Phys · pharmacological
Poisoning — Approach, Decontamination and Antidotes
Also known as poisoning · overdose · toxicology · toxidrome · sympathomimetic toxidrome · anticholinergic toxidrome · cholinergic toxidrome · opioid toxidrome · sedative-hypnotic toxidrome · SLUDGE · DUMBELS · activated charcoal · whole bowel irrigation · urinary alkalinisation · multi-dose activated charcoal · antidote · naloxone · flumazenil · N-acetylcysteine · fomepizole · pralidoxime · digoxin Fab antibodies · sodium bicarbonate · deferoxamine · hydroxocobalamin · octreotide · lipid emulsion
Consultant-physician-depth guide to the systematic approach to the poisoned patient — ABCDE resuscitation, toxidrome identification (sympathomimetic, anticholinergic, cholinergic, opioid, sedative-hypnotic), gastrointestinal decontamination (activated charcoal, whole bowel irrigation), enhanced elimination (urinary alkalinisation, multi-dose charcoal, haemodialysis), and the antidote reference table. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Poisoning — Approach, Decontamination and Antidotes

The answer first
Poisoning is a resuscitation problem before it is a toxin-identification problem. The patient who has collapsed after an unknown ingestion is killed by airway loss, hypoxia, aspiration and dysrhythmia — not by the delay in naming the drug. The registrar who stabilises first, then hunts the toxidrome, then deploys decontamination and antidotes in the correct order will manage any overdose. The one who reaches for the antidote before securing the airway will lose the patient [1].
The sequence is fixed and reproducible: [1]
- Resuscitate — ABCDE. Protect the airway; intubate early if the conscious state is falling. Give oxygen, glucose (check a bedside level first), thiamine in the malnourished or alcoholic patient, and naloxone titrated to respiratory effort when the pupils are pinpoint.
- Identify the toxidrome — the constellation of vital signs, pupil size, skin, bowel sounds and mental state that fingerprints a class of toxin. The toxidrome narrows the differential faster than any blood test.
- Decontaminate — activated charcoal within one hour of a charcoal-binding ingestion, provided the airway is protected. Whole bowel irrigation for iron, lithium, sustained-release formulations and body packers.
- Enhance elimination — urinary alkalinisation for salicylates; multi-dose charcoal for carbamazepine, phenobarbital, theophylline; haemodialysis for salicylates, lithium, methanol, ethylene glycol and metformin.
- Give the specific antidote — naloxone, N-acetylcysteine, fomepizole, digoxin Fab, atropine plus pralidoxime, sodium bicarbonate for tricyclic cardiotoxicity, deferoxamine, hydroxocobalamin, octreotide, lipid emulsion. [1]
The single most dangerous error in poisoning is giving activated charcoal to a patient with an unprotected airway. Aspiration of charcoal into an unprotected bronchial tree causes a devastating chemical pneumonitis and is frequently fatal. Secure the airway first; decontaminate second [3].
Viva trap: "What is the first thing you do for a patient found collapsed beside empty bottles?" Lead with the answer: "I secure the airway and breathing, check a bedside glucose, and only then consider decontamination. Activated charcoal is contraindicated until the airway is protected." [1]
The ABCDE approach to the poisoned patient
The standard ABCDE framework is adapted for toxidromes. Each step carries a toxicology-specific action that the examiner will probe. [1]
Airway. The leading cause of death in the poisoned patient is loss of airway protection with aspiration. Depressed conscious state from opioids, sedative-hypnotics, alcohols and TCAs abolishes the gag reflex. Intubate early — the threshold is lower than for a sober patient, because the poison will deepen before it improves. A GCS of 8 or less, or a rapidly falling conscious state, is an indication for rapid sequence intubation. [1]
Breathing. Respiratory depression narrows the toxidrome to opioid, sedative-hypnotic, or a poison causing a severe acidaemia that fatigues the respiratory muscles. Hyperventilation points to salicylate toxicity (direct medullary stimulation), a compensatory response to a metabolic acidosis, or early stimulant toxicity. Check a venous or arterial blood gas — it reveals both the respiratory status and the underlying metabolic derangement. [1]
Circulation. Hypotension in poisoning is usually distributive (venodilatation from sedatives) or cardiogenic (sodium-channel blockade from TCAs). The discriminator is the QRS width: a wide QRS signals myocardial sodium-channel toxicity and mandates intravenous sodium bicarbonate. Tachycardia with hypertension points to a sympathomimetic; tachycardia with hypotension to anticholinergic or tricyclic toxicity. [1]
