Phys · oncological
Oncologic Emergencies
Also known as oncologic emergency · oncological emergency · cancer emergency · neutropenic sepsis · febrile neutropenia · tumour lysis syndrome · malignant spinal cord compression · superior vena cava syndrome · hypercalcaemia of malignancy · hyperviscosity syndrome
Consultant-physician-depth guide to the oncologic emergencies for FRACP DWE and DCE — febrile neutropenia (the one-hour door-to-antibiotic rule, MASCC risk stratification, empiric piperacillin-tazobactam), tumour lysis syndrome (Cairo-Bishop criteria, rasburicase for high risk), malignant spinal cord compression (dexamethasone 16 mg, MRI whole spine, the Patchell surgery decision), superior vena cava obstruction (stent for severe, treat the cancer), hypercalcaemia of malignancy (PTHrP-mediated, fluids then zoledronic acid then denosumab), hyperviscosity syndrome (urgent plasmapheresis), SIADH from small cell lung cancer, neoplastic cardiac tamponade, and leukostasis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Oncologic Emergencies
The answer first
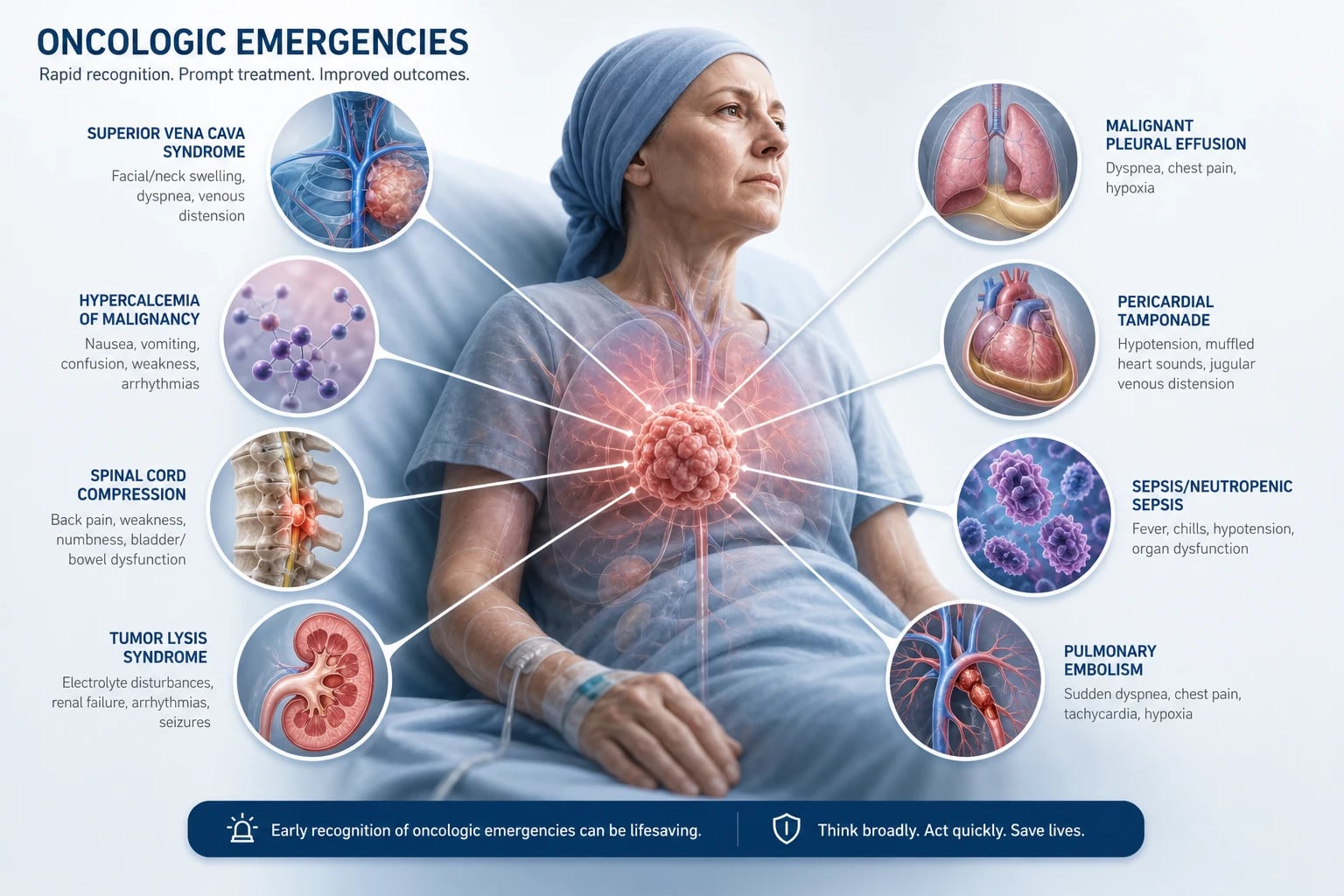
An oncologic emergency is any acute, potentially reversible event in a cancer patient that threatens life or a critical function and for which timely intervention changes the outcome. The unifying rule is door-to-treatment time: the first dose of antibiotic in febrile neutropenia within one hour, the dexamethasone dose the moment cord compression is suspected, the plasmapheresis session for hyperviscosity, the pericardiocentesis for tamponade. These are not conditions to "review on the ward round" — they are conditions to act on now. [1]
Ten emergencies dominate the examinable and the clinical landscape. In approximate order of frequency and urgency for a general physician: [1]
- Febrile neutropenia — empiric piperacillin-tazobactam within one hour, risk-stratify with the MASCC score [2][1].
- Tumour lysis syndrome — the Cairo-Bishop criteria; rasburicase for high risk, allopurinol for low risk [3][4].
- Malignant spinal cord compression — dexamethasone 16 mg, MRI whole spine, surgery or radiotherapy [5][6][7].
- Superior vena cava obstruction — stent for severe, treat the underlying cancer [10].
- Hypercalcaemia of malignancy — fluids, then zoledronic acid, then denosumab if refractory [8][9].
- Hyperviscosity syndrome — urgent plasmapheresis.
- SIADH from small cell lung cancer — fluid restriction.
- Neoplastic cardiac tamponade — emergency pericardiocentesis.
- Leukostasis — leukapheresis and hydroxyurea for urgent cytoreduction.
- Immune-related adverse events from checkpoint inhibitors — corticosteroids and drug cessation.
