Phys · oncological
Immune Checkpoint Inhibitor Toxicity
Also known as immune-related adverse events · irAEs · checkpoint inhibitor toxicity · immunotherapy toxicity · immune checkpoint blockade adverse effects · anti-PD-1 toxicity · anti-CTLA-4 toxicity · nivolumab toxicity · pembrolizumab toxicity · ipilimumab toxicity
Consultant-physician-depth guide to immune-related adverse events from checkpoint inhibitors — the mechanism of CTLA-4 and PD-1/PD-L1 blockade, the organ-specific irAE spectrum (skin, colitis, hepatitis, pneumonitis, endocrinopathy, myocarditis, nephritis, neurotoxicity), the CTCAE grading framework, the steroid-dose ladder, second-line infliximab, vedolizumab and mycophenolate, and the recognition of the fatal toxicities (myocarditis, pneumonitis). Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Immune Checkpoint Inhibitor Toxicity
The answer first
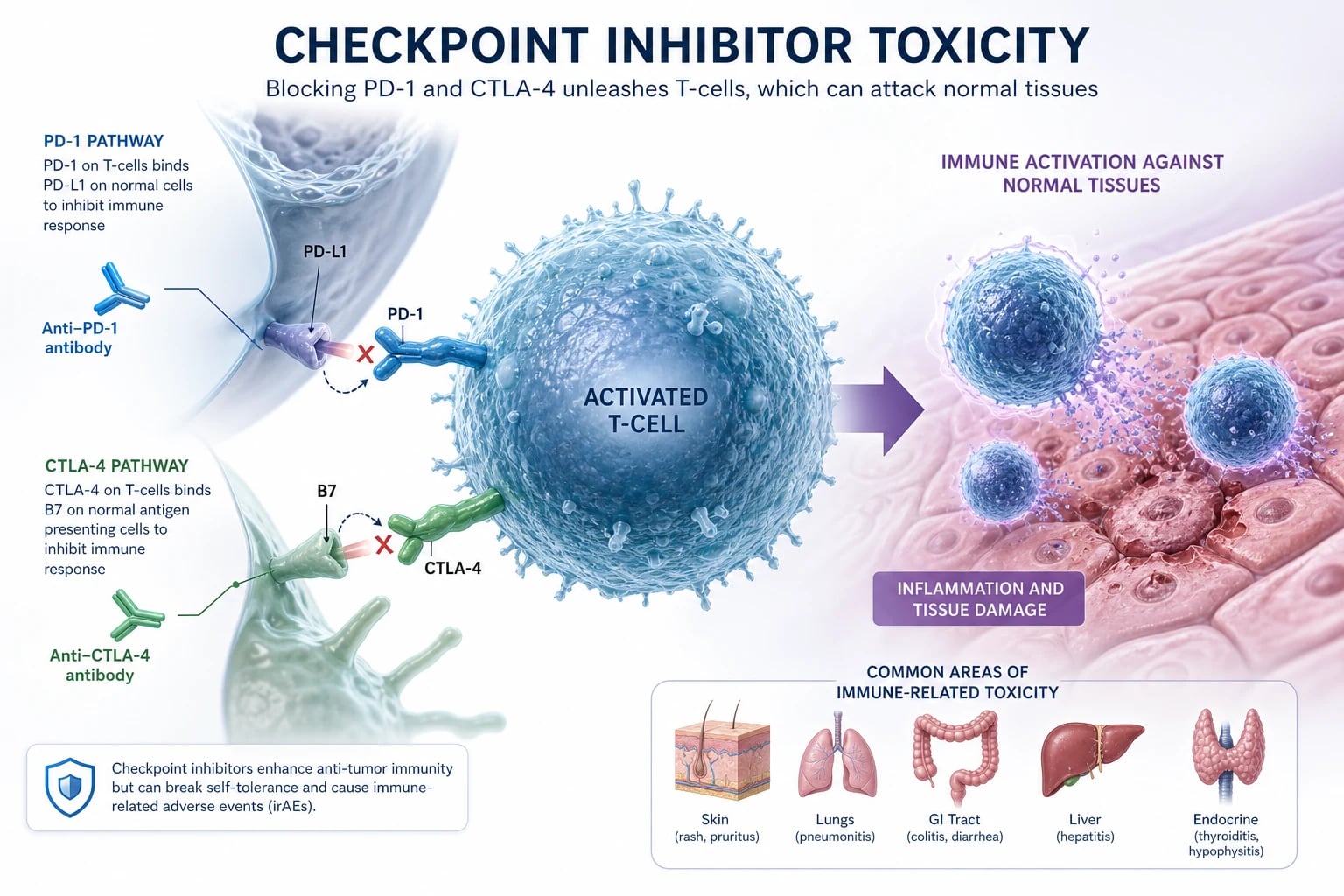
Immune checkpoint inhibitors are monoclonal antibodies that release the physiological brakes on T-cell activation — anti-CTLA-4 (ipilimumab) at the priming phase, and anti-PD-1 (nivolumab, pembrolizumab) or anti-PD-L1 (atezolizumab, durvalumab) at the effector phase [1][2][3]. The same brake-release that produces durable antitumour immunity also removes self-tolerance, so almost any organ can develop an immune-related adverse event (irAE) that is clinically and histologically indistinguishable from idiopathic autoimmune disease [6].
Three rules govern everything that follows: [1]
- Any new symptom in a patient on a checkpoint inhibitor is an irAE until proven otherwise — but you must simultaneously exclude infection, progression and alternative drug causes, because giving high-dose steroids for sepsis or an infective colitis is harmful [5][6].
- Grade the toxicity, then act on the grade. CTCAE grade 1 means continue and monitor; grade 2 means hold and use oral steroid; grade 3 to 4 means intravenous steroid, specialist input and usually permanent discontinuation. The grade drives the dose and the drug decision.
- The two diagnoses you cannot afford to miss are myocarditis and colitis. Myocarditis is rare (around 1 per cent) but kills up to half of those who develop it; colitis is common and can perforate. Both are managed with early, adequate-dose steroid [7][8].
