Phys · pharmacological
Lithium Toxicity
Also known as lithium toxicity · lithium poisoning · lithium intoxication · lithium overdose · lithium carbonate · lithium citrate · EXTRIP · nephrogenic diabetes insipidus · SILENT · syndrome of irreversible lithium-effectuated neurotoxicity · chronic interstitial nephritis · inositol monophosphatase · IMPase · glycogen synthase kinase-3 · GSK-3 · haemodialysis
Consultant-physician guide to lithium toxicity — the narrow-therapeutic-index monovalent cation whose entirely renal elimination makes it vulnerable to dehydration, drug interactions (thiazides, ACE inhibitors, NSAIDs), and acute kidney injury. Covers the pharmacology (inositol depletion, GSK-3 inhibition, 0.6 to 1.0 mmol/L maintenance target, 0.8 to 1.2 for acute mania, toxicity above 1.5, severe above 2.5), the three clinical patterns (acute, acute-on-chronic, chronic), the clinical features by severity (mild: coarse tremor, gastrointestinal, ataxia, hyperreflexia; severe: seizures, coma, hyperthermia, QT prolongation, myoclonus), the chronic end-organ effects (nephrogenic diabetes insipidus, chronic interstitial nephritis, hypothyroidism, hyperparathyroidism, SILENT), and the management (stop lithium, aggressive IV saline, haemodialysis by EXTRIP criteria, post-dialysis rebound monitoring). Structured for FRACP DWE and DCE, MRCP, and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Lithium Toxicity

The answer first
Lithium is a monovalent cation used as the gold-standard mood stabiliser for bipolar disorder, with unmatched efficacy for mania prophylaxis and suicide prevention. Its great limitation is a narrow therapeutic index: the target serum concentration for maintenance therapy is 0.6 to 1.0 mmol per litre, with a higher target of 0.8 to 1.2 mmol per litre for acute mania. Toxicity emerges above 1.5 mmol per litre, becomes severe above 2.5 mmol per litre, and warrants haemodialysis above 4.0 mmol per litre [1][2].
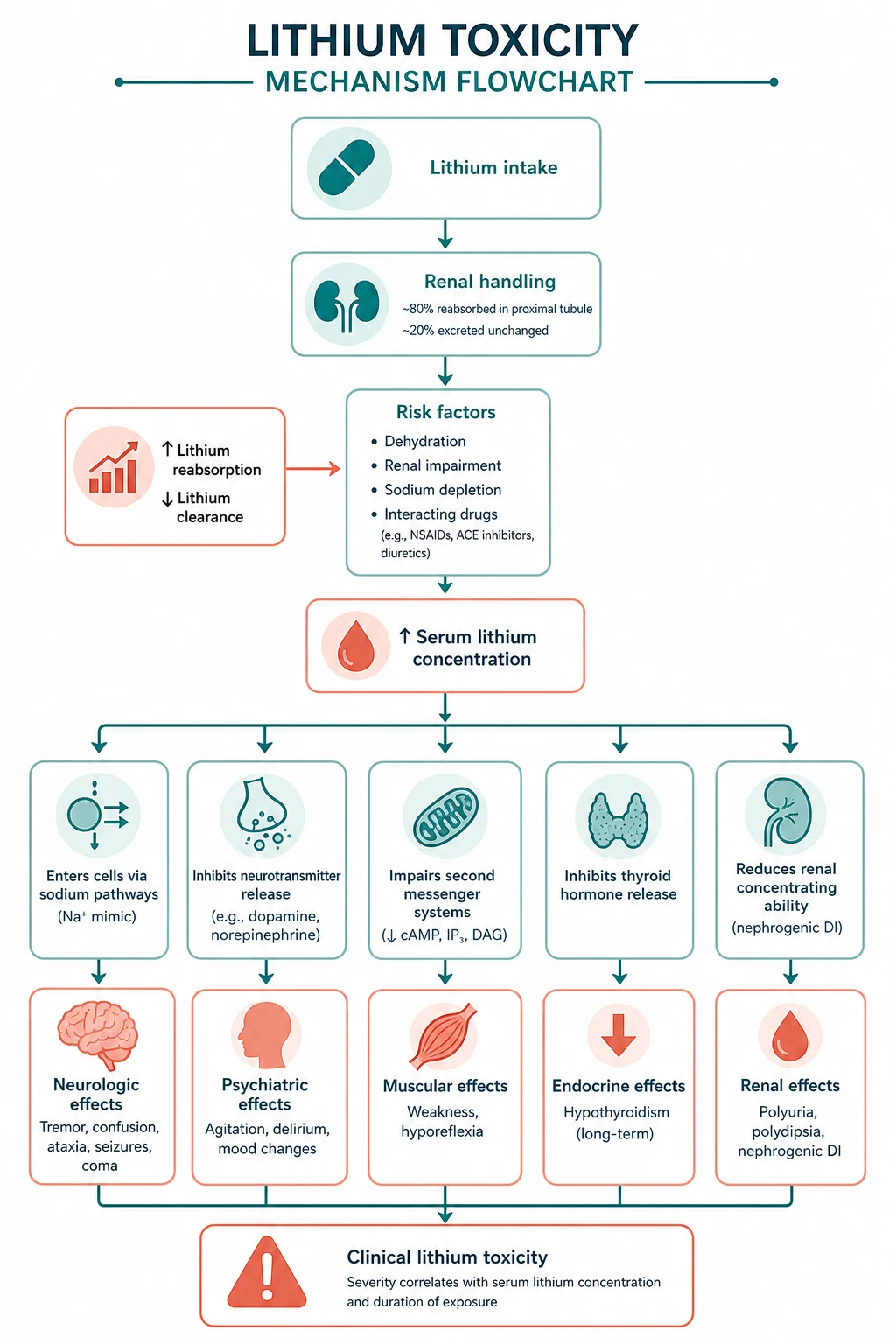
The single organising principle: lithium is entirely renally eliminated — freely filtered at the glomerulus, not protein-bound — so anything that reduces glomerular filtration or enhances tubular reabsorption of lithium (dehydration, acute kidney injury, thiazides, ACE inhibitors, NSAIDs) precipitates toxicity. The brain is the target organ. Management hinges on stopping the lithium, restoring intravascular volume with intravenous normal saline to enhance renal lithium excretion, and haemodialysing patients who meet the EXTRIP criteria (level above 4.0 regardless of symptoms; level above 2.5 with symptoms; renal failure not responding to fluids; decreased consciousness or seizures) [1].
