Phys · pharmacological
Serotonin Syndrome and Neuroleptic Malignant Syndrome
Also known as serotonin syndrome · serotonin toxicity · neuroleptic malignant syndrome · NMS · drug-induced hyperthermia syndrome · malignant catatonia
Consultant-physician-depth guide to the drug-induced hyperthermia syndromes — serotonin syndrome (excess serotonergic activity) and neuroleptic malignant syndrome (dopamine blockade) — including the clinical triad, the Hunter criteria, the SS-versus-NMS-versus-malignant-hyperthermia comparison, cyproheptadine and dantrolene pharmacology, and ICU supportive care, structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Serotonin Syndrome and Neuroleptic Malignant Syndrome



The one-minute consultant answer
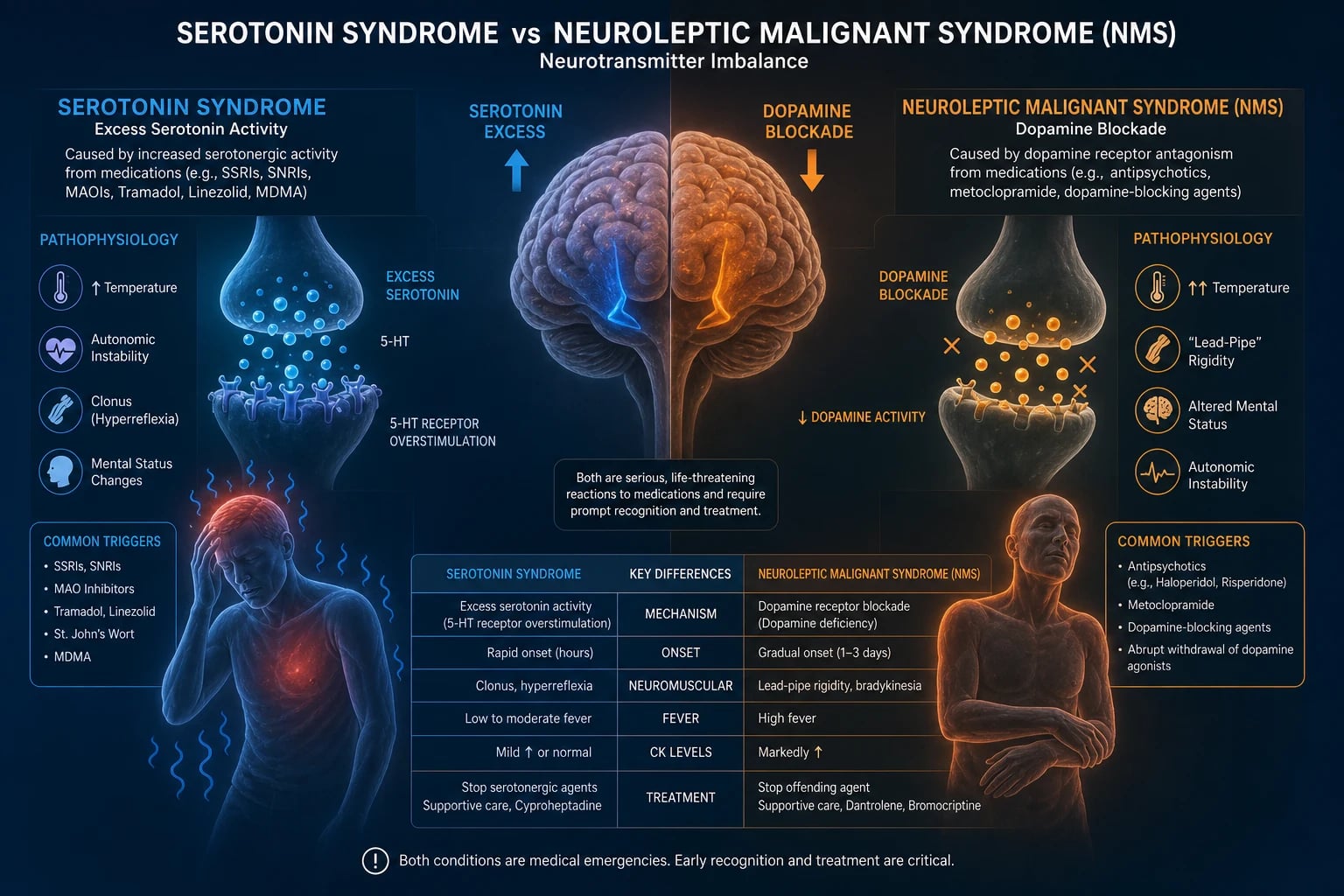
Serotonin syndrome is drug-induced excess serotonergic activity in the central and peripheral nervous systems, producing the clinical triad of neuromuscular hyperactivity (clonus — especially inducible or ocular, hyperreflexia, myoclonus, rigidity that is greater in the lower than the upper limbs), autonomic instability (hyperthermia, tachycardia, hypertension, mydriasis, diaphoresis, flushing) and altered mental status (agitation, confusion, delirium) with onset within hours of a dose change or a serotonergic drug interaction [1][2]. Neuroleptic malignant syndrome (NMS) is the mirror image: profound dopamine D2 receptor blockade (or sudden withdrawal of dopaminergic therapy in Parkinson disease) producing lead-pipe rigidity (greater in the upper than the lower limbs), hyperthermia often above 40 degrees, altered mental status, autonomic instability, and a gradual onset over days to weeks with elevated creatine kinase and leukocytosis [3][4].
The discriminating bedside rule is simple: onset in hours plus clonus and hyperreflexia points to serotonin syndrome; onset over days plus lead-pipe rigidity and bradyreflexia points to NMS [5]. Management of both is: stop the offending agent, provide aggressive supportive care (cooling, benzodiazepines for agitation and rigidity, airway protection), and treat the cause pharmacologically — cyproheptadine (a 5-HT2A antagonist) for moderate-to-severe serotonin syndrome, and dantrolene plus bromocriptine or amantadine for severe NMS [1][6]. Both are medical emergencies; the febrile, rigid, agitated patient needs the diagnosis made at the bedside, not after the bloods return.
