-negative metastatic breast cancer, endocrine-based therapy is preferred over chemotherapy for bone-only or low-burden visceral disease. First-line after progression on a non-steroidal aromatase inhibitor: a CDK4/6 inhibitor (palbociclib, ribociclib, or abemaciclib) combined with fulvestrant, or exemestane plus everolimus. These significantly improve progression-free survival. Chemotherapy is reserved for visceral crisis, endocrine resistance, or rapid progression. [1]
Olaparib for BRCA-mutated disease
The OlympiA trial established that 1 year of adjuvant olaparib (a PARP inhibitor) significantly improves invasive disease-free survival and distant disease-free survival in patients with germline BRCA1 or BRCA2 mutations and high-risk HER2-negative early breast cancer [9]. Olaparib exploits synthetic lethality: the PARP enzyme repairs single-strand DNA breaks; inhibiting it in a cell that already has defective homologous recombination (BRCA loss) causes lethal double-strand breaks selectively in the tumour. Olaparib is now a standard adjuvant therapy for germline BRCA-mutated HER2-negative breast cancer after completion of standard chemotherapy.
Metastatic disease — site-specific management
Bone metastases
Bone is the commonest site of breast cancer metastasis. Sclerotic (osteoblastic) lesions are characteristic, particularly in ER-positive disease. Management includes: [1]
- Bone-targeted therapy: Zoledronic acid (bisphosphonate) or denosumab (RANKL inhibitor) every 4 weeks to reduce skeletal-related events (pathological fractures, spinal cord compression, hypercalcaemia, need for radiotherapy or surgery).
- Palliative radiotherapy for painful lesions (single 8 Gy fraction is often sufficient).
- Orthopaedic intervention for impending pathological fractures (prophylactic fixation).
- Systemic therapy guided by receptor subtype. [1]
Visceral metastases
Liver, lung, and pleural metastases are managed with systemic therapy guided by the receptor subtype. Pleural effusions are drained and may require pleurodesis. Pericardial effusion is an oncological emergency requiring drainage. [1]
Brain metastases
Breast cancer is the second commonest cause of brain metastases after lung cancer. HER2-positive and triple-negative subtypes have higher rates of brain metastasis. Management depends on the number and size of lesions: [1]
- Single or oligometastatic (1 to 3 lesions): Stereotactic radiosurgery (SRS) — Gamma Knife or linac-based — preserves cognitive function better than whole-brain radiotherapy.
- Multiple lesions or leptomeningeal disease: Whole-brain radiotherapy (WBRT) with hippocampal sparing where possible.
- Systemic therapy: Tucatinib (for HER2-positive) penetrates the blood-brain barrier. Lapatinib and trastuzumab also have some CNS activity. [1]
Complications of treatment
| Complication | Cause | Management |
|---|---|---|
| Lymphoedema | Axillary clearance, radiotherapy | Compression garments, manual lymphatic drainage, physiotherapy; prevent by avoiding venepuncture and blood pressure cuffs on the affected arm |
| Cardiotoxicity | Anthracyclines (dose-dependent, irreversible); trastuzumab (reversible LV dysfunction) | Baseline and serial echocardiography; hold trastuzumab if LVEF drops below 50 percent or falls by 10 percent; ACE inhibitor and beta-blocker for LV dysfunction |
| Osteoporosis | Aromatase inhibitors reduce bone mineral density | Baseline DEXA; calcium and vitamin D; bisphosphonate or denosumab prophylaxis |
| Endometrial cancer | Tamoxifen (partial oestrogen agonist on uterus) | Investigate any postmenopausal bleeding with transvaginal ultrasound and biopsy; consider switching to AI if postmenopausal |
| VTE | Tamoxifen, especially in the first 2 years and with surgery | Assess VTE risk; consider prophylactic anticoagulation during hospitalisation; avoid tamoxifen in high-VTE-risk patients |
| Peripheral neuropathy | Taxane chemotherapy (docetaxel, paclitaxel) | Dose reduction; may be persistent; supportive care |
| Premature menopause | Chemotherapy, ovarian function suppression | Vasomotor symptom management; fertility preservation counselling before treatment; bone health monitoring |
| Skin toxicity | Anti-EGFR therapy (rash, though not used in breast cancer); radiation dermatitis | Supportive skin care |
Hereditary breast cancer and risk reduction
BRCA1 and BRCA2
Germline mutations in BRCA1 (chromosome 17q) and BRCA2 (chromosome 13q) impair homologous recombination DNA repair and confer a high lifetime risk of breast and ovarian cancer. BRCA1-associated breast cancers are more often triple-negative, while BRCA2-associated cancers are usually ER-positive [9].
