Phys · pharmacological
Adverse Drug Reactions — Classification, Recognition and Management
Also known as adverse drug reaction · ADR · drug side effect · adverse drug event · DRESS · drug reaction with eosinophilia and systemic symptoms · Stevens-Johnson syndrome · SJS · toxic epidermal necrolysis · TEN · drug-induced agranulocytosis · drug-induced liver injury · Hy's law · drug-induced interstitial lung disease · pharmacovigilance
Consultant-physician-depth guide to adverse drug reactions (ADRs): the Rawlins and Thompson ABCDEF classification, causality assessment (Naranjo), the high-yield severe reactions a physician must not miss (DRESS, SJS/TEN, drug-induced agranulocytosis and thrombocytopenia, DILI and Hy's Law, drug-induced interstitial lung disease, QT prolongation), Type E withdrawal syndromes, Type F treatment failure, Yellow Card and TGA reporting, and prevention through medication reconciliation and electronic alerts — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Adverse Drug Reactions — Classification, Recognition and Management

The one-minute consultant answer
An adverse drug reaction (ADR) is an appreciably harmful or unpleasant reaction resulting from the use of a medicinal product, which predicts hazard from future administration and warrants prevention, specific treatment, dose alteration, or withdrawal of the drug [1]. ADRs are common, often preventable, and account for roughly 6 to 7 per cent of all hospital admissions, with the burden concentrated in older patients on multiple medications [2][11]. The Pirmohamed BMJ study of 18,820 admissions found aspirin, diuretics, warfarin and NSAIDs were the commonest culprits, and that most reactions were definitely or possibly avoidable [2].
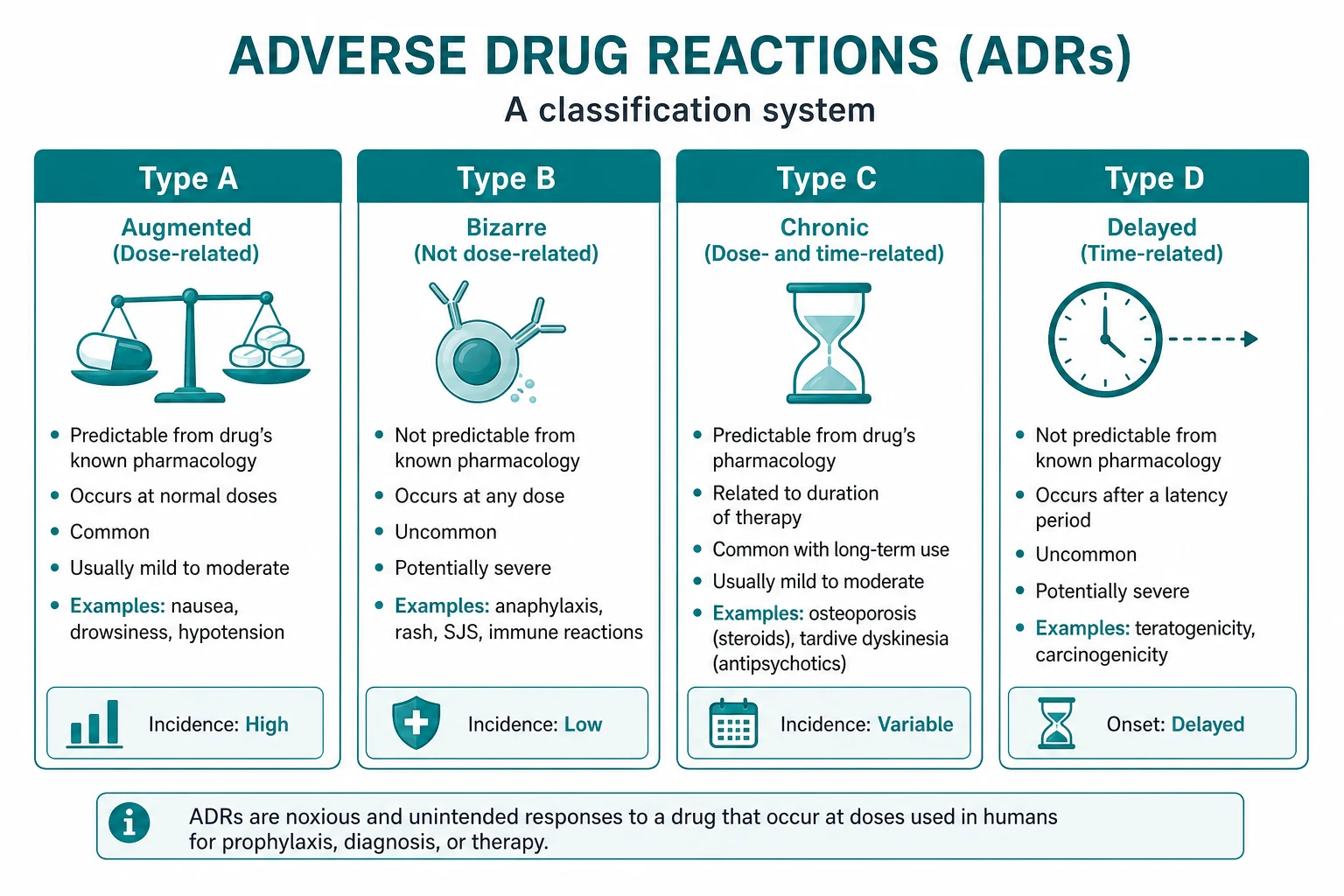
The conceptual anchor for the whole topic is the Rawlins and Thompson classification, refined by Edwards and Aronson, which sorts reactions into six types by their relationship to dose and time [1]:
- Type A (Augmented) — an exaggerated but otherwise normal pharmacological action; dose-dependent, predictable, common, low mortality. Examples: beta-blocker bradycardia, anticoagulant bleeding, opioid constipation.
- Type B (Bizarre) — a reaction novel to the drug's pharmacology; dose-independent, unpredictable, rare, high mortality when severe. Examples: anaphylaxis, DRESS, SJS/TEN, drug-induced agranulocytosis.
- Type C (Chronic) — cumulative dose over time. Examples: bisphosphonate osteonecrosis of the jaw, methotrexate hepatic fibrosis, amiodarone pulmonary toxicity.
- Type D (Delayed) — delayed in time, sometimes long after the drug is stopped. Examples: teratogenesis (thalidomide, isotretinoin), carcinogenesis (DES and vaginal clear-cell carcinoma).
- Type E (End-of-treatment) — withdrawal. Examples: opiate withdrawal, adrenal suppression after long-term steroids, clonidine rebound hypertension.
