Phys · renal
Acute Kidney Injury
Also known as AKI · acute renal failure · ARF · acute tubular necrosis · ATN · acute kidney failure · pre-renal AKI · intrinsic AKI · post-renal AKI · contrast-induced nephropathy · contrast-associated AKI · acute interstitial nephritis · AIN · sepsis-associated AKI · SA-AKI
Consultant-physician-depth guide to acute kidney injury — KDIGO definition and staging, pre-renal/intrinsic/post-renal classification, pathophysiology, investigation strategy, management principles, RRT indications, nephrotoxic agents, drug dosing, and prognosis. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Acute Kidney Injury
The answer first
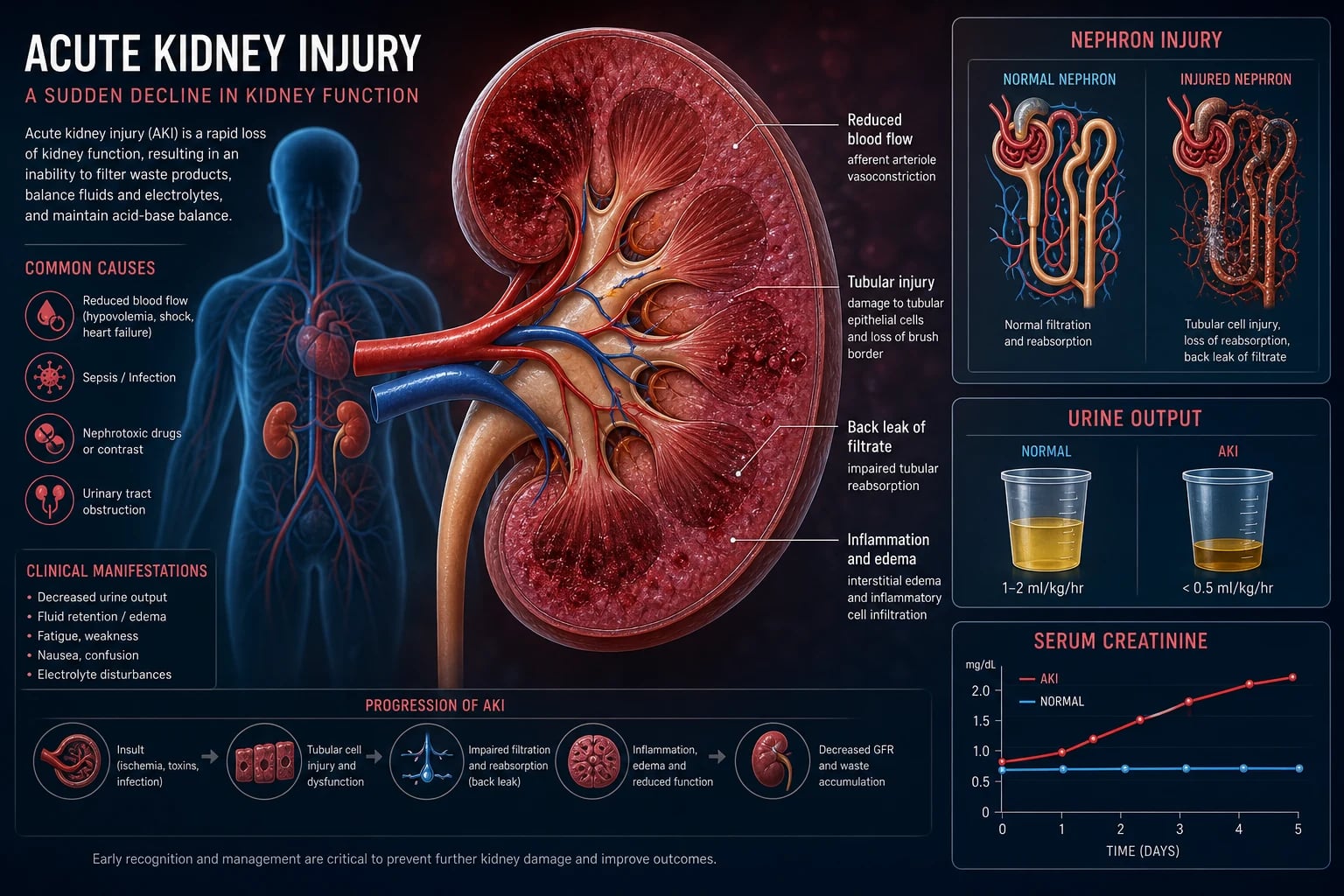
Acute kidney injury (AKI) is an abrupt reduction in kidney function over hours to days, resulting in retention of nitrogenous waste products (rise in creatinine and urea) and impairment of fluid, electrolyte, and acid-base homeostasis. The KDIGO definition requires one of: creatinine rise of ≥26.5 micromol/L (0.3 mg/dL) within 48 hours; creatinine ≥1.5 times baseline within 7 days; or urine output <0.5 mL/kg/h for ≥6 hours [1].
The management mandate is simple to state, hard to execute well: [1]
- Resuscitate and assess volume status first — is this volume-responsive? Give fluid if depleted, remove fluid if overloaded.
- Treat the underlying cause — sepsis, obstruction, nephrotoxin, hypoperfusion.
- Remove all nephrotoxic agents and adjust every renally-cleared drug dose.
- Manage complications — hyperkalaemia, acidosis, fluid overload.
