Phys · renal
Chronic Kidney Disease
Also known as CKD · chronic renal failure · CRF · chronic renal impairment · predialysis · end-stage kidney disease · ESKD · ESRD · kidney failure · diabetic nephropathy · hypertensive nephrosclerosis · chronic glomerulonephritis · reflux nephropathy · adult polycystic kidney disease
Consultant-physician-depth guide to chronic kidney disease — KDIGO definition and CGA staging, pathophysiology of nephron loss and progressive fibrosis, aetiology, complications (CKD-MBD, renal anaemia, acidosis, hyperkalaemia, cardiovascular risk), progression-slowing therapy (RAAS blockade, SGLT2 inhibitors, finerenone, blood pressure control), dialysis preparation, transplant workup, conservative care, and drug dosing. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Chronic Kidney Disease
The answer first
Chronic kidney disease (CKD) is an abnormality of kidney structure or function present for more than three months, with implications for health [1]. Operationally, the KDIGO definition requires any of: eGFR <60 mL/min/1.73 m² for over three months; markers of kidney damage (albuminuria [ACR >3 mg/mmol], urine sediment abnormalities, imaging abnormalities, or kidney transplant); or a kidney biopsy showing chronic disease.
The two clinical questions that dominate CKD management: [1]
- What is causing the kidney disease, and is it treatable or reversible? Always name the cause — CKD is a syndrome, not a diagnosis.
- What is the risk of progression to kidney failure, and how do I reduce that risk and the cardiovascular risk that dwarfs it? [1]
The management mandate, in priority order: [1]
- Identify and treat the underlying cause — and exclude any superimposed acute-on-chronic process.
- Slow progression with the evidence-based quartet: RAAS blockade for albuminuria, SGLT2 inhibition, blood pressure control, and (in diabetic CKD) finerenone. Reduce proteinuria as a surrogate endpoint.
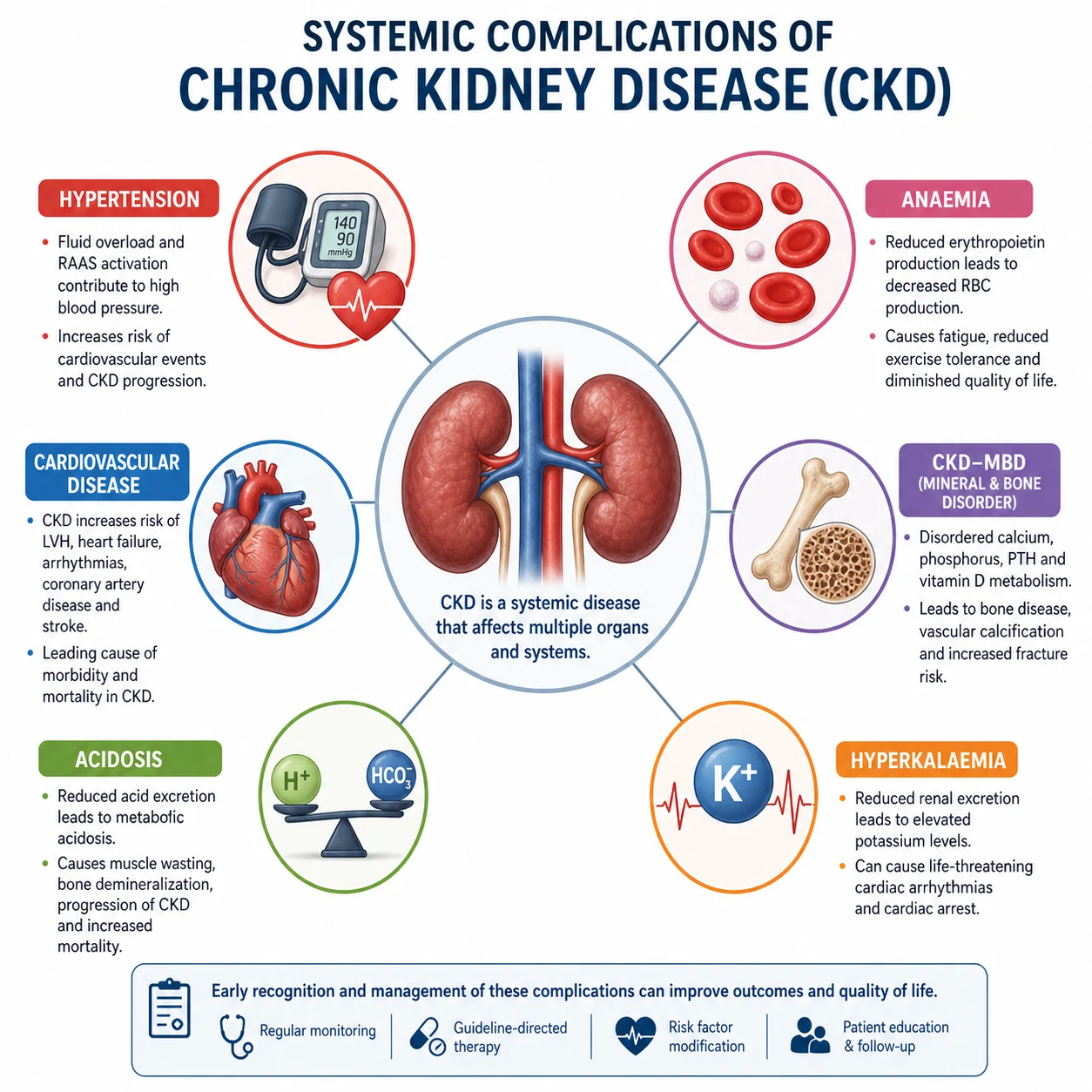
- Prevent and manage complications — CKD-MBD, anaemia, acidosis, hyperkalaemia, volume overload, and the dominant risk of cardiovascular disease.
- Prepare for kidney replacement therapy (KRT) early — at eGFR <30 refer for dialysis education, plan vascular access at eGFR 15-20, and arrange pre-emptive transplant workup. Offer a conservative care pathway for those who will not benefit from dialysis.