- Type F (Failure) — unexpected failure of therapy. Examples: oral contraceptive failure with enzyme inducers or antibiotics, warfarin failure with concurrent vitamin K. [1]
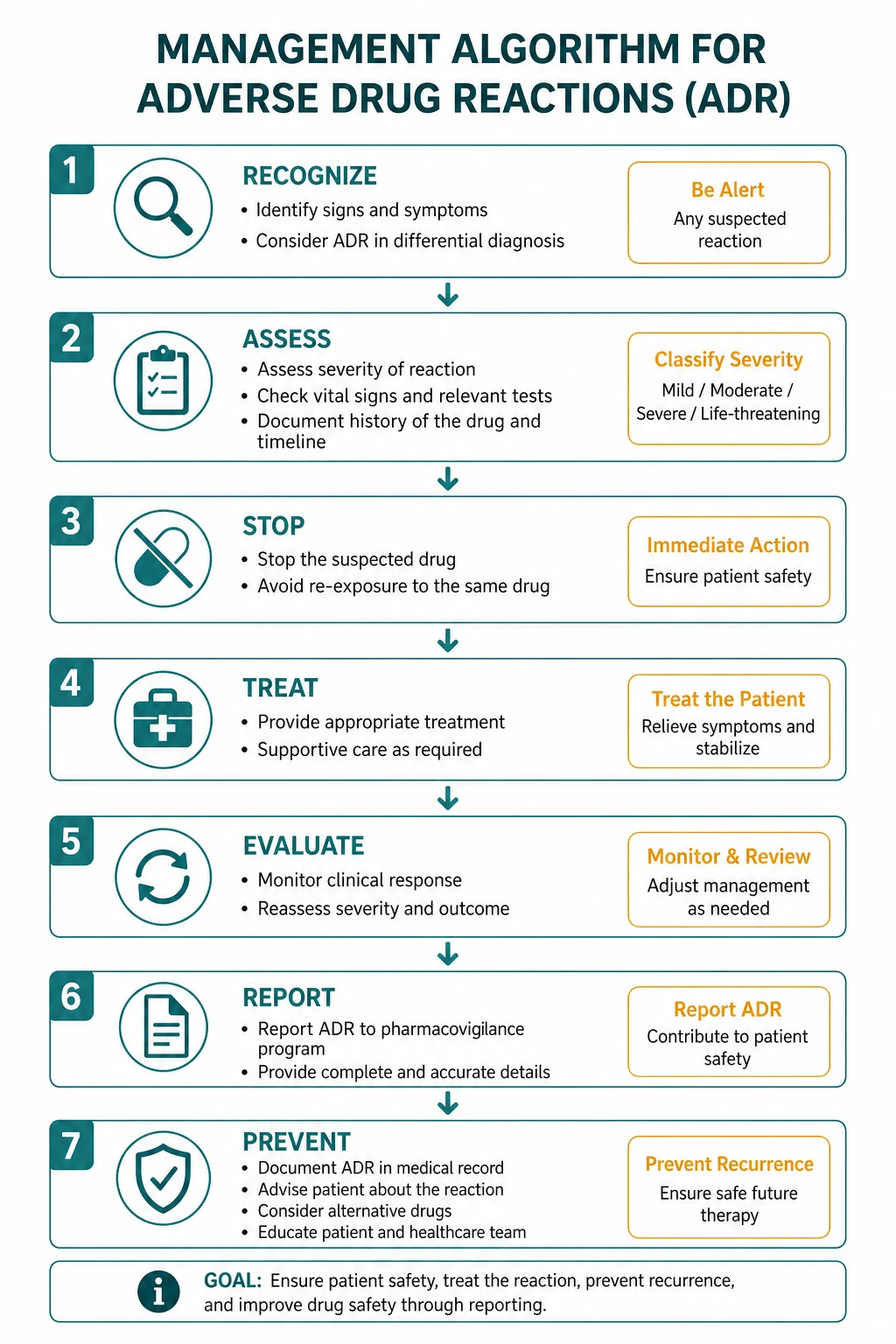
The clinical task at the bedside is threefold: recognise the reaction as drug-related, stop or substitute the offending agent, and report it. Recognition rests on a careful drug history with temporal association and the application of a causality tool such as the Naranjo scale [3]. For the severe Type B reactions — DRESS, SJS/TEN, agranulocytosis, HIT, severe DILI and DI-ILD — early recognition is the difference between recovery and death. Every severe or previously unrecognised reaction should be reported to the TGA in Australia (the Blue Card) or through the MHRA Yellow Card scheme in the UK, because pharmacovigilance depends on clinician reporting [1].
The ABCDEF classification — the table you must memorise

The classification is the spine of the topic because it predicts how a reaction will behave and what to do about it. Learn the mnemonic letter, the property it stands for, and one canonical example for each [1].
| Type | Mnemonic | Property | Dose link | Frequency | Severity | Canonical examples |
|---|---|---|---|---|---|---|
| A | Augmented | Exaggerated normal pharmacology | Dose-dependent | Common (about 80 per cent of all ADRs) | Usually low mortality | Beta-blocker bradycardia, warfarin bleeding, opioid constipation, ACE inhibitor cough, statin myopathy |
| B | Bizarre | Novel, not from known pharmacology | Dose-independent | Rare | High mortality when severe | Anaphylaxis, DRESS, SJS/TEN, drug-induced agranulocytosis, HIT |
| C | Chronic | Cumulative dose over time | Dose and time-related | Variable | Often irreversible | Bisphosphonate osteonecrosis of the jaw, methotrexate hepatic fibrosis, amiodarone pulmonary and thyroid toxicity, analgesic nephropathy |
| D | Delayed | Delayed, sometimes years later | Time-related | Rare | Serious | Thalidomide and isotretinoin teratogenesis, diethylstilboestrol and clear-cell vaginal carcinoma, cyclophosphamide and bladder cancer |
| E | End-of-treatment | Withdrawal syndrome | Timing of cessation | Common for the drug | Usually reversible | Opiate and benzodiazepine withdrawal, adrenal suppression after long-term steroids, clonidine rebound hypertension, beta-blocker rebound tachycardia |
| F | Failure | Unexpected therapeutic failure | Effectiveness | Common for the combination | Indirect harm | Oral contraceptive failure with rifampicin or enzyme inducers; warfarin failure with vitamin K or concurrent cholestyramine |
The exam-tested discriminating question is: is this dose-dependent and predictable (Type A), or dose-independent and bizarre (Type B)? Almost everything that can kill a patient quickly is Type B; almost everything that is dose-related, common and avoidable is Type A [1].
