Phys · pharmacological
Pharmacokinetics in Organ Failure — Renal, Hepatic and Polypharmacy Dosing
Also known as pharmacokinetics · drug dosing in renal failure · drug dosing in hepatic failure · renal dose adjustment · hepatic dose adjustment · creatinine clearance · Cockcroft-Gault · CKD-EPI · eGFR · Child-Pugh · Child-Turcotte-Pugh · therapeutic drug monitoring · TDM · vancomycin AUC dosing · gentamicin extended interval dosing · Hartford nomogram · phenytoin free level · Sheiner-Tozer · Beers criteria · STOPP START criteria · polypharmacy · deprescribing · sick-day rules
Consultant-physician-depth guide to pharmacokinetic principles in organ failure — renal and hepatic dose adjustment, estimating renal function (Cockcroft-Gault and the 2021 CKD-EPI race-free equation with its limitations), the water-soluble vs lipid-soluble drug distinction, Child-Pugh hepatic dosing, therapeutic drug monitoring (vancomycin AUC, aminoglycoside extended-interval dosing, phenytoin free levels, digoxin, lithium), drug-induced organ failure, and polypharmacy in the elderly (Beers criteria, STOPP/START). Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Pharmacokinetics in Organ Failure — Renal, Hepatic and Polypharmacy Dosing
The answer first
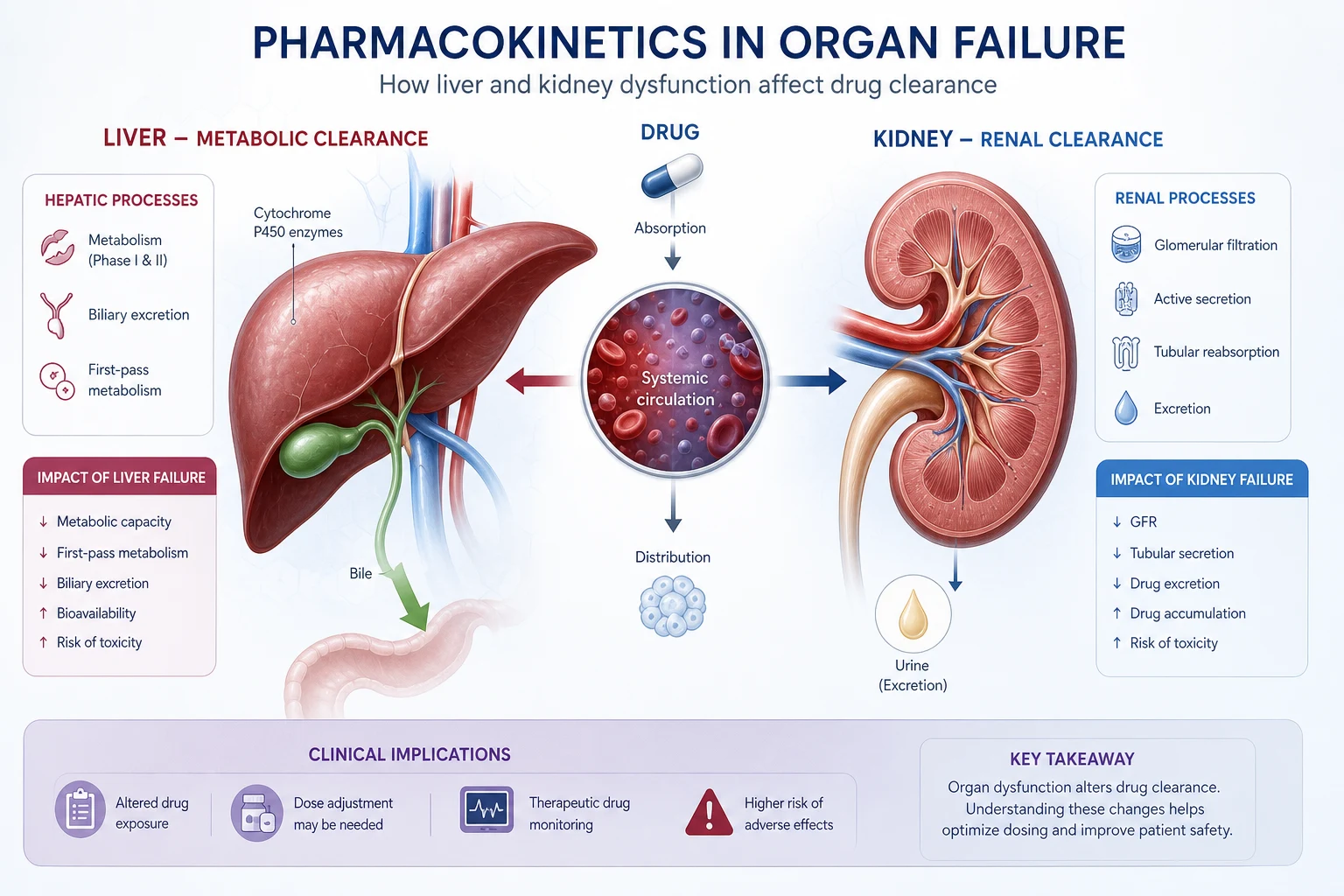
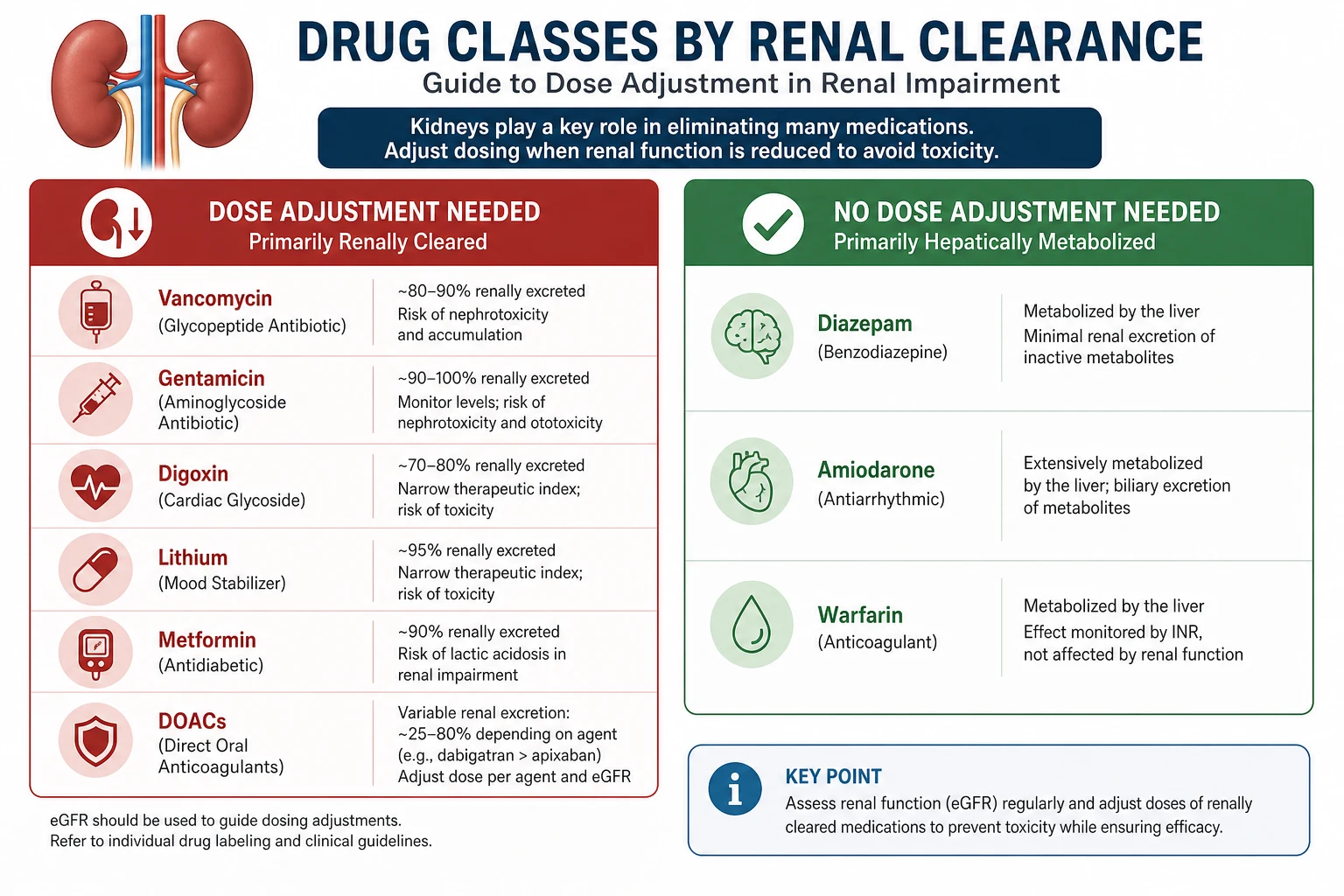
Safe prescribing in organ failure rests on one discriminating question: how is this drug cleared? A water-soluble (hydrophilic) drug is cleared by the kidney and accumulates in renal failure — vancomycin, gentamicin, digoxin, lithium, metformin, atenolol, allopurinol, the direct oral anticoagulants and the gabapentinoids. A lipid-soluble (lipophilic) drug is cleared by the liver and is largely unaffected by renal function — diazepam, amiodarone, warfarin, phenytoin. Get that split right, then estimate renal function honestly, dose off the correct equation (Cockcroft-Gault for most drug labels, CKD-EPI 2021 for staging), and apply therapeutic drug monitoring where the therapeutic index is narrow. [1]
The registrar who can do four things will pass any pharmacology viva: estimate renal function correctly, identify the renally-cleared drugs, adjust the hepatically-metabolised drugs in cirrhosis, and defend a structured medication review in the elderly. The one who doses vancomycin off an uncorrected eGFR, interprets a phenytoin total level in renal failure, or co-prescribes lithium with a thiazide will cause harm and fail the station. [1]
Pharmacokinetic principles that govern every dosing decision
Four processes determine what a drug does in the body: absorption, distribution, metabolism and excretion (ADME). Organ failure distorts the last three most often. [1]