The Three Drug-Induced Hyperthermia Syndromes
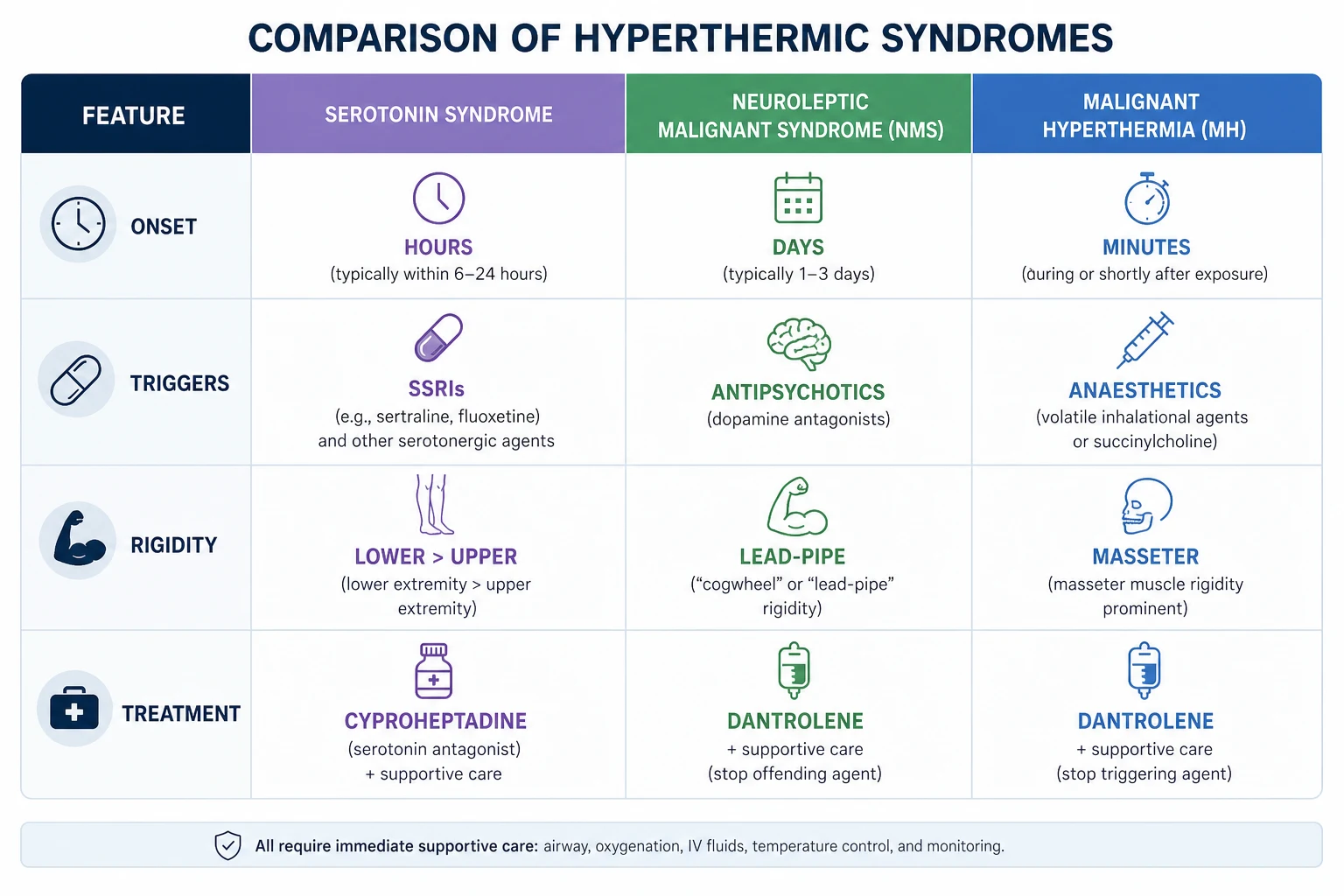
Three syndromes share the core features of hyperthermia, rigidity and autonomic instability but have entirely different triggers, mechanisms, onset, rigidity patterns and treatments. Confusing them kills patients. The table below is the high-yield discriminator you must memorise. [1]
| Feature | Serotonin syndrome | Neuroleptic malignant syndrome | Malignant hyperthermia |
|---|---|---|---|
| Mechanism | Excess 5-HT (5-HT2A stimulation) | Dopamine D2 blockade | Ryanodine receptor (RYR1) defect |
| Classic trigger | SSRI/SNRI plus MAOI, tramadol, linezolid, methylene blue, triptan, St John's wort, MDMA | Antipsychotic (typical or atypical), metoclopramide; withdrawal of dopaminergic drugs in Parkinson disease | Volatile anaesthetics (halothane, sevoflurane, desflurane), succinylcholine |
| Onset | Hours (within 24 hours, often minutes after an interaction) | Days to weeks (median 4 to 7 days; up to 30 days) | Minutes to hours of anaesthesia |
| Rigidity | Lower greater than upper; clonus, hyperreflexia, myoclonus | Upper greater than lower; lead-pipe, bradyreflexia | Generalised, especially masseter; rhabdomyolysis |
| Reflexes | Hyperreflexia, clonus (inducible, ocular) | Bradyreflexia, rigidity | Variable |
| Temperature | Mild in most; severe cases may exceed 41 | Often above 40 | Rapid rise above 39 |
| Creatine kinase | Mildly elevated | Markedly elevated (rhabdomyolysis) | Markedly elevated |
| Definitive treatment | Cyproheptadine (5-HT2A antagonist), benzodiazepines | Dantrolene, bromocriptine or amantadine | Dantrolene (ryanodine receptor antagonist) |
The single most-tested contrast is the onset and the rigidity pattern: rapid onset with clonus is serotonin; gradual onset with lead-pipe rigidity is NMS [5].