The mnemonic: ABCDEF — Augmented, Bizarre, Chronic, Delayed, End-of-use, Failure. A frequent follow-up asks for two examples per type; the table above is the answer. [1]
Why ADRs happen — the pharmacological reasoning
Type A reactions are simply the pharmacology of the drug acting at an inconvenient dose or in a susceptible patient. The dose–response curve is shifted: the same drug that controls angina at 25 mg of metoprolol produces symptomatic bradycardia at 100 mg in a 78-year-old with renal impairment and concurrent diltiazem. The keys to predicting Type A reactions are the drug's known mechanism, the patient's clearance (renal and hepatic function), and the concurrent medications that add to or potentiate the effect [1].
Type B reactions are mechanistically heterogeneous. Most are immune-mediated, driven by the drug or a reactive metabolite acting as a hapten that binds to a host protein and triggers a T-cell or antibody response. The HLA associations make this explicit: HLA-B1502 strongly predicts carbamazepine-induced SJS/TEN in Han Chinese and Southeast Asian populations (prevalence-driven pre-prescription screening is standard of care in those groups), and HLA-B5801 predicts allopurinol-induced SJS/TEN, especially in Han Chinese, Thai and Korean populations. A subset of Type B reactions are pseudoallergic (direct mast-cell activation, e.g., vancomycin infusion reaction, radiocontrast) and mimic allergy without an immune mechanism [1][4].
The clinically useful corollary: Type A reactions are usually managed by reducing the dose or stopping the drug and re-challenging cautiously; Type B reactions mandate stopping the drug permanently and never re-challenging [1].
Causality assessment — the Naranjo scale
Once you suspect an ADR, the next question is whether the drug really caused it. The Naranjo Adverse Drug Reaction Probability Scale is a validated 10-item questionnaire that categorises the relationship as definite, probable, possible or doubtful [3].
The ten items each carry a weighted score (1, 0, or minus 1): [1]
| Naranjo item | Score if yes |
|---|---|
| Are there previous conclusive reports of this reaction? | plus 1 |
| Did the reaction appear after the suspected drug was administered? | plus 1 |
| Did the reaction improve when the drug was discontinued or a specific antagonist was given? | plus 1 |
| Did the reaction reappear when the drug was re-administered? | plus 2 |
| Are there alternative causes that could on their own have caused the reaction? | minus 1 |
| Did the reaction reappear when a placebo was given? | minus 1 |
| Was the drug detected in blood or other fluids in concentrations known to be toxic? | plus 1 |
| Was the reaction more severe when the dose was increased, or less severe when the dose was decreased? | plus 1 |
| Did the patient have a similar reaction to the same or similar drugs in any previous exposure? | plus 1 |
| Was the reaction confirmed by any objective evidence? | plus 1 |
Interpretation of the total score: [1]
| Total score | Causality |
|---|---|
| More than 9 | Definite |
| 5 to 8 | Probable |
| 1 to 4 | Possible |
| 0 or less | Doubtful |
The two most heavily weighted items are rechallenge (plus 2) and the presence of an alternative cause (minus 1). In practice, rechallenge is ethically barred in severe Type B reactions — you do not re-challenge DRESS or SJS — so most causality assignment in clinical practice rests on the temporal relationship, dechallenge (improvement on withdrawal), and exclusion of alternatives [1][3].
The exam trap: Naranjo classifies causality, not severity. Severity is a separate axis (mild, moderate, severe). [1]
The severe Type B reactions — recognise or the patient dies
The reactions that kill patients are clustered in Type B. The physician's job is to recognise each by its trigger list, its clinical signature and its timeline, then act immediately. [1]

DRESS — Drug Reaction with Eosinophilia and Systemic Symptoms
DRESS is a delayed, immune-mediated, multi-organ hypersensitivity reaction. It carries a mortality of around 5 to 10 per cent, usually from liver failure or overwhelming infection related to immunosuppression [4].
The classical trigger list is aromatic anticonvulsants (phenytoin, carbamazepine, lamotrigine, phenobarbital), allopurinol, minocycline, sulfonamide antibiotics, dapsone, and abacavir. The reaction begins 2 to 8 weeks after first exposure — long after a simple allergy would have declared itself. The exam-wary candidate hears "rash four weeks after starting allopurinol" and reaches for DRESS, not for simple urticaria. [1]
The clinical signature is a triad of fever, rash, and internal organ involvement with eosinophilia [4]:
- Fever — typically above 38.5 degrees, often the first sign.
- Rash — a morbilliform, sometimes exfoliative eruption, often with facial oedema, which distinguishes it from a simple drug rash. Scaling and desquamation may follow.
- Lymphadenopathy — generalised, sometimes massive.
- Eosinophilia — characteristically above 0.5 times ten to the ninth per litre, and often above 1.5; atypical lymphocytes are also seen.
- Organ involvement — the liver is the most commonly affected (hepatitis with transaminitis, sometimes progressing to fulminant failure); the kidney (interstitial nephritis with AKI); the lung (pneumonitis); and the heart (myocarditis, which carries the highest mortality). The pattern of organ involvement depends on the culprit. [1]
The RegiSCAR scoring system (used for research classification but useful clinically) assigns points for fever, lymphadenopathy, the type of rash, eosinophilia, organ involvement and the exclusion of alternatives. A score above 5 is definite DRESS, 4 to 5 is probable, 2 to 3 is possible, and below 2 is no DRESS [4].
The key teaching point: DRESS can flare and relapse for weeks after the drug is stopped, partly because of reactivation of human herpesvirus 6 (HHV-6). The patient is not "better" when the rash fades; they need close follow-up. [1]
Management: [1]
- Stop the offending drug — and any cross-reactive agents (e.g., all aromatic anticonvulsants if phenytoin is the culprit).
- Supportive care and organ-specific monitoring — daily liver function and renal function for the first week.
- Systemic corticosteroids for visceral involvement — oral prednisolone 0.5 to 1 mg per kg per day (or IV methylprednisolone for severe disease), tapered slowly over weeks to months to prevent relapse.
- Avoid rechallenge — document the reaction and the culprit clearly in the medication record. [1]
The exam trap: a patient started on allopurinol for gout (often at too high a dose in chronic kidney disease) who presents four weeks later with fever, rash, eosinophilia and hepatitis. The HLA-B5801 association means this is commoner in Han Chinese, Thai and Korean patients; in many ANZ centres HLA-B5801 screening is recommended before starting allopurinol in these populations. [1]
Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN)
SJS and TEN are a spectrum of the same disease defined by the extent of epidermal detachment: SJS involves less than 10 per cent of body surface area, SJS-TEN overlap 10 to 30 per cent, and TEN more than 30 per cent [5]. Mortality is roughly 10 per cent for SJS, 30 per cent for TEN, and approaches 50 per cent for extensive TEN — making it the most lethal of the drug eruptions.
