Phys · renal
Hypertensive Nephrosclerosis and Renovascular Disease
Also known as renal artery stenosis · RAS · renovascular hypertension · ischaemic nephropathy · fibromuscular dysplasia · FMD · atherosclerotic renal artery stenosis · hypertensive nephrosclerosis · malignant hypertension · Pickering syndrome · flash pulmonary oedema · resistant hypertension · secondary hypertension
Consultant-physician-depth guide to renovascular hypertension and hypertensive nephrosclerosis — when to hunt for secondary hypertension, renin-angiotensin physiology (one-clip vs two-clip), atherosclerotic renal artery stenosis versus fibromuscular dysplasia, the imaging sequence, the CORAL/ASTRAL evidence for medical-therapy-first, defined revascularisation subsets, malignant hypertension, and the biopsy distinction — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Hypertensive Nephrosclerosis and Renovascular Disease

The answer first
Renovascular disease is the great over-imaged and over-stented corner of hypertension. Four rules carry you through the DWE and the long-case defence [1]:
- Look for secondary hypertension with triggers, not by reflex. Young or abrupt onset, truly resistant pressure on three agents including a diuretic, severe hypertension with target-organ damage, or specific clues — a bruit, asymmetric kidneys, recurrent flash pulmonary oedema, a creatinine surge on ACEi/ARB [8] [15].
- The physiology predicts the behaviour. A unilateral stenosis is renin-driven (one-clip physiology); bilateral disease or a stenosed single kidney is volume-driven (two-clip physiology) — and that is why bilateral disease gives you flash pulmonary oedema and sodium retention while unilateral disease gives you high renin and a pressor response to blockade [16].
- For atherosclerotic disease, pills beat stents. CORAL, ASTRAL and STAR all failed to show that adding stenting to optimal medical therapy improves renal function, blood pressure or outcomes — so optimal medical therapy is the default, and revascularisation is reserved for defined subsets [1] [2] [3].
- The exceptions are the exam. Fibromuscular dysplasia in the young woman (angioplasty can cure), bilateral tight stenosis or a single functioning kidney with declining GFR, and recurrent flash pulmonary oedema — these are the patients you revascularise [6] [18].
When to look — the secondary hypertension framework
Most hypertension is essential. The skill is not screening everyone; it is recognising the phenotypes where a secondary cause is common enough to justify a hunt [15].
| Trigger | Why it matters | The cause it points to |
|---|---|---|
| Onset under age 30, especially without obesity or family history | Essential hypertension is rare here | Fibromuscular dysplasia, renal parenchymal disease, coarctation [4] |
| Abrupt onset, or sudden worsening of previously controlled pressure | A new lesion is driving it | Atherosclerotic RAS, renal infarct, scleroderma |
| Resistant hypertension — uncontrolled on three agents including a diuretic at best tolerated doses | Enriched for secondary causes; also mandates a hunt for pseudo-resistance | Primary aldosteronism (commonest), RAS, OSA, drugs [7] |
| Severe hypertension with acute target-organ damage | Malignant-phase physiology | Malignant hypertension from any cause [19] |
| Specific clues — abdominal bruit, asymmetric kidneys, flash pulmonary oedema, creatinine rise on ACEi/ARB | Point directly at the renal artery | Renovascular disease [16] |
Before any imaging, exclude pseudo-resistance: white-coat effect (get ambulatory or home readings), non-adherence (ask directly, without blame — this is the commonest finding), an inadequate regimen (no diuretic, submaximal doses), cuff artefacts, and pressor drugs — NSAIDs, the oral contraceptive, calcineurin inhibitors, sympathomimetics, liquorice [7]. The AHA scientific statement is explicit that true resistant hypertension requires all of these to be addressed first, because each is more common than renal artery stenosis [7].
The screening bloods you send on every suspected-secondary workup are cheap and high-yield: electrolytes (hypokalaemia with a non-suppressed renin suggests primary aldosteronism), creatinine with eGFR, and urinalysis with protein quantification — renal parenchymal disease is the commonest secondary cause overall. Plasma aldosterone-renin ratio, metanephrines, thyroid function and a sleep study are added according to the phenotype [8] [15].