- Initiate renal replacement therapy (RRT) when absolute indications arise (AEIOU). [1]
The single most important exam principle: AKI is a syndrome, not a diagnosis. Always identify and name the cause. [1]
KDIGO definition and staging
Diagnostic criteria (KDIGO 2012)
AKI is diagnosed when any one of the following is present: [1]
| Criterion | Threshold |
|---|---|
| Creatinine rise | ≥26.5 micromol/L (0.3 mg/dL) within 48 hours OR ≥1.5 times baseline within prior 7 days |
| Urine output | <0.5 mL/kg/h for ≥6 hours |
The baseline creatinine is the most important variable. Use a known stable creatinine within the previous 3 months. If none is available, back-calculate using the MDRD equation assuming an eGFR of 75 mL/min/1.73 m². A common clinical error is using a single elevated creatinine from an emergency presentation as the baseline — this under-stages AKI. [1]
Staging (KDIGO severity)
| Stage | Serum creatinine | Urine output |
|---|---|---|
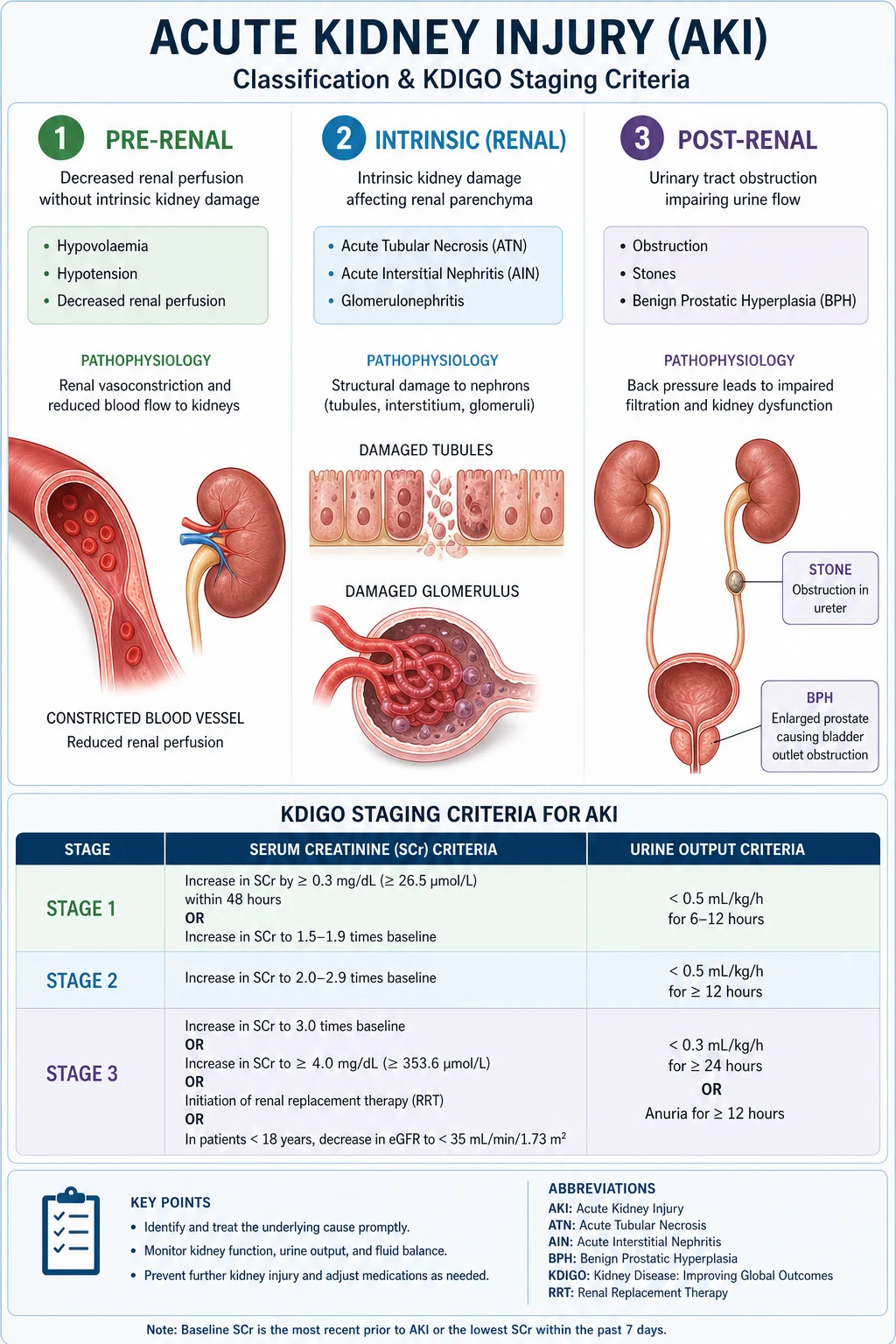
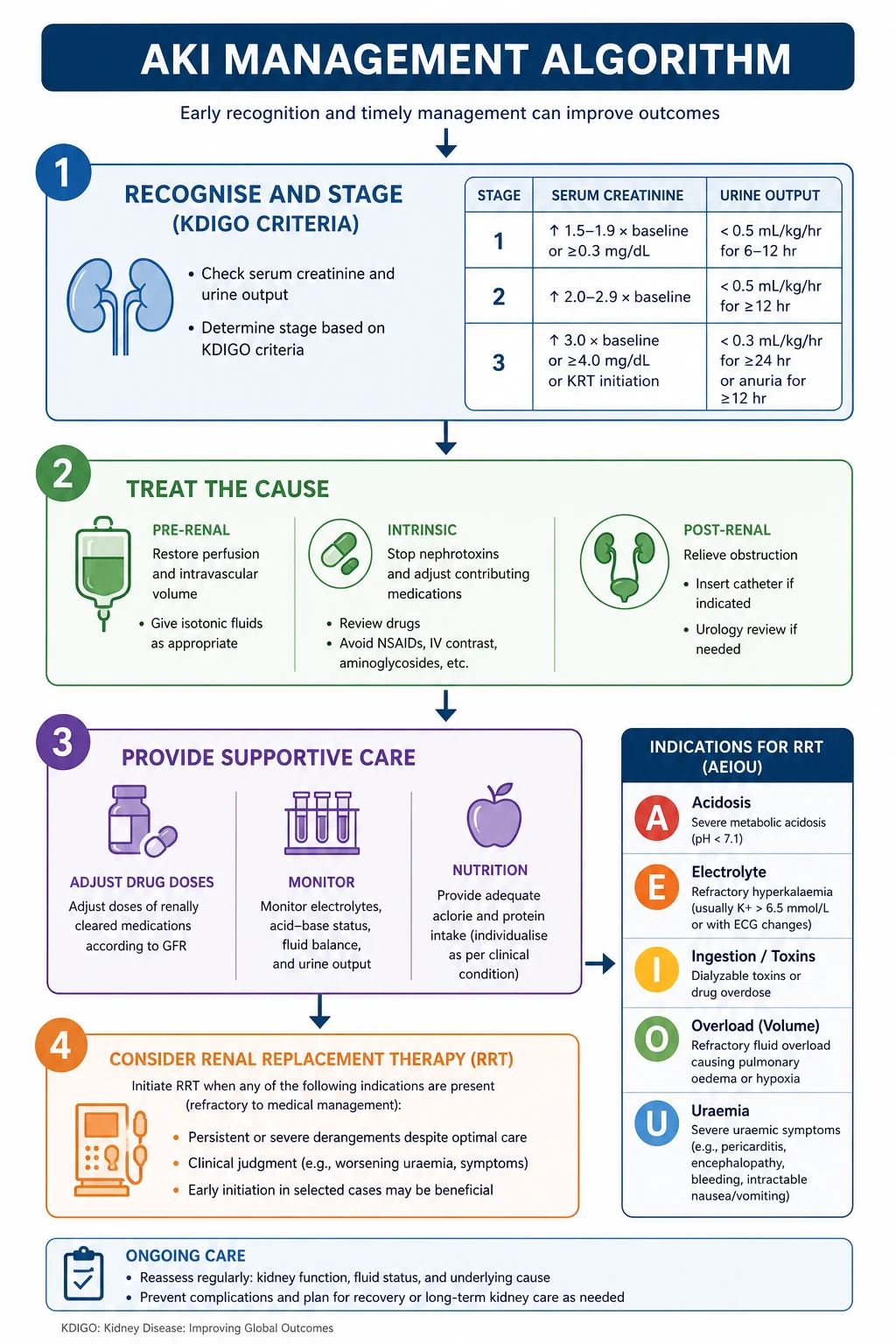
| 1 | 1.5–1.9 times baseline OR ≥26.5 micromol/L increase | <0.5 mL/kg/h for 6–12 hours |
| 2 | 2.0–2.9 times baseline | <0.5 mL/kg/h for ≥12 hours |
| 3 | 3.0 times baseline OR creatinine ≥353.6 micromol/L (4.0 mg/dL) OR initiation of RRT OR in patients <18 years, eGFR <35 mL/min/1.73 m² | <0.3 mL/kg/h for ≥24 hours OR anuria for ≥12 hours |
DWE high-yield: Stage is assigned by the worst creatinine or urine output criterion — you do not need both to meet a stage. A patient with creatinine 2.5 times baseline (stage 2 by creatinine) who is anuric for 12 hours is stage 3 by urine output criteria. [1]
Classification: pre-renal, intrinsic, post-renal
Every AKI must be classified by anatomical site of injury. This framework drives your investigation strategy and immediate management. [1]
Pre-renal (volume-responsive / haemodynamic) — ~60–70% of cases
The kidney is structurally normal. Reduced perfusion causes a functional drop in GFR. The kidney avidly retains sodium and water — if perfusion is restored early, function normalises within 24–48 hours. If ischaemia persists, it progresses to intrinsic AKI (ATN). [1]
Causes:
- Volume depletion: haemorrhage, vomiting, diarrhoea, burns, diuretics, septic vasodilation
- Decreased cardiac output: heart failure, cardiogenic shock
- Systemic vasodilation: sepsis, anaphylaxis, antihypertensives
- Renal vasoconstriction: NSAIDs (afferent arteriole), ACE inhibitors/ARBs (efferent arteriole), hepatorenal syndrome, calcineurin inhibitors
