Phys · pharmacological
Australian Envenomation — Snake, Spider and Marine
Also known as snake bite · snake envenomation · venom-induced consumption coagulopathy · VICC · Australian elapid envenomation · brown snake bite · tiger snake bite · funnel-web spider bite · red-back spider bite · box jellyfish sting · latrodectism · pressure immobilisation bandage
Consultant-physician-depth guide to Australian envenomation — the five major elapid snake groups (brown, tiger, taipan, death adder, black snake) and their clinical syndromes (neurotoxic, venom-induced consumption coagulopathy, myotoxic, renal, cardiovascular collapse), the pressure immobilisation bandage as first aid, the Snake Venom Detection Kit, monovalent and polyvalent antivenom selection and dosing, the critical VICC-versus-DIC distinction, funnel-web and red-back spider envenomation, and marine envenomation (box jellyfish, blue-ringed octopus, stonefish, sea snake). Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Australian Envenomation — Snake, Spider and Marine

The answer first
Australia is home to the most venomous snakes in the world. Of the 140 terrestrial snake species, about 100 are venomous and the top five medically important groups are all elapids — the brown snake, tiger snake, taipan, death adder and black snake. Brown snakes cause the most deaths (approximately two per year nationally) because they are widespread, fast-moving, and their venom produces a coagulopathy that can kill within hours if a head injury accompanies the collapse [1].
Three rules govern everything that follows: [1]
-
First aid is the pressure immobilisation bandage (PBI). It retards lymphatic spread of venom, which is how elapids cause systemic effects. Applied early and correctly, it buys hours. Sutherland proved this in 1979 and it remains the foundation of Australian snakebite management [8][9].
-
VICC is not DIC. The venom-induced consumption coagulopathy looks terrifying on the bloods — an INR above 10 and undetectable fibrinogen — but it is a toxin-driven defibrination, not a disseminated intravascular process. There are no microthrombi, no end-organ damage from thrombosis, and the coagulopathy is self-limiting once the venom is neutralised [4][5].
-
Antivenom is monovalent, one vial, guided by the SVDK. The Australian Snakebite Project (ASP-20) showed that the median antivenom dose fell from four vials to one over a decade with no change in outcomes — one vial of the correct monovalent antivenom is the standard [1][2].
DCE trap: In every snake bite long case, state the syndrome first — "this is a VICC-dominant envenomation consistent with a brown snake" — because the syndrome drives the antivenom choice, the monitoring plan, and the complications you must watch for. The snake identity matters, but the syndrome matters more. [1]
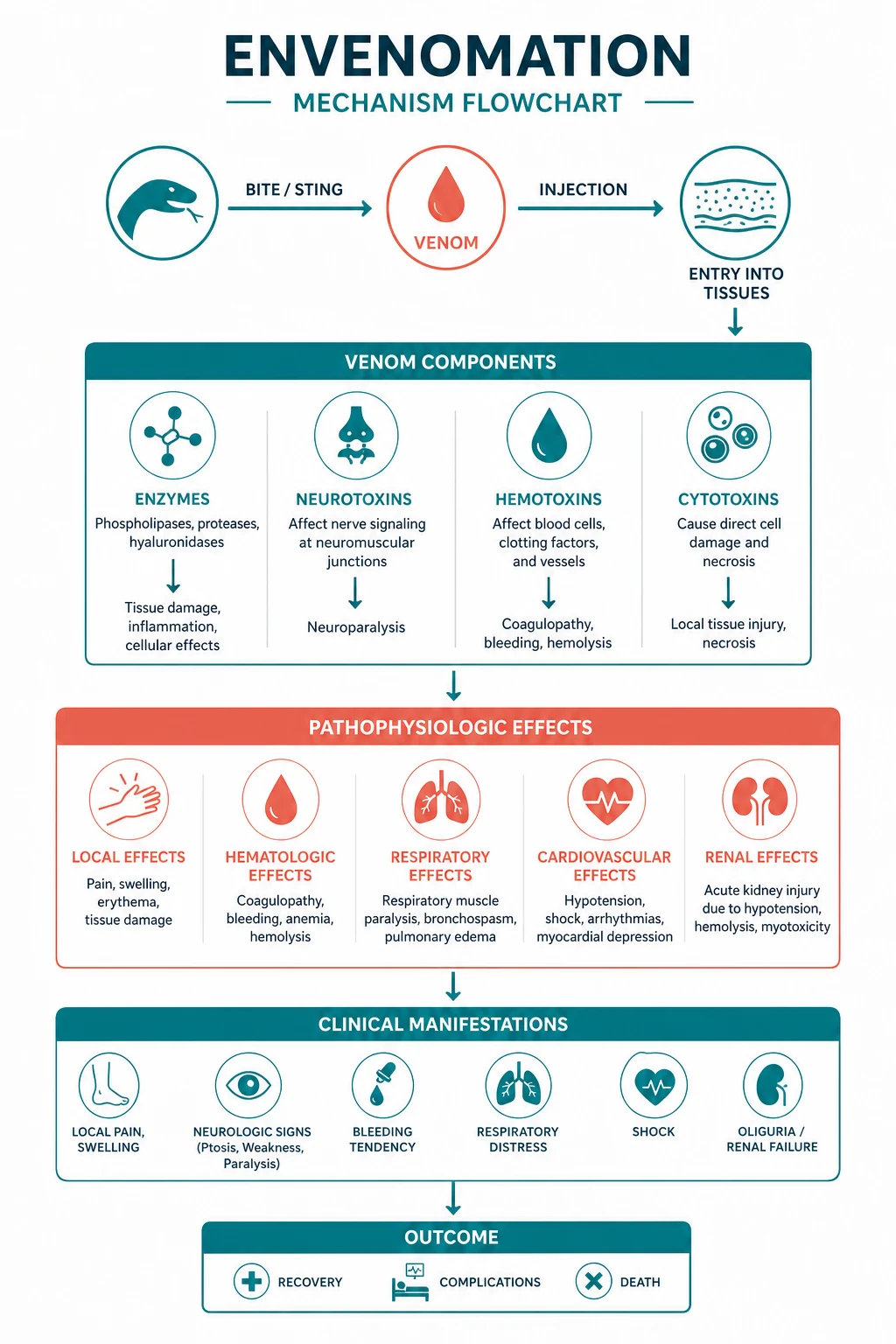
The five major clinical syndromes

Australian elapids produce venom that acts on five target systems. A single snake may produce several syndromes, but each species has a dominant pattern that tells you which snake it is and what to watch for [1][2].
