Phys · pharmacological
Beta Blocker AND Calcium Channel Blocker Toxicity
Also known as Beta Blocker AND Calcium Channel Blocker Toxicity · beta blocker and calcium channel blocker toxicity
Consultant-physician depth guide to Beta Blocker AND Calcium Channel Blocker Toxicity for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
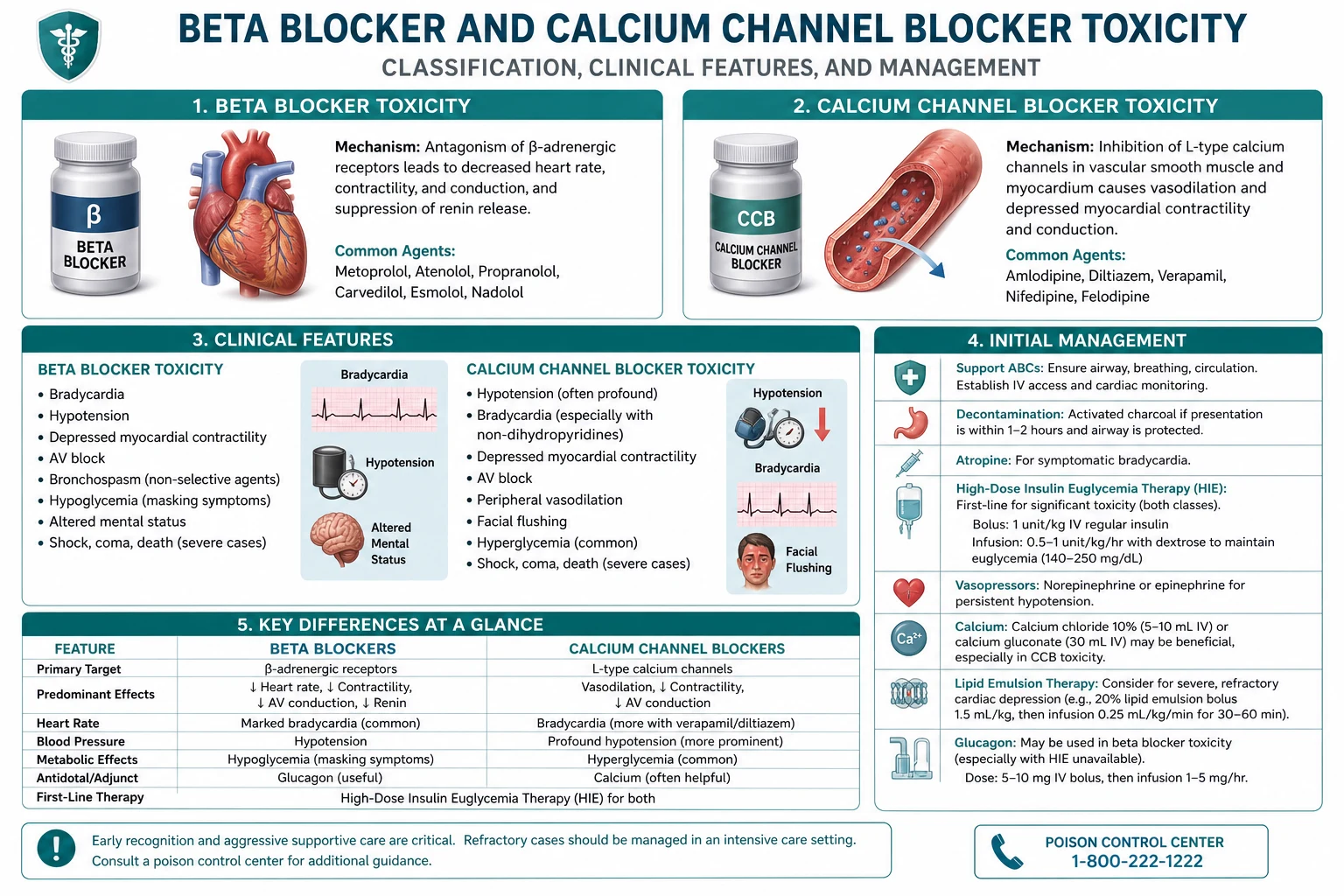
Beta Blocker AND Calcium Channel Blocker Toxicity is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
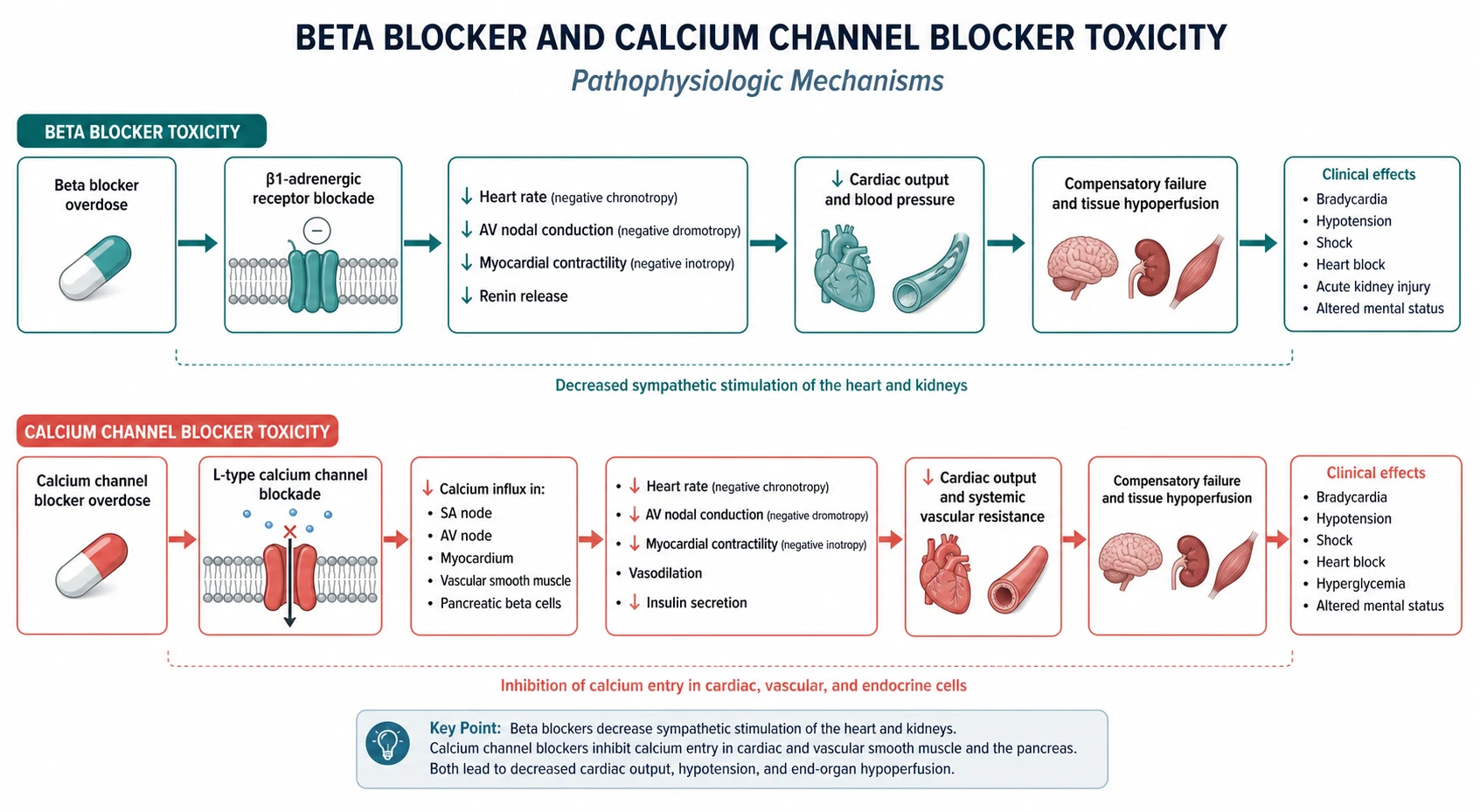
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
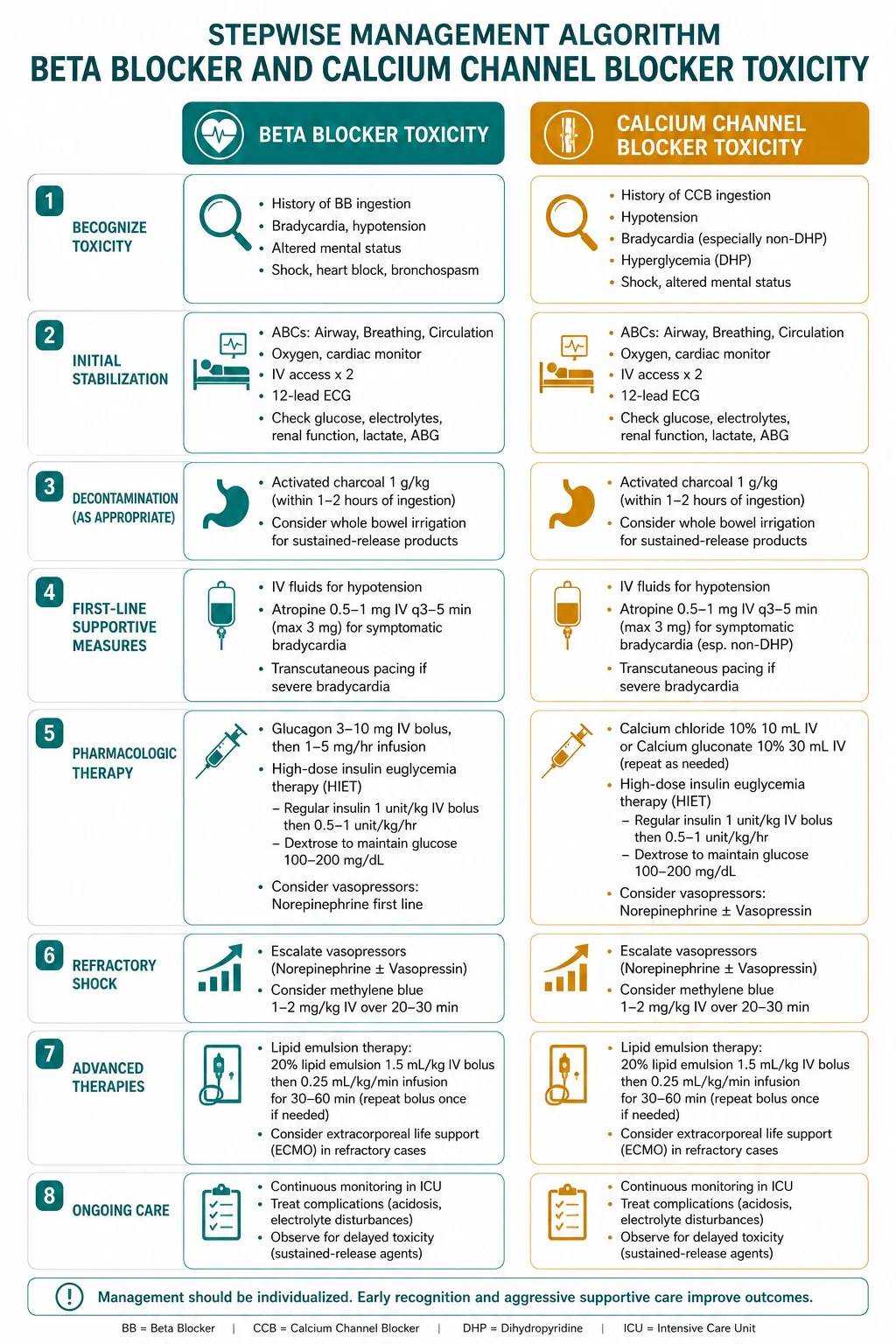
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]
Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Beta Blocker AND Calcium Channel Blocker Toxicity to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Meamar R, Samsamshariat S, Dorvashi G, Feizi A, et al. Intravenous Lipid Emulsion in Beta-Blocker With or Without Calcium Channel Blocker Toxicity: A Systematic Review of Human Case Reports and Series J Appl Toxicol, 2026.PMID 42365995