- Abdominal compartment syndrome [1]
Intrinsic (renal) — ~25–30% of cases
Structural injury within the kidney itself. Classified by compartment: [1]
| Compartment | Key causes |
|---|---|
| Vascular | Vasculitis (ANCA, anti-GBM), thrombotic microangiopathy (TTP/HUS), malignant hypertension, renal vein thrombosis, cholesterol emboli |
| Glomerular | Rapidly progressive glomerulonephritis (RPGN), lupus nephritis, post-infectious GN, IgA nephropathy flare |
| Tubular (ATN) | Ischaemia (progressed from untreated pre-renal), nephrotoxins (aminoglycosides, contrast, rhabdomyolysis, myeloma cast), sepsis |
| Interstitial (AIN) | Drug reaction (beta-lactams, PPIs, NSAIDs, sulfonamides), infection (pyelonephritis, leptospirosis), autoimmune (Sjogren, TINU) |
Post-renal (obstructive) — ~5–10% of cases
Obstruction anywhere from the renal pelvis to the urethra. Always exclude this first — it is rapidly reversible if treated. [1]
Causes:
- Prostatic: BPH, prostate cancer (elderly men)
- Ureteric: stones (bilateral or solitary kidney), retroperitoneal fibrosis, external compression (pelvic malignancy)
- Bladder: neurogenic bladder, clot retention, bladder cancer
- Urethral: strictures, phimosis [1]
DCE trap: A single functioning kidney with ureteric obstruction (e.g., a transplant kidney or a patient with prior nephrectomy) presents as obstructive AKI — always ask about prior nephrectomy or transplant when a unilateral obstruction is found. [1]
Pathophysiology
Pre-renal AKI — the prerenal-ATN continuum
When renal perfusion drops, the kidney activates compensatory mechanisms to maintain GFR: afferent arteriolar vasodilation (prostaglandin-mediated) and efferent arteriolar vasoconstriction (angiotensin II-mediated). This is why NSAIDs (blocking prostaglandins) and ACE inhibitors/ARBs (blocking angiotensin II) cause AKI — they remove both compensatory legs. [1]
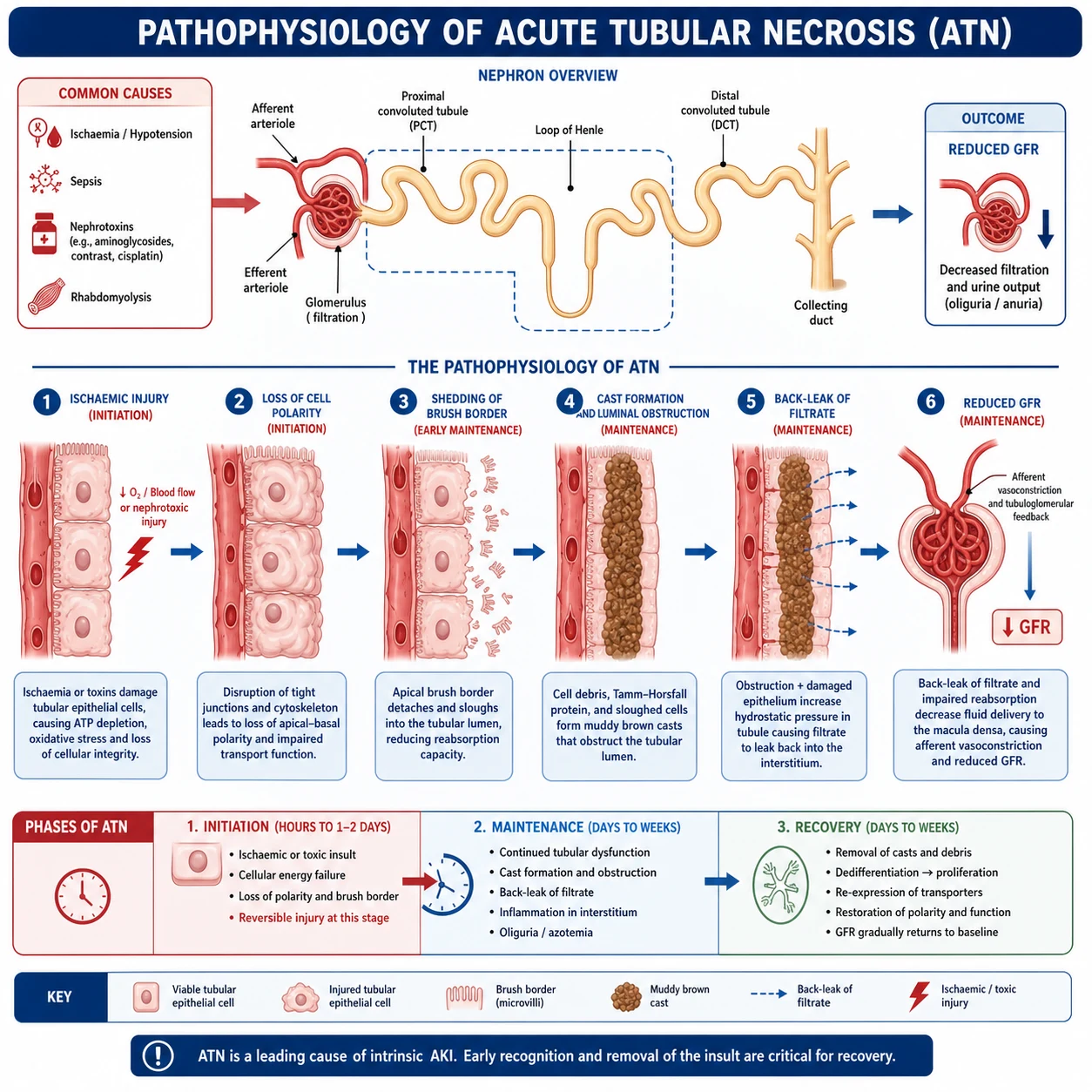
If perfusion is not restored, tubular epithelial cells become ischaemic. These cells have high metabolic demand and are exquisitely sensitive to oxygen deprivation. Ischaemic injury causes ATP depletion, cytoskeletal disruption, shedding of brush border and viable cells into the tubular lumen, and cast formation. This is the transition from pre-renal azotaemia to acute tubular necrosis (ATN). [1]
Once ATN has occurred, the injury is no longer immediately volume-responsive. Recovery requires tubular epithelial regeneration over days to weeks. [1]
Sepsis-associated AKI