Pathophysiology — the renin axis, one clip versus two
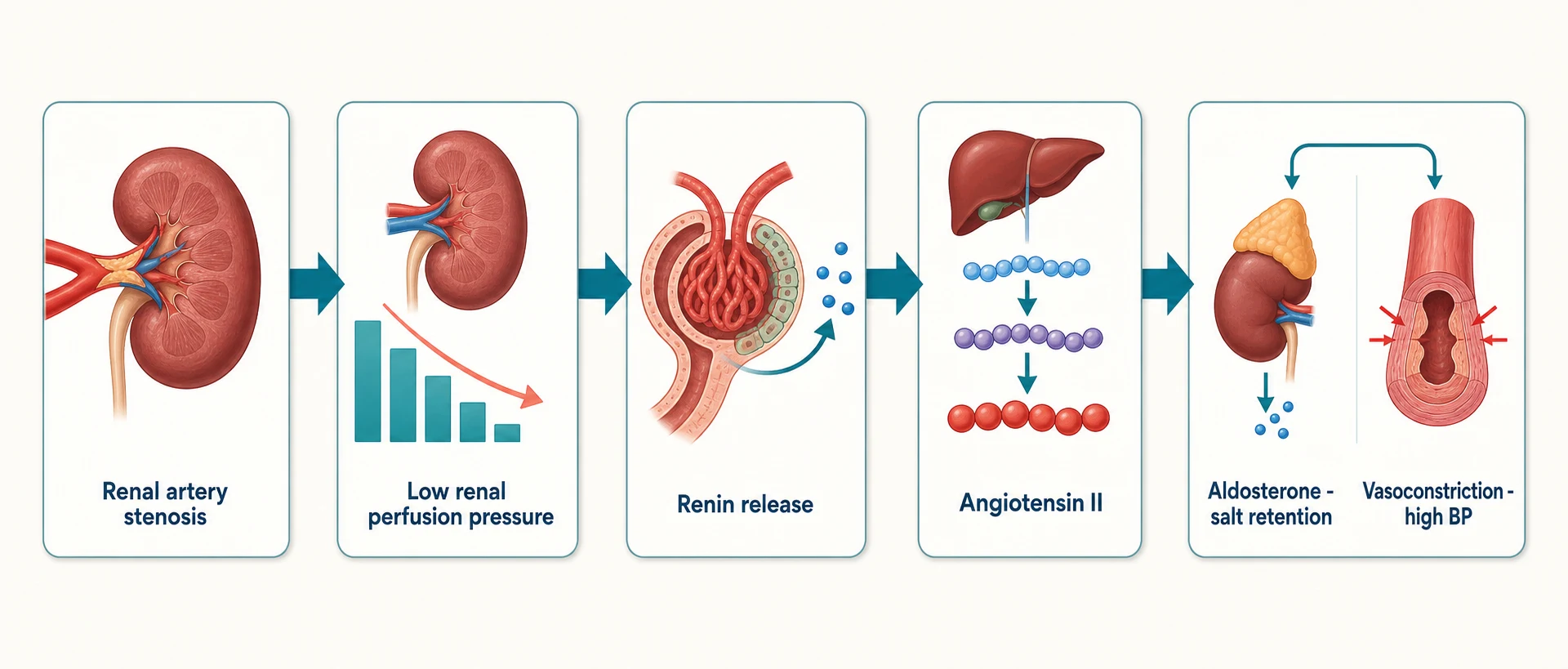
A haemodynamically significant stenosis drops perfusion pressure at the afferent arteriole. The juxtaglomerular apparatus reads this as systemic hypotension and releases renin, which generates angiotensin II — a direct vasoconstrictor and efferent-arteriolar constrictor that defends glomerular filtration pressure — and aldosterone, which retains salt and water. The hypertension is the system working as designed, against a lesion it cannot see past [16].
The Goldblatt experiments give you the two physiologies examiners want distinguished [16]:
| Model | Lesion | Driver | Plasma renin | Volume status | Response to ACEi/ARB | Response to revascularisation |
|---|---|---|---|---|---|---|
| One-clip (unilateral stenosis, contralateral kidney normal) | One renal artery clipped | Renin-dependent — angiotensin II is the pressor | High | Normal — the healthy kidney excretes the salt load | Pressure falls briskly | Often cures or markedly improves pressure |
| Two-clip (bilateral stenosis, or stenosis of a single functioning kidney) | Both arteries clipped | Volume-dependent — neither kidney can excrete sodium; renin is suppressed by the expanded volume | Low or normal | Expanded — this is the flash-pulmonary-oedema physiology | Pressure falls, but GFR may crash | Relieves the sodium retention — the subset that benefits most [18] |
Three consultant-level corollaries. First, ACEi/ARB cause a haemodynamic creatinine rise in a stenosed kidney because angiotensin II was holding the efferent arteriole tight to preserve filtration pressure; remove it and intraglomerular pressure — and GFR — fall. A rise up to about 30% is expected pharmacology, not injury, and is a clue to haemodynamically significant disease [16]. Second, in chronic atherosclerotic disease the kidney beyond the stenosis develops its own microvascular injury — rarefaction, oxidative stress and fibrosis — which is why opening the artery late does not restore the parenchyma, the central biological explanation for the negative stent trials [16]. Third, the contralateral "normal" kidney in unilateral disease is exposed to the full systemic pressure and itself sustains hypertensive damage over time [16].