Serotonin Syndrome
Pathophysiology — why excess serotonin does what it does
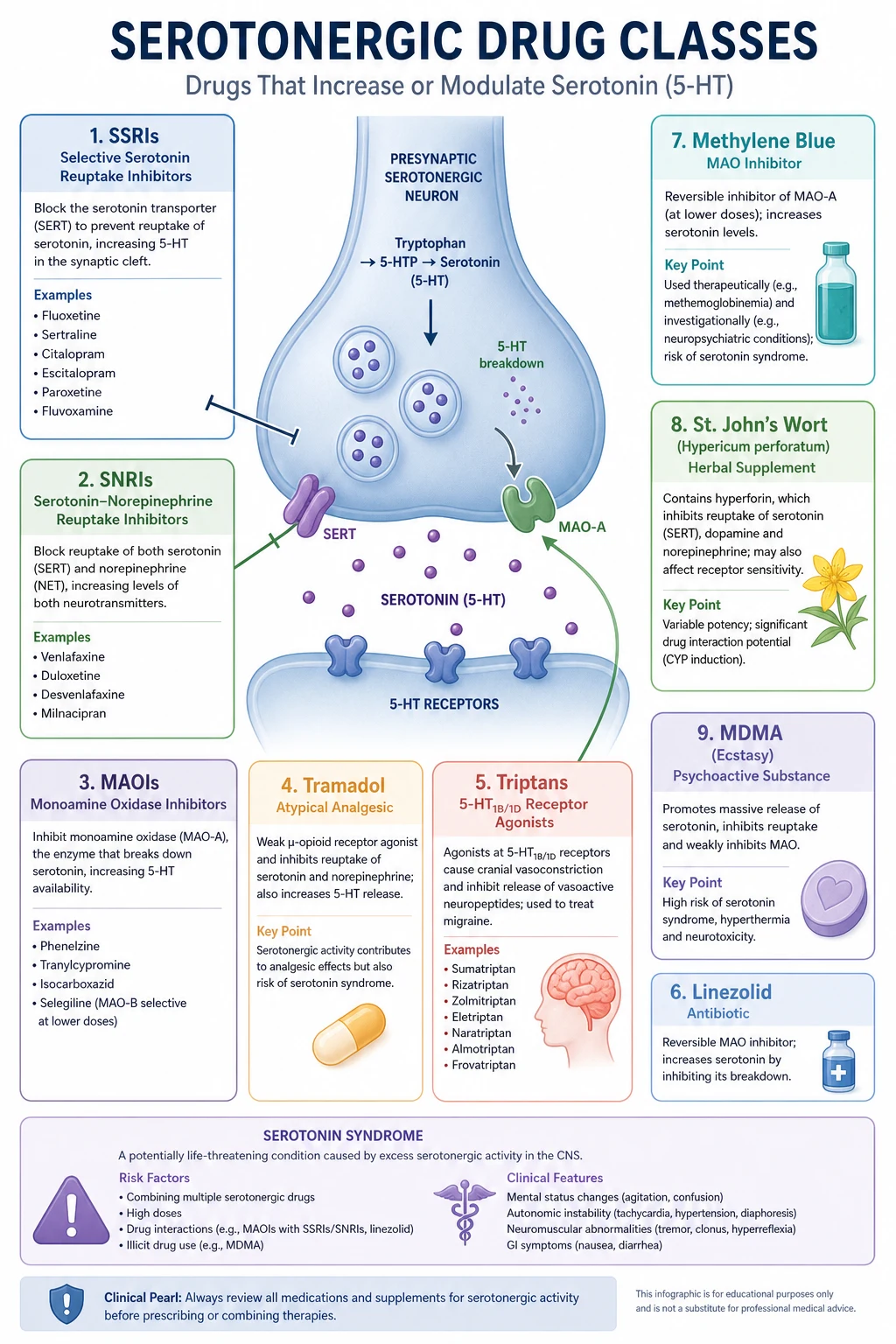
Serotonin (5-hydroxytryptamine, 5-HT) is a monoamine neurotransmitter synthesised from tryptophan, stored in presynaptic vesicles by the vesicular monoamine transporter, and released into the synapse. Its synaptic action is terminated largely by reuptake via the serotonin transporter (SERT) and by metabolism by monoamine oxidase A (MAO-A) to 5-hydroxyindoleacetic acid (5-HIAA). About 90 per cent of body serotonin is in the enterochromaffin cells of the gut; central serotonin is synthesised in the raphe nuclei of the brainstem [1].
Serotonin syndrome results from excessive 5-HT activity at synaptic receptors, most importantly the 5-HT2A receptor (responsible for neuromuscular hyperactivity — clonus, hyperreflexia, rigidity) and to a lesser extent the 5-HT1A receptor (behavioural activation). Excess serotonin can accumulate by four mechanisms: [1]
- Increased synthesis — not a drug target clinically.
- Increased release — amphetamines, MDMA, cocaine, fenfluramine release serotonin from vesicles.
- Decreased reuptake — SSRIs (sertraline, fluoxetine, citalopram, escitalopram, paroxetine), SNRIs (venlafaxine, duloxetine), TCAs (clomipramine, imipramine), tramadol, meperidine (pethidine), dextromethorphan, cocaine all block SERT.
- Decreased metabolism — MAOIs (phenelzine, tranylcypromine, moclobemide), linezolid, methylene blue, procarbazine inhibit MAO-A [1][8].
The critical pharmacological principle: combining drugs from two different mechanisms (e.g., an SSRI that blocks reuptake plus an MAOI that blocks metabolism) produces a multiplicative, not additive, rise in synaptic serotonin. This is why the SSRI-plus-MAOI combination is the classic lethal trigger and why the washout intervals exist: two weeks between an SSRI and an MAOI (five weeks for fluoxetine because of its long-active metabolite norfluoxetine) [1].
The serotonergic drug list — what to look for on the medication chart
The diagnosis cannot be made without identifying a serotonergic agent. Learn these by mechanism so you can predict interactions, not just memorise a list. [1]
| Mechanism | Drugs |
|---|---|
| Serotonin reuptake inhibition | SSRIs (sertraline, fluoxetine, citalopram, escitalopram, paroxetine, fluvoxamine, vortioxetine), SNRIs (venlafaxine, duloxetine, desvenlafaxine), TCAs (clomipramine, imipramine), tramadol, pethidine (meperidine), dextromethorphan, tapentadol, cocaine, St John's wort |
| MAO-A inhibition | MAOIs (phenelzine, tranylcypromine, isocarboxazid), reversible MAOIs (moclobemide), linezolid, methylene blue, procarbazine |
| Serotonin release | MDMA (ecstasy), amphetamines, fenfluramine, mCPP |
| 5-HT receptor agonism | Triptans (sumatriptan, zolmitriptan), buspirone (5-HT1A) |
| Other or uncertain | Ondansetron, metoclopramide, carbamazepine, valproate (rare), lithium (enhances serotonergic effect) |
Linezolid deserves special attention because it is a weak, reversible MAOI and is commonly prescribed on medical wards. A 2023 meta-analysis found the absolute risk of serotonin toxicity with linezolid plus a serotonergic agent is low (pooled prevalence around 0.013 per cent, odds ratio 1.78), but the risk rises steeply when multiple serotonergic agents are combined (odds ratio 5.18) [11]. Methylene blue is a potent MAOI; its use in parathyroid surgery or diagnostic procedures in a patient on an SSRI is a well-described trigger [8]. The exam trap: the patient on sertraline who develops agitation and clonus two days after linezolid is started for an MRSA infection.
Clinical presentation — the clinical triad and the Hunter criteria
Serotonin syndrome produces a clinical triad: neuromuscular hyperactivity, autonomic instability, and altered mental status. The severity ranges from a mild, easily missed tremor and diarrhoea through to life-threatening hyperthermia, seizures and death [1].
