Phys · renal
Kidney Transplantation
Also known as renal transplantation · kidney transplant · renal allograft · deceased donor transplant · living donor transplant · pre-emptive transplant · delayed graft function · acute rejection · antibody-mediated rejection · chronic allograft nephropathy · interstitial fibrosis and tubular atrophy · post-transplant lymphoproliferative disorder · new-onset diabetes after transplant · panel reactive antibody
Consultant-physician-depth guide to kidney transplantation — the indications (ESKD from any cause, refer for workup once the eGFR is below 20), the donor types (deceased donor DBD versus DCD, living donor, pre-emptive), the contraindications and workup, the immunosuppression regimen (induction with basiliximab or anti-thymocyte globulin; maintenance tacrolimus plus mycophenolate plus steroid), the surgical and medical complications (rejection classified by mechanism, the infection timeline, malignancy including PTLD and skin cancer, CNI nephrotoxicity, recurrent disease, NODAT, cardiovascular disease), and pregnancy after transplant. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Kidney Transplantation

The answer first
Kidney transplantation is the treatment of choice for end-stage kidney disease (ESKD) from any cause: it improves survival, quality of life and cost-effectiveness compared with dialysis, and it does so for almost every recipient who has no absolute contraindication [1]. The single rule that prevents the most missed opportunities in clinical practice: refer every patient with chronic kidney disease to a transplant unit for workup once the eGFR falls below 20 mL/min/1.73 m2. A pre-emptive transplant — performed before the patient starts dialysis — gives the best graft and patient survival of all, because the recipient has not yet accumulated the vascular, infective and nutritional burden of time on dialysis [2].
The organising principle for the whole topic, the one sentence a candidate can repeat under viva pressure: transplantation trades the disease of kidney failure for the controlled disease of immunosuppression. Every management decision — induction, maintenance, biopsy, infection prophylaxis, malignancy surveillance, pregnancy, drug interaction — is a re-balancing of that single trade-off: enough immunosuppression to prevent rejection, little enough to avoid infection, malignancy and toxicity. [1]

DWE high-yield: The triad of tacrolimus plus mycophenolate plus prednisolone is the global standard maintenance regimen. The SYMPHONY study established tacrolimus-based low-dose regimens as the best balance of efficacy and nephrotoxicity [5]. Know the regimen, the levels, the toxicities and the interactions cold — they generate more MCQs than any other part of the topic.
Indications — who gets transplanted
Any patient with end-stage kidney disease is a potential candidate. The cause of ESKD does not by itself exclude a patient, but it does shape the workup and the recurrent-disease risk. The common causes of ESKD leading to transplant, in approximate descending frequency in ANZ practice, are diabetic kidney disease, glomerulonephritis (especially IgA nephropathy), hypertension and vascular disease, polycystic kidney disease, reflux nephropathy, and autoimmune disease (lupus nephritis, ANCA vasculitis). [1]
The referral threshold is an eGFR below 20 mL/min/1.73 m2, endorsed by the KDIGO candidate guideline [3]. The reasons are practical: the workup takes three to six months (cardiac assessment, cancer screening, infection screening, immunological workup, psychosocial evaluation, donor evaluation), and the goal is to transplant pre-emptively — before dialysis — wherever a living donor is available. Wolfe's landmark study showed that, although there is a short-term mortality risk in the peri-operative period, the long-term survival of transplant recipients substantially exceeds that of patients who remain on the waiting list on dialysis [1], and Hariharan's cohort analysis showed the survival advantage has grown over time [2].