DCE trap: In every long case involving a patient on immunotherapy, name the agent, the cycle number, and the organ system involved in the opening sentence. "This 64-year-old man on cycle 4 of ipilimumab-nivolumab for metastatic melanoma presents with grade 3 colitis" is a diagnosis and a management plan in one breath. [1]
Mechanism — why the brakes, and why toxicity
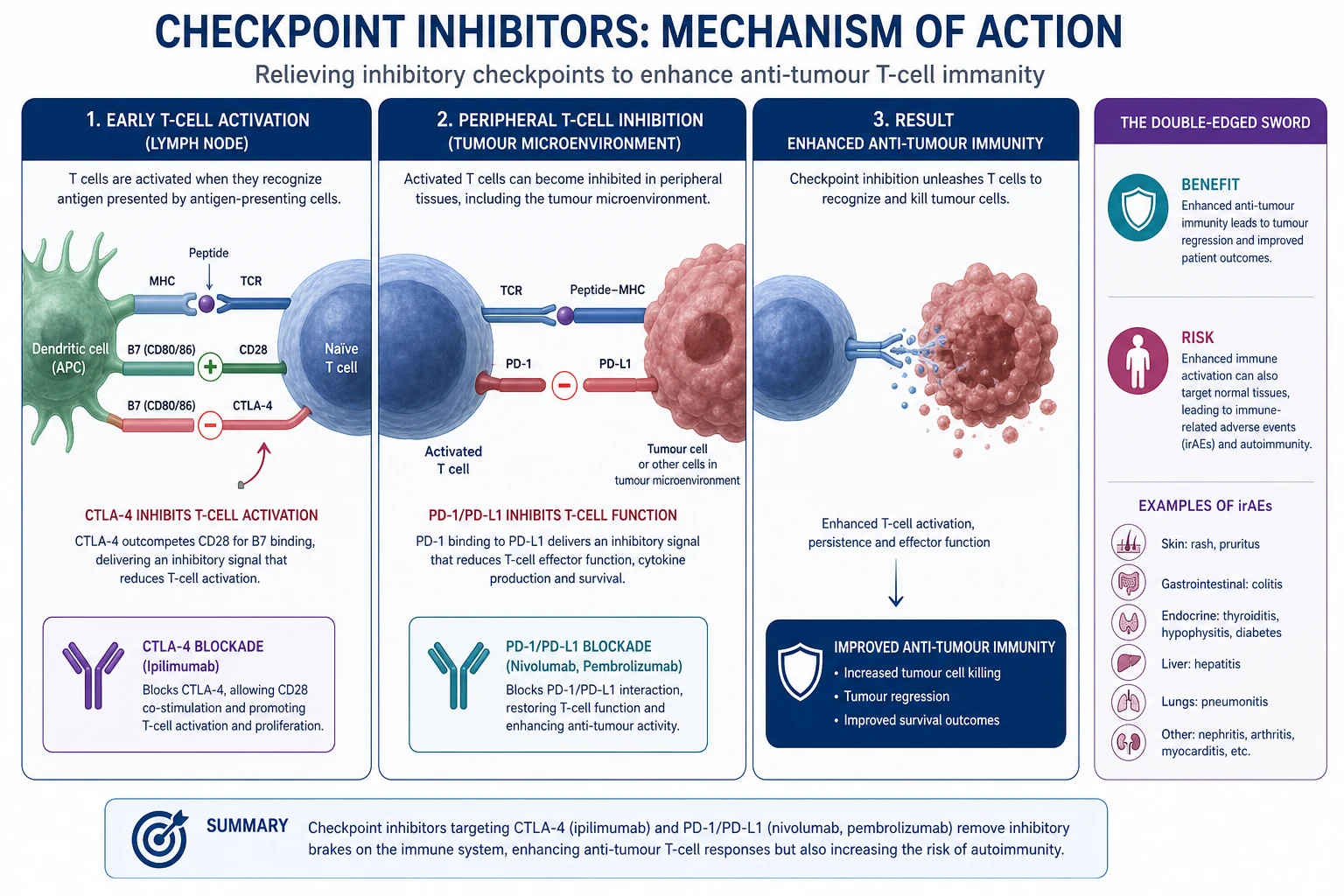
T-cell activation is a two-signal event: the T-cell receptor recognises antigen presented on MHC, and a co-stimulatory signal (CD28 binding B7) confirms it. To prevent runaway autoimmunity, the immune system has two checkpoint brakes, both targets of drug therapy [6].
CTLA-4 is upregulated on the T cell hours after activation and competes with CD28 for the B7 molecules on the antigen-presenting cell. By out-competing CD28, CTLA-4 dampens T-cell priming and proliferation — it operates in the lymph node, during priming. [1]
PD-1 is induced later, on T cells that have reached the periphery and become "exhausted" by chronic antigen exposure. It binds PD-L1 and PD-L2 on target cells (including tumour cells that have co-opted the pathway to evade immune attack) and suppresses the T cell at the effector site, in tissue. [1]
Blocking either checkpoint restores T-cell activity. Hodi and colleagues showed in 2010 that ipilimumab, an anti-CTLA-4 antibody, was the first treatment ever to improve overall survival in metastatic melanoma [1]; Topalian and Brahmer extended the paradigm to PD-1 and PD-L1 blockade in 2012 [2][3]. The drugs work because tumours exploit these brakes to hide; the drugs cause toxicity because the brakes also prevent autoimmunity.
| Checkpoint | Drug class | Agents | Site of action | Typical toxicity profile |
|---|---|---|---|---|
| CTLA-4 | Anti-CTLA-4 IgG1 | Ipilimumab, tremelimumab | Lymph node (priming) | Frequent and severe: colitis, hypophysitis, rash, hepatitis |
| PD-1 | Anti-PD-1 IgG4 | Nivolumab, pembrolizumab | Tissue (effector) | Better tolerated; pneumonitis, thyroiditis, colitis |
| PD-L1 | Anti-PD-L1 IgG1 | Atezolizumab, durvalumab, avelumab | Tissue (effector) | Lower pneumonitis than anti-PD-1; hepatitis, nephritis |
The toxicity burden scales with the target and the combination. Anti-CTLA-4 monotherapy produces grade 3 to 4 irAEs in roughly 10 to 30 per cent; anti-PD-1 in 10 to 15 per cent; and combination ipilimumab plus nivolumab in 55 per cent or more [6][9]. Combination therapy also shortens the time to onset of toxicity — most events cluster in the first 12 weeks — and lowers the threshold for permanent discontinuation.
