Phys · oncological
Palliative Care and Symptom Management
Also known as palliative care · symptom management · end of life care · terminal care · supportive care · WHO analgesic ladder · cancer pain · anticipatory prescribing · palliative sedation · breaking bad news
Consultant-physician-depth guide to palliative care and symptom management for FRACP DWE and DCE — the WHO definition and the early-integration principle (Temel trial), the WHO three-step analgesic ladder for cancer pain (morphine, oxycodone, fentanyl; adjuvants gabapentin and dexamethasone; breakthrough at one-sixth; opioid rotation and methadone for refractory pain), cause-specific nausea and vomiting (metoclopramide for gastric stasis, haloperidol and olanzapine for chemical causes, cyclizine and hyoscine for bowel obstruction, dexamethasone for raised ICP), refractory breathlessness (oxygen if hypoxic, low-dose morphine, benzodiazepines, fan and positioning — Abernethy showed no benefit of oxygen over air in the non-hypoxaemic patient), terminal delirium and agitation (haloperidol first-line, midazolam for refractory), opioid-induced constipation (always co-prescribe a stimulant plus osmotic laxative), anorexia-cachexia (megestrol and corticosteroids with limited benefit), end-of-life care and anticipatory prescribing (the four injectable medicines), advance care planning, the SPIKES protocol for breaking bad news, and the ethics of capacity, substitute decision-making and voluntary assisted dying.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Palliative Care and Symptom Management

The answer first
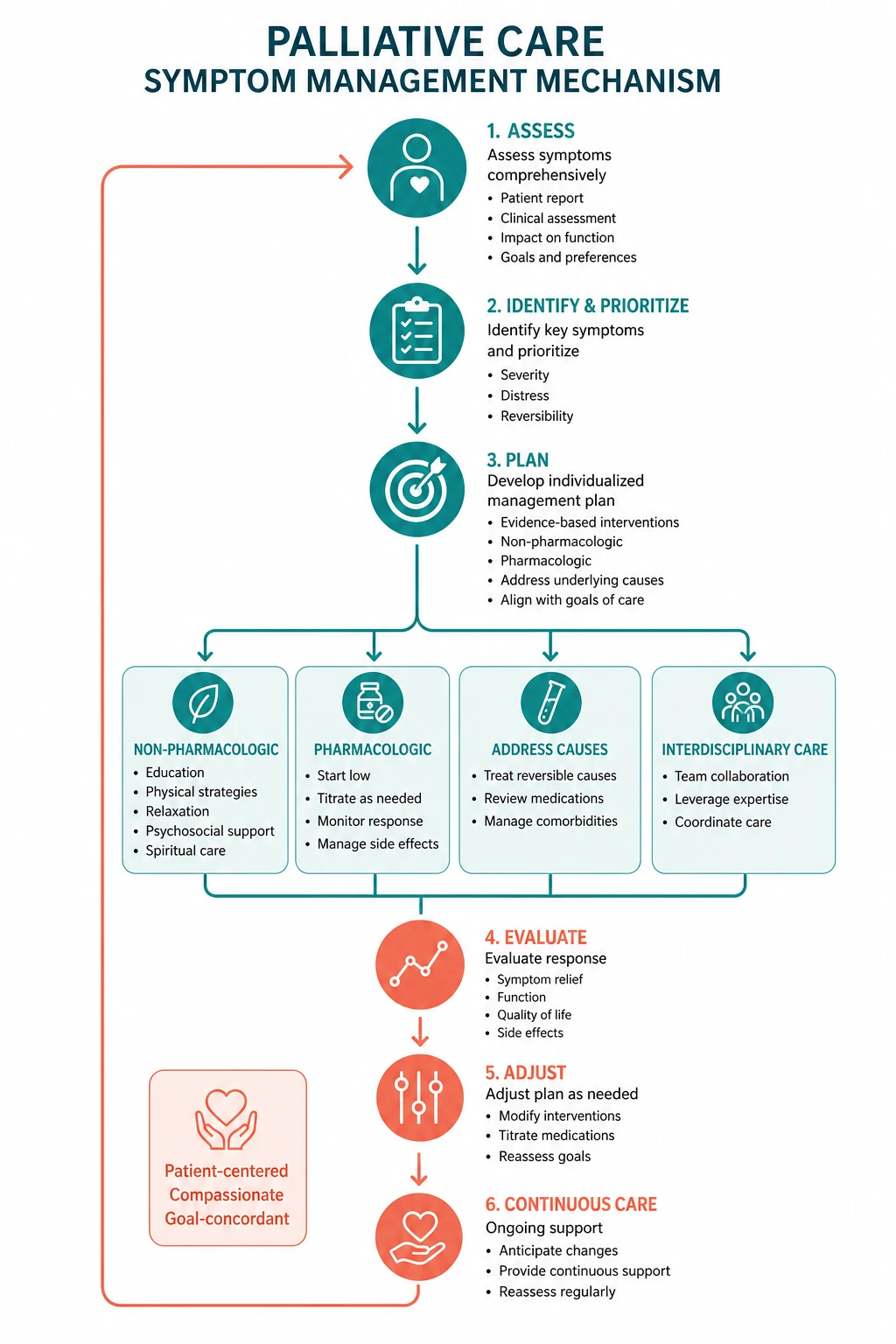
Palliative care is the active holistic care of patients of all ages with serious health-related suffering, aimed at improving the quality of life of patients, their families and their caregivers. The two ideas that define it for a physician trainee are these: palliative care is introduced early and in parallel with disease-directed therapy, not only at the end of life, and the unit of care is the patient and the family together. The Temel 2010 randomised trial — early palliative care in metastatic non-small-cell lung cancer — established that integrated palliative care alongside oncology improved quality of life and mood, reduced aggressive end-of-life care, and was associated with longer median survival (11.6 versus 8.9 months) [1]. This single trial reframes palliative care from a terminal service to an active clinical specialty that improves outcomes.
