Phys · pharmacological
Paracetamol Toxicity
Also known as acetaminophen toxicity · paracetamol overdose · paracetamol poisoning · acetaminophen poisoning · NAPQI hepatotoxicity · paracetamol-induced acute liver failure · N-acetylcysteine therapy
Consultant-physician-depth guide to paracetamol (acetaminophen) toxicity — CYP2E1 metabolism to NAPQI and glutathione depletion, the toxic dose in acute and staggered overdose, the four-stage clinical course, the Rumack-Matthew nomogram, the 21-hour N-acetylcysteine regimen, adverse reactions to NAC, and the King's College Criteria for transplant referral. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Paracetamol Toxicity
The answer first
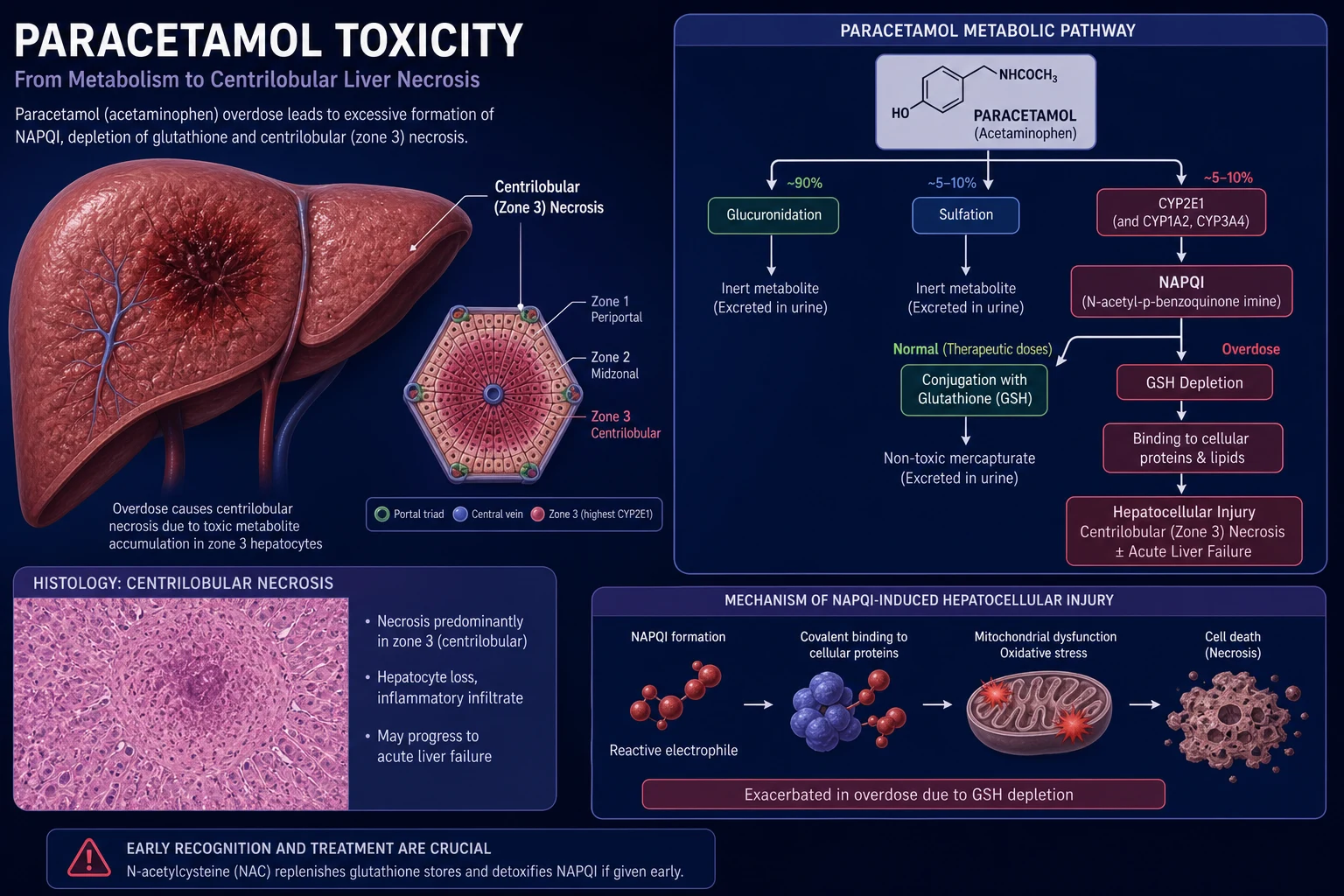
Paracetamol (acetaminophen) is the single most important overdose a physician must master, because it is the leading cause of acute liver failure in the developed world and the one overdose in which an antidote given early prevents death. The mechanism is tight and examinable: in overdose the drug's minor oxidative pathway through CYP2E1 produces the reactive metabolite N-acetyl-p-benzoquinone imine (NAPQI), which overwhelms hepatic glutathione and binds covalently to hepatocyte proteins, causing centrilobular (zone 3) necrosis [7].
Three rules govern everything that follows: [1]
- The early stage is asymptomatic, and that is exactly when N-acetylcysteine (NAC) works. The decision to treat is driven by the paracetamol level and the time of ingestion, never by how well the patient looks [3].
- The Rumack-Matthew nomogram applies only to a single acute ingestion with a known time. Staggered, repeated-supratherapeutic, or unknown-time overdoses are treated empirically — the nomogram does not work and these patients do worse [8].