Two equations matter clinically. Clearance (CL) is the volume of plasma cleared of drug per unit time, and it sets the maintenance dose: at steady state, maintenance dose = CL x target concentration x dosing interval. Volume of distribution (Vd) is the apparent volume the drug occupies, and it sets the loading dose: loading dose = Vd x target concentration. Renal failure lowers CL of renally-cleared drugs (so the maintenance dose falls); it can also raise Vd of some drugs through volume overload, lengthening half-life further. [1]
Half-life (t½ = 0.693 x Vd / CL) tells you how long a drug takes to reach steady state (about 4-5 half-lives) and how long toxicity persists after you stop the drug. When CL halves in renal failure, t½ doubles — so digoxin (normal t½ ~36 hours) takes over a week to reach a new steady state in CKD, and toxicity persists for days after withdrawal. This is why we check levels and adjust gradually. [1]
Two kinetic patterns recur. First-order kinetics (most drugs): elimination is proportional to concentration, t½ is constant, and steady state is reached predictably. Zero-order (saturable, Michaelis-Menten) kinetics: elimination is constant regardless of concentration because the enzyme is saturated. Phenytoin is the canonical example — above a certain concentration, a small dose increase causes a disproportionate rise in level and toxicity. Ethanol and high-dose aspirin behave similarly. This is why phenytoin dose titration above 300 mg/day must be in small increments (30-50 mg) with level checks. [1]
Viva trap: "Why does phenytoin go from sub-therapeutic to toxic with a small dose increase?" Answer: Michaelis-Menten saturable metabolism. Above the Km, the metabolising enzyme is saturated, elimination becomes zero-order, and level rises non-linearly. Dose-titrate in 30-50 mg steps and check a level. [1]
Estimating renal function — which equation, and when it lies
Two equations coexist. They answer different questions, and conflating them is a common exam error. [1]
Cockcroft-Gault — the drug-dosing equation
The Cockcroft-Gault equation estimates creatinine clearance (CrCl) and is the equation drug labels were validated against [1].
CrCl (mL/min) = (140 − age) × weight (kg) / (72 × SCr in mg/dL), multiplied by 0.85 for females. [1]
In SI units (SCr in micromol/L), the denominator becomes roughly 0.815 or you convert SCr to mg/dL first (divide micromol/L by 88.4). Use actual body weight in normal-weight patients; in obesity, adjusted body weight (ideal + 0.4 × (actual − ideal)) avoids overestimating. The weight matters — a cachected patient with a low muscle mass generates little creatinine, so SCr understates the severity of renal impairment. [1]
CKD-EPI 2021 — the staging equation
The 2021 CKD-EPI race-free equation estimates GFR (eGFR) and is now the recommended standard for diagnosing and staging CKD, replacing the race-adjusted 2009 equation [2]. Race was removed because it is a social construct, not a biological variable, and its inclusion systematically assigned higher eGFR (and therefore less apparent disease) to Black patients, with downstream effects on dialysis referral and transplant listing.