DCE trap: Late referral to a transplant unit — after the patient has already started dialysis — is one of the most common and most preventable failures of nephrology care. A patient who arrives at the transplant clinic on dialysis with a central venous catheter, no cardiac workup and no donor evaluation has lost the chance at a pre-emptive graft and faces a longer, riskier wait. [1]
Why pre-emptive transplant is best
A pre-emptive transplant (performed before dialysis) gives the best survival because it avoids the cardiovascular, infectious and nutritional consequences of dialysis itself. Time on dialysis is an independent predictor of worse graft and patient survival — each year on dialysis before transplant measurably shortens the graft lifespan. This is why living-donor transplantation, which can be planned and timed, is so powerful: the recipient is transplanted at the optimum moment. [1]
Donor types — know the classification and what it predicts
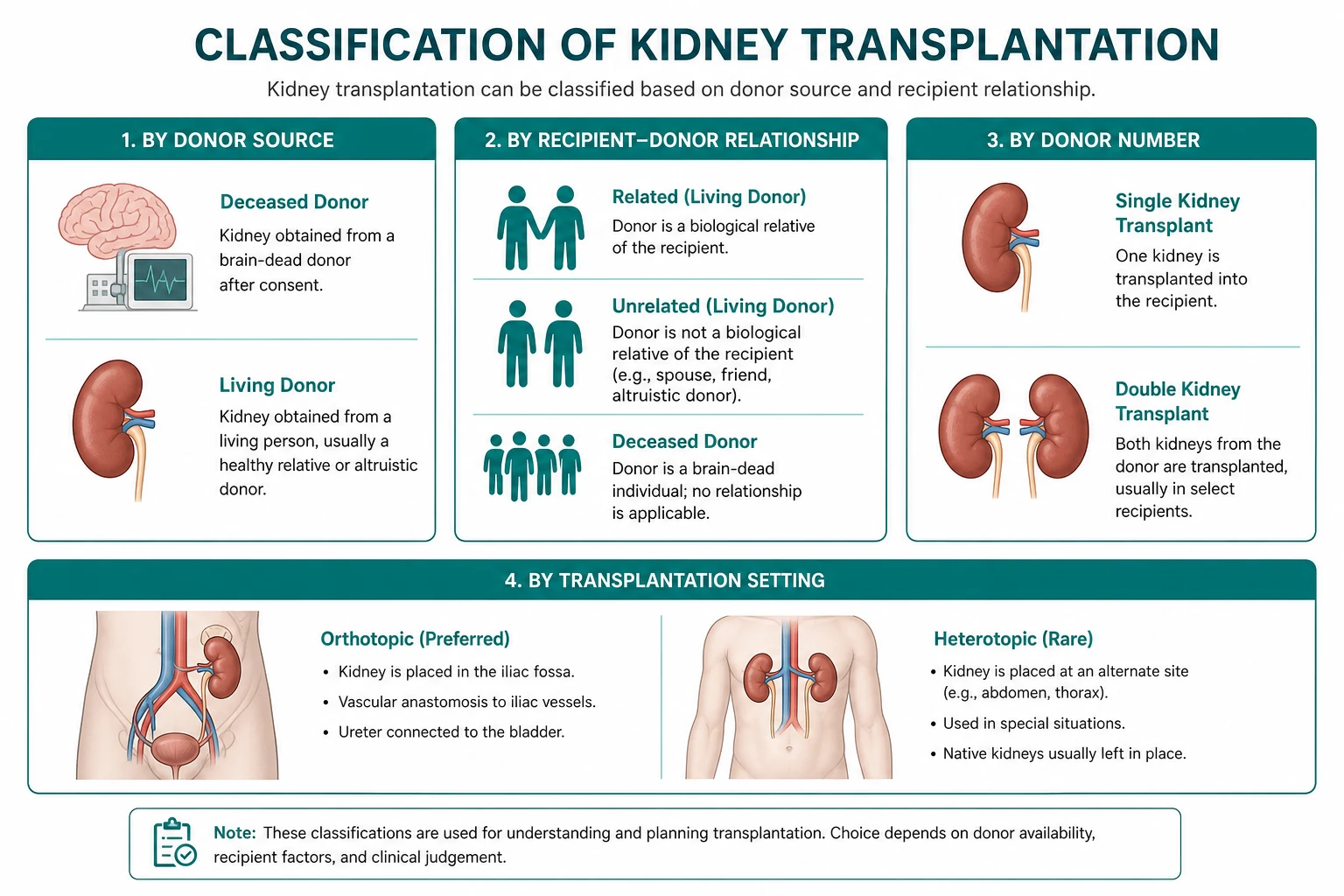
| Donor type | Definition | Graft survival | Key points |
|---|---|---|---|
| Living donor (related or unrelated) | A healthy person donates a kidney electively | Best (15 to 20 years median) | Planned, short cold ischaemia, healthy kidney; unrelated donors do nearly as well as related |
| Deceased donor after brain death (DBD) | Donation after brain-stem death, heart beating | Good (10 to 15 years) | Minimal warm ischaemia; the standard deceased-donor kidney |
| Deceased donor after circulatory death (DCD) | Donation after cardiac death following withdrawal of care | Acceptable, slightly lower early | More delayed graft function; long-term survival approaches DBD |
| Extended-criteria donor (ECD) | Older donor (above 60, or 50 to 59 with hypertension, stroke or elevated creatinine) | Lower | Used to expand the donor pool; informed consent on expected graft survival |
The two distinctions an examiner expects you to articulate: DBD versus DCD (the heart is beating in DBD, so warm ischaemia is minimal; in DCD the heart has stopped, so there is a period of warm ischaemia before retrieval, which increases delayed graft function but does not substantially harm long-term survival in modern practice), and living versus deceased (a living-donor kidney is healthy, retrieved under ideal conditions with minimal cold ischaemia, and gives the best survival — which is why a living unrelated donor does almost as well as a living related donor, the HLA match being less important than the quality of the kidney and the timing of the operation). [1]