DWE high-yield: The serum level alone never determines management — interpret it with the clinical pattern. A level of 3.0 mmol per litre in a pure acute overdose (tissue levels still low) is less dangerous than 2.5 mmol per litre in chronic toxicity (tissue-saturated, brain already affected). Dialyse on the combination of level, symptoms, and renal function, per EXTRIP [1][2].
Pharmacology — why lithium is a toxicological tightrope
Lithium is a simple monovalent cation (Li+) with no metabolism, no protein binding, and a volume of distribution that approximates total body water (around 0.7 to 0.9 litres per kilogram). It is freely filtered at the glomerulus and reabsorbed in the proximal tubule (about 80 percent of filtered load, tracking sodium handling). Elimination is entirely renal. The elimination half-life is approximately 12 to 24 hours in patients on chronic therapy, but is longer in the elderly and in renal impairment. These pharmacokinetic properties make lithium entirely dependent on kidney function for clearance, and they explain why dehydration and sodium-depleting drugs are the commonest precipitants of toxicity [2][3].
The two mechanisms of action
Lithium's therapeutic and toxic effects arise from two principal molecular targets: [1]
- Inositol depletion. Lithium non-competitively inhibits inositol monophosphatase (IMPase), the enzyme that recycles myo-inositol in the phosphatidylinositol signalling pathway. The resulting depletion of intracellular myo-inositol dampens the phosphatidylinositol second-messenger cascade, reducing the overactivity of neurotransmitter signalling that underpins mania [2].
- GSK-3 inhibition. Lithium directly inhibits glycogen synthase kinase-3 (GSK-3 alpha and beta), competing with magnesium at the enzyme's active site. GSK-3 is a central hub for cellular signalling — synaptic plasticity, circadian rhythms, neuroprotection, and apoptosis — and its inhibition is increasingly regarded as the more compelling explanation for lithium's broad clinical effects and its neuroprotective properties [2].
These same mechanisms — disruption of neuronal second-messenger signalling and cellular signalling cascades — explain why the brain is the primary target organ of toxicity. Lithium also affects the kidney (aquaporin-2 downregulation in the collecting duct, via entry through the epithelial sodium channel ENaC) and the thyroid and parathyroid glands. [1]
The narrow therapeutic index
The narrowness of the therapeutic window is the clinical reality. The maintenance target of 0.6 to 1.0 mmol per litre sits close to the toxicity threshold. Small reductions in clearance — a gastrointestinal illness with dehydration, a new thiazide, an acute kidney injury — can push a stable patient into toxicity within days. This is why every patient on lithium must be counselled about the early symptoms and why every new prescription in a lithium-treated patient demands a level check. [1]

DWE high-yield: Know the levels by heart — maintenance 0.6 to 1.0, acute mania 0.8 to 1.2, toxicity above 1.5, severe above 2.5, dialyse above 4.0 (or above 2.5 with symptoms). These thresholds appear in MCQ stems constantly [1][2].
Risk factors — who becomes toxic
Because lithium clearance tracks renal function and proximal sodium handling, the risk factors for toxicity all converge on reduced glomerular filtration or increased proximal lithium reabsorption [2][3]:
| Risk factor | Mechanism | Clinical consequence |
|---|---|---|
| Acute kidney injury | Reduced GFR reduces filtered lithium load | Rapid accumulation in hours to days |
| Dehydration / volume depletion | Sodium avidity increases proximal lithium reabsorption | The commonest precipitant in practice |
| Sodium depletion | Increased proximal sodium (and lithium) reabsorption | Vomiting, diarrhoea, low-salt diet |
| Thiazide diuretics | Volume and sodium depletion at the distal tubule feeds back to proximal lithium reabsorption | Level rises 25 to 40 percent within days |
| Loop diuretics | Less than thiazides, but still increase lithium reabsorption | Use with caution, monitor closely |
| ACE inhibitors / ARBs | Reduced GFR and altered proximal handling via angiotensin II | Level rises over 1 to 4 weeks |
| NSAIDs | Reduced renal prostaglandin, reduced renal blood flow, increased lithium reabsorption | All NSAIDs, indometacin the greatest |
| Age above 65 | Reduced GFR, reduced total body water, polypharmacy | Lower doses, lower targets, closer monitoring |
| Reduced renal function (CKD) | Lower baseline clearance, smaller safety margin | The progressive creatinine rise over years |
DWE trap: The classic MCQ scenario is the older patient on stable lithium who is started on a thiazide for hypertension, or an ACE inhibitor for heart failure, or who takes NSAIDs for a few days for back pain — and presents a week later with confusion and a coarse tremor. The interaction is the cause. Reduce the lithium dose by 25 to 50 percent when starting any of these drugs, and check a level within 5 to 7 days [2][3].