1. Neuromuscular hyperactivity (the most discriminating domain):
- Clonus — the hallmark. It may be spontaneous (present at rest), inducible (provoked by ankle dorsiflexion or patellar reflex), or ocular (rhythmic vertical or horizontal eye movements on extreme lateral gaze). Inducible clonus is the single most useful bedside sign.
- Hyperreflexia — more pronounced in the lower limbs than the upper limbs (this is the opposite of NMS and reflects the spinal cord serotonergic pathways). Patellar hyperreflexia with sustained clonus is classic.
- Myoclonus — sudden, shock-like muscle jerks, often multifocal.
- Rigidity — more prominent in the lower limbs; in severe cases generalised rigidity can mimic NMS, but the hyperreflexia and clonus persist.
- Tremor — a low-amplitude, high-frequency tremor in the lower limbs, especially elicited in the lower extremity [2].
2. Autonomic instability:
- Hyperthermia (usually mild, 38 to 40 degrees; above 41 suggests severe disease)
- Tachycardia, hypertension (early), later hypotension
- Mydriasis (dilated pupils), diaphoresis, flushing
- Diarrhoea, abdominal cramps (enteric serotonin)
- Tachypnoea [1]
3. Altered mental status:
- Agitation, restlessness, pressure of speech
- Confusion, delirium
- In severe cases, seizures and coma [1]
The Hunter Serotonin Toxicity Criteria are the validated diagnostic tool, derived from 2,222 admissions to the Hunter Area Toxicology Service in Australia with sensitivity 84 per cent and specificity 97 per cent — superior to the older Sternbach criteria [2][10]. Diagnosis requires exposure to a serotonergic agent in the past five weeks, plus any one of the following:
| Hunter criterion |
|---|
| Spontaneous clonus |
| Inducible clonus plus agitation or diaphoresis |
| Ocular clonus plus agitation or diaphoresis |
| Tremor plus hyperreflexia |
| Hypertonia plus temperature above 38 degrees plus ocular or inducible clonus |
The exam trap: the Hunter criteria are not a score — any single criterion is positive. The classic Sternbach triad (mental status change, autonomic instability, neuromuscular changes) is now considered less specific because it over-diagnoses and misses the clonus that is the true discriminator [2].
Severity grading and what it means for management
Boyer and Shannon frame severity by the dominant clinical feature, which directly determines management intensity [1]:
- Mild — mild autonomic signs, tremor, myoclonus, hyperreflexia; afebrile or low-grade fever; patient talkative and agitated. Management: stop the agent, benzodiazepine, observe.
- Moderate — hyperthermia (above 40 degrees), tachycardia, hypertension, mydriasis, ocular or inducible clonus, agitation, pressured speech, autonomic instability. Management: add cyproheptadine, active cooling, consider ICU.
- Severe — severe hyperthermia (above 41 degrees, reflecting a life-threatening degree of muscle activity), rigidity causing the fever (the hyperthermia is driven by muscle tone), seizures, delirium, DIC, rhabdomyolysis, renal failure, arrhythmias. This is a medical emergency requiring intubation, paralysis with a non-depolarising neuromuscular blocker, and ICU admission. Mortality is significant if untreated. [1]
The key teaching point: in severe serotonin syndrome the hyperthermia is driven by sustained muscle activity, so it will not respond to antipyretics — you must paralyse the patient [1].
Neuroleptic Malignant Syndrome
Pathophysiology — why dopamine blockade does what it does
NMS results from sudden and profound reduction in central dopaminergic neurotransmission, most often through D2 receptor blockade by antipsychotic drugs, or through abrupt withdrawal of dopaminergic therapy in a patient with Parkinson disease [3][4]. The dopamine pathways affected are:
- Nigrostriatal (motor) — produces the lead-pipe rigidity, tremor, and (unlike serotonin syndrome) bradyreflexia.
- Mesolimbic and mesocortical — produces the altered mental status (mutism, catatonia, delirium).
- Tuberoinfundibular and hypothalamic — produces the autonomic instability and hyperthermia (hypothalamic dopamine blockade disrupts thermoregulation) [3].
The rigidity generates sustained muscle contraction, which drives the marked creatine kinase elevation and rhabdomyolysis that distinguishes NMS biochemically from most serotonin syndrome cases. Rhabdomyolysis in turn causes acute kidney injury, and the catabolic state produces leukocytosis and transaminitis. [1]
NMS triggers — the medication history
NMS is caused by dopamine D2 receptor antagonists or withdrawal of dopamine agonists [6][9]:
| Mechanism | Drugs |
|---|---|
| Typical (first-generation) antipsychotics | Haloperidol, chlorpromazine, fluphenazine (especially depot), trifluoperazine |
| Atypical (second-generation) antipsychotics | Risperidone, olanzapine, quetiapine, clozapine, aripiprazole, ziprasidone, paliperidone, amisulpride |
| Antiemetics (D2 antagonists) | Metoclopramide, prochlorperazine, promethazine, droperidol |
| Dopamine agonist withdrawal (Parkinson disease) | Abrupt cessation of levodopa, bromocriptine, amantadine — the "withdrawal-emergent NMS" or parkinsonism-hyperpyrexia syndrome |
A critical exam point: atypical antipsychotics can and do cause NMS, though the risk is lower than with typical agents [9]. Clozapine-induced NMS is notable for often lacking the classic lead-pipe rigidity because clozapine has anticholinergic and 5-HT activity that can mask the extrapyramidal features. The withdrawal of levodopa or a dopamine agonist in a patient with Parkinson disease produces a clinically identical syndrome (parkinsonism-hyperpyrexia syndrome) and is treated by reinstating the dopamine agonist [3].
NMS occurs in roughly 0.02 to 0.3 per cent of patients on antipsychotics, typically within the first one to four weeks of starting treatment or after a dose increase. Risk factors include rapid dose escalation, high-potency typical agents, dehydration, catatonia, agitation, iron deficiency, and underlying brain injury [3][4].
Clinical presentation of NMS
NMS is a clinical diagnosis. The international Delphi consensus (Gurrera 2011) defines it by recent dopamine exposure (or withdrawal), hyperthermia, rigidity, and mental status alteration, with associated autonomic and laboratory features [4].
The classical presentation evolves over hours to days: [1]
- Hyperthermia — typically above 38.5 degrees, often above 40; a core feature.