For a known BRCA carrier who has not developed cancer: [1]
- Risk-reducing bilateral mastectomy reduces breast cancer risk by over 90 percent. It is the most effective prevention strategy but is a personal decision requiring thorough counselling on surgical morbidity, body image, and psychosocial impact.
- Bilateral salpingo-oophorectomy (BSO) is recommended around age 35 to 40 (BRCA1) or 40 to 45 (BRCA2), after childbearing, to reduce ovarian cancer risk (BRCA1: 40 to 60 percent lifetime; BRCA2: 15 to 25 percent). BSO also reduces breast cancer risk by approximately 50 percent if performed premenopausally.
- Enhanced surveillance: Annual breast MRI from age 30 to 50, then annual mammography. [1]
For a BRCA carrier diagnosed with breast cancer: [1]
- Olaparib for 1 year as adjuvant therapy for high-risk HER2-negative disease (OlympiA) [9].
- Discussion of contralateral risk-reducing mastectomy (the contralateral breast cancer risk in a BRCA carrier is 3 to 4 percent per year).
Other hereditary syndromes
- PALB2: Partner and localiser of BRCA2; 30 to 60 percent lifetime breast risk. Management similar to BRCA, though data on olaparib benefit are emerging.
- TP53 (Li-Fraumeni syndrome): Very high lifetime cancer risk (breast, sarcoma, brain, adrenocortical, leukaemia). Breast cancer risk approaches 90 percent by age 60. Annual whole-body MRI surveillance from childhood. Avoidance of radiation therapy where possible (due to radiation-induced second cancers).
- CHEK2: Moderate lifetime risk (20 to 40 percent). Management is individualised; enhanced screening is recommended. [1]
Survivorship and long-term care
Breast cancer survivors represent a growing population, and the physician plays a central role in their long-term care. The key domains are: [1]
Surveillance for recurrence: Clinical review every 6 to 12 months for 5 years then annually; annual mammography (for the conserved and contralateral breast). Routine blood tests and imaging are not recommended in asymptomatic women with early-stage disease (they do not improve survival and increase false positives), but are indicated for symptoms or stage III disease. [1]
Late effects of treatment:
- Cardiac surveillance: Women who received anthracyclines and/or trastuzumab require ongoing cardiac monitoring, as late cardiotoxicity can emerge years later.
- Bone health: Aromatase inhibitor users need DEXA monitoring and bone-protective therapy.
- Lymphoedema management: Chronic, progressive; early intervention with compression and physiotherapy.
- Endocrine side effects: Vasomotor symptoms, vaginal dryness, sexual dysfunction, and musculoskeletal symptoms may persist for years.