Disability. Check pupils, glucose and temperature together. Pinpoint pupils, respiratory depression and coma are the opioid triad. Dilated pupils with agitation are sympathomimetic or anticholinergic. Hypoglycaemia mimics almost every toxidrome — a bedside glucose is mandatory and treats a reversible cause of coma instantly. Hypothermia suggests a sedative or environmental exposure; hyperthermia is a sympathomimetic, anticholinergic, serotonin syndrome, neuroleptic malignant syndrome or salicylate until proven otherwise. [1]
Exposure. Look for the clues: needle marks, intra-nasal powder, transdermal patches (fentanyl, rivastigmine), pill fragments, body-packer packets on a plain film, and the so-called toxidrome skin findings (diaphoretic and pale in sympathomimetic, dry and flushed in anticholinergic). [1]
DWE high-yield: The "coma cocktail" is largely historical, but two elements remain: glucose (check and treat) and naloxone (titrate when the picture fits). Thiamine is given before glucose to the malnourished or chronic alcoholic patient to avoid precipitating Wernicke encephalopathy. Flumazenil is no longer given empirically — it precipitates seizures in chronic benzodiazepine users and TCA co-ingestions. [1]
Toxidrome identification
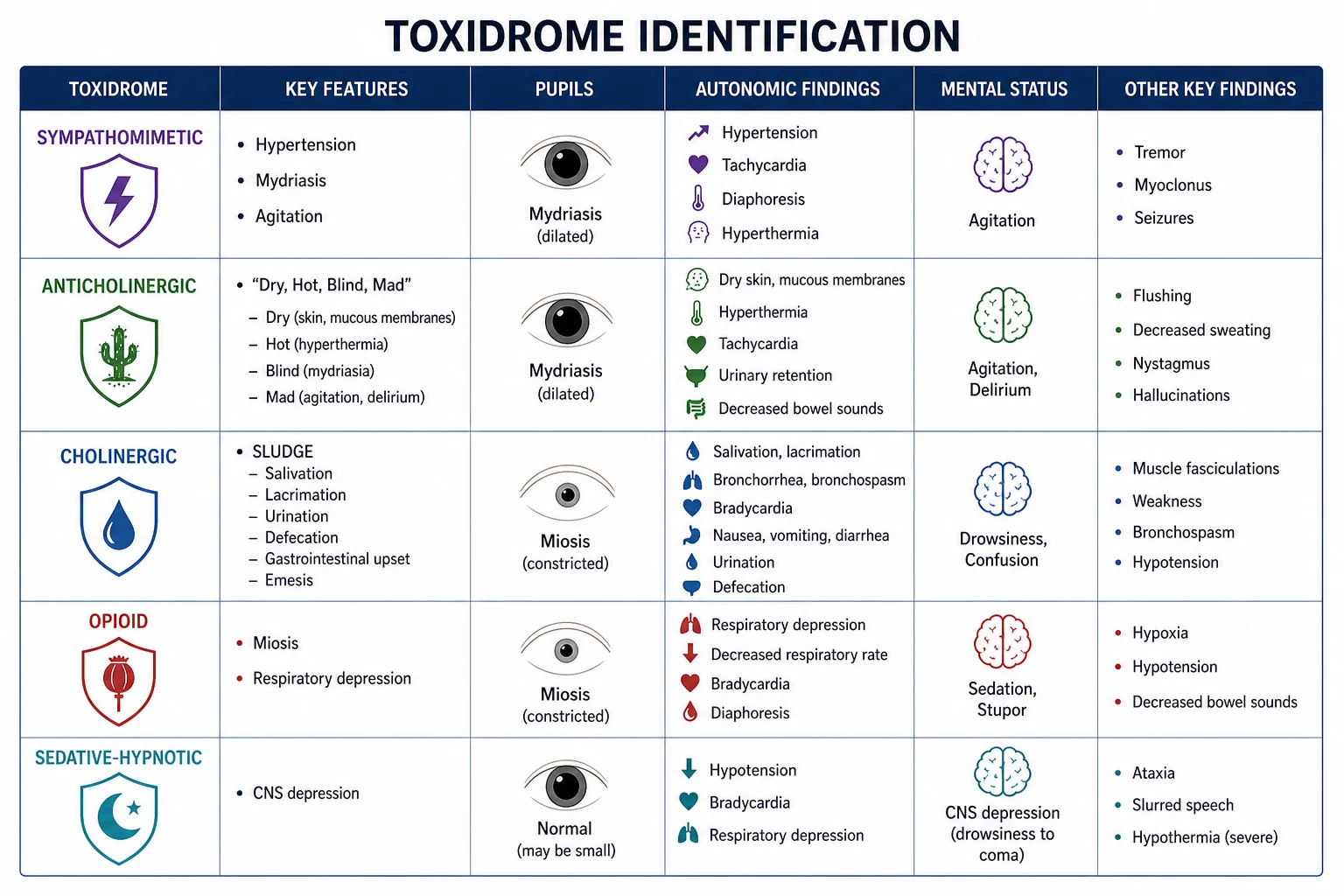
A toxidrome is a syndrome cluster of clinical signs produced by a class of toxin acting on a common receptor system. Five core toxidromes cover the majority of presentations. Recognising the toxidrome immediately narrows the differential, predicts the complications, and points to the antidote [1].
The examination must capture six data points: mental state, pupil size, vital signs (temperature, pulse, blood pressure, respiratory rate), skin (moist or dry, flushed or pale), bowel sounds, and secretions (salivation, lacrimation, bronchorrhoea, urination, defecation). Memorise the table below — every element is examinable. [1]
| Toxidrome | Mental state | Pupils | Vitals | Skin | Bowel sounds | Secretions |
|---|---|---|---|---|---|---|
| Sympathomimetic (cocaine, amphetamines, MDMA) | Agitated, hyperalert | Large (mydriasis) | Hyperthermia, tachycardia, hypertension, tachypnoea | Diaphoretic, pale | Increased | None |
| Anticholinergic (atropine, antihistamines, TCA) | Agitated, delirious ("mad as a hatter") | Large (mydriasis, "blind as a bat") | Hyperthermia, tachycardia | Dry, flushed ("dry as a bone, red as a beet") | Decreased | Dry (anhidrosis) |
| Cholinergic (organophosphates, nerve agents) | Confused, then coma | Small (miosis) | Bradycardia (early) or tachycardia, may be normothermic or hypothermic | Diaphoretic | Increased | Profuse (SLUDGE/DUMBELS) |
| Opioid (heroin, morphine, oxycodone, fentanyl) | Sedated, coma | Pinpoint (miosis) | Bradypnoea, bradycardia, hypotension, hypothermia | Normal | Decreased | None |
| Sedative-hypnotic (benzodiazepines, alcohol, barbiturates) | Sedated, ataxia, slurred speech | Normal or small | Bradypnoea, hypotension, hypothermia | Normal | Normal or decreased | None |
DCE examiner question: "This patient is agitated, hot, and has large pupils but dry skin. What is the toxidrome, and how do you distinguish it from a sympathomimetic?" Lead with the answer: "This is an anticholinergic toxidrome — the dry flushed skin and absent bowel sounds are the discriminators. The sympathomimetic patient is also hot and agitated with large pupils, but the skin is diaphoretic and the gut is overactive. The antidote question is the next step: physostigmine is rarely used for anticholinergic toxicity; I would manage supportively with cooling and benzodiazepines." [1]
The five toxidromes — pathophysiology to pattern
Sympathomimetic. Cocaine and amphetamines drive sympathetically mediated catecholamine release and reuptake blockade. The result is hypertension, tachycardia, mydriasis, hyperthermia, agitation and seizures. The diaphoresis is the discriminator from anticholinergic toxicity. The dangerous complications are hyperthermia (precipitates rhabdomyolysis, disseminated intravascular coagulation, multi-organ failure), hypertensive emergency, intracerebral haemorrhage, and coronary vasospasm causing ischaemia and dysrhythmia. Management is benzodiazepines (first-line, for both agitation and hyperthermia), active cooling, and alpha-blockade with a titratable agent for hypertension — never a beta-blocker alone, because unopposed alpha stimulation worsens vasospasm. [1]