DWE high-yield: The mechanism in one line: the drugs block the physiological off-switches on T cells (CTLA-4 in the lymph node, PD-1 in tissue), restoring antitumour immunity at the cost of autoimmunity. Know the agents by class — the class predicts the toxicity profile. [1]
The timing of irAEs
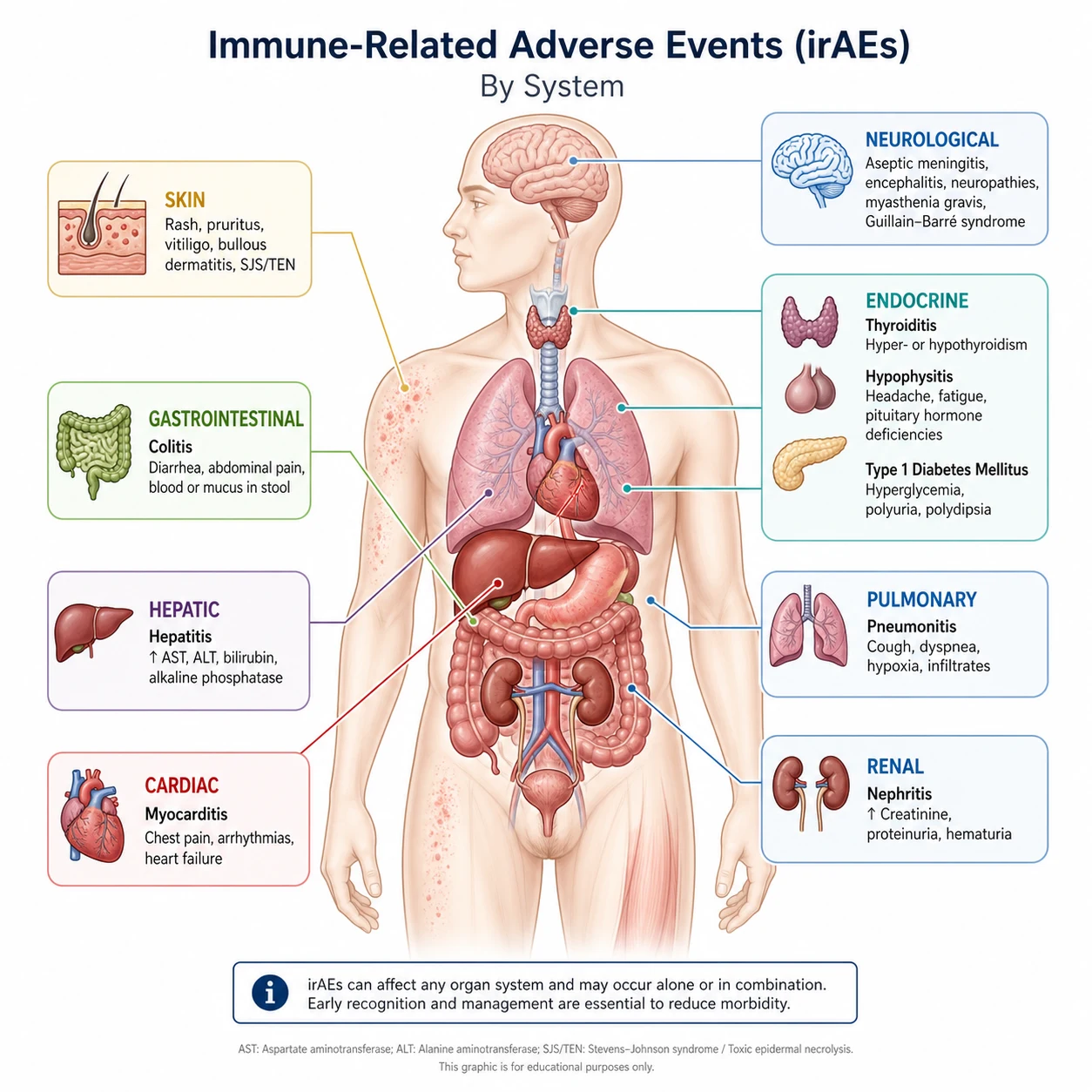
Most irAEs occur within the first 3 to 6 months of therapy, but some (notably endocrine events and neurological toxicity) can appear late, even months after the last dose. Knowing the typical timeline helps you anticipate and recognise [6].
| System | Typical onset | Comment |
|---|---|---|
| Skin (rash, pruritus) | 2 to 6 weeks | Usually the earliest; maculopapular rash on trunk |
| Gastrointestinal (colitis) | 5 to 10 weeks | Earlier with anti-CTLA-4 |
| Hepatic (transaminitis) | 6 to 14 weeks | Often silent on examination |
| Endocrine (thyroid, hypophysitis) | 4 to 12 weeks | Can be delayed; hypophysitis peaks around 9 weeks |
| Pulmonary (pneumonitis) | 2 to 12 months | Later than most; higher with anti-PD-1 and combination |
| Renal (nephritis) | 3 to 12 months | Often insidious |
| Cardiac (myocarditis) | First 3 months | Median around 30 days; can be fulminant |
| Neurological | Any time | Myasthenia, GBS, encephalitis |
Grading — the CTCAE framework that drives every decision
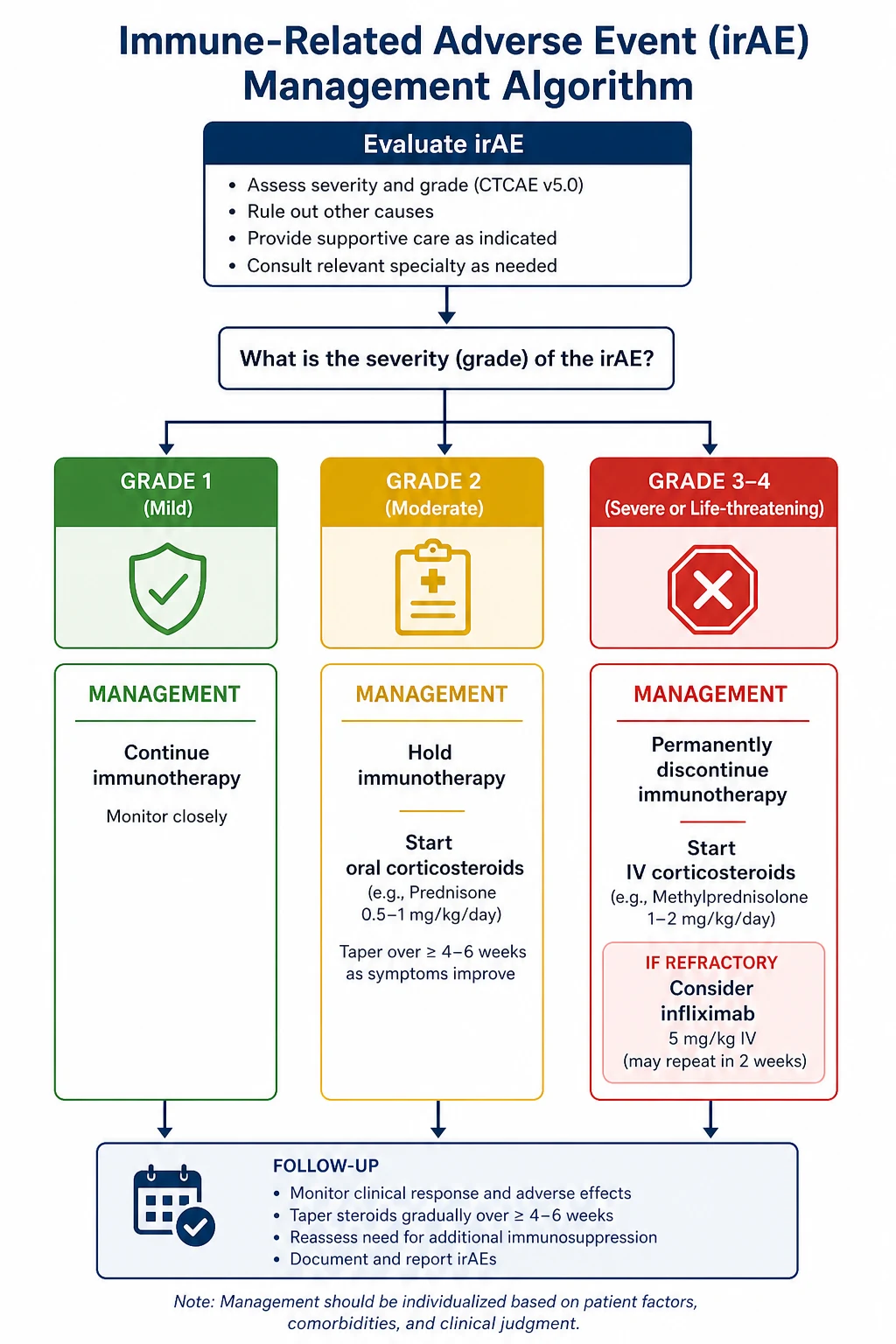
All major guidelines (ASCO, ESMO, SITC, NCCN, eviQ) use the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 to grade irAEs [5][4]. The grade, not the organ in isolation, drives the steroid dose and the decision to hold or permanently stop the drug.
| Grade | Severity | Drug decision | Steroid strategy |
|---|---|---|---|
| 1 | Mild; asymptomatic or mild symptoms; no intervention | Usually continue with close monitoring | None, or topical |
| 2 | Moderate; limits self-care; non-life-threatening | Hold until recovery to grade 1 or less | Oral prednisolone 0.5 to 1 mg/kg per day |
| 3 | Severe; hospitalisation indicated | Hold; usually permanently discontinue for vital organs | IV methylprednisolone 1 to 2 mg/kg per day |
| 4 | Life-threatening; urgent intervention | Permanently discontinue | IV methylprednisolone 1 to 2 mg/kg, often pulse 500 mg to 1 g daily |