The classical triggers are allopurinol, anticonvulsants (lamotrigine, carbamazepine, phenytoin), sulfonamide antibiotics, nevirapine, and oxicam NSAIDs. As with DRESS, the HLA associations are strong and racially patterned: HLA-B1502 for carbamazepine SJS/TEN in Han Chinese and Southeast Asians; HLA-B5801 for allopurinol. [1]
The clinical signature: [1]
- A prodrome of fever, malaise and upper respiratory symptoms, followed by a painful or burning skin.
- Mucocutaneous blistering with target lesions, atypical targets and flaccid bullae. Mucosal involvement of at least two sites (oral, conjunctival, urogenital, tracheobronchial) is characteristic.
- Sheet-like epidermal detachment with a positive Nikolsky sign (gentle lateral pressure shears the epidermis).
- Systemic involvement — hepatitis, gastrointestinal erosions, pneumonitis, and acute kidney injury from fluid loss and sepsis. [1]
Severity is scored with the SCORTEN, calculated at admission and again at 48 hours [5]. Each of the following scores one point:
| SCORTEN component | Threshold |
|---|---|
| Age | Above 40 years |
| Malignancy | Present |
| Heart rate | Above 120 beats per minute |
| Initial detached body surface area | Above 10 per cent |
| Serum urea | Above 10 mmol per litre |
| Serum glucose | Above 14 mmol per litre |
| Serum bicarbonate | Below 20 mmol per litre |
| SCORTEN | Predicted mortality |
|---|---|
| 0 to 1 | About 3 per cent |
| 2 | About 12 per cent |
| 3 | About 35 per cent |
| 4 | About 58 per cent |
| 5 or more | Above 90 per cent |
Management: [1]
- Stop all suspected drugs immediately — especially those started in the preceding 1 to 8 weeks.
- Transfer to an ICU or specialist burns unit for extensive disease; the management is the same as for severe thermal burns — fluid resuscitation (using the burn formula), nutritional support, analgesia, infection surveillance and meticulous eye care (early ophthalmology review is mandatory to prevent synechiae and blindness).
- IVIG — historically used but now controversial; recent meta-analyses show no clear mortality benefit, and some guidelines have moved away from it.
- Corticosteroids — also controversial; short courses are used by some units early, but most contemporary practice avoids them in extensive disease because of the infection risk.
- Supportive and rehabilitative care — long-term sequelae include skin scarring, ocular damage (dry eye, corneal ulceration, blindness), urethral strictures and post-inflammatory hyperpigmentation. Avoid lifelong re-exposure. [1]
The discriminating question between DRESS and SJS/TEN: DRESS is eosinophilia and internal organ involvement with a morbilliform rash and facial oedema at 2 to 8 weeks; SJS/TEN is painful blistering, mucosal involvement and epidermal detachment [4][5].
Drug-induced agranulocytosis
Drug-induced agranulocytosis is a profound fall in neutrophil count (below 0.5 times ten to the ninth per litre) caused by immune-mediated or direct myelotoxic destruction of neutrophil precursors. The patient presents with fever and sore throat (the neutropenic sepsis presentation), and the diagnosis is made on an urgent full blood count [9].
The classical trigger list: [1]
| Drug class | Examples |
|---|---|
| Antithyroid drugs | Carbimazole, methimazole, propylthiouracil |
| Antipsychotics | Clozapine (cumulative incidence around 0.8 per cent at one year, peaking in the first 18 weeks; mandatory weekly to fortnightly FBC monitoring in most countries) [9] |
| Disease-modifying antirheumatic drugs | Sulfasalazine, methotrexate (usually myelosuppression rather than true agranulocytosis), leflunomide |
| Antibiotics | Co-trimoxazole (also causes thrombocytopenia), chloramphenicol (aplastic anaemia), linezolid |
| Chemotherapy and immunosuppressants | Most cytotoxic agents; also anti-CD20 and other biologics |
| Anti-epileptics (rare) | Carbamazepine, valproate |
The clozapine data are the best-characterised: in the United States Clozaril Patient Management System, the cumulative incidence of agranulocytosis was 0.80 per cent at one year and 0.91 per cent at 18 months, the risk rose with age and was higher in women, and 61 of 73 cases occurred in the first 18 weeks [9].
Management: [1]
- Stop the suspect drug immediately and do not re-challenge.
- Take cultures (blood, urine, throat, sputum, any line site) before starting antibiotics.
- Empirical broad-spectrum antibiotics per the local neutropenic sepsis protocol — typically an antipseudomonal beta-lactam (piperacillin-tazobactam, ceftazidime, or meropenem), with vancomycin added for suspected line infection, mucositis, or haemodynamic instability.
- G-CSF (filgrastim) is commonly used, especially in severe or prolonged neutropenia, to shorten the nadir.
- Reverse isolation and infection control precautions, with daily FBC monitoring.
- Document the reaction clearly; the patient must avoid the drug for life. [1]
Drug-induced thrombocytopenia — with heparin as the prototype
Drug-induced thrombocytopenia is separated into two mechanisms: myelosuppression (chemotherapy, linezolid, hydroxyurea) and immune-mediated destruction (HIT, quinine, vancomycin, abciximab, glycoprotein IIb/IIIa inhibitors). [1]
Heparin-induced thrombocytopenia (HIT) is the highest-yield member of this family because it is paradoxical — a fall in platelet count with a prothrombotic rather than a bleeding tendency — and because missing it is dangerous [7]. HIT is caused by IgG antibodies against the complex of platelet factor 4 (PF4) and heparin. The antibody activates platelets, producing both thrombocytopenia and a striking thrombotic tendency (venous and arterial, including limb gangrene and pulmonary embolism).
The classical diagnostic pattern: [1]
- The platelet count falls by 50 per cent or more from baseline.
- The fall occurs 5 to 14 days after first heparin exposure, or more rapidly (within 24 hours) if the patient has been exposed to heparin in the previous 30 to 100 days (the "rapid-onset HIT" of preformed antibody).
- The 4T score estimates pre-test probability: Thrombocytopenia, Timing, Thrombosis or other sequelae, and oTher cause of thrombocytopenia. A low 4T score (less than 3) effectively excludes HIT; a moderate or high score warrants stopping heparin and sending a PF4 antibody or serotonin release assay [7].