- Minimise iatrogenic harm — dose-adjust every renally cleared drug, avoid nephrotoxins (NSAIDs, gadolinium in severe CKD), and hold the sick-day medications during intercurrent illness. [1]
The single most important exam principle: cardiovascular disease kills more CKD patients than kidney failure does. A stage 3b patient is far more likely to die of an MI than reach dialysis. CKD is a coronary risk equivalent, and management must reflect this. [1]
KDIGO definition and CGA staging
Diagnostic criteria (KDIGO)
CKD is present when any of the following persist for more than three months: [1]
| Marker | Threshold |
|---|---|
| eGFR | <60 mL/min/1.73 m² |
| Urine sediment | Persistent abnormalities (haematuria, red cell or white cell casts, granular casts) |
| Imaging | Structural abnormalities (polycystic kidneys, reflux nephropathy, scarring, hydronephrosis) |
| Transplant | Solid organ kidney transplant |
| Biopsy | Histological evidence of chronic kidney damage |
The three-month duration is non-negotiable. A single low eGFR may reflect acute kidney injury (AKI); it is only CKD if it persists. Always seek prior results — and if none exist, repeat at 3 months before labelling a patient with CKD. [1]
DWE exam trap: A common MCQ stem is an elderly patient with a one-off eGFR of 52 on presentation with sepsis. This is not CKD — it is AKI until proven otherwise. The diagnosis requires the abnormality to persist for more than three months, or other markers of chronicity (small kidneys, anaemia, CKD-MBD) to support it. [1]
The CGA staging — Cause, GFR, Albuminuria
KDIGO 2012 abandoned the old "stage 1-5" label alone and replaced it with CGA staging — Cause, GFR category, Albuminuria category [1]. This matters because two patients with the same eGFR can have wildly different prognoses depending on albuminuria.
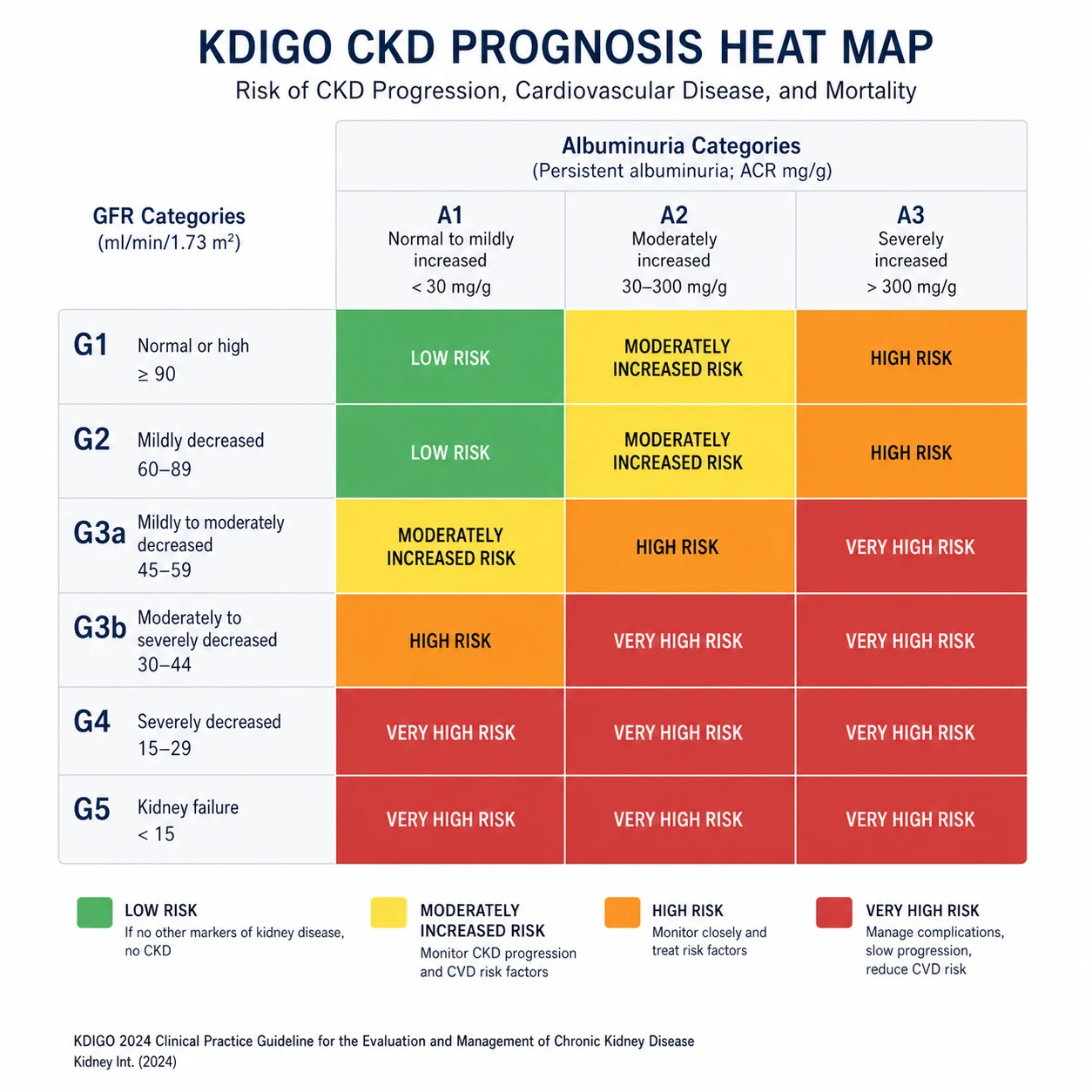
GFR categories: [1]
| Category | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal or high — must have another marker of kidney damage to call it CKD |
| G2 | 60–89 | Mildly decreased — must have another marker if under 60 is not yet met |
| G3a | 45–59 | Mildly to moderately decreased |
| G3b | 30–44 | Moderately to severely decreased |
| G4 | 15–29 | Severely decreased |
| G5 | <15 (or dialysis) | Kidney failure |
Albuminuria categories: [1]
| Category | ACR (mg/mmol) | ACR (mg/g) | Description |
|---|---|---|---|
| A1 | <3 | <30 | Normal to mildly increased |
| A2 | 3–30 | 30–300 | Moderately increased (microalbuminuria) |
| A3 | >30 | >300 | Severely increased (macroalbuminuria, nephrotic-range if >220 mg/mmol) |
Why the heat map matters
The KDIGO heat map plots GFR category against albuminuria category and colour-codes the cells by risk — green (low), yellow (moderately increased), orange (high), red (very high). Two clinical facts emerge that every physician must carry: [1]
- Albuminuria upstages risk. A patient with eGFR 55 (G3a) and ACR 50 (A3) is high risk — they progress faster and have more cardiovascular events than a patient with eGFR 25 (G4) and ACR 2 (A1). Albuminuria is not just a marker of glomerular damage; it is a tubulo-toxic driver of fibrosis.
- A G3b-A3 patient has a 5-year kidney-failure risk similar to a G5-A1 patient. Use the Kidney Failure Risk Equation (KFRE, Tangri 4-variable: age, sex, eGFR, ACR) to quantify risk and triage referral and dialysis planning [11].