Anticholinergic. Atropine, antihistamines (diphenhydramine), tricyclic antidepressants, antiparkinsonian agents and plant toxins (deadly nightshade, Datura) block muscarinic receptors. The classic mnemonic — "mad as a hatter, blind as a bat, dry as a bone, red as a beet, hot as a hare, full as a flask" — captures the delirium, mydriasis, anhidrosis, flushed skin, hyperthermia and urinary retention. The dangerous complications are hyperthermia and dysrhythmia (the latter from the sodium-channel-blocking property shared by many anticholinergics, notably TCAs). Management is supportive — benzodiazepines for agitation and seizure control, active cooling, and intravenous sodium bicarbonate for QRS widening. Physostigmine, a centrally acting cholinesterase inhibitor, reverses the central anticholinergic delirium but carries a risk of bradycardia, seizures and asystole; it is reserved for pure anticholinergic poisoning with severe agitation unresponsive to benzodiazepines, and is contraindicated if a TCA co-ingestion is possible. [1]
Cholinergic. Organophosphate and carbamate insecticides and nerve agents (sarin, VX) inhibit acetylcholinesterase, causing acetylcholine accumulation at muscarinic and nicotinic receptors. The muscarinic effects are captured by the mnemonics SLUDGE (Salivation, Lacrimation, Urination, Defecation, GI upset, Emesis) or DUMBELS (Diarrhoea, Urination, Miosis, Bronchorrhoea/bronchospasm/bradycardia, Emesis, Lacrimation, Salivation/secretions). The nicotinic effects — muscle fasciculations, weakness, paralysis, and the "days of the week" weakness pattern — are the muscle endplate overload. The most dangerous feature is bronchorrhoea causing respiratory failure, and the miosis and bronchospasm. Atropine dries the secretions (muscarinic effects) but does not reverse the nicotinic muscle weakness — that requires pralidoxime, which reactivates acetylcholinesterase before the enzyme-organophosphate bond "ages" irreversibly. Give pralidoxime early. [1]
Opioid. Heroin, morphine, oxycodone, fentanyl, methadone and codeine act on mu receptors causing the classic triad of pinpoint pupils, respiratory depression and coma. The danger is death from hypoxia. Naloxone is the antidote — a competitive mu antagonist. Titrate it to respiratory effort, not to full wakefulness: a dose that fully reverses a chronic user precipitates acute withdrawal, agitation, vomiting and aspiration. Start at 0.04 mg intravenously and double every two minutes up to 10 mg if there is no response. A non-responder at 10 mg is not opioid-toxic. For long-acting opioids (methadone, sustained-release morphine, fentanyl patches), a naloxone infusion is required because the opioid outlasts the antidote. [1]
Sedative-hypnotic. Benzodiazepines, alcohol, barbiturates and gamma-hydroxybutyrate (GHB) potentiate GABA or act at the GABA-A receptor. The result is slurred speech, ataxia, CNS depression, and in severe overdose, respiratory depression and hypotension. Flumazenil is the benzodiazepine antidote, but it is used far more selectively than naloxone: in a chronic benzodiazepine user or a mixed overdose with a pro-convulsant (notably a TCA), flumazenil precipitates seizures that are refractory to standard treatment. Reserve it for iatrogenic over-sedation from a known, isolated benzodiazepine in a benzodiazepine-naive patient. The management of most sedative-hypnotic overdose is supportive — airway, ventilation, and time. [1]
Gastrointestinal decontamination
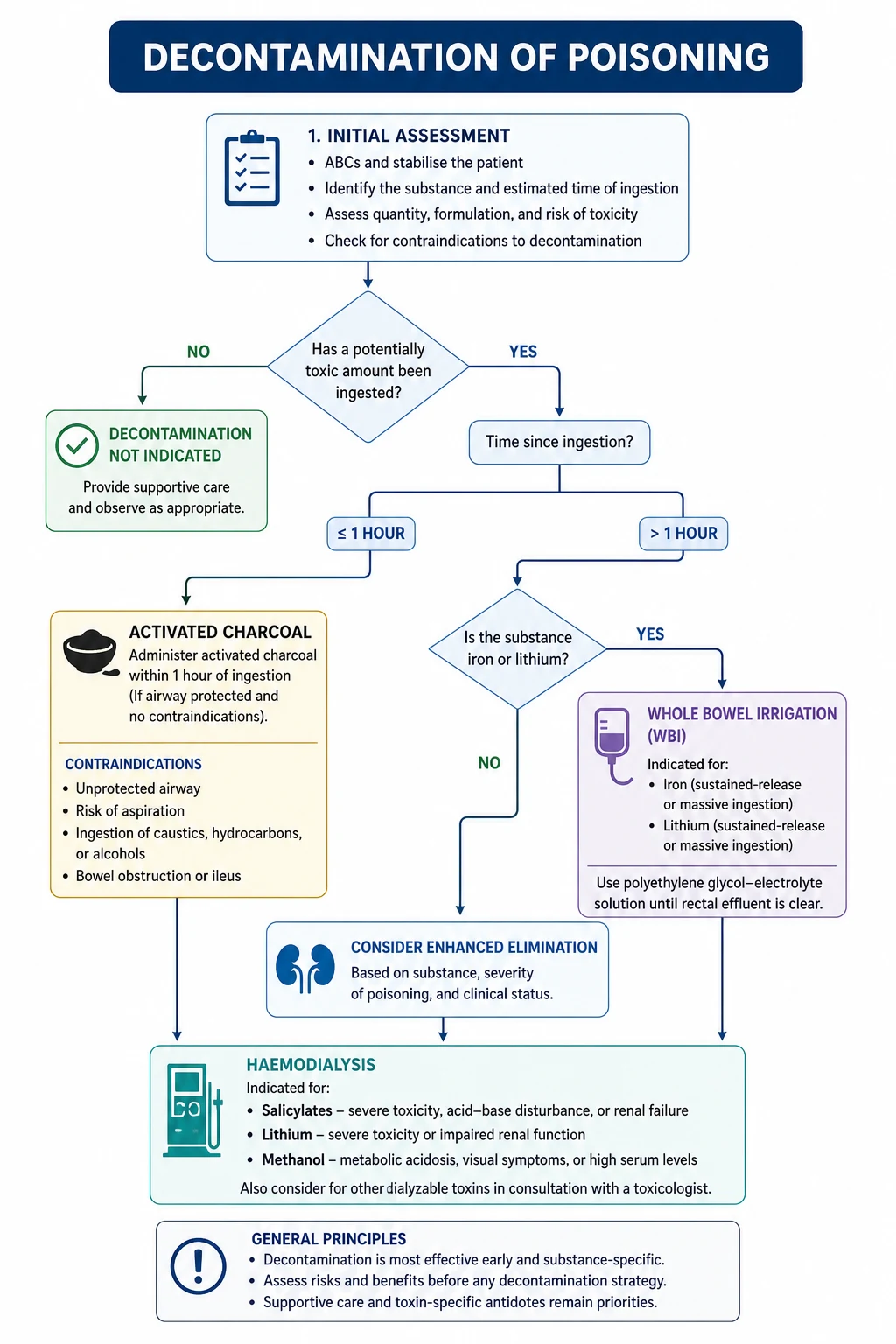
Decontamination removes toxin from the gut before it is absorbed. Three modalities survive in modern practice — activated charcoal, whole bowel irrigation, and (rarely) gastric lavage. Ipecac and cathartics as routine therapy have been abandoned. The overarching principle: decontamination is never performed before resuscitation and airway protection, and it is never routine — it is a targeted intervention for a toxin that binds charcoal, taken recently, in a patient whose airway is safe [3][4].
Activated charcoal
Activated charcoal is a fine black powder with an enormous surface area that adsorbs toxin in the gut lumen, preventing absorption. It is the workhorse of decontamination. [1]
When to give it: single-dose activated charcoal may be considered if a patient has ingested a potentially toxic amount of a charcoal-binding substance within the previous hour [3]. Volunteer data show a mean reduction in drug absorption of approximately 47% at 30 minutes, falling to 16% at two hours — the benefit after one hour is questionable. Dose: 50–100 g in adults (1 g/kg in children), given orally or via nasogastric tube.