Two principles override the table. First, some organs demand permanent discontinuation at grade 3 regardless of the general rule — pneumonitis, myocarditis, neurological irAEs, severe colitis, severe hepatitis and severe nephritis all generally mandate stopping for good. Second, endocrine irAEs are the exception that proves the grade rule — they are usually managed with hormone replacement alone (thyroxine, hydrocortisone, insulin, desmopressin), the checkpoint inhibitor is often continued, and steroids are reserved for acute inflammation such as symptomatic hypophysitis [5].
DCE trap: Never give a flat answer like "stop the drug and start steroids." The grade determines the dose and the hold-versus-stop decision. An endocrine event may need neither stopping the drug nor steroids. [1]
Skin toxicity — the common and usually the earliest
A maculopapular rash is the single most common irAE, affecting up to half of patients. It usually appears within 3 to 6 weeks, is most prominent on the trunk, and is generally mild. The danger signs that escalate the diagnosis are mucosal involvement (Stevens-Johnson syndrome or toxic epidermal necrolysis), blistering (bullous pemphigoid-like), skin pain, and eosinophilia with systemic symptoms (DRESS) [6].
Management by grade:
- Grade 1 (under 10 per cent body surface area) — continue the drug, emollients and a topical steroid, oral antihistamine for pruritus.
- Grade 2 (10 to 30 per cent body surface area) — hold the drug, oral prednisolone 0.5 to 1 mg/kg, resume when grade 1 or less.
- Grade 3 to 4 (over 30 per cent body surface area, or mucosal involvement, or blistering, or SJS/TEN features) — permanently discontinue, IV methylprednisolone 1 to 2 mg/kg, urgent dermatology and, for SJS/TEN, burns-unit transfer. [1]
Pruritus without rash is also common and responds to antihistamines; if severe, treat as grade 2 with oral steroid. Vitiligo is a recognised late sign that actually correlates with antitumour response and needs no specific treatment beyond camouflage and sun protection. [1]
Gastrointestinal toxicity — colitis is the emergency
Immunotherapy colitis is the most common reason a patient on checkpoint inhibition is admitted under general medicine, and the most common cause of fatal gastrointestinal toxicity [8]. It presents with increasing stool frequency, abdominal pain, urgency, and bloody diarrhoea; fever and peritonism signal severe disease or perforation. The median onset is 5 to 10 weeks, earlier and more severe with anti-CTLA-4.