| Syndrome | Mechanism | Clinical features | Classic snakes |
|---|---|---|---|
| Neurotoxicity | Presynaptic PLA2 or postsynaptic alpha-neurotoxin | Ptosis, ophthalmoplegia, bulbar palsy, respiratory paralysis | Death adder (postsynaptic), tiger snake (presynaptic), taipan (presynaptic) |
| VICC (haemotoxic) | Prothrombin activator causes defibrination | INR above 10, undetectable fibrinogen, extreme D-dimer, possible bleeding | Brown snake (most common), tiger snake, taipan, black snake |
| Myotoxicity | PLA2 myotoxin destroys skeletal muscle | CK above 10 000 U/L, myoglobinuria, muscle pain, AKI | Sea snake, mulga (king brown) snake, tiger snake |
| Nephrotoxicity | Direct venom effect or pigment nephropathy | AKI, rising creatinine, oliguria | Brown snake (via TMA), tiger snake (via rhabdomyolysis), sea snake |
| Cardiovascular collapse | Anaphylactoid reaction or direct cardiotoxicity | Early hypotension, cardiac arrest | Brown snake (5 per cent cardiac arrest), box jellyfish |
DWE high-yield: The syndrome, not the snake name, is what you treat. Brown snake equals VICC plus possible collapse and TMA. Tiger snake equals VICC plus neurotoxicity plus possible rhabdomyolysis. Death adder equals pure neurotoxicity with NO VICC. These three pairings answer most DWE snakebite questions. [1]
The five elapid groups in detail
Brown snake (Pseudonaja species) — the killer
The brown snake is responsible for most snakebite deaths in Australia. It is fast-moving, widespread across the mainland, and its venom is dominated by a Group C prothrombin activator called pseutarin C, which directly activates prothrombin to thrombin independent of the normal coagulation cascade [2].
The clinical picture of brown snake envenomation has four pillars from the ASP-14 study of 149 patients [2]:
- VICC — universal. Every envenomed patient develops VICC. The INR becomes unrecordable (above 10), fibrinogen is undetectable and D-dimer is extreme. The defibrination occurs within 1 to 2 hours of the bite.
- Collapse or hypotension — in one-third. The patient may collapse at the scene, sometimes with a brief loss of consciousness. Cardiac arrest occurs in approximately 5 per cent.
- Thrombotic microangiopathy (TMA) — in 10 per cent. A triad of thrombocytopenia, microangiopathic haemolytic anaemia (schistocytes on the blood film) and AKI [3]. This resembles atypical HUS and is managed supportively.
- Neurotoxicity — rare and mild. Despite containing neurotoxins, brown snake envenomation rarely produces clinically significant neurotoxicity in humans. At most, a mild ptosis or diplopia. This is the key discriminator from tiger snake.
DWE rule: If the question describes a patient with an unrecordable INR, undetectable fibrinogen and no neurotoxicity, the answer is brown snake. If it adds neurotoxicity (ptosis, ophthalmoplegia), the answer is tiger snake. [1]
Tiger snake (Notechis species) — VICC plus neurotoxicity
The tiger snake produces VICC through its prothrombin activator (oscutarin C) AND neurotoxicity through a presynaptic PLA2 neurotoxin called notexin. It also produces myotoxicity in some cases. The combination of coagulopathy and neurotoxicity is the clinical signature. [1]
The neurotoxicity is presynaptic — notexin destroys the nerve terminal membrane. This means antivenom prevents further damage but cannot reverse established paralysis, because the terminal must regenerate (which takes days). The patient may need ventilation even after adequate antivenom [6].