Management of suspected HIT: [1]
- Stop all heparin — including low-molecular-weight heparin, heparin flushes, and heparin-coated lines.
- Start an alternative non-heparin anticoagulant at a therapeutic dose — argatroban (hepatically cleared, preferred in renal failure), bivalirudin, danaparoid, fondaparinux, or a direct oral anticoagulant (rivaroxaban, apixaban) per local protocol.
- Do not give platelets unless life-threatening bleeding — they can fuel thrombosis.
- Confirm with laboratory testing — the PF4 enzyme immunoassay is the screening test; the serotonin release assay is the gold-standard functional test.
- Warfarin transition is delayed until the platelet count has recovered to at least 150, and is overlapped with the alternative anticoagulant because warfarin alone can cause skin necrosis in HIT. [1]
The non-HIT causes of drug-induced immune thrombocytopenia include quinine (the classic "cocktail and tonic water" cause, presenting with profound thrombocytopenia and bleeding), vancomycin, sulfonamides, abciximab, and the antimalarial and antiarrhythmic drugs. [1]
Drug-induced liver injury (DILI) and Hy's Law
DILI is divided into intrinsic (dose-dependent, predictable, the prototype is paracetamol hepatotoxicity) and idiosyncratic (dose-independent, unpredictable, the prototype is flucloxacillin and flutamide). The idiosyncratic form is the one that catches the physician [6].
The injury pattern is classified by the R-ratio (ALT divided by ALP, both as multiples of the upper limit of normal): hepatocellular (R above 5), cholestatic (R below 2), or mixed. The hepatocellular pattern is the more dangerous [6].
The high-yield trigger list for idiosyncratic DILI: [1]
| Pattern | Classic culprits |
|---|---|
| Hepatocellular | Isoniazid, rifampicin, pyrazinamide, diclofenac, nefazodone, ketoconazole, statins (rare but real), paracetamol (intrinsic at toxic dose), black cohosh |
| Cholestatic | Flucloxacillin (classic, especially in older patients), amoxicillin-clavulanate (the single commonest cause of DILI hospitalisation in many series), erythromycin, anabolic steroids, chlorpromazine, oral contraceptives |
| Mixed | Phenytoin, sulfonamides, tricyclics, carbamazepine, allopurinol (which may also produce DRESS) |
| Chronic | Nitrofurantoin (chronic active hepatitis), methyldopa, minocycline, amiodarone, methotrexate (fibrosis, see Type C) |
Hy's Law is the most important single rule in DILI. Named after Hyman Zimmerman, it predicts the lethality of a drug-induced hepatocellular injury. Hy's Law is present when all three of the following hold [6]:
- ALT or AST more than three times the upper limit of normal.
- Serum bilirubin more than two times the upper limit of normal, without significant cholestasis (ALP should be less than two times the upper limit of normal) and without an alternative explanation for the rise in bilirubin (such as haemolysis or Gilbert syndrome).
- No other cause — viral hepatitis, alcoholic hepatitis, ischaemic hepatitis ("shock liver"), biliary obstruction — that better explains the picture. [1]
The reason Hy's Law matters is that its presence carries a case fatality of around 10 per cent from acute liver failure. The FDA and EMA use Hy's Law as a stopping rule in drug development and in post-marketing surveillance: any drug that produces a Hy's Law case must be presumed to be capable of causing fatal hepatotoxicity until proven otherwise [6].
Management of DILI: [1]
- Stop the offending drug (and any hepatotoxic concomitant drugs) as soon as the diagnosis is suspected.
- Exclude alternative causes — viral hepatitis (A, B, C, E), EBV and CMV, autoimmune hepatitis, biliary obstruction (ultrasound and MRCP), ischaemic hepatitis, Wilson disease.
- Grade severity and consider liver transplantation for acute liver failure — the King's College criteria for paracetamol and non-paracetamol ALF apply (see the acute liver failure topic).
- N-acetylcysteine for paracetamol and, increasingly, for non-paracetamol acute liver failure.
- Corticosteroids for the immune-mediated variant (drug-induced autoimmune-like hepatitis, as seen with nitrofurantoin and minocycline).
- Report — DILI is among the commonest reasons a drug is withdrawn from the market. [1]
Drug-induced interstitial lung disease (DI-ILD)
DI-ILD is an inflammatory or fibrotic lung reaction caused by a drug. It is easily missed because the symptoms — progressive dyspnoea and dry cough — overlap with the underlying disease the drug was treating [8].
The high-yield trigger list: [1]
| Drug | Pattern of DI-ILD |
|---|---|
| Amiodarone | Chronic (Type C); interstitial pneumonitis, organising pneumonia, and rarely pulmonary fibrosis; related to cumulative dose and the drug's long half-life and phospholipid accumulation in type II pneumocytes |
| Methotrexate | Hypersensitivity pneumonitis (acute) or chronic fibrosis; can occur at any time during therapy; rule out infection |
| Nitrofurantoin | Acute (eosinophilic pneumonitis) or chronic pulmonary fibrosis; the chronic form is often irreversible |
| Bleomycin | Dose-related pulmonary fibrosis; the risk is higher with oxygen exposure, renal impairment and radiotherapy; oxygen should be used cautiously in patients with prior bleomycin |
| Checkpoint inhibitors (nivolumab, pembrolizumab, ipilimumab) | Pneumonitis at any time; immune-mediated; treated by holding the drug and giving corticosteroids (see the checkpoint inhibitor toxicity topic) |
| Other | Gold, penicillamine, sulfasalazine, hydralazine, amiodarone, busulfan, cyclophosphamide, methysergide, and many targeted anticancer agents |
The diagnosis is one of exclusion: the patient on an at-risk drug develops new respiratory symptoms, a high-resolution CT shows ground-glass, reticulation or consolidation that fits a drug pattern, and infection, heart failure and underlying disease progression have been ruled out. Bronchoalveolar lavage may show eosinophilia (nitrofurantoin, sulfasalazine) or lymphocytosis (methotrexate) but is not diagnostic [8].
Management: stop the drug, give corticosteroids for the inflammatory pattern (prednisolone 0.5 to 1 mg per kg per day tapering), and monitor with serial imaging and lung function. Fibrotic disease may not reverse. [1]
QT prolongation and torsade de pointes
QT prolongation is a Type A reaction (dose-dependent, pharmacological) that crosses into Type B territory when it is idiosyncratic or driven by an interaction. Drugs prolong the QT interval by blocking the delayed rectifier potassium current (I-Kr, the hERG channel). The risk is torsade de pointes, which can cause syncope, seizure or sudden death [10].