The 2021 equation uses serum creatinine (and an optional cystatin C version for greater accuracy). It is indexed to a standard body surface area of 1.73 m², which is a key limitation for drug dosing: a drug-dosing decision needs absolute clearance in mL/min for a particular patient, not a normalised value. [1]
When eGFR lies — the five traps
| Situation | Why eGFR is wrong | What to do |
|---|---|---|
| Unstable AKI | Creatinine reflects past function, not current; eGFR lags by hours to days | Do not quote a single eGFR. State "renal function is changing"; dose off current creatinine and urine output, assume low clearance, and reassess daily |
| Pregnancy | GFR rises 50% normally; CKD-EPI and Cockcroft-Gault were not validated | Use 24-hour creatinine clearance; do not rely on eGFR |
| Extremes of body size | eGFR is normalised to 1.73 m²; overestimates clearance in small patients, underestimates in large | Multiply eGFR by (BSA / 1.73) to "de-index", or use Cockcroft-Gault |
| Dialysis | Residual renal function is near-zero; eGFR is meaningless | Dose as for eGFR below 10, give post-dialysis doses of renally-cleared drugs, check supplemental dosing |
DWE exam trap: The classic discriminator is the cachectic 78-year-old with cirrhosis whose SCr is 70 micromol/L and whose eGFR reports as "greater than 60". The eGFR overestimates true GFR because muscle mass (and therefore creatinine generation) is low. Cockcroft-Gault with actual weight, or a measured 24-hour creatinine clearance, will reveal a clearance of 35-40 mL/min — and the renally-cleared drugs (vancomycin, digoxin, gabapentin) must be dose-reduced. Never dose renally-cleared drugs off an uncorrected eGFR in a low-muscle-mass patient. [1]
Dosing in chronic kidney disease
In stable CKD, dose off the eGFR (or Cockcroft-Gault) and a percentage-of-normal-dose table as a starting point only — then individualise with levels where TDM applies. [1]
| eGFR (mL/min/1.73 m²) | Dose of renally-cleared drug | Example |
|---|---|---|
| Above 50 | Full dose | Most drugs |
| 30-50 | 50-100% — reduce or extend interval | Apixaban unchanged unless other criteria; metformin review |
| 10-30 | 25-75% — reduce and extend interval | Gabapentin major reduction; allopurinol cap 200 mg |
| Below 10 / dialysis | 25% or avoid; give post-HD if removed | Metformin contraindicated; lithium dose and monitor |
The interval-extension strategy (give the same dose less often) preserves the peak concentration needed for efficacy (important for antibiotics) while allowing more time for elimination. The dose-reduction strategy (give a smaller dose at the usual interval) suits drugs where a flat concentration is desired (digoxin). Most drug labels give both. [1]
Dosing in AKI is different from CKD
AKI is dynamic — renal function is changing, often daily. The eGFR today reflects yesterday's creatinine and is unreliable. Principles: [1]
- Dose for current function, not baseline. Assume the worst until function recovers. A patient whose eGFR was 60 last month and who is now oliguric has an effective clearance near zero for renally-cleared drugs until urine output returns.
- Stop nephrotoxins (NSAIDs, ACEi/ARB if hyperkalaemic, aminoglycosides unless essential, contrast, tenofovir).
- Review every drug daily as renal function recovers or worsens — under-dosing is as dangerous as over-dosing in sepsis.
- Use TDM aggressively for vancomycin and aminoglycosides; levels guide dose far better than any equation in AKI. [1]
Dosing in dialysis
Drugs that are water-soluble, have low protein binding and a small volume of distribution are removed by haemodialysis — give them after the dialysis session or as a supplementary dose. Examples: gentamicin (largely removed), most beta-lactams and vancomycin (partially), gabapentin and pregabalin (heavily removed), metformin (removed — relevant in overdose), lithium (removed), ethanol, salicylate. [1]
Drugs that are highly protein-bound or have a large Vd are not significantly removed — digoxin (large Vd), amiodarone (enormous Vd), warfarin (highly protein-bound), phenytoin (protein-bound), the macrolides. Vancomycin is partially removed by HD and usually needs a supplementary dose; the dosing interval is typically extended to after each dialysis session or using a level drawn before HD. [1]
High-yield: "Which antibiotic needs a top-up after dialysis?" — a water-soluble beta-lactam or aminoglycoside. "Which drug is NOT removed by dialysis?" — digoxin or amiodarone, because of large Vd or high protein binding. [1]
Specific renally-cleared drugs — the high-yield list
Vancomycin — AUC-guided dosing
Vancomycin is renally cleared with a narrow therapeutic index. The 2020 ASHP/IDSA consensus guideline moved monitoring from trough-only to AUC-guided dosing for serious MRSA infections, targeting an AUC/MIC of 400-600 mg·h/L (assuming MIC 1 mg/L) [3]. The trough-only era (targeting 15-20 mg/L for serious infection) over-dosed patients and caused vancomycin-associated AKI, especially with concurrent piperacillin-tazobactam. AUC-guided dosing — increasingly via Bayesian software using one or two levels — achieves efficacy with less nephrotoxicity.
In renal failure, the dosing interval extends markedly (e.g., from 12-hourly to 48-hourly or longer) and levels are essential. On dialysis, vancomycin is partially removed and is typically given post-HD or guided by a pre-HD level. [1]
Aminoglycosides — extended-interval dosing
Gentamicin and tobramycin are concentration-dependent killers with a post-antibiotic effect, so a high peak drives efficacy and a low trough drives safety (nephrotoxicity, ototoxicity). This pharmacodynamic rationale supports extended-interval (once-daily) dosing — typically 5-7 mg/kg gentamicin — monitored with the Hartford nomogram using a random level drawn 6-14 hours post-dose [4]. Once-daily dosing is as effective as divided dosing and marginally less nephrotoxic.