- Once acute liver failure is established, the question becomes transplant. The King's College Criteria (a UK product, applied worldwide) define who is referred, and arterial lactate gives you the answer hours earlier [4][6].
DCE trap: In every overdose long case, name the ingestion pattern first. "Single acute, known time — nomogram applies" is a very different patient from "staggered over two days — nomogram invalid, treat empirically, worse prognosis." The pattern drives the entire management plan. [1]
Pathophysiology — the mechanism that explains the management
Paracetamol is absorbed rapidly and reaches peak serum concentration within 30 to 60 minutes (faster with the liquid formulation). In a healthy adult at therapeutic dose the liver handles it through three pathways [7]:
| Pathway | Fraction | Enzyme | Product | Fate |
|---|---|---|---|---|
| Glucuronidation | 40 to 67 per cent | UGT | Glucuronide conjugate | Renal excretion |
| Sulfation | 20 to 46 per cent | SULT | Sulfate conjugate | Renal excretion |
| Oxidation | 5 to 15 per cent | CYP2E1 (mainly), CYP1A2, CYP3A4 | NAPQI | Conjugated by glutathione to non-toxic mercapturic acid |
The oxidative pathway is the entire story. NAPQI is the toxic metabolite. In health it is mopped up immediately by conjugation with glutathione. In overdose, two things happen: the glucuronidation and sulfation pathways saturate, and a larger fraction of the drug is shunted through CYP2E1 to NAPQI; and hepatic glutathione stores are consumed. When glutathione falls to roughly 30 per cent of normal, free NAPQI accumulates and binds covalently to cysteine residues on hepatocyte proteins, forming stable protein adducts [7]. The adducted proteins are principally mitochondrial. The downstream consequences are mitochondrial dysfunction, adenosine triphosphate depletion, oxidative stress, disruption of calcium homeostasis, and — over the next 24 to 72 hours — coagulative necrosis of the hepatocytes.
The necrosis is centrilobular (zone 3). This is not accidental. The hepatocytes around the central vein have the highest CYP2E1 expression and the lowest oxygen tension in the acinus, making them the most vulnerable to NAPQI adduct formation and the least able to withstand oxidative injury. On histology you see a sharp band of necrosis around the central veins with a preserved periportal rim — the architecture that explains why the patient may survive even massive injury (the periportal hepatocytes regenerate). [1]
DWE high-yield: The mechanism is NAPQI, the cell is the hepatocyte, the region is zone 3, the enzyme is CYP2E1, and the protective molecule is glutathione. If you can hold those five facts together you can answer every paracetamol mechanism question. [1]
What increases NAPQI and lowers the toxic threshold
Anything that induces CYP2E1 or depletes glutathione moves a patient onto the high-risk treatment line (a lower threshold for NAC). The clinically important inducers and depleters: [1]
- Chronic alcohol use — induces CYP2E1 and depletes glutathione through malnutrition; this is the most tested high-risk factor.
- Isoniazid — a potent CYP2E1 inducer; patients on tuberculosis treatment are at markedly increased risk.
- Fasting, malnutrition, anorexia, chronic illness, HIV, decompensated cirrhosis — glutathione depletion.
- Other enzyme inducers — rifampicin, carbamazepine, phenytoin, phenobarbitone, zidovudine, St John's wort. [1]
These are the patients for whom the 4-hour treatment line is 150 mg/L rather than 200 mg/L, and for whom a staggered or chronic ingestion is dangerous at doses that would be safe in a well-nourished adult [7].
Toxic dose — acute, staggered, and chronic
| Ingestion pattern | Toxic threshold in an adult | Nomogram | Threshold for NAC |
|---|---|---|---|
| Single acute, healthy adult | 150 mg/kg or 10 g (whichever is less) | Applies | Level above standard 200 mg/L line |
| Staggered over more than 1 to 2 hours | Any dose above 4 g per day | Does NOT apply | Treat empirically if any detectable paracetamol or AST elevation |
| Repeated supratherapeutic (chronic) | Above 4 g per day (above 60 mg/kg per day in children) | Does NOT apply | Treat if detectable paracetamol plus AST above reference range |
| Unknown time of ingestion | Assume the worst | Does NOT apply | Treat empirically |
The acute toxic dose of 150 mg/kg or 10 g in an adult (whichever is lower) is the number to remember. In children the figure is the same per kilogram: 150 mg/kg. A therapeutic adult dose is 0.5 to 1 g every four to six hours up to a maximum of 4 g per day (4 g in a well adult; 2 to 3 g per day in chronic alcohol use, malnutrition, or the elderly). The margin between therapy and toxicity is narrow, which is why repeated supratherapeutic dosing is dangerous [7].
Staggered overdose — taking multiple doses over hours or days — is the trap. These patients often ingest a smaller total dose than a single-overdose patient, present later, and look worse. Craig and colleagues showed that staggered overdose and delayed presentation beyond 24 hours are independently associated with higher rates of encephalopathy, mechanical ventilation, renal replacement therapy, and death, and that the King's College Criteria have reduced sensitivity in this group [8]. The clinical rule is simple: do not use the nomogram in staggered overdose — treat empirically and involve the liver unit early.