The high-yield trigger list: [1]
| Drug class | Examples |
|---|---|
| Antiarrhythmics (class IA and III) | Sotalol, amiodarone, quinidine, procainamide, disopyramide, ibutilide, dofetilide |
| Macrolides and fluoroquinolones | Erythromycin (especially IV), clarithromycin, moxifloxacin, ciprofloxacin (weaker) |
| Antipsychotics | Haloperidol (especially IV), droperidol, thioridazine, ziprasidone, and to a lesser extent olanzapine and quetiapine |
| Antidepressants | Citalopram and escitalopram (dose-related, the highest-risk SSRIs), and to a lesser extent the TCAs |
| Opioids | Methadone (dose-dependent, a common and under-recognised cause of sudden death) |
| Antifungals and antimalarials | Fluconazole, pentamidine, halofantrine |
| Antihistamines (older) | Terfenadine, astemizole (now largely withdrawn), diphenhydramine at high dose |
| GI motility (withdrawn or restricted) | Cisapride, domperidone at high dose |
| Antiemetics | Ondansetron (modest, higher IV), dolasetron |
The risk is multiplicative when two QT-prolonging drugs are combined, or when a QT-prolonging drug meets hypokalaemia, hypomagnesaemia, hypocalcaemia, bradycardia, structural heart disease, or female sex (women have a longer baseline QT and a higher torsade risk) [10].
The AHA/ACC scientific statement on preventing torsade in hospital settings recommends: identify patients with baseline QT prolongation or risk factors before prescribing a QT-prolonging drug; correct electrolytes (keep potassium above 4.0 mmol per litre and magnesium above 0.8 mmol per litre); avoid combinations; and monitor with serial ECGs, reducing the dose or stopping the drug if the QTc exceeds 500 ms or rises by more than 60 ms from baseline [10].
The exam trap: the patient on amiodarone who is given IV erythromycin for community-acquired pneumonia, or the patient on methadone who develops vomiting and hypokalaemia. Either may torsade. [1]
Serotonin syndrome, NMS, and the pharmacological fever syndromes
These are covered in the dedicated topic. From the ADR perspective, serotonin syndrome is a Type A reaction (excess serotonergic activity, dose-dependent on the combination, predictable from the pharmacology) and NMS is closer to Type B (idiosyncratic response to dopamine blockade, not simply dose-related) [12]. The key ADR principle: both are diagnosed clinically, both require stopping the offending agent, and both are reported.
Type C, Type D, Type E and Type F — the reactions that are missed because they are slow or paradoxical
Type C — cumulative-dose and cumulative-time reactions
The exam favourite here is bisphosphonate osteonecrosis of the jaw, which is related to cumulative dose and is commoner with the IV bisphosphonates (zoledronate, pamidronate) used in oncology than with the oral agents used for osteoporosis. Patients present with exposed, non-healing mandibular or maxillary bone; prevention is good dental hygiene and dental review before starting therapy. [1]
Other Type C examples: methotrexate hepatic fibrosis (monitored with fibroscan or liver biopsy after a cumulative dose of around 1.5 g, with routine monitoring of AST, ALT and albumin every few months); amiodarone pulmonary and thyroid toxicity (the drug's phospholipid accumulation produces chronic interstitial pneumonitis and both hyper- and hypothyroidism; baseline and 6-monthly lung function and thyroid function are standard); analgesic nephropathy (chronic combination analgesic use causing papillary necrosis and chronic kidney disease); and ergotamine-induced valvular heart disease (now rare). [1]
Type D — delayed reactions, including teratogenesis and carcinogenesis
The classic examples are thalidomide phocomelia (the disaster that created modern pharmacovigilance), isotretinoin teratogenesis (mandating pregnancy prevention programmes and iPLEDGE-style registries), diethylstilboestrol and clear-cell vaginal adenocarcinoma in daughters of women who took it in pregnancy, and cyclophosphamide and bladder cancer (prevented by aggressive hydration and the use of mesna). [1]
Type E — end-of-treatment (withdrawal) syndromes
These are misdiagnosed as deterioration of the underlying disease. The high-yield examples: [1]
| Withdrawal syndrome | Drug stopped | Presentation |
|---|---|---|
| Adrenal crisis | Long-term systemic corticosteroids | Hypotension, hyponatraemia, hyperkalaemia, fatigue, nausea; the HPA axis takes months to a year to recover |
| Opiate withdrawal | Opioids (prescribed or illicit) | Agitation, mydriasis, piloerection, lacrimation, rhinorrhoea, diarrhoea, yawning, muscle cramps; clonidine or methadone/buprenorphine for symptom control |
| Benzodiazepine withdrawal | Benzodiazepines | Anxiety, insomnia, tremor, perceptual disturbance, and in severe cases seizures; managed by a slow taper over weeks to months |
| Clonidine rebound hypertension | Clonidine | Severe hypertension, tachycardia, diaphoresis within 24 to 48 hours of stopping; managed by restarting and tapering |
| Beta-blocker rebound | Beta-blockers | Tachycardia, angina, and in patients with ischaemic heart disease, myocardial infarction; never stop suddenly |
| SSRI discontinuation syndrome | SSRIs (especially paroxetine and venlafaxine with short half-lives) | Dizziness, electric-shock sensations, nausea, anxiety; managed by restarting and tapering slowly or switching to fluoxetine |
The exam principle: a patient on long-term steroids who becomes unwell with hypotension and hyponatraemia has adrenal suppression until proven otherwise, and must be treated empirically with hydrocortisone [1].
Type F — treatment failure
Type F is the most easily missed because the patient "just does not get better." The classic examples are oral contraceptive failure with enzyme inducers (rifampicin, rifabutin, certain anticonvulsants, St John's wort) and (less certainly) broad-spectrum antibiotics, and warfarin failure with concurrent vitamin K (including from nutritional supplements or enteral feeds) or cholestyramine (which binds warfarin in the gut). Always think of Type F when a previously well-controlled drug suddenly stops working — the answer is often a new drug interaction [1].
ADRs in special populations — the long-case perspective
The older patient
Older patients have the highest ADR burden because of polypharmacy, altered pharmacokinetics (reduced renal clearance with a preserved serum creatinine from low muscle mass, reduced hepatic mass and phase I metabolism, increased body fat prolonging the half-life of lipophilic drugs), and altered pharmacodynamics (increased sensitivity to CNS depressants, anticholinergics, anticoagulants and volume-active drugs). The Pirmohamed data and the systematic review by Kongkaew both show the ADR burden rises steeply with age and number of medications [2][11]. The prevention tools — STOPP/START, the AGS Beers Criteria, medication reconciliation and deprescribing — are covered in the polypharmacy topic.