The non-negotiable first step is to exclude infection before steroids. Send stool culture (including Salmonella, Shigella, Campylobacter, Yersinia, E. coli), Clostridioides difficile toxin, ova cysts and parasites, and consider CMV PCR in the immunosuppressed. Starting steroids first makes the stool uninterpretable and risks treating the wrong diagnosis [5][6].
| Colitis grade | Stool frequency / features | Drug | Steroid | Second line |
|---|---|---|---|---|
| 1 | 4 stools per day above baseline | Continue with loperamide and hydration | None | — |
| 2 | 4 to 6 above baseline, or abdominal pain, blood | Hold | Oral prednisolone 1 mg/kg | — |
| 3 | 7 or more above baseline, or peritonism, hospitalisation | Hold, usually permanent | IV methylprednisolone 1 to 2 mg/kg | Infliximab 5 mg/kg at 48 to 72 h |
| 4 | Life-threatening (perforation, toxic megacolon, shock) | Permanent stop | IV methylprednisolone 2 mg/kg | Infliximab or vedolizumab; surgical review |
Colonoscopy confirms the diagnosis (mucosal oedema, loss of vascular pattern, ulceration) and excludes CMV and pseudomembranous colitis histologically; a flexible sigmoidoscopy is sufficient if the patient is unstable. CT abdomen is needed if perforation or toxic megacolon is suspected. A surgical review is mandatory at the first sign of peritonism. [1]
Steroid-refractory colitis — if there is no improvement at 48 to 72 hours of adequate IV steroid, add infliximab 5 mg/kg at weeks 0, 2 and 6 (screen for tuberculosis and hepatitis B first; avoid in active infection or uncontrolled sepsis) [5]. For patients in whom infliximab is contraindicated or ineffective, vedolizumab (a gut-selective anti-alpha-4-beta-7 integrin) is the alternative — it has a slower onset but a better safety profile in coexisting hepatitis [10]. Thromboprophylaxis is essential because colonic inflammation and immobilisation are a high VTE risk.
DWE trap: The classic MCQ scenario is the patient on ipilimumab with bloody diarrhoea. The correct next step is always stool studies first, then steroids — not steroids first, not colonoscopy before stool, and not infliximab before confirming refractoriness. [1]
Hepatic toxicity — the silent transaminitis
Immune-mediated hepatitis typically presents as an asymptomatic rise in AST and ALT on routine monitoring, 6 to 14 weeks into therapy. It is essential to exclude viral and drug causes before attributing it to the checkpoint inhibitor: send hepatitis A, B, C and E serology, CMV and EBV PCR, autoimmune markers (ANA, SMA, anti-LKM), review hepatotoxic drugs (antibiotics, statins, paracetamol, alcohol), and rule out biliary obstruction with ultrasound [5].
| Hepatitis grade | AST/ALT (x ULN) | Drug | Steroid | Second line |
|---|---|---|---|---|
| 1 | 1 to 3 x ULN | Continue, monitor twice weekly | None | — |
| 2 | 3 to 5 x ULN | Hold | Oral prednisolone 0.5 to 1 mg/kg | — |
| 3 | 5 to 20 x ULN | Hold, usually permanent | IV methylprednisolone 1 to 2 mg/kg | Mycophenolate 500 to 1000 mg twice daily |
| 4 | Over 20 x ULN | Permanent stop | IV methylprednisolone 2 mg/kg | Mycophenolate; hepatology |
Mycophenolate mofetil is the preferred second-line agent for steroid-refractory hepatitis — infliximab is avoided in liver toxicity because it is itself hepatotoxic and can worsen the picture. A liver biopsy is reserved for atypical or refractory cases. Most patients recover fully with steroid and drug hold, but fulminant liver failure has been reported [8].
Pulmonary toxicity — pneumonitis kills
Checkpoint-inhibitor pneumonitis is less common than skin or gut toxicity but is a leading cause of fatal irAEs, particularly with anti-PD-1 and combination regimens [8]. It presents with new dyspnoea, cough, and sometimes chest pain or fever, and the key exam finding is hypoxia out of proportion to the chest signs. The differential is broad — infection, disease progression, pulmonary embolism, radiation pneumonitis, and heart failure all mimic it — so CT chest (showing ground-glass opacity, organising pneumonia, or interstitial infiltrates) plus cultures and, in selected cases, bronchoalveolar lavage are needed [5][6].
| Pneumonitis grade | Features | Drug | Steroid |
|---|---|---|---|
| 1 | Asymptomatic radiographic changes | Hold, monitor | None or observation |
| 2 | Symptomatic; dyspnoea on exertion | Hold, usually permanent | Oral prednisolone 1 mg/kg |
| 3 | Oxygen required; severe symptoms | Permanent stop | IV methylprednisilone 1 to 2 mg/kg |
| 4 | Life-threatening respiratory failure | Permanent stop | IV methylprednisolone 2 mg/kg; pulse; ICU |
Empirical broad-spectrum antibiotics are reasonable while infection is being excluded. For severe or steroid-refractory disease, escalate to pulse methylprednisolone 500 mg to 1 g daily for 3 days, then 1 to 2 mg/kg per day, and consider infliximab, mycophenolate or IVIG. The steroid taper must be slow (over 4 to 6 weeks at minimum) because pneumonitis relapses easily [6].
Endocrine toxicity — manage with replacement, not necessarily steroids
Endocrine irAEs differ from all others in one crucial respect: most are managed with hormone replacement alone, the checkpoint inhibitor is often continued, and steroids are reserved for acute inflammation. The four classic endocrine events are thyroiditis, hypophysitis, type 1 diabetes, and primary adrenal insufficiency. A baseline thyroid function and morning cortisol before starting therapy is essential — without it, later abnormalities are uninterpretable [5].
Thyroiditis
The classic pattern is an early destructive hyperthyroid phase (low TSH, raised free T4, with palpitations and weight loss) followed weeks later by hypothyroidism (high TSH, low free T4, with fatigue, cold intolerance and bradycardia). The hyperthyroid phase is treated with a beta-blocker for symptom control — not with carbimazole or radioactive iodine, because the pathology is thyroid destruction releasing preformed hormone, not overproduction. The hypothyroid phase is treated with levothyroxine lifelong. Thyroid events usually do not require stopping the checkpoint inhibitor. [1]
Hypophysitis
Hypophysitis (pituitary inflammation) classically affects patients on anti-CTLA-4, peaking around 9 weeks, and presents with headache, visual disturbance (bitemporal hemianopia from pituitary enlargement), fatigue, and hyponatraemia from secondary adrenal insufficiency [4]. The pituitary panel shows low morning cortisol, low ACTH, low FSH/LH, low TSH with low free T4, low testosterone or oestradiol, and sometimes raised prolactin. MRI pituitary shows an enlarged, homogeneously enhancing gland.