When to avoid extended-interval dosing: endocarditis (especially enterococcal, where divided dosing with a beta-lactam synergistic combination is standard), pregnancy (altered Vd, fetal accumulation), burns (high clearance), severe renal impairment or dialysis, and paediatric dosing in some settings. In these, traditional divided dosing (1-1.7 mg/kg 8-hourly) with peak/trough monitoring applies. [1]
Aminoglycosides are themselves nephrotoxic (proximal tubular injury, usually reversible) and ototoxicity (often irreversible). Risk rises with duration beyond 5-7 days, concurrent nephrotoxins, hypovolaemia, older age and pre-existing CKD. [1]
Digoxin — the renal clearance trap
Digoxin is predominantly renally cleared with a narrow therapeutic index. In CKD the half-life lengthens from ~36 hours to several days, levels accumulate, and toxicity (nausea, visual disturbance with yellow-green halos, confusion, arrhythmia) occurs. Toxicity is precipitated or worsened by hypokalaemia (digoxin binds the same K+ site on the Na+/K+-ATPase), hypomagnesaemia, hypercalcaemia and renal failure — the combination of a loop diuretic (hypokalaemia) and digoxin in CKD is the classic set-up. The therapeutic range is lower than historically taught (0.5-0.9 ng/mL for heart failure; up to 2 ng/mL for rate control in AF) — higher levels add toxicity, not benefit. Severe poisoning is treated with digoxin-specific antibody fragments (Digibind), dosed from the serum level or ingested dose. [1]
Lithium — the multiple-interaction trap
Lithium is handled like sodium by the proximal tubule: anything that reduces GFR or increases proximal sodium reabsorption raises lithium levels. The classic precipitants are thiazide diuretics (volume depletion, increased proximal sodium and lithium reabsorption), ACE inhibitors and NSAIDs (reduced renal lithium clearance), and dehydration. Toxicity (coarse tremor, ataxia, confusion, seizures, coma) correlates poorly with level but worsens with chronicity. Management of acute toxicity is aggressive intravenous normal saline to restore GFR and enhance lithium excretion; haemodialysis is indicated for severe toxicity (level above 4 mmol/L in acute, above 2.5 in chronic with symptoms, or neurologic deterioration). [1]
Metformin — the eGFR cutoff
Metformin is renally cleared and, in accumulation, causes metformin-associated lactic acidosis (Type B lactic acidosis). The risk is highest in AKI, dehydration, hypoxia and sepsis — hence the sick-day rule (hold metformin, ACEi, diuretics, NSAIDs and SGLT2i during intercurrent illness). The eGFR thresholds: avoid if eGFR below 30; review benefit/risk and reduce dose at 30-45; continue above 45 in stable CKD. In AKI, eGFR is unreliable — stop metformin and do not restart until renal function returns to baseline. [1]
Allopurinol — the dose-reduction rule
Allopurinol and its active metabolite oxypurinol are renally cleared. Full-dose allopurinol in CKD is the single biggest risk factor for allopurinol hypersensitivity syndrome (DRESS / Stevens-Johnson syndrome), which carries high mortality. The rule: start 100 mg daily and increase gradually, with a maximum of 200 mg/day if eGFR is below 30 (some guidelines permit titration higher if the target urate is not met and the drug is tolerated). The HLA-B*5801 allele (common in Han Chinese, Korean, Thai populations) markedly increases risk — screen before starting in high-prevalence populations. [1]
Direct oral anticoagulants (DOACs)
DOACs are partly renally cleared and dose-reduction depends on the agent and indication. Apixaban (Eliquis) has specific dose-reduction criteria: reduce 5 mg BD to 2.5 mg BD if two or more of: age above 80, weight below 60 kg, serum creatinine above 133 micromol/L. Rivaroxaban and dabigatran have their own eGFR-based reductions (dabigatran is the most renally cleared, ~80%, and is contraindicated below eGFR 30). Warfarin is the anticoagulant of choice in severe renal impairment (eGFR below 30) because it is hepatically cleared. [1]
Gabapentin and pregabalin
Both are renally cleared essentially unchanged and accumulate in CKD, causing sedation, ataxia and myoclonus. Dose-reduce in proportion to eGFR and give a supplementary post-HD dose (both are removed by dialysis). [1]
Mnemonic — renally-cleared drugs to dose-adjust: VAncomycin, Gentamicin, Digoxin, Lithium, Metformin, Allopurinol, Atenolol, Apixaban/DOACs, Gabapentin. The "VANG LIMAAG" drugs. The corollary: diazepam, amiodarone, warfarin, phenytoin, doxycycline are hepatically cleared and need no renal adjustment. [1]
Dosing in hepatic failure
Hepatic drug dosing is less predictable than renal dosing. There is no single accurate "hepatic eGFR". The Child-Pugh (Child-Turcotte-Pugh) score is the crude surrogate clinicians use, but it correlates only modestly with drug clearance because cirrhosis affects extraction ratio, protein binding, bile flow and portosystemic shunting in variable combinations [7].
The Child-Pugh classification
Five components, each scored 1-3, total 5-15: [1]
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (micromol/L) | Below 34 | 34-50 | Above 50 |
| Albumin (g/L) | Above 35 | 28-35 | Below 28 |
| INR / prothrombin time | INR below 1.7 | INR 1.7-2.3 | INR above 2.3 |
| Ascites | None | Mild (controlled medically) | Moderate-severe (refractory) |
| Encephalopathy | None | Grade 1-2 | Grade 3-4 |
Class A = 5-6 (compensated); Class B = 7-9 (significant functional impairment); Class C = 10-15 (decompensated). FDA drug labels advise a maximum 50% dose reduction in Child-Pugh B for many drugs and avoidance in Child-Pugh C — but each label must be checked individually. [1]
Which drugs are affected in cirrhosis
Two pharmacokinetic effects dominate. [1]
Loss of first-pass metabolism in high-extraction-ratio drugs. A drug that is normally extensively metabolised on first pass through the liver reaches the systemic circulation in only small amounts. Cirrhosis plus portosystemic shunting removes this first-pass effect, so bioavailability rises dramatically and a standard dose produces an exaggerated effect. The classic examples: propranolol (used to reduce portal pressure, but standard doses over-treat), morphine and other opioids (sedation and precipitated encephalopathy), levodopa, labetalol, verapamil. Start at a low dose and titrate. [1]
Impaired CYP450 metabolism. Drugs metabolised by cytochrome P450 enzymes accumulate. Warfarin sensitivity in cirrhosis is partly impaired metabolism and partly impaired hepatic synthesis of clotting factors — the INR is already abnormal, and warfarin effect is hard to judge. Phenytoin, the macrolides (via CYP3A4 inhibition, also raising levels of co-administered drugs), statins (hepatotoxicity and increased transaminases), and most benzodiazepines fall here. [1]
Drugs to avoid or use with great caution in cirrhosis: [1]
- Sedatives and opioids (precipitate hepatic encephalopathy — even small doses).