The three clinical patterns of poisoning
Lithium poisoning falls into three patterns, each with a different relationship between the serum level and the clinical effect. Knowing the pattern changes the interpretation of the level and the urgency of management [2].
Acute poisoning
An acute ingestion by a lithium-naive patient (or a single large overdose in a patient on therapy). The serum level can be very high initially, but because the tissue compartment (including the brain) is not yet saturated, the patient may look relatively well. Gastrointestinal symptoms (nausea, vomiting, diarrhoea) dominate the early picture, and neurological toxicity develops as lithium distributes into tissues over the following hours. The peak level may be delayed with modified-release formulations, so repeated levels are essential. Management is aggressive supportive care; haemodialysis is reserved for the EXTRIP criteria, recognising that a very high acute level may fall rapidly with good renal clearance once absorption is complete [1][2].
Acute-on-chronic poisoning
An acute overdose superimposed on chronic therapy. The tissue compartment is already saturated, so the patient develops toxicity at lower serum levels than a purely acute overdose. Both the gastrointestinal symptoms of acute ingestion and the neurological toxicity of chronic exposure are present. This pattern carries an intermediate risk and requires careful monitoring and a low threshold for dialysis if symptoms progress. [1]
Chronic poisoning (accumulation toxicity)
The most dangerous pattern, and the most common in clinical practice. Toxicity develops insidiously as lithium accumulates — usually from a reduction in clearance (dehydration, a new interacting drug, an intercurrent illness, progressive CKD). Because the tissue compartment is already saturated, the serum level correlates poorly with severity: a level of 2.5 mmol per litre in a chronically toxic patient reflects a brain that has been exposed to toxic tissue levels for days, and the patient will already have significant neurological toxicity. Chronic toxicity carries the highest risk of irreversible neurological injury (SILENT) [2][3].
DWE high-yield: The most tested concept is the level does not predict severity across patterns. A level of 3.0 in acute overdose may be tolerated; the same level in chronic toxicity is a medical emergency. Always interpret the level with the history and the clinical state [2].
Clinical features by severity
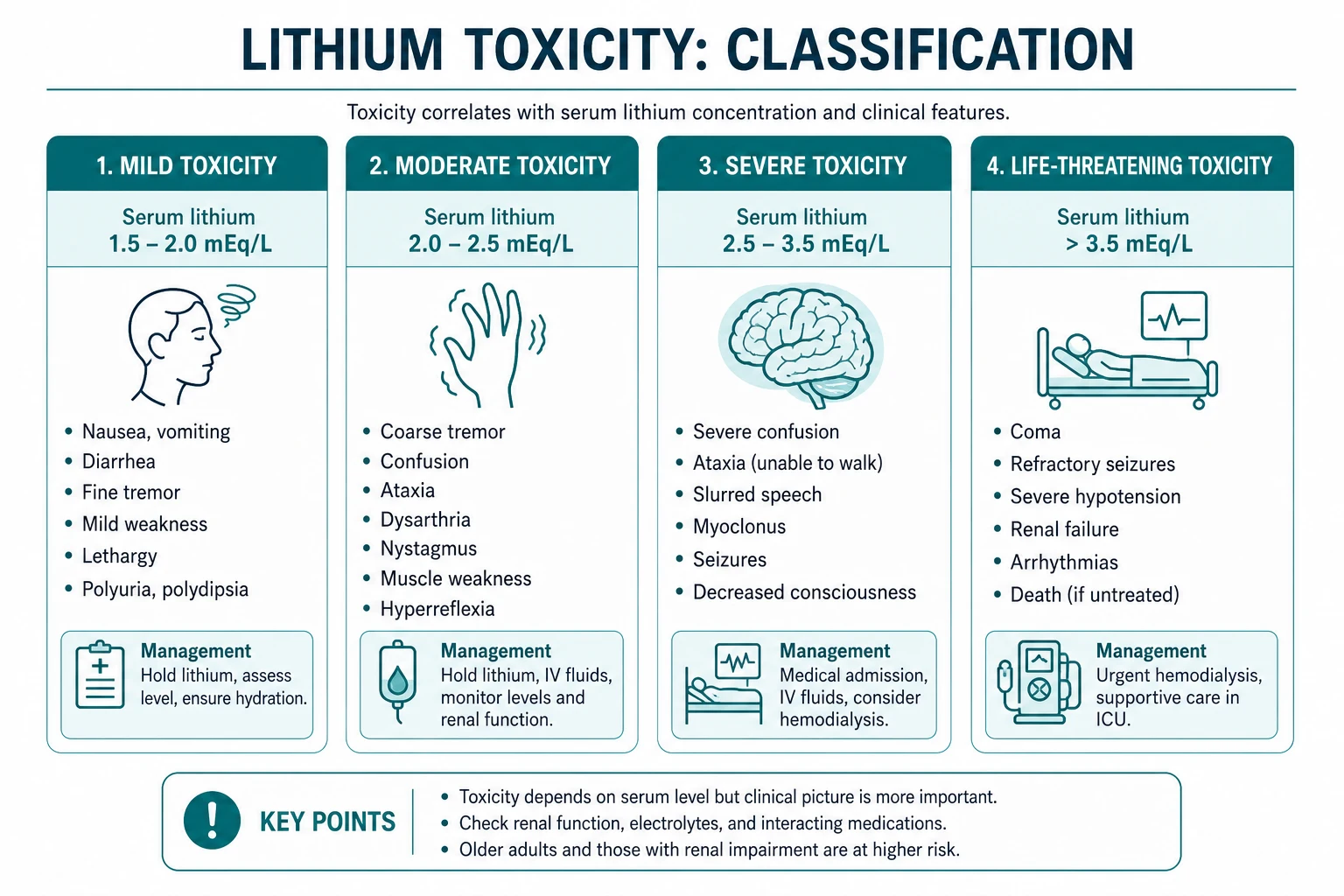
Mild toxicity (1.5 to 2.5 mmol per litre) [1]
The earliest signs are neurological and gastrointestinal. A coarse tremor (distinguished from the fine physiological tremor that many patients on lithium develop at therapeutic levels) is often the first sign, affecting the hands and sometimes the jaw. Gastrointestinal symptoms — nausea, vomiting, diarrhoea, and abdominal pain — are common, particularly in acute ingestion. The patient may be mildly confused or lethargic, with slurred speech. Neurological examination reveals hyperreflexia, ataxia, and muscle fasciculations. These features are easily mistaken for the underlying psychiatric illness, an intercurrent infection, or simple frailty — the index of suspicion must be high [2].