Contraindications — memorise these:
- Altered mental status without a protected airway — the single most important contraindication. Aspiration of charcoal is catastrophic.
- Caustic ingestion (acids, alkalis) — charcoal does not bind caustics, endoscopically obscures the mucosa during assessment for burns, and may worsen injury.
- Bowel obstruction or ileus.
- Ingestion of a substance charcoal does not bind — metals (iron, lithium, lead), alcohols (ethanol, methanol, ethylene glycol), hydrocarbons, and corrosives. [1]
DWE exam trap: A patient presents 90 minutes after an overdose of a charcoal-binding drug with a normal conscious state. Should you give charcoal? The position paper says the benefit after one hour is questionable but "cannot be excluded." In a fully conscious patient with a charcoal-binding ingestion and a potentially toxic dose, many toxicologists still offer charcoal up to two hours, particularly for sustained-release formulations. The key discriminator is the airway and the conscious state, not a rigid clock. [1]
Gastric lavage
Gastric lavage — passing a large-bore orogastric tube and washing the stomach — has been abandoned as a routine intervention. The 2013 position paper update concluded there is no evidence it improves outcome and it carries real harms: hypoxia, aspiration, dysrhythmia, laryngospasm and perforation [4]. It is now considered only in the rare case of a life-threatening ingestion of a non-charcoal-binding substance within an hour of arrival, performed by an experienced operator with a protected airway. In practice it is almost never done.
Whole bowel irrigation
Whole bowel irrigation (WBI) flushes the entire gastrointestinal tract with a polyethylene glycol electrolyte solution at 1–2 L/hour via nasogastric tube until the effluent is clear. It does not rely on adsorption and works for substances charcoal cannot bind [5].
Indications:
- Iron overdose (charcoal does not bind iron; WBI and deferoxamine are the tools).
- Lithium overdose with sustained-release formulations.
- Sustained-release or enteric-coated drug ingestions presenting more than two hours after ingestion (the drug is still in transit).
- Body packers (ingested packets of illicit drug) and body stuffers (hurriedly swallowed loose drug).
- Potentially toxic ingestions of agents poorly adsorbed by charcoal. [1]
Contraindications: bowel obstruction, perforation, ileus, haemodynamic instability, and an unprotected airway. [1]
Enhanced elimination
Once the toxin is absorbed, the question becomes whether elimination can be accelerated. Three techniques are in regular use: urinary alkalinisation, multi-dose activated charcoal, and haemodialysis (and related extracorporeal therapies). Forced diuresis and the obsolete "alkaline/forced diuresis" regimens have been abandoned — the position paper explicitly retired the term, because pH manipulation, not diuresis, is the active mechanism [7].
Urinary alkalinisation
Weak acids are trapped in an alkaline urine as their ionised (charged) form, which cannot be reabsorbed across the tubular epithelium and is excreted. The clinical application is salicylate toxicity. [1]
Give intravenous sodium bicarbonate (1–2 mmol/kg bolus, then an infusion of roughly 100–150 mmol sodium bicarbonate in 1 L of 5% dextrose with 20–40 mmol potassium chloride at 1.5–2 times maintenance) to achieve a urine pH of 7.5–8.0. The target is the urine pH, not the serum pH. Hypokalaemia must be corrected first, because potassium depletion prevents the distal tubule from excreting hydrogen ion and alkalinising the urine [7].
The same principle applies to phenobarbital and methotrexate. It does not apply to most other toxins, and it does not apply to TCAs (whose cardiotoxicity is itself treated with bicarbonate, but not by the alkalinisation-elimination mechanism). [1]
Multi-dose activated charcoal
Repeated doses of charcoal (25–50 g every four hours, or 12.5 g/hour) enhance elimination by interrupting the enterohepatic and enterogastric recirculation of drugs that have already been absorbed — the gut acts as a dialyser, pulling drug back out of the bloodstream across the intestinal wall ("gastrointestinal dialysis") [6].
The 1999 position statement recommends multi-dose charcoal for life-threatening ingestion of carbamazepine, dapsone, phenobarbital, quinine, or theophylline. Volunteer data show enhanced elimination for many other drugs — digoxin, phenytoin — but clinical outcome benefit is unproven. It must not be given if the airway is unprotected, if there is bowel obstruction, or if ileus has developed. [1]
Haemodialysis and extracorporeal removal
Haemodialysis removes toxins that are small, water-soluble, low in protein binding, and small in volume of distribution. The EXTRIP (Extracorporeal Treatments in Poisoning) workgroup has issued toxin-specific recommendations using a modified Delphi and GRADE methodology. [1]
The toxins that are dialysable and for which dialysis changes outcome are captured by the mnemonic SLIME (and a few additions): [1]
- Salicylates — haemodialysis for severe toxicity (altered mental status, refractory acidosis, salicylate level over 7.2 mmol/L or 100 mg/dL, or pulmonary oedema) [8].
- Lithium — haemodialysis for severe acute or acute-on-chronic toxicity with renal failure, seizures, or a level above 4–5 mmol/L in an acute overdose [9].
- Methanol and ethylene glycol (toxic alcohols) — haemodialysis to remove the parent alcohol and its toxic metabolites, correct the acidosis, and supply fomepizole or ethanol during the run [2].
- E — and the additions: metformin (metformin-associated lactic acidosis, MALA), theophylline, valproate, barbiturates (long-acting), and salicylates (already named).
Lithium deserves a specific point: it has a small volume of distribution but diffuses slowly out of cells, so a single dialysis run is followed by a rebound. Repeat dialysis or a sustained low-efficiency dialysis (SLED) is often required [9].