DWE high-yield: The single most important factor in deceased-donor graft survival is donor age, followed by HLA-DR matching and cold ischaemia time. The single most important factor overall is living versus deceased donation. A living donor kidney outperforms every deceased-donor category. [1]
Contraindications — who is not a candidate
| Absolute contraindications | Relative contraindications |
|---|---|
| Active malignancy (within 2 to 5 years, depending on type) | BMI above 35 (surgical risk, delayed healing) |
| Uncontrolled infection | Poorly controlled psychiatric illness |
| Severe uncorrectable cardiovascular disease | Active peptic ulcer disease |
| Active substance abuse | Limited life expectancy from non-renal disease |
| Life-limiting comorbidity | Heavy smoking (must counsel cessation) |
| Inability to adhere to immunosuppression | Older age with frailty (not age alone) |
The cardinal teaching point: age alone is not a contraindication. A physiologically fit 70-year-old can do very well; a frail 60-year-old with severe vascular disease cannot. The KDIGO candidate guideline stresses a patient-centred, individualised assessment rather than a rigid age cut-off [3].
The adherence point deserves emphasis. Non-adherence is the leading modifiable cause of graft loss, especially in adolescents and young adults. A patient who cannot reliably take twice-daily tacrolimus for the life of the graft will lose the graft and is not, at that point, a re-transplant candidate until the adherence problem is sustainably resolved. This is an ethical as well as a clinical judgement. [1]
The transplant workup
The workup runs in parallel streams. It takes months, which is why early referral matters. [1]
Immunological assessment
- ABO blood group — the first barrier. ABO-incompatible transplant is possible but requires desensitisation (rituximab, plasmapheresis, IVIG) and carries a higher rejection risk.
- HLA typing — the recipient's HLA-A, HLA-B and HLA-DR (plus C, DQ, DP) antigens. DR matching has the strongest effect on graft survival.
- Panel reactive antibody (PRA) — the proportion of the population against whom the recipient has pre-formed anti-HLA antibodies, generated by pregnancy, transfusion or prior transplant. A high PRA means a longer wait and a higher rejection risk.