Tiger snake VICC is biochemically identical to brown snake VICC — undetectable fibrinogen, unrecordable INR, extreme D-dimer. The difference is the neurological examination. [1]
Taipan (Oxyuranus species) — the most venomous
The inland taipan has the most toxic venom of any land snake, but the coastal taipan causes most bites. The venom contains a powerful prothrombin activator (trocarin D) and a presynaptic neurotoxin (taipoxin), producing VICC and neurotoxicity similar to the tiger snake but often more severe. Taipan bites are medical emergencies — the patient can deteriorate within 30 minutes. [1]
Death adder (Acanthophis species) — pure neurotoxicity
The death adder is unique among Australian elapids because its venom is a postsynaptic alpha-neurotoxin that binds the nicotinic acetylcholine receptor at the neuromuscular junction. It produces a pure flaccid paralysis — ptosis, external ophthalmoplegia, facial diplegia, bulbar palsy, progressive limb weakness and respiratory failure — WITHOUT VICC and WITHOUT myotoxicity [1].
Because the block is postsynaptic, it is reversible. Antivenom displaces the toxin from the receptor, and a trial of neostigmine (with glycopyrrolate) can partially reverse the paralysis as a temporising measure while antivenom takes effect. [1]
DWE discriminator: A snake bite with descending flaccid paralysis and normal coagulation is a death adder. The postsynaptic block means neostigmine works and antivenom reverses it — unlike tiger snake or taipan neurotoxicity, which is presynaptic and irreversible once established. [1]
Black snake (Pseudechis species) — myotoxic
The mulga snake (king brown, Pseudechis australis) and the red-bellied black snake (Pseudechis porphyriacus) produce a myotoxic venom. The mulga snake causes significant rhabdomyolysis with CK above 10 000 U/L, myoglobinuria and AKI. It also causes a mild anticoagulant coagulopathy (from a phospholipase that interferes with the clotting assay) but NOT true VICC. The red-bellied black snake causes a milder illness with local pain, swelling and mild systemic features. [1]
VICC — the coagulopathy that looks like DIC but is not
The mechanism
VICC is the most important syndrome to understand because it is the most common and the most biochemically alarming. The mechanism is tight [4][5]:
- The venom contains a prothrombin activator — a protease that directly converts prothrombin to thrombin, bypassing the entire intrinsic and extrinsic coagulation cascade.
- The massive thrombin burst converts fibrinogen to fibrin throughout the circulation.
- The fibrin is immediately lysed by plasmin (secondary fibrinolysis), producing fibrin degradation products and an extreme D-dimer.
- The net result is consumption of fibrinogen, prothrombin and factors V, VIII and XIII — a defibrination syndrome. [1]
The blood picture is: INR unrecordable (above 10), aPTT unrecordable, fibrinogen undetectable (below 0.1 g/L), D-dimer extreme (above 10 to 100 micrograms per millilitre), and platelet count variable (may be normal early, may fall if TMA develops). [1]
Why VICC is not DIC
| Feature | VICC | DIC |
|---|---|---|
| Trigger | Snake venom (prothrombin activator) | Sepsis, malignancy, obstetric catastrophe, trauma |
| Microthrombi | NO | YES — causing renal, hepatic, cerebral, digital ischaemia |
| End-organ damage from thrombosis | NO | YES |
| Platelets | Variable (may be normal) | Low and falling |
| Fibrinogen | Undetectable | Low |
| D-dimer | Extreme | High |
| Management | Antivenom plus supportive (FFP if bleeding) | Treat the trigger, blood products, no heparin in most cases |
| Course | Self-limiting over 12 to 24 hours once venom neutralised | Depends on the underlying condition |
Isbister has argued consistently that the term "VICC" should replace the misleading label "snakebite DIC" because the two conditions have different mechanisms, different management and different prognoses [4].
DCE trap: If an examiner says "this patient has DIC from a snake bite," correct them — it is VICC, not DIC. This distinction is a consultant-level insight that earns marks. The mechanism is direct prothrombin activation, not a disseminated intravascular process. [1]
Recovery
VICC recovers spontaneously. The liver resynthesises fibrinogen over 6 to 12 hours and the other factors over 12 to 24 hours. The INR begins to fall within hours of antivenom and is usually below 2 within 24 hours. The D-dimer may remain elevated for days. The ASP prospective study confirmed that recovery follows a predictable time course regardless of whether antivenom accelerates it — antivenom prevents ongoing consumption but does not reverse the established deficit [6].
First aid — the pressure immobilisation bandage

The PBI is the single most important pre-hospital intervention for Australian elapid snakebite. Sutherland introduced it in 1979 based on animal studies showing that firm pressure on a bandaged limb retards lymphatic flow, which is how elapid venom spreads systemically [8]. The technique [9][10]:
- Do not move the patient. Keep them still and supine.
- Apply a broad crepe bandage over the bite site first, then bandage the entire limb from the fingers or toes proximally to the groin or armpit. The pressure should be similar to a compression bandage for a sprained ankle — firm enough to indent the tissue but not to occlude arterial flow (approximately 50 to 70 mmHg).
- Immobilise the limb with a splint. The bandage alone is insufficient — muscle movement pumps lymphatic fluid. The limb must be still.
- Do NOT remove the bandage until antivenom is ready in hospital. Removing it releases the trapped venom as a systemic bolus, which can precipitate collapse or VICC.