The emergency is adrenal crisis. If the patient is hypotensive, hyponatraemic or unwell, give IV hydrocortisone 100 mg stat then 50 mg every 6 hours immediately — do not wait for the MRI or the cortisol result, because untreated adrenal insufficiency is fatal. Once stable, add physiological hydrocortisone (15 to 20 mg in the morning, 5 to 10 mg in the afternoon) and plan a slow taper if pituitary function recovers — though most patients need lifelong hydrocortisone, levothyroxine, and sex-steroid replacement. Steroid itself (the hydrocortisone) treats the inflammation, so high-dose glucocorticoids for hypophysitis are reserved for severe headache, visual loss, or an acutely enlarging gland. [1]
DCE trap: Hypophysitis often presents as the adrenal crisis the examiner wants you to recognise. The hyponatraemic, hypotensive patient on ipilimumab needs hydrocortisone before the MRI — thyroid replacement alone, without cortisol, can precipitate adrenal crisis. [1]
Type 1 diabetes
Fulminant type 1 diabetes is a recognised irAE that can present as diabetic ketoacidosis with new insulin dependence, sometimes within weeks of the first dose. There is no prodrome and no gradual phase — the beta cells are destroyed rapidly. The management is DKA protocol (IV fluids, insulin infusion, potassium replacement) followed by lifelong insulin. Check HbA1c (often near-normal, confirming acuity) and C-peptide (low, confirming insulin dependence). The checkpoint inhibitor may be resumed once glucose is controlled [5].
Primary adrenal insufficiency
Less common than secondary (hypophysitis) adrenal insufficiency, primary adrenal insufficiency presents with hyperpigmentation, hyperkalaemia, hyponatraemia, postural hypotension, and a high ACTH with a low cortisol. It is treated identically with hydrocortisone and fludrocortisone (the mineralocorticoid is needed because the adrenal, not the pituitary, is the target) and patient education on sick-day rules and an emergency intramuscular hydrocortisone injection kit. [1]
Renal toxicity — exclude other causes first
Immune-mediated nephritis is typically an acute kidney injury with an interstitial pattern on urinalysis (mild proteinuria, leucocytes, sometimes eosinophiluria), developing weeks to months into therapy. The single most important step is to exclude other causes — pre-renal AKI from dehydration or sepsis, obstruction (ultrasound), nephrotoxic drugs (NSAIDs, PPIs, contrast, antibiotics), and tumour lysis. A renal biopsy is reserved for persistent or steroid-refractory disease [5].
Grade 1 (creatinine under 1.5 x baseline) — continue, monitor, treat other causes. Grade 2 (1.5 to 3 x) — hold, oral prednisolone 0.5 to 1 mg/kg. Grade 3 to 4 (over 3 x or dialysis) — permanent stop, IV methylprednisolone 1 to 2 mg/kg, and mycophenolate for refractory disease (infliximab is avoided in renal failure). Most cases resolve with steroid and drug hold; renal recovery is the rule if recognised early. [1]
Cardiac toxicity — myocarditis is the one you must not miss
Checkpoint-inhibitor myocarditis is rare (around 1 per cent in the largest registry) but is the irAE with the highest case fatality — Mahmood and colleagues reported deaths in 25 to 50 per cent of severe cases, often within days of onset, and frequently coexisting with myositis (raised creatine kinase) and myasthenia gravis (ptosis, diplopia, fatigability) [7]. It typically presents in the first 3 months, with a median onset of around 30 days.
The rule: any cardiac symptom, any unexplained tachycardia, or any dyspnoea without a clear alternative in a patient on a checkpoint inhibitor warrants a troponin and an ECG. Additional investigations are echocardiogram (reduced ejection fraction, wall-motion abnormality), cardiac MRI (late gadolinium enhancement, oedema), and a creatine kinase to screen for myositis [7].
Management is permanent discontinuation of the checkpoint inhibitor at any grade of myocarditis, IV methylprednisolone 500 mg to 1 g daily (pulse dosing) in addition to standard heart-failure and arrhythmia management, early cardiology and intensive-care involvement, and mycophenolate or antithymocyte globulin for fulminant disease. Plasmapheresis is considered in severe cases with myasthenia overlap. The dose is higher than for other irAEs because undertreated myocarditis is fatal [7][8].
DWE trap: The MCQ stem is "patient on pembrolizumab, three weeks in, with chest pain and troponin 2 ng/mL." The answer is checkpoint-inhibitor myocarditis; the management is permanent discontinuation, pulse methylprednisolone, cardiology admission. Do not anchor on acute coronary syndrome — the angiogram will be normal. [1]
Neurological toxicity — broad, severe, and often missed
Neurological irAEs are uncommon but severe and have a high mortality in the meta-analysis of fatal events [8]. The spectrum includes myasthenia gravis (new ptosis, diplopia, fatigability, respiratory involvement), Guillain-Barre syndrome (ascending weakness, areflexia, respiratory failure), immune encephalitis (confusion, seizures, focal deficit), aseptic meningitis, transverse myelitis (sensory level, sphincter disturbance), and peripheral neuropathy.
Investigations are MRI brain and/or spine, lumbar puncture (cells, protein, oligoclonal bands, exclusion of infection), EMG and nerve conduction studies, and acetylcholine-receptor antibodies for myasthenia. Management is permanent discontinuation of the drug, IV methylprednisolone 1 to 2 mg/kg (pulse for severe disease), IVIG or plasmapheresis for myasthenia, GBS and severe encephalitis, and early neurology involvement. Respiratory function (forced vital capacity) must be monitored in any patient with neuromuscular weakness because respiratory failure can develop rapidly. [1]
The fatal toxicities — know them by heart
Wang and colleagues systematically reviewed fatal irAEs across 7,936 patients and identified the leading causes of death as myocarditis, pneumonitis, hepatitis, colitis (with perforation), and neurological events (especially myasthenia and GBS) [8]. The combination ipilimumab plus nivolumab carried the highest fatality rate. The practical lesson is that every severe irAE in these organs warrants early senior review, early high-dose steroid, and a low threshold for permanent discontinuation and ICU admission.