- Crossmatch — recipient serum tested against donor lymphocytes. A positive crossmatch is an absolute contraindication to transplant because it causes hyperacute rejection. A virtual crossmatch using single-antigen bead assays predicts compatibility from a distance and is central to national allocation. [1]
Cardiac assessment
Cardiovascular disease is the leading cause of death with a functioning graft, so cardiac clearance is rigorous. Most centres perform an echocardiogram and a functional stress test (stress echo or myocardial perfusion scan); high-risk patients (diabetic, older, known coronary disease) undergo coronary angiography with revascularisation as needed. [1]
Cancer screening
Transplantation accelerates malignancy, so occult cancer must be excluded before listing. Age-appropriate screening (colorectal, breast, cervical, prostate) plus a careful history and examination. A recent cancer is an absolute contraindication; the waiting period after curative treatment depends on the tumour type (commonly 2 to 5 years). [1]
Infection screening
A comprehensive infection screen: hepatitis B and C (with viral loads if positive, because controlled HBV and HCV are not contraindications and are treated before transplant), HIV (no longer a contraindication with modern antiretroviral therapy), CMV and EBV serostatus (the D+/R- mismatch is the highest-risk combination for CMV disease and PTLD respectively), tuberculosis (interferon-gamma release assay or tuberculin skin test, with treatment of latent TB before immunosuppression), syphilis, toxoplasma, and strongyloides in endemic populations. A dental review excludes septic foci. Urological assessment (cystoscopy, urodynamics where indicated) ensures the bladder will accept the ureteric anastomosis. [1]
DWE high-yield: The serostatus pairings an examiner expects you to know: CMV D+/R- is the highest-risk combination for CMV disease (prophylaxis or pre-emptive therapy required); EBV D+/R- is the highest-risk combination for PTLD (some centres avoid this pairing in high-intensity regimens). HIV, hepatitis B and hepatitis C are no longer absolute contraindications with modern therapy. [1]
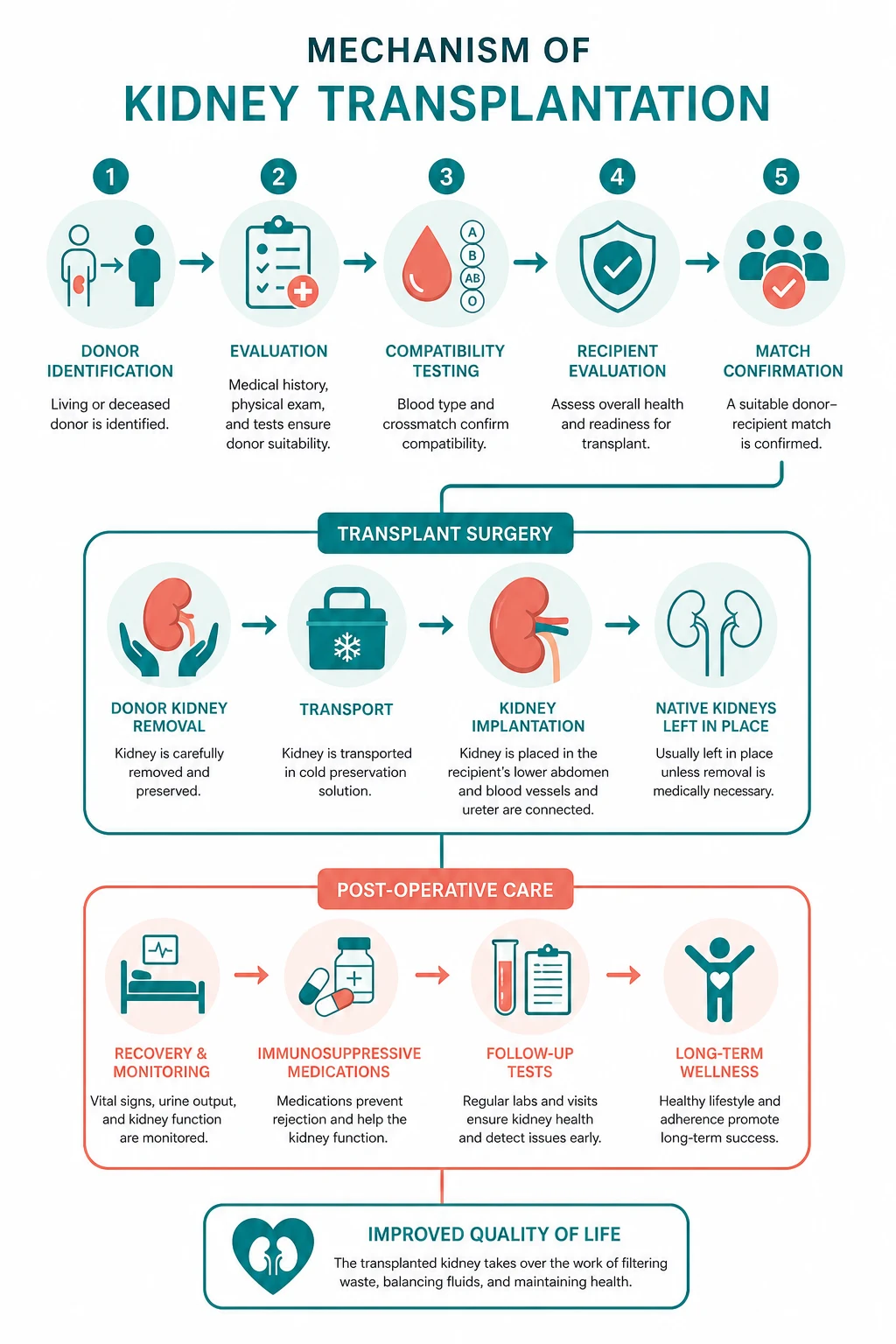
Immunosuppression — the regimen you must know cold
The standard regimen is induction followed by triple maintenance therapy. The logic is layered: induction provides potent cover during the peri-operative period when the immune system first sees the new antigens; maintenance provides long-term balance. [1]
Induction
- Basiliximab — a chimeric monoclonal antibody to the interleukin-2 receptor (CD25) on activated T cells. It is the standard for low to moderate immunological risk because it is non-depleting, has few side effects, and reduces acute rejection. Nashan's trial showed a substantial reduction in biopsy-proven acute rejection at 6 months (29.8 per cent with basiliximab versus 44.0 per cent with placebo) [4].