Sepsis is the single most common cause of AKI in the ICU. The mechanism is not simple ischaemia — it is a complex syndrome of:
- Microcirculatory dysfunction: heterogeneity of peritubular capillary blood flow, areas of shunting
- Inflammatory injury: cytokines (TNF-alpha, IL-6), endothelial activation, leukocyte adhesion
- Mitochondrial dysfunction: cellular energy failure without overt necrosis
- Tubular cell dedifferentiation and cell cycle arrest: cells enter G2/M arrest as a protective mechanism, but prolonged arrest prevents recovery [1]
This explains why septic AKI can occur without a drop in renal blood flow — the old "acute renal success" concept (intact tubular function despite low GFR) reflects active downregulation of filtration as a protective response. [1]
Nephrotoxic AKI
Different toxins injure different segments: [1]
| Agent | Mechanism | Segment |
|---|---|---|
| Aminoglycosides | Lysosomal accumulation in proximal tubule, phospholipid toxicity | Proximal tubule |
| NSAIDs | Inhibit prostaglandins → afferent arteriolar vasoconstriction | Haemodynamic |
| ACE inhibitors/ARBs | Dilate efferent arteriole → drop in glomerular pressure | Haemodynamic |
| Contrast media | Renal vasoconstriction + direct tubular toxicity + osmotic load | Medullary + proximal tubule |
| Rhabdomyolysis (myoglobin) | Cast formation + direct tubular toxicity + lipid peroxidation | Proximal and distal tubule |
| Tenofovir | Mitochondrial toxicity in proximal tubule | Proximal tubule |
| Calcineurin inhibitors | Afferent arteriolar vasoconstriction | Haemodynamic |
| Myeloma (light chains) | Cast nephropathy — toxic intratubular precipitation | Distal tubule |
Contrast-associated AKI
Formerly "contrast-induced nephropathy" — now called contrast-associated AKI (CA-AKI) because causality is hard to prove. Defined as creatinine rise ≥44.2 micromol/L (0.5 mg/dL) or ≥25% from baseline within 48–72 hours of contrast exposure. The pathophysiology is dual: renal vasoconstriction (reducing medullary oxygen supply) and direct tubular toxicity. The risk is highest in CKD (eGFR <30), diabetes, heart failure, hypovolaemia, and high-contrast volume. [1]
DWE exam trap: The PRESERVE trial (PMID 29130810) definitively showed that neither intravenous sodium bicarbonate nor oral acetylcysteine prevents contrast-associated AKI or improves outcomes [5]. Intravenous isotonic saline is the only proven preventive strategy. If an MCQ offers acetylcysteine or bicarbonate as the answer, it is wrong.