The clinical skill is recognition. A febrile patient on chemotherapy is neutropenic until proven otherwise. New back pain with a neurological sign in a cancer patient is cord compression until proven otherwise. A confused cancer patient is hypercalcaemic until proven otherwise. Treat the immediately life-threatening problem first, then treat the underlying cancer as the unifying solution. [1]
The classification table — all ten emergencies at a glance
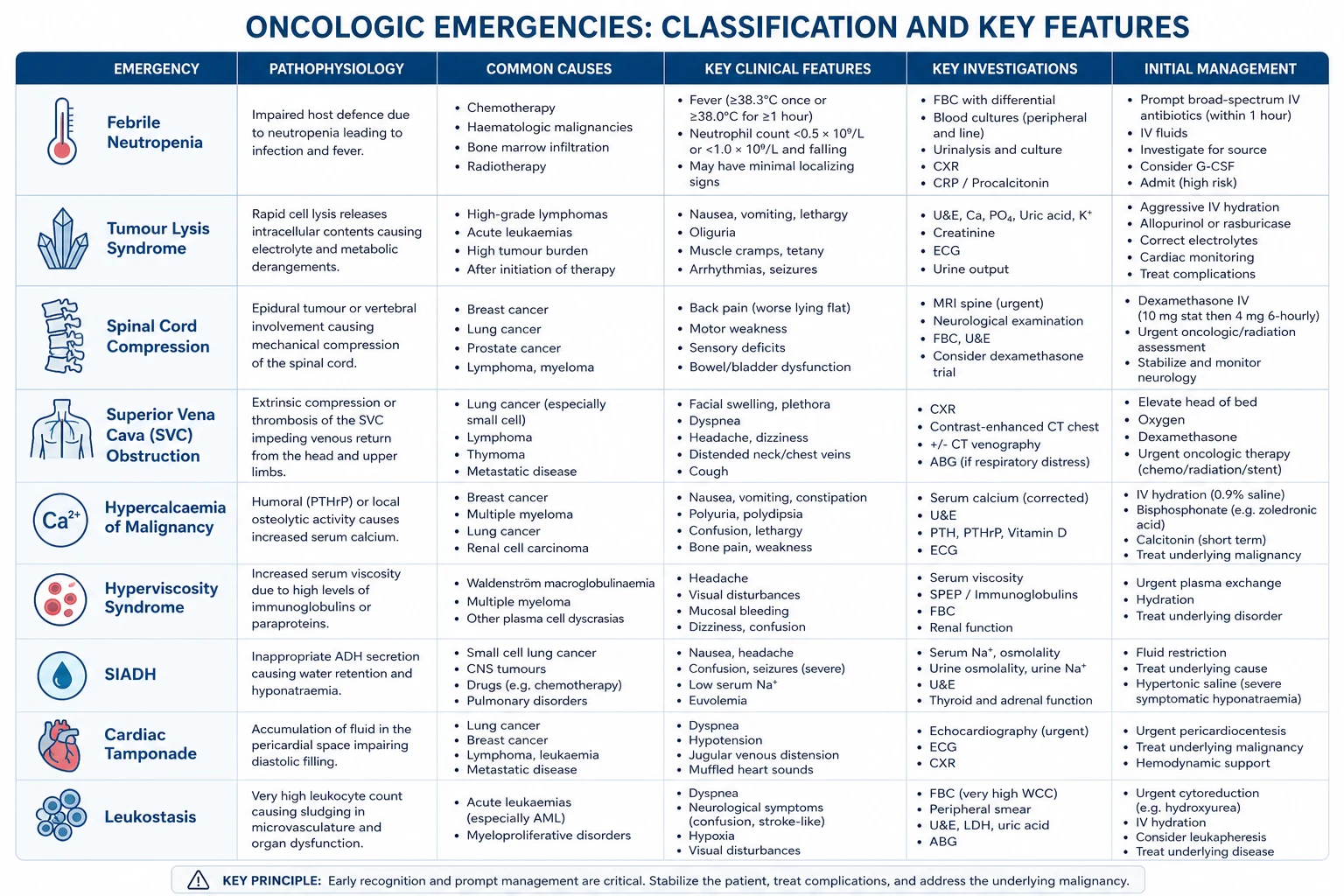
| Emergency | Presenting syndrome | Key investigation | First-line emergency treatment |
|---|---|---|---|
| Febrile neutropenia | Fever (above 38.3 single or 38.0 sustained for 1 hour) in a patient on chemotherapy | Neutrophil count, blood cultures | Empiric piperacillin-tazobactam within 1 hour |
| Tumour lysis syndrome | Hyperkalaemia, hyperphosphataemia, hyperuricaemia, hypocalcaemia, AKI after cytotoxic therapy | Urate, potassium, phosphate, calcium, creatinine (6-hourly) | Aggressive hydration, rasburicase for high risk |
| Superior vena cava obstruction | Facial and upper limb swelling, distended neck and chest veins | Contrast CT thorax | Endovascular stent if severe; treat the cancer |
| Hypercalcaemia of malignancy | Confusion, constipation, polyuria, lethargy | Corrected calcium, PTH, phosphate | IV normal saline, then zoledronic acid |
| Hyperviscosity syndrome | Visual disturbance, headache, mucosal bleeding | Serum viscosity, paraprotein level | Urgent plasmapheresis |
| SIADH (small cell lung cancer) | Euvolaemic hyponatraemia, confusion, seizure | Serum and urine osmolality and sodium | Fluid restriction; hypertonic saline if severe |
| Neoplastic cardiac tamponade | Hypotension, raised JVP, muffled heart sounds, pulsus paradoxus | Bedside echocardiography | Emergency pericardiocentesis |
| Leukostasis | Dyspnoea, confusion, visual disturbance with WCC above 100 | Blood count, blood film | Leukapheresis and hydroxyurea |
| Immune-related adverse event | Autoimmune-like toxicity weeks to months after a checkpoint inhibitor | Organ-specific inflammatory markers | Hold the drug, corticosteroids, other immunosuppression |
DWE high-yield: The table above is the single most examinable page on this topic. A stem that names the syndrome almost always asks for the first intervention — and the answer is almost always a single drug, procedure or time threshold, not a diagnostic workup. Antibiotics in one hour, dexamethasone before the MRI, plasmapheresis for hyperviscosity, pericardiocentesis for tamponade. [1]
1. Febrile neutropenia
Definition and the one-hour rule
Febrile neutropenia (also called neutropenic sepsis) is defined as a single oral temperature above 38.3 degrees, or a sustained temperature above 38.0 degrees for one hour, in a patient with a neutrophil count below 0.5 x 10^9 per litre (or expected to nadir below 0.5) [1]. The definition is deliberately sensitive: cancer patients on cytotoxic chemotherapy have breached mucosal barriers, indwelling central lines and absent neutrophils, so a fever is bacteraemia until proven otherwise, and a delay of even a few hours converts a treatable infection into septic shock.
The single most important quality metric in oncologic supportive care is the door-to-antibiotic time of one hour. The IDSA 2011 guideline states that empiric broad-spectrum antibiotic therapy must be started immediately, after cultures but without waiting for their results [1]. Retrospective data and quality-improvement studies have consistently shown that delays beyond an hour are associated with higher mortality, particularly in patients with haematological malignancy and profound neutropenia. This is the answer to "what is the first thing you do?" in any febrile neutropenia stem.
Pathophysiology — why the neutropenic patient is defenceless
Cytotoxic chemotherapy damages the rapidly dividing cells of the gastrointestinal tract mucosa, creating microscopic breaches through which enteric bacteria (Gram-negative rods, streptococci, enterococci) translocate. The indwelling central venous catheter is a nidus for skin organisms (coagulase-negative staphylococci, Staphylococcus aureus, and increasingly Gram-negatives in the biofilm). The neutrophil — the primary defence against bacteria and fungi — is absent. The patient therefore cannot mount a localising inflammatory response: there may be no pus, no infiltrate on the chest radiograph, and no peritoneal signs even in the presence of typhlitis (neutropenic enterocolitis) or a perianal abscess. Fever may be the only sign. [1]
The microbiology has shifted over decades. Gram-positive organisms (coagulase-negative staphylococci from lines, viridans streptococci from mucositis) now predominate in many series, but Gram-negative bacteraemia (Pseudomonas aeruginosa, Escherichia coli, Klebsiella) carries the highest mortality and drives the empiric antibiotic choice. The emergence of extended-spectrum beta-lactamase producers and carbapenem-resistant organisms is a growing threat that mandates adherence to local antibiograms. [1]
Empiric antibiotic therapy
The IDSA-recommended empiric therapy is an antipseudomonal beta-lactam given as monotherapy [1]:
- Piperacillin-tazobactam 4.5 g intravenously every eight hours (the most common first choice in ANZ and UK practice).
- Ceftazidime 2 g intravenously every eight hours (an alternative, narrower-spectrum option).