- Anti-thymocyte globulin (rabbit polyclonal, ATG) — a broadly T-cell-depleting antibody used for high immunological risk (sensitised recipients, re-transplants, DCD donors, African-American ethnicity in US practice). Side effects are cytokine release, serum sickness, leucopenia, thrombocytopenia, and a higher long-term infection and malignancy risk that is dose-related.
Maintenance — the triple therapy
The global standard is tacrolimus plus mycophenolate plus prednisolone. The SYMPHONY study randomised patients to standard-dose ciclosporine, low-dose ciclosporine, low-dose tacrolimus, or low-dose sirolimus, all with mycophenolate and steroid; the low-dose tacrolimus arm gave the best renal function, the lowest acute rejection rate, and the best graft survival at one year [5], establishing tacrolimus as the standard calcineurin inhibitor.
| Agent | Class | Mechanism | Key toxicities | Monitoring |
|---|---|---|---|---|
| Tacrolimus | Calcineurin inhibitor | Binds FKBP-12, inhibits calcineurin, reduces IL-2 transcription | Nephrotoxicity, tremor, diabetes, hypertension, alopecia, hyperkalaemia | Trough 5 to 10 early, lower long-term |
| Mycophenolate | Antimetabolite | Inhibits IMPDH, blocks lymphocyte purine synthesis | Diarrhoea, marrow suppression, teratogenicity | FBC; not level-monitored routinely |
| Prednisolone | Corticosteroid | Broad anti-inflammatory and immunosuppressive | Diabetes, osteoporosis, hypertension, cataracts, infection | Taper to maintenance 5 mg by 3 months |
Alternatives and when to use them
- Ciclosporin — the original calcineurin inhibitor, now second-line to tacrolimus because of more nephrotoxicity, hirsutism, gum hypertrophy and hypertension; still used in pregnancy (more data than tacrolimus in some centres) and when tacrolimus is not tolerated.
- mTOR inhibitors (sirolimus, everolimus) — bind FKBP-12 and inhibit the mammalian target of rapamycin, blocking T- and B-cell proliferation. They are used to spare calcineurin inhibitors (reduce nephrotoxicity) and to lower skin cancer risk (a major advantage in patients with recurrent non-melanoma skin cancer). Their limiting toxicities are impaired wound healing (avoid for at least one month post-operatively), dyslipidaemia, proteinuria, mouth ulcers, interstitial pneumonitis and marrow suppression.
- Belatacept — a co-stimulation blocker (CTLA4-Ig) that is an alternative to calcineurin inhibitors, with less nephrotoxicity, lower blood pressure and a better cardiovascular profile, but a higher early acute rejection rate and a PTLD risk in EBV-seronegative recipients (it is contraindicated in EBV-seronegative patients).