- Do NOT wash the bite site, cut it, suck it, or apply a tourniquet. Washing removes venom that the SVDK needs to detect. A tourniquet causes ischaemia and a venom surge on release. [1]
DWE rule: PBI is the answer when the question asks about first aid for an Australian snakebite. It is NOT the answer for a UK adder bite (a viperid whose venom causes local tissue injury, not lymphatic spread) or a red-back spider bite (latrodectism, which requires analgesia and antivenom, not PBI). PBI IS used for funnel-web spider bites and box jellyfish tentacle attachment in some protocols. [1]
Limitations and controversies
The evidence for PBI is largely experimental (animal models and human tracer studies) rather than from randomised trials in the field [10]. Currie noted that real-world application is often incorrect — too loose, not covering the whole limb, or without a splint — which undermines its effectiveness [10]. There are also reports of harm from prolonged or overly tight bandaging, including compartment syndrome and localised tissue injury. Despite these limitations, PBI remains the standard recommendation for all Australian elapid bites [8].
Hospital assessment
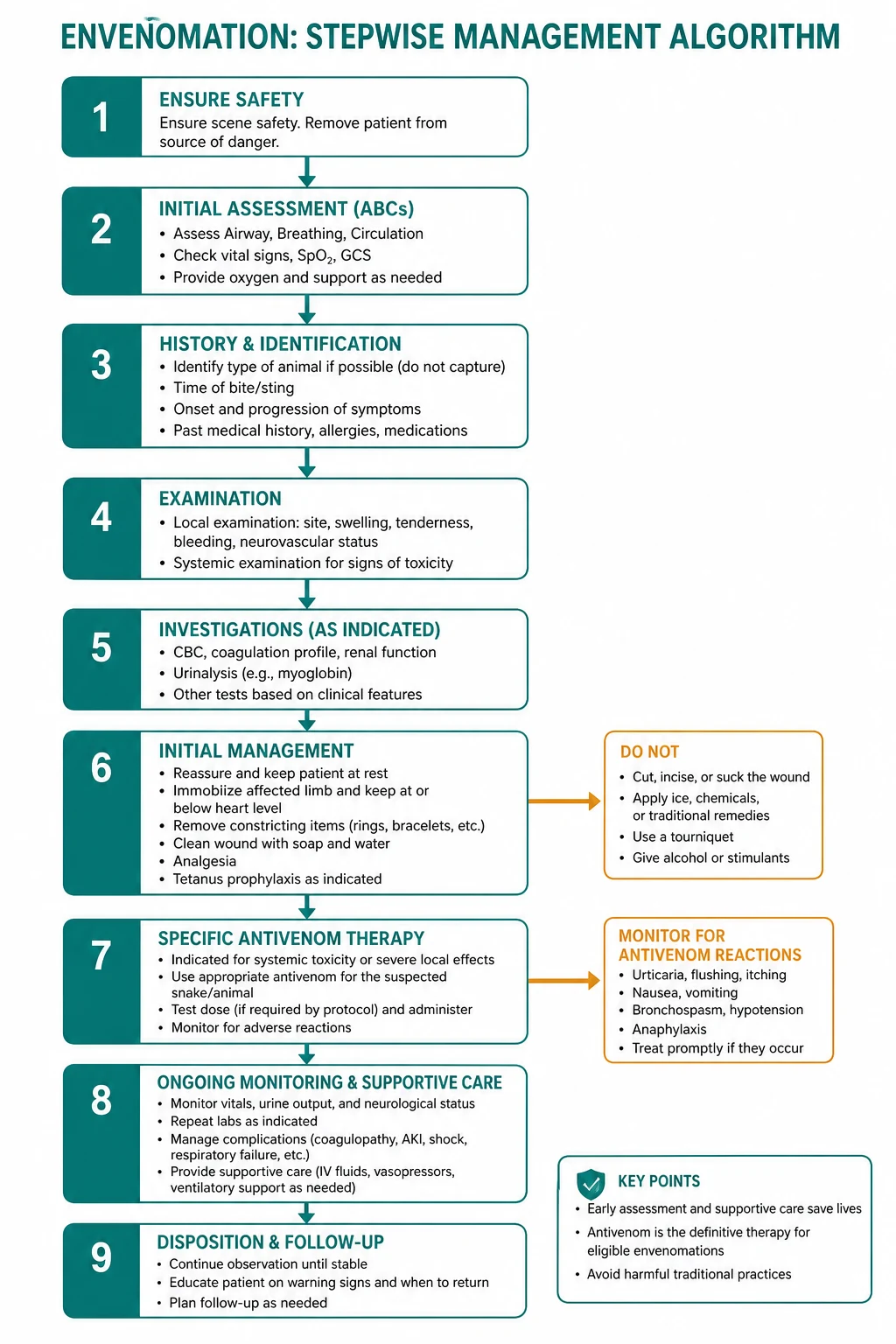
The clinical sequence
When the patient arrives in the emergency department: [1]
- ABC resuscitation. Assess airway (neurotoxicity can compromise it), breathing (respiratory rate, oxygen saturation, vital capacity), and circulation (heart rate, blood pressure — collapse and hypotension are common early).
- Keep the PBI in situ. Do not remove it yet. Set up monitoring, IV access (on the opposite limb or centrally if needed), and draw blood while the bandage is still on.
- Clinical assessment. Examine the bite site (fang marks, local swelling), palpate regional lymph nodes (tender nodes suggest lymphatic spread), perform a full neurological examination (ptosis, external ophthalmoplegia, facial weakness, bulbar function, limb power and reflexes), and examine the respiratory system (accessory muscle use suggests impending respiratory failure).