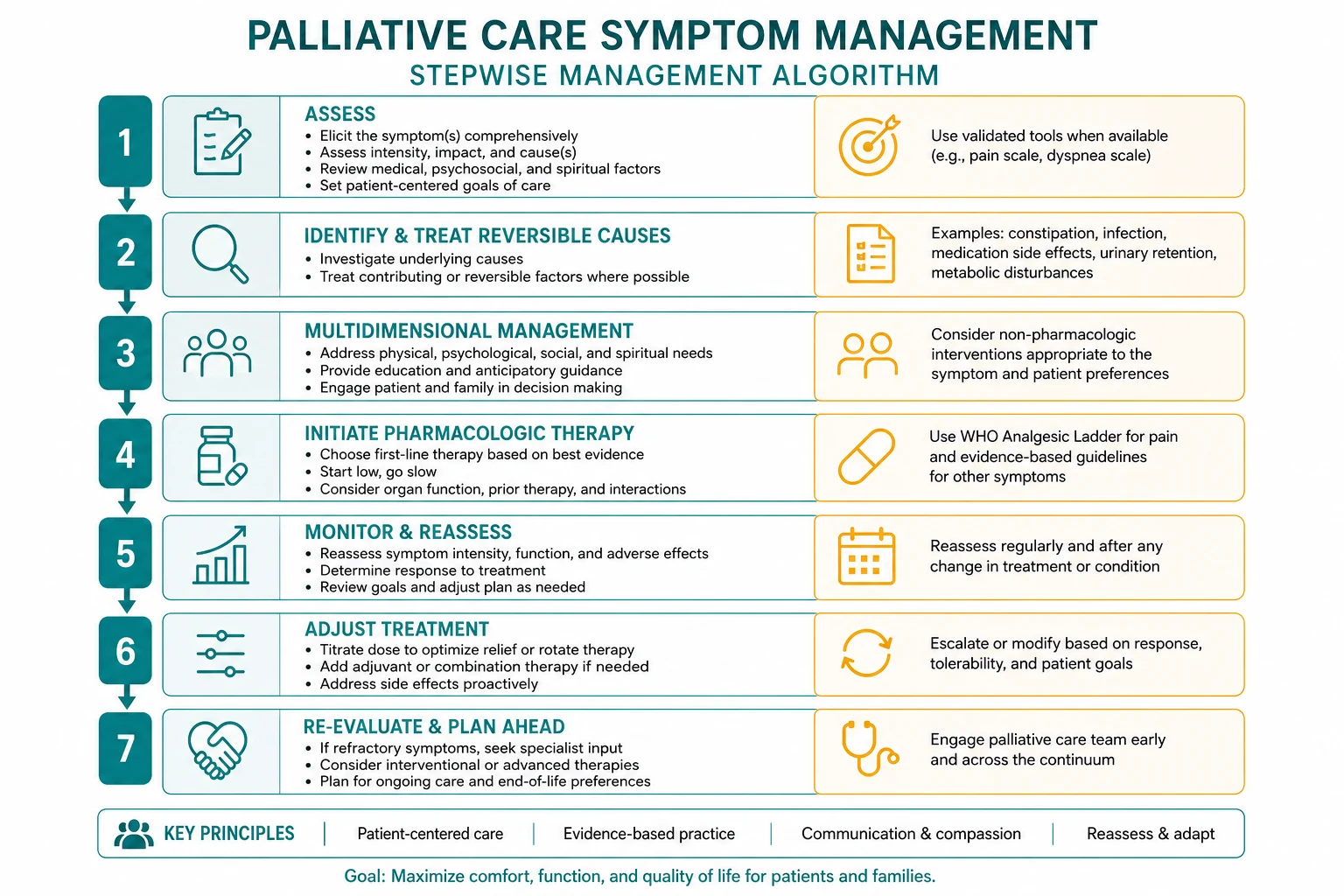
The clinical skill is symptom management by mechanism, with the WHO analgesic ladder as the framework for pain and a cause-specific pharmacological approach for every other symptom. The skill that examiners most often probe is the reasoning: why this drug, at this dose, for this mechanism of this symptom, in this patient. The unifying rule is that you treat the cause of each symptom first (drain the effusion, decompress the obstruction, treat the hypercalcaemia), and then you treat the symptom with the agent whose mechanism matches the pathophysiology. [1]

DWE high-yield: The two most examinable facts in palliative care are the WHO analgesic ladder (Step 1 non-opioid, Step 2 weak opioid, Step 3 strong opioid, adjuvants at every step) and the breakthrough opioid dose (one-sixth of the total 24-hour long-acting dose). Every cancer pain stem turns on these two facts. [1]
The symptom-management table — six symptoms at a glance

| Symptom | Mechanism / cause | First-line agent and dose |
|---|---|---|
| Cancer pain | Somatic, visceral or neuropathic nociception | WHO ladder: morphine 2.5 to 5 mg q4h titrated; breakthrough at 1/6 of total daily dose |
| Nausea — chemical | Opioids, hypercalcaemia, uraemia, drugs | Haloperidol 0.5 to 1.5 mg nocte, or olanzapine 2.5 to 5 mg |
| Nausea — bowel obstruction | Mechanical or functional obstruction | Cyclizine 50 mg tds or hyoscine butylbromide 20 mg q4 to 6h |
| Refractory breathlessness | Ventilatory drive, anxiety, parenchymal disease | Low-dose oral morphine 2.5 mg; oxygen only if hypoxaemic |
| Opioid-induced constipation | Mu-receptor effect on the gut | Stimulant (senna) + osmotic (macrogol) — always co-prescribed |
| Terminal delirium or agitation | Multi-factorial; reversible causes first | Haloperidol 0.5 to 2 mg; midazolam 2.5 to 5 mg SC if refractory |
| Terminal respiratory secretions | Pooling of saliva the dying patient cannot clear | Glycopyrronium 200 micrograms SC q4h or hyoscine butylbromide 20 mg SC |
Examiner trap: The table above is a mechanism map, not a recipe. The most common prescribing error is a one-size-fits-all antiemetic — metoclopramide worsens bowel obstruction, cyclizine worsens gastric stasis, and the antiemetic choice must follow the mechanism. [1]
1. The principles of palliative care and the early-integration model
The WHO definition and what it changes
The 2018 WHO consensus definition re-framed palliative care as the active holistic care of individuals of all ages with serious health-related suffering due to severe illness, aimed at improving the quality of life of patients, their families and their caregivers. The definition has four operational consequences for a physician: [1]
- It is active, not passive. Palliative care is not the withdrawal of care; it is the active, systematic management of suffering alongside — not instead of — disease-directed therapy.
- It applies from diagnosis. A patient newly diagnosed with metastatic cancer needs symptom control, prognostic framing, family support and advance care planning from the day of diagnosis, not only in the last weeks of life.
- The family is a unit of care. Serious illness affects the family, and the family's grief, burden and bereavement are clinical concerns.