Moderate-to-severe toxicity (above 2.5 mmol per litre) [1]
As the level rises, the neurological toxicity deepens. The patient develops marked confusion, agitation, or delirium, progressing to seizures and coma. Hyperthermia may develop (and must be distinguished from neuroleptic malignant syndrome). The neuromuscular examination shows prominent fasciculations, myoclonus, and extrapyramidal rigidity. Cardiac conduction defects appear on the ECG — QT prolongation, T-wave inversion or flattening, and occasionally sinus node dysfunction or bradycardia. These features indicate tissue-saturated toxicity and mandate urgent management, including haemodialysis if the criteria are met [1][2].
| Severity | Serum level (mmol/L) | Key features |
|---|---|---|
| Mild | 1.5 to 2.5 | Coarse tremor, nausea, vomiting, diarrhoea, mild confusion, hyperreflexia, ataxia, fasciculations |
| Severe | above 2.5 | Seizures, coma, hyperthermia, myoclonus, extrapyramidal rigidity, QT prolongation, T-wave inversion |
| Life-threatening | above 4.0 (or above 2.5 with symptoms) | Refractory seizures, deep coma, cardiac arrhythmia — haemodialysis indicated |
DWE high-yield: The tremor of lithium toxicity is coarse, present at rest and on action, at roughly 6 to 8 Hz. It contrasts with the fine, action tremor (8 to 12 Hz) of therapeutic lithium levels or essential tremor, and the resting, pill-rolling tremor (4 to 6 Hz) of Parkinson disease. The appearance of a coarse tremor in a patient on lithium is a red flag [2].
Chronic end-organ effects — the long-term toxicities
Beyond acute and subacute toxicity, long-term lithium therapy produces a distinct set of end-organ effects that the physician must screen for in every long-term patient and that feature in the DCE long case. The McKnight systematic review and meta-analysis quantified these risks [3].
Nephrogenic diabetes insipidus
Lithium enters the principal cells of the collecting duct through the epithelial sodium channel (ENaC) and, once intracellular, is not efficiently pumped out. It downregulates aquaporin-2 (AQP2) water channels — both by reducing cAMP-mediated signalling downstream of vasopressin and through cAMP-independent pathways including GSK-3 beta disruption. The result is a concentrating defect: the collecting duct becomes insensitive to vasopressin, and the patient develops polyuria (often 3 to 5 litres per day or more) and polydipsia. This affects an estimated 20 to 40 percent of patients on chronic lithium, making it the most common renal effect [2][3].
The diagnosis is confirmed by an inappropriately dilute urine (low specific gravity, low osmolality) despite an elevated or normal-high serum osmolality — the kidneys cannot concentrate even when the body needs them to. A water deprivation test or desmopressin trial confirms the nephrogenic (vasopressin-resistant) nature. Amiloride (an ENaC blocker that reduces lithium entry into the principal cell) can partially reverse the concentrating defect and is the preferred diuretic in lithium-treated patients who need one [2].