Pathophysiology — why CKD progresses
The intact nephron hypothesis and hyperfiltration
The kidney loses nephrons throughout CKD, but the surviving nephrons hypertrophy and hyperfilter to maintain total GFR. This is the intact nephron hypothesis. Each surviving nephron bears a higher single-nephron GFR (SNGFR), and the glomerulus is exposed to increased pressure. [1]
Hyperfiltration is adaptive in the short term — total GFR appears preserved — but maladaptive in the long term. The raised glomerular capillary pressure drives: [1]
- Mechanical strain on podocytes — detachment, foot-process effacement, protein leak
- Glomerular hypertrophy — eventually sclerosis of the glomerulus
- Passage of filtered protein into the tubule — reabsorbed by proximal tubular cells, triggering tubulo-interstitial inflammation and fibrosis [1]
This is why an eGFR can look "normal" (G1 or G2) while the kidney is silently destroying itself through hyperfiltration. Diabetes is the prototype: early diabetic nephropathy shows hyperfiltration (high eGFR) before albuminuria appears, then progressive loss once albuminuria sets in. [1]
Albuminuria as both marker and mechanism
Albumin in the urine is not a passive consequence of glomerular damage. Filtered albumin and other proteins are endocytosed by proximal tubular cells, which become inflamed and fibrogenic. The tubule secretes cytokines (TGF-beta, MCP-1, RANTES) that recruit inflammatory cells and activate fibroblasts. The end-point is tubulo-interstitial fibrosis — the strongest histological predictor of progression. [1]
This is the mechanistic rationale for proteinuria reduction as a therapeutic target: lowering albuminuria with an ACE inhibitor or SGLT2 inhibitor reduces tubular injury and slows fibrosis, independent of blood pressure. [1]
The shared final common pathway: fibrosis
Regardless of cause — diabetes, hypertension, glomerulonephritis, reflux, polycystic disease — CKD converges on tubulo-interstitial fibrosis, glomerulosclerosis, and vascular rarefaction. The mediators are: [1]
- TGF-beta — drives fibroblast activation and epithelial-to-mesenchymal transition
- RAAS activation — angiotensin II raises glomerular pressure, is directly profibrotic, and drives oxidative stress
- Endothelial dysfunction and microvascular rarefaction — capillary loss starves tubules
- Chronic inflammation — macrophages, cytokines, uraemic toxins
- Metabolic and acid-base stress — ammoniagenesis, phosphate retention [1]
Once enough nephrons are lost, the surviving nephrons are under such strain that the disease becomes self-perpetuating, even if the original cause is removed. This is why we speak of "slowing progression" rather than curing CKD — and why the earlier you intervene, the better. [1]
Loss of endocrine and exocrine function
The kidney is not just a filter. As nephrons are lost: [1]
- Erythropoietin production falls — renal anaemia appears, typically from stage 3 onwards, proportional to eGFR loss.
- 1-alpha hydroxylation of vitamin D fails — hypocalcaemia, secondary hyperparathyroidism, and CKD-MBD.
- Bicarbonate generation and ammoniagenesis fail — metabolic acidosis, which itself accelerates muscle wasting and progression.
- Phosphate excretion falls — phosphate retention, which stimulates PTH and drives vascular calcification.
- Sodium and water handling fails — hypertension and volume overload. [1]
These consequences are the complications of CKD, and each requires its own management track alongside progression-slowing therapy. [1]
Causes — name the diagnosis
| Cause | Clues from history, examination, investigation |
|---|---|
| Diabetic nephropathy | Long-standing diabetes, retinopathy, albuminuria (often nephrotic), normal-sized or enlarged kidneys, no haematuria. Commonest single cause worldwide. |
| Hypertensive nephrosclerosis | Long-standing hypertension, LVH, mild albuminuria, small kidneys. Often a co-contributor rather than sole cause. |
| Chronic glomerulonephritis | Haematuria (dysmorphic RBCs, casts), proteinuria, prior episodes. Includes IgA nephropathy, membranous, FSGS, lupus nephritis. |
| Adult polycystic kidney disease (ADPKD) | Family history (autosomal dominant), bilateral cystic kidneys (often palpable), hypertension, haematuria, large kidneys on imaging. |
| Reflux nephropathy | Childhood UTI/recurrent pyelonephritis, focal renal scarring, hypertension, often asymmetric kidneys. |
| Obstructive uropathy | Prostatic disease, neurogenic bladder, pelvic tumour, retroperitoneal fibrosis. Bilateral hydronephrosis on imaging (but obstruction may be chronic and non-dilated). |
| Tubulointerstitial disease | Chronic NSAID use, analgesic nephropathy, lithium, heavy metals, sarcoidosis, Sjogren. |
| Vascular disease | Atherosclerotic renovascular disease (flash pulmonary oedema, asymmetric kidneys, abdominal bruit), hypertensive emergency. |
| Myeloma cast nephropathy | Elderly, anaemia out of proportion, hypercalcaemia, back pain. Check serum free light chains. |
| Other | Lupus, ANCA vasculitis, anti-GBM, Alport syndrome, post-transplant, HIV-associated nephropathy, APOL1-mediated disease. |
How to discriminate at the bedside
Two pieces of information narrow the differential more than any others: [1]
- Kidney size on ultrasound. Small kidneys (<9 cm) indicate chronic irreversible scarring (most often hypertensive, reflux, or chronic GN). Enlarged kidneys suggest diabetic nephropathy, amyloid, infiltration, or polycystic disease. Asymmetric kidneys suggest reflux nephropathy or renovascular disease.