- NSAIDs (renal failure from prostaglandin inhibition, variceal bleeding from platelet effects, sodium and water retention).
- Diuretics (over-diuresis precipitates hepatorenal syndrome and encephalopathy; spironolactone and frusemide in a 100:40 ratio is the standard ascites regimen).
- Paracetamol — reduced but not banned: up to 2 g/day in stable cirrhosis is safe (the concern is dose-dependent glutathione depletion); avoid in decompensated or alcoholic cirrhosis.
- ACEi/ARBs — lower blood pressure and renal perfusion; risk hepatorenal syndrome. [1]
DWE exam trap: "Why does a small dose of morphine sedate a cirrhotic patient excessively?" Answer: loss of first-pass metabolism (high extraction ratio) plus impaired CYP450 metabolism — systemic bioavailability rises several-fold. Avoid opioids and benzodiazepines; if essential, use a fraction of the usual dose (e.g., fentanyl or oxycodone at 25-50% with careful monitoring). [1]
Therapeutic drug monitoring — the five drugs to know
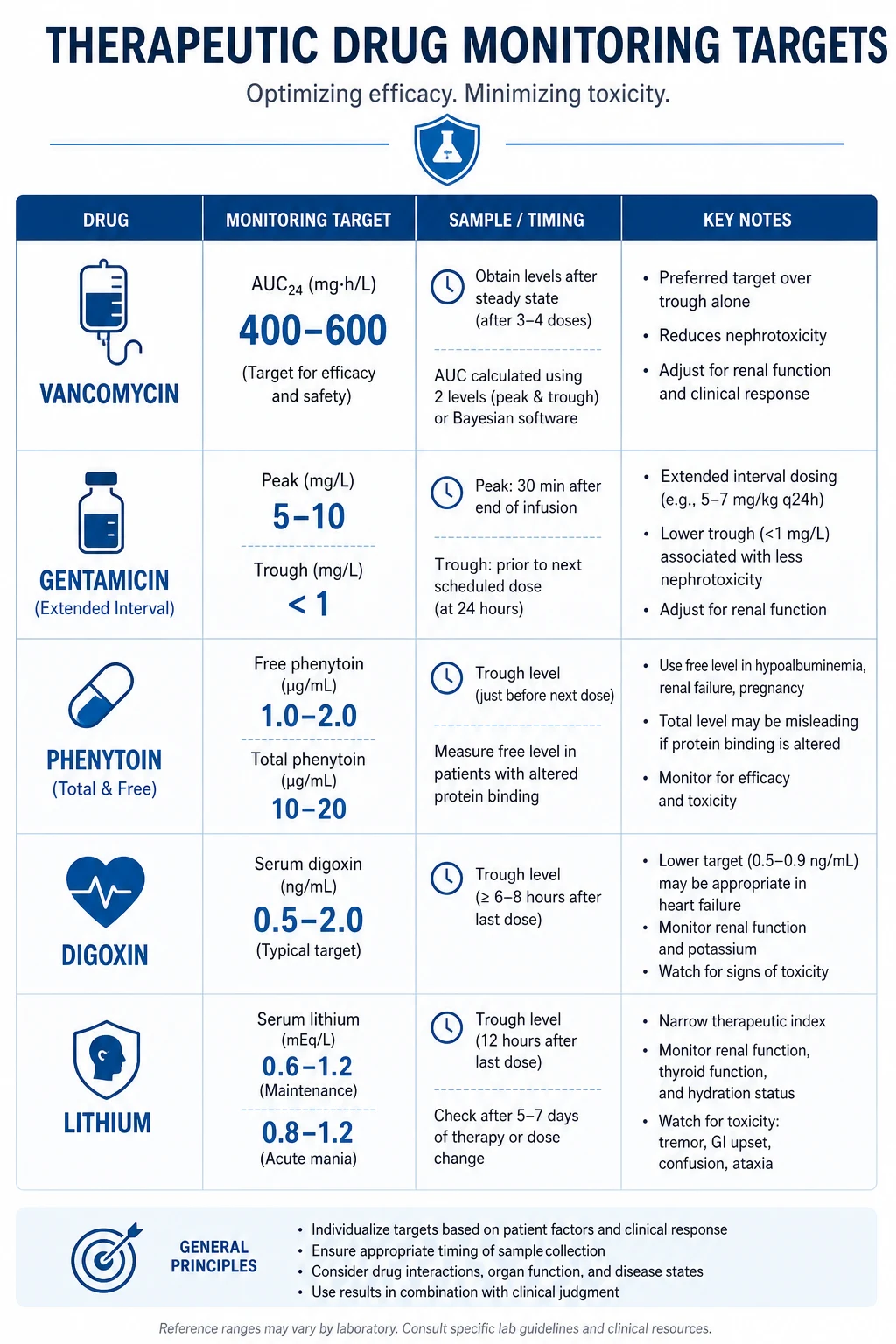
TDM applies to drugs with a narrow therapeutic index, concentration-related efficacy or toxicity, and unpredictable pharmacokinetics. The five drugs tested routinely: vancomycin, aminoglycosides, phenytoin, digoxin, lithium (ciclosporin/tacrolimus and other anti-epileptics extend the list). [1]
| Drug | Target | Sampling | Pitfall |
|---|---|---|---|
| Vancomycin | AUC 400-600 mg·h/L; trough 10-15 (moderate) / 15-20 (serious) | Pre-4th dose at steady state | Trough-only over-doses; concurrent piperacillin-tazobactam raises AKI risk |
| Phenytoin | Total 10-20 mg/L; free 1-2 mg/L | Pre-dose at steady state (5-7 half-lives) | Total level underestimates toxicity in hypoalbuminaemia/renal failure — use Sheiner-Tozer or free level |
| Digoxin | 0.5-0.9 ng/mL (HF); up to 2 (rate control) | Pre-dose at steady state | Toxicity at lower levels with hypokalaemia, renal failure;Digibind for severe |
| Lithium | 0.4-1.0 mmol/L (maintenance); 0.8-1.2 (acute mania) | Pre-dose, 12 h post-dose | Toxicity with thiazides, ACEi, NSAIDs, dehydration |
Phenytoin and the Sheiner-Tozer correction
Phenytoin is 90% protein-bound to albumin; only the free (unbound) 10% is pharmacologically active. In hypoalbuminaemia (cirrhosis, nephrotic syndrome, critical illness) or renal failure (uraemic compounds displace phenytoin from albumin), the free fraction rises. The total phenytoin level falls (less bound drug) while the free (active) level stays the same or rises — so a patient can be toxic on a "therapeutic" total level. [1]
The Sheiner-Tozer equation corrects the measured total level for albumin: [1]
Corrected phenytoin = measured total / [(0.2 × albumin in g/dL) + 0.1] (for normal patients, denominator ~1.0). [1]
In renal failure (creatinine above ~180 micromol/L or significant uraemia), a second term accounts for uraemic displacement: [1]
Corrected phenytoin = measured total / [(0.2 × albumin in g/dL) + 0.1] but with the uraemia coefficient the denominator becomes [(0.48 × (albumin/4.4 − 0.01)) + 0.1] — in practice, send a free phenytoin level (target 1-2 mg/L) rather than struggle with corrections. [1]
Viva discriminator: "A patient on the ICU has a phenytoin total of 12 mg/L (therapeutic range 10-20) but is nystagmic and ataxic. Why?" Answer: albumin is 18 g/L. Correct the level: 12 / [(0.2 × 1.8) + 0.1] = 12 / 0.46 = 26 mg/L — toxic. The free fraction is elevated because albumin is low. Send a free level (will be above 2 mg/L) and reduce the dose. [1]
Drug-induced organ failure — preventing iatrogenic harm
Nephrotoxins
| Drug | Mechanism | Pattern |
|---|---|---|
| NSAIDs | Afferent arteriolar constriction (inhibit prostaglandins) | Haemodynamically-mediated AKI; acute interstitial nephritis |
| ACEi / ARB | Efferent arteriolar dilation (remove angiotensin II tone) | Functional drop in GFR; hyperkalaemia; worse with bilateral renal artery stenosis |