The two causes you must separate
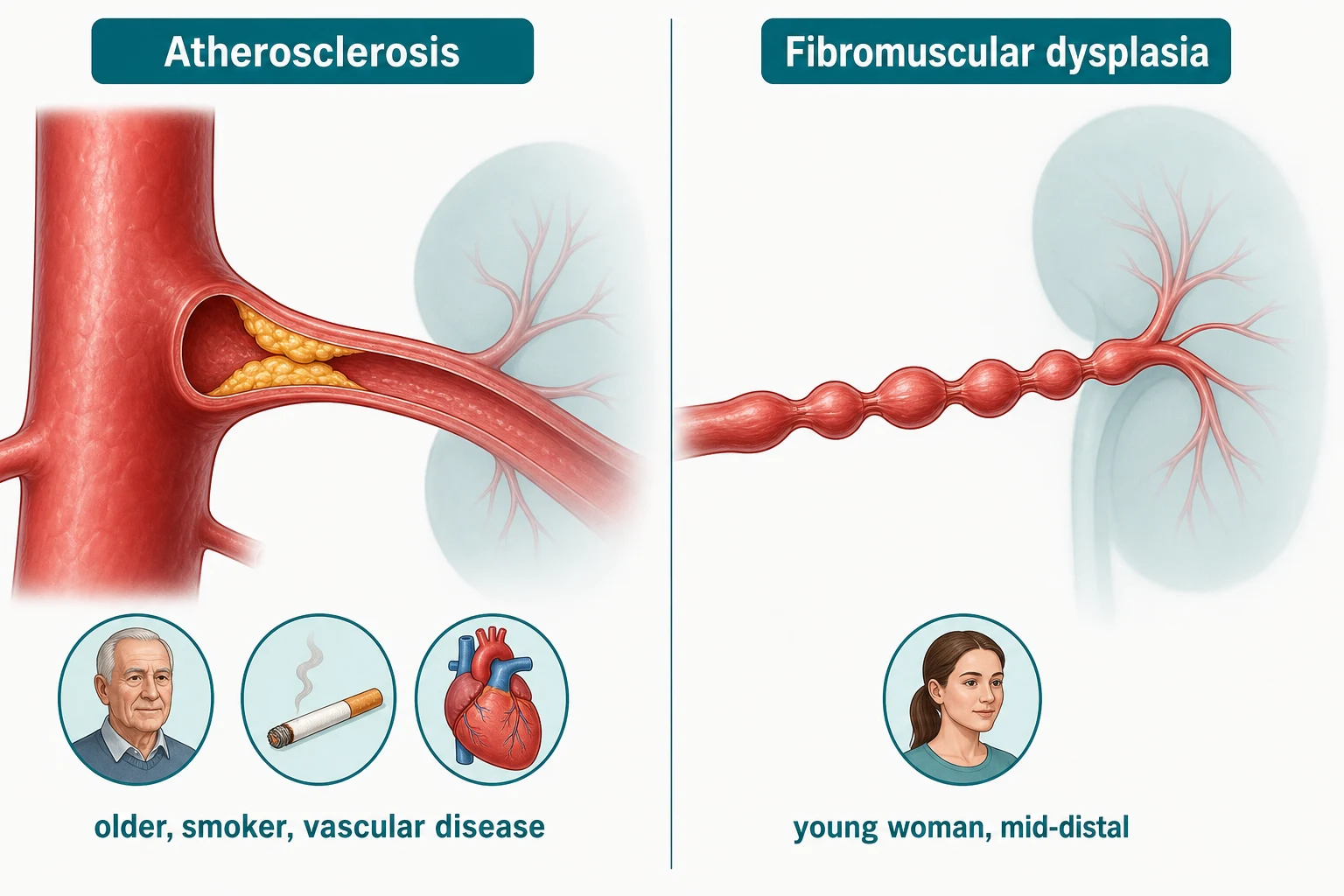
Two diseases produce almost all renovascular hypertension, and the entire clinical game is telling them apart because their management differs fundamentally [5].
| Feature | Atherosclerotic RAS (ARAS) | Fibromuscular dysplasia (FMD) |
|---|---|---|
| Patient | Older; smoker; diabetes; known coronary, peripheral or cerebrovascular disease | Young woman — median diagnosis in the 40s, overwhelmingly female in registry data [4] |
| Lesion site | Ostium and proximal third — it is aortic plaque encroaching on the renal artery | Mid-to-distal renal artery, often branch disease [5] |
| Angiographic look | Eccentric proximal narrowing | String-of-beads (multifocal FMD — alternating webs and aneurysmal outpouchings); less commonly a smooth focal tubular stenosis [4] |
| Natural history | Progressive; part of total-body atheroma — prognosis driven by cardiovascular events | Non-atherosclerotic, non-inflammatory medial disease; can dissect or aneurysm; screen other beds (cervicocephalic) [5] |
| Revascularisation | Rarely helps — OMT first (CORAL/ASTRAL) | Angioplasty without a stent — can cure or substantially improve pressure, especially in the young with short hypertension duration [6] |
| Medical therapy | Whole-body risk reduction: RAAS blockade, statin, antiplatelet, smoking cessation [1] | Antihypertensives while awaiting or if angioplasty unsuitable; antiplatelet commonly used for the arterial disease itself [5] |
The US FMD registry (first 447 patients) fixed the classic phenotype: over 90% women, hypertension the commonest presenting feature in those with renal involvement, multifocal string-of-beads the dominant lesion — and importantly, headache, pulsatile tinnitus and cervical bruits from associated cervicocephalic FMD [4]. The European consensus adds the discipline: FMD is a diagnosis made on imaging, one lesion type per arterial bed, and renal angioplasty is the treatment for hypertension driven by renal FMD — balloon only, no stent, because the lesions are webs and the results are durable [5] [6].