- Meropenem 1 g intravenously every eight hours (for patients already on broad-spectrum prophylaxis, known colonisation with a resistant organism, or severe sepsis). [1]
Add vancomycin (or another agent active against resistant Gram-positive organisms) when there is: a suspected catheter-line infection (erythema, tenderness, purulence at the exit site or along the tunnel); haemodynamic instability; severe mucositis (a risk of viridans streptococcal bacteraemia); known colonisation with MRSA; or a positive blood culture with a Gram-positive organism before identification and sensitivities. Vancomycin is not routine in the stable, well-appearing febrile neutropenic patient. [1]
Do not delay the first antibiotic dose for imaging, a microbiology review, or a senior review. The sequence is: recognise the fever, check the neutrophil count, take two sets of blood cultures (including one from each lumen of the central line and one peripheral), urine and any relevant swabs, and give the antibiotic within the hour. Cultures are taken first so that they are not contaminated by the antibiotic, but the antibiotic is given immediately afterwards. [1]
Risk stratification — the MASCC score
The MASCC (Multinational Association of Supportive Care in Cancer) risk index is a validated scoring system that identifies febrile neutropenic patients at low risk of serious complications, who may be candidates for oral antibiotics or early discharge [2]. The score allocates points for seven clinical factors:
| Clinical factor | Points |
|---|---|
| Burden of illness — none or mild symptoms | 5 |
| Burden of illness — moderate symptoms | 3 |
| No hypotension (systolic blood pressure at least 90 mmHg) | 5 |
| No chronic obstructive pulmonary disease | 4 |
| Solid tumour, or haematological malignancy with no previous fungal infection | 4 |
| Outpatient at onset of fever | 3 |
| No dehydration requiring parenteral fluids | 3 |
| Age below 60 years | 2 |
A score of at least 21 identifies a patient as low risk. A score below 21 is high risk. The maximum score is 26. [1]
The MASCC score is a decision-support tool, not a rule. Several factors override a "low-risk" classification and mandate inpatient intravenous therapy regardless of the score: anticipated prolonged neutropenia (more than 7 days), profound neutropenia (ANC below 0.1), mucositis, an uncontrolled or progressive cancer, a documented infection at presentation, liver or renal dysfunction, or any haemodynamic instability. The ASCO-IDSA 2018 update further refined the low-risk criteria and endorsed oral ciprofloxacin plus amoxicillin-clavulanate as an option for carefully selected low-risk inpatients, with close follow-up [1].
DWE discriminator: The MASCC score is the only validated risk-stratification tool in febrile neutropenia that an examiner will expect you to name. The cut-point is 21. A stable, well-appearing outpatient with a solid tumour and a MASCC score of 24 is low-risk and may be considered for oral therapy or early discharge; a patient with acute leukaemia, expected prolonged neutropenia, mucositis or hypotension is high-risk regardless of the score and must receive inpatient intravenous therapy. [1]
Workup of the febrile neutropenic patient
The minimum dataset, all obtainable within the first hour: [1]
- Two sets of blood cultures — one from each lumen of the central line and one peripheral (or, if no line, two peripheral sets from separate sites). Paired line and peripheral cultures help distinguish line infection (line culture positive much earlier) from bacteraemia.
- Urine microscopy and culture — the urinary tract is a common source, though pyuria may be absent in the neutropenic patient.
- Chest imaging — a chest radiograph as a minimum; a CT chest if there are respiratory symptoms or persistent fever, to look for pulmonary nodules, consolidations or the halo sign of invasive pulmonary aspergillosis.
- Swabs and cultures of any obvious source — perianal examination (but avoid digital rectal examination in neutropenia, as it may precipitate bacteraemia from a perianal lesion), line exit site, skin lesions, mouth and throat.
- Blood tests — full blood count, urea and electrolytes, liver function, lactate, C-reactive protein, and a group and screen. [1]
Persistent fever beyond 4 to 7 days raises the concern of an invasive fungal infection (aspergillosis, candidiasis). The workup then includes a CT chest (looking for the halo and reverse-halo signs), serum galactomannan and beta-D-glucan assays, and consultation with infectious diseases and microbiology about empiric or targeted antifungal therapy (liposomal amphotericin B, caspofungin, voriconazole). [1]
Duration of therapy and step-down
Antibiotics are continued until the patient is afebrile for at least 48 hours and the neutrophil count is recovering (above 0.5), the patient is clinically well, and any documented infection has been treated. For the patient who defervesces quickly with an unidentifying source, a typical course is 7 to 14 days. For documented bacteraemia, the duration follows the organism and the syndrome (e.g. 14 days for staphylococcal bacteraemia, longer for endocarditis). Step-down to an oral agent is appropriate for the low-risk patient who has defervesced and is clinically well. Granulocyte colony-stimulating factor (G-CSF) is not routine — it is reserved for patients with severe or prolonged neutropenia, a documented infection that is not responding, or as secondary prophylaxis after a life-threatening episode of febrile neutropenia in a subsequent cycle. [1]
Exam trap: The most common DWE error is delaying antibiotics while waiting for the neutrophil count, the cultures, or a senior review. The one-hour door-to-antibiotic time is the answer to "what is the first thing you do?" in any febrile neutropenia stem — cultures first, antibiotic immediately afterwards, do not wait. [1]
2. Tumour lysis syndrome
Definition and the Cairo-Bishop criteria
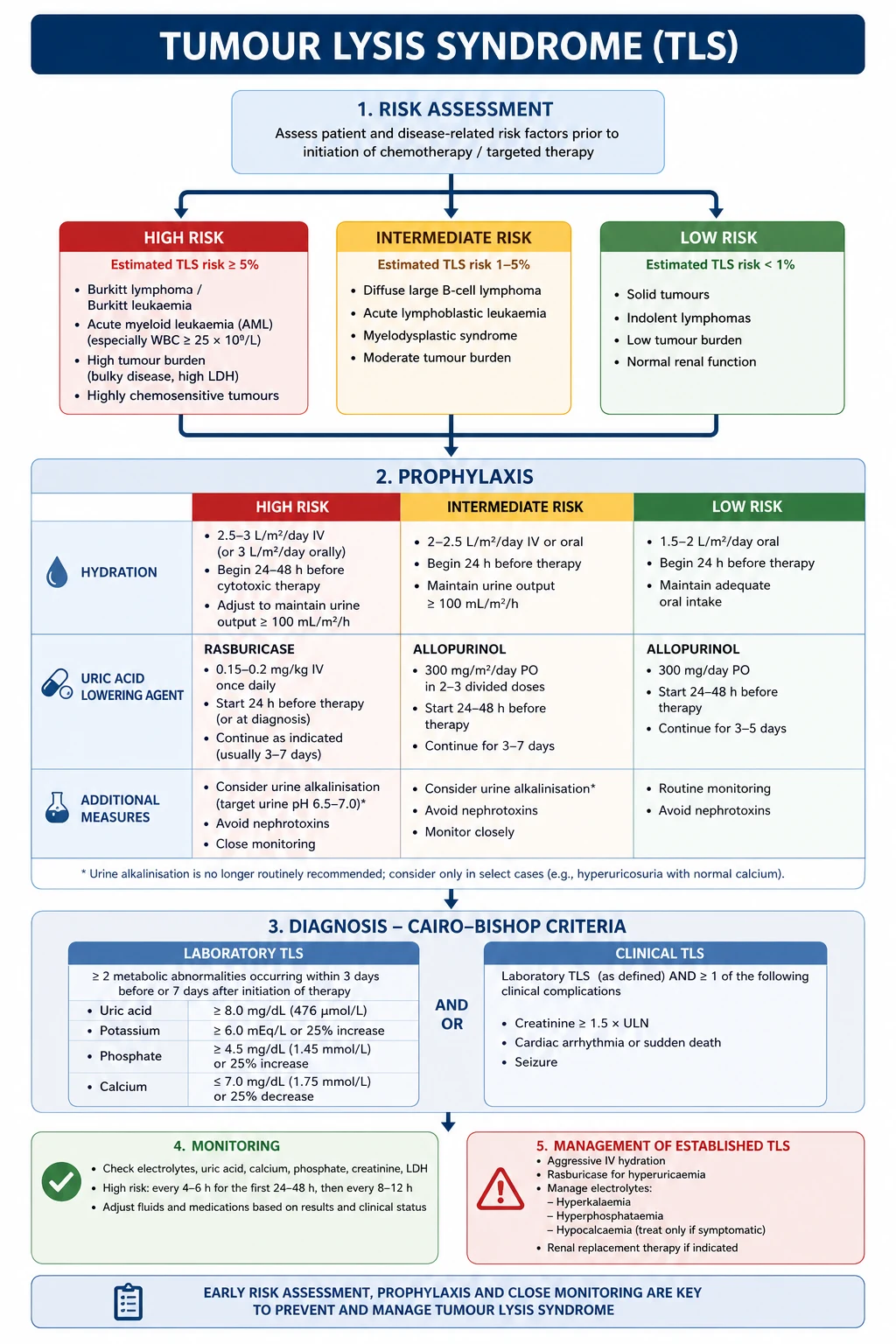
Tumour lysis syndrome (TLS) is a metabolic emergency caused by the rapid release of intracellular contents when tumour cells are lysed by cytotoxic therapy. The Cairo-Bishop classification (2004) is the standard definition and distinguishes laboratory TLS from clinical TLS [3].