Clinical course — the four stages
The clinical course unfolds over four stages. Memorising the timing is the most efficient way to organise the long case, because the stage determines the likely problems and the monitoring strategy. [1]
| Stage | Timing | Clinical features | Laboratory |
|---|---|---|---|
| 1 | 0 to 24 hours | Asymptomatic, or nausea, vomiting, malaise, pallor, diaphoresis. The patient looks well. | AST and ALT normal. Paracetamol level may be high. INR normal. |
| 2 | 24 to 72 hours | Right upper quadrant pain, tender hepatomegaly. Nausea may ease — the patient is "improving" while the liver is dying. | AST and ALT rise (can exceed 10 000 U/L). INR begins to climb. Creatinine rises. |
| 3 | 72 to 96 hours | Peak hepatotoxicity: jaundice, encephalopathy, coagulopathy, acute kidney injury, hypoglycaemia, metabolic acidosis. Multi-organ failure. | AST and ALT peak then fall (not a sign of recovery — the cells are dead). INR at its highest. Lactate high. Phosphate low. |
| 4 | Days to weeks | Recovery in survivors, or progression to death or transplant. Hepatic regeneration begins. | INR falls, AST falls, renal and cerebral function recover. |
DCE trap: The stage 2 "improvement" is a classic exam pitfall. The patient who was vomiting at 12 hours and feels better at 36 hours is not recovering — the nausea is subsiding as the drug is cleared, but the hepatocyte injury is only beginning. The transaminases tell the truth. This is why you do not discharge an overdose patient at 24 hours without an ALT and INR. [1]
Progression to acute liver failure
Acute liver failure is defined by encephalopathy in the setting of acute hepatic injury without pre-existing chronic liver disease. In paracetamol toxicity the other hallmarks are coagulopathy (rising INR), jaundice (less prominent early than the transaminitis), hypoglycaemia (impaired gluconeogenesis), metabolic acidosis with elevated lactate, acute kidney injury (a direct NAPQI effect on the proximal tubule, not only hepatorenal physiology), and in grade 3 to 4 encephalopathy the risk of cerebral oedema. Paracetamol is the prototype cause of hyperacute liver failure — encephalopathy develops within 7 days of the insult — which is why the clinical course is so compressed and the transplant window so narrow [4].
Investigations
The paracetamol level and the Rumack-Matthew nomogram
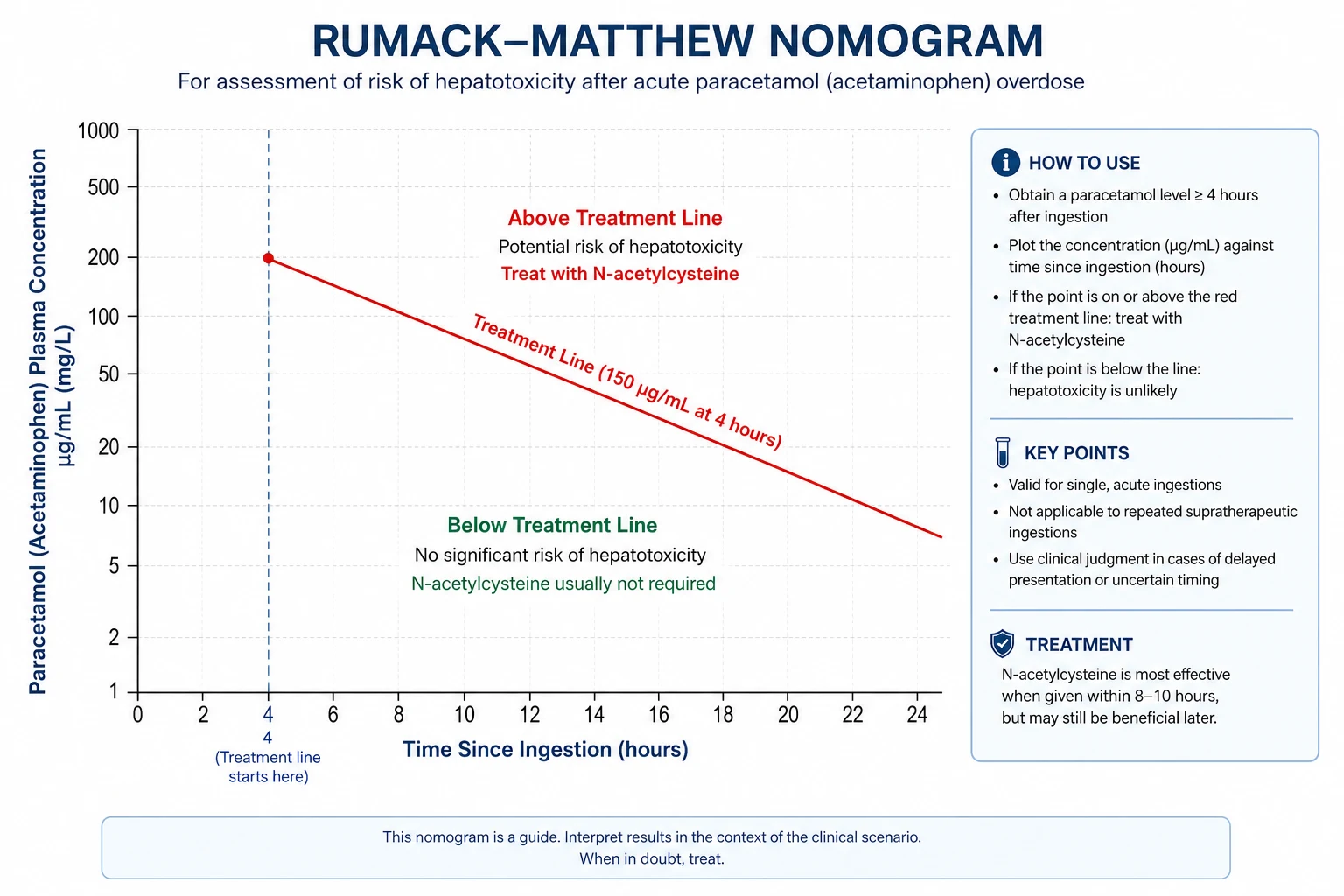
The serum paracetamol level taken at 4 hours after a single ingestion is the pivotal investigation. Drawn before 4 hours it cannot be interpreted because absorption is ongoing and the level will keep rising. Drawn between 4 and 24 hours it is plotted on the Rumack-Matthew nomogram — the treatment-decision tool introduced by Rumack and Matthew in 1975 [1].