- Blood tests. Full blood count (platelet count for TMA), coagulation profile (INR, aPTT, fibrinogen, D-dimer), urea and electrolytes, creatinine kinase, blood group and hold, venous blood gas (lactate, acidosis), and urine for myoglobin.
- SVDK. Swab the bite site (through or adjacent to the bandage without removing it) or test the urine. The SVDK identifies the venom group — brown, tiger, black, death adder or taipan — which determines which monovalent antivenom to use. [1]
When to remove the PBI
The bandage is removed only when antivenom is drawn up and ready at the bedside, AND the patient has been fully assessed. If the patient is not envenomed (normal bloods, no clinical features), the PIB can be removed after a period of observation, but the bloods must be repeated to catch a delayed VICC. [1]
The observation protocol
A patient with a suspected snake bite but no initial features of envenomation is observed for at least 12 hours with serial coagulation at baseline, 1 to 2 hours, 6 hours and 12 hours. If all remain normal and there are no clinical features, the patient is discharged with advice to return if symptoms develop. [1]
DCE trap: The observation protocol is the answer when the examiner asks what to do with a suspected snake bite and normal initial bloods. Do NOT give antivenom prophylactically — it carries a reaction risk and is unnecessary. Observe and repeat the coagulation. [1]
The Snake Venom Detection Kit (SVDK)
The SVDK is a two-step enzyme immunoassay that identifies the snake venom group from a bite-site swab or a urine sample [1]. It distinguishes five groups: brown, tiger, black, death adder and taipan.
Two critical points about the SVDK: [1]
- It does NOT measure venom quantity. A positive SVDK does not mean the patient is envenomed — it means venom is present at the bite site or in the urine. The decision to give antivenom is made on clinical and laboratory grounds, not on the SVDK result alone.
- It guides antivenom choice, not the decision to treat. If the patient is envenomed, the SVDK tells you which monovalent antivenom to give. If the SVDK is unavailable and the patient is critically ill, start polyvalent antivenom. [1]
DWE trap: The SVDK is not a screening test. A positive SVDK in a patient with normal bloods and no clinical features does NOT warrant antivenom. The SVDK is used only in patients who are already confirmed as envenomed, to select the monovalent antivenom. [1]
Antivenom

The five monovalent antivenoms
Australian snake antivenoms are equine whole IgG preparations. There are five monovalent antivenoms — brown snake, tiger snake, black snake, death adder and taipan — plus a polyvalent antivenom that contains all five. The monovalent antivenoms cross-react to some degree within groups (for example, tiger snake antivenom neutralises copperhead and rough-scaled snake venom). [1]
Dosing — one vial
The ASP-20 study was the pivotal evidence for the one-vial regimen. Over the decade 2005 to 2015, the median antivenom dose fell from four vials to one, with no change in outcomes [1]. The ASP-14 brown snake study confirmed this — one vial of brown snake monovalent antivenom is the standard dose [2].
| Situation | Antivenom | Dose |
|---|---|---|
| Snake group identified (SVDK or geography) | Monovalent | One vial IV over 15 to 30 minutes |
| Snake group unknown, patient critically ill | Polyvalent | One to two vials IV |
| Death adder with neurotoxicity | Death adder monovalent | One vial IV, plus neostigmine trial |
| VICC with active bleeding | Monovalent plus FFP | One vial antivenom, then FFP guided by coagulation |
Premedication — NOT recommended
Current Australian guidelines do NOT recommend routine premedication before snake antivenom. The Premawardhena 1999 Sri Lankan trial showed that subcutaneous adrenaline reduced reactions to Indian polyvalent antivenom [13], but Australian antivenom is a purer product with a lower reaction rate, and prophylactic adrenaline carries its own risks (hypertension, cardiac events). The clinical rule is: have adrenaline drawn up and ready, but do not give it prophylactically [1].
Adverse reactions
Antivenom reactions fall into three types: [1]
- Immediate hypersensitivity (anaphylaxis) — within 30 minutes. Urticaria, flushing, bronchospasm, hypotension. Manage by stopping or slowing the infusion, giving intramuscular adrenaline 0.5 mg (adult), oxygen, IV fluids and an antihistamine. Most reactions are mild.
- Pyrogenic reaction — fever and rigors from endotoxin contamination. Managed by slowing the infusion and giving paracetamol.
- Serum sickness (type III hypersensitivity) — 5 to 14 days after exposure. Fever, arthralgia, rash and lymphadenopathy. Occurs in 20 to 40 per cent of patients who receive antivenom and is more common with larger doses and polyvalent antivenom. It is self-limiting but may require a short course of oral corticosteroids. Warn every patient who receives antivenom about it. [1]
DWE rule: The answer to "what premedication before antivenom" is: NONE routinely. Adrenaline is drawn up and ready, but not given prophylactically. This is a change from older practice and is a common trap. [1]
VICC management — antivenom, FFP and the recovery timeline
Antivenom neutralises circulating venom and prevents ongoing prothrombin activator activity, but it does NOT reverse the consumption that has already occurred — the clotting factors must be resynthesised by the liver [6]. The recovery timeline:
- Fibrinogen begins to rise within 6 to 12 hours and is measurable by 12 hours.
- INR begins to fall within hours of antivenom and is usually below 2 within 24 hours.