Clinical clues that earn the imaging request
Renovascular disease rarely announces itself directly; it accumulates circumstantial evidence. Know the clue list cold — each is a favourite DWE stem component [16]:
- Abdominal bruit — systolic-diastolic, lateralised to the renal angle; specific but insensitive, and remember aortic bruits are common in the same vascular population [16].
- Asymmetric kidney sizes — more than about 1.5 cm length difference on ultrasound; the smaller kidney is the ischaemic one, and asymmetry in a hypertensive is RAS until excluded [15].
- Creatinine rise on ACEi/ARB — a bump up to about 30% is haemodynamic and acceptable; beyond that, or a steep decline, suggests bilateral disease or a stenosed single kidney and mandates investigation [16].
- Recurrent flash pulmonary oedema with preserved ejection fraction and no ischaemic explanation — the Pickering syndrome: bilateral (or single-kidney) stenosis, sodium retention and abrupt afterload surges; the original 1988 Lancet series showed revascularisation abolished the episodes [17] [18].
- Refractory or accelerating hypertension — control lost in a previously controlled patient, or pressures escalating despite a good regimen [7].
- Unexplained atrophic kidney, or AKI on starting RAAS blockade in a vascular patient [16].
Hypertensive nephrosclerosis — the other half of the topic
Long-standing hypertension scars the kidney directly, and this is the commonest attributed cause of CKD in clinic populations — yet it remains a diagnosis of exclusion and a contested entity [21].
Benign nephrosclerosis is the slow disease of chronic moderate hypertension: hyaline arteriolosclerosis (plasma-protein deposition thickening afferent arterioles), glomerular ischaemic wrinkling and collapse, global sclerosis, and tubular atrophy with interstitial fibrosis in strips. Clinically it produces slowly declining GFR, bland urine sediment, and modest proteinuria — typically under 1 g/day — over years [21] [22].
Malignant nephrosclerosis is the vascular injury of malignant-phase hypertension: hyperplastic arteriolosclerosis — the "onion-skin" concentric laminated thickening of interlobular arteries — with fibrinoid necrosis of afferent arterioles and glomerular tuft necrosis. It presents with AKI, haematuria, active sediment and microangiopathic haemolysis in the setting of severe pressure [22]. The onion-skin lesion is the biopsy answer the DWE wants when it describes malignant hypertension kidneys [22].
| Feature | Benign nephrosclerosis | Malignant nephrosclerosis |
|---|---|---|
| Clinical setting | Years of moderate hypertension | Malignant-phase hypertension (papilloedema, acute organ damage) [19] |
| Arteriolar lesion | Hyaline arteriolosclerosis | Hyperplastic arteriolosclerosis (onion-skin) + fibrinoid necrosis [22] |