- Generalised rigidity — lead-pipe rigidity (uniform, velocity-independent resistance throughout the range of movement), greater in the upper limbs than the lower (the mirror image of serotonin syndrome). May be accompanied by tremor ("cogwheeling") and bradyreflexia.
- Altered mental status — mutism, catatonia, obtundation, agitation, delirium. The patient is often mute and staring — quite different from the agitated, pressure-of-speech patient with serotonin syndrome.
- Autonomic instability — tachycardia, labile blood pressure (hypertension and hypotension), diaphoresis, sialorrhoea (especially with clozapine), incontinence, tachypnoea.
- Laboratory features — elevated creatine kinase (often into the thousands), leukocytosis, transaminitis, hypocalcaemia, hypomagnesaemia, low serum iron; later AKI from rhabdomyolysis, and DIC in severe cases [3][6].
Differential Diagnosis — what else makes a patient hot, rigid and confused
The febrile, rigid, agitated patient has a wide differential. The diagnosis is made by combining the medication history (the single most powerful discriminator), the onset tempo, and the neuromuscular examination [5][7].
| Condition | Key distinguishing features |
|---|---|
| Serotonin syndrome | Hours of onset, serotonergic drug, clonus, hyperreflexia (lower greater than upper), mydriasis, diarrhoea |
| Neuroleptic malignant syndrome | Days of onset, antipsychotic or dopamine-agonist withdrawal, lead-pipe rigidity (upper greater than lower), bradyreflexia, markedly raised CK |
| Malignant hyperthermia | Anaesthesia exposure, masseter rigidity, rapid CK rise, family history of anaesthetic death, treated with dantrolene |
| Sepsis / CNS infection | Infection source, no clonus or lead-pipe rigidity, positive cultures, responds to antibiotics; always exclude — these may coexist |
| Anticholinergic toxicity | Dry skin (not diaphoretic), urinary retention, hyperthermia, mydriasis, confusion; "mad as a hatter, blind, red as a beet, hot as a hare, dry as a bone" |
| Heat stroke | Exertional or environmental exposure; dry or sweaty, no rigidity, no drug trigger |
| Malignant catatonia / lethal catatonia | Stereotypies, posturing, negativism, no recent antipsychotic; treated with benzodiazepines and ECT; overlaps biologically with NMS |
| Thyroid storm | Hyperthyroid signs (goitre, eye signs), atrial fibrillation, high T3/T4, suppressed TSH |
| Status epilepticus (non-convulsive) | Subtle motor activity, EEG diagnosis |
| Symptathomimetic toxicity (cocaine, amphetamine) | Agitation, hypertension, tachycardia; can mimic mild serotonin syndrome; usually lacks clonus |
| Alcohol or benzodiazepine withdrawal | Tremor, autonomic signs, seizure risk, history; no rigidity or clonus |
The two conditions most commonly confused are serotonin syndrome and NMS — the comparison above resolves this. Anticholinergic toxicity is the most commonly missed mimic: it has dry skin and urinary retention (serotonin syndrome has diaphoresis and diarrhoea), and it has no clonus [8]. Sepsis must always be excluded and may coexist — do not let a serotonergic drug history stop you from culturing a febrile patient [7].
Investigations
There is no confirmatory blood test for either syndrome. Diagnosis is clinical, and investigations serve to exclude mimics and assess severity and complications [1][3].
Mandatory initial panel:
- Full blood count — leukocytosis common in both; platelets for DIC screen
- Urea and electrolytes, creatinine — baseline for AKI
- Creatine kinase — the key biomarker. Markedly elevated in NMS and malignant hyperthermia; mild or normal in mild serotonin syndrome, but rises in severe cases with rigidity
- Liver function tests — transaminitis in both; more pronounced in NMS
- Coagulation (INR, APTT, fibrinogen, D-dimer) — to screen for DIC
- Lactate — elevated with severe rigidity and tissue hypoperfusion
- Glucose, calcium, magnesium — correct derangements
- Blood cultures, urine culture, chest X-ray — exclude sepsis, which may coexist
- Troponin and ECG — assess for arrhythmia and myocardial injury
- Arterial or venous blood gas — acidosis, hypoxia, hypercapnia if airway threatened
- Urine drug screen and serum paracetamol/salicylate levels — exclude toxidromes and co-ingestions
- TSH, free T4 — exclude thyroid storm
- CT brain and, if indicated, lumbar puncture — exclude CNS infection or structural cause, especially in the febrile confused patient
- Iron studies — low serum iron is associated with NMS and may predict severity [4]
Not useful: serotonin levels are not measurable or interpretable clinically and should not be ordered. Cyproheptadine response is not a diagnostic test. [1]
Management of Serotonin Syndrome
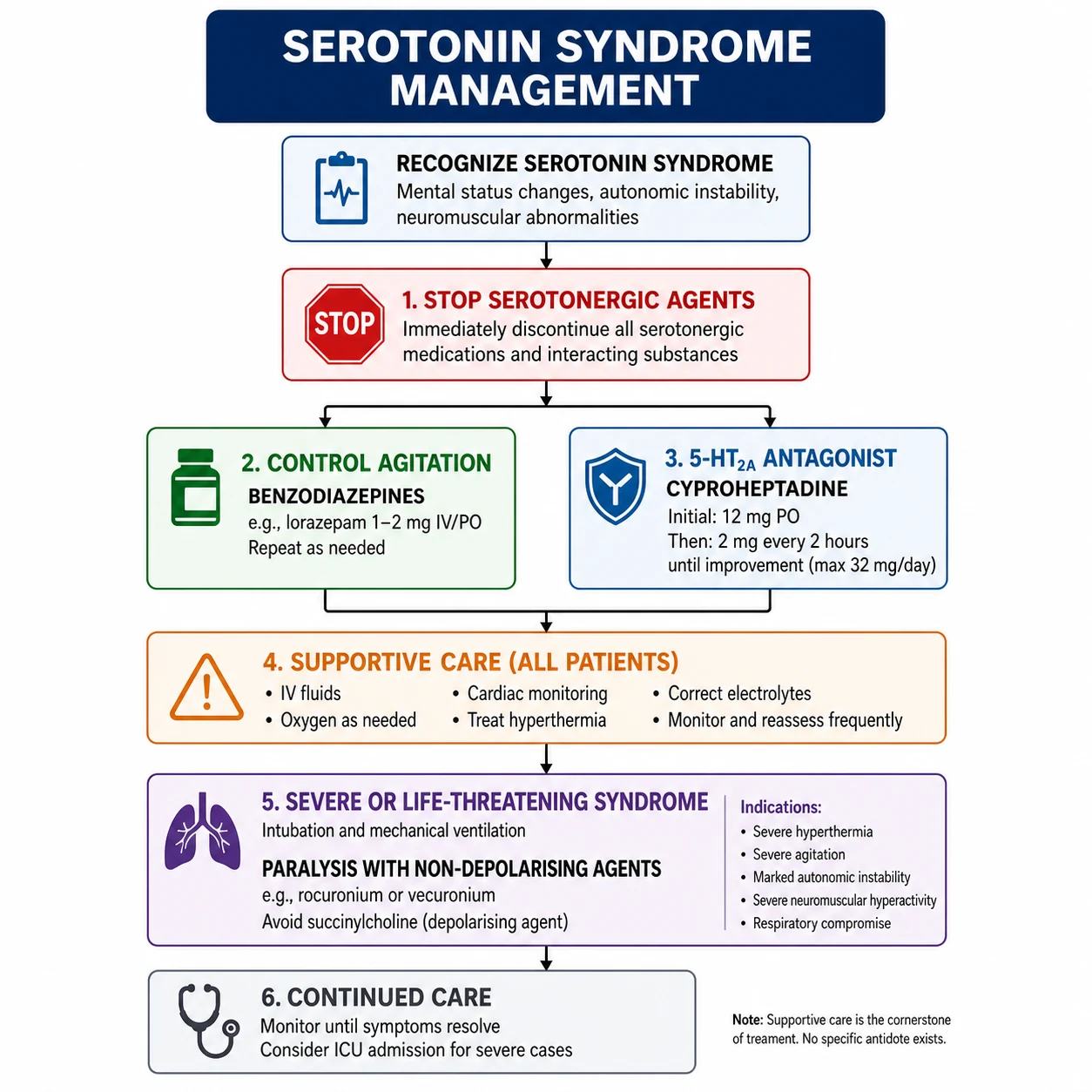
The management of serotonin syndrome is built on four pillars: remove the trigger, supportive care, control agitation and neuromuscular activity, and treat severe disease with cyproheptadine and paralysis [1][8].