The nomogram plots paracetamol concentration (mg/L on a logarithmic axis) against time after ingestion (hours on a linear axis). Two treatment lines run from a concentration at 4 hours down to zero at 16 hours: [1]
- Standard treatment line — 200 mg/L at 4 hours. For a healthy adult without risk factors.
- High-risk treatment line — 150 mg/L at 4 hours. For patients with CYP2E1 induction or glutathione depletion (chronic alcohol, isoniazid, malnutrition, fasting, decompensated cirrhosis). [1]
If the plotted level lies on or above the relevant treatment line, NAC is indicated. If it lies below, hepatotoxicity is very unlikely and NAC is not required — provided the ingestion was genuinely a single acute event with a reliable time [1][3].
DWE trap: The nomogram is valid only for a single acute ingestion with a known time of ingestion between 4 and 24 hours. It cannot be used for staggered overdose, repeated supratherapeutic ingestion, unknown-time ingestion, or co-ingestion with a delayed-absorption agent. In all of those, treat empirically. [1]
The full blood panel
Beyond the level, every paracetamol overdose patient should have: [1]
- Liver function tests — AST, ALT, bilirubin, albumin. The transaminases can exceed 10 000 U/L in stage 3; a falling AST late in the course is not recovery but cell death.
- Coagulation — INR and prothrombin time. The INR is the single most important prognostic marker and a King's College Criterion. Do not routinely correct the INR with fresh frozen plasma in a patient being assessed for transplant — it destroys your prognostic information. Reserve correction for active bleeding or before invasive procedures.
- Renal function and creatinine — acute kidney injury is common (up to 25 per cent of severe overdoses) and is a direct NAPQI effect on the proximal tubule.
- Venous or arterial blood gas with lactate — the lactate is an early predictor of outcome (see King's College Criteria); the pH defines acidosis and is itself a criterion.
- Glucose — hypoglycaemia reflects impaired gluconeogenesis and is a poor prognostic sign.
- Phosphate — hypophosphataemia (below 0.5 mmol/L) at 48 to 96 hours is associated with poor outcome and reflects renal injury and ATP depletion. [1]- Amylase and lipase — paracetamol can cause pancreatitis.
- Beta-hCG in women of childbearing age.
- Salicylate level and ethanol level on every overdose patient — co-ingestion is common.
- Viral serology, autoimmune markers, ceruloplasmin and urinary copper (in patients under 40), and a Doppler ultrasound of the hepatic vessels — to exclude other causes of acute liver failure. [1]
Management
Step 1 — Immediate assessment and decontamination
Take a focused history (amount, formulation, time of each dose, co-ingestants, risk factors) and examine for encephalopathy, hydration, and signs of chronic liver disease. Assess and protect the airway if the patient is drowsy or has co-ingested sedatives. [1]
Activated charcoal — 50 g orally (1 g/kg in children) — reduces absorption and is given within 1 to 2 hours of ingestion if the airway is protected. Beyond 2 hours the benefit falls, but it can still be considered for a massive or staggered ingestion or where a sustained-release or delayed-absorption formulation is involved. Charcoal given before the 4-hour level is back can reduce the proportion of patients who need NAC, because it lowers the peak level. Charcoal does not significantly reduce the efficacy of subsequent intravenous NAC [7].
DWE rule: Activated charcoal is the answer when the question says "within 1 to 2 hours, airway protected, large ingestion." It is not the answer when the patient is drowsy without a protected airway, or more than 2 to 4 hours have passed (unless sustained-release). [1]
Step 2 — The N-acetylcysteine decision
N-acetylcysteine is the antidote. It is a glutathione precursor that replenishes hepatic glutathione and allows conjugation of NAPQI. It also enhances sulfation, scavenges free radicals, and — in established liver failure — improves microcirculatory oxygen delivery and mitochondrial function [5][7].
Start NAC if any of the following is true: [1]
- The 4-hour paracetamol level is on or above the relevant treatment line (200 mg/L standard, 150 mg/L high-risk).
- The ingestion was staggered over more than 1 to 2 hours, or was a repeated supratherapeutic ingestion.
- The time of ingestion is unknown.
- Presentation is more than 8 to 10 hours after a significant ingestion (the level is less reliable as the window closes — treat first, confirm with the level).