Laboratory TLS requires two or more of the following abnormalities, occurring within 3 days before to 7 days after the initiation of cytotoxic therapy: [1]
- Uric acid at or above 476 micromol per litre (8 mg per dL) or a 25 per cent rise from baseline.
- Potassium at or above 6.0 mmol per litre or a 25 per cent rise from baseline.
- Phosphate at or above 1.45 mmol per litre (4.5 mg per dL) in adults or a 25 per cent rise from baseline.
- Calcium at or below 1.75 mmol per litre (7.0 mg per dL) or a 25 per cent fall from baseline. [1]
Clinical TLS is laboratory TLS plus one or more of: acute kidney injury (creatinine at or above 1.5 times the upper limit of normal), cardiac arrhythmia, seizure, or death [3].
Pathophysiology — why the cells dying causes the kidney to fail
When tumour cells lyse, three intracellular products flood the extracellular fluid: [1]
- Potassium — released from every lysed cell, raising the serum potassium within hours and threatening the cardiac rhythm.
- Nucleic acids — DNA and RNA are catabolised through purines to hypoxanthine, then to xanthine, then to uric acid (catalysed by xanthine oxidase). Uric acid is poorly soluble at acidic urine pH, and crystallises in the renal tubules, causing obstruction and tubular injury.
- Phosphate — released in large quantities from tumour cells (which have a high phosphate content). Phosphate complexes with calcium, producing a calcium phosphate precipitate that deposits in the renal tubules (worsening the AKI) and lowering the serum calcium (the hypocalcaemia of TLS). [1]
The kidney is therefore hit twice: by uric acid crystals and by calcium phosphate deposition. Add the volume depletion that often accompanies the acutely ill cancer patient, and the result is an acute kidney injury that can progress to oligoanuria and dialysis-dependence. [1]
High-risk tumours and treatments
TLS is most likely when a large, sensitive tumour is treated with an effective cytotoxic agent. The classical high-risk settings: [1]
- Burkitt lymphoma and lymphoblastic lymphoma with a high tumour burden (high LDH, bulky disease).
- Acute lymphoblastic leukaemia with a high white cell count (above 100) or a high tumour burden.
- Acute myeloid leukaemia with a high white cell count (above 50 to 100) or monocytic subtype.
- High-grade non-Hodgkin lymphoma with bulky disease or a high LDH.
- High tumour burden of any kind — large masses, extensive marrow involvement, organomegaly, elevated LDH, elevated uric acid or creatinine at baseline.
- Highly proliferative tumours and highly cytotoxic regimens — the more effective the lysis, the higher the risk. [1]
Solid tumours (small cell lung cancer, germ cell tumours, breast cancer) can cause TLS but are lower risk. Spontaneous TLS (before any therapy) occurs in high-burden lymphoproliferative disease and in paediatric tumours. [1]
Prevention — hydration, allopurinol and rasburicase
The principles of prevention apply to every high-risk patient beginning cytotoxic therapy: [1]
- Aggressive intravenous hydration — the cornerstone. Give isotonic saline at 3 litres per square metre per day (approximately 100 mL per hour in a typical adult), aiming for a urine output above 100 mL per hour. Hydration expands the intravascular volume, dilutes the released solutes, and maintains tubular flow to prevent crystal deposition. Alkalinisation of the urine (with sodium bicarbonate) is no longer recommended routinely, because it increases calcium phosphate deposition and is not clearly beneficial.
- Allopurinol — a xanthine oxidase inhibitor that prevents the formation of new uric acid from the lysed nucleic acids. It is prophylaxis for low-to-intermediate-risk patients. It does not lower uric acid that has already formed, and so is insufficient for established hyperuricaemia or for the highest-risk patients. The oral dose is 300 mg daily (dose-reduced for renal impairment). Rash and interstitial nephritis are the main adverse effects.
- Rasburicase — a recombinant urate oxidase that directly converts existing uric acid to the soluble allantoin, which is then excreted. It lowers the serum uric acid within hours, is effective in established TLS, and is the agent of choice for high-risk patients and for any patient who already has laboratory TLS with hyperuricaemia [4]. The standard dose is 0.2 mg per kg intravenously daily for up to 5 days (a single dose is often sufficient and single-dose strategies are widely used). Rasburicase is contraindicated in G6PD deficiency because the hydrogen peroxide generated during uric acid breakdown causes haemolysis and methaemoglobinaemia; screen G6PD before giving it in at-risk populations (African, Mediterranean, South-East Asian ancestry).
DWE discriminator: The single most common exam error is treating established TLS with allopurinol. Allopurinol only prevents new uric acid formation; it does not lower the uric acid that has already formed. For established TLS, or for high-risk prophylaxis, the answer is rasburicase. The GRAAL1 trial established rasburicase as rapidly and reliably urate-lowering in adult lymphoma [4].
Monitoring and treatment of established TLS
In the high-risk window (the first 3 to 7 days of cytotoxic therapy), monitor: [1]
- Electrolytes and creatinine every 6 hours — potassium, phosphate, calcium, urate, urea and creatinine.
- Cardiac monitoring for the hyperkalaemic ECG changes (peaked T waves, widened QRS) that precede arrhythmia.
- Fluid balance — aim for a urine output above 100 mL per hour; if oliguria develops despite hydration, the patient is heading for dialysis. [1]
Treat the specific abnormalities: [1]
- Hyperkalaemia — calcium gluconate for membrane stabilisation if there are ECG changes; insulin and dextrose to shift potassium intracellularly; and renal replacement therapy for refractory or severe hyperkalaemia.
- Hypocalcaemia — do not correct the calcium unless the patient is symptomatic (tetany, carpopedal spasm, Chvostek or Trousseau sign, seizure, arrhythmia). Correcting calcium in the presence of hyperphosphataemia worsens calcium phosphate deposition and renal injury. Treat the hyperphosphataemia and the underlying TLS, and the calcium will rise.