- Azathioprine — the predecessor to mycophenolate, less potent but safe in pregnancy (mycophenolate is teratogenic and must be switched to azathioprine before conception). [1]
Surgical complications
| Complication | When | Presentation | Management |
|---|---|---|---|
| Renal artery or vein thrombosis | First hours to days | Abrupt fall in urine output, pain, falling haemoglobin, graft tenderness | Surgical emergency — urgent Doppler or CT angiography, immediate exploration |
| Renal artery stenosis | Weeks to months | Hypertension, rising creatinine, graft bruit, flash pulmonary oedema | Angiography, angioplasty with or without stenting |
| Ureteric leak | First days to weeks | Falling urine output, pain, peri-graft collection, rising creatinine | Nephrostomy, stent, surgical repair |
| Ureteric stenosis | Months to years | Rising creatinine, hydronephrosis on ultrasound | Nephrostomy, balloon dilatation or surgical repair |
| Lymphocoele | Weeks to months | Graft compression, ipsilateral leg swelling, infection | Percutaneous drainage, marsupialisation if recurrent |
| Wound infection or dehiscence | First weeks | Wound breakdown, discharge | Higher risk with diabetes, obesity, sirolimus; antibiotics, surgical review |
DWE high-yield trap: Renal artery thrombosis presents in the first hours to days with abrupt anuria, pain and a falling haemoglobin, and it is a surgical emergency. Graft loss occurs within hours without exploration. Never attribute early anuria to ATN until vascular thrombosis has been excluded by Doppler. [1]
Rejection — classification by mechanism

Rejection is classified by mechanism and timing. The classification drives the treatment, so the biopsy is not optional — it is the pivot on which management turns. [1]
| Type | Timing | Mechanism | Histology | Treatment |
|---|---|---|---|---|
| Hyperacute | Minutes to hours | Pre-formed donor-specific antibodies (positive crossmatch) | Neutrophilic glomerular thrombi, graft infarction | Prevention (never transplant across a positive crossmatch); graft nephrectomy usually needed |
| Acute T-cell mediated (TCMR) | Days to weeks (can recur) | Recipient T cells recognise donor HLA | Tubulitis, interstitial inflammation, intimal arteritis (Banff grades) | Pulse IV methylprednisolone; ATG if steroid-resistant |
| Antibody-mediated (AMR) | Any time | Donor-specific antibodies activate complement on endothelium | Microvascular inflammation (glomerulitis, peritubular capillaritis), C4d in peritubular capillaries | Plasmapheresis, IVIG, rituximab; bortezomib if refractory |
| Chronic allograft injury (interstitial fibrosis and tubular atrophy) | Months to years | Multifactorial (chronic AMR, CNI toxicity, recurrent disease, hypertension) | Interstitial fibrosis, tubular atrophy, vascular changes | Optimise immunosuppression, control blood pressure, address reversible factors |
The Banff classification and the death of "chronic allograft nephropathy"
The Banff schema is the international consensus on allograft pathology. A critical point that examiners love: the term "chronic allograft nephropathy" was formally eliminated at the Banff 2005 meeting because it was non-specific — it lumped together chronic antibody-mediated rejection, calcineurin inhibitor toxicity, hypertension and recurrent disease under one vague label [6]. The modern term is interstitial fibrosis and tubular atrophy (IFTA), graded I to III by the percentage of fibrosed cortex (6 to 25 per cent, 26 to 50 per cent, more than 50 per cent), with the instruction to identify the specific cause whenever possible.
DWE high-yield: If you are asked "what is the leading cause of long-term graft loss?", the answer is chronic allograft injury (IFTA), a multifactorial endpoint driven by chronic antibody-mediated rejection, calcineurin inhibitor nephrotoxicity, recurrent disease and hypertension. If you are asked "what is the most common cause of graft loss overall?", the answer is death with a functioning graft — most often cardiovascular. [1]
Diagnosing rejection — the workup of a rising creatinine
A rising creatinine in a transplant recipient is not "probably rejection, give steroids". It is a structured differential that ends, in most cases, with a biopsy. The pathway: [1]
- History — adherence (the commonest hidden cause), recent changes in medication (especially tacrolimus-interacting drugs), infections, diarrhoea (which alters drug absorption), new symptoms.
- Examination — graft tenderness (a red flag), fever, fluid status, blood pressure.
- Bloods — tacrolimus trough level, full blood count, eGFR, electrolytes, BK virus PCR (if beyond one month), CMV PCR (if high risk), donor-specific antibodies.
- Urine — spot protein-to-creatinine ratio, culture, and in some centres urinary chemoattractant and inflammatory markers.
- Imaging — ultrasound with Doppler to exclude obstruction (hydronephrosis) and vascular thrombosis, and to assess graft perfusion.