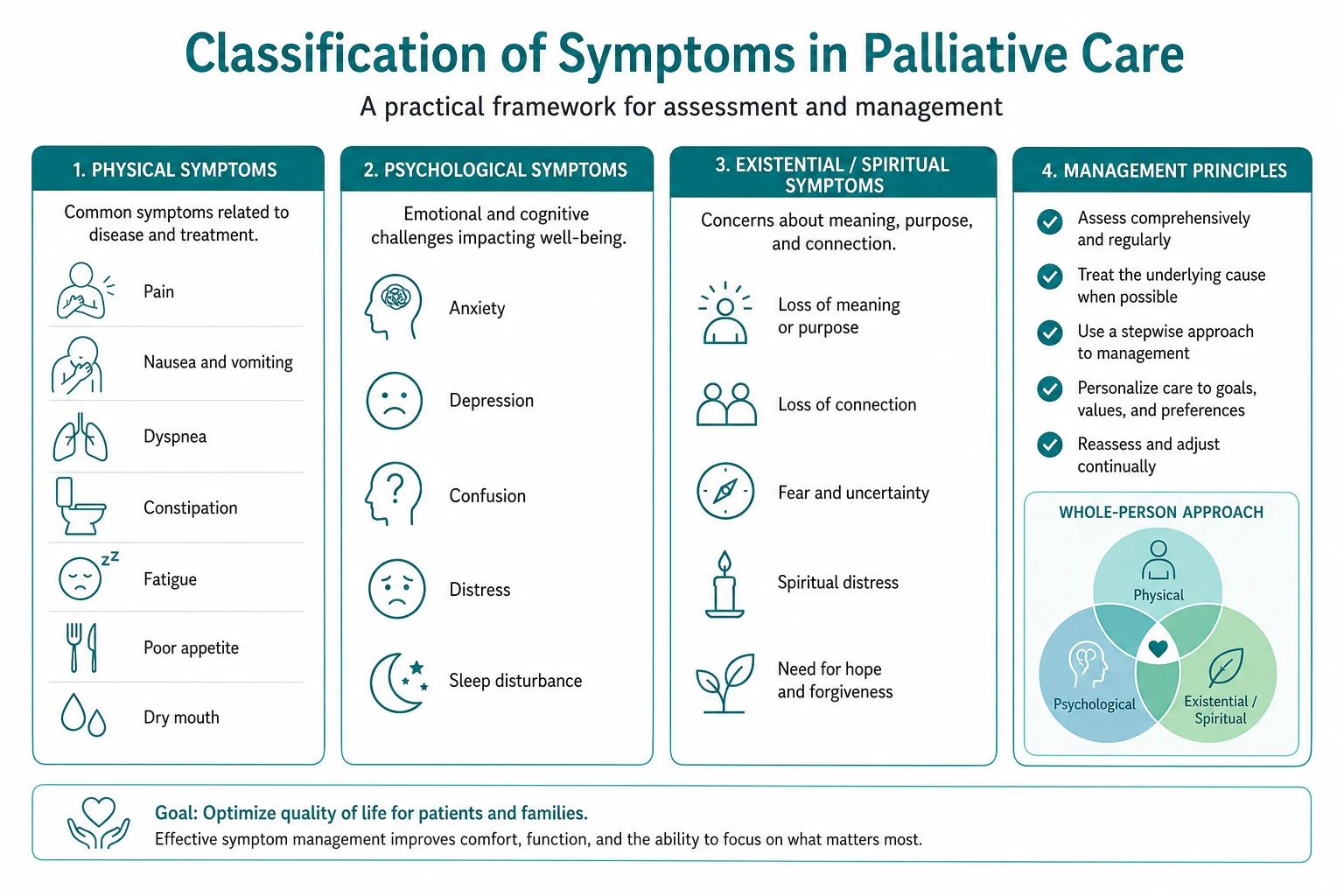
- It is holistic. Physical symptoms are addressed alongside psychological, social, spiritual and cultural needs. [1]
The shift from a terminal-care model to an early-integration model is the most important change in modern palliative medicine. The Temel 2010 trial randomised patients with newly diagnosed metastatic non-small-cell lung cancer to early palliative care integrated with standard oncology versus oncology alone [1]. The early palliative care group had better quality-of-life scores, fewer depressive symptoms, less aggressive end-of-life care (less chemotherapy in the last 14 days of life), and a longer median survival (11.6 versus 8.9 months). The survival benefit was the unexpected finding that established early palliative care as a quality marker.
DCE long-case insight: When asked "how would you manage this patient's cancer?", a registrar answer is "chemotherapy and radiotherapy". A consultant answer is "disease-directed therapy in parallel with early palliative care for symptom control, prognostic understanding, advance care planning and family support". The examiner is listening for the integration. [1]
The domains of care
The clinical practice guidelines of the National Consensus Project (NCP, US) and the European Association for Palliative Care (EAPC) structure palliative care into domains that every physician should be able to address at a primary level, escalating to specialist palliative care for complex problems: [1]
- Physical — pain, breathlessness, nausea, constipation, delirium, anorexia, fatigue, insomnia.
- Psychological — anxiety, depression, fear, demoralisation, adjustment.
- Social — finances, housing, family roles, work, caregiving.
- Spiritual — meaning, purpose, hope, dignity, religious practice.
- Cultural — language, beliefs about illness and death, family structure.
- Ethical — capacity, consent, ceilings of treatment, advance directives, substitute decision-making.
- Care of the imminently dying — recognition of the dying phase, anticipatory prescribing, family support, bereavement. [1]
In ANZ practice, Palliative Care Australia and the Australian and New Zealand Society of Palliative Medicine (ANZSPM) set the national standards, with the expectation that every physician can deliver primary palliative care and refer to a specialist service for complex symptoms, refractory pain, psychosocial complexity or end-of-life care. [1]
2. Cancer pain and the WHO analgesic ladder
The five principles of the ladder
The WHO three-step analgesic ladder, first published in 1986 and refined in the 2018 WHO cancer pain guideline, remains the single most examinable framework in palliative care. Its five operational principles are as important as the steps themselves: [1]
- By the mouth — use the oral route wherever possible; reserve parenteral routes for the patient who cannot swallow or absorb.
- By the clock — prescribe analgesics on a regular schedule (around the clock), not as needed, so that the next dose is given before the previous one wears off.
- By the ladder — escalate stepwise from non-opioid, to weak opioid, to strong opioid, adding adjuvants at any step.
- For the individual — titrate the dose to the patient's pain; there is no standard maximum dose for morphine in cancer pain, and the correct dose is the one that relieves the pain with acceptable side effects.
- With attention to detail — co-prescribe for predictable side effects (always a laxative with an opioid), review regularly, and treat breakthrough pain promptly. [1]
The three steps
- Step 1 — non-opioid for mild pain. Paracetamol 1 g four times daily (the maximum safe adult dose; reduce in frailty and liver disease) and, if not contraindicated, a non-steroidal anti-inflammatory (ibuprofen, naproxen, celecoxib) for inflammatory, bone and soft-tissue pain. Non-opioids are not stepped up; they are added at every step.