Chronic interstitial nephritis and progressive CKD
Long-term lithium produces a chronic tubulointerstitial nephritis — a slowly progressive scarring of the renal interstitium and tubules that, over years to decades, can reduce the GFR. The McKnight meta-analysis found a reduction in urinary concentrating ability (mean difference of roughly negative 15 milliosmoles per kilogram) and evidence of an increased risk of renal failure, though the absolute risk of progression to end-stage renal disease was small (around 0.5 percent in the reviewed cohorts) [3]. The key clinical point is that a progressively rising creatinine in a patient on long-term lithium is lithium-induced chronic interstitial nephritis until proven otherwise, and warrants nephrology assessment and a decision, made jointly with the treating psychiatrist, about whether to continue, dose-reduce, or switch to an alternative mood stabiliser.
Thyroid effects
Lithium accumulates in the thyroid gland and inhibits thyroid hormone synthesis and release. The McKnight meta-analysis found a significantly increased risk of clinical hypothyroidism (odds ratio 5.78 compared to placebo), with a mean TSH elevation of around 4 milli-international units per litre [3]. A goitre may develop. Female sex, older age, a family history of thyroid disease, and the presence of thyroid autoantibodies increase the risk. Most patients can be managed with levothyroxine replacement without stopping the lithium.
Hyperparathyroidism and hypercalcaemia
Lithium increases the set-point of the calcium-sensing receptor in the parathyroid gland, leading to inappropriately non-suppressed parathyroid hormone (PTH) and hypercalcaemia. The prevalence of lithium-associated hyperparathyroidism is around 4 to 6 percent — far higher than the 0.5 percent population prevalence of primary hyperparathyroidism. Unlike sporadic primary hyperparathyroidism, lithium-induced hyperparathyroidism has a higher rate of multiglandular disease (around 50 percent), which has implications for surgical management. Every patient on long-term lithium should have a calcium checked at baseline and at each monitoring visit [3].

SILENT — Syndrome of Irreversible Lithium-Effectuated NeuroToxicity
A feared complication, SILENT describes the persistence of neurological deficits — most commonly cerebellar dysfunction (ataxia, nystagmus, dysarthria) and cognitive impairment — after the serum lithium level has normalised. It occurs after a severe or prolonged episode of toxicity, and the deficits may be permanent. The mechanism is thought to be irreversible neuronal injury in the cerebellum and cortex from prolonged exposure to toxic tissue lithium levels. There is no specific treatment; prevention through early recognition and management of toxicity is paramount [2].
Management of acute and subacute toxicity
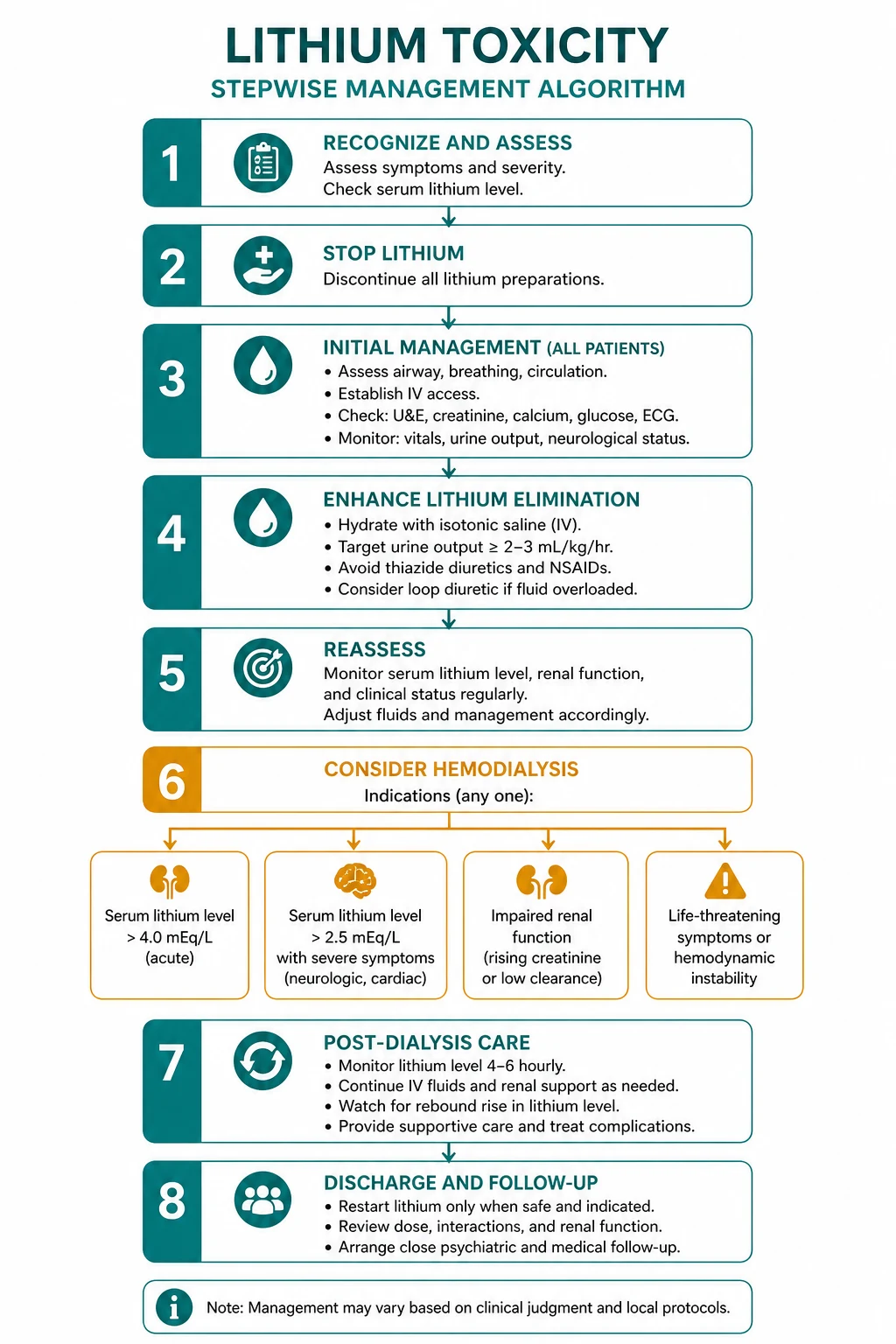
Step 1 — Stop the lithium, assess, and resuscitate (ABCDE)
The first action on suspecting lithium toxicity is to stop the lithium and assess the patient with a structured ABCDE approach. The airway is at risk in the comatose or seizing patient. Breathing may be compromised by decreased consciousness or aspiration. Circulation is usually preserved but may be impaired by dehydration from gastrointestinal losses or nephrogenic diabetes insipidus. Disability assessment includes the Glasgow Coma Scale, pupillary examination, blood glucose, and a seizure assessment. An ECG is mandatory to identify QT prolongation or conduction defects [1][2].