| Urine | Bland; proteinuria usually under 1 g/day | Active sediment, haematuria, heavier proteinuria |
| Course | Slowly progressive CKD | AKI, MAHA, can progress to ESKD without pressure control |
Investigation — confirm, then image, then measure
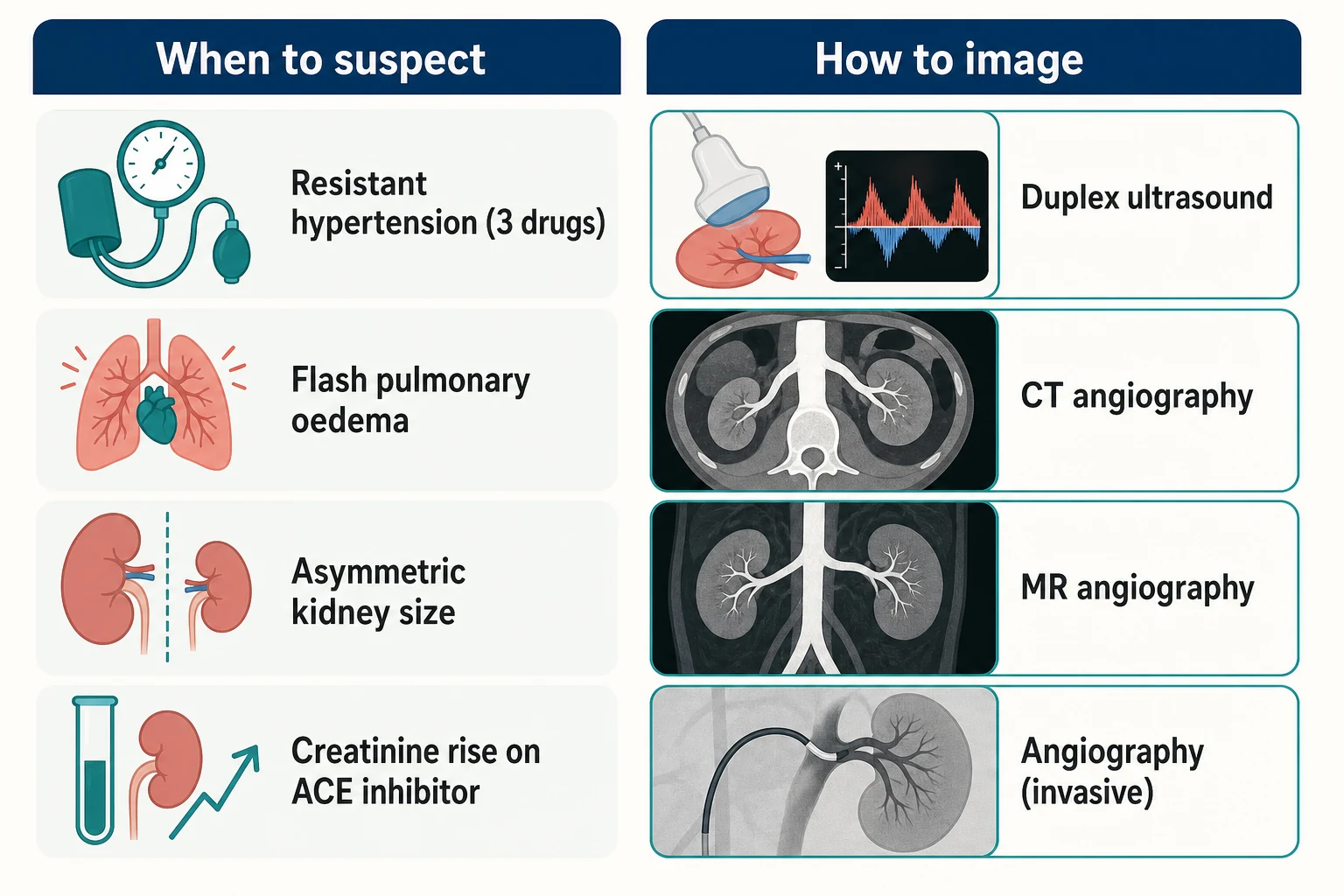
The sequence matters more than any single test: confirm true hypertension and true resistance, screen with bloods and renal ultrasound, then choose an anatomic imaging test, reserving catheter angiography for planned intervention or borderline lesions [7] [12].
| Test | Strengths | Limitations | Role |
|---|---|---|---|
| Duplex ultrasound | Cheap, safe, functional data — peak systolic velocity (about 180–200 cm/s thresholds), renal-aortic ratio, resistive indices; also gives kidney size | Operator-dependent; bowel gas, obesity; accessory arteries missed | First-line where skilled — meta-analytic accuracy is high in experienced hands [14] |
| CT angiography | Excellent spatial resolution; near-catheter accuracy in RADISH; fast; shows aortic plaque burden | Contrast nephrotoxicity in CKD; radiation | First-line anatomic test when GFR permits [13] |
| MR angiography | No iodinated contrast (gadolinium caveat below), good accuracy | Gadolinium contraindicated at low GFR (nephrogenic systemic fibrosis risk); overcalls moderate stenosis; cost, availability | Alternative to CTA, preferred in younger patients needing surveillance (FMD) [13] |
| Captopril renogram | Once the functional screening test | Poor accuracy with bilateral disease, impaired GFR, or small kidneys | Declining to historical role — do not choose it in the modern exam answer [12] |
| Catheter angiography | Gold standard anatomy plus translesional pressure gradients (resting and hyperaemic, renal FFR) for borderline lesions; same-session intervention | Invasive; contrast; atheroembolism risk | Reserved for planned revascularisation or discordant non-invasive results [16] |
The evidence behind the table: Vasbinder's 2001 meta-analysis put CTA and gadolinium MRA at the top of the accuracy hierarchy, with duplex and the captopril renogram well behind [12]; the RADISH cohort (2004) confirmed CTA/MRA near-catheter accuracy but also showed how rarely imaging changed management in unselected hypertensives — the argument for imaging only trigger-positive patients [13]; and Williams' paired analysis established the duplex thresholds and confirmed duplex's dependence on local expertise [14].
Do not forget the simple renal ultrasound that precedes all of this: kidney length and cortical thickness. A kidney under about 8 cm with a thin cortex is chronically damaged — revascularising it rarely recovers function, whatever the artery looks like [16].