- Acute kidney injury — renal replacement therapy for refractory hyperkalaemia, severe acidosis, or volume overload. Haemodialysis removes uric acid and phosphate effectively; continuous renal replacement therapy is preferred in the haemodynamically unstable patient. [1]
3. Malignant spinal cord compression
The time-critical neurological emergency
Malignant spinal cord compression (MSCC) is compression of the spinal cord or cauda equina by an epidural metastasis, producing neurological deficit that becomes irreversible if not decompressed promptly. It affects 5 to 10 per cent of cancer patients and is one of the most feared complications because the difference between walking and paraplegia is measured in hours. [1]
The tumour reaches the epidural space by haematogenous spread to the vertebral body (the most common route, from breast, lung, prostate, kidney and myeloma) or by direct extension from a paravertebral mass (as in lymphoma). Once in the epidural space, the tumour compresses the cord and, critically, its venous plexus, producing venous congestion, vasogenic oedema, ischaemia and finally infarction. The neurological deficit is reversible while the pathology is oedema and ischaemia; it becomes permanent once infarction occurs. This is why dexamethasone (which reduces oedema) and decompression (which relieves the mechanical and vascular compromise) are time-critical. [1]
Presentation — the pain that comes first
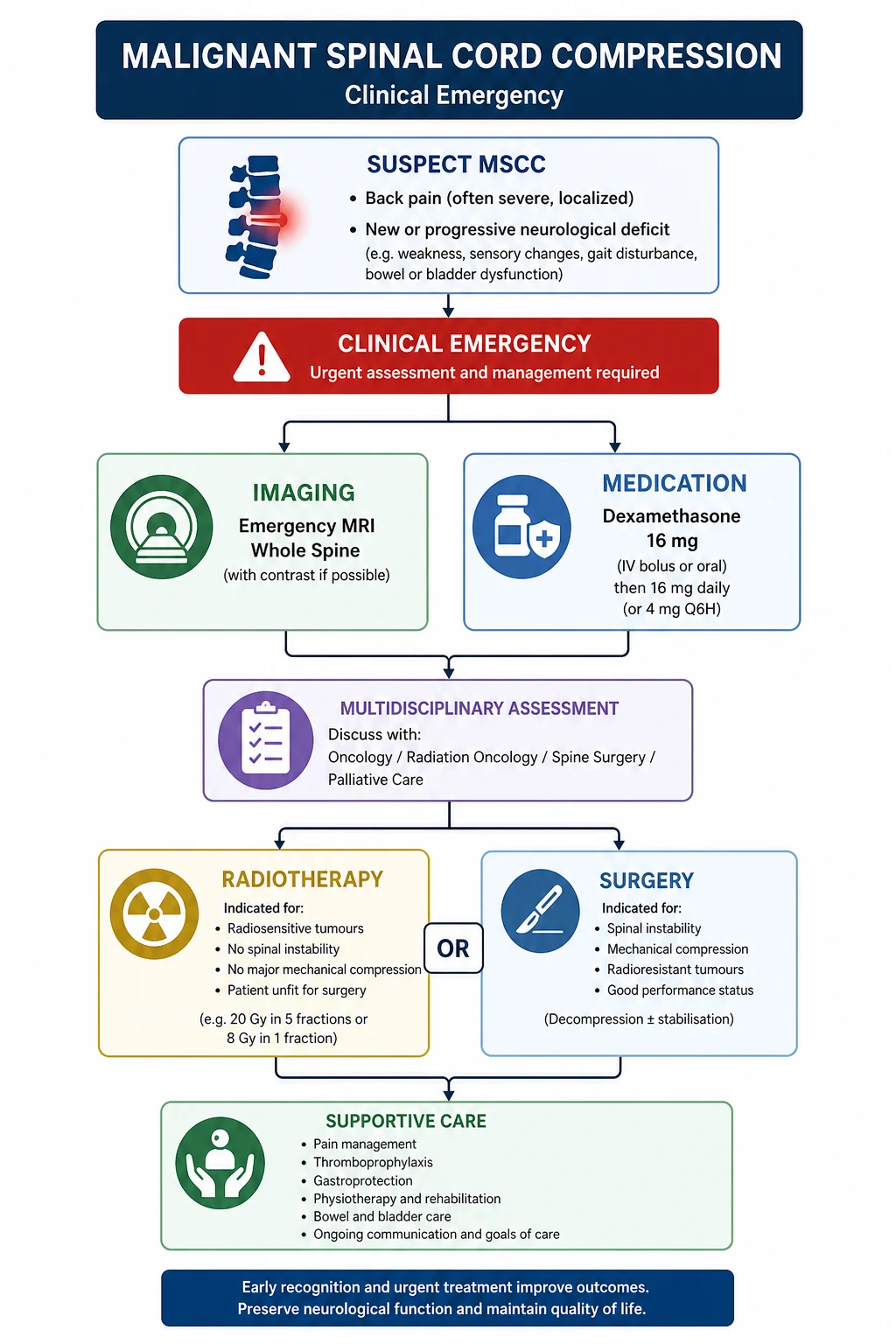
The cardinal sequence is back pain, followed by neurological deficit: [1]
- Back pain is the first symptom in over 95 per cent of patients and may precede the neurological deficit by days to weeks. The pain is typically progressive, worse at night, unrelated to activity, and may be radicular (a band-like or dermatomal distribution). Night pain and pain unrelated to posture are the discriminating features from mechanical back pain.
- Neurological deficit then develops — weakness (first the legs, then the arms if the lesion is cervical), a sensory level, sphincter disturbance (urinary retention, constipation, faecal incontinence), and, in advanced cases, a complete cord syndrome. [1]
The neurological status at presentation is the single strongest predictor of the ambulatory outcome. Patients who are ambulatory at presentation almost always remain ambulatory with prompt treatment. Patients who are non-ambulatory at presentation have a much lower chance of regaining the ability to walk, and those with complete paraplegia for more than 24 to 48 hours rarely recover. This is the basis of the urgency. [1]
Emergency management — steroid, scan, decompress
The moment MSCC is suspected: [1]
- Dexamethasone 16 mg intravenously immediately. This reduces vasogenic oedema around the cord and is the first intervention; it relieves pain and may improve the neurological deficit within hours. The dose is then continued as 16 mg daily in divided doses (for example 8 mg twice daily) and tapered during radiotherapy. Higher loading doses (up to 96 mg) have been used but increase steroid complications without clear additional benefit [5][7].
- Urgent MRI of the whole spine. Not the symptomatic level alone — multiple levels of disease are common, and the symptomatic level may be a vertebral compression fracture while the cord is compressed at an adjacent or distant level. Plain films, bone scans and CT myelography have been superseded; MRI is the modality of choice. CT is used only if MRI is contraindicated (a non-MRI-compatible pacemaker, severe claustrophobia).
- Urgent clinical oncology and neurosurgical review. The two treatment modalities are radiotherapy and direct decompressive surgery plus radiotherapy.
Surgery versus radiotherapy — the Patchell trial
The Patchell 2005 randomised trial transformed the surgical management of MSCC [6]. It randomised 101 patients with a single area of cord compression (and a life expectancy of at least 3 months) to either direct decompressive surgery followed by radiotherapy or radiotherapy alone. The trial was stopped early after an interim analysis because the surgery group was dramatically superior:
- 84 per cent of the surgery group were ambulatory after treatment, versus 57 per cent of the radiotherapy group.
- Patients who underwent surgery retained the ability to walk for a median of 122 days, versus 13 days in the radiotherapy group.
- Among patients who were non-ambulatory at presentation, 62 per cent of the surgery group regained the ability to walk, versus 19 per cent of the radiotherapy group.
- Surgery patients also retained continence and quality of life for longer. [1]
The patients who benefit from surgery are those with: a single compressive level (Patchell's key inclusion criterion); spinal instability or bone retropulsion into the canal; neurological deterioration despite steroids or radiotherapy; an unknown primary tumour needing tissue; or a radio-resistant tumour (sarcoma, melanoma, renal cell). Patients with multiple levels of compression, a very poor prognosis (life expectancy under 3 months), or complete paraplegia for over 24 to 48 hours are generally managed with radiotherapy and supportive care. The Loblaw systematic review and 2011 update underpin the guideline framework [5][7].
DWE discriminator: The answer to "best management of MSCC in a patient with a single compressive level and spinal instability" is direct decompressive surgery plus radiotherapy, based on the Patchell trial [6]. The answer to "best management of MSCC in a patient with multiple compressive levels and a poor performance status" is dexamethasone and palliative radiotherapy. The discriminator is the number of levels and the fitness for surgery.
Supportive care and complications
- Urinary catheterisation for retention and to monitor output.
- Pressure area care and DVT prophylaxis (the immobile cancer patient is at high risk of both).
- Bowel regimen for constipation (opioids and the neurological deficit both contribute).
- Pain control with analgesia appropriate to the severity (opioids are often needed; consider a pain service and neuropathic agents for radicular pain).
- Dexamethasone adverse effects — hyperglycaemia, immunosuppression, psychosis, gastritis; monitor and manage.
- Radiotherapy adverse effects — transient worsening of oedema (continue the steroid), radiation myelopathy (rare, late), skin reaction. [1]
4. Superior vena cava obstruction
The syndrome of upper-body venous hypertension
Superior vena cava (SVC) obstruction is obstruction of the SVC by external compression (most often a right-sided lung tumour, mediastinal lymphoma, or a metastatic mediastinal node) or by intraluminal thrombosis (often around an indwelling central venous catheter). The obstruction raises the venous pressure in the upper body, producing the characteristic clinical syndrome. [1]
The patient describes facial fullness and swelling, worse on bending forward or lying flat, arm swelling, dyspnoea, and sometimes cough and hoarseness (from recurrent laryngeal nerve involvement by the underlying tumour). The examination shows facial and periorbital oedema, distended neck veins that do not collapse with inspiration, collateral veins over the chest and abdomen (engorged superficial epigastric veins draining the upper body into the systemic circulation below the obstruction), and upper limb oedema. Severe obstruction produces stridor (laryngeal oedema), syncope (reduced cerebral venous return), visual disturbance and headache (cerebral venous congestion), and, at the extreme, upper airway obstruction — a true emergency. [1]
Investigation and the role of tissue diagnosis
- Contrast-enhanced CT of the thorax is the key investigation — it shows the level and length of the obstruction, the cause (a mass, thrombosis, nodal disease), and the collateral circulation.