Step 2 — Aggressive intravenous fluid resuscitation
The cornerstone of management is aggressive intravenous normal saline (0.9 percent sodium chloride) to restore intravascular volume, correct dehydration, and enhance renal lithium excretion. Lithium clearance tracks renal function and proximal sodium handling — volume expansion increases GFR and suppresses the sodium avidity that drives proximal lithium reabsorption. In the volume-depleted patient, this alone can substantially lower the lithium level over several hours. The rate is tailored to the volume status and the cardiac and renal function — typically 1 to 2 litres over the first few hours in the dehydrated patient, then a maintenance rate adjusted to the urine output and the ongoing losses. Normal saline is preferred over Hartmann solution (which contains less sodium and may be less effective at suppressing lithium reabsorption) [2].
DWE high-yield: Do not give loop diuretics in lithium toxicity. Loop diuretics increase distal sodium delivery, which feeds back to increased proximal sodium and lithium reabsorption, paradoxically raising the lithium level. The correct fluid is normal saline alone. Amiloride is the one diuretic that may be useful in chronic lithium therapy (it blocks ENaC and reduces lithium entry into the principal cell), but it is not an acute management tool [2].
Step 2b — Gastrointestinal decontamination (acute overdose only)
In the patient who has taken an acute overdose of lithium (particularly modified-release formulations), gastrointestinal decontamination has a role. Activated charcoal is not effective for lithium — lithium is a small monovalent ion, not an organic molecule, and charcoal does not adsorb it. Do not give activated charcoal for a pure lithium overdose [2].
Whole-bowel irrigation with polyethylene glycol solution, however, may be useful in the acute ingestion of a large quantity of lithium, particularly modified-release tablets that may form pharmacobezoars and release drug over many hours. The evidence is limited, and the decision is made with the toxicology service, weighing the risk of aspiration (in the drowsy or comatose patient) against the potential benefit of reducing ongoing absorption. Whole-bowel irrigation is contraindicated in the patient with an unprotected airway, ileus, or gastrointestinal obstruction. [1]
The practical point: in the chronic accumulation pattern (the most common), there is no role for gastrointestinal decontamination — the overdose is not acute, the drug has already been fully absorbed, and the problem is reduced clearance. Decontamination is a consideration only in the genuine acute overdose, guided by the toxicology service [2].
Step 3 — Haemodialysis (the EXTRIP criteria)
Lithium is ideal for haemodialysis: it has a small molecular weight, it is water-soluble, it is not protein-bound, and it has a small volume of distribution. Intermittent haemodialysis can reduce the serum lithium level rapidly. The EXTRIP (Extracorporeal Treatments in Poisoning) Workgroup published a systematic review and consensus guideline in 2015 that is the current standard for when to dialyse [1].
The EXTRIP recommendations: [1]
| Indication | EXTRIP grade | Detail |
|---|---|---|
| Severe lithium poisoning (clinical judgement) | Recommended (1D) | The decision integrates level, symptoms, and renal function |
| Level above 4.0 mmol/L | Recommended (1D) | Regardless of symptoms — dialyse |
| Renal impairment and level above 4.0 | Recommended (1D) | The kidney cannot clear it |
| Level above 5.0 mmol/L | Suggested (2D) | Even without severe symptoms |
| Significant confusion | Suggested (2D) | A symptom-based threshold |
| Expected time to level below 1.0 exceeds 36 hours | Suggested (2D) | A kinetic threshold |
Intermittent haemodialysis is the preferred modality (1D). Continuous renal replacement therapy (CRRT) is an acceptable alternative if haemodialysis is unavailable, but it clears lithium more slowly. The EXTRIP guidance is to continue extracorporeal treatment until there is clear clinical improvement or the level is below 1.0 mmol per litre — and if the level is not readily measurable, a minimum of 6 hours of treatment is recommended [1].