Step 1 — Stop all serotonergic agents
Discontinue every serotonergic drug immediately — antidepressants, opioids (especially tramadol, pethidine, fentanyl), antiemetics, triptans, cough suppressants (dextromethorphan), herbal agents (St John's wort), linezolid, methylene blue. Review the entire medication list, the over-the-counter list, and recreational drugs. This alone resolves most mild cases within 24 to 72 hours. [1]
Step 2 — Supportive care
- ABC: secure the airway; intubate early if the airway is threatened or for severe disease.
- Intravenous fluids to maintain urine output and protect the kidneys from rhabdomyolysis.
- Active cooling — remove clothing, use evaporative cooling, fans, ice packs to groins and axillae; in severe cases consider intravascular cooling devices. Antipyretics (paracetamol) do not work — the hyperthermia is muscle-generated, not prostaglandin-mediated.
- Cardiac monitoring — arrhythmias from autonomic instability and electrolyte derangement.
- Correct electrolyte abnormalities, especially potassium, calcium, magnesium.
- Treat rhabdomyolysis with aggressive isotonic crystalloid (target urine output 1 to 2 mL/kg/hour); consider sodium bicarbonate if severe acidosis or myoglobinuria. [1]
Step 3 — Benzodiazepines for agitation and neuromuscular control
Benzodiazepines are the first-line pharmacological agent in serotonin syndrome [1]. They reduce agitation, lower muscle tone (and therefore heat generation), and control myoclonus. They work by enhancing GABAergic inhibition, which indirectly reduces serotonergic tone.
- Diazepam 5 to 10 mg intravenously, repeated every 5 to 10 minutes as required, titrated to mild sedation and control of agitation.
- Lorazepam 1 to 2 mg intravenously is an alternative.
- In severe agitation, a continuous midazolam infusion may be required. [1]
The critical teaching point: benzodiazepines are not just sedatives here — they reduce the muscle-generated heat that is driving the hyperthermia. Control the agitation and you control the temperature [1].
Step 4 — Cyproheptadine for moderate to severe disease
Cyproheptadine is a 5-HT2A receptor antagonist and is the specific antidote for moderate-to-severe serotonin syndrome [1][8]. It also has antihistamine (H1) and anticholinergic activity.
- Initial dose 12 mg orally, then 2 mg every two hours until clinical response (maximum 32 mg in 24 hours; maintenance 8 mg every six hours).
- The usual effective total dose is 12 to 32 mg in 24 hours.
- Limitations: it is only available as an oral tablet (no intravenous formulation), so it cannot be given to a patient who is intubated and paralysed or vomiting; absorption in the critically ill is unpredictable; evidence is limited to case series and there are no randomised controlled trials. It is therefore adjunctive, not a substitute for supportive care and paralysis in severe disease [8].
Step 5 — Severe disease: intubation and paralysis
In severe serotonin syndrome with uncontrolled hyperthermia (above 41 degrees), rigidity, seizures or loss of airway reflexes, the priority is endotracheal intubation and neuromuscular paralysis [1]. Paralysis stops the muscle-generated heat, allowing the temperature to fall rapidly.
- Use a non-depolarising neuromuscular blocker (rocuronium 1.0 to 1.2 mg/kg for intubation, vecuronium or cisatracurium infusion for maintenance). Avoid succinylcholine — there is a theoretical risk of hyperkalaemia and of unmasking malignant hyperthermia, and it causes potassium release from damaged muscle in rhabdomyolysis.
- Sedate and analgesiate adequately (propofol or midazolam plus fentanyl infusion).
- Provide mechanical ventilation with lung-protective settings.
- Continue active cooling and cyproheptadine via nasogastric tube. [1]
What NOT to do
- Do not give antipyretics — they do not work in muscle-generated hyperthermia and may delay recognition that the patient is not cooling [1].
- Do not give propranolol — a common exam trap. Propranolol was historically recommended but is harmful: its 5-HT1A antagonism can prolong toxicity, and its cardiovascular effects can worsen hypotension. Avoid it.
- Do not give antipsychotics (haloperidol, olanzapine) — they are ineffective and can worsen the picture by adding dopamine blockade (risking NMS or prolonging confusion) [8].
- Do not restart serotonergic agents prematurely — wait until symptoms fully resolve, then re-challenge cautiously with a single agent at low dose.
Management of Neuroleptic Malignant Syndrome
NMS management mirrors the supportive framework but adds specific pharmacotherapy directed at the dopamine deficit and the muscle rigidity [3][6].