- Tissue biopsy is essential before definitive treatment, because the management is dictated by the histology. A small cell lung cancer responds to chemotherapy; a non-small cell lung cancer is treated with chemo-radiotherapy; a lymphoma is treated with disease-specific chemotherapy; a thrombosis around a catheter is treated with anticoagulation and line removal. Biopsy may be by bronchoscopy (for an endobronchial lesion), mediastinoscopy (for a mediastinal mass), CT-guided biopsy (for a peripheral lesion), or biopsy of an accessible lymph node.
- Doppler ultrasound of the upper limb and neck veins may identify associated thrombosis. [1]
The Rowell and Gleeson systematic review established that the evidence base for the treatment of SVC obstruction is dominated by small series and that the priorities are to obtain a tissue diagnosis and to treat the underlying cancer [10].
Treatment — stent for severe, treat the cancer
The treatment of SVC obstruction depends on the severity and the underlying cause: [1]
- Endovascular stenting is the treatment of choice for severe or life-threatening obstruction (stridor, cerebral symptoms, haemodynamic compromise, or severe symptoms not tolerating the workup). It provides rapid relief within 24 to 48 hours and does not preclude subsequent oncologic treatment. Anticoagulation is usually given after stenting.
- Treat the underlying cancer is the definitive treatment for the stable patient. Small cell lung cancer and lymphoma are chemosensitive and respond within days to weeks; non-small cell lung cancer is treated with chemo-radiotherapy. Symptom relief from cancer-directed therapy takes longer than stenting, so stenting is preferred when rapid relief is needed.
- Corticosteroids (dexamethasone) may provide temporary relief in lymphoma and in inflammatory obstruction, but are not a substitute for definitive treatment.
- Anticoagulation is indicated when thrombosis is present (catheter-related, or a hypercoagulable state from the cancer). [1]
Exam trap: The most common SVC error is treating it as an emergency in every patient. Most SVC obstruction is subacute; the priority is a tissue diagnosis and treatment of the underlying cancer. Stenting is reserved for severe or life-threatening obstruction (stridor, cerebral symptoms). Treat the cancer; do not assume every patient needs a stent. [1]
5. Hypercalcaemia of malignancy
The metabolic emergency of the cancer patient
Hypercalcaemia is the most common metabolic emergency in cancer, affecting up to 30 per cent of patients at some point in their course. It presents with the non-specific symptoms that are easily attributed to the cancer or to depression: confusion and cognitive change, lethargy, constipation, nausea, polyuria and polydipsia (a nephrogenic diabetes insipidus-like state from renal concentrating defect), and, in severe cases, coma and arrhythmia. The ECG shows a shortened QT interval. The diagnosis is easily missed in the confused cancer patient — a corrected calcium is part of the workup of any acutely confused cancer patient. [1]
Two mechanisms — PTHrP and lytic bone disease
Hypercalcaemia of malignancy arises by two principal mechanisms: [1]
- Humoral hypercalcaemia of malignancy (PTHrP-mediated) — the most common mechanism (about 80 per cent of cases). The tumour secretes parathyroid hormone-related peptide (PTHrP), which binds the PTH receptor and behaves biochemically like primary hyperparathyroidism: a high calcium, a low phosphate, increased renal calcium reabsorption, and increased bone resorption. Classically seen in squamous cell carcinomas (lung, head and neck, oesophagus, cervix), renal cell carcinoma, bladder cancer, and ovarian cancer. The intact PTH is appropriately suppressed (distinguishing it from primary hyperparathyroidism).
- Local osteolytic hypercalcaemia — the tumour directly activates osteoclasts in the bone via RANKL, releasing calcium from the lytic lesions. Classically seen in multiple myeloma and breast cancer with extensive bone metastases. The phosphate is normal or high (no phosphaturic PTH-like effect), and the PTHrP is normal. [1]
Ectopic PTH secretion by a tumour is vanishingly rare and is mentioned only to be excluded. [1]
Emergency management — fluids, bisphosphonate, calcitonin
The treatment of hypercalcaemia of malignancy follows a clear sequence: [1]
- Aggressive intravenous normal saline — the first and most important intervention. Give 3 to 6 litres of normal saline over the first 24 hours, guided by the volume status and the cardiac and renal function. Saline expands the intravascular volume, promotes a natriuresis (and calcium is passively excreted with sodium in the proximal tubule), and corrects the dehydration that almost always accompanies symptomatic hypercalcaemia. Avoid thiazide diuretics (they retain calcium); a loop diuretic (frusemide) is used only for volume overload, not for routine calcium-lowering.
- A bisphosphonate — the definitive calcium-lowering agent. Zoledronic acid 4 mg intravenously over 15 minutes is the standard first-line agent, established as superior to pamidronate by the Major pooled analysis [8]. It takes 48 to 72 hours to lower the calcium, with a nadir at about 5 to 7 days and a duration of about 4 weeks. The dose is reduced in renal impairment (the creatinine clearance threshold varies by region; consult the local protocol). The main adverse effects are an acute phase reaction (fever, myalgia, bone pain) in the first 48 hours, nephrotoxicity (dose-related, and the reason for the slow infusion and the renal dose reduction), and osteonecrosis of the jaw (a rare but serious late complication — a dental check before starting is standard).
- Calcitonin 4 to 8 IU per kg subcutaneously every 12 hours — provides a rapid but transient calcium-lowering effect (within hours) by inhibiting osteoclast activity and increasing renal calcium excretion. Its effect is lost after 48 to 72 hours (tachyphylaxis), so it is used as a bridge while waiting for the bisphosphonate to work, in the severely symptomatic patient or the patient with a very high calcium. It is not a substitute for the bisphosphonate.
- Denosumab 120 mg subcutaneously — a monoclonal antibody against RANK ligand, used for bisphosphonate-refractory hypercalcaemia or in renal failure (where bisphosphonates are problematic). The Hu trial established its efficacy in bisphosphonate-refractory disease [9]. Because it is not renally cleared, it is safe in renal impairment; the main adverse effect is hypocalcaemia (more frequent than with bisphosphonates), so calcium and vitamin D supplementation is mandatory.
- Glucocorticoids (prednisolone 40 to 60 mg daily) are useful in specific settings — vitamin D-mediated hypercalcaemia (lymphoma, granulomatous disease) and myeloma — but are not first-line for the typical PTHrP-mediated case.
DWE discriminator: The single most common hypercalcaemia error is failing to rehydrate before giving the bisphosphonate. The first intervention is always aggressive intravenous normal saline. The bisphosphonate is added after the patient is rehydrated, and calcitonin bridges the 48-hour gap in the symptomatic patient. The calcium falls over days, not minutes. [1]
6. Hyperviscosity syndrome
The IgM pentamer and the sausage-link veins
Hyperviscosity syndrome is a clinical syndrome caused by a markedly elevated serum viscosity, almost always from a high concentration of a monoclonal immunoglobulin. It is classically a feature of Waldenstrom macroglobulinaemia (the IgM-secreting lymphoplasmacytic lymphoma) because IgM is a pentamer with a very high intrinsic viscosity; it also occurs in IgM and IgA myeloma at very high paraprotein levels, and rarely in polycythaemia (from a very high red cell count) or severe leukaemia (from a very high white cell count — see leukostasis). [1]
The classic triad is visual disturbance, mucosal bleeding and neurological symptoms: [1]
- Visual disturbance — blurred vision, from retinal venous engorgement and the characteristic "sausage-link" or "boxcar" appearance of the retinal veins on fundoscopy, with retinal haemorrhages and exudates.
- Mucosal bleeding — epistaxis, gingival bleeding, gastrointestinal bleeding, from platelet dysfunction imposed by the paraprotein coating the platelets and from the increased shear stress on the fragile mucosal capillaries.