| Contrast media | Direct tubular toxicity + vasoconstriction | Contrast-induced nephropathy, peak at 48-72 h |
| Aminoglycosides | Proximal tubular accumulation | Non-oliguric AKI after 5-7 days; usually reversible |
| Tenofovir (and other NRTIs) | Mitochondrial toxicity in proximal tubule | Fanconi syndrome, hypophosphataemia, eGFR decline |
| Tacrolimus / ciclosporin | Afferent arteriolar vasoconstriction | Functional then structural nephropathy; hyperkalaemia |
| Lithium | Concentrated in collecting duct | Chronic tubulointerstitial nephritis, nephrogenic DI |
| Amphotericin B | Membrane pore-forming in tubule | Distal RTA, hypokalaemia, AKI |
The triple whammy — ACEi/ARB + diuretic + NSAID — is a high-yield exam stem and a common real-world cause of AKI in older patients. The combination simultaneously removes afferent arteriolar tone (NSAID), efferent arteriolar tone (ACEi) and intravascular volume (diuretic). The GFR, which depends on the pressure gradient across the glomerulus, collapses. Avoid the triple combination; if AKI develops, stop all three. [1]
Hepatotoxins
| Drug | Pattern | Note |
|---|---|---|
| Paracetamol | Dose-related centrilobular necrosis | #1 cause of acute liver failure in many countries; treat with N-acetylcysteine |
| Statins | Transaminitis, rarely acute hepatitis | Monitor LFTs; usually mild and adaptive |
| Anti-TB (isoniazid, rifampicin, pyrazinamide) | Mixed hepatocellular; risk rises with age, alcohol, hepatitis B/C | Baseline and monthly LFTs |
| Methotrexate | Chronic fibrosis/cirrhosis with long-term low-dose use | Monitor LFTs, FBC, albumin; some recommend FibroScan/liver biopsy after cumulative dose |
| Amiodarone | Phospholipidosis, pseudo-alcoholic hepatitis | Baseline and 6-monthly LFTs and TFTs |
| Sodium valproate | Microvesicular steatosis (mitochondrial) | Monitor LFTs; high risk in young children, metabolic disorders |
| Herbal / complementary products | Variable | Anabolic steroids, kava, black cohoga, green tea extract |
Contrast-induced nephropathy prevention
For patients at risk (CKD, diabetes, dehydration, multiple myeloma, high contrast volume): intravenous isotonic saline (1 mL/kg/h for 6-12 h pre- and post-procedure), hold metformin and NSAIDs around the procedure, use the lowest necessary contrast volume with low- or iso-osmolar agents, and consider the (modest) evidence for statin coverage and oral N-acetylcysteine. The role of N-acetylcysteine is debated; saline volume expansion is the intervention with the strongest evidence. [1]
Polypharmacy and the elderly
Physiological changes that alter drug handling
- Reduced renal clearance — GFR falls with age even with a "normal" creatinine (low muscle mass masks it). Cockcroft-Gault is preferred for elderly dosing.
- Reduced hepatic mass and blood flow — slower metabolism of high-extraction drugs; CYP450 activity preserved in relative terms.
- Increased body fat, reduced total body water — lipid-soluble drugs (diazepam, amiodarone) distribute more widely and accumulate; half-life lengthens.
- Reduced gastric acid, slower gastric emptying — minor effect on absorption.
- Reduced albumin (in illness) and increased alpha-1-acid glycoprotein (in inflammation) — altered free fraction of protein-bound drugs.
- Increased sensitivity — benzodiazepines cause more sedation and falls; opioids more respiratory depression; anticholinergics more confusion. [1]
Beers Criteria (AGS 2023)
The AGS Beers Criteria 2023 [5] list potentially inappropriate medications (PIMs) in adults aged 65 and over across five categories: PIMs to avoid generally; PIMs to avoid in specific diseases/syndromes; drugs to use with caution; clinically important drug-drug interactions; and drugs to dose differently in renal impairment.