Clinical approach
ABCDE and immediate assessment
AKI frequently coexists with critical illness. Start with the resuscitation ABCDE:
- Airway/Breathing: Is there pulmonary oedema from volume overload? Give oxygen; consider NIV if respiratory failure.
- Circulation: Assess volume status — this is the single most important clinical decision. Check blood pressure, heart rate, JVP, capillary refill, skin turgor, mucous membranes, peripheral warmth, lung bases, and sacral/ankle oedema.
- Disability: Uraemic encephalopathy (asterixis, confusion, seizures) is an indication for RRT.
- Exposure: Look for sources of sepsis (cellulitis, pneumonia, line sites), rashes (vasculitis, AIN), evidence of volume loss. [1]
Volume status assessment — the core skill
This is the single most tested DCE short-case skill. You must classify the patient as hypovolaemic, euvolaemic, or hypervolaemic: [1]
| Finding | Hypovolaemic | Hypervolaemic |
|---|---|---|
| JVP | Low/flat | Elevated |
| Skin turgor | Reduced | Normal |
| Mucous membranes | Dry | Moist |
| Capillary refill | Prolonged (>2 s) | Normal |
| Peripheral oedema | Absent | Present (sacral, ankle) |
| Lung bases | Clear | Crackles (pulmonary oedema) |
| Blood pressure | Low/postural drop | Normal or high |
If hypovolaemic: give balanced crystalloid (Plasma-Lyte, Hartmann's) in aliquots of 250–500 mL, reassessing between boluses. Normal saline in large volumes causes hyperchloraemic metabolic acidosis, which itself worsens renal vasoconstriction. [1]
If hypervolaemic: the patient needs fluid removal, not fluid. Start or increase loop diuretics. If refractory, proceed to RRT. [1]
DCE short-case trap: A patient with septic AKI may be intravascularly volume-depleted but peripherally oedematous (capillary leak). The JVP is your best guide to intravascular volume. Do not withhold fluid because the legs are swollen if the JVP is flat. [1]
Focused history
- Onset and trajectory: When was the last normal creatinine? What changed in the days before the rise?
- Volume loss: vomiting, diarrhoea, bleeding, drains
- Drug history: NSAIDs (including over-the-counter ibuprofen), ACE inhibitors/ARBs, antibiotics, chemotherapy, herbal/alternative medicines, recent contrast
- Infection sources: urinary symptoms, chest, abdomen, line sites
- Comorbidities: CKD, diabetes, heart failure, cirrhosis, myeloma, autoimmune disease
- Systemic symptoms: rash, arthralgia, haemoptysis, sinusitis (vasculitis), dark urine (glomerulonephritis, rhabdomyolysis) [1]
Investigation strategy
Essential for every patient
| Investigation | What it tells you |
|---|---|
| U&E (repeat) | Confirms AKI, tracks trajectory; K+ guides urgency |
| FBC | Anaemia (haemolysis in TMA, CKD), eosinophilia (AIN), leucocytosis (sepsis) |
| CRP | Infection/inflammation marker |
| Venous blood gas | Acid-base status, lactate (sepsis/tissue hypoperfusion) |
| CK | Rhabdomyolysis (check if any muscle pain, immobility, statin use) |
| LFTs | Hepatorenal syndrome, sepsis source |
| Calcium, phosphate | Tumour lysis, rhabdomyolysis |
| Glucose, troponin | Comorbidity assessment |
| Urinalysis | The single most useful bedside test (see below) |
| Urine microscopy | Sediment diagnosis (see below) |
| Bladder scan / catheter | Exclude obstruction immediately |
| ECG | Hyperkalaemia changes (peaked T, wide QRS, sine wave) |
| Medication review | Identify and stop nephrotoxins |
Urinalysis and urine sediment
| Finding | Interpretation |
|---|---|
| Dipstick: blood++ and protein++ | Glomerular disease (GN, vasculitis) — request microscopy urgently |
| Dipstick: leucocytes, nitrites | UTI / pyelonephritis |
| Dipstick: protein only | AIN, myeloma (light chains not detected by standard dipstick) |
| Dipstick: blood + protein on dipstick but no RBCs on microscopy | Myoglobinuria (rhabdomyolysis) or haemoglobinuria |
| Muddy brown granular casts | Acute tubular necrosis (ATN) |
| RBC casts | Glomerulonephritis / vasculitis — nephrology emergency |
| WBC casts | Acute interstitial nephritis, pyelonephritis |
| Eosinophiluria | AIN (historically, now Hansel stain) |
Urine electrolytes
The fractional excretion of sodium (FENa) helps distinguish pre-renal from intrinsic (ATN) AKI: [1]
FENa = (urine Na × plasma creatinine) / (plasma Na × urine creatinine) × 100 [1]
| Pre-renal | ATN | |
|---|---|---|
| FENa | <1% | >2% |
| Urine Na | <20 mmol/L | >40 mmol/L |
| BUN/creatinine ratio | >20:1 | <10–20:1 |
| Urine sediment | Bland | Muddy brown casts |
DWE exam trap: FENa is invalidated by diuretics (which force sodium excretion regardless of tubular integrity). If the patient has received frusemide, use the fractional excretion of urea (FEUN) instead — threshold <35% suggests pre-renal. This is one of the most commonly tested AKI MCQ discriminators. [1]
Imaging
| Investigation | When |
|---|---|
| Bladder scan | Every AKI — immediate exclusion of lower urinary tract obstruction |
| Renal ultrasound | All AKI not clearly pre-renal and volume-responsive — check for hydronephrosis, kidney size (small = chronic), cysts, stones. Resistive index can help. |
| CT KUB / CT urogram | If obstruction suspected but not seen on ultrasound (retroperitoneal fibrosis, small stones) |
| CT angiography | If renal artery occlusion suspected (flank pain, AF, sudden anuria) |
| Renal biopsy | If intrinsic AKI of unclear cause, especially with active sediment or systemic disease — urgently if RPGN suspected |
Selected investigations (based on clinical context)
| Investigation | When to order |
|---|---|
| ANA, anti-dsDNA, ANCA, anti-GBM | Glomerulonephritis or vasculitis suspected |
| Complement C3, C4 | Lupus, post-infectious GN, cryoglobulinaemia |
| Hepatitis B/C, HIV serology | Secondary glomerular disease, pre-transplant |
| Serum electrophoresis, serum free light chains, urine Bence-Jones | Myeloma cast nephropathy (elderly, unexplained AKI) |
| Creatine kinase | Rhabdomyolysis (immobility, statins, drugs, trauma) |
| Myoglobin | If CK elevated or suspicion high |
| Troponin | Myocardial infarction as cause (cardiogenic shock) |
| [TIMP-2]x[IGFBP7] biomarker | Research/emerging — risk stratifies for moderate-severe AKI within 12 hours |
Management principles
Step 1: Resuscitate and optimise haemodynamics
- Correct hypovolaemia with balanced crystalloid aliquots (250–500 mL boluses, reassess between).