- Neurological symptoms — headache, dizziness, ataxia, vertigo, hearing loss, somnolence and seizures, from sluggish cerebral blood flow.
- Other features include fatigue, anorexia and, in severe cases, heart failure from hypervolaemia. [1]
Emergency management — plasmapheresis first, cytoreduction second
The treatment is urgent plasmapheresis (plasma exchange) to lower the paraprotein acutely. A single exchange of 1.0 to 1.5 plasma volumes lowers the paraprotein (and the viscosity) by approximately 50 per cent, with rapid symptomatic relief. The trigger for plasmapheresis is clinical (the symptomatic triad), not a viscosity number — though a serum viscosity above 4 centipoise (or a relative serum viscosity above 6) supports the decision. Daily or alternate-day exchanges are continued until the symptoms resolve and the paraprotein has fallen. [1]
The definitive treatment is cytoreduction of the underlying clonal disease: a rituximab-based regimen (rituximab with bendamustine or with dexamethasone) for Waldenstrom macroglobulinaemia, and a bortezomib-based regimen for myeloma. The cytoreduction takes weeks to lower the paraprotein, so plasmapheresis is the bridge. [1]
Exam trap: The most common hyperviscosity error is waiting for the viscosity result or the paraprotein quantification before acting. The diagnosis is clinical — the triad of visual disturbance, mucosal bleeding and neurological symptoms in a patient with a high paraprotein (especially IgM). The treatment is urgent plasmapheresis. [1]
7. Syndrome of inappropriate antidiuretic hormone (SIADH)
Small cell lung cancer and the euvolaemic hyponatraemia
SIADH is the most common cause of euvolaemic hyponatraemia in cancer, classically from small cell lung cancer (which ectopically secretes ADH) and also from pancreatic, prostate, bladder and head-and-neck cancers. In the cancer patient it is also frequently drug-induced — vincristine, cyclophosphamide, cisplatin, opioids, SSRIs, carbamazepine — and the two causes may coexist. [1]
The diagnosis requires the four classical criteria: [1]
- Hypotonic hyponatraemia (serum sodium below 135, serum osmolality below 275).
- Inappropriately concentrated urine (urine osmolality above 100, typically above 300).
- High urinary sodium (above 40, reflecting the euvolaemic state and the intact renal sodium handling).
- Euvolamia — no oedema, no dehydration, no signs of hypovolaemia or hypervolaemia; normal renal, thyroid and adrenal function (exclude hypothyroidism and adrenal insufficiency, which also cause hyponatraemia). [1]
The patient presents with the symptoms of hyponatraemia: headache, nausea, confusion, lethargy, and in severe cases (sodium below 120), seizure and coma. The rapidity of the fall matters more than the absolute value — a sodium of 125 reached over 48 hours is more dangerous than a sodium of 115 reached over months. [1]
Management — fluid restriction and the correction rate
The management depends on the severity and the symptom profile: [1]
- Fluid restriction (500 to 1000 mL below the insensible losses, typically 800 to 1000 mL per day) is the first-line treatment for the mild-to-moderate, asymptomatic or minimally symptomatic case. It is effective because the kidney, under the influence of ADH, retains free water; restricting intake limits the dilution.
- Hypertonic saline (3 per cent saline) is reserved for the severe symptomatic case (seizure, coma, sodium below 120 with symptoms). The correction must be slow — no more than 8 to 10 mmol per litre in 24 hours, and certainly not more than 18 mmol in the first 48 hours, to avoid osmotic demyelination (central pontine myelinolysis). Frequent sodium monitoring (every 2 to 4 hours during active correction) is essential.
- Vasopressin V2-receptor antagonists (vaptans, e.g. tolvaptan, demeclocycline) have a role in chronic or refractory SIADH but are not first-line for the acute case and must be used with care to avoid over-rapid correction.
- Treat the underlying cancer — the SIADH of small cell lung cancer often resolves with effective chemotherapy. [1]
DWE discriminator: The rate of correction of hyponatraemia is the most examinable point. The safe rate is no more than 8 to 10 mmol per litre in 24 hours. Over-rapid correction causes osmotic demyelination — a devastating, often irreversible brainstem injury. In a severe symptomatic patient, give 100 mL of 3 per cent saline over 10 minutes (repeated up to three times if needed for ongoing seizure), then stop and reassess. [1]
8. Neoplastic cardiac tamponade
The cancer that fills the pericardium
Neoplastic cardiac tamponade is the accumulation of a malignant pericardial effusion to a volume and rate that impairs diastolic filling, producing the clinical syndrome of obstructive shock. The common causes are lung cancer, breast cancer, lymphoma, leukaemia and melanoma — cancers that metastasise to the pericardium or the epicardium. The effusion may be haemorrhagic (from the tumour's vascular surface) or serous. [1]
The clinical picture is Beck's triad — hypotension, a raised jugular venous pressure, and muffled heart sounds — together with pulsus paradoxus (a fall in systolic blood pressure of more than 10 mmHg on inspiration), tachycardia, dyspnoea, and, in advanced cases, shock and collapse. The ECG may show low voltages and electrical alternans (a beat-to-beat variation in the QRS amplitude from the swinging heart). The diagnosis is confirmed by bedside echocardiography, which shows the effusion, the right atrial and right ventricular diastolic collapse (the echo signs of tamponade physiology), and the inspiratory collapse of the right ventricle. [1]
Emergency management — pericardiocentesis
The treatment is emergency pericardiocentesis — aspiration of the effusion, typically via a subxiphoid approach under echocardiographic guidance. The aspiration of even a small volume (50 to 100 mL) may dramatically relieve the tamponade, as the pericardium is a relatively non-compliant structure. A drain is often left in situ for 24 to 48 hours. For recurrent effusion, a pericardial window (surgical creation of a pericardio-pleural communication) or intrapericardial sclerosant therapy is performed. The definitive treatment is of the underlying cancer. [1]
Do not confuse tamponade with constrictive pericarditis (a chronic, thickened pericardium with a equalised diastolic pressures and a knock) or with a large but non-tamponading effusion (no haemodynamic compromise). The haemodynamic compromise is what makes tamponade an emergency. [1]
9. Leukostasis
Hyperleukaemia and the sludged circulation
Leukostasis (symptomatic hyperleukocytosis) is the clinical syndrome caused by a very high white cell count (typically above 100 x 10^9 per litre) that increases the blood viscosity and obstructs the microcirculation, most critically in the lungs and the brain. It is classically a complication of acute myeloid leukaemia (in which the large, sticky myeloblasts are particularly likely to cause leukostasis at counts above 50 to 100) and chronic myeloid leukaemia in blast crisis, and less commonly of the lymphoid leukaemias. [1]
The patient presents with: [1]
- Pulmonary symptoms — dyspnoea, hypoxaemia, diffuse pulmonary infiltrates (from leukocyte obstruction of the pulmonary capillaries).
- Neurological symptoms — confusion, headache, visual disturbance, focal deficits, and the catastrophic complication of intracranial haemorrhage (from leukocyte obstruction of the cerebral vessels, vessel wall damage and the coagulopathy that often accompanies acute leukaemia).
- Other features — priapism (venous obstruction), digital ischaemia, retinal vein engorgement, and acute kidney injury. [1]
Emergency management — cytoreduction before chemotherapy
The treatment is urgent cytoreduction of the white cell count: [1]
- Leukapheresis — mechanical removal of the white cells from the circulation, lowering the count within hours. It is the fastest intervention and is indicated for symptomatic leukostasis or a very high count with end-organ effects.
- Hydroxyurea — an oral cytotoxic agent that rapidly lowers the white cell count (over 24 to 48 hours), used in conjunction with leukapheresis or when leukapheresis is not available.
- Aggressive intravenous hydration — to reduce viscosity and support renal perfusion.
- Allopurinol and TLS prophylaxis — because cytoreduction of a high white count carries a high TLS risk.