Second-line immunosuppression — beyond steroids
When a grade 3 to 4 irAE has not improved after 48 to 72 hours of adequate-dose IV steroid, the diagnosis is steroid-refractory disease and a second-line immunosuppressant is added [5][10]. The choice depends on the organ.
| Organ irAE | First second-line agent | Alternative | Comment |
|---|---|---|---|
| Colitis | Infliximab 5 mg/kg at 0, 2, 6 weeks | Vedolizumab; tofacitinib | Screen TB and hepatitis B; avoid in active infection |
| Pneumonitis | Infliximab, mycophenolate, IVIG | Rituximab | Pulse methylprednisolone first |
| Nephritis | Mycophenolate | Tacrolimus | Avoid infliximab in renal failure |
| Myocarditis | Mycophenolate, antithymocyte globulin | Plasmapheresis | Pulse methylprednisolone first |
| Neurological | IVIG, plasmapheresis | Rituximab | Myasthenia and GBS protocols |
A long-standing fear has been that immunosuppression blunts the antitumour effect. Schadendorf and colleagues provided reassuring data: in a pooled analysis of patients who discontinued nivolumab plus ipilimumab because of toxicity, the antitumour response and survival were at least as good as in patients who continued therapy [9]. The principle is to treat the toxicity decisively and not under-dose steroids out of oncological anxiety.
Restarting versus permanent discontinuation
The decision to re-challenge after recovery is one of the most common long-case discussion points. The general rules [5][4]:
- Re-challenge is reasonable for grade 1 to 2 events that have resolved to grade 1 or less, especially isolated skin events and endocrine events managed with replacement (these do not require drug discontinuation at all).
- Re-challenge is contraindicated for grade 3 to 4 events in vital organs — pneumonitis, myocarditis, hepatitis, nephritis, severe colitis, and any neurological event — where permanent discontinuation is the rule.
- Combination therapy lowers the threshold for permanent discontinuation; switching to monotherapy (e.g., from ipilimumab-nivolumab to nivolumab alone) is a reasonable strategy for lower-grade events.
- The decision is always multidisciplinary (oncologist, the relevant organ specialist, the patient) and documented, weighing the risk of recurrence against the oncological alternatives. [1]
Baseline workup and surveillance
Before starting a checkpoint inhibitor, establish:
- Full blood count, liver and renal function, electrolytes.
- Thyroid function and morning cortisol (the endocrine baseline that makes later interpretation possible).
- Fasting glucose and HbA1c.
- Troponin and ECG in patients at cardiac risk (baseline troponin is increasingly recommended).
- Hepatitis B and C, HIV, and tuberculosis screening if infliximab is a likely future need.
- Baseline CT for tumour response and later comparison.
- A patient-held irAE alert card and education on reporting any new symptom. [1]
During therapy, the minimum surveillance is regular (every cycle) clinical review with targeted bloods (FBC, LFTs, creatinine, TSH and cortisol periodically, glucose, and troponin if symptomatic). Most endocrine and hepatic events are detected on monitoring before they are symptomatic [5].
Long case — the multisystem irAE patient
A 64-year-old man on cycle 4 of ipilimumab-nivolumab for metastatic melanoma presents with a three-week history of progressive diarrhoea (now 8 stools per day with blood and mucus), a diffuse itchy rash, fatigue, and dark urine. He is tachycardic, hypotensive on standing, has abdominal tenderness, a maculopapular rash over the trunk, and jaundice. Bloods show sodium 128, potassium 5.1, creatinine 140, ALT 240, ALP 180, bilirubin 60, INR 1.4, TSH 18 (high), free T4 6 (low), morning cortisol 80 (low), ACTH low. [1]
Opening statement (SASPOP): "This 64-year-old retired engineer (Occupation) presents with multisystem toxicity (Presentation) three weeks into cycle 4 of combination ipilimumab-nivolumab (Symptoms) for metastatic melanoma, manifesting as grade 3 colitis, grade 2 hepatitis, hypophysitis with secondary adrenal insufficiency and hypothyroidism, and a grade 2 maculopapular rash." [1]
Prioritised problem list:
- Grade 3 colitis — the index emergency; perforation risk.
- Secondary adrenal insufficiency from hypophysitis — adrenal crisis with hyponatraemia and postural drop; the immediate life threat.
- Grade 2 hepatitis — exclude viral and obstructive causes.
- Hypothyroidism — treat, but only after cortisol replacement.
- Grade 2 rash — manageable alongside the above.
- Metastatic melanoma — oncological decision on therapy continuation. [1]
Integrated management plan:
- Adrenal crisis first — IV hydrocortisone 100 mg stat then 50 mg every 6 hours, IV fluids, correct sodium slowly; do not give levothyroxine until hydrocortisone is running. [1]2. Colitis — stool studies (including C. difficile) before steroids; IV methylprednisolone 1 to 2 mg/kg once infection is addressed; surgical review; abdominal CT; infliximab at 48 to 72 hours if refractory.
- Hepatitis — viral and autoimmune serology, abdominal ultrasound; hold the checkpoint inhibitors; IV steroid (already given for colitis) covers hepatitis; mycophenolate if refractory.
- Rash — topical steroid and antihistamine; escalate to systemic if it worsens (already covered).
- Permanent discontinuation of combination therapy after this multisystem grade 3 event; discuss single-agent continuation with oncology if the melanoma responds.
- Patient education, GP communication, steroid taper plan, thromboprophylaxis. [1]
Short case — examining the immunotherapy patient
Examination routine:
- General inspection — rash distribution, Cushingoid features (if on steroids), alopecia, vitiligo, hydration, dyspnoea.
- Vital signs including oxygen saturation and postural blood pressure — postural drop signals adrenal insufficiency or dehydration.
- Skin — morphology (maculopapular, bullous, pruritic), body surface area, mucous membranes (exclude SJS/TEN), nails and scalp.
- Abdomen — tenderness, distension, peritonism, bowel sounds (colitis and its complications).
- Respiratory — fine crackles (pneumonitis); exclude heart failure.
- Cardiovascular — new murmur, rub, raised JVP, signs of heart failure (myocarditis).