- The urine dipstick and sediment. Albuminuria alone points to diabetic or hypertensive disease. Haematuria plus proteinuria suggests glomerular disease. A bland urine with rising creatinine suggests tubulointerstitial disease, myeloma, or post-renal causes. [1]
When to biopsy
Renal biopsy is the definitive investigation for cause, and is indicated when: [1]
- The diagnosis is unclear from non-invasive testing
- There is active urine sediment (haematuria, casts) suggesting glomerular disease
- Albuminuria is in the nephrotic range without an obvious cause
- There is rapidly progressive disease (consider RPGN — this is a nephrology emergency)
- The kidneys are normal-sized (small shrunken kidneys usually preclude useful biopsy) [1]
Biopsy is generally not performed when the diagnosis is clear from clinical features (e.g., classic diabetic nephropathy with retinopathy, or small kidneys with long-standing hypertension), or when the kidneys are too small to safely biopsy. [1]
Acute-on-chronic kidney disease
A patient with CKD who presents with a further rise in creatinine has acute-on-chronic kidney disease — a superimposed AKI on a background of CKD. This is one of the most common scenarios in clinical medicine and a high-yield DWE topic. [1]
The causes are the same as for AKI (see the AKI topic), but the threshold for injury is lower and the consequences more severe. The classic contributors in CKD: [1]
- Volume depletion from diuretics, illness, GI losses
- Nephrotoxins — NSAIDs (including over-the-counter), iodinated contrast, certain antibiotics
- RAAS blockade — ACE inhibitors and ARBs cause a functional drop in GFR; in volume depletion or renal artery stenosis this becomes clinically significant
- SGLT2 inhibitors during acute illness — hold as part of sick-day rules (see below)
- Urinary tract obstruction — prostatic disease is common in this population
- Sepsis and other systemic illness [1]
The management is identical to AKI: identify and treat the precipitant, restore perfusion if volume-depleted, remove nephrotoxins, and manage complications. Most acute-on-chronic episodes are at least partly reversible — do not assume the new baseline is the new chronic state until recovery has plateaued. [1]
Sick-day rules — the safety contract
Every patient on ACE inhibitors, ARBs, SGLT2 inhibitors, diuretics, metformin, and NSAIDs must be taught to hold these medications during any acute illness with reduced oral intake, vomiting, diarrhoea, or fever — and to resume them when recovered and eating and drinking normally. This single intervention prevents a large fraction of acute-on-chronic presentations and is a high-yield communication point for the long case. [1]
Investigation strategy
The baseline panel — at every CKD encounter
| Investigation | What it tells you |
|---|---|
| eGFR (CKD-EPI 2021 race-free creatinine) | Confirms chronicity when repeated at 3 months; tracks progression. Use cystatin C or measured GFR when creatinine is unreliable (low muscle mass, amputation, pregnancy, very high or low body mass). |
| Urinary ACR | Quantifies albuminuria — the single most important prognostic marker and the staging variable. |
| Urine dipstick and microscopy | Detects haematuria, leucocytes, nitrites, casts — directs toward glomerular, infective, or tubulointerstitial causes. |
| Renal ultrasound | Kidney size (small = chronic), cortical thickness, scarring, hydronephrosis (exclude obstruction), cysts. |
| FBC | Anaemia of CKD (typically normocytic normochromic). |
| Iron studies (ferritin, TSAT) | Absolute and functional iron deficiency — common in CKD, must be corrected before ESA. |
| U&E (Na, K, bicarbonate) | Hyperkalaemia, metabolic acidosis. |
| Ca, PO4, PTH, 25-OH vitamin D | CKD-MBD surveillance from stage 3. |
| Lipids, HbA1c | Cardiovascular risk and glycaemic control. |
| ECG (and echo if indicated) | LVH, ischaemia, structural heart disease — CV risk assessment. |
Confirming the cause — selective testing
| Test | Indication |
|---|---|
| HbA1c, fasting glucose | Diabetes |
| ANA, anti-dsDNA, ANCA, anti-GBM, complements | Suspected glomerulonephritis, lupus, vasculitis |
| Hepatitis B, C, HIV serology | Secondary glomerular disease; pre-transplant workup |
| Serum electrophoresis, serum free light chains, urine Bence-Jones | Suspected myeloma (elderly, unexplained CKD, anaemia, hypercalcaemia) |
| APOL1 genotype | Suspected APOL1-mediated disease in patients of recent West African ancestry (high-yield but selective) |
| Genetic testing (PKD1/PKD2) | Atypical or pre-donor workup in suspected ADPKD |
| Renal doppler ultrasound / CT/MR angiography | Suspected renovascular disease (asymmetric kidneys, abdominal bruit, flash pulmonary oedema, AKI on ACEi) |
| Renal biopsy | Intrinsic CKD of unclear cause, especially with active sediment or nephrotic-range proteinuria |
The Kidney Failure Risk Equation
The 4-variable KFRE (age, sex, eGFR, ACR) predicts the 2-year and 5-year probability of progression to kidney failure (need for dialysis or transplant) [11]. It is validated globally and integrated into KDIGO 2024. Use it to:
- Triage nephrology referral — high risk (>5% at 5 years) warrants referral; very high risk (>15%) warrants dialysis education and access planning.
- Time vascular access creation — AVF needs 6-12 months to mature; predict when dialysis is likely and work backwards.
- Counsel patients — translate the abstract "stage" into a concrete risk number. [1]
Slowing progression — the evidence-based quartet
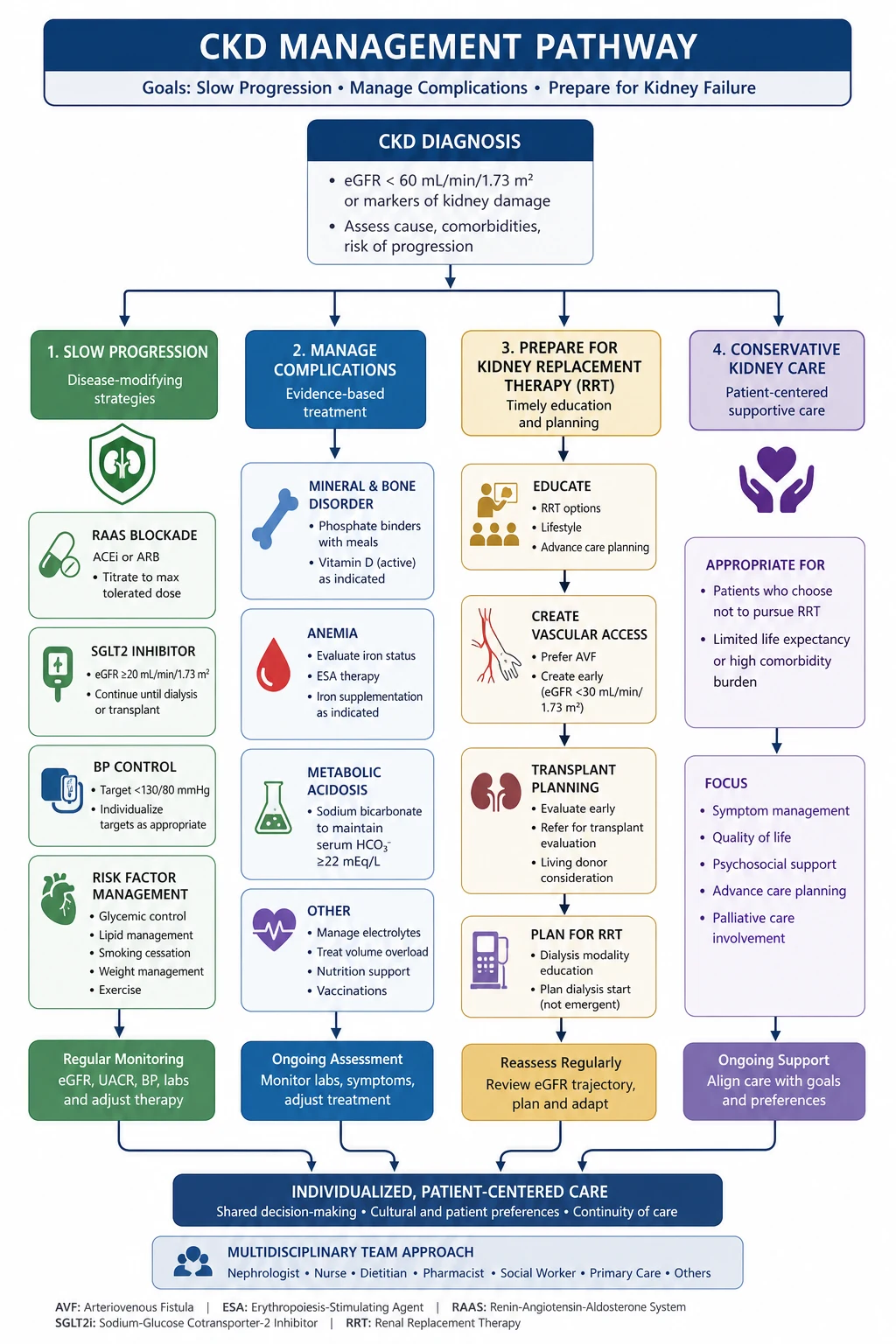
This is the highest-yield section for the DWE and DCE. Every CKD patient with albuminuria should be on, or considered for, four interventions. The evidence base is large, recent, and testable. [1]
1. RAAS blockade — ACE inhibitor or ARB
Angiotensin II raises efferent arteriolar tone, raising glomerular capillary pressure and single-nephron GFR. Blocking it with an ACE inhibitor or ARB lowers intraglomerular pressure, reduces albuminuria, and slows progression. The benefit is above and beyond blood pressure lowering. [1]
- Indication: any CKD patient with ACR >3 mg/mmol (albuminuria), particularly diabetes, hypertension, or glomerular disease. RAAS blockade is the foundation of proteinuric CKD management.