- Step 2 — weak opioid for moderate pain. Codeine 30 to 60 mg every four hours (with paracetamol, watching the daily paracetamol ceiling) or tramadol 50 to 100 mg every four to six hours. Both have a ceiling effect and are a bridge to Step 3 when pain persists. Avoid combining two weak opioids.
- Step 3 — strong opioid for severe pain, or for pain uncontrolled at Step 2. Oral morphine is the first-line strong opioid worldwide. Start at 2.5 to 5 mg every four hours, with the same dose available for breakthrough, and reassess within 24 hours. Once the 24-hour requirement is established, convert to a sustained-release preparation (twice daily) or a transdermal system, with breakthrough immediate-release morphine at one-sixth of the total daily long-acting dose available on demand. Oxycodone (10 to 20 per cent more potent than morphine milligram-for-milligram, often better tolerated) and transdermal fentanyl (for stable opioid-tolerant patients with a stable pain pattern, not for opioid-naive patients or rapid titration) are alternatives. [1]
DWE discriminator: The single most examinable number in cancer pain is the breakthrough opioid dose = one-sixth of the total 24-hour long-acting dose. A patient on 60 mg of sustained-release morphine twice daily (120 mg per 24 hours) takes 20 mg of immediate-release morphine for breakthrough pain. Recalculate the breakthrough dose every time the background dose changes. [1]
Adjuvant analgesics
Adjuvants are drugs whose primary indication is not pain but which have an analgesic action in specific pain types. They are added at any step of the ladder. [1]
- Neuropathic pain (burning, shooting, electric, allodynia from nerve infiltration or compression) responds poorly to opioids alone and requires a gabapentinoid. Gabapentin (start 100 to 300 mg nocte, titrate to 300 to 1200 mg three times daily, reduce in renal impairment) or pregabalin (start 75 mg bd, titrate to 150 to 300 mg bd) are first-line [6]. A tricyclic (nortriptyline 10 to 75 mg nocte) is an alternative. Dexamethasone (4 to 8 mg daily) reduces perineural oedema around an infiltrating tumour and is particularly useful for brachial and lumbosacral plexus pain.
- Bone pain responds to NSAIDs, dexamethasone, a bisphosphonate (zoledronic acid 4 mg) or denosumab, and palliative radiotherapy (single 8 Gy fraction for an uncomplicated painful bone metastasis).
- Smooth-muscle colic (renal or biliary) responds to an antispasmodic (hyoscine butylbromide 20 mg subcutaneously every four hours).
Opioid rotation and methadone for refractory pain
Opioid rotation is the switch from one opioid to another when side effects are unmanageable (neurotoxicity, myoclonus, delirium, intractable nausea) or when dose escalation fails. The method is: [1]
- Calculate the total 24-hour dose of the current opioid and convert to oral morphine equivalents using published equianalgesic ratios (oral morphine 30 mg = parenteral morphine 10 mg = oral oxycodone 20 mg = parenteral oxycodone 10 mg = transdermal fentanyl approximately 12 micrograms per hour).
- Reduce the calculated equivalent dose by 25 to 50 per cent for incomplete cross-tolerance between opioids.
- Choose the new opioid and route; give breakthrough immediate-release at one-sixth of the new daily dose.
- Reassess within 24 hours. [1]
Methadone is reserved for refractory cancer pain or neurotoxicity from other opioids and must be initiated by a specialist [7][8]. It is unique because it combines mu-receptor agonism with NMDA antagonism and noradrenaline and serotonin reuptake inhibition, giving it efficacy in neuropathic and opioid-resistant pain. Its challenges are the long and variable half-life (8 to 75 hours) causing accumulation and delayed toxicity, the variable and dose-dependent equianalgesic ratio with morphine (the rotation ratio varies from 4:1 at low morphose doses to 12:1 or higher at high doses), QT prolongation (baseline and periodic ECG), and CYP3A4 and CYP2B6 drug interactions. The Bruera 2004 trial established methadone as a viable first-line strong opioid, though morphine remains the global default [7].
Patient-controlled analgesia (PCA)
A PCA delivers a bolus of opioid on patient demand, with a lockout interval and an optional background infusion. It is used for severe acute pain (post-operative, painful procedures, titration of severe cancer pain) and for end-of-life pain when the oral route is lost. A typical morphine PCA is a 1 mg bolus with a 5 to 10 minute lockout; the bolus and lockout are titrated to pain control and sedation. PCA is a titration tool, not a long-term strategy. [1]
Exam trap: The most common opioid error is failing to reduce for incomplete cross-tolerance on rotation. The second is prescribing a fixed breakthrough dose and forgetting to recalculate it when the background dose changes. The third is starting a strong opioid without a laxative. [1]
3. Nausea and vomiting — a cause-specific approach
Why mechanism matters
Nausea in advanced cancer is rarely a single disease; it is a syndrome with several mechanisms, and the antiemetic must match the mechanism. A one-size-fits-all antiemetic is the most common prescribing error. The pathophysiology is centred on four receptor pathways in the chemoreceptor trigger zone, the vomiting centre and the gut: [1]
- Dopamine (D2) — the chemoreceptor trigger zone and the gut. Antagonised by haloperidol, metoclopramide, prochlorperazine, olanzapine.
- Histamine (H1) and muscarinic — the vomiting centre and the vestibular apparatus. Antagonised by cyclizine, promethazine, hyoscine.
- Serotonin (5-HT3) — the gut and the chemoreceptor trigger zone. Antagonised by ondansetron (more useful for chemotherapy than for chronic palliative nausea).
- Substance P (NK1) — the vomiting centre. Antagonised by aprepitant (largely a chemotherapy adjunct). [1]
The four clinical patterns and their first-line agents
Gastric stasis (impaired gastric emptying from opioids, autonomic failure, ascites or pressure) presents with early satiety, reflux, hiccup, and small-volume vomiting. The first-line agent is a prokinetic, because the problem is failure of forward propulsion. Metoclopramide 10 mg three times daily (a prokinetic and a D2 antagonist) is the standard; it should be given 30 minutes before meals. An avoidable error is giving an anticholinergic (cyclizine) here — it slows the gut and worsens the stasis. [1]
Chemical causes (opioids, hypercalcaemia, uraemia, drugs, chemotherapy) stimulate the chemoreceptor trigger zone. The first-line agent is a D2 antagonist: haloperidol 0.5 to 1.5 mg nocte (low dose, long duration, subcutaneous or oral) or olanzapine 2.5 to 5 mg nocte (broad spectrum, useful for multifactorial nausea). Olanzapine has randomised-trial evidence for advanced cancer-related nausea [10]. The underlying cause must also be treated — correct the hypercalcaemia, review the opioid, manage the renal failure.