- There is already any evidence of hepatotoxicity (AST or ALT elevation, INR rise) with a detectable paracetamol level. [1]
The safety margin of NAC is wide and the cost of a course is trivial. When in doubt, treat. The risk of hepatotoxicity from a missed course is real; the risk of an unnecessary course is a reversible reaction and a day in hospital. [1]
Step 3 — The 21-hour intravenous regimen
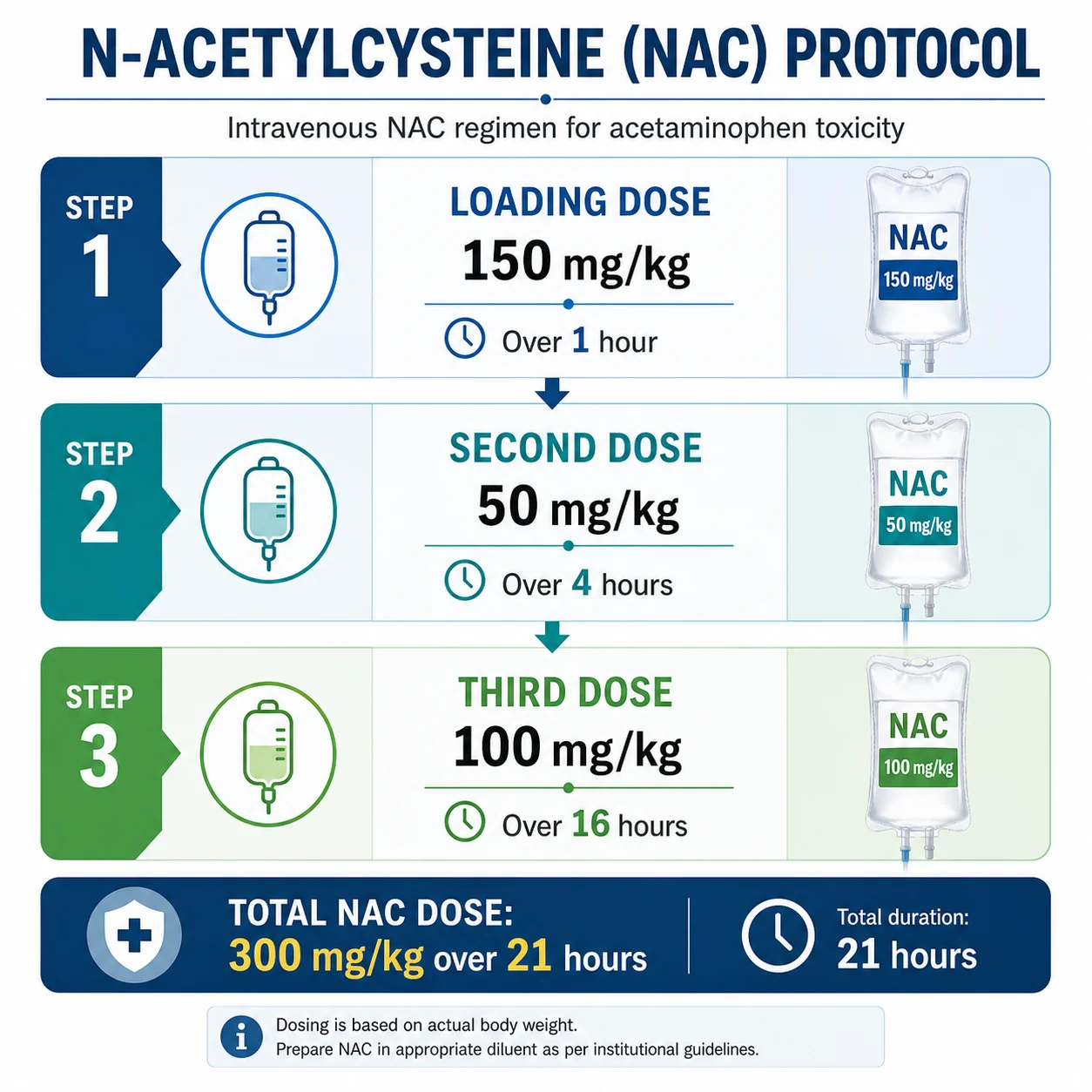
The standard ANZ and UK regimen is the 21-hour intravenous course, which has replaced the older 72-hour oral course because it is shorter, reliably bioavailable, better tolerated (no vomiting), and at least as effective [2][3].
| Bag | Dose | Diluent | Duration | Cumulative |
|---|---|---|---|---|
| 1 (loading) | 150 mg/kg | 200 mL 5 per cent dextrose | over 1 hour | 150 mg/kg |
| 2 | 50 mg/kg | 500 mL 5 per cent dextrose | over 4 hours | 200 mg/kg |
| 3 | 100 mg/kg | 1000 mL 5 per cent dextrose | over 16 hours | 300 mg/kg |
Total: 300 mg/kg over 21 hours. In children and fluid-restricted adults, reduce the diluent volume accordingly. The loading bag delivers the antidote fastest during the window when NAPQI is actively forming [2].
Step 4 — When to continue NAC beyond 21 hours
In a patient who presents early and whose liver function is normal, 21 hours is sufficient: stop the infusion, check the INR and ALT (they should be normal), recheck the paracetamol level (it should be below 10 mg/L), and discharge once medically and psychiatrically cleared. [1]
In a patient who has established hepatotoxicity, NAC is continued beyond 21 hours using a modified prolonged regimen (the same rate as the third bag, 100 mg/kg over 16 hours, repeated). The endpoint is a falling INR below 1.3, a falling AST, an undetectable paracetamol level, and clinical recovery. Keays and colleagues showed that even after fulminant hepatic failure has developed, intravenous NAC improves survival, reduces cerebral oedema, and reduces the need for inotropes — so the antidote is not only preventive [5].