- Choice: either an ACE inhibitor (ramipril, perindopril, enalapril) or an ARB (losartan, valsartan, telmisartan) — they are equivalent. RENAAL established losartan's renoprotection in diabetic nephropathy [7]. Do not combine an ACEi and an ARB — dual blockade increases AKI and hyperkalaemia without outcome benefit (ONTARGET).
- Initiation and monitoring:
- Check creatinine and K+ at 1-2 weeks after starting and after each dose titration.
- An early rise in creatinine of up to 30% is expected and acceptable — it reflects the desired reduction in intraglomerular pressure. A rise >30% or within 4 weeks suggests volume depletion, renal artery stenosis, or over-diuresis: review and investigate.
- Monitor K+ — hyperkalaemia is the main limitation (see below).
- When to stop: significant hyperkalaemia unresponsive to measures, pregnancy, bilateral renal artery stenosis, or a creatinine rise >30% that does not settle with adjustment of diuretics and volume.
DWE high-yield: The most common long-case error is stopping the ACEi because the creatinine rises 15-25%. This rise is expected and acceptable and is a sign the drug is working (lowering intraglomerular pressure). Stop only if the rise exceeds 30% or hyperkalaemia is refractory. [1]
2. SGLT2 inhibition — dapagliflozin, empagliflozin
The SGLT2 inhibitors are the single biggest advance in CKD management in the last decade. They reduce proximal tubular glucose and sodium reabsorption, restoring tubuloglomerular feedback, lowering intraglomerular pressure, and reducing albuminuria — independently of their glucose-lowering effect. [1]
- Evidence:
- CREDENCE (canagliflozin, type 2 diabetes with albuminuric CKD) — 30% reduction in kidney failure and CV death; stopped early for efficacy [5].
- DAPA-CKD (dapagliflozin, CKD with or without diabetes, eGFR 25-75 with albuminuria) — 39% reduction in the composite of sustained eGFR decline, kidney failure, or renal/CV death [3].
- EMPA-KIDNEY (empagliflozin, broad CKD population including non-diabetic and low-albuminuria patients, eGFR 20-45) — 28% reduction in progression of kidney disease or CV death, across all causes of CKD including glomerular disease [4].
- Indication: any CKD patient with eGFR ≥20 mL/min/1.73 m², regardless of cause or diabetes status. Albuminuric patients benefit most, but EMPA-KIDNEY extended the benefit to lower-albuminuria patients.
- Dosing: dapagliflozin 10 mg daily or empagliflozin 10 mg daily. Can be initiated at eGFR as low as 20 mL/min/1.73 m² and continued once started, even as eGFR falls further.
- Cautions: hold during acute illness (sick-day rules), volume depletion, or fasting (risk of euglycaemic ketoacidosis). Modest initial dip in eGFR (2-5 mL/min) is expected. Genital mycotic infections are common; rare Fournier's gangrene. No dose adjustment for the glucose effect in non-diabetics — the renoprotection is independent of glycaemia. [1]- Sick day rule: hold during acute illness, surgery, or fasting; resume once recovered.
3. Blood pressure control — the SPRINT target
Tight blood pressure control reduces both CKD progression and cardiovascular events. The KDIGO 2021 update recommended a standardised systolic blood pressure target of <120 mmHg in adults with CKD and albuminuria, based on SPRINT [8].
- SPRINT showed a 25% reduction in CV events and 27% reduction in mortality with intensive (target systolic <120 mmHg, measured by automated office BP) versus standard (<140 mmHg) control in non-diabetic high-risk patients, including a CKD subgroup [8].
- Practical target: in most CKD patients with albuminuria, target systolic <120 mmHg by standardised office measurement. Use caution in the elderly, frail, or those with postural hypotension — individualise.
- Agent choice: an ACEi or ARB is first-line in albuminuric CKD. Add a dihydropyridine calcium channel blocker (amlodipine) then a thiazide-like diuretic (chlorthalidone, indapamide) as needed. Loop diuretics replace thiazides at eGFR <30.
4. Finerenone — for diabetic CKD
A non-steroidal mineralocorticoid receptor antagonist, finerenone adds renoprotection on top of maximum-tolerated ACEi/ARB in patients with type 2 diabetes and albuminuric CKD. [1]
- FIDELIO-DKD showed an 18% reduction in the composite of kidney failure, sustained eGFR decline, or renal death, and a 14% reduction in CV events [6].
- Indication: type 2 diabetes with CKD and albuminuria (ACR >30 mg/g), already on maximum-tolerated ACEi/ARB, with eGFR ≥25 mL/min/1.73 m² and K+ <4.8.
- Dose: 10 mg or 20 mg daily, dose-adjusted by eGFR; monitor K+ at 4 weeks and each dose change. Lower hyperkalaemia burden than spironolactone.
- Caveat: do not combine finerenone with spironolactone or eplerenone — additive hyperkalaemia.