Step 1 — Stop the offending antipsychotic
Discontinue the antipsychotic or antiemetic immediately. For withdrawal-emergent NMS (parkinsonism-hyperpyrexia syndrome), the action is the opposite: reinstate the dopamine agonist (levodopa, bromocriptine, or amantadine) [3].
Step 2 — Supportive care
The same aggressive supportive care as serotonin syndrome: airway protection, intravenous fluids for rhabdomyolysis, active cooling, correction of electrolytes, DVT prophylaxis (immobility), and monitoring for AKI, DIC and arrhythmia. Rhabdomyolysis management is more prominent in NMS because the CK is typically much higher. [1]
Step 3 — Specific pharmacotherapy (severe or refractory disease)
Two classes of agent are used in moderate-to-severe NMS, with evidence from case series and clinical experience (no randomised trials exist) [3][6]:
Dantrolene — a direct-acting skeletal muscle relaxant that blocks ryanodine receptor-mediated calcium release from the sarcoplasmic reticulum, uncoupling excitation-contraction and reducing the rigidity-driven heat and rhabdomyolysis.
- Dose: 1 mg/kg intravenously, repeated every 5 minutes to a maximum of 10 mg/kg, then 1 mg/kg every 6 hours until symptoms resolve.
- Used in severe NMS with marked rigidity and hyperthermia. It is also the definitive treatment for malignant hyperthermia.
- Caution: hepatotoxicity with cumulative dosing; monitor liver function. [1]
Bromocriptine — a dopamine D2 receptor agonist that directly reverses the dopamine blockade.
- Dose: 2.5 mg orally (or via nasogastric tube) every 8 hours, titrated up to 5 mg every 6 hours as tolerated.
- Onset over hours to days; continue for 7 to 10 days after resolution then taper over a week to prevent recurrence.
- Caution: hypotension, vomiting, psychosis; contraindicated in pregnancy. [1]
Amantadine — an alternative dopamine agonist (also NMDA antagonist and enhances dopamine release) for patients who cannot tolerate bromocriptine.
- Dose: 100 mg orally twice daily. [1]
The combination of dantrolene plus a dopamine agonist is used in severe NMS. Benzodiazepines (lorazepam) are adjunctive for catatonic features and agitation; in malignant catatonia (a related syndrome), electroconvulsive therapy (ECT) may be life-saving [3].
When to restart antipsychotic therapy
After recovery (typically 2 weeks symptom-free), antipsychotic therapy can usually be reintroduced cautiously — switching to a lower-potency or atypical agent at a low dose, with gradual titration. The risk of recurrence is roughly 10 to 30 per cent [6][9]. The underlying psychiatric illness must not be neglected: weigh the risk of NMS recurrence against the risk of uncontrolled psychosis.
Cyproheptadine, Dantrolene and Bromocriptine — the pharmacology you must know
| Drug | Mechanism | Indication | Dose | Key cautions |
|---|---|---|---|---|
| Cyproheptadine | 5-HT2A antagonist (also H1 antihistamine, anticholinergic) | Serotonin syndrome (moderate to severe) | 12 mg PO load, then 2 mg every 2 hours to clinical response (max 32 mg/24 h), then 8 mg every 6 hours | Oral only; anticholinergic effects; no RCT evidence |
| Bromocriptine | Dopamine D2 agonist | NMS; parkinsonism-hyperpyrexia syndrome | 2.5 mg PO/NG every 8 hours, titrate to 5 mg every 6 hours | Hypotension, vomiting, psychosis; pregnancy caution |
| Amantadine | Dopamine release enhancer, weak NMDA antagonist | NMS (alternative to bromocriptine) | 100 mg PO twice daily | Confusion, livedo reticularis, oedema |
The exam favourite: cyproheptadine is for serotonin syndrome; dantrolene is for malignant hyperthermia and severe NMS; bromocriptine is for NMS. Do not confuse the antidotes with the syndromes. [1]
Special Situations
Linezolid and methylene blue — the hidden MAOIs
Linezolid is a weak reversible MAO-A inhibitor; methylene blue is a potent MAO-A inhibitor. Both can precipitate serotonin syndrome when combined with SSRIs, SNRIs, tramadol or TCAs [8][11]. The 2023 meta-analysis confirms the absolute risk is low but rises with multiple serotonergic agents [11]. Practical guidance: review the patient's antidepressant list before starting linezolid; if an SSRI cannot be ceased (severe depression), use linezolid only if essential and monitor closely; for methylene blue, consider alternatives (e.g., 1 per cent isosulfan blue for parathyroid localisation) in patients on SSRIs.
Parkinson disease — the dopamine withdrawal syndrome
Abrupt cessation of levodopa, amantadine or a dopamine agonist in a patient with Parkinson disease produces a syndrome clinically identical to NMS — the parkinsonism-hyperpyrexia syndrome (also called neuroleptic-like malignant syndrome) [3]. The treatment is to reinstate the dopaminergic therapy, not to add bromocriptine (which may be insufficient). This is a high-yield exam point and a common clinical error — a patient admitted for surgery whose Parkinson medications are withheld perioperatively.
Antidepressant therapy after serotonin syndrome
After recovery, serotonergic antidepressants can often be re-introduced cautiously — usually a single agent at low dose with careful monitoring, avoiding combinations and MAOIs. The underlying mood disorder must be treated; the risk of recurrence with a single SSRI at standard dose is low [1].
The perioperative patient
Patients on SSRIs undergoing procedures using methylene blue, or patients on antipsychotics having surgery, are at risk. Review the medication list at preadmission. The patient with Parkinson disease should have their dopaminergic therapy continued through the perioperative period wherever possible [3].
High-Yield Exam Discriminators
- Onset is the master discriminator — hours favours serotonin syndrome; days to weeks favours NMS [5].
- Clonus and hyperreflexia are specific for serotonin syndrome — inducible or ocular clonus is the Hunter criterion. NMS has bradyreflexia, never clonus.
- Lead-pipe rigidity is specific for NMS — velocity-independent resistance; the rigidity of serotonin syndrome is more tremulous and clonic.
- Rigidity distribution — lower greater than upper in serotonin syndrome; upper greater than lower in NMS.
- Creatine kinase — markedly elevated (into the thousands) in NMS; mild or normal in mild serotonin syndrome.
- The drug history is the diagnosis — a serotonergic agent plus clonus equals serotonin syndrome; an antipsychotic or dopamine withdrawal plus lead-pipe rigidity equals NMS [5].
- Mydriasis and diarrhoea suggest serotonin syndrome (cholinergic and enteric serotonin effects); sialorrhoea and incontinence suggest NMS or anticholinergic toxicity (dry).