Management — pills first, stents for the chosen few
The trial evidence, in the order examiners expect it
| Trial | Population | Comparison | Result | What it changed |
|---|---|---|---|---|
| STAR (2009) | ARAS with impaired renal function | Stent + medical therapy vs medical therapy | No benefit in renal function; excess periprocedural harm including deaths | First modern signal that stenting stable disease is futile and not benign [3] |
| ASTRAL (2009) | ARAS with substantial stenosis, physician uncertainty | Revascularisation + medical therapy vs medical therapy | No benefit in renal function, BP, renal events or mortality; serious periprocedural complications | Shifted default to medical therapy for the uncertain majority [2] |
| CORAL (2014) | ARAS with stenosis over 60% plus hypertension or CKD, on defined OMT | Stent + OMT vs OMT alone | No difference in the composite of cardiovascular/renal events, mortality or BP | The definitive trial — stenting adds nothing on top of modern OMT for most [1] |
The criticisms you should volunteer — they show consultant balance: all three trials enrolled patients in whom clinicians were uncertain, excluding the very subsets (flash pulmonary oedema, rapidly declining GFR, bilateral tight lesions) most likely to benefit; ASTRAL in particular randomised many with mild disease. So the honest conclusion is not "never stent" but "stenting unselected atherosclerotic disease adds harm without benefit — select" [1] [2].
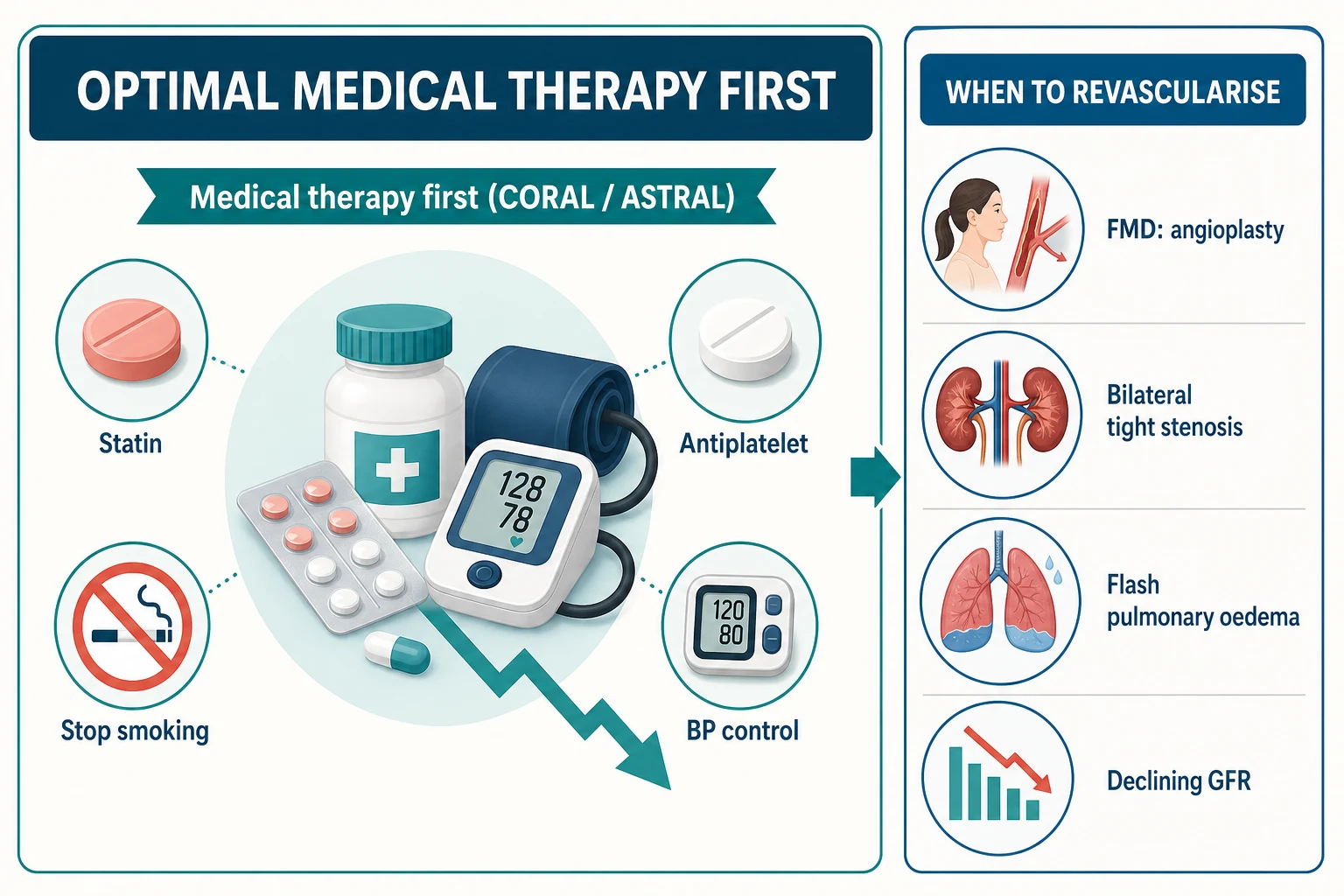
Optimal medical therapy — what it actually is
OMT in CORAL was a protocol, not a shrug, and your answer should sound like one [1]:
- RAAS blockade is first-line even in RAS. ACEi/ARB are the most effective agents in renin-driven hypertension and carry cardiovascular and renal protection; monitor creatinine and potassium at 1–2 weeks — accept a creatinine rise up to about 30% as haemodynamic, investigate beyond it. The caution is bilateral disease or a single stenosed kidney, where blockade can collapse GFR — even then it is dose-adjusted and monitored, not automatically banned, unless function deteriorates [16] [9].