DWE high-yield: The classic distractor is "what is dialysable?" The answer is NOT "everything that is small." Protein binding and volume of distribution dominate. Digoxin is highly protein-bound and has a huge volume of distribution — it is NOT dialysable, and the antidote is digoxin-specific Fab antibodies. TCAs are similarly not dialysable. The dialysable list is short: salicylate, lithium, methanol, ethylene glycol, metformin, theophylline, valproate, barbiturates. [1]
The antidote reference table
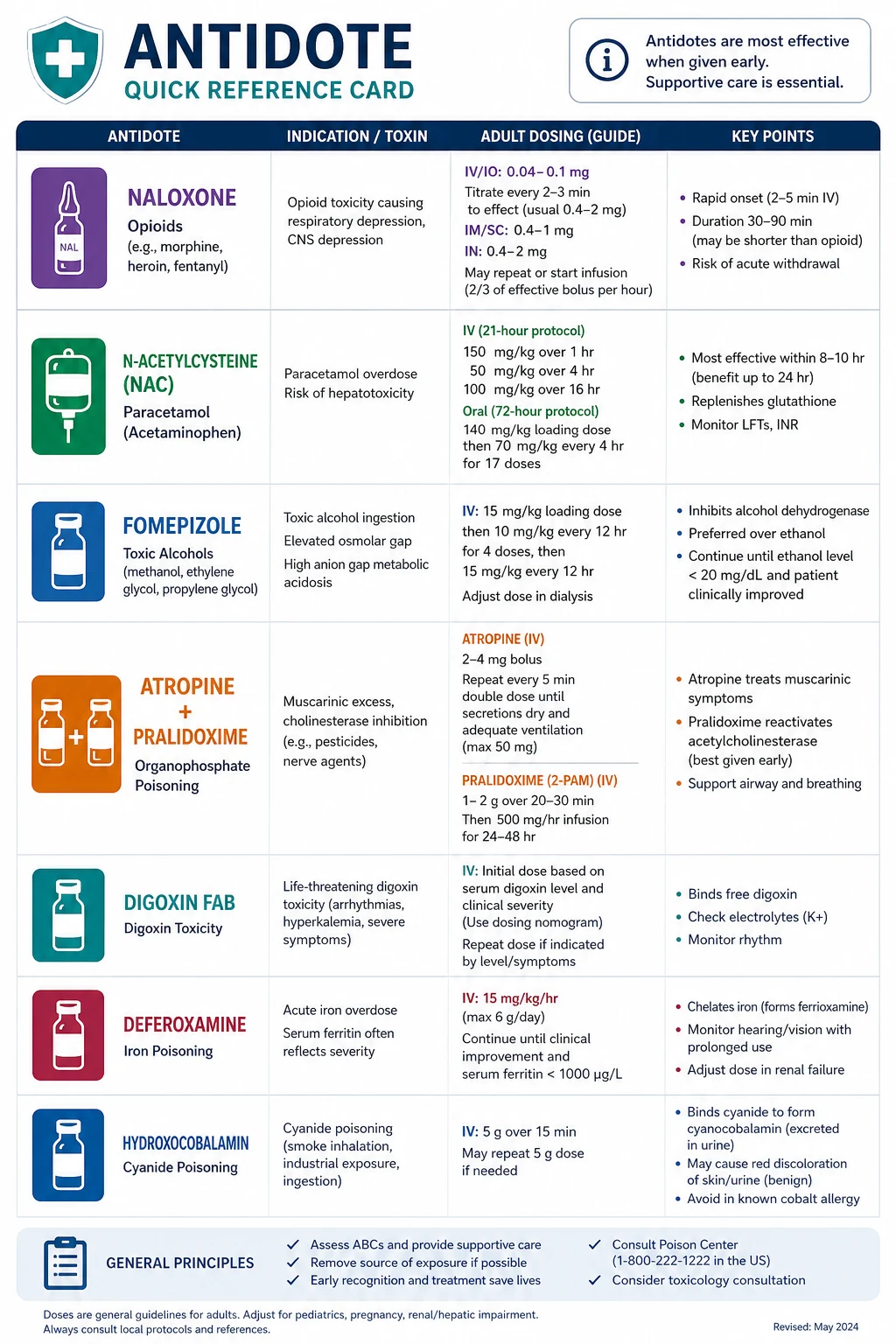
A working physician needs the core antidote table committed to memory. Every entry below is examinable at viva depth. [1]
| Toxin / class | Antidote | Mechanism | Key dose and point |
|---|---|---|---|
| Opioids | Naloxone | Competitive mu-receptor antagonist | 0.04–0.4 mg IV titrated to respiratory effort; infusion for long-acting opioids |
| Paracetamol | N-acetylcysteine (NAC) | Restores glutathione; sulphates the toxic NAPQI metabolite | 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours; effective up to and beyond 24 hours if there is hepatotoxicity |
| Methanol / ethylene glycol | Fomepizole (or ethanol) | Inhibits alcohol dehydrogenase, preventing formation of toxic metabolites | Fomepizole 15 mg/kg loading, then 10 mg/kg q12h; plus haemodialysis for severe toxicity |
| Digoxin | Digoxin-specific Fab antibody fragments | Bind digoxin for renal elimination | Life-threatening dysrhythmia, hyperkalaemia over 5 mmol/L, or chronic level over 6 nmol/L; dose by serum level or body load |
| Tricyclic antidepressants | Sodium bicarbonate | Overcomes sodium-channel blockade; raises serum pH, shifting drug off the channel | 1–2 mmol/kg IV bolus to narrow the QRS; target pH 7.50–7.55 |
| Cyanide | Hydroxocobalamin | Binds cyanide to form cyanocobalamin (vitamin B12) | 5 g IV (70 mg/kg), repeat once; first-line in smoke inhalation; avoids the hypotension of sodium thiossulphate and the methaemoglobinaemia of the nitrite kit |
| Sulfonylureas | Octreotide | Somatostatin analogue; suppresses pancreatic insulin secretion | 50 mcg subcutaneously q8h; for hypoglycaemia refractory to or rebounding after dextrose [10] |
| Beta-blockers | High-dose insulin / euglycaemia therapy | Shifts myocardial metabolism to carbohydrate; inotropic | Regular insulin 1 unit/kg bolus then 0.5–1 unit/kg/hour with glucose to maintain euglycaemia |
| Local anaesthetic (LAST) / lipophilic drugs | 20% lipid emulsion | Lipid sink — sequesters lipophilic toxin from the receptor | 1.5 mL/kg bolus then 0.25 mL/kg/min infusion; first-line for bupivacaine cardiovascular collapse |
| Calcium-channel blockers | Calcium, high-dose insulin, lipid emulsion | Calcium overcomes channel blockade; insulin is inotropic | Calcium chloride 10 mL of 10% IV; insulin as above; lipid for refractory cases |
| Warfarin / superwarfarins | Vitamin K (phytomenadione) | Cofactor for factors II, VII, IX, X | 5–10 mg IV slowly for warfarin reversal; much higher doses and prolonged course for superwarfarin (rat poison) |
| Methaemoglobinaemia (nitrates, dapsone, benzocaine) | Methylene blue | Reduces methaemoglobin to haemoglobin | 1–2 mg/kg IV; avoid in G6PD deficiency (causes haemolysis) |
Toxin-specific deep dives — the high-yield poisonings
Paracetamol (acetaminophen) — the antidote is time-critical
Paracetamol is the commonest cause of acute liver failure in the developed world. At therapeutic doses, paracetamol is metabolised by glucuronidation and sulphation, with a small fraction passing through cytochrome P450 2E1 to form the hepatotoxic intermediate NAPQI. Glutathione detoxifies NAPQI. In overdose, the conjugation pathways saturate, NAPQI accumulates, glutathione is depleted, and NAPQI binds hepatocytes causing centrilobular necrosis. [1]
The management logic: N-acetylcysteine (NAC) replenishes glutathione and is a sulphate donor for direct paracetamol conjugation. It is most effective within 8 hours of ingestion, but it is still beneficial in established hepatotoxicity — the "late NAC" benefit reduces mortality even in patients who present with acute liver failure up to and beyond 24 hours. The trap is to withhold NAC because the patient "presented too late." If there is hepatotoxicity, give NAC. [1]
Plot the serum paracetamol level against the Rumack-Matthew nomogram (treatment line starting at 150 mg/L or 1000 micromol/L at four hours, declining semi-logarithmically) for single acute ingestions between 4 and 24 hours. Levels before four hours are uninterpretable. After 24 hours, treat on clinical and biochemical grounds (transaminitis, coagulopathy, acidosis). [1]
DWE exam trap: The patient with a staggered overdose or an unknown time of ingestion cannot be plotted on the nomogram. Treat with NAC. The nomogram applies only to a single acute ingestion with a known time. [1]
Salicylates — the mixed acid-base pattern
Salicylate toxicity produces a characteristic mixed respiratory alkalosis and high anion gap metabolic acidosis. Salicylates directly stimulate the medullary respiratory centre (respiratory alkalosis) and uncouple oxidative phosphorylation, driving lactic and ketoacid production (high anion gap metabolic acidosis). A patient who is hyperventilating, tinnitus-affected, agitated or confused, and has a mixed disorder on the blood gas has salicylate toxicity until proven otherwise. [1]
Management is urinary alkalinisation (sodium bicarbonate to a urine pH of 7.5–8.0) for moderate toxicity, and haemodialysis for severe toxicity. The EXTRIP workgroup recommends haemodialysis for altered mental status, pulmonary oedema or refractory acidosis, and for a salicylate level over 7.2 mmol/L (100 mg/dL) regardless of symptoms [8]. Do not intubate a salicylate-toxic patient without being ready to dialyse — the loss of their compensatory hyperventilation under sedation causes a precipitous fall in pH and cardiac arrest. Dialyse before, or concurrent with, intubation.