- [2]Justin A, Manisha C, Banerjee S, Venu G, et al. Navigating the maze of Alzheimer's: nimodipine and pioglitazone combination in the spotlight through inhibition of P2X7 dependent NLRP3 inflammasome activation Inflammopharmacology, 2026.PMID 41984340
- [3]Suarez F, Koyfman A, Long B Pearls and Pitfalls for the Emergency Clinician: Beta Blocker and Calcium Channel Blocker Toxicity J Emerg Med, 2026.PMID 41833262
- [4]Lavonas EJ, Akpunonu PD, Arens AM, Babu KM, et al. 2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation, 2023.PMID 37721023
- [5]Lindeman E, Baer Eriksson L, Thorsson M, Nordmark Grass J [High dose insulin euglycemia therapy – an important addition to the treatment arsenal in severe toxic myocardial depression] Lakartidningen, 2017.PMID 28994852
- [6]Darracq MA, Thornton SL, Do HM, Bok D, et al. Utilization of hyperinsulinemia euglycemia and intravenous fat emulsion following poison center recommendations J Med Toxicol, 2013.PMID 23412936
- [7]Doan HN, Chang MC Comparative Effectiveness of Unstable Versus Stable Resistance Training on Lower Limb Strength, Mobility, and Fear of Falling in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials Am J Phys Med Rehabil, 2026.PMID 42468010
- [8]Liu HW, Tsai TL Virtual Reality-assisted Physiotherapeutic Training for Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis Am J Phys Med Rehabil, 2026.PMID 42468005
- [9]Osborne AK, Brown RD, Sillence E Effects of Social Media Narratives on Affective and Behavioral Responses to Menopause Content: Randomized Online Experimental Study JMIR Form Res, 2026.PMID 42467962
- [10]Ouwerkerk JJJ, Poublon NA, Westra AF, Kraaijvanger N VA-ECMO and HIET for toxic cardiogenic shock in an elderly patient following severe poly-intoxication: A case report Toxicol Rep, 2026.PMID 42434173
- [11]Tomar N, Vennela AT, Mukhopadhyay S, Kondapi AK Targeted nano delivery of p53 DNA and carvedilol for the treatment of dilated cardiomyopathy in a rat model Nanomedicine (Lond), 2026.PMID 41738451
- [12]Sterpi AE, Theodorou A, Keramida A, Papagiannopoulou G, et al. Blood Pressure Control With Clevidipine Is Associated With Hematoma Volume Reduction in Acute Hypertensive Intracerebral Hemorrhage: A Single-Center Prospective Cohort Study Eur J Neurol, 2026.PMID 42397158