Bowel obstruction (mechanical or functional, from intra-abdominal tumour, adhesions or opioid-induced gut dysmotility) presents with colic, distension, constipation and visible peristalsis. The antiemetic must not be a prokinetic — metoclopramide increases colic against a blockage. The first-line agent is cyclizine 50 mg three times daily (an antihistamine and anticholinergic) or hyoscine butylbromide 20 mg subcutaneously every four to six hours (an antispasmodic for the colic). A proton pump inhibitor or H2 antagonist reduces gastric secretions; a faecal regulator (macrogol or a stool-softener if there is a trickle of stool, avoiding a stimulant laxative in complete obstruction) manages the constipation. Dexamethasone 4 to 8 mg daily reduces peritumoural oedema and may partially relieve an obstruction; consider a venting gastrostomy, a stent or palliative surgery in selected patients. [1]
Raised intracranial pressure (brain metastasis, leptomeningeal disease) presents with morning headache, vomiting on waking, and sometimes papilloedema. The first-line agent is dexamethasone 8 to 16 mg daily, which reduces vasogenic oedema; whole-brain radiotherapy or focal treatment follows. An antiemetic is added for symptomatic relief. [1]
DWE discriminator: A stem describing a palliative patient with nausea will name the mechanism — "early satiety and small-volume vomiting" means gastric stasis (metoclopramide); "opioids started 48 hours ago and now vomiting" means chemical (haloperidol); "distended abdomen with visible peristalsis and colic" means obstruction (cyclizine, not metoclopramide); "morning headache and vomiting" means raised intracranial pressure (dexamethasone). Match the mechanism to the drug. [1]
4. Refractory breathlessness
The burden and the assessment
Breathlessness is the symptom that patients with advanced cancer and advanced respiratory disease fear most, and it drives more suffering than pain in the last months of life. It is out of proportion to objective measures — a patient with a near-normal saturation and only mildly abnormal lung fields can be in extremis with the effort of breathing, because breathlessness is a central perceptual experience involving the cortex, the mechanoreceptors of the chest wall and the chemoreceptors, not a simple reflection of gas exchange. [1]
The assessment combines the intensity (0 to 10 at rest and on exertion), the pattern (constant, episodic, on exertion, at rest, nocturnal), the impact (activities limited, anxiety, fear of suffocating), and a focused search for reversible contributors — pleural effusion, pulmonary embolism, anaemia, heart failure, COPD exacerbation, pneumonia, pneumothorax, pericardial effusion, ascites, pain with splinting, and anxiety. A reversible cause that can be treated (a pleural effusion drained, a pulmonary embolism anticoagulated, an effusion aspirated) relieves the breathlessness more than any drug. [1]
Oxygen — when it helps and when it does not
Oxygen helps the hypoxaemic patient (saturation below 90 per cent or a PaO2 below 60 mmHg), for whom supplemental oxygen relieves the hypoxic ventilatory drive and the work of breathing. Oxygen does not help the non-hypoxaemic patient with refractory dyspnoea. The landmark Abernethy randomised double-blind crossover trial of sustained-release morphine in refractory dyspnoea (BMJ 2003) and the subsequent 2010 multicentre trials showed that supplemental oxygen provided no symptomatic benefit over medical air in patients who were not hypoxaemic [9]. The corollary is that oxygen should be prescribed for a physiological indication (hypoxaemia), not as a comfort measure in the non-hypoxaemic patient.
The pharmacological management of refractory breathlessness
The first-line drug for refractory breathlessness in the non-hypoxaemic patient is low-dose oral morphine. In the opioid-naive patient, start at 2.5 mg of immediate-release oral morphine every four hours or as needed, titrating cautiously to symptom relief. In the patient already on an opioid for pain, give a dose equivalent to around 25 to 50 per cent of the existing breakthrough dose. The mechanism is a reduction in the ventilatory drive and the central perception of breathlessness; at these low doses, clinically significant respiratory depression does not occur when the dose is titrated carefully and reviewed [9]. The predictable side effects — constipation and transient nausea — are managed as for any opioid.
Benzodiazepines are useful when anxiety is a prominent component (the panic-dyspnoea-panic cycle). Lorazepam 0.5 mg sublingually as needed, or a small regular dose, breaks the cycle. Benzodiazepines are not first-line for breathlessness itself — they treat the anxiety component. [1]
Non-pharmacological measures are the foundation: sit the patient upright and leaning forward over a table (to use the accessory muscles and the diaphragm), pursed-lip breathing, a fan directed to the face (the cool airflow reduces the perceived work of breathing through trigeminal afferents), relaxation techniques, carer education, and pacing of activity. These measures are as important as the drugs and are the first thing to teach the patient and the family. [1]
DWE discriminator: The answer to "best drug for refractory breathlessness in a non-hypoxaemic patient with advanced cancer?" is low-dose oral morphine, not oxygen. Oxygen is reserved for the hypoxaemic patient; a fan to the face and upright positioning are first-line non-pharmacological measures; a benzodiazepine is added for the anxiety component. [1]
5. Delirium, terminal restlessness and agitation
A multi-factorial syndrome
Delirium is extremely common in advanced cancer and at the end of life, affecting up to 80 per cent of patients in the final days. It is an acute fluctuating disturbance of attention and cognition with a perceptual component (hallucinations, delusions) and a motor component (hyperactive, hypoactive, or mixed). The error is to dismiss it as "the patient is dying" — delirium is a syndrome with a cause, and a reversible cause must be sought first. [1]
The reversible precipitants of delirium in the palliative patient are: [1]
- Drugs — opioids (especially accumulation of morphine-6-glucuronide in renal impairment), corticosteroids, anticholinergics, benzodiazepines.
- Metabolic — hypercalcaemia, hyponatraemia, hypoglycaemia, uraemia, hepatic failure, hypoxia.
- Infection — urinary tract, pneumonia, line infection.
- Structural — brain metastasis, leptomeningeal disease, cerebral haemorrhage or infarct.
- Retained products — urinary retention, constipation, faecal impaction.