- Add a calcium-channel blocker and a thiazide-like diuretic to reach target; move to a loop diuretic as GFR falls [7].
- Treat the atheroma, not just the artery: high-intensity statin, antiplatelet therapy, smoking cessation, diabetic control — the same package as any established cardiovascular disease, because ARAS patients die of myocardial infarction and stroke, not of their renal artery [11].
- BP target: individualised intensive control — SPRINT supports lower targets in high-risk non-diabetic patients, and KDIGO 2021 recommends a standardised-office SBP under 120 in CKD where tolerated [10] [9].
The revascularisation subsets — where you DO intervene
The exam answer is a list, and the list is short [16]:
- Fibromuscular dysplasia — balloon angioplasty without stent; the meta-analysis shows high technical success with hypertension cure or improvement in a large fraction, best in the young with short hypertension duration [6].
- Recurrent flash pulmonary oedema (Pickering syndrome) — revascularisation abolishes episodes in bilateral disease [17] [18].
- Bilateral tight stenosis, or stenosis of a single functioning kidney, with declining GFR — the two-clip physiology where relieving the lesion relieves the sodium retention [16].
- Selected cases of rapidly deteriorating renal function with a tight lesion and preserved kidney size, after honest multidisciplinary discussion that the trial evidence does not cover this phenotype [11].
The ESC/ESVS guideline frames it identically: balloon angioplasty (with provisional stent for complications) is reasonable in FMD and in the defined haemodynamic subsets; routine stenting of atherosclerotic ostial lesions on top of medical therapy is not recommended [11].
Malignant hypertension — when the pressure itself is the emergency
Malignant hypertension is severe hypertension with acute bilateral retinal haemorrhages, exudates or papilloedema, usually with microangiopathic haemolysis and acute kidney injury — a hypertensive emergency, not a number [19]. It has not disappeared: contemporary series describe a young, often male, frequently under-investigated population with high rates of secondary causes — including renovascular disease — and substantial subsequent ESKD [19].
The vascular pathology is a feed-forward loop: pressure exceeds autoregulation, arterioles suffer endothelial damage (the onion-skin and fibrinoid lesions of malignant nephrosclerosis), natriuresis triggers renin release, and pressure climbs further [22]. Underlying triggers to screen for once the patient is safe: renal artery stenosis, primary aldosteronism, phaeochromocytoma, scleroderma renal crisis, and drug withdrawal (clonidine) or sympathomimetics [19] [20].
The lowering rule is the DWE number: reduce mean arterial pressure by no more than about 20–25% in the first hour, then toward about 160/100 over the next 2–6 hours, and normalise over 24–48 hours. Faster falls drop patients off the right-shifted autoregulation curve and precipitate cerebral, coronary and renal ischaemia — the exam's favourite iatrogenic catastrophe [20].
| Agent | Class | Notes for the exam |
|---|---|---|
| Nicardipine | IV dihydropyridine CCB | Titratable, predictable; common first-line [20] |
| Labetalol | Combined alpha/beta blocker | Titratable infusion; avoid in decompensated heart failure, severe asthma [20] |
| Glyceryl trinitrate | Venodilator | Best when acute pulmonary oedema or coronary ischaemia dominates |
| Sodium nitroprusside | Direct arteriolar/venodilator | Potent but cyanide toxicity with prolonged use or renal impairment — know it, rarely start it [20] |
| Fenoldopam / urapidil / hydralazine | Alternatives by local availability | Hydralazine is unpredictable — avoid for tight control targets [20] |
Oral therapy is for hypertensive urgency (severe pressure without acute organ damage) — restart or up-titrate the patient's agents and arrange close follow-up; do not admit for IV control, and do not crash the pressure with sublingual nifedipine, which belongs to the hall of historical errors [20].
DCE angles — how this topic is actually examined
The long case is the 66-year-old with resistant hypertension whose creatinine has drifted up on ramipril plus indapamide, found to have a 70% left renal artery stenosis on CTA. The examiner's question — "the vascular surgeon has offered to stent it; what do you think?" — is the CORAL defence. Your structure: confirm true resistance (adherence, ambulatory readings, diuretic in the regimen), quantify the haemodynamic significance (kidney sizes, the trajectory of the creatinine, whether the rise stayed within the accepted range), then state the trial position and your selection criteria. Bonus depth: distinguish renin-dependent from volume-dependent physiology, name the stent subsets, and close with the vascular-risk package that actually changes his prognosis [1] [7] [16].