- D-dimer may remain elevated for days but does not guide management. [1]
The ASP-18 trial (Isbister 2013) randomised VICC patients to FFP versus no FFP after antivenom and found that FFP resulted in faster correction — more patients had an INR below 2 at 6 hours [7]. Current practice considers FFP in patients with active bleeding, before invasive procedures, or in selected cases of severe VICC. It is NOT given routinely to every patient — the coagulopathy is self-limiting and corrects spontaneously in most cases, and routine FFP exposes the patient to transfusion risk.
DCE management trap: Do not panic at an INR above 10 and rush to give FFP and vitamin K. VICC is not warfarin toxicity, and vitamin K is useless (the factor synthesis is intact — the problem is consumption, not production). Give antivenom, observe, and reserve FFP for active bleeding or procedures. Avoid all non-essential invasive procedures (central lines, arterial gases, lumbar punctures) until the INR is below 2, because the coagulopathy dramatically increases procedural bleeding risk. [1]
Spider bite
Funnel-web spider (Atrax and Hadronyche species) — a medical emergency
The Sydney funnel-web (Atrax robustus) and its relatives in the Hadronyche genus produce a neurotoxic venom (delta-hexatoxin) that causes massive release of neurotransmitters at autonomic and neuromuscular junctions. The result is a syndrome of autonomic and neuromuscular excitation [11]:
- Neuromuscular: fasciculations (visible muscle twitching over the whole body), muscle spasms.
- Autonomic (parasympathetic): lacrimation, salivation, sweating, piloerection, miosis.
- Autonomic (sympathetic): hypertension, tachycardia, then bradycardia as the autonomic storm progresses.
- Pulmonary oedema from the hypertensive crisis and direct capillary leak. [1]
Management: This is a time-critical emergency. The first aid is the pressure immobilisation bandage (same technique as snake bite — the venom spreads via lymphatics). The treatment is funnel-web spider antivenom (derived from sheep immunised with Atrax robustus venom), given as two vials intravenously for systemic envenomation. The antivenom is highly effective — there have been no deaths since its introduction in 1981 [11]. Have adrenaline ready.
DWE discriminator: Funnel-web spider bite is the ONLY spider bite in Australia where PBI is the first aid. Red-back spider bites do NOT get PBI. This distinction is tested. [1]
Red-back spider (Latrodectus hasselti) — latrodectism
The red-back spider produces alpha-latrotoxin, which causes massive presynaptic neurotransmitter release. The syndrome is latrodectism: [1]
- Severe local pain at the bite site, radiating and often described as burning or throbbing.
- Sweating and piloerection localised to the bite area or generalised.
- Hypertension and mild tachycardia.
- Regional lymph node tenderness.
- The illness can last days to weeks untreated. [1]
Management: First aid is NOT PBI — the venom acts locally and systemically through a different mechanism. The management is analgesia (oral and parenteral, including opioids) and red-back spider antivenom in selected cases. The RAVE study (Isbister 2008) compared IV versus IM routes and found no significant difference in pain relief [12]. A subsequent placebo-controlled trial (RAVE-II) raised questions about whether antivenom adds benefit over standard analgesia. Current practice: give antivenom (IV preferred) for persistent severe pain unresponsive to opioids, after discussion with a toxicologist.
DWE rule: Red-back spider bite management is analgesia plus or minus antivenom. The first aid is a cold compress, NOT a pressure bandage. The antivenom is NOT funnel-web antivenom. These three facts answer most red-back questions. [1]
Marine envenomation
Box jellyfish (Chironex fleckeri) — the deadliest
The box jellyfish is found in tropical Australian waters (north Queensland, Northern Territory, Western Australia). Its tentacles fire millions of nematocysts that deliver a cardiotoxic and dermatonecrotic venom. The clinical picture is dramatic [1]:
- Immediate severe pain at the sting site — described as the worst pain imaginable.
- Cross-hatched welts on the skin where the tentacles contacted.
- Cardiac arrest can occur within minutes from direct cardiotoxicity (ventricular arrhythmia, hypotension). [1]
Management: [1]
- Vinegar (acetic acid, 4 to 6 per cent) poured copiously over the tentacles to inactivate the nematocysts and prevent further discharge. Do NOT use fresh water, urine, alcohol or methylated spirits — these cause further nematocyst discharge.
- Carefully remove the tentacles after vinegar application (wear gloves).
- IV box jellyfish antivenom (three vials IV) for systemic envenomation — cardiac arrhythmia, hypotension, respiratory depression.
- CPR if cardiac arrest occurs. The cardiotoxicity may be reversible with antivenom, CPR and time. [1]
DWE rule: The answer to "what do you pour on a box jellyfish sting" is vinegar. This is one of the most frequently tested first-aid facts in Australian exams. [1]
Blue-ringed octopus (Hapalochlaena) — tetrodotoxin
The blue-ringed octopus delivers tetrodotoxin, a potent sodium channel blocker that produces rapid onset flaccid paralysis with preserved consciousness and preserved pupil reflexes. There is NO antivenom. Management is purely supportive — mechanical ventilation until the toxin wears off (hours to a day). The patient is conscious but paralysed — they must be told this, and sedation is NOT routinely needed unless anxiety is severe. [1]
DWE discriminator: Blue-ringed octopus bite produces paralysis with PRESERVED pupils and PRESERVED consciousness. This distinguishes it from botulism (pupils dilated, descending) and organophosphate poisoning (miosis, bronchorrhoea, fasciculations). [1]
Stonefish (Synanceia) — hot water and antivenom
The stonefish has 13 dorsal spines that deliver a venom causing severe local pain and systemic features. The management is: [1]
- Hot water immersion at 40 to 42 degrees Celsius (as hot as the patient can tolerate) — heat denatures the venom and dramatically reduces pain.