- Sensory — uncorrected hearing or visual impairment, sleep deprivation, an unfamiliar environment. [1]
The management
The first step is always to seek and treat the reversible cause. A catheter for retention, an enema for impaction, oxygen for hypoxia, antibiotics for a symptomatic infection (not routinely for asymptomatic colonisation in the dying patient), a change of opioid for neurotoxicity, a decrease of the dexamethasone dose, and correction of the metabolic abnormalism. [1]
The first-line drug for delirium in palliative care is haloperidol 0.5 to 2 mg orally or subcutaneously, repeated as needed. The Hui 2017 randomised trial (haloperidol plus lorazepam versus haloperidol alone for agitated delirium in advanced cancer) found that adding lorazepam improved the agitation control without excess sedation [4], and the Hui 2020 INPTSED cluster-randomised trial compared neuroleptic strategies (haloperidol escalation, chlorpromazine rotation, or combination) for refractory terminal agitation [5]. The practical message is: haloperidol first-line; add lorazepam or rotate to a more sedating antipsychotic (chlorpromazine, levomepromazine) for refractory agitation.
Midazolam 2.5 to 5 mg subcutaneously, followed by a continuous subcutaneous infusion (10 to 60 mg over 24 hours), is the agent of choice for terminal agitation refractory to an antipsychotic. The benzodiazepine is reserved for terminal agitation (and for alcohol or benzodiazepine withdrawal) because benzodiazepines paradoxically worsen delirium when given first-line. [1]
Exam trap: The most common delirium error is using a benzodiazepine first. Benzodiazepines worsen delirium and are reserved for withdrawal or for terminal agitation refractory to an antipsychotic. First-line for delirium in palliative care is haloperidol. [1]
6. Constipation and the opioid-laxative contract
Opioid-induced constipation is universal, develops within days of starting an opioid, and — uniquely among opioid side effects — tolerance never develops. The mechanism is mu-receptor agonism in the enteric nervous system, which increases non-propulsive intestinal tone, decreases secretions, and slows transit. The result is hard, dry stools that do not respond to softening alone. [1]
The contract is that an opioid is never started without a laxative. The first-line regimen is a stimulant laxative plus an osmotic agent: [1]
- Stimulant — senna 15 mg (two tablets) nocte, titrated to effect, or bisacodyl 5 to 10 mg nocte. The stimulant provides the propulsive activity the opioid has abolished.
- Osmotic — macrogol (one sachet in water once or twice daily) or lactulose 15 to 30 mL bd. The osmotic draws water into the bowel to soften the stool. [1]
The dose is titrated at every review to achieve a comfortable stool pattern. For established faecal impaction, a rectal measure (a glycerine suppository, a phosphate enema, or manual evacuation under sedation in extreme cases) is required before the oral regimen can work. [1]
For opioid-induced constipation refractory to conventional laxatives in the advanced-illness patient, methylnaltrexone (a peripherally acting mu-antagonist that does not cross the blood-brain barrier and so does not reverse analgesia) is given as 8 mg subcutaneously every other day and produces a bowel motion within hours in most patients. It is reserved for refractory cases because of cost and the need to exclude mechanical obstruction first (it causes colic against a blockage). [1]
DWE discriminator: A stem describing a patient with severe constipation on morphine asks for the best management. The answer is a stimulant laxative (senna) plus an osmotic (macrogol), not a stool softener alone — docusate is too weak for opioid-induced constipation. The stimulant is the essential component because it provides the propulsive activity the opioid has abolished. [1]
7. Anorexia, cachexia and fatigue
The cancer anorexia-cachexia syndrome
The cancer anorexia-cachexia syndrome is a cytokine-mediated metabolic disorder characterised by loss of skeletal muscle disproportionate to fat loss, anorexia, weight loss, inflammation, insulin resistance, and increased resting energy expenditure. It is distinct from starvation (which preserves muscle until late and responds to feeding) — feeding alone does not reverse cachexia because the cytokine-driven catabolism persists. It affects the majority of patients with advanced cancer and is a major driver of fatigue, weakness, functional decline, and reduced tolerance to treatment. [1]
Pharmacological options (limited benefit)
The pharmacological options are limited and the benefit modest: [1]
- Corticosteroids — prednisolone 20 to 40 mg daily or dexamethasone 2 to 4 mg daily for one to two weeks improve appetite, wellbeing and energy for a short period. They do not increase lean body mass and the benefit wanes; they are most useful for a short-term boost in the last weeks of life.
- Megestrol acetate — a progestogen with appetite-stimulant effect. The landmark randomised trials showed a dose-response for appetite and weight gain at 160 to 800 mg daily [3], but the weight gained is largely fat and fluid, the survival benefit is unproven, and there is a risk of thromboembolism. A typical dose is 160 to 320 mg daily.
- Other agents — olanzapine has appetite and weight effects (see the olanzapine antiemetic evidence [10]); the cannabinoid dronabinol has modest appetite effects in some trials but with significant central side effects. Neither is first-line.
The realistic goal
The realistic goal is to set the family's expectations honestly — that the appetite will not return to normal, that forcing food does not reverse the cachexia and may cause nausea and aspiration, and that the focus is on comfort feeding (small amounts of preferred foods for pleasure) rather than caloric targets. A dietitian's input helps with texture modification, oral nutritional supplements in selected patients, and the management of dry mouth and taste change. The single most important intervention is often to lift the burden of guilt from the family who feel they are starving their loved one. [1]
8. The last days of life — recognising the dying patient
The clinical signs of the dying phase
The recognition that a patient is in the last days of life is a clinical judgement based on a constellation of signs and on the trajectory of the illness. The signs are: [1]
- Progressive weakness and reduced mobility — the patient becomes bed-bound and needs assistance with all care.
- Reduced oral intake — loss of appetite, difficulty swallowing, and reduced thirst; this is a natural part of the dying process, not a cause of suffering that requires forced hydration.
- Reduced urine output — concentrated or scant urine as the kidneys shut down.
- Increasing drowsiness and reduced consciousness — the patient spends increasing time asleep and is harder to rouse.
- Changes in breathing — Cheyne-Stokes respiration (periods of apnoea alternating with deepening breaths), noisy respiratory secretions (the "death rattle").
- Peripheral changes — mottling and cooling of the extremities, a weak or thready pulse.