Tricyclic antidepressants — the QRS is the predictor
TCAs (amitriptyline, nortriptyline, dothiepin) cause toxicity through three mechanisms: sodium-channel blockade (cardiotoxicity, QRS widening, ventricular dysrhythmia), alpha-1 blockade (hypotension), and anticholinergic effects (tachycardia, delirium). The QRS duration predicts the risk of dysrhythmia and seizures — a QRS over 100 ms warrants bicarbonate; over 160 ms carries a 50% seizure risk. The terminal R wave in aVR (over 3 mm) is a high-yield ECG discriminator. [1]
The antidote is intravenous sodium bicarbonate. It works by two mechanisms: providing a sodium load to overcome the channel blockade, and alkalinising the serum, which increases the fraction of the drug in its neutral (sodium-channel-unbound) form. Give 1–2 mmol/kg as a bolus, repeat to narrow the QRS, then infuse to maintain a pH of 7.50–7.55. Avoid class Ia and Ic antiarrhythmics (they worsen the blockade) — ventricular dysrhythmias are treated with bicarbonate and, if needed, lipid emulsion. [1]
Digoxin — the Fab antibody calculation
Digoxin toxicity (chronic accumulation in renal failure, or acute overdose) presents with nausea, vomiting, confusion, hyperkalaemia (from inhibition of the Na-K ATPase), and a characteristic spectrum of dysrhythmias — premature ventricular beats, bradycardia, atrial tachycardia with block, and bidirectional ventricular tachycardia. Hyperkalaemia in digoxin toxicity is a marker of toxicity, not a target for standard hyperkalaemia therapy — give the Fab antibodies; do not give calcium (theoretical risk of "stone heart," although the evidence is weak). [1]
The Fab antibody dose is calculated from the serum digoxin level and the estimated volume of distribution, or from the ingested dose, or empirically (10–20 vials for an acute overdose in a patient who has not yet developed levels). Digoxin is NOT dialysable — high protein binding and a large volume of distribution. [1]
Methanol and ethylene glycol — the osmolar and anion gaps
Toxic alcohols are metabolised by alcohol dehydrogenase to highly toxic organic acids. Methanol becomes formic acid (causing blindness through retinal and optic nerve toxicity); ethylene glycol becomes glycolic and oxalic acid (causing severe metabolic acidosis, hypocalcaemia, and acute kidney injury from calcium oxalate crystallisation). [1]
The classic finding early is a high osmolar gap (the parent alcohol is osmotically active) and, as metabolism proceeds, a high anion gap metabolic acidosis. As the parent alcohol is metabolised, the osmolar gap falls and the anion gap rises — a late-presenting patient may have a normal osmolar gap with a severe anion-gap acidosis. Examine the urine for crystals (envelope-shaped calcium oxalate monohydrate) in ethylene glycol [2].
Fomepizole (15 mg/kg loading, then 10 mg/kg every 12 hours) blocks alcohol dehydrogenase and halts the production of toxic metabolites. Add folate (methanol, to accelerate formate metabolism) and thiamine and pyridoxine (ethylene glycol, to divert metabolism away from oxalate). Haemodialysis removes both the parent alcohol and the metabolites and corrects the acidosis — indicated for severe acidosis, renal failure, visual symptoms (methanol), or a high level. [1]
Organophosphates — atropine plus pralidoxime
Organophosphate poisoning is a leading cause of poisoning death globally, from agricultural insecticide exposure. The cholinergic crisis is dominated by bronchorrhoea, bronchospasm, miosis, and muscle fasciculations with weakness. The immediate threat to life is respiratory failure from bronchorrhoea and respiratory muscle weakness. [1]
Atropine reverses the muscarinic effects — titrate to the drying of secretions (target a clear chest, dry mouth), NOT to the heart rate or pupil size. Doses of tens to hundreds of milligrams may be required. Pralidoxime reactivates acetylcholinesterase, reversing the nicotinic effects (muscle weakness) — give it early, because the enzyme-inhibitor bond "ages" irreversibly over hours (the aging time varies: soman ages in minutes, parathion in hours), after which pralidoxime is ineffective. The classic exam error is to use atropine alone and to leave the patient with residual muscle weakness that pralidoxime would have reversed. [1]
Sulfonylurea — octreotide for rebound hypoglycaemia
Sulfonylureas (glibenclamide/glyburide, glipizide, gliclazide) stimulate pancreatic beta-cell insulin release. Overdose causes profound and prolonged hypoglycaemia. The trap is that intravenous dextrose stimulates further insulin release, causing rebound hypoglycaemia as soon as the dextrose infusion is stopped. Octreotide, a somatostatin analogue, suppresses insulin secretion and prevents the rebound [10]. Give dextrose to correct the hypoglycaemia, then octreotide 50 mcg subcutaneously every 8 hours. Observe for at least 12–24 hours, because sulfonylurea-induced hypoglycaemia can recur for a prolonged period.