- Stonefish antivenom (one vial IM or IV per two spine punctures) for severe envenomation. [1]
DWE rule: Hot water immersion is the first-aid answer for stonefish and other fish stings (stingray, catfish, scorpionfish). This is a different answer from box jellyfish (vinegar) and snake bite (PBI). [1]
Sea snake (Hydrophiidae) — myotoxic
Sea snakes produce a myotoxic venom causing rhabdomyolysis with CK above 10 000 U/L, myoglobinuria and AKI. The management is the same as for a terrestrial snake bite — PBI first aid, hospital assessment, and sea snake antivenom (which is tiger snake monovalent antivenom, as the venoms cross-react). Management of rhabdomyolysis includes aggressive IV fluids to maintain urine output and renal monitoring. [1]
Complications and their management
| Complication | When it occurs | Management |
|---|---|---|
| Thrombotic microangiopathy (TMA) | 10 per cent of brown snake bites, days 1 to 3 | Supportive — renal support, transfusion, monitor for dialysis need; antivenom does not reverse established TMA |
| Acute kidney injury | From TMA, pigment nephropathy, or direct venom effect | IV fluids, renal replacement therapy if needed; usually resolves over days to weeks |
| Major haemorrhage (intracranial) | Under 5 per cent; risk highest with head injury from collapse or invasive procedures | Antivenom, FFP, neurosurgical referral; avoid all non-essential procedures during coagulopathy |
| Respiratory failure | Presynaptic neurotoxicity (tiger snake, taipan) — antivenom cannot reverse established terminal destruction | Mechanical ventilation for days; antivenom prevents further damage |
| Serum sickness | 5 to 14 days after antivenom | Oral corticosteroids (prednisone 25 to 50 mg daily for 5 days); self-limiting |
Long-term outcomes and follow-up
The prognosis for Australian snakebite is excellent with early PBI and appropriate antivenom. The ASP-20 study reported 23 deaths over 10 years (a median of two per year) among 1548 suspected snakebites and 835 confirmed envenomations [1]. Most deaths are from brown snake VICC with a head injury from collapse, or from delayed presentation in remote areas.
Follow-up after discharge should address: [1]
- Serum sickness — warn the patient and provide a return plan. Symptoms at 1 to 2 weeks: fever, arthralgia, rash.
- VICC recovery — the coagulation normalises within 24 to 48 hours but the patient should avoid contact sports and elective surgery for at least one week.
- Renal recovery — patients who developed AKI need renal follow-up to confirm complete recovery. TMA-associated AKI may take weeks.
- Psychological support — a snake bite is a traumatic event, particularly if the patient was intubated or experienced collapse. Offer referral to a psychologist or a trauma service.
- Snake avoidance education — appropriate footwear, carrying a PBI kit in snake-prone areas, and knowing the local emergency number. [1]
DWE high-yield summary
| Question | Answer |
|---|---|
| First aid for Australian snake bite | Pressure immobilisation bandage (PBI) |
| Most common cause of snakebite death in Australia | Brown snake |
| VICC dominant syndrome | Brown snake |
| VICC plus neurotoxicity | Tiger snake |
| Pure neurotoxicity, no VICC | Death adder |
| VICC is NOT DIC because | No microthrombi, no end-organ damage from thrombosis, toxin-driven prothrombin activation |
| Antivenom dose | One vial of monovalent (guided by SVDK) |
| Premedication before antivenom | NOT recommended; have adrenaline ready |
| What reverses death adder neurotoxicity | Antivenom (postsynaptic block is reversible) and neostigmine trial |
| What does NOT reverse tiger snake neurotoxicity | Antivenom (presynaptic destruction is irreversible once established) |
| First aid for funnel-web spider bite | Pressure immobilisation bandage |
| First aid for red-back spider bite | Cold compress (NOT PBI) |
| Pour on box jellyfish tentacles | Vinegar |
| Blue-ringed octopus toxin | Tetrodotoxin (sodium channel blocker) |
| First aid for stonefish sting | Hot water immersion at 40 to 42 degrees |
| FFP role in VICC | After antivenom, for active bleeding or procedures (ASP-18 trial) |
| Serum sickness | 5 to 14 days after antivenom; fever, arthralgia, rash; oral steroids |
Guideline and regional deltas
- ANZ (primary): Australian Therapeutic Guidelines — Toxicology. PBI first aid, one vial of monovalent antivenom guided by SVDK, no routine premedication, observation protocol for non-envenomed patients. The RAVE and ASP trials are the ANZ evidence base.
- UK (secondary): The UK has one native venomous snake — the adder (Vipera beris), a viperid. First aid is NOT PBI (the venom causes local tissue injury, not lymphatic spread). Management is observation and European viper antivenom for systemic features. UK guidelines (Toxbase, NPIS) are relevant to MRCP but are a different clinical scenario.