- Target MAP ≥65 mmHg. Use vasopressors (noradrenaline) for vasodilatory shock after volume repletion — do not flood a patient who is vasoplegic but already volume-replete.
- Correct the underlying cause of hypoperfusion: sepsis source control, treat heart failure, stop bleeding. [1]
Step 2: Treat the underlying cause
This is disease-specific:
- Sepsis: antibiotics within 1 hour, source control, follow Surviving Sepsis guidelines
- Obstruction: urinary catheter or nephrostomy — can produce dramatic diuresis post-relief (monitor electrolytes and volume)
- Rhabdomyolysis: aggressive IV fluid (target urine output 200–300 mL/h), consider sodium bicarbonate if severe acidosis [1]- Glomerulonephritis/vasculitis: urgent nephrology referral, immunosuppression (cyclophosphamide + glucocorticoids), plasma exchange for anti-GBM
- AIN: stop offending drug, glucocorticoids if severe or persistent
- Tumour lysis syndrome: rasburicase, allopurinol, aggressive hydration [1]
Step 3: Remove all nephrotoxic agents
Review every medication. Stop: [1]
| Drug class | Reason |
|---|---|
| NSAIDs (all) | Afferent arteriolar vasoconstriction |
| ACE inhibitors / ARBs | Efferent arteriolar dilation — drop in glomerular pressure |
| Aminoglycosides | Direct proximal tubular toxicity |
| Metformin | Risk of lactic acidosis (not nephrotoxic but contraindicated in significant AKI) |
| Diuretics | If not needed for volume overload |
| Certain antimicrobials | Adjust or withhold based on renal function (see drug dosing) |
| Herbal/alternative | Some contain aristolochic acid or heavy metals |
Step 4: Manage complications
Hyperkalaemia (K+ ≥6.0 mmol/L or ECG changes) [1]
This is a medical emergency. Treat in parallel: [1]
- Stabilise myocardium: calcium gluconate 10 mL of 10% IV over 2–5 minutes (onset seconds, duration 30–60 min). Repeat if ECG changes persist.
- Shift potassium into cells: insulin-dextrose (10 units Actrapid in 25 g glucose IV over 15 min; onset 15 min, duration 4–6 h) ± salbutamol 10–20 mg nebulised.
- Remove potassium: the above are temporising. Definitive removal requires RRT (if refractory) or restoration of renal function. Gastrointestinal potassium binders (patiromer, sodium zirconium cyclosilicate) are too slow for emergency use. [1]
If hyperkalaemia is refractory or recurrent with ECG changes, initiate RRT. [1]
Metabolic acidosis
Treat the cause (lactic acidosis from sepsis, ketoacidosis). Sodium bicarbonate is not routinely recommended for lactic acidosis in AKI (BICARB-ICU trial showed no mortality benefit). It may be considered if pH <7.1 or for specific indications (TCA overdose, hyperkalaemia). If acidosis is refractory, RRT is indicated. [1]
Volume overload
- Trial of IV frusemide (40–80 mg bolus or infusion). Response predicts need for RRT.
- If refractory oliguria with pulmonary oedema, proceed to RRT. [1]
Step 5: Drug dosing in AKI
Every renally-cleared drug must be dose-adjusted. Key principles:
- Use the estimated creatinine clearance (Cockcroft-Gault) or eGFR at the current (worsened) function, not baseline.
- Vancomycin: therapeutic drug monitoring by trough level (target 15–20 mg/L for serious infections). In AKI, extend dosing interval — do not use fixed frequency. Many centres use AUC-guided dosing. [1]- Aminoglycosides (gentamicin): extended-interval dosing with trough monitoring. In AKI, the interval may be 36–48 hours or longer. Consider avoiding if possible.
- Beta-lactams: reduce frequency (not dose) for renal clearance. Piperacillin-tazobactam and cefepime can cause neurotoxicity (encephalopathy, myoclonus) if not adjusted.
- Anticoagulants: enoxaparin reduces dose or switch to UFH (unfractionated heparin) which can be titrated by APTT. DOACs are often contraindicated in significant AKI.
- Opioids: morphine metabolites (M6G) accumulate — use fentanyl or reduce dose. [1]
DWE high-yield: In the ICU with AKI, the simplest and safest approach to vancomycin and aminoglycosides is therapeutic drug monitoring. If an MCQ asks "best way to dose vancomycin in AKI", the answer is trough-guided or AUC-guided dosing, not a fixed formula. [1]
Indications for renal replacement therapy — AEIOU
RRT in AKI is initiated for absolute (life-threatening) or relative (progressive) indications. The mnemonic AEIOU captures the absolute indications: [1]
| Letter | Indication | Detail |
|---|---|---|
| A | Acidosis | Severe metabolic acidosis (pH <7.1) refractory to medical therapy |
| E | Electrolytes | Refractory hyperkalaemia (K+ persistently >6.5 mmol/L or with ECG changes despite medical therapy) |
| O | Overload | Refractory volume overload / pulmonary oedema unresponsive to diuretics |
| U | Uraemia | Uraemic complications — pericarditis, encephalopathy, bleeding |
Progressive anuria or rapidly rising creatinine without absolute indication is a relative indication — discuss with nephrology/ICU early. [1]
Timing of RRT initiation — the evidence
Three landmark trials shape practice: [1]
- AKIKI (PMID 27181456): In critically ill adults with KDIGO stage 3 AKI, early vs delayed RRT showed no difference in 60-day mortality. Critically, 49% of the delayed group never needed RRT — early initiation exposed half the patients to an unnecessary procedure [2].