Local anaesthetic systemic toxicity (LAST) — lipid emulsion
Bupivacaine and ropivacaine, when intravascularly absorbed or overdosed, cause CNS excitation (tinnitus, perioral tingling, seizures) followed by cardiovascular collapse from potent sodium-channel blockade in the myocardium. The collapse is refractory to standard resuscitation. 20% lipid emulsion creates a "lipid sink" — an intravascular lipid phase that sequesters the lipophilic local anaesthetic away from cardiac receptors. Give 1.5 mL/kg bolus, then 0.25 mL/kg/min infusion, with a maximum of about 12 mL/kg. Continue standard ACLS (the prolonged resuscitation in LAST is justified — recovery can occur after a long arrest). The ASRA LAST checklist is the bedside reference. [1]
DCE long-case approach
Patient scenario
Mr David Chen, 28, software engineer, is brought to the emergency department by ambulance after being found drowsy at home by his partner, with empty blister packs of amitriptyline (50 mg, perhaps 40 tablets) and paracetamol (500 mg, perhaps 30 tablets) beside him, and an unknown amount of alcohol. The time of ingestion is uncertain but the partner estimates 4–6 hours ago. [1]
Candidate's opening statement (SASPOP)
"Mr Chen is a 28-year-old software engineer who presents with a deliberate mixed overdose of amitriptyline and paracetamol with alcohol, an uncertain 4 to 6 hours ago. He is drowsy but rousable. His main problems are: a tricyclic antidepressant overdose with impending cardiotoxicity, a paracetamol ingestion that requires urgent risk stratification and likely N-acetylcysteine, alcohol co-ingestion, and an underlying psychiatric crisis. My immediate priorities are the ABCDE assessment with attention to the QRS for TCA cardiotoxicity, a four-hour paracetamol level against the nomogram, and early N-acetylcysteine." [1]
Problem list
- TCA overdose — monitor ECG continuously for QRS widening; have sodium bicarbonate ready.
- Paracetamol overdose — send a level at four hours; plot on the Rumack-Matthew nomogram; expect to start NAC.
- Alcohol co-ingestion — check glucose (risk of hypoglycaemia); BAC.
- Airway risk — drowsy and deteriorating; protect before any decontamination.
- Psychiatric — once medically stable, risk assessment and mental health review. [1]
Integrated management plan
- Resuscitate and protect the airway: ABCDE, oxygen, continuous cardiac monitoring, two large-bore cannulae. Intubate early if the GCS falls or the airway is threatened. The TCA and alcohol are both CNS depressants; the trajectory is downward.
- ECG and cardiac monitoring: measure the QRS. If over 100 ms, give sodium bicarbonate 1–2 mmol/kg IV bolus and repeat to narrow. The QRS is the single most important prognostic marker. [1]3. Decontamination — charcoal is contraindicated initially: his conscious state is falling and his airway is not protected. If he is intubated, give 50 g activated charcoal via NG tube for the TCA (charcoal binds amitriptyline). Do not give charcoal before the airway is secured.
- Paracetamol management: send a paracetamol level at four hours post-ingestion. Plot on the nomogram. Given the dose (15 g) and unknown timing, he is likely above the treatment line — start NAC at the four-hour mark if the level is not yet back, and stop if it is below the line.
- Glucose: check a bedside glucose immediately — alcohol plus a reduced oral intake risks hypoglycaemia. Give 50% dextrose if low.
- Investigations: ECG, venous gas, electrolytes including magnesium, liver function and coagulation (paracetamol baseline), lipase, beta-hCG in a woman of reproductive age, and a serum paracetamol and salicylate level on all overdoses.
- ICU referral: for a TCA overdose with cardiotoxicity or a falling GCS, refer to ICU early.
- Psychiatric: once medically cleared, suicide-risk assessment and psychiatric review. [1]
DCE examiner probing questions:
- "His QRS is 140 ms. What do you do?" → "Give intravenous sodium bicarbonate 1 to 2 mmol per kilogram as a bolus, repeated to narrow the QRS, then an infusion to maintain a serum pH of 7.50 to 7.55. The QRS over 100 ms predicts cardiotoxicity, and over 160 ms carries a 50% seizure risk."
- "When would you give charcoal?" → "Only after his airway is protected by intubation. He is drowsy and his conscious state is falling — the single most dangerous contraindication to charcoal is an unprotected airway, because aspiration of charcoal causes a catastrophic chemical pneumonitis. If he is intubated, I give 50 g via NG tube for the amitriptyline, which binds charcoal."
- "Would you use flumazenil?" → "No. Flumazenil is contraindicated in a mixed overdose with a pro-convulsant such as a TCA — it precipitates seizures. I would reserve flumazenil for isolated, iatrogenic benzodiazepine over-sedation in a benzodiazepine-naive patient." [1]
DCE short-case discussion: the toxidrome at the bedside
Instruction: "This patient was brought in unconscious. Examine him and tell me what you find." [1]
Systematic examination routine
- End of the bed: unconscious patient, respiratory rate and pattern, colour, any diaphoresis or flushing, any needle marks or transdermal patches on inspection.
- Vital signs: temperature, pulse, blood pressure, respiratory rate, oxygen saturation, glucose.
- Eyes: pupil size and reactivity (pinpoint, dilated, or normal), presence or absence of nystagmus, lacrimation.
- Skin: moist or dry, flushed or pale, any track marks, any transdermal patches, capillary refill.
- Chest: auscultate for bronchorrhoea (wet crackles that do not clear) or bronchospasm (wheeze), bowel sounds, bladder (urinary retention).
- Neurological: GCS, tone, reflexes, muscle fasciculations (cholinergic nicotinic effect), ataxia. [1]
Presentation template
"I have examined an unconscious patient. He has pinpoint pupils, a respiratory rate of 6, a slow pulse of 50, and is hypothermic at 35. His skin is normal and he has no fasciculations. This is the classic opioid toxidrome — pinpoint pupils, respiratory depression, and coma. My immediate action is to give naloxone 0.04 milligrams intravenously, titrated to his respiratory effort, while preparing to secure his airway." [1]
Discussion questions
Examiner: "How would you distinguish this from a sedative-hypnotic overdose?" [1]
"The pupils are the discriminator. The opioid toxidrome has pinpoint pupils; the sedative-hypnotic toxidrome has normal or only mildly small pupils. The respiratory depression overlaps. If the patient does not respond to a naloxone challenge of up to 10 milligrams, I would conclude this is not primarily opioid-mediated and broaden the differential — sedative-hypnotic, alcohol, a severe metabolic encephalopathy, or a structural brainstem lesion." [1]
Examiner: "Name three toxidromes that cause a depressed conscious state, and the antidote for each." [1]
"First, opioid — naloxone, a competitive mu antagonist, titrated to respiratory effort. Second, benzodiazepine — flumazenil, used only in a benzodiazepine-naive patient with an isolated overdose. Third, there is no single antidote for alcohol or barbiturate toxicity; management is supportive. If I may add a fourth, organophosphate poisoning causes a depressed conscious state in its later phase, treated with atropine and pralidoxime." [1]
Examiner: "What is the most common error candidates make when giving naloxone?" [1]
"Giving a large bolus to reverse the patient fully, rather than titrating to respiratory effort. A full reversal in a chronic opioid user precipitates acute withdrawal — agitation, vomiting, aspiration, and pain. I titrate to restore an adequate respiratory rate, accepting that the patient may remain drowsy." [1]
Key DWE MCQ patterns
- Identify the toxidrome from the sign cluster. Agitation, mydriasis, hyperthermia, diaphoresis, tachycardia — sympathomimetic. Same picture with dry flushed skin and absent bowel sounds — anticholinergic. The skin and bowel sounds are the discriminators.