The short case is the hypertension examination. Perform it as a target-organ survey with secondary-cause detection built in: correct cuff technique on both arms; fundi graded from silver wiring and AV nipping through flame haemorrhages to papilloedema; precordium for the displaced apex and fourth sound of LVH; auscultate for renal bruits over the aorta and both renal angles; palpate for ballotable kidneys; check radiofemoral delay and all peripheral pulses (coarctation, diffuse atheroma); finish with fluid status and ankle oedema. Present the findings as a synthesis — "grade 2 hypertensive retinopathy, LVH, a right renal bruit and 1.5 cm renal asymmetry on last ultrasound; I would investigate for renovascular disease" — not as a list [8] [15].
Exam traps, collected
References
- [1]Cooper CJ, Murphy TP, Cutlip DE, et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis N Engl J Med, 2014.PMID 24245566
- [2]ASTRAL Investigators, Wheatley K, Ives N, et al. Revascularization versus medical therapy for renal-artery stenosis N Engl J Med, 2009.PMID 19907042
- [3]Bax L, Woittiez AJ, Kouwenberg HJ, et al. Stent placement in patients with atherosclerotic renal artery stenosis and impaired renal function: a randomized trial Ann Intern Med, 2009.PMID 19414832
- [4]Olin JW, Froehlich J, Gu X, et al. The United States Registry for Fibromuscular Dysplasia: results in the first 447 patients Circulation, 2012.PMID 22615343
- [5]Persu A, Giavarini A, Touzé E, et al. European consensus on the diagnosis and management of fibromuscular dysplasia J Hypertens, 2014.PMID 24842696
- [6]Trinquart L, Mounier-Vehier C, Sapoval M, et al. Efficacy of revascularization for renal artery stenosis caused by fibromuscular dysplasia: a systematic review and meta-analysis Hypertension, 2010.PMID 20625080
- [7]Carey RM, Calhoun DA, Bakris GL, et al. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association Hypertension, 2018.PMID 30354828
- [8]Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines Hypertension, 2018.PMID 29133356
- [9]Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease Kidney Int, 2021.PMID 33637192
- [10]SPRINT Research Group, Wright JT Jr, Williamson JD, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control N Engl J Med, 2015.PMID 26551272
- [11]Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS) Eur Heart J, 2018.PMID 28886620
- [12]Vasbinder GB, Nelemans PJ, Kessels AG, et al. Diagnostic tests for renal artery stenosis in patients suspected of having renovascular hypertension: a meta-analysis Ann Intern Med, 2001.PMID 11560453
- [13]Vasbinder GB, Nelemans PJ, Kessels AG, et al. Accuracy of computed tomographic angiography and magnetic resonance angiography for diagnosing renal artery stenosis Ann Intern Med, 2004.PMID 15520423
- [14]Williams GJ, Macaskill P, Chan SF, et al. Comparative accuracy of renal duplex sonographic parameters in the diagnosis of renal artery stenosis: paired and unpaired analysis AJR Am J Roentgenol, 2007.PMID 17312071
- [15]Viera AJ, Neutze DM Diagnosis of secondary hypertension: an age-based approach Am Fam Physician, 2010.PMID 21166367
- [16]Textor SC Current approaches to renovascular hypertension Med Clin North Am, 2009.PMID 19427501
- [17]Pickering TG, Herman L, Devereux RB, et al. Recurrent pulmonary oedema in hypertension due to bilateral renal artery stenosis: treatment by angioplasty or surgical revascularisation Lancet, 1988.PMID 2900930
- [18]Messerli FH, Bangalore S, Makani H, et al. Flash pulmonary oedema and bilateral renal artery stenosis: the Pickering syndrome Eur Heart J, 2011.PMID 21406441
- [19]Shantsila A, Lip GYH Malignant hypertension: not quite an obsolete diagnosis yet J Hypertens, 2019.PMID 30640869
- [20]Varon J The diagnosis and treatment of hypertensive crises Postgrad Med, 2009.PMID 19179809
- [21]Meyrier A Nephrosclerosis: a term in quest of a disease Nephron, 2015.PMID 25871843
- [22]Marcantoni C, Fogo AB A perspective on arterionephrosclerosis: from pathology to potential pathogenesis J Nephrol, 2007.PMID 17918136
- [23]Marcantoni C, Ma LJ, Federspiel C, et al. Hypertensive nephrosclerosis in African Americans versus Caucasians Kidney Int, 2002.PMID 12081576
- [24]Genovese G, Friedman DJ, Ross MD, et al. Association of trypanolytic ApoL1 variants with kidney disease in African Americans Science, 2010.PMID 20647424