- STARRT-AKI (PMID 32668114): The largest trial (3019 patients, 168 hospitals, 15 countries). Accelerated vs standard strategy. No mortality benefit from early RRT, and worse outcomes — higher RRT dependence at 90 days (10.4% vs 6.0%) and more adverse events [3].
- ELAIN (PMID 27209269): Single-centre, surgical-heavy population. Early initiation at KDIGO stage 2 showed a mortality benefit (39.3% vs 54.7% at 90 days) [4].
The synthesis: For the typical critically ill patient, a delayed/standard strategy — waiting for KDIGO stage 3 and absolute indications — is supported by AKIKI and STARRT-AKI. ELAIN's benefit has not been replicated in larger multicentre trials. Early RRT may be considered in specific populations (post-cardiac surgery, rapidly progressive AKI) but is not the default. [1]
DWE examiner question: "When would you start RRT in this patient?" Model answer: "I would use a standard strategy, reserving RRT for absolute indications (AEIOU) or progressive AKI with no evidence of recovery despite treating the cause. I would not initiate RRT early based on AKIKI and STARRT-AKI, which showed no benefit and potential harm from early initiation. I would discuss with nephrology and ICU early to plan vascular access and modality." [1]
RRT modalities
| Modality | Setting | Advantages | Disadvantages |
|---|---|---|---|
| Intermittent haemodialysis (IHD) | Ward, haemodynamically stable | Efficient solute clearance, established | Hypotension, requires stable access |
| Continuous RRT (CVVHDF/CVVH) | ICU, haemodynamically unstable | Gentle fluid removal, stable haemodynamics | Anticoagulation, cost, immobilisation |
| Sustained low-efficiency dialysis (SLED) | ICU stepdown | Compromise between IHD and CRRT | Requires specialised machine time |
| Peritoneal dialysis | Paediatrics, resource-limited | No vascular access or anticoagulation | Lower efficiency, peritonitis risk |
Fluid choice — the evidence
The choice of crystalloid matters: [1]
- Balanced crystalloids (Plasma-Lyte, Hartmann's, Ringer's lactate) are preferred over 0.9% saline in patients at risk of AKI.
- SMART trial (2019): In critically ill adults, balanced crystalloids reduced the composite of major adverse kidney events (MAKE30: death, RRT, or persistent renal dysfunction) compared with saline.
- SPLIT trial (2015): In ICU patients, no difference in AKI rates between balanced and saline — but the study was underpowered and used buffered saline. [1]
The mechanism: large-volume saline causes hyperchloraemic metabolic acidosis, which causes renal vasoconstriction (afferent arteriole) and reduces renal blood flow. Balanced solutions avoid this. [1]
Practical rule: For AKI resuscitation, use balanced crystalloid unless there is a specific indication for saline (hyponatraemia, hypochloraemia, TCA overdose). [1]
Prognosis and recovery
Mortality
AKI carries a substantial mortality burden that correlates with severity:
- Hospital-acquired AKI stage 1: ~10–20% in-hospital mortality
- ICU-acquired AKI requiring RRT: 50–60% mortality
- The mortality is driven by the underlying illness (sepsis, multi-organ failure), not the AKI alone [1]
Recovery trajectories
| Outcome | Proportion |
|---|---|
| Complete recovery (return to baseline creatinine) | ~60–70% |
| Partial recovery (new CKD or worsened baseline) | ~15–20% |
| Dialysis dependence at discharge | ~5–10% (higher in CKD, diabetes, older age) |
Long-term consequences
Even patients who "recover" biochemically are at increased risk of:
- Progression to CKD: AKI accelerates CKD progression. Every AKI episode increases the long-term risk of CKD stage 4–5 by 2–3 fold.
- Recurrent AKI: 20–30% within 1 year.
- Cardiovascular events: AKI is an independent risk factor for subsequent MI, heart failure, and stroke. [1]
Follow-up
All patients with AKI stage 2 or higher should have:
- Creatinine checked at 1–3 months post-discharge to confirm recovery or detect new CKD
- Medication review — reinstate ACE inhibitors/ARBs only after recovery, especially in heart failure and CKD
- Nephrology referral if CKD persists (eGFR <60 at 3 months) or if recurrent AKI
- Patient education on avoiding NSAIDs, maintaining hydration during illness ("sick day rules") [1]
DCE long-case approach
Opening statement (SASPOP)
"Mrs Patel is a 74-year-old woman with type 2 diabetes, hypertension, and ischaemic heart disease who presents with a 3-day history of diarrhoea and vomiting, reduced oral intake, and oliguria. She takes metformin, perindopril, frusemide, and ibuprofen for osteoarthritis. [1]
Her main problems are:
- Acute kidney injury, KDIGO stage 2 — multifactorial: volume depletion from gastroenteritis, superimposed nephrotoxicity from NSAIDs and ACE inhibitor, on a background of diabetic CKD
- Hyperkalaemia (K+ 6.2 mmol/L) — requiring emergency management [1]3. Metabolic acidosis (pH 7.24, bicarbonate 14)
- Likely sepsis — source to identify (urine, blood cultures)
- Polypharmacy with multiple nephrotoxins" [1]
Integrated management plan
Present the plan in five domains: [1]
- Resuscitate: ABCDE. She is hypovolaemic (flat JVP, dry mucous membranes) — give 500 mL balanced crystalloid boluses, reassess. Treat hyperkalaemia immediately: calcium gluconate, insulin-dextrose.
- Treat the cause: Stop ibuprofen and perindopril. Withhold metformin (lactic acidosis risk). Send cultures, start antibiotics if sepsis suspected. Fluid resuscitate until euvolaemic.
- Manage complications: Monitor K+ and acid-base. If hyperkalaemia refractory or acidosis worsens with pulmonary oedema, discuss RRT early.
- Adjust medications: Dose-adjust all renally-cleared drugs. Review antibiotic doses.
- Plan recovery: Monitor creatinine trajectory. Reinstate ACE inhibitor only after recovery and if indicated. Arrange follow-up creatinine at 1 month. Educate on sick day rules (hold ACE inhibitor, diuretics, metformin, SGLT2i during acute illness). [1]
DCE examiner probing questions:
- "Would you give her fluids or diuretics?" → Assess volume status first. She is hypovolaemic — fluids.