Reducing proteinuria as a therapeutic endpoint
Across all four therapies, reducing albuminuria is the surrogate marker of success. The KDIGO goal is the lowest achievable ACR with tolerated therapy. A patient who reduces their ACR from 80 to 20 mg/mmol has substantially slowed their progression and lowered their CV risk, even if the eGFR does not change. [1]
Complications and their management
Cardiovascular disease — the dominant risk
CKD is a coronary risk equivalent. A patient with stage 3b CKD is more likely to die of cardiovascular disease than reach dialysis. The risk is exponential, not linear — it begins at eGFR 60 and accelerates as function declines. The mechanisms are multiple: [1]
- Accelerated atherosclerosis — hypertension, dyslipidaemia, diabetes, inflammation
- Vascular calcification — driven by CKD-MBD (calcium-phosphate product, PTH)
- Left ventricular hypertrophy — from hypertension, volume, anaemia, AV fistula
- Heart failure — both reduced and preserved ejection fraction (HFpEF common in CKD)
- Arrhythmia — electrolyte shifts, uraemic cardiomyopathy, sudden cardiac death [1]
Management priorities: [1]
- Statin for all CKD patients ≥50 years (KDIGO lipid guideline) — atorvastatin 40-80 mg. Do not target an LDL threshold; the benefit is absolute risk reduction. In dialysis, do not initiate a statin (4D, AURORA were negative) but continue if already on one.
- Aspirin for secondary prevention; consider for primary prevention in high-risk CKD after individualised assessment.
- Blood pressure control to the SPRINT target.
- Avoid nephrotoxic contrast — use alternative imaging where possible; if contrast is essential (e.g., PCI), use the lowest dose of iso-osmolar contrast with pre-procedure hydration.
- Glycaemic control in diabetes — HbA1c 53-58 mmol/mol (7-7.5%) is reasonable; avoid over-tight control in CKD (risk of hypoglycaemia from reduced insulin clearance and changed drug pharmacokinetics). [1]
Renal anaemia — iron first, then ESA
Anaemia of CKD is typically normocytic normochromic, appears from stage 3, and is caused by EPO deficiency, uraemic inhibition of erythropoiesis, shortened red cell survival, and blood loss. Iron deficiency (absolute or functional) is almost universal in CKD and must be corrected before and during ESA therapy. [1]
Workup: exclude other causes (GI blood loss, B12/folate deficiency, haemolysis, myelodysplasia) before attributing anaemia to CKD. Check ferritin and transferrin saturation (TSAT). [1]
Step 1 — correct iron deficiency first.
- Iron targets: ferritin >100 micrograms/L and TSAT >20% (non-dialysis); ferritin >200 micrograms/L and TSAT >20% (dialysis).
- Oral iron is poorly tolerated (constipation, nausea) and poorly absorbed in CKD. IV iron (ferric carboxymaltose, ferric derisomaltose, iron polymaltose) is preferred in CKD and is more effective. Single-dose IV ferric carboxymaltose is the standard ANZ approach. [1]
Step 2 — ESA if Hb remains <100 g/L after iron repletion.
- Epoetin alfa/beta, darbepoetin alfa, or methoxy polyethylene glycol-epoetin beta (Mircera).
- Target Hb 100-110 g/L. Do NOT target >115 g/L. TREAT showed that targeting higher Hb with darbepoetin in diabetic CKD did not improve outcomes and doubled the risk of stroke [9]. The FDA and KDIGO recommend against targeting Hb >115 g/L.
- Hold ESA if Hb >115 g/L.
- Monitor BP (ESA can worsen hypertension) and iron stores regularly.
DWE exam trap: The classic MCQ asks "a 68-year-old with diabetic CKD stage 4 has Hb 96 g/L, ferritin 30, TSAT 12%. Best next step?" The answer is IV iron, not an ESA. Iron deficiency must be corrected first — ESAs are ineffective and potentially harmful in iron-deficient patients, and iron alone may correct the anaemia. [1]
CKD-MBD — the bone-mineral axis
CKD-MBD is the systemic disorder of mineral metabolism, bone, and vasculature that accompanies CKD. It begins early (stage 3) and is a major driver of vascular calcification, fracture, and mortality. [1]
Pathophysiology — the cascade: [1]
- Phosphate retention — falling GFR reduces phosphate excretion; serum phosphate rises.
- Hypocalcaemia — phosphate binds calcium, and reduced 1,25-dihydroxyvitamin D reduces gut calcium absorption.
- Secondary hyperparathyroidism (SHPT) — hypocalcaemia, hyperphosphataemia, and low calcitriol all stimulate PTH secretion; parathyroid glands hyperplasia.
- High bone turnover — osteitis fibrosa cystica from PTH-driven bone resorption.
- Vascular calcification — calcium-phosphate product drives medial calcification (Monckeberg sclerosis), stiffening arteries and raising pulse pressure.
- Tertiary hyperparathyroidism — autonomous PTH secretion after long-standing SHPT, with hypercalcaemia. [1]
Surveillance — from stage 3:
- Calcium, phosphate, PTH, 25-OH vitamin D, alkaline phosphatase — at least annually (more often as CKD advances). [1]
Management — treat the cascade, not the number: [1]
| Target | Intervention |
|---|---|
| Dietary phosphate | Dietitian referral — limit processed foods, phosphate additives; protein from low-phosphate sources. |
| Phosphate binders | Take with meals. Non-calcium binders preferred (sevelamer, lanthanum, sucroferric oxyhydroxide) to avoid calcium load and vascular calcification. Calcium-based binders (calcium acetate, calcium carbonate) are cheap but add to calcium burden and calcification risk — limit total elemental calcium intake. |
| Vitamin D | Correct 25-OH vitamin D deficiency with cholecalciferol (first step). |
| Calcitriol / vitamin D analogues | For SHPT with PTH rising despite phosphate control — calcitriol or paricalcitol. Reduce PTH but watch for hypercalcaemia and over-suppression. |
| Calcimimetics | Cinacalcet (oral) or etelcalcetide (IV, dialysis) — directly lower PTH by sensitising the calcium-sensing receptor. Used for moderate-severe SHPT, especially with hypercalcaemia. EVOLVE showed cinacalcet lowered PTH and reduced parathyroidectomy but did not significantly reduce the primary CV composite [10]. |
| Parathyroidectomy | For refractory severe SHPT with hypercalcaemia, especially when medical therapy fails or symptomatic (bone pain, fractures, pruritus, calciphylaxis). |
DWE high-yield: Avoid calcium-based phosphate binders in patients with vascular calcification or hypercalcaemia — choose sevelamer or lanthanum. Avoid over-suppressing PTH (adynamic bone disease) — target a PTH roughly 2-9 times the upper limit of normal in dialysis, not normal. [1]
Metabolic acidosis
As CKD advances, the kidney's capacity to generate bicarbonate (via ammoniagenesis) falls, producing a normal anion gap metabolic acidosis early, progressing to a high anion gap acidosis with retained organic acids in advanced CKD. Acidosis accelerates muscle wasting, worsens bone disease, and may itself accelerate progression. [1]
Management:
- Treat when serum bicarbonate <22 mmol/L (KDIGO threshold). [1]- Oral sodium bicarbonate 600 mg two to three times daily, titrated to bicarbonate 22-26 mmol/L.