- Neurological — ptosis and fatigability (myasthenia), reflexes (GBS, myelitis), sensorium (encephalitis).
- Endocrine screen — thyroid, adrenal stigmata, visual fields (hypophysitis). [1]
Presentation template: "I examined Mr X, a 64-year-old man on combination checkpoint inhibition for melanoma. The positive findings are a confluent maculopapular rash over 25 per cent of his body surface area with no mucosal involvement, abdominal tenderness with increased bowel sounds, a postural drop of 20 mmHg, and bitemporal visual field restriction on confrontation. The cardinal finding is the combination of colitis, hypophysitis and rash in a patient on ipilimumab-nivolumab, consistent with multisystem immune-related toxicity. My integrated diagnosis is grade 3 immunotherapy toxicity with colitis, hypophysitis and grade 2 skin involvement. I would admit, exclude infection, start hydrocortisone for adrenal insufficiency and IV methylprednisolone for the colitis, hold the checkpoint inhibitors, and involve gastroenterology, endocrinology and oncology." [1]
Exam traps and high-yield discriminators
- "Any new symptom is an irAE until proven otherwise" AND "exclude infection before steroids." The two halves of the rule must travel together; an examinee who forgets the second half gives steroids for C. difficile colitis.
- Myocarditis has the highest case fatality. Troponin and ECG for any cardiac symptom or unexplained tachycardia; permanent discontinuation and pulse methylprednisolone.
- Hypophysitis presents as adrenal crisis. Give hydrocortisone empirically before the MRI; thyroid replacement alone precipitates adrenal crisis.
- Infliximab for colitis, mycophenolate for hepatitis and nephritis, IVIG or plasmapheresis for neurological irAEs. Never infliximab for hepatitis (it is hepatotoxic).
- Endocrine events are managed with replacement and the drug is often continued. This is the exception to the grade-based stop rule.
- Combination therapy is the most toxic. Grade 3 to 4 irAEs in over half of patients; lowest threshold for permanent discontinuation.
- Discontinuation for toxicity does not lose antitumour benefit. The Schadendorf data — treat the toxicity decisively.
- Steroid taper must be slow (4 to 6 weeks minimum). Pneumonitis and colitis relapse easily if tapered too fast. [1]
Guideline anchoring — regional and global
- ANZ (primary): eviQ and Cancer Council Australia endorse the CTCAE-based framework; infliximab is funded for refractory irAE colitis and vedolizumab is increasingly used; broad PBS access to pembrolizumab and nivolumab has made irAE management a core general-physician competency.
- US (secondary): ASCO (Brahmer et al, 2018) and NCCN provide the most cited grade-based algorithms [5]; SITC consensus (Puzanov et al) gives detailed organ-specific terminology and tables.
- Europe (secondary): ESMO (Haanen et al, 2017, updated 2022) [4] is broadly congruent with ASCO, with greater emphasis on early multidisciplinary specialist input and vedolizumab as an infliximab alternative.
- Global: the three guidelines agree on the core algorithm — grade the toxicity, exclude infection, steroids by grade, second-line immunosuppression for refractory disease, permanent discontinuation for grade 3 to 4 events in vital organs. There are no material regional deltas in the dose or the drug of choice.
References
Hodi FS, O'Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010;363:711-723 (20525992); Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 2012;366:2443-2454 (22658127); Brahmer JR, Tykodi SS, Chow LQ, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 2012;366:2455-2465 (22658128); Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines. Ann Oncol 2017;28(suppl 4):iv119-iv142 (28881921); Brahmer JR, Lacchetti C, Thompson JA, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO Clinical Practice Guideline. J Clin Oncol 2018;36:1714-1768 (29442540); Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med 2018;378:158-168 (29320654); Mahmood SS, Fradley MG, Cohen JV, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol 2018;71:1755-1764 (29567210); Wang DY, Salem JE, Wilson JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol 2018;4:1721-1728 (30242316); Schadendorf D, Wolchok JD, Hodi FS, et al. Efficacy and safety outcomes in patients with advanced melanoma who discontinued treatment with nivolumab and ipilimumab because of adverse events: a pooled analysis. J Clin Oncol 2017;35:3807-3814 (28841387); Bergqvist V, Hertervig E, Gedeon P, et al. Vedolizumab treatment for immune checkpoint inhibitor-induced enterocolitis. J Crohns Colitis 2017;11:722-723 (28204866); Hansen E, Kossai M, Le Cesne A, et al. Systematic review of immune-related adverse event reporting in clinical trials of immune checkpoint inhibitors. Ann Oncol 2015;26:1522 (25888611). [1]
References
- [1]Hodi FS, O'Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma N Engl J Med, 2010.PMID 20525992
- [2]Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer N Engl J Med, 2012.PMID 22658127
- [3]Brahmer JR, Tykodi SS, Chow LQ, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer N Engl J Med, 2012.PMID 22658128
- [4]Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol, 2017.PMID 28881921
- [5]Brahmer JR, Lacchetti C, Thompson JA, et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline J Clin Oncol, 2018.PMID 29442540
- [6]Postow MA, Sidlow R, Hellmann MD Immune-Related Adverse Events Associated with Immune Checkpoint Blockade N Engl J Med, 2018.PMID 29320654
- [7]Mahmood SS, Fradley MG, Cohen JV, et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors J Am Coll Cardiol, 2018.PMID 29567210
- [8]Wang DY, Salem JE, Wilson JV, et al. Fatal Toxic Effects Associated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis JAMA Oncol, 2018.PMID 30242316
- [9]Schadendorf D, Wolchok JD, Hodi FS, et al. Efficacy and Safety Outcomes in Patients With Advanced Melanoma Who Discontinued Treatment With Nivolumab and Ipilimumab Because of Adverse Events: A Pooled Analysis of Randomized Phase II and III Trials J Clin Oncol, 2017.PMID 28841387
- [10]Bergqvist V, Hertervig E, Gedeon P, et al. Vedolizumab treatment for immune checkpoint inhibitor-induced enterocolitis Cancer Immunol Immunother, 2017.PMID 28204866
- [11]Hansen E, Kossai M, Le Cesne A, et al. A systematic review of immune-related adverse event reporting in clinical trials of immune checkpoint inhibitors Ann Oncol, 2015.PMID 25888611