- Avoid blood transfusion until the white count has fallen — transfusing packed red cells increases the viscosity and may worsen the leukostasis; if transfusion is essential (e.g. for symptomatic anaemia or a platelet count below 20 with bleeding), do so after or during leukapheresis. [1]
The definitive treatment is induction chemotherapy for the underlying leukaemia, begun once cytoreduction is underway. Do not delay cytoreduction for chemotherapy — the leukapheresis and hydroxyurea are the emergency interventions that prevent the fatal complications of leukostasis, and chemotherapy takes days to work. [1]
Exam trap: The most common leukostasis error is treating the white count with chemotherapy alone, before cytoreduction. Leukapheresis and hydroxyurea lower the count within hours and prevent the fatal intracranial haemorrhage and pulmonary failure; chemotherapy takes days. Transfuse only after cytoreduction, never before. [1]
10. Immune-related adverse events from checkpoint inhibitors
Autoimmunity on a timer
Checkpoint inhibitors — the anti-PD-1, anti-PD-L1 and anti-CTLA-4 monoclonal antibodies — release the brakes on the adaptive immune system to attack the tumour, but they also produce a spectrum of autoimmune-like toxicities that can affect any organ system. These immune-related adverse events (irAEs) arise weeks to months after the first dose (and sometimes months after the last dose) and are managed by holding the drug, corticosteroids, and, for severe cases, other immunosuppression (infliximab, mycophenolate, rituximab). The full spectrum — colitis, pneumonitis, hepatitis, dermatitis, endocrinopathy (thyroiditis, hypophysitis, type 1 diabetes, adrenal insufficiency), nephritis, myocarditis, encephalitis, myositis, uveitis — is covered in detail in the immunotherapy toxicity topic. The oncologic-emergency relevance is that an irAE can mimic any of the syndromes above (a checkpoint inhibitor pneumonitis mimics a neutropenic pneumonia; a checkpoint inhibitor colitis mimics a neutropenic enterocolitis; a checkpoint inhibitor myocarditis mimics tamponade) and the management is the opposite — immunosuppression, not antibiotics or antineoplastics. The temporal relationship to the checkpoint inhibitor and the inflammatory picture (lymphocytic infiltrate on biopsy, an elevated inflammatory marker) are the clues. [1]
Prognosis and the goals of care
The prognosis of an oncologic emergency is dominated by the underlying cancer and the patient's overall trajectory. A patient with a chemosensitive tumour (small cell lung cancer with SIADH, lymphoma with SVC obstruction, myeloma with hypercalcaemia) may have the emergency resolved by effective cancer therapy and go on to a prolonged remission. A patient with a refractory cancer and a poor performance status may have the emergency as the harbinger of the terminal phase, in which case the goal shifts from disease-modifying treatment to symptom control and a dignified death. [1]
The goals-of-care conversation is part of the emergency management. Explore what the patient understands about their prognosis, what matters most to them now, whether they would accept intensive treatment (ICU, further chemotherapy) or prefer to focus on comfort, and document the agreed plan with regular review. Involve the palliative care team early — not only for end-of-life care, but for symptom control, prognostic framing and family support throughout the illness trajectory. [1]
Exam traps and high-yield discriminators
- The one-hour door-to-antibiotic time in febrile neutropenia is the answer to "what is the first thing you do?" in any febrile chemotherapy patient. Cultures first, antibiotic immediately afterwards, do not wait.
- Rasburicase, not allopurinol, for established or high-risk TLS. Allopurinol prevents new uric acid; rasburicase converts existing uric acid to allantoin [4].
- MRI of the whole spine for suspected cord compression — not the symptomatic level alone [5].
- Direct decompressive surgery plus radiotherapy for a single-level cord compression with instability (Patchell [6]); dexamethasone and radiotherapy for multiple levels or a poor surgical candidate.
- Rehydrate first, bisphosphonate second, calcitonin as the bridge for hypercalcaemia [8].
- Urgent plasmapheresis for hyperviscosity syndrome — the trigger is clinical, not a viscosity number.
- Leukapheresis and hydroxyurea before chemotherapy for leukostasis; transfuse only after cytoreduction.
- Emergency pericardiocentesis for neoplastic tamponade — Beck's triad and a bedside echo.
- Correct hyponatraemia at no more than 8 to 10 mmol per litre in 24 hours to avoid osmotic demyelination.
- Stent the severe SVC obstruction; treat the cancer for the stable case. Do not assume every patient needs a stent [10].
Cross-links
- Acute leukaemia — the tumour lysis syndrome and leukostasis topics integrate with the acute leukaemia page.
- Multiple myeloma — the hypercalcaemia of malignancy, hyperviscosity and cast nephropathy topics integrate with the myeloma page.
- Lymphoma — the SVC obstruction and TLS topics integrate with the lymphoma page.
- Sepsis — the febrile neutropenia topic builds on the sepsis page's framework for septic shock and the Surviving Sepsis bundle.
- Electrolyte disorders (sodium and potassium) — the SIADH and the hyperkalaemia of TLS integrate with the electrolyte pages.
- Acute kidney injury — the TLS-related AKI integrates with the AKI page.
- Immunotherapy toxicity — the immune-related adverse events topic is covered in detail on the immunotherapy toxicity page. [1]
References and guidelines
IDSA 2011 febrile neutropenia guideline (Freifeld, Clin Infect Dis) [1]; MASCC risk index (Klastersky, JCO 2000) [2]; Cairo-Bishop tumour lysis classification (Cairo, Br J Haematol 2004) [3]; GRAAL1 rasburicase in adult lymphoma (Coiffier, JCO 2003) [4]; Loblaw systematic review of malignant spinal cord compression (JCO 2005) [5]; Patchell direct decompressive surgery trial (Lancet 2005) [6]; Loblaw 2011 updated systematic review (IJROBP 2012) [7]; Major zoledronic acid versus pamidronate in hypercalcaemia of malignancy (JCO 2001) [8]; Hu denosumab in bisphosphonate-refractory hypercalcaemia (JCO 2013) [9]; Rowell and Gleeson SVC obstruction systematic review (Clin Oncol 2002) [10]. NCCN supportive-care guidelines; eviQ cancer treatment protocols (Australia); NICE NG12 suspected cancer recognition and referral; Cancer Council Australia clinical guidelines.
References
- [1]Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america Clin Infect Dis, 2011.PMID 21258094
- [2]Klastersky J, Paesmans M, Rubenstein EB, et al. The Multinational Association for Supportive Care in Cancer risk index: A multinational scoring system for identifying low-risk febrile neutropenic cancer patients J Clin Oncol, 2000.PMID 10944139
- [3]Cairo MS, Bishop M Tumour lysis syndrome: new therapeutic strategies and classification Br J Haematol, 2004.PMID 15384972
- [4]Coiffier B, Mounier N, Bologna S, et al. Efficacy and safety of rasburicase (recombinant urate oxidase) for the prevention and treatment of hyperuricemia during induction chemotherapy of aggressive non-Hodgkin's lymphoma: results of the GRAAL1 (Groupe d'Etude des Lymphomes de l'Adulte Trial on Rasburicase Activity in Adult Lymphoma) study J Clin Oncol, 2003.PMID 14581437
- [5]Loblaw DA, Perry J, Chambers A, Laperriere NJ Systematic review of the diagnosis and management of malignant extradural spinal cord compression: the Cancer Care Ontario Practice Guidelines Initiative's Neuro-Oncology Disease Site Group J Clin Oncol, 2005.PMID 15774794
- [6]Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial Lancet, 2005.PMID 16112300
- [7]Loblaw DA, Mitera G, Ford M, Laperriere NJ A 2011 updated systematic review and clinical practice guideline for the management of malignant extradural spinal cord compression Int J Radiat Oncol Biol Phys, 2012.PMID 22420969
- [8]Major P, Lortholary A, Hon J, et al. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials J Clin Oncol, 2001.PMID 11208851
- [9]Hu MI, Glezerman IG, Leboulleux S, et al. Denosumab for patients with persistent or relapsed hypercalcemia of malignancy despite recent bisphosphonate treatment J Natl Cancer Inst, 2013.PMID 23990665
- [10]Rowell NP, Gleeson FV Steroids, radiotherapy, chemotherapy and stents for superior vena caval obstruction in carcinoma of the bronchus: a systematic review Clin Oncol (R Coll Radiol), 2002.PMID 12555872