DWE high-yield: The EXTRIP criteria are exam gold. Memorise them: dialyse above 4.0 regardless of symptoms; dialyse above 2.5 with symptoms; dialyse for seizures or decreased consciousness irrespective of the level; dialyse for renal failure not responding to fluids. The preference is intermittent haemodialysis over CRRT [1].

Step 4 — Post-dialysis rebound monitoring
Post-dialysis rebound is the rule, not the exception. Lithium redistributes from the tissue compartment (which holds the vast majority of the body burden) back into the plasma after a dialysis session lowers the serum level. The level can rebound above the toxic threshold within 4 to 6 hours of completing dialysis. The EXTRIP guidance is to obtain serial lithium measurements over 12 hours after stopping extracorporeal treatment to determine whether a further session is required [1][2]. In practice, check a level at 4 to 6 hours post-dialysis, and repeat the session if it has rebounded significantly. Some centres use a continuous low-dose dialysis or CRRT after the initial intermittent session to blunt the rebound.
Step 5 — The role of sodium bicarbonate
Sodium bicarbonate can enhance renal lithium excretion by alkalinising the urine and increasing lithium solubility, but it is much less effective than haemodialysis and is not a substitute for dialysis in the patient who meets the criteria. It may have a role as an adjunct in the patient who does not meet dialysis criteria, but it must be used carefully — aggressive alkalinisation can cause hypokalaemia, fluid overload, and a shift in the calcium and potassium that complicate the picture. Normal saline alone is the standard [2].
Monitoring during management
During active management, check the serum lithium level every 2 hours until it is clearly falling and the patient is clinically improving. Monitor the renal function, the electrolytes (especially sodium and potassium), the ECG (for QT prolongation), the temperature (for hyperthermia), and the neurological state (Glasgow Coma Scale, seizure activity) continuously. Involve the toxicology service and the nephrology team early — the decision to dialyse and the management of the rebound are multidisciplinary [1][2].
Monitoring the patient on long-term lithium — prevention is the best management
The best management of lithium toxicity is prevention. A structured monitoring program catches the rising level, the falling GFR, and the developing end-organ effect before they become emergencies. The RANZCP clinical practice guidelines for mood disorders and the NICE guideline (CG185) provide the framework. [1]
Baseline (before starting lithium)
- Renal function — creatinine, eGFR, urinalysis
- Thyroid function — TSH, free T4
- Calcium — corrected serum calcium
- Full blood count
- ECG (especially in older patients or those with cardiac disease)
- Pregnancy test in women of childbearing age (lithium is teratogenic, Ebstein anomaly)
- Body weight and BMI
- Counselling on the signs of toxicity, the need for hydration during illness, and the drug interactions [1]
During therapy
| Parameter | Frequency |
|---|---|
| Serum lithium level (12-hour trough) | Every 1 to 2 weeks until stable, then every 3 months |
| Renal function (creatinine, eGFR) | Every 3 months in the first year, then every 6 months |
| Thyroid function (TSH) | Every 3 months in the first year, then every 6 months |
| Calcium | Every 6 to 12 months |
| Weight | Every 6 months |
DWE high-yield: The serum lithium level is a 12-hour trough — drawn 12 hours after the last dose. A level drawn sooner reflects the absorption peak and will be falsely high. The target range (0.6 to 1.0 for maintenance) is defined for the 12-hour trough. This is a classic pharmacology MCQ point [3].
The differential diagnosis of the toxic patient on lithium
When a patient on lithium presents acutely unwell, several conditions mimic lithium toxicity and must be distinguished: [1]
- Serotonin syndrome — if the patient is also on an SSRI, SNRI, or tramadol. Look for clonus (highly specific), hyperreflexia, autonomic instability, and rigidity. The clonus and the rapid onset distinguish it from lithium toxicity, which has a more subacute course and prominent ataxia.
- Neuroleptic malignant syndrome — if the patient is on an antipsychotic. Look for lead-pipe rigidity, profound hyperthermia, and a markedly raised creatine kinase.
- Hepatic encephalopathy — check the liver function and ammonia.
- Wernicke encephalopathy — especially in the malnourished or alcoholic patient; give thiamine empirically.
- Meningoencephalitis — fever, meningism, and a lumbar puncture.
- Psychiatric relapse — but never assume confusion or ataxia in a patient on lithium is psychiatric until toxicity and the other organic differentials are excluded. [1]
The serum lithium level and the clinical context usually resolve the differential, but the mimic is the trap: treating lithium toxicity as serotonin syndrome with cyproheptadine, or as NMS with dantrolene, will not address the rising lithium and will delay dialysis [2].
Long-term management decisions — continue, reduce, or switch
A patient who has recovered from an episode of toxicity, or whose renal function is progressively declining, presents a longitudinal decision that the physician must navigate jointly with the psychiatrist and the patient. [1]
The decision balances the proven benefit of lithium (unmatched for mania prophylaxis, bipolar depression prophylaxis, and suicide prevention) against the accumulating harm (progressive CKD, the risk of irreversible neurotoxicity, the thyroid and parathyroid effects). The evidence is reassuring on the renal trajectory in most patients — the decline is usually slow and the absolute risk of ESRD is small — but the precautionary principle demands that a patient with a progressive or accelerating decline in renal function is assessed for a switch [3].