- Cognitive effects: Chemobrain (cognitive impairment after chemotherapy) is real and may persist. [1]
Psychosocial support: Anxiety, depression, fear of recurrence, body image concerns, and relationship and work impacts are common. Access to psychology, peer support, and survivorship programmes improves quality of life. [1]
Comorbidity management: The leading cause of death in long-term breast cancer survivors is cardiovascular disease, not breast cancer — cardiovascular risk factor management is essential. [1]
The physician at the coalface
The physician encounters breast cancer in several distinct contexts, each requiring a different emphasis: [1]
-
The symptomatic patient (ED or outpatient): A woman with a new breast lump, nipple discharge, or bone pain. The physician's role is to initiate the triple assessment (clinical examination, imaging, core biopsy) urgently and to recognise red flags (inflammatory changes, pathological fracture, neurological symptoms suggesting cord compression). [1]
-
The perioperative patient: The physician may be asked to optimise a patient for breast surgery (cardiac risk assessment, management of anticoagulation, comorbidity optimisation) or to manage postoperative complications (infection, seroma, lymphoedema). [1]
-
The treatment-complication patient: The physician is the first port of call for treatment-related complications — febrile neutropenia, cardiotoxicity, VTE, endometrial bleeding on tamoxifen, osteoporotic fracture on an aromatase inhibitor. Recognising these and managing them promptly is critical. [1]
-
The metastatic patient: The physician may be the first to see a breast cancer survivor presenting with bone pain, breathlessness, jaundice, or neurological symptoms. Urgent imaging (CT, MRI for spinal cord compression), staging, and referral to medical oncology are the priorities. [1]
-
The survivor: The physician provides longitudinal care, managing comorbidities, surveillance, late effects, and psychosocial support — the model of the physician as the coordinator of complex, chronic, multisystem care. [1]
DWE summary: Breast cancer management is driven by the receptor subtype (ER, PR, HER2) and the TNM stage. ER-positive: endocrine therapy (tamoxifen if premenopausal, AI if postmenopausal, add OFS if high-risk premenopausal). HER2-positive: chemotherapy plus trastuzumab for 1 year (TCHP neoadjuvantly, T-DM1 for residual disease). Triple-negative: pembrolizumab plus chemotherapy neoadjuvantly (KEYNOTE-522). BRCA-mutated HER2-negative: olaparib (OlympiA). Never give an AI to a premenopausal woman without ovarian suppression. Always investigate postmenopausal bleeding on tamoxifen. Monitor cardiac function with trastuzumab and anthracyclines. Screen BRCA carriers with annual MRI from age 30 [3][4][5][8][9].
BreastScreen Australia biennial mammography 50 to 74; BRCA carriers annual MRI 30 to 50; Cancer Australia and EviQ treatment protocols; NICE NG101; NCCN Breast Cancer Guidelines; ASCO biomarker and survivorship guidelines. [1]
References
- [1]Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin, 2024.PMID 38572751
- [2]Early Breast Cancer Trialists Collaborative Group (EBCTCG) Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials Lancet, 2011.PMID 22019144
- [3]Howell A, Cuzick J, Baum M, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years' adjuvant treatment for breast cancer Lancet, 2005.PMID 15639680
- [4]Francis PA, Regan MM, Fleming GF, et al. Adjuvant ovarian suppression in premenopausal breast cancer N Engl J Med, 2015.PMID 25495490
- [5]Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer N Engl J Med, 2005.PMID 16236737
- [6]Baselga J, Cortes J, Kim SB, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer N Engl J Med, 2012.PMID 22149875
- [7]von Minckwitz G, Huang CS, Mano MS, et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer N Engl J Med, 2019.PMID 30516102
- [8]Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for Early Triple-Negative Breast Cancer N Engl J Med, 2020.PMID 32101663
- [9]Tutt ANJ, Garber JE, Kaufman B, et al. Adjuvant Olaparib Improves Disease-Free Survival in Early, High-Risk, BRCA-Mutated, HER2- Breast Cancer Oncologist, 2021.PMID 34152054
- [10]Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial Lancet Oncol, 2010.PMID 20863759
- [11]Giuliano AE, Hunt KK, Ballman KV, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial JAMA, 2011.PMID 21304082
- [12]Sparano JA, Gray RJ, Makower DF, et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer N Engl J Med, 2018.PMID 29860917