- Recognise the cholinergic crisis and choose atropine plus pralidoxime. Miosis, bronchorrhoea, fasciculations, SLUDGE — organophosphate. Atropine alone leaves the muscle weakness; pralidoxime is required early, before the enzyme ages.
- The contraindication to charcoal. The stem describes a drowsy patient after an overdose; the trap is to reach for charcoal. The airway is unprotected — charcoal is contraindicated.
- Choose the dialysable toxin. Among digoxin, TCA, lithium, beta-blocker — only lithium is dialysable. Protein binding and volume of distribution dominate the decision.
- Salicylate toxicity — the blood gas. A mixed respiratory alkalosis and high anion gap metabolic acidosis in an agitated, tinnitus-affected patient — salicylates. The answer is urinary alkalinisation, and haemodialysis for severe toxicity.
- TCA cardiotoxicity — the ECG and bicarbonate. A wide QRS after TCA overdose — intravenous sodium bicarbonate. Avoid class Ia/Ic antiarrhythmics.
- Octreotide for sulfonylurea rebound. A patient on glibenclamide with refractory hypoglycaemia after dextrose — the answer is octreotide to suppress insulin release; dextrose alone causes rebound.
- Toxic alcohol — fomepizole before the level returns. A high anion gap acidosis with a high osmolar gap and visual symptoms — methanol. Give fomepizole empirically; the osmolar gap falls as the parent alcohol metabolises, so a late presentation may have a normal osmolar gap. [1]
References
[1] Erickson TB, Thompson TM, Lu JJ. The approach to the patient with an unknown overdose. Emerg Med Clin North Am 2007;25(2):249–81. The canonical review of the systematic ABCDE approach, toxidrome recognition, and the logic of decontamination and antidotes for the undifferentiated poisoned patient.
[2] Kraut JA, Mullins ME. Toxic alcohols. N Engl J Med 2018;378:270–80. The definitive modern review of methanol, ethylene glycol and related alcohols — the anion and osmolar gaps, fomepizole, cofactors and haemodialysis.
[3] Chyka PA, Seger D, Krenzelok EP, Vale JA. Position paper: Single-dose activated charcoal. Clin Toxicol 2005;43(2):61–87. The AACT/EAPCCT consensus on the one-hour window, the charcoal-binding substances, and the airway contraindication.
[4] Benson BE, Hoppu K, Troutman WG, et al. Position paper update: gastric lavage for gastrointestinal decontamination. Clin Toxicol 2013;51(3):140–6. The consensus that retires routine gastric lavage because of unproven benefit and real harms.
[5] Thanacoody R, Caravati EM, Troutman WG, et al. Position paper update: whole bowel irrigation for gastrointestinal decontamination of overdose patients. Clin Toxicol 2015;53(1):5–12. The modern indications for WBI — iron, lithium, sustained-release formulations, body packers.
[6] American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. J Toxicol Clin Toxicol 1999;37(6):731–51. The consensus restricting multi-dose charcoal to life-threatening carbamazepine, dapsone, phenobarbital, quinine and theophylline.
[7] Proudfoot AT, Krenzelok EP, Vale JA. Position paper on urine alkalinization. J Toxicol Clin Toxicol 2004;42(1):1–26. The consensus defining urinary alkalinisation (not "forced alkaline diuresis") as a pH-manipulation strategy for salicylates and phenobarbital.
[8] Juurlink DN, Gosselin S, Kielstein JT, et al. Extracorporeal treatment for salicylate poisoning: systematic review and recommendations from the EXTRIP workgroup. Ann Emerg Med 2015;66(2):165–81. The evidence-based thresholds for haemodialysis in salicylate toxicity.
[9] Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal treatment for lithium poisoning: systematic review and recommendations from the EXTRIP workgroup. Clin J Am Soc Nephrol 2015;10(5):875–87. The indications for haemodialysis in lithium toxicity and the need for repeat dialysis due to rebound.
[10] Fasano CJ, O'Malley G, Dominici P, Aguilera E, Latta DR. Comparison of octreotide and standard therapy versus standard therapy alone for the treatment of sulfonylurea-induced hypoglycemia. Ann Emerg Med 2008;51(4):400–6. The randomised trial demonstrating that octreotide reduces recurrent hypoglycaemia in sulfonylurea overdose.
Erickson et al., Emerg Med Clin North Am 2007; Kraut & Mullins, NEJM 2018; AACT/EAPCCT position papers; EXTRIP workgroup recommendations; ASRA Pain Medicine LAST Checklist. [1]
References
- [1]Erickson TB, Thompson TM, Lu JJ The approach to the patient with an unknown overdose Emerg Med Clin North Am, 2007.PMID 17482020
- [2]Kraut JA, Mullins ME Toxic Alcohols N Engl J Med, 2018.PMID 29342392
- [3]Chyka PA, Seger D, Krenzelok EP, Vale JA Position paper: Single-dose activated charcoal Clin Toxicol (Phila), 2005.PMID 15822758
- [4]Benson BE, Hoppu K, Troutman WG, et al. Position paper update: gastric lavage for gastrointestinal decontamination Clin Toxicol (Phila), 2013.PMID 23418938
- [5]Thanacoody R, Caravati EM, Troutman WG, et al. Position paper update: whole bowel irrigation for gastrointestinal decontamination of overdose patients Clin Toxicol (Phila), 2015.PMID 25511637
- [6]American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists J Toxicol Clin Toxicol, 1999.PMID 10584586
- [7]Proudfoot AT, Krenzelok EP, Vale JA Position Paper on urine alkalinization J Toxicol Clin Toxicol, 2004.PMID 15083932
- [8]Juurlink DN, Gosselin S, Kielstein JT, et al. Extracorporeal Treatment for Salicylate Poisoning: Systematic Review and Recommendations From the EXTRIP Workgroup Ann Emerg Med, 2015.PMID 25986310
- [9]Decker BS, Goldfarb DS, Dargan PI, et al. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [10]Fasano CJ, O'Malley G, Dominici P, Aguilera E, Latta DR Comparison of octreotide and standard therapy versus standard therapy alone for the treatment of sulfonylurea-induced hypoglycemia Ann Emerg Med, 2008.PMID 17764782