- Biopsy — the gold standard. The Banff grade determines whether the treatment is steroids (TCMR), plasmapheresis and IVIG (AMR), reduction of immunosuppression (BK nephropathy), or modification of the regimen (CNI toxicity). [1]
The infection timeline — the highest-yield single page

The infection timeline is the framework that organises almost every post-transplant fever. Learn it cold. [1]
| Period | Infection profile | Examples |
|---|---|---|
| Month 0 to 1 | Nosocomial and donor-derived | Wound infection, urinary tract infection, line-related bacteraemia, donor-derived infection (sepsis, viral) |
| Month 1 to 6 | Opportunistic (immunosuppression at its peak) | BK virus nephropathy, CMV disease, Pneumocystis jirovecii pneumonia, fungal infection (Aspergillus, Cryptococcus), reactivation of latent TB |
| Beyond 6 months | Community-acquired, with ongoing opportunistic risk proportional to immunosuppression | Community respiratory and urinary infections, plus late opportunistic infection if intensification for rejection |
BK virus nephropathy
BK polyomavirus reactivates under calcineurin-inhibitor-based immunosuppression, typically between month 1 and 6. The 2024 international consensus guideline recommends screening plasma BK viral load monthly for the first 9 months, then every 3 months to 2 years [8]. A persistently high viral load (above 10,000 copies/mL) predicts nephropathy. The diagnosis is confirmed on biopsy (viral inclusions in tubular epithelial cells, with immunohistochemistry). The management is reduction of immunosuppression — reduce mycophenolate first, then tacrolimus. Current guidelines do not support cidofovir, leflunomide, fluoroquinolones or IVIG, which have no proven benefit and real toxicity [8].
DWE high-yield trap: BK nephropathy is a clinical chameleon — it presents as a rising creatinine with viral inclusions on biopsy, and it can coexist with acute rejection. The lesson: screen BK viral load in any rising creatinine beyond one month, and biopsy before assuming rejection, because treating BK as rejection (more immunosuppression) makes it dramatically worse. [1]
CMV disease
Cytomegalovirus is the most important viral opportunistic infection in the first 3 to 6 months, especially in the D+/R- mismatch. It presents as a syndrome (fever, malaise, leucopenia, thrombocytopenia) or with tissue-invasive disease (colitis, pneumonitis, hepatitis, retinitis). The third international consensus guideline recommends either universal prophylaxis with valganciclovir for 3 to 6 months in D+/R- pairs, or pre-emptive therapy guided by weekly CMV PCR for the first 12 weeks [7]. Treatment of established disease is intravenous ganciclovir (or oral valganciclovir for mild disease), with reduction of immunosuppression.
Pneumocystis jirovecii pneumonia
Rare with prophylaxis but lethal without it. Co-trimoxazole prophylaxis is given for the first 6 to 12 months (and during any rejection treatment that intensifies immunosuppression). It presents with fever, dyspnoea, a dry cough and a disproportionate hypoxia with diffuse bilateral infiltrates. [1]
Malignancy after transplant
Immunosuppression impairs immune surveillance of oncogenic viruses and of tumour antigens, producing a distinctive malignancy profile. [1]
- Non-melanoma skin cancer is the most common post-transplant malignancy. Squamous cell carcinoma is 65 to 100 times more common than in the general population (a striking and much-tested figure), related to HPV and ultraviolet light. Annual dermatological review and rigorous sun protection are mandatory. Recurrent or high-risk skin cancers are an indication to switch from a calcineurin inhibitor to an mTOR inhibitor, which has anti-tumour activity.
- Post-transplant lymphoproliferative disorder (PTLD) is an EBV-driven B-cell proliferation that ranges from benign hyperplasia to aggressive lymphoma. It is most common in EBV-seronegative recipients (typically children and young adults) and usually presents in the first year. The first step in management is reduction of immunosuppression, which alone can induce regression in early EBV-positive disease; rituximab (anti-CD20) and chemotherapy are used for progressive or EBV-negative disease [9].
- Kaposi sarcoma (HHV-8 driven) and other virus-associated cancers are increased; solid-organ cancers are moderately increased.