- The patient's own sense — many patients verbalise that they are dying, and the family often senses it too. [1]
Recognition triggers a change in the care plan from active treatment to comfort-focused care, the withdrawal of non-essential medications, and the institution of anticipatory prescribing. [1]
Withdrawing non-essential medications
In the dying patient, the burden of polypharmacy outweighs the benefit of most preventive medications. Stop the statins, the antihypertensives, the oral hypoglycaemics (with a sliding scale if symptomatic), the disease-modifying treatments, the supplements, and the antibiotics for a non-symptomatic infection. Continue the drugs that contribute to comfort — analgesics, antiemetics, anxiolytics, anticonvulsants, antimuscarinics for secretions — converting them to the subcutaneous route or a continuous subcutaneous infusion (syringe driver) when the oral route is lost. The syringe driver is the delivery system of choice for the dying patient who can no longer swallow; it allows several compatible medicines to be combined in a single 24-hour infusion. [1]

Anticipatory prescribing — the four medicines
The NICE NG31 guideline (Care of dying adults in the last days of life) recommends that four injectable medicines be prescribed in advance for the common symptoms of the dying patient, available for subcutaneous administration by the community or ward nurse. The principle is that a symptom should not go untreated for want of an available drug, particularly out of hours. [1]
| Symptom | Drug | Subcutaneous dose |
|---|---|---|
| Pain or breathlessness | Morphine (or oxycodone) | 2.5 to 5 mg hourly as needed |
| Nausea or vomiting | Haloperidol (or cyclizine for obstruction) | 0.5 to 1.5 mg as needed, or 5 to 10 mg over 24 hours |
| Respiratory secretions | Glycopyrronium (or hyoscine butylbromide) | 200 micrograms as needed, up to every 4 hours |
If a patient requires several doses of an anticipatory medicine in 24 hours, the requirement is converted to a continuous subcutaneous infusion in a syringe driver, with the as-needed dose retained for breakthrough. The syringe driver is reviewed daily, the dose is titrated to symptom control, and the family is kept informed. [1]
DWE discriminator: The four anticipatory medicines — morphine, midazolam, haloperidol, glycopyrronium — are a high-yield exam fact. A stem describing a dying patient at home with new agitation asks for the best drug: midazolam 2.5 to 5 mg subcutaneously. A stem describing noisy respiratory secretions asks for glycopyrronium or hyoscine butylbromide, not a suction catheter. [1]
9. Advance care planning and goals of care
The goals-of-care conversation
The goals-of-care conversation is the cornerstone of good palliative care. It is not a single event but a series of conversations that evolve with the illness. The structure is: [1]
- Explore understanding — "Tell me what you understand about your illness and what the doctors have told you."
- Explore values and priorities — "What is most important to you right now? What are you hoping for? What are you worried about?"
- Share information — honest prognostic framing in plain language, including the realistic outcomes of treatment options.
- Align — connect the medical recommendations to the patient's values, and propose a plan that fits.
- Document and review — record the agreed plan, communicate it to the team and the family, and review it as the illness changes. [1]
Advance directives and substitute decision-making
An advance care directive (also called an advance decision, advance statement, or living will, depending on jurisdiction) is a document in which a competent adult records their preferences for future medical treatment, to apply at a time when they have lost capacity. In ANZ, an advance care directive is legally recognised in most states and territories, and may be binding or persuasive depending on the jurisdiction and the wording. A patient may also appoint an enduring guardian (or a medical enduring power of attorney, or a "person responsible") to make health and lifestyle decisions on their behalf. [1]
When a patient lacks capacity, the physician acts in the patient's best interests using the substituted judgement standard — what would this patient have wanted, based on their prior statements, values, the advance directive, and the substitute decision-maker's knowledge of the patient. Where there is dispute or no substitute, a guardianship tribunal or board may be consulted. [1]
Ceilings of treatment and not-for-resuscitation orders
A ceiling of treatment agreement documents the level of intervention that is appropriate in the event of deterioration — for example, ward-based care but not ICU, or symptom-focused care with no escalation. A not-for-resuscitation (or not-for-cardiopulmonary resuscitation) order documents the decision not to attempt CPR in the event of cardiac arrest. The conversation should frame CPR in the context of the patient's overall illness — in advanced cancer, frailty and end-stage organ disease, CPR rarely succeeds and may cause harm — and should be paired with a clear statement of what will be done (focused on comfort, symptom relief and dignity), not only what will not be done. The decision is documented with the rationale and communicated to the team. [1]
10. Communication — breaking bad news and supporting the family
The SPIKES protocol
The SPIKES protocol (Baile 2000) is the standard six-step framework for delivering bad news [2]. It is examinable in the DCE long case and in communication stations.
- S — Setting. A private space, seated, with a senior clinician and a nurse, time set aside, interruptions minimised, and a key family member or friend present if the patient wishes.
- P — Perception. Ask what the patient already understands: "What have the doctors told you about your illness?" This avoids both information overload and information denial.
- I — Invitation. Ask how much information the patient wants: "Would you like me to go through the results in detail, or would you prefer a summary?" Respect a wish not to know in detail.
- K — Knowledge. Give a warning shot ("I'm afraid the news is not what we hoped for"), then deliver the information in plain language, in small chunks, with pauses to check understanding. Avoid jargon.
- E — Emotions. Acknowledge and name the emotion, validate it, and allow silence: "This is clearly a great shock. I can see how hard this is. Take a moment." This is the step most often skipped and the most important.
- S — Strategy and Summary. Agree a clear plan, give a written summary, name a single point of contact, and arrange follow-up. [1]
DCE long-case insight: The most common communication error is information overload — delivering a monologue of detail that the patient cannot absorb. The SPIKES protocol emphasises assessing perception and invitation before delivering information, and the most important step is responding to the emotion with empathy and silence. [1]
Supporting the family and bereavement
The family is a unit of care. The physician supports them by giving honest information in plain language, offering time for questions and for grief, attending to cultural and spiritual needs (the involvement of pastoral care if wished), providing a written plan and a named contact, and arranging bereavement support before and after the death. A bereavement risk assessment identifies those at risk of complicated grief — anticipatory grief, a sudden or traumatic death, prior mental illness, social isolation, a dependent relationship, and a death perceived as preventable. Specialist bereavement services are offered to those at risk. [1]
11. Ethical issues — capacity, voluntary assisted dying and palliative sedation
Capacity
Capacity is decision-specific and time-specific — a patient may have capacity to consent to a blood transfusion but not to a complex chemotherapy regimen, and capacity may fluctuate with delirium. It is assessed by the four-step functional test: the patient can understand the information, retain it, weigh it (use it in the decision), and communicate the decision (by any means). Capacity is presumed unless demonstrated otherwise, and a capacitous refusal of treatment — even a life-sustaining treatment — must be respected. [1]
Voluntary assisted dying and the distinction from palliative sedation
Voluntary assisted dying (VAD) — the administration of a lethal substance at the voluntary, informed request of a competent adult with a terminal illness — is lawful in a growing number of jurisdictions, including all Australian states under specific legislation with eligibility criteria (terminal illness, expected death within a defined period, decision-making capacity, voluntary and enduring request). The physician's role is to respond to a request with care: explore the reasons (often unrelieved pain, depression, fear, loss of autonomy, perceived burden), address any reversible suffering, involve specialist palliative care and mental health input, be honest about what is legally available, and do not abandon the patient whether or not they pursue VAD. [1]
Palliative sedation is distinct from VAD and from euthanasia. It is the proportionate use of sedatives (typically midazolam) to relieve a refractory symptom — pain, breathlessness, delirium or agitation that has not responded to standard management. The intent is symptom relief, the dose is titrated to effect, and death is neither hastened nor prolonged. The doctrine of double effect — that an action with a foreseen but unintended bad consequence (sedation, possibly a shorter survival) is permissible when the intended consequence (relief of suffering) is good and proportionate — underpins the ethical legitimacy of palliative sedation. It is not euthanasia, and the distinction (intent and proportionality) is a high-yield DCE discussion point. [1]
Exam traps and high-yield discriminators
- The WHO analgesic ladder — Step 1 non-opioid, Step 2 weak opioid, Step 3 strong opioid, adjuvants at every step. The breakthrough opioid dose is one-sixth of the total 24-hour long-acting dose.