Step 5 — Adverse reactions to NAC
Adverse reactions occur in up to 20 per cent of patients, almost always during the 1-hour loading bag. The mechanism is non-IgE-mediated mast-cell activation and the reactions are rate-related, not true allergy [7].
| Severity | Features | Management |
|---|---|---|
| Mild | Flushing, warmth, itch, transient urticaria | Slow or pause the infusion; the reaction usually settles; an antihistamine (chlorphenamine 4 to 8 mg) may help; restart at half the rate once settled |
| Moderate | Widespread urticaria, mild bronchospasm, angioedema | Stop the infusion; chlorphenamine and hydrocortisone; restart at a slower rate once settled, with monitoring |
| Severe (anaphylactoid) | Bronchospasm, hypotension, oxygen desaturation | Stop the infusion; intramuscular adrenaline 0.5 mg; oxygen; IV fluids; ICU involvement; discuss with toxicology before re-challenge |
The key principle: most reactions are rate-related and do not contraindicate continuing NAC. Stop, treat the reaction, and restart at a slower rate. Permanent cessation is reserved for true anaphylaxis and is rare. The two-bag (modified) regimen, which uses a slower initial bag (200 mg/kg over 4 hours rather than 150 mg/kg over 1 hour), has been adopted in some centres specifically to reduce these reactions [7].
Acute liver failure and the King's College Criteria
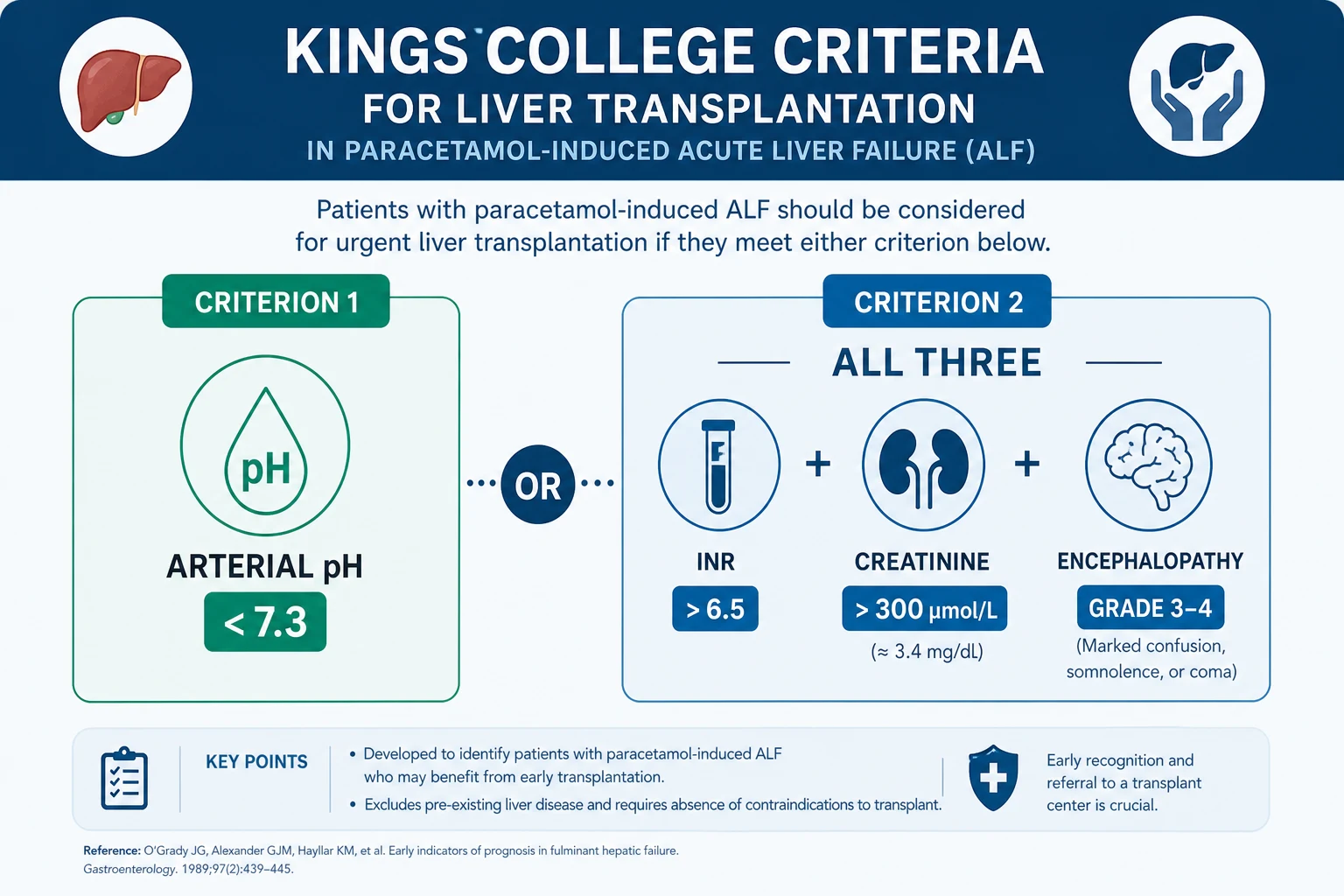
When hepatotoxicity progresses to acute liver failure, the central question becomes liver transplantation. The King's College Criteria, derived from the 1989 King's College Hospital cohort, remain the most widely used and best-validated prognostic tool for paracetamol-induced acute liver failure [4].