- Antipyretics do not work in either syndrome — the hyperthermia is muscle-generated [1].
- Benzodiazepines are first-line in serotonin syndrome; cyproheptadine is the antidote; paralyse the severe case.
- Dantrolene is the antidote for malignant hyperthermia and is used in severe NMS; bromocriptine is the dopamine agonist for NMS.
Exam Traps and Pitfalls
- The most common DWE error is diagnosing NMS in a patient with hours of onset and clonus — that is serotonin syndrome. The onset tempo and the presence of clonus settle it [2][5].
- The propranolol trap: do not give propranolol in serotonin syndrome — it prolongs toxicity and worsens hypotension [1].
- The antipyretic trap: paracetamol and NSAIDs do not reduce muscle-generated hyperthermia; active cooling and paralysis do [1].
- The antipsychotic trap: do not treat agitation in serotonin syndrome with haloperidol or olanzapine — they add dopamine blockade and can precipitate or worsen NMS. Use benzodiazepines [8].
- The succinylcholine trap: in severe disease requiring paralysis, use a non-depolarising agent (rocuronium, vecuronium) to avoid hyperkalaemia and theoretical malignant hyperthermia unmasking [1].
- The atypical-antipsychotic trap: atypicals (olanzapine, risperidone, clozapine, aripiprazole) DO cause NMS — the risk is lower but not zero [9].
- The linezolid trap: a patient on an SSRI who develops agitation and clonus days after linezolid is started has serotonin syndrome from the MAOI effect of linezolid [11].
- The withdrawal trap: abrupt cessation of Parkinson medications causes NMS-like syndrome — treat by reinstating the dopamine agonist, not by adding bromocriptine alone [3].
- The washout trap: two weeks between an SSRI and an MAOI; five weeks for fluoxetine (long-active norfluoxetine) [1].
- The mimic trap: anticholinergic toxicity has dry skin and urinary retention; serotonin syndrome has diaphoresis and diarrhoea. Do not confuse them [8].
Regional Guideline Deltas
| Aspect | ANZ | UK | US |
|---|---|---|---|
| Primary toxicology resource | NSW Poisons Information Centre (13 11 26); ANZ toxicology consensus | Toxbase / National Poisons Information Service | AAPCC / local poison control |
| Serotonin syndrome criteria | Hunter criteria (Australian origin) widely used | Hunter criteria; NICE clinical knowledge summaries | Hunter criteria; Boyer and Shannon framework |
| Cyproheptadine availability | Oral tablet only | Oral tablet only | Oral tablet only |
| Malignant hyperthermia hotline | ANZ MHAUS equivalent; state anaesthetic retrieval | UK MHA hotline | MHAUS 24-hour hotline |
The Hunter criteria are an Australian contribution (Isbister and colleagues, Newcastle) and are the internationally accepted diagnostic standard — this is a point of pride and a likely exam reference for ANZ candidates [2].
Communication and Shared Decision-Making
In the acute phase, communication is with the family and the psychiatric team. The message: "Your relative has developed a serious reaction to their medication. It is treatable. We have stopped the responsible drug and started specific treatment. The next 24 to 48 hours are critical." Be honest about mortality — untreated severe serotonin syndrome or NMS carries a mortality of 5 to 20 per cent, but with prompt recognition and management the prognosis is good [3].
The longitudinal issue is psychiatric continuity: a patient who has had NMS or serotonin syndrome still needs their underlying schizophrenia, depression or Parkinson disease treated. Engage the psychiatric and neurology teams early to plan a safe re-challenge or alternative agent. Document the reaction in the medication record and warn the patient and family about the offending drug for the future. For malignant hyperthermia, refer the patient and first-degree relatives for RYR1 genetic testing and issue a MedicAlert bracelet [3].
Summary: the hyperthermia syndrome consultation in one paragraph
In the hot, rigid, agitated patient, ask three questions: what drug did they take, how fast did it come on, and what does the neuromuscular exam show. Serotonergic drug plus hours of onset plus clonus and lower-limb hyperreflexia is serotonin syndrome — stop the agent, give benzodiazepines, add cyproheptadine, and paralyse the severe case with a non-depolarising blocker. Antipsychotic or dopamine withdrawal plus days of onset plus lead-pipe rigidity and upper-limb predominance is neuroleptic malignant syndrome — stop the antipsychotic (or reinstate the dopamine agonist), give supportive care, and add dantrolene and bromocriptine for severe disease. Volatile anaesthetic or succinylcholine with masseter rigidity is malignant hyperthermia — stop triggers, give dantrolene immediately. In all three, antipyretics do not work, active cooling and airway control are essential, and sepsis must be excluded. Recognise the syndrome at the bedside from the drug history and the reflexes — the bloods will not make the diagnosis for you. [1]
References
- [1]Boyer EW, Shannon M The serotonin syndrome N Engl J Med, 2005.PMID 15784664
- [2]Dunkley EJC, Isbister GK, Sibbritt D, Dawson AH, Whyte IM The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity QJM, 2003.PMID 12925718
- [3]Berman BD Neuroleptic malignant syndrome: a review for neurohospitalists Neurohospitalist, 2011.PMID 23983836
- [4]Gurrera RJ, Caroff SN, Cohen A, et al. An international consensus study of neuroleptic malignant syndrome diagnostic criteria using the Delphi method J Clin Psychiatry, 2011.PMID 21733489
- [5]Perry PJ, Wilborn CA Serotonin syndrome vs neuroleptic malignant syndrome: a contrast of causes, diagnoses, and management Ann Clin Psychiatry, 2012.PMID 22563571
- [6]Pileggi DJ, Cook AM Neuroleptic Malignant Syndrome Ann Pharmacother, 2016.PMID 27423483
- [7]Seitz DP, Gill SS Neuroleptic malignant syndrome complicating antipsychotic treatment of delirium or agitation in medical and surgical patients: case reports and a review of the literature Psychosomatics, 2009.PMID 19213967
- [8]Volpi-Abadie J, Kaye AM, Kaye AD Serotonin syndrome Ochsner J, 2013.PMID 24358002
- [9]Trollor JN, Chen X, Sachdev PS Neuroleptic malignant syndrome associated with atypical antipsychotic drugs CNS Drugs, 2009.PMID 19480467
- [10]Sternbach H The serotonin syndrome Am J Psychiatry, 1991.PMID 2035713
- [11]Wang R, Zhang J, Liu Y, et al. The Association of Serotonin Toxicity with Combination Linezolid-Serotonergic Agent Therapy: A Systematic Review and Meta-Analysis Pharmacy (Basel), 2023.PMID 37987392