- Always co-prescribe a laxative with an opioid — a stimulant (senna) plus an osmotic (macrogol). Docusate alone is too weak. Opioid-induced constipation is universal and tolerance never develops.
- Antiemetics are cause-specific — metoclopramide for gastric stasis, haloperidol or olanzapine for chemical causes, cyclizine or hyoscine for bowel obstruction, dexamethasone for raised intracranial pressure. Never give metoclopramide in bowel obstruction.
- Low-dose oral morphine is first-line for refractory breathlessness in the non-hypoxaemic patient; oxygen offers no benefit over room air in this group (Abernethy, BMJ 2003 [9]). Oxygen is reserved for the hypoxaemic patient.
- Haloperidol is first-line for delirium in palliative care; benzodiazepines (midazolam) are reserved for terminal agitation refractory to an antipsychotic and for withdrawal states.
- The four anticipatory medicines are morphine (pain, breathlessness), midazolam (agitation), haloperidol (nausea, delirium), and glycopyrronium (secretions). All subcutaneous.
- Palliative care is introduced early and in parallel with disease-directed therapy — the Temel 2010 trial showed improved quality of life and survival (NEJM [1]).
- Methadone rotation requires specialist input because of the variable equianalgesic ratio, accumulation, and QT prolongation. Reduce for incomplete cross-tolerance on any opioid rotation.
- Palliative sedation is not euthanasia — the intent is symptom relief, the dose is titrated, and death is neither hastened nor prolonged. The distinction is intent and proportionality.
Cross-links
- Oncologic emergencies — malignant spinal cord compression, hypercalcaemia of malignancy and superior vena cava obstruction present as acute events in the palliative population; their emergency management is detailed in the oncologic emergencies topic.
- Delirium — the full assessment and management of delirium in the older hospital patient, including the differentiation from dementia and depression, is detailed in the delirium topic.
- Dementia — advance care planning, capacity assessment and substitute decision-making in the cognitively impaired patient are covered in the dementia topic.
- Electrolyte and metabolic disturbances — hypercalcaemia, hyponatraemia and other metabolic disturbances that cause symptoms in the palliative patient are detailed in the relevant electrolyte topics.
- The deteriorating ward patient — recognising and responding to clinical deterioration, and the goals-of-care conversation that follows, are covered in the deteriorating ward patient topic. [1]
References and guidelines
Temel early palliative care in metastatic NSCLC (NEJM 2010) [1]; Baile SPIKES protocol for delivering bad news (The Oncologist 2000) [2]; Loprinzi megestrol acetate for cancer anorexia and cachexia (JNCI 1990) [3]; Hui lorazepam plus haloperidol for agitated delirium in advanced cancer (JAMA 2017) [4]; Hui INPTSED neuroleptic strategies for terminal agitation (Lancet Oncol 2020) [5]; Wiffen gabapentin for chronic neuropathic pain (Cochrane 2017) [6]; Bruera methadone versus morphine as a first-line strong opioid (JCO 2004) [7]; Bruera opioid rotation and dose ratios (Cancer 1996) [8]; Abernethy sustained-release morphine for refractory dyspnoea (BMJ 2003) [9]; olanzapine for advanced cancer-related nausea and vomiting (JAMA Oncol 2020) [10]. WHO 2018 definition of palliative care and WHO 2018 cancer pain guideline; NICE NG31 care of dying adults in the last days of life; NICE NG142 end of life care for adults: service delivery; EAPC and NCP Clinical Practice Guidelines for Quality Palliative Care; Palliative Care Australia national standards; ANZSPM clinical guidance.
References
- [1]Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer N Engl J Med, 2010.PMID 20818875
- [2]Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer Oncologist, 2000.PMID 10964998
- [3]Loprinzi CL, Ellison NM, Schaid DJ, et al. Controlled trial of megestrol acetate for the treatment of cancer anorexia and cachexia J Natl Cancer Inst, 1990.PMID 2193166
- [4]Hui D, Frisbee-Hume S, Wilson A, et al. Effect of Lorazepam With Haloperidol vs Haloperidol Alone on Agitated Delirium in Patients With Advanced Cancer Receiving Palliative Care: A Randomized Clinical Trial JAMA, 2017.PMID 28975307
- [5]Hui D, Dev R, Pimental L, et al. Neuroleptic strategies for terminal agitation in patients with cancer and delirium at an acute palliative care unit: a single-centre, double-blind, parallel-group, randomised trial Lancet Oncol, 2020.PMID 32479786
- [6]Wiffen PJ, Derry S, Bell RF, et al. Gabapentin for chronic neuropathic pain in adults Cochrane Database Syst Rev, 2017.PMID 28597471
- [7]Bruera E, Palmer JL, Bosnjak S, et al. Methadone versus morphine as a first-line strong opioid for cancer pain: a randomized, double-blind study J Clin Oncol, 2004.PMID 14701781
- [8]Bruera E, Pereira J, Watanabe S, Belzile M, Kuehn N, Hanson J Dose ratio between morphine and methadone in patients with cancer pain: a retrospective study Cancer, 1998.PMID 9506365
- [9]Abernethy AP, Currow DC, Frith P, Fazekas BS, McHugh A, Bui C Randomised, double blind, placebo controlled crossover trial of sustained release morphine for the management of refractory dyspnoea BMJ, 2003.PMID 12958109
- [10]Navari RM, Nagy C, Gray R, et al. Olanzapine for the Prevention of Chemotherapy-Induced Nausea and Vomiting N Engl J Med, 2016.PMID 27410922