- Watch for volume overload and hypertension (sodium load) — adjust other sodium intake and diuretics.
- Dietary acid reduction (plant-based protein, more fruits and vegetables) is an adjunct — but watch potassium. [1]
Hyperkalaemia
Hyperkalaemia is the common limiting factor for RAAS blockade, SGLT2i co-administration, and finerenone in CKD. It reflects reduced potassium excretion, acidosis, and often dietary load. [1]
Chronic management strategy — keep the patient on the disease-modifying drugs:
- Dietary potassium counselling — dietitian review; identify hidden sources (salt substitutes, fruit, tomatoes, chocolate, nuts).
- Correct metabolic acidosis — bicarbonate lowers K+.
- Optimise diuretics — loop and thiazide diuretics promote kaliuresis; combining a loop and thiazide is kaliuretic.
- Gastrointestinal potassium binders — patiromer or sodium zirconium cyclosilicate (SZC) — allow patients to remain on RAAS blockade despite chronic mild-moderate hyperkalaemia. These are chronic adjuncts, not emergency therapy (they take hours to days to work).
- Reduce or split doses of RAAS agents if refractory. [1]
Acute management (K+ ≥6.0 with ECG changes, or ≥6.5 regardless) is identical to AKI management — calcium gluconate, insulin-dextrose, salbutamol, and dialysis if refractory. See the hyperkalaemia and AKI topics. [1]
Dyslipidaemia
Statin for all CKD patients aged ≥50 (atorvastatin 40-80 mg). Do not initiate in dialysis (4D, AURORA showed no benefit) but continue if already on. Ezetimibe can be added for high-risk patients. The 2013 KDIGO lipid guideline replaced LDL targets with absolute risk-based therapy. [1]
Volume overload and hypertension
Loop diuretics (frusemide) become necessary at eGFR <30, where thiazides lose efficacy. Combine a loop and thiazide (e.g., frusemide plus metolazone) for refractory volume overload — sequential nephron blockade. Monitor sodium, potassium, magnesium, and volume status closely. [1]
Drug dosing in CKD
Every renally cleared drug must be dose-adjusted to the current eGFR (or measured creatinine clearance by Cockcroft-Gault), not the baseline. Key principles: [1]
| Drug class | Action in CKD |
|---|---|
| NSAIDs | Avoid entirely in CKD (afferent arteriolar vasoconstriction; AKI and progression risk). Patient education is critical — many are over-the-counter. |
| Metformin | Reduce dose at eGFR <45 (lactic acidosis risk); contraindicated at eGFR <30. |
| SGLT2 inhibitors | Initiate at eGFR ≥20; can continue once started. Hold during acute illness. |
| DOACs | Dose-adjust by eGFR and indication. Apixaban can be used down to eGFR 15 (dose-adjusted); rivaroxaban is more restricted; avoid dabigatran at eGFR <30 (renally cleared, bleeding risk). UFH is safe at any eGFR. |
| Opioids | Morphine metabolites (M6G) accumulate — prefer fentanyl or oxycodone (dose-adjusted). Avoid pethidine (norpethidine neurotoxicity). |
| Gabapentin, pregabalin | Renally cleared — dose-adjust; start low and titrate slowly. |
| Antibiotics | Vancomycin by trough/AUC; aminoglycosides extended-interval with monitoring; reduce beta-lactam frequency (not dose) to avoid neurotoxicity; nitrofurantoin and tetracycline contraindicated at eGFR <30. |
| Gadolinium contrast | Avoid in eGFR <30 (nephrogenic systemic fibrosis risk); if essential, use a macrocyclic group II agent at the lowest dose. |
| Iodinated contrast | Use only if essential at eGFR <30; pre-hydrate with isotonic saline; consider temporary RAAS blockade hold. |
| Bisphosphonates | Avoid IV bisphosphonates at eGFR <30-35 (acute tubular necrosis risk). |
Dialysis preparation and modality choice
Start dialysis preparation at eGFR <30 (stage 4) using the KFRE to time it. The goals are: informed modality choice, mature access at the time of need, and a pre-emptive transplant where possible. [1]
Vascular access — the AVF timeline
An arteriovenous fistula (AVF) requires 6-12 months to mature after creation. Plan backwards from the predicted dialysis date. [1]
- Refer for vascular surgical assessment at eGFR 15-20 mL/min/1.73 m², or earlier if rapid progression (KFRE high risk).
- AVF preferred over arteriovenous graft (AVG) and tunnelled catheter — lower infection, longer patency, lower mortality. Create in the non-dominant arm, distal (radiocephalic) first, then brachiocephalic.
- Vein preservation from the day of CKD diagnosis — no cannula or blood pressure cuff on the non-dominant arm of a predialysis patient. Educate the patient and every clinician.
- Tunnelled catheter is the last resort — high infection and stenosis risk. [1]
Modality choice — shared decision-making
| Modality | Setting | Advantages | Disadvantages |
|---|---|---|---|
| Haemodialysis (centre) | In-centre, 3x weekly | Staff supervision, social support, no home storage | Travel, fluid/diet restrictions, AVF, post-dialysis fatigue |
| Home haemodialysis | Home | Flexible schedule, more frequent, better BP and phosphate control | Training, home modification, partner strain |
| Peritoneal dialysis (PD) | Home | Needle-free, gentler, preserves residual kidney function, flexible | Catheter, peritonitis risk, glucose load, technique failure over years |
| Kidney transplant | Surgery | Best survival and quality of life for suitable candidates; pre-emptive best | Immunosuppression, rejection, donor availability, surgical risk |
ANZ context: Kidney Health Australia and the ANZDATA Registry show higher PD uptake than many countries, supported by "home-first" modality education. Pre-emptive transplant (transplant before dialysis) offers the best outcomes and should be the goal where a living donor is available. [1]
Transplant workup
Work up for transplant early — ideally before dialysis starts. Pre-emptive living-donor transplant is the gold standard. [1]
- Recipient assessment: cardiac (often coronary angiography in diabetic patients), infection screen (hepatitis B/C, HIV, CMV, EBV), immunological (blood group, HLA typing, panel-reactive antibody, crossmatch), cancer screen, psychological, social.