The patient with renal or hepatic impairment
Renal and hepatic impairment change drug clearance and therefore shift the dose–response curve toward Type A reactions. The pharmacokinetics topic covers the dose-adjustment rules. From the ADR perspective: always recalculate the dose of renally cleared drugs (digoxin, gabapentin, pregabalin, allopurinol, the direct oral anticoagulants, low-molecular-weight heparin, metformin, many antibiotics) in CKD, and avoid hepatotoxic combinations in liver disease. [1]
The patient at risk of pharmacogenomic ADRs
The clinically actionable pharmacogenomic associations are HLA-B1502 (carbamazepine SJS/TEN, Han Chinese and Southeast Asian), HLA-B5801 (allopurinol SJS/TEN, Han Chinese, Thai, Korean), HLA-B5701 (abacavir hypersensitivity, all populations — screen before starting abacavir), HLA-A3101 (carbamazepine DRESS and SJS in Europeans and Japanese), and the TPMT and NUDT15 polymorphisms (thiopurine myelosuppression — screen before starting azathioprine or 6-mercaptopurine). In ANZ practice these screens are increasingly standard of care in the relevant populations [1][4].
ADR prevention — the systems-level interventions
Prevention operates at three levels: [1]
- At the point of prescribing — medication reconciliation at every care transition (admission, transfer, discharge), application of the AGS Beers Criteria and STOPP/START in older patients, dose adjustment for renal and hepatic function, and explicit checking for drug–drug interactions (the QT-prolonging and serotonergic combinations are the highest-yield).
- At the point of monitoring — FBC monitoring for clozapine, sulfasalazine and carbimazole; LFT and creatinine monitoring for methotrexate, isoniazid and statins; INR monitoring for warfarin; lung function and thyroid function for amiodarone.
- At the point of detection and reporting — every severe or previously unrecognised reaction should be reported to the TGA (Blue Card in Australia) or through the MHRA Yellow Card scheme in the UK. Spontaneous reporting is the cornerstone of pharmacovigilance; signal detection relies on it, and the system fails when physicians do not report [1].
The Australian Commission on Safety and Quality in Health Care's Medication Safety Standard and the World Health Organization's Global Patient Safety Challenge (Medication Without Harm) both frame ADR reduction as a system-level responsibility, not just an individual prescriber's job. [1]
ADR reporting — the Yellow Card and Blue Card
Pharmacovigilance is the science of detecting, assessing and preventing ADRs after marketing, and it depends on clinician reporting. The key principles [1]:
- In Australia, report to the Therapeutic Goods Administration (TGA) via the Blue Card system (now online). Report all suspected reactions to new drugs (those with the "black triangle"), all serious reactions regardless of drug age, and any unexpected reaction of clinical interest.
- In the United Kingdom, report to the MHRA through the Yellow Card scheme (online or via the app). The same rules apply — black triangle drugs and serious reactions.
- In the United States, the FDA MedWatch programme.
- A reaction is serious if it is fatal, life-threatening, requires or prolongs hospitalisation, causes persistent or significant disability, or is a congenital anomaly. [1]
Reporting is voluntary (except for marketed drugs in some jurisdictions) and you do not need certainty — a suspicion is enough. Causality is assessed centrally using tools including the Naranjo scale [3].
Differential diagnosis — what else looks like an ADR
When a patient deteriorates on a drug, the differential is wide. The structured approach is: [1]
| Pattern | ADR possibility | Also consider |
|---|---|---|
| New rash plus fever | DRESS, SJS/TEN, drug hypersensitivity | Viral exanthem (EBV, CMV, measles), sepsis, connective tissue disease, Kawasaki disease (in children) |
| Acute transaminitis | DILI | Viral hepatitis, ischaemic hepatitis, biliary obstruction, autoimmune hepatitis, alcoholic hepatitis |
| Acute thrombocytopenia | HIT, quinine, vancomycin | ITP, sepsis, DIC, TTP/HUS, leukaiaemic infiltration, hypersplenism |
| Acute neutropenia with fever | Drug-induced agranulocytosis | Sepsis-related margination, viral marrow suppression, leukaemia, aplastic anaemia |
| Acute dyspnoea with infiltrates | DI-ILD | Pneumonia (including opportunistic), pulmonary oedema, pulmonary embolism, disease progression |
| Acute AKI | Drug-induced interstitial nephritis, NSAID haemodynamics, ACE inhibitor | Sepsis, hypovolaemia, obstruction, acute tubular necrosis, glomerulonephritis |
| QT prolongation with syncope | Drug-induced torsade | Congenital long QT, ischaemia, electrolyte disturbance independent of drugs |
The single most powerful discriminator in every case is the medication history: a new drug in the relevant time window raises the probability of an ADR enormously. Take a full history including over-the-counter drugs, herbal and complementary medicines (St John's wort, black cohosh, kava), and recreational drugs [1].
Investigations — the ADR work-up
The work-up is tailored to the suspected reaction, but the core set is: [1]
- Full blood count with differential — eosinophilia for DRESS, neutropenia for agranulocytosis, thrombocytopenia for HIT and quinine.
- Liver function tests — for DILI; apply Hy's Law if ALT above three times ULN and bilirubin above two times ULN.
- Renal function and electrolytes — for interstitial nephritis, ACE-inhibitor AKI, and to correct the hypokalaemia and hypomagnesaemia that drive torsade.
- C-reactive protein and blood cultures — to distinguish ADR fever from sepsis (which may coexist).
- ECG — for QT prolongation; measure the QTc (Bazett or Fridericia correction).
- Chest X-ray and high-resolution CT — for DI-ILD.
- Viral serology — hepatitis A, B, C, E, EBV, CMV, HIV — to exclude alternative causes of hepatitis.
- Drug-specific assays where available — paracetamol level, tryptase (for anaphylaxis and mast-cell activation), PF4 antibody and serotonin release assay for HIT.
- Skin biopsy — for SJS/TEN (shows full-thickness epidermal necrosis) and for DRESS (lymphocytic infiltrate with eosinophils); biopsy is not always needed when the clinical picture is clear. [1]
Communication and shared decision-making
When you identify an ADR, the communication is as important as the diagnosis. Three points: [1]
- Tell the patient what happened, in plain language — "the antibiotic caused your liver inflammation, and we have stopped it; you must not take it again."
- Document the reaction clearly in the medication record and the allergy/adverse-reaction field — name the drug, the reaction, the date, and the severity. An entry of "allergy" without the reaction is a common source of future error.