High-yield Beers-listed drugs and safer alternatives: [1]
| Drug / class | Problem | Safer alternative |
|---|---|---|
| Long-acting benzodiazepines (diazepam, clonazepam) | Falls, delirium, prolonged sedation, fractures | If a benzodiazepine is essential, short-acting (lorazepam) at lowest dose, short course; treat insomnia non-pharmacologically |
| First-generation antihistamines (diphenhydramine, chlorpheniramine) | Strong anticholinergic; sedation, confusion | Second-generation (cetirizine, loratadine) |
| Long-acting sulfonylureas (glyburide/glibenclamide) | Prolonged severe hypoglycaemia | Glipizide, or a DPP-4 inhibitor / SGLT2i |
| NSAIDs (chronic systemic) | GI bleeding, AKI, hypertension, heart failure | Paracetamol first-line; topical NSAID; if oral NSAID essential, add a PPI for the shortest possible time |
| Skeletal muscle relaxants (cyclobenzaprine) | Anticholinergic, sedation, falls | Non-pharmacological; topical therapies |
| Anticholinergics for overactive bladder (oxybutynin) | Confusion, dry mouth, constipation, retention | Mirabegron (beta-3 agonist), or tolterodine |
| First-generation TCAs (amitriptyline, doxepin above 6 mg) | Anticholinergic, orthostatic hypotension, falls | SSRI/SNRI for depression; gabapentinoid or duloxetine for neuropathic pain |
| Sliding-scale insulin (without basal) | Hypoglycaemia; poor control | Basal-bolus regimen; avoid reactive sliding scales |
STOPP / START criteria (version 3)
The STOPP/START criteria version 3 [6] complement Beers with a European, physiology-based tool: STOPP (Screening Tool of Older Persons' Prescriptions) flags potentially inappropriate medications; START (Screening Tool to Alert to Right Treatment) flags prescribing omissions — drugs that should be prescribed but are not. Version 3 contains 133 STOPP and 57 START criteria.
High-yield STOPP flags: any drug without a clear clinical indication; duplicate drug class; long-acting benzodiazepines beyond 4 weeks; NSAID with significant hypertension, heart failure, or CKD; PPI at full dose beyond 8 weeks without indication; anticholinergic burden (sum of anticholinergic drugs). [1]
High-yield START flags (common omissions in the exam): statin in diabetes or established vascular disease unless contraindicated; ACE inhibitor (or ARB) in systolic heart failure; anticoagulation (DOAC or warfarin) in atrial fibrillation with CHA2DS2-VASc above threshold; beta-blocker in stable systolic heart failure; metformin in type 2 diabetes (if not contraindicated); bone protection (bisphosphonate and calcium/vitamin D) in glucocorticoid therapy or proven osteoporosis; PPI with a NSAID in high-risk patients; influenza and pneumococcal vaccination. [1]
Performing a structured medication review
In any complex patient, work through the list drug by drug: [1]
- Reconcile — what is actually being taken (ask the patient, the pharmacist, the brown bag; count the tablets).
- Indication — does each drug have a current, defensible indication?
- Benefit vs harm — is the benefit likely to be realised in this patient's prognosis (time-to-benefit matters for statins and bisphosphonates in limited-prognosis patients)?
- Interactions — pharmacokinetic (CYP450 induction/inhibition) and pharmacodynamic (additive toxicity such as the triple whammy).
- Organ function — re-dose for renal and hepatic function; flag the renally-cleared and high-extraction drugs.
- Anticholinergic and sedative burden — deprescribe where possible.
- Deprescribe — one drug at a time, with monitoring; communicate with the patient and GP. [1]
Sick-day rule (patient counselling): "If you develop vomiting, diarrhoea or fever and cannot keep fluids down, temporarily stop your 'sick-day pills' — the water tablet (diuretic), the blood-pressure tablet (ACEi/ARB), the diabetes tablet (metformin) and any anti-inflammatory (NSAID), and restart when you are eating and drinking normally for 24-48 hours. Seek help if you are not improving." These four drug classes cause AKI, hyperkalaemia, lactic acidosis and hypoglycaemia respectively during dehydration. [1]
DCE long-case approach — the medication review
Opening statement (SASPOP)
"Mrs Whitlam is a 78-year-old woman, a retired schoolteacher, admitted with a fall and confusion. She has a background of type 2 diabetes for 18 years, chronic kidney disease stage 3b (baseline eGFR 32), ischaemic heart disease with atrial fibrillation, hypertension, gout, osteoporosis and depression. She takes metformin 1 g BD, gliclazide 80 mg BD, apixaban 5 mg BD, bisoprolol 5 mg, perindopril 10 mg, frusemide 40 mg, indomethacin 50 mg BD, allopurinol 300 mg, amitriptyline 50 mg nocte, and a multivitamin." [1]
"Her main problems are:
- Acute kidney injury (KDIGO stage 2) on chronic CKD stage 3b — precipitated by the triple whammy of perindopril, frusemide and indomethacin during a presumed viral illness
- Polypharmacy with several potentially inappropriate medications — indomethacin (NSAID in CKD), amitriptyline (anticholinergic in a falls-prone older patient), full-dose allopurinol in CKD, metformin in acute renal impairment
- Hyperkalaemia, K 5.9, secondary to the AKI and ACEi
- A fall with confusion — likely multifactorial (dehydration, anticholinergic amitriptyline, hypoglycaemia from gliclazide, possible sepsis)
- Atrial fibrillation on anticoagulation — apixaban dose appropriateness to review given age and renal function." [1]
Integrated medication review
- Stop the offending agents now: cease indomethacin (NSAID in CKD and the third arm of the triple whammy), hold perindopril (hyperkalaemia, AKI), hold frusemide once volume status assessed, hold metformin (AKI, lactic acidosis risk), cease amitriptyline (anticholinergic, falls).
- Re-dose for renal function (current eGFR ~25 during AKI):
- Allopurinol — reduce to 100 mg daily (eGFR below 30; full dose is the biggest risk factor for DRESS). [1] - Apixaban — check criteria: she is above 80? No (78). Weight below 60? Unknown — check. Creatinine above 133? Likely in AKI. If two of three are met, reduce to 2.5 mg BD; otherwise continue 5 mg BD and reassess. (In severe AKI with bleeding risk, consider holding or switching to LMWH/heparin temporarily.)
- Gliclazide — risk of hypoglycaemia in renal impairment; reduce or hold temporarily; consider short-acting insulin if needed.
- Treat the hyperkalaemia — calcium resonium orally, or insulin/dextrose if ECG changes; recheck.
- Investigate the precipitant — urinalysis, blood cultures, CXR; treat sepsis if present.
- Deprescribe on recovery:
- Replace amitriptyline with an SSRI (sertraline) if depression persists; non-pharmacological sleep strategies.
- Replace indomethacin with paracetamol for gout pain; colchicine for the acute flare (dose-reduced in CKD).
- Restart perindopril only when renal function returns to baseline and potassium is normal; if AF and hypertension, a beta-blocker and rate control may suffice.