- Donor workup: living donor (related, unrelated, altruistic, paired exchange) or deceased donor. Living donors undergo extensive medical and psychological assessment; their long-term risk is minimised but real.
- Contraindications: active malignancy, uncontrolled infection, severe CV disease, non-adherence, active substance abuse. Age itself is not a contraindication. [1]
Conservative care pathway
For patients in whom dialysis will not extend meaningful life — typically the very elderly, the frail, those with advanced comorbidity (dementia, advanced heart failure, metastatic cancer) — a conservative (non-dialysis) care pathway is appropriate and should be offered explicitly. [1]
Conservative care is not "no care". It includes:
- Symptom-focused management (nausea, pruritus, oedema, pain, breathlessness)
- Fluid and electrolyte management (low-dose diuretics, dietary advice)
- Anaemia management (ESA to symptomatic Hb)
- Advance care planning, goals-of-care discussions, end-of-life care
- Renal palliative care involvement [1]
Prognostic tools (e.g., the Cohen surprise question, the RSC-EPI) help identify patients for whom dialysis offers little benefit. Shared decision-making, family involvement, and clear documentation are essential. [1]
Follow-up, surveillance and preventive care
| Stage | Surveillance | Action focus |
|---|---|---|
| G1-G2 (with markers) | Annual | Treat cause; RAAS if albuminuric; lifestyle |
| G3a-G3b | 6-12 monthly | Four-pillar progression therapy; CKD-MBD/anaemia; vaccinations |
| G4 | 3-6 monthly | Dialysis education; access planning; transplant workup; conservative care discussion |
| G5 | 1-3 monthly; nephrology-led | Initiate KRT or conservative care |
Preventive care: annual influenza, COVID-19, pneumococcal, hepatitis B (check titres — response reduced in CKD), herpes zoster. Permanent NSAID avoidance, contrast caution, sick-day rules in writing and reviewed every visit. Protect the non-dominant arm from cannulae from the day of diagnosis. Statin, BP, glycaemia, smoking cessation, weight, exercise, fall prevention. [1]
DCE integration — high-yield patterns
Long case — the cardiorenal-metabolic patient (68-year-old, type 2 diabetes 20 years, hypertension, ischaemic heart disease, stage 3b CKD with albuminuria). The integrated plan reconciles: diabetes (SGLT2i, GLP-1 RA, individualised HbA1c, dose-adjusted metformin); hypertension and proteinuria (ACEi/ARB to SPRINT target, add CCB then diuretic); cardiovascular protection (statin, aspirin if secondary, SGLT2i); cardiorenal overlap (SGLT2i is the bridge); CKD complications screened each visit; polypharmacy reconciliation; KFRE-based prognosis and planning. The model opening: "I will manage this patient as a whole, with the four-pillar approach to CKD, and the recognition that his cardiovascular risk is his greatest threat." [1]
Short case — AVF routine: look for needle tracks and surgical scar, feel a continuous thrill (systolic and diastolic) at the anastomosis, listen for a machinery bruit, and check for steal syndrome (cool hand, reduced radial pulse) and high-output failure. Report: "There is a functioning left brachiocephalic AVF with a continuous thrill and machinery bruit, no steal syndrome." [1]
Short case — transplant routine: look for the iliac fossa scar and Tenckhoff catheter scar, palpate the graft, listen for a graft bruit, note immunosuppression signs (cushingoid appearance, gingival hypertrophy from calcineurin inhibitors, skin cancers). General uraemic signs include pallor, scratch marks, asterixis, pericardial rub, pigmentation. [1]
Common exam traps and high-yield discriminators
- Do not diagnose CKD on a single eGFR — confirm chronicity (3 months) and exclude AKI. Prior results, kidney size, anaemia, and CKD-MBD all support chronicity.
- An ACEi-induced creatinine rise up to 30% is acceptable — do not stop the drug. This is the expected haemodynamic effect. Stop only if the rise exceeds 30% or hyperkalaemia is refractory.
- SGLT2 inhibitors are not just for diabetics — EMPA-KIDNEY extended benefit to non-diabetic CKD, including glomerular disease. A 2024 DWE MCQ is very likely to test this.
- Iron first, then ESA — never start an ESA without correcting iron deficiency. Target Hb 100-110 g/L; never >115 g/L (TREAT stroke risk). [1]5. Non-calcium phosphate binders — sevelamer, lanthanum — preferred in vascular calcification or hypercalcaemia. Calcium-based binders add to calcium burden and calcification risk.
- Cardiovascular disease is the leading cause of death in CKD — not kidney failure. Statin, BP, glycaemia, and SGLT2i are the levers.
- AVF planning begins at eGFR 15-20 — protect the non-dominant arm from day of diagnosis.
- Conservative care is a valid choice — not a failure. Offer it explicitly to frail, multi-morbid patients.
- Sick-day rules save kidneys — teach every patient to hold ACEi, ARB, SGLT2i, diuretics, metformin, and NSAIDs during acute illness.
- Race-free eGFR — use CKD-EPI 2021 (no race coefficient). Cystatin C confirms when creatinine is unreliable [2].
Sources
KDIGO 2012 CKD Guideline [1]; KDIGO 2024 CKD update; NICE NG203 (2021); CARI Guidelines; Kidney Health Australia; CREDENCE [5]; DAPA-CKD [3]; EMPA-KIDNEY [4]; FIDELIO-DKD [6]; RENAAL [7]; SPRINT [8]; TREAT [9]; EVOLVE [10]; Kidney Failure Risk Equation [11]; CKD-EPI 2021 race-free equation [2].
References
- [1]Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline Ann Intern Med, 2013.PMID 23732715
- [2]Inker LA, Eneanya ND, Coresh J, et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race N Engl J Med, 2021.PMID 34554658
- [3]Wheeler DC, Stefánsson BV, Bachtus M, et al. Dapagliflozin in Patients with Chronic Kidney Disease N Engl J Med, 2020.PMID 32970396
- [4]The EMPA-KIDNEY Collaborative Group Empagliflozin in Patients with Chronic Kidney Disease N Engl J Med, 2023.PMID 36331190
- [5]Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy N Engl J Med, 2019.PMID 30990260
- [6]Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes N Engl J Med, 2020.PMID 33264825
- [7]Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy N Engl J Med, 2001.PMID 11565518
- [8]Wright JT Jr, Williamson JD, Whelton PK, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control N Engl J Med, 2015.PMID 26551272
- [9]Pfeffer MA, Burdmann EA, Chen CY, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease N Engl J Med, 2009.PMID 19880844
- [10]EVOLVE Trial Investigators, Chertow GM, Block GA, et al. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis N Engl J Med, 2012.PMID 23121374
- [11]Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure JAMA, 2011.PMID 21482743