- Report it to the TGA or MHRA, and tell the patient you have done so — it gives the event a purpose and supports future patients. [1]
The shared decision is about the next drug: if a patient has had DRESS to phenytoin, they cannot take carbamazepine, phenobarbital or lamotrigine (cross-reactivity among the aromatic anticonvulsants), and the choice of an alternative (levetiracetam, sodium valproate, or a non-pharmacological option) must be made jointly with the patient, weighing the risk of recurrence of their underlying disease against the risk of a new ADR. [1]
Long-term outcomes and follow-up
The outcomes depend on the reaction: [1]
- Type A — usually resolve fully on dose reduction or withdrawal.
- DRESS — relapses are common in the first weeks; mortality around 5 to 10 per cent, usually from liver failure; long-term autoimmune sequelae (autoimmune hepatitis, thyroiditis, diabetes) are described [4].
- SJS/TEN — mortality 10 to 30 per cent; long-term sequelae include ocular damage, skin scarring, urethral strictures, and post-inflammatory hyper- or hypopigmentation; quality of life is often severely impaired.
- Drug-induced agranulocytosis — mortality around 5 to 10 per cent without prompt antibiotics; with rapid recognition and G-CSF, most patients recover in one to two weeks [9].
- HIT — the thrombotic risk persists for weeks; the condition is the prototype of a drug reaction that paradoxically anticoagulates the patient's drug management for months [7].
- DILI — most idiosyncratic DILI resolves on withdrawal, but 5 to 10 per cent progress to acute liver failure and transplantation; chronic DILI can mimic chronic hepatitis.
- DI-ILD — inflammatory patterns usually respond to steroids and drug withdrawal; fibrotic patterns (bleomycin, chronic nitrofurantoin) may be irreversible.
Follow-up is lifelong in the sense that the patient must never be re-exposed to the culprit, and the reaction must be recorded in every future medication review. [1]
High-yield exam traps and discriminators
- A 38-year-old man started on phenytoin four weeks ago presents with fever, rash, facial oedema, eosinophilia and hepatitis. This is DRESS, not simple urticaria. Stop the phenytoin, avoid all aromatic anticonvulsants, give corticosteroids for visceral involvement, and report.
- A 68-year-old woman on allopurinol (started at too high a dose for her CKD) presents with blistering, oral mucosal involvement and epidermal detachment. This is SJS/TEN, not DRESS. Stop all drugs, calculate SCORTEN, transfer to a burns unit.
- A 55-year-old woman on warfarin for atrial fibrillation develops a painful, blistering rash on her leg with a rising INR. This is warfarin-induced skin necrosis, a rare reaction in the first week of therapy caused by microvascular thrombosis from protein C depletion; stop the warfarin, give vitamin K and heparin (after excluding HIT), and look for protein C or S deficiency.
- A 72-year-old man five days into heparin for a pulmonary embolism has a platelet count that has fallen from 280 to 110, and new femoral deep vein thrombosis. This is HIT. Stop the heparin, start argatroban or fondaparinux, send a PF4 antibody, do not give platelets.
- A 60-year-old woman on amiodarone and methadone is admitted with syncope; the ECG shows QTc of 560 ms. This is drug-induced QT prolongation with torsade; give IV magnesium, correct potassium, stop both drugs, and avoid all QT-prolonging agents thereafter.
- A 65-year-old man three weeks into anti-tubercular therapy (isoniazid, rifampicin, pyrazinamide) has ALT 420 U per litre (ULN 40) and bilirubin 52 micromol per litre (ULN 20) with no other cause. This is Hy's Law. Stop the anti-tubercular drugs, re-introduce sequentially when the LFTs recover, and consider liver transplantation if acute liver failure develops.
- An 80-year-old woman on long-term prednisolone for polymyalgia rheumatica is admitted with hypotension, hyponatraemia and hyperkalaemia after a gastrointestinal illness. This is adrenal suppression (Type E). Give empirical hydrocortisone 100 mg IV and fluid, do not wait for the cortisol level.
- A 42-year-old woman on the oral contraceptive pill started on rifampicin for tuberculosis becomes pregnant. This is Type F (treatment failure) from an enzyme-inducing interaction. Counsel on barrier contraception for the duration of rifampicin therapy. [1]
Summary — the consultant's five rules
- Every unexplained symptom in a patient on medications is an ADR until proven otherwise. Take a complete drug history, including over-the-counter and herbal medicines.
- Classify the reaction with ABCDEF. Dose-dependent and common is Type A; bizarre and rare is Type B; cumulative is Type C; delayed is Type D; withdrawal is Type E; failure is Type F [1].
- Stop the offending drug. Reduce the dose or stop for Type A; stop permanently and never re-challenge for severe Type B; reinstate the missing agent for Type E.
- Recognise the severe Type B reactions early — DRESS, SJS/TEN, agranulocytosis, HIT, severe DILI with Hy's Law, DI-ILD and torsade are the ones that kill [4][5][6][7][8][9][10].
- Report every severe or unexpected ADR to the TGA or MHRA. Pharmacovigilance depends on you [1].
References
- [1]Edwards IR, Aronson JK Adverse drug reactions: definitions, diagnosis, and management Lancet, 2000.PMID 11072960
- [2]Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients BMJ, 2004.PMID 15231615
- [3]Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions Clin Pharmacol Ther, 1981.PMID 7249508
- [4]Cacoub P, Musette P, Descamps V, et al. The DRESS syndrome: a literature review Am J Med, 2011.PMID 21592453
- [5]Bastuji-Garin S, Fouchard N, Bertocchi M, et al. SCORTEN: a severity-of-illness score for toxic epidermal necrolysis J Invest Dermatol, 2000.PMID 10951229
- [6]Hoofnagle JH, Bjornsson ES Drug-Induced Liver Injury - Types and Phenotypes N Engl J Med, 2019.PMID 31314970
- [7]Greinacher A CLINICAL PRACTICE. Heparin-Induced Thrombocytopenia N Engl J Med, 2015.PMID 26176382
- [8]Schwaiblmair M, Behr W, Haeckel T, et al. Drug induced interstitial lung disease Open Respir Med J, 2012.PMID 22896776
- [9]Alvir JM, Lieberman JA, Safferman AZ, et al. Clozapine-induced agranulocytosis. Incidence and risk factors in the United States N Engl J Med, 1993.PMID 8515788
- [10]Drew BJ, Ackerman MJ, Funk M, et al. Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation Circulation, 2010.PMID 20142454
- [11]Kongkaew C, Noyce PR, Ashcroft DM Hospital admissions associated with adverse drug reactions: a systematic review of prospective observational studies Ann Pharmacother, 2008.PMID 18594048
- [12]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664