For paracetamol-induced acute liver failure, the criteria are met and transplant referral is indicated if either: [1]
- Arterial pH below 7.3 after adequate fluid resuscitation, OR
- All three of the following are present (within a 24-hour window):
- INR above 6.5 (prothrombin time above 100 seconds)
- Serum creatinine above 300 micromol/L
- Grade 3 or 4 hepatic encephalopathy [1]
DCE trap: The logic is "pH alone OR (INR AND creatinine AND encephalopathy)." A single criterion — the arterial pH — is sufficient for referral. But the second limb requires all three components; two of three does not meet the criterion. This is the single most examined fact in paracetamol toxicology. [1]
Arterial lactate — the early predictor
The King's College Criteria are highly specific but only moderately sensitive, and they declare themselves late — often only after irreversible injury. Bernal and colleagues showed that arterial lactate identifies non-survivors substantially earlier [6]. The thresholds:
- Arterial lactate above 3.5 mmol/L on early admission (before fluid resuscitation), OR
- Arterial lactate above 3.0 mmol/L after fluid resuscitation (around 12 hours after admission). [1]
These lactate thresholds have similar predictive accuracy to the King's College Criteria combined but identify poor outcome at a median of 4 hours versus 10 hours, buying critical time for transplant workup and transfer [6].
Managing the complications of acute liver failure
Once acute liver failure is established, management moves to an intensive care or specialist liver unit. The problems and their management: [1]
| Complication | Management |
|---|---|
| Encephalopathy | Grade and monitor; lactulose (limited evidence but widely used); head of bed elevated 30 degrees; avoid sedatives; intubate for grade 4 or airway protection |
| Cerebral oedema | Mannitol 0.5 g/kg or hypertonic saline to a sodium of 145 to 155; neuroprotection (normocapnia, normoglycaemia, normothermia); consider intracranial pressure monitoring in grade 4 |
| Hypoglycaemia | 10 per cent dextrose infusion; monitor hourly; target glucose above 4 mmol/L |
| Acute kidney injury | Continuous renal replacement therapy (preferred over intermittent haemodialysis for haemodynamic stability); NAC continued |
| Infection | Surveillance cultures; low threshold for broad-spectrum antibiotics (sepsis precipitates encephalopathy and is frequently fatal); antifungal cover if prolonged |
| Haemodynamics | Noradrenaline for vasodilatory shock; adrenaline if myocardial depression; adrenal insufficiency common — consider physiological hydrocortisone in refractory shock |
Special situations
Staggered and repeated-supratherapeutic overdose
The nomogram does not apply. Treat empirically if there is any detectable paracetamol and any AST elevation, or if the daily intake has exceeded 4 g in an adult (60 mg/kg per day in a child) over more than 1 to 2 hours, especially with risk factors. These patients present later, have established injury, and the King's College Criteria are less sensitive in them — so involve the liver unit early and have a low threshold for transplant referral [8].
Pregnancy
Paracetamol crosses the placenta. The fetus is at risk because fetal CYP2E1 activity is low but maternal glutathione is shared; maternal hepatotoxicity threatens the fetus directly. NAC is safe in pregnancy and crosses the placenta. Treat on the standard nomogram, with a lower threshold to treat because the consequence of missing hepatotoxicity is fetal loss. Paracetamol overdose in pregnancy is not an indication for termination or delivery in itself — manage the overdose first [7].
Chronic alcohol use
Chronic alcohol induces CYP2E1 and depletes glutathione, so these patients are treated on the high-risk (150 mg/L) treatment line. Acute alcohol co-ingestion does not reliably protect (despite competitive CYP2E1 inhibition), and should not change management. Plan for alcohol withdrawal prophylaxis during the admission. [1]
The elderly and patients with chronic liver disease
Pre-existing cirrhosis depletes glutathione and impairs regeneration, so the toxic threshold is lower and the outcome worse. The maximum daily therapeutic dose in chronic alcohol users, the malnourished, and the frail elderly should be 2 to 3 g per day, not 4 g. Elderly patients are also more likely to be taking a paracetamol-containing combination analgesic and to present with staggered overdose. [1]
Differentials in the patient with acute liver injury
When the history is uncertain, keep a structured differential for acute liver injury with a paracetamol history: [1]
| Cause | Discriminator |
|---|---|
| Ischaemic hepatitis (shock liver) | A hypotensive episode (sepsis, cardiac arrest, heart failure); AST and ALT fall rapidly over days; no paracetamol level |
| Viral hepatitis (A, B, E) | Travel, risk factors, prodrome; serology positive; AST and ALT in the thousands but bilirubin more prominent |
| Autoimmune hepatitis | Young to middle-aged woman; high IgG; positive ANA, SMA, anti-LKM1 |
| Wilson disease (acute) | Patient under 40; Coombs-negative haemolytic anaemia; low ceruloplasmin; high urinary copper; Kayser-Fleischer rings |
| Budd-Chiari syndrome | Tender hepatomegaly, ascites; absent hepatic veins on Doppler |
| Drug-induced liver injury | Exposure history (amoxicillin-clavulanate, isoniazid, statins, antiepileptics, NSAIDs); eosinophilia; pattern of injury |
| Amanita phalloides poisoning | Mushroom meal; delayed vomiting and diarrhoea; multi-organ failure |
| Alcoholic hepatitis | Long history; AST to ALT ratio above 2; bilirubin high; AST below 400 |
In every patient with acute liver failure of unclear cause, send the paracetamol level — it may be the answer even when the history does not suggest it [4][7].
Long-term outcomes, follow-up, and prevention
Outcomes
With NAC given within 8 hours of a single acute ingestion, hepatotoxicity is prevented in over 90 per cent of patients and mortality is essentially zero [3]. Once acute liver failure develops, mortality without transplant is 20 to 40 per cent in paracetamol-induced failure (better than non-paracetamol causes, because regeneration is robust); with transplant, one-year survival exceeds 75 per cent. Patients who meet King's College Criteria and do not receive a transplant have a survival of around 20 per cent, which is why the criteria are a trigger for urgent referral [4].