- Restart metformin only when eGFR returns above 30 and the patient is well hydrated.
- Continue apixaban (the CHA2DS2-VASc strongly favours anticoagulation; renal-adjusted).
- Ensure bone protection (bisphosphonate, calcium/vitamin D) and statin (unless contraindicated) are in place. [1]
DCE examiner probing question: "How would you counsel this patient at discharge?" Answer: "I would explain the sick-day rule in plain language — temporarily stop the water tablet, the blood-pressure tablet, the diabetes tablet and any painkillers when she has vomiting, diarrhoea or fever and cannot drink, and restart when eating and drinking normally for 24 hours. I would give her a written medication list, arrange GP follow-up within a week, and a pharmacy home medicines review. I would explain why we have stopped the anti-inflammatory and the amitriptyline and what we are using instead, and check her understanding with teach-back." [1]
Key DWE MCQ patterns
- Renally- vs hepatically-cleared drug. The stem gives a drug and asks whether to dose-adjust in CKD. Know the lists cold: water-soluble (vancomycin, gentamicin, digoxin, lithium, metformin, atenolol, allopurinol, DOACs, gabapentinoids) vs lipid-soluble (diazepam, amiodarone, warfarin, phenytoin).
- AUC-guided vancomycin. The stem describes serious MRSA infection and asks for the monitoring target — AUC/MIC 400-600 mg·h/L, not trough. [1]3. Phenytoin in hypoalbuminaemia. A "therapeutic" total level with toxicity — correct with Sheiner-Tozer or send a free level.
- Apixaban dose-reduction criteria. Two of three: age above 80, weight below 60 kg, creatinine above 133.
- Allopurinol in CKD. DRESS precipitated by full-dose allopurinol; start 100 mg, cap 200 mg below eGFR 30. [1]6. The triple whammy. AKI in a patient on ACEi + diuretic + NSAID — the combination is the answer.
- Lithium interaction. Toxicity precipitated by a newly-added thiazide, ACEi or NSAID.
- Child-Pugh classification. Identify the class from the five components; high-extraction drugs (morphine, propranolol) most affected.
- Beers criteria. Long-acting benzodiazepine, glyburide, first-generation antihistamine, chronic NSAID — identify the PIM and the safer alternative.
- eGFR in low muscle mass. A cachectic/cirrhotic patient with a falsely reassuring eGFR — Cockcroft-Gault or 24-hour creatinine clearance reveals the truth. [1]
Exam pearls
- Water-soluble = renal; lipid-soluble = hepatic. This single distinction answers most dosing MCQs.
- Cockcroft-Gault for dosing, CKD-EPI 2021 for staging — and neither is reliable in unstable AKI, low muscle mass, pregnancy or dialysis.
- Vancomycin: think AUC, not trough. Trough-only monitoring causes nephrotoxicity, especially with piperacillin-tazobactam.
- Phenytoin: think free level. A "therapeutic" total level with albumin 18 g/L is toxic; correct or send a free level. [1]- Lithium: think interactions. Thiazide, ACEi, NSAID, dehydration — each raises lithium.
- Allopurinol: think DRESS. Reduce the dose in CKD; screen HLA-B*5801 in high-risk populations.
- The triple whammy is the most testable nephrotoxicity. ACEi/ARB + diuretic + NSAID.
- Child-Pugh B = halve; Child-Pugh C = avoid (as a general rule, check each label).
- Beers for the older adult: benzodiazepines, glyburide, first-generation antihistamines, chronic NSAIDs, anticholinergics.
- Sick-day rule: "water pill, BP pill, diabetes pill, painkiller" — stop during illness. [1]
References
[1] Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976;16:31-41. The original Cockcroft-Gault equation — the creatinine clearance estimate that most drug labels were validated against, and still the preferred equation for renal drug dosing in many formularies. [2] Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. NEJM 2021;385:1737-49. The 2021 CKD-EPI race-free equation — the current recommended standard for diagnosing and staging CKD, with its known limitations for drug dosing in low muscle mass and unstable AKI. [3] Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: a revised consensus guideline and review. Clin Infect Dis 2020;71:1361-4. The ASHP/IDSA/PIDS/SIDP consensus that moved vancomycin monitoring from trough-only to AUC-guided dosing (target AUC/MIC 400-600 mg.h/L), reducing nephrotoxicity. [4] Barza M, Ioannidis JP, Cappelleri JC, Lau J. Single or multiple daily doses of aminoglycosides: a meta-analysis. BMJ 1996;312:338-45. The meta-analysis of 21 trials (3091 patients) supporting once-daily (extended-interval) aminoglycoside dosing as equally effective and marginally less nephrotoxic than divided dosing. [5] 2023 American Geriatrics Society Beers Criteria Update Expert Panel. AGS 2023 updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2023;71:2052-81. The current US standard list of PIMs in adults aged 65 and over, across five categories including drugs to dose differently in renal impairment. [6] O'Mahony D, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med 2023;14:627-64. The European physiology-based tool with 133 STOPP criteria (inappropriate prescriptions) and 57 START criteria (prescribing omissions) for the medication review. [7] Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973;60:646-9. The paper that introduced the modified Child-Turcotte-Pugh classification — the five-component score (bilirubin, albumin, INR, ascites, encephalopathy) still used to grade hepatic functional reserve and guide hepatic drug dosing.
AGS Beers Criteria 2023; KDIGO CKD Guideline (drug dosing); Australian Medicines Handbook; FDA drug labels (DailyMed); UpToDate — dosing in renal and hepatic impairment. [1]
References
- [1]Cockcroft DW, Gault MH Prediction of creatinine clearance from serum creatinine Nephron, 1976.PMID 1244564
- [2]Inker LA, Eneanya ND, Coresh J, et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race N Engl J Med, 2021.PMID 34554658
- [3]Rybak MJ, Le J, Lodise TP, et al. Therapeutic Monitoring of Vancomycin for Serious Methicillin-resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review by the American Society of Health-system Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists Clin Infect Dis, 2020.PMID 32658968
- [4]Barza M, Ioannidis JP, Cappelleri JC, Lau J Single or multiple daily doses of aminoglycosides: a meta-analysis BMJ, 1996.PMID 8611830
- [5]2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [6]O'Mahony D, O'Connor MN, Eustace J, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3 Eur Geriatr Med, 2023.PMID 37256475
- [7]Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R Transection of the oesophagus for bleeding oesophageal varices Br J Surg, 1973.PMID 4541913