The alternatives to lithium for bipolar prophylaxis include valproate (with its own monitoring and teratogenicity profile), lamotrigine (particularly for bipolar depression prophylaxis), and the atypical antipsychotics (quetiapine, olanzapine, aripiprazole, lurasidone), each with its own adverse-effect profile. The choice depends on the patient's response history, the polarity of their illness, and their comorbidities. The physician's role is to present the evidence, to coordinate the renal and endocrine monitoring, and to support the shared decision — not to make the psychiatric prescribing decision alone [3].
The common exam traps
- Treating the serum level in isolation — always interpret the level with the clinical pattern. A level of 3.0 in acute overdose is less dangerous than 2.5 in chronic toxicity.
- Missing the drug interaction — thiazides, ACE inhibitors, ARBs, and NSAIDs all raise lithium levels. Any new prescription in a lithium-treated patient is a potential precipitant.
- Failing to dialyse when indicated — seizures, decreased consciousness, and life-threatening dysrhythmias are indications for dialysis irrespective of the serum level. Do not wait for a confirmatory level.
- Forgetting the post-dialysis rebound — lithium redistributes from the tissues after dialysis. Check a level at 4 to 6 hours and be prepared to repeat the session.
- Giving loop diuretics — they paradoxically raise the lithium level by increasing distal sodium delivery and proximal lithium reabsorption. Normal saline is the correct fluid.
- Drawing the level at the wrong time — the target ranges are for the 12-hour trough. A random level is uninterpretable unless the time of the last dose is known.
- Missing the chronic end-organ effects — every patient on long-term lithium needs renal, thyroid, and calcium monitoring. A rising creatinine or a high calcium is lithium-related until proven otherwise.
- Confusing the tremors — the coarse tremor of toxicity (6 to 8 Hz, at rest and on action) is distinct from the fine therapeutic tremor and the Parkinsonian resting tremor [1][2][3].
Regional guideline anchoring
- ANZ (RANZCP) — the RANZCP clinical practice guidelines for mood disorders (Malhi et al, 2015) provide the lithium monitoring framework: 12-hour trough levels, 3-monthly renal and thyroid in the first year then 6-monthly, calcium at baseline and annually. The ANZ Poisons Information Centre (13 11 26) and TOXINZ are the toxicology resources. Haemodialysis access and the EXTRIP criteria are the standard.
- UK (NICE) — NICE CG185 (bipolar disorder) recommends lithium as a first-line maintenance option, with monitoring broadly aligned with the RANZCP schedule.
- US — the American Psychiatric Association guideline and the EXTRIP criteria are the references for dialysis decisions in ABIM-style questions. [1]
Drug doses are verified. Lithium is dosed as lithium carbonate, typically 400 to 1200 mg per day in divided doses (or once daily for modified release), titrated to the 12-hour trough level. The ANZ brand is Lithicarb (carbonate). No specific antidote exists for lithium toxicity — the management is extracorporeal removal and supportive care [1][2].
Summary
Lithium toxicity is the clinical consequence of a narrow-therapeutic-index, entirely renally cleared drug whose clearance is vulnerable to dehydration, drug interactions (thiazides, ACE inhibitors, ARBs, NSAIDs), and acute or chronic kidney disease. The three clinical patterns (acute, acute-on-chronic, chronic) differ in the relationship between the serum level and the clinical effect, and the serum level must always be interpreted with the clinical context. Mild toxicity (1.5 to 2.5 mmol per litre) presents with a coarse tremor, gastrointestinal symptoms, ataxia, and hyperreflexia; severe toxicity (above 2.5) progresses to seizures, coma, hyperthermia, QT prolongation, and myoclonus. Management is stop-lithium, ABCDE, aggressive intravenous normal saline, and haemodialysis by the EXTRIP criteria (above 4.0 regardless; above 2.5 with symptoms; seizures or decreased consciousness irrespective of level; renal failure not responding to fluids), with mandatory post-dialysis rebound monitoring. The chronic end-organ effects — nephrogenic diabetes insipidus, chronic interstitial nephritis, hypothyroidism, hyperparathyroidism, and SILENT — require structured lifelong surveillance. [1]
One-line answer for the viva: "I manage lithium toxicity by first stopping the drug and resuscitating with ABCDE and intravenous normal saline to enhance renal excretion. I interpret the serum level with the clinical pattern — chronic toxicity at 2.5 is more dangerous than acute toxicity at 3.0 because the tissue compartment is already saturated. I dialyse by the EXTRIP criteria — above 4.0 regardless of symptoms, above 2.5 with symptoms, seizures or decreased consciousness irrespective of level, and renal failure not responding to fluids — using intermittent haemodialysis, and I check a post-dialysis rebound level at 4 to 6 hours because lithium redistributes from the tissues. I avoid loop diuretics, which paradoxically raise the level. Every patient on long-term lithium needs structured renal, thyroid, and calcium monitoring, and I work with the psychiatrist to decide whether to continue, dose-reduce, or switch after an episode of toxicity." [1]
References
- [1]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [2]Baird-Gunning J, Lea-Henry T, Hoegberg LCG, Gosselin S, Roberts DM Lithium Poisoning J Intensive Care Med, 2017.PMID 27516079
- [3]McKnight RF, Adida M, Budge K, Stockton S, Goodwin GM, Geddes JR Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699