- "Why did her NSAID contribute?" → Afferent arteriolar vasoconstriction from prostaglandin inhibition, removing compensatory vasodilation in a volume-depleted kidney.
- "Should you restart her ACE inhibitor on discharge?" → Only after AKI recovery. In a patient with diabetes and likely CKD, ACE inhibitor is renoprotective long-term, but must wait until stable.
- "What are her sick day rules?" → Hold ACE inhibitor, ARB, diuretics, metformin, SGLT2i, and NSAIDs during acute illness with reduced intake. Resume when recovered and eating/drinking normally. [1]
DCE short-case approach: volume status assessment
Instruction: "Assess this patient's volume status." [1]
Systematic routine
- Hands: Warm and dry (well perfused) or cold and clammy (vasoconstriction from shock). Capillary refill time at the nailbed — normal <2 seconds; prolonged suggests hypoperfusion. Skin turgor — pinch skin over clavicle; tenting suggests dehydration.
- Pulse: Rate and character. Thready pulse with postural drop suggests hypovolaemia. Bounding pulse suggests sepsis.
- Blood pressure: Check lying and standing (postural drop >20 mmHg systolic suggests significant volume depletion). Compare to patient's baseline.
- JVP: The single most useful bedside sign. Elevated (>3 cm above sternal angle at 45 degrees) suggests volume overload or right heart failure. Flat/impalpable suggests hypovolaemia. In atrial fibrillation, average over several beats.
- Mucous membranes and eyes: Dry tongue and sunken eyes suggest dehydration.
- Lungs: Bilateral basal crackles suggest pulmonary oedema (volume overload). Clear lungs with flat JVP suggest hypovolaemia.
- Heart: Gallop rhythm (S3) suggests heart failure and volume overload.
- Abdomen: Ascites and sacral oedema suggest volume overload. Bladder distension may suggest obstruction.
- Peripheral oedema: Ankle and sacral — present in overload, CKD, heart failure, cirrhosis. Absent in pure hypovolaemia. [1]
Presentation template
"I assessed this patient's volume status. The hands are warm and well perfused with capillary refill of 2 seconds. The pulse is regular at 92 beats per minute, with normal volume and character. Blood pressure is 105/60 lying, 95/55 standing — a postural drop of 10 mmHg systolic. The JVP is flat. The mucous membranes are dry and the tongue is furrowed. The lungs are clear. There is no peripheral or sacral oedema. [1]
In summary, these findings are consistent with intravascular volume depletion. I would manage this patient with intravenous balanced crystalloid resuscitation, giving 500 mL boluses with reassessment between each." [1]
Key DWE MCQ patterns
- KDIGO staging from creatinine/urine output data: Calculate the stage using the worst criterion. Common trap: under-staging by using only creatinine when urine output criteria meet a higher stage.
- FENa interpretation with diuretics: If the patient has received frusemide, use FEUN instead. FENa <1% suggests pre-renal; FEUN <35% suggests pre-renal.
- Contrast nephropathy prevention: PRESERVE trial — intravenous isotonic saline is the only proven strategy. Acetylcysteine and bicarbonate are not effective.
- Timing of RRT: AKIKI and STARRT-AKI — delayed strategy is preferred for most patients. Do not initiate early unless absolute indication (AEIOU).
- Fluid choice: Balanced crystalloids over 0.9% saline (SMART trial) — saline causes hyperchloraemic acidosis and worsens renal outcomes.
- Drug nephrotoxicity mechanism: NSAIDs (afferent arteriole), ACEi (efferent arteriole), aminoglycosides (proximal tubule), contrast (medullary + tubular).
- Nephrology emergency: RBC casts or rapid creatinine rise with active sediment = RPGN/vasculitis — urgent biopsy and immunosuppression.
- Post-obstructive diuresis: After relief of obstruction, monitor for massive diuresis with electrolyte disturbance — replace fluid and electrolytes. [1]
References
[1] KDIGO 2012 Clinical Practice Guideline for AKI — international consensus definition, staging (creatinine + urine output), and management recommendations. Kidney Int Suppl 2012;2:1–138. [2] AKIKI — Early vs delayed RRT in KDIGO stage 3 AKI. No mortality difference; 49% of delayed group never needed RRT. [3] STARRT-AKI — Accelerated vs standard RRT initiation. No benefit; worse outcomes (higher RRT dependence) with accelerated strategy. [4] ELAIN — Early vs delayed RRT at KDIGO stage 2. Single-centre, showed mortality benefit for early initiation (not replicated in larger trials). [5] PRESERVE — Sodium bicarbonate and acetylcysteine for contrast-associated AKI prevention. Neither effective; IV isotonic saline is the only proven prophylaxis. [6] ADQI 21 — Lung-kidney interactions in critical illness: consensus on the pathophysiology of organ crosstalk. [7] Joannidis et al. — Septic AKI: systematic review of incidence and outcomes.
KDIGO 2012 AKI Guideline; NICE NG148 (2019); Renal Association AKI Guideline; Kidney Health Australia. [1]
References
- [1]Ronco C, Bellomo R, Kellum JA. Acute kidney injury Lancet, 2019.PMID 31777389
- [2]Gaudry S, Hajage D, Schortgen F, et al. Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit N Engl J Med, 2016.PMID 27181456
- [3]STARRT-AKI Investigators, Bagshaw SM, Wald R, et al. Timing of Initiation of Renal-Replacement Therapy in Acute Kidney Injury N Engl J Med, 2020.PMID 32668114
- [4]Zarbock A, Kellum JA, Schmidt C, et al. Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial JAMA, 2016.PMID 27209269
- [5]Weisbord SD, Gallagher M, Jneid H, et al. Outcomes after Angiography with Sodium Bicarbonate and Acetylcysteine N Engl J Med, 2018.PMID 29130810
- [6]Joannidis M, Forni LG, Klein SJ, et al. Lung-kidney interactions in critically ill patients: consensus report of the Acute Disease Quality Initiative (ADQI) 21 Workgroup Intensive Care Med, 2020.PMID 31820034
- [7]Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL; AWARE Investigators. Epidemiology of Acute Kidney Injury in Critically Ill Children and Young Adults N Engl J Med, 2017.PMID 27959707