- US (tertiary): ABIM candidates should understand the elapid principles (PBI, antivenom, VICC) as they apply globally, though the US has fewer elapids (coral snake) and more viperids (rattlesnakes, copperheads, cottonmouths). Viperid management uses CroFab (Crotalidae polyvalent immune Fab) and does NOT use PBI.
- Global (WHO): The WHO snakebite guidelines for South and Southeast Asia differ from Australian practice — multi-vial antivenom regimens (10 to 20 vials) are used because the venoms and antivenoms are different; the Premawardhena adrenaline premedication finding applies to these higher-reaction-rate products [13].
References (summary)
Johnston CI, Ryan NM, Page CB, et al. The Australian Snakebite Project 2005 to 2015 (ASP-20). Med J Aust 2017 (28764620); Isbister GK, et al. Brown snake (Pseudonaja) envenoming — ASP-14. Med J Aust 2012 (23300888); Isbister GK, et al. Thrombotic microangiopathy from Australian brown snake envenoming. Intern Med J 2007 (17640187); Isbister GK. Snakebite doesn't cause DIC: VICC. Semin Thromb Hemost 2010 (20614396); Isbister GK, et al. VICC in snakebite: systematic review. PLoS Negl Trop Dis 2014 (25340841); Isbister GK, et al. Recovery of VICC in Australian snakebite. QJM 2009 (19570990); Isbister GK, et al. RCT of FFP for VICC (ASP-18). J Thromb Haemost 2013 (23565941); Sutherland SK, Coulter AR, Harris RD. Rationalisation of first-aid measures for elapid snakebite. Lancet 1979 (84206); Pearn J, et al. First-aid for snake-bite: efficacy of constrictive bandage. Med J Aust 1981 (7300763); Currie BJ. Pressure-immobilisation first aid: fact and fiction. Med J Aust 2008 (18549384); Hartman LJ, Sutherland SK. Funnel-web spider antivenom. Med J Aust 1984 (6503783); Isbister GK, et al. RAVE: IV vs IM red-back antivenom. QJM 2008 (18400776); Premawardhena AP, et al. Low-dose adrenaline for antivenom reactions. BMJ 1999 (10205101). [1]
References
- [1]Johnston CI, Ryan NM, Page CB, et al. The Australian Snakebite Project, 2005-2015 (ASP-20) Med J Aust, 2017.PMID 28764620
- [2]Isbister GK, O'Leary MA, Elliott M, Liddell J, Caldicott D, Currie BJ, Brown SG, ASP Investigators Clinical effects and antivenom dosing in brown snake (Pseudonaja spp.) envenoming--Australian snakebite project (ASP-14) PLoS One, 2012.PMID 23300888
- [3]Isbister GK, Little M, Cull G, McCoubrie D, Lawton P, Szabo F, Kennedy J, Trethewy P, Ruscoe T, Brown SG Thrombotic microangiopathy from Australian brown snake (Pseudonaja) envenoming Intern Med J, 2007.PMID 17640187
- [4]Isbister GK Snakebite doesn't cause disseminated intravascular coagulation: coagulopathy and thrombotic microangiopathy in snake envenoming Semin Thromb Hemost, 2010.PMID 20614396
- [5]Isbister GK, Maduwage K, Scorgie FE, Shahmy S, Mohamed F, Ariaratnam CA, Meyer WP, McCoubrie D, Cull G, Smith WK, Ouvrier R, Silva HA Current treatment for venom-induced consumption coagulopathy resulting from snakebite PLoS Negl Trop Dis, 2014.PMID 25340841
- [6]Isbister GK, Williams V, Brown SG, White J, Currie BJ, ASP Investigators Failure of antivenom to improve recovery in Australian snakebite coagulopathy QJM, 2009.PMID 19570990
- [7]Isbister GK, Buckley NA, Page CB, Scorgie FE, Lincz LF, Seldon M, Brown SG, ASP Investigators A randomized controlled trial of fresh frozen plasma for treating venom-induced consumption coagulopathy in cases of Australian snakebite (ASP-18) J Thromb Haemost, 2013.PMID 23565941
- [8]Sutherland SK, Coulter AR, Harris RD Rationalisation of first-aid measures for elapid snakebite Lancet, 1979.PMID 84206
- [9]Pearn J, Morrison J, Charles N, Muir G First-aid for snake-bite: efficacy of a constrictive bandage with limb immobilization in the management of human envenomation Med J Aust, 1981.PMID 7300763
- [10]Currie BJ Effectiveness of pressure-immobilization first aid for snakebite requires further study Emerg Med Australas, 2008.PMID 18549384
- [11]Hartman LJ, Sutherland SK Funnel-web spider (Atrax robustus) antivenom in the treatment of human envenomation Med J Aust, 1984.PMID 6503783
- [12]Isbister GK, Brown SG, Miller M, Laczko D, Currie BJ, ASP Investigators A randomised controlled trial of intramuscular vs. intravenous antivenom for latrodectism--the RAVE study QJM, 2008.PMID 18400776
- [13]Premawardena AP, de Silva CE, Fonseka MM, Gunasekera AS, de Silva AM, Gunatilake SB, de Silva HJ Low dose subcutaneous adrenaline to prevent acute adverse reactions to antivenom serum in people bitten by snakes: randomised, placebo controlled trial BMJ, 1999.PMID 10205101