Follow-up
After recovery, most patients return to full hepatic function within weeks to months because the liver regenerates. There is no chronic liver disease from a single paracetamol overdose in a previously well patient. Follow-up should focus on: [1]
- Psychiatric review and a safety plan before discharge; the risk of repeat overdose is highest in the first year.
- Substance use assessment — alcohol, opioids, benzodiazepines.
- Patient and family education on safe paracetamol dosing (4 g per day in a well adult; 2 to 3 g in chronic alcohol use and the elderly; check combination products).
- General practitioner follow-up with a repeat liver function test at 1 to 2 weeks to confirm resolution.
- Limited dispensing — advise the pharmacist and general practitioner to dispense small quantities. [1]
Prevention
Pack-size restrictions (blister packs, reduced pack sizes) and the move to unit-dose packaging have reduced the death rate from paracetamol overdose in the UK since their introduction in 1998. Combination analgesic products (for example, with an opioid) carry a particular risk of inadvertent staggered overdose and are increasingly restricted [7].
How this is examined
DWE MCQ — the high-yield patterns
- Nomogram application — a 4-hour level plotted against time; "treat above the line" is the answer. The trap is a staggered or unknown-time ingestion, where the answer is "treat empirically, nomogram does not apply."
- NAC regimen — a question on the loading dose (150 mg/kg over 1 hour) or the total course (300 mg/kg over 21 hours). The trap is confusing oral and IV dosing. [1]- King's College Criteria — the pH-alone-versus-all-three logic. The trap is two of three, which does not meet the criterion.
- Activated charcoal — within 1 to 2 hours, airway protected. The trap is charcoal at 6 hours.
- High-risk patient — chronic alcohol, isoniazid, malnutrition; treat on the 150 mg/L line. [1]
DCE long case — the overdose patient
The classic long case is a patient with chronic alcohol use, a staggered or late-presentation overdose, and evolving acute liver failure. Open with the pattern of ingestion, the stage, and the risk profile. Build a problem list that integrates the medical management (NAC, monitoring, transplant criteria), the comorbidity (alcohol withdrawal, malnutrition), and the psychosocial plan (psychiatric liaison, safeguarding). Be ready to apply the King's College Criteria live and to discuss the transplant decision and the ethics of transplantation in deliberate self-harm. [1]
DCE short case — the encephalopathic patient
A short case on assessing encephalopathy grade, examining for stigmata of acute liver failure (jaundice, asterixis, tender hepatomegaly, bruising), and presenting the findings synthesised into paracetamol-induced acute liver failure with the King's College Criteria applied. The trap is over-correcting the INR before the criteria are applied. [1]
References
Rumack BH, Matthew H. Acetaminophen poisoning and toxicity. Pediatrics 1975;55:871-876 (1134886); Prescott LF, Illingworth RN, Critchley JAJH, et al. Intravenous N-acetylcysteine: the treatment of choice for paracetamol poisoning. BMJ 1979;2:1097-1100 (519312); Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH. Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. N Engl J Med 1988;319:1557-1562 (3059186); O'Grady JG, Alexander GJM, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology 1989;97:439-445 (2490426); Keays R, Harrison PM, Wendon JA, et al. Intravenous acetylcysteine in paracetamol induced fulminant hepatic failure. BMJ 1991;303:1026-1029 (1954453); Bernal W, Donaldson N, Wyncoll D, Wendon J. Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure. Lancet 2002;359:558-563 (11867109); Hodgman MJ, Garrard AR. A review of acetaminophen poisoning. Crit Care Clin 2012;28:499-516 (22998987); Craig DGN, et al. Staggered overdose pattern and delay to hospital presentation are associated with adverse outcomes following paracetamol-induced hepatotoxicity. Br J Clin Pharmacol 2012;73:285-294 (22106945). Regional guidelines: Australian Therapeutic Guidelines — Toxicology; National Poisons Information Service / Toxbase (UK); AASLD Practice Guidance on Acute Liver Failure (2023); NICE Clinical Knowledge Summary — Paracetamol overdose. [1]
References
- [1]Rumack BH, Matthew H Acetaminophen poisoning and toxicity Pediatrics, 1975.PMID 1134886
- [2]Prescott LF, Illingworth RN, Critchley JAJH, et al. Intravenous N-acetylcystine: the treatment of choice for paracetamol poisoning Br Med J, 1979.PMID 519312
- [3]Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. Analysis of the national multicenter study (1976 to 1985) N Engl J Med, 1988.PMID 3059186
- [4]O'Grady JG, Alexander GJM, Hayllar KM, Williams R Early indicators of prognosis in fulminant hepatic failure Gastroenterology, 1989.PMID 2490426
- [5]Keays R, Harrison PM, Wendon JA, et al. Intravenous acetylcysteine in paracetamol induced fulminant hepatic failure: a prospective controlled trial BMJ, 1991.PMID 1954453
- [6]Bernal W, Donaldson N, Wyncoll D, Wendon J Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure: a cohort study Lancet, 2002.PMID 11867109
- [7]Hodgman MJ, Garrard AR A review of acetaminophen poisoning Crit Care Clin, 2012.PMID 22998987
- [8]Craig DGN, Bates CM, Davidson JS, Martin KG, Hayes PC, Simpson KJ Staggered overdose pattern and delay to hospital presentation are associated with adverse outcomes following paracetamol-induced hepatotoxicity Br J Clin Pharmacol, 2012.PMID 22106945