DCE high-yield: When a transplant recipient presents with a new lymphadenopathy, fever or extranodal mass, think PTLD. Send EBV viral load, image, biopsy the lesion, and reduce the immunosuppression in consultation with the transplant unit and haematology. Do not simply add antibiotics. [1]
Calcineurin inhibitor nephrotoxicity
Tacrolimus and ciclosporin cause renal injury through two mechanisms: acute afferent arteriolar vasoconstriction (reversible, dose-related, presents as a rising creatinine that falls when the dose is reduced) and chronic arteriolar hyalinosis with striped interstitial fibrosis (irreversible, the long-term cost of CNIs). The chronic form overlaps with chronic allograft injury on biopsy. Management is dose minimisation (the rationale for low-dose tacrolimus regimens) and, where toxicity dominates, conversion to an mTOR inhibitor or belatacept. [1]
Recurrent disease
Some primary diseases recur in the graft and can cause graft loss. [1]
| Disease | Recurrence risk | Presentation |
|---|---|---|
| Focal segmental glomerulosclerosis (FSGS) | 30 to 50 per cent, often early | Heavy proteinuria within days to weeks; plasmapheresis for recurrence |
| IgA nephropathy | Common histologically (up to 50 per cent), clinically significant in a minority | Haematuria and proteinuria years after transplant |
| Diabetic kidney disease | Universal histologically over time | Slowly progressive proteinuria and decline over years |
| Membranous nephropathy | 10 to 30 per cent | Nephrotic-range proteinuria |
| Primary hyperoxaluria | High, and catastrophic | Early graft loss; combined liver-kidney transplant is the solution |
DWE high-yield: The disease with the most feared and earliest recurrence is FSGS, which can recur within hours to days of transplant with nephrotic-range proteinuria, treated with plasmapheresis (a circulating permeability factor is implicated). The disease that mandates a combined liver-kidney transplant is primary hyperoxaluria (the liver is the source of the oxalate). [1]
New-onset diabetes after transplant (NODAT)
NODAT is common — it complicates 15 to 30 per cent of transplants — and it matters because it accelerates cardiovascular disease and impairs graft survival. The main drivers are tacrolimus and corticosteroids, with contributions from obesity, hepatitis C, older age and certain genetic polymorphisms. Diagnosis is by fasting glucose and HbA1c, typically at 3 to 6 months and then annually. Management is diet, metformin (if the eGFR permits), and insulin as needed; in difficult cases, conversion from tacrolimus to ciclosporin or belatacept can be considered. The broader point: cardiovascular disease is the leading cause of death with a functioning graft, so aggressive cardiovascular risk factor modification (blood pressure below 130/80, statin for almost all, smoking cessation, glycaemic control) is central to long-term management. [1]
Pregnancy after transplant
Pregnancy is reasonable in a stable recipient, but it must be planned. The criteria: at least 1 to 2 years after transplant, stable graft function (creatinine below 150 micromol/L, proteinuria below 500 mg per day), blood pressure controlled below 140/90, and no recent rejection. [1]
The critical pharmacology point: mycophenolate is teratogenic (the mycophenolate embryopathy) and must be switched to azathioprine at least 6 weeks before conception. Tacrolimus is continued (trough levels fall in pregnancy because of expanded volume and increased clearance, so the dose often needs to increase). Prednisolone is continued at the lowest effective dose. Management is shared between obstetric medicine, nephrology and the transplant unit. Expected complications include a higher rate of pre-eclampsia, gestational diabetes, preterm delivery and fetal growth restriction. Delivery is usually planned at 36 to 37 weeks. [1]
DWE high-yield trap: A transplant recipient planning pregnancy who is still taking mycophenolate is a medication error waiting to happen. The switch to azathioprine with a 6-week washout is non-negotiable and is one of the most tested transplant pharmacology facts. [1]
The long-case shape
A transplant recipient in the DCE long case is a gift for the candidate who is organised. The patient has a transplant scar, an immunosuppression regimen, a set of metabolic complications, a surveillance agenda, and a story that touches nephrology, immunology, infectious diseases, cardiology, oncology and obstetric medicine. Structure the presentation: [1]
- Opening statement (SASPOP) — the patient, the graft (donor type, date, regimen), the presenting problem.
- Problem list — graft function and immunosuppression; cardiovascular risk; infection and malignancy surveillance; metabolic complications (diabetes, hypertension, bone disease); the original disease and recurrence risk; adherence and psychosocial factors.
- Integrated plan — for each problem, the monitoring, the drug levels, the surveillance interval, and the guideline anchor.
- Insight — the trade-off between rejection and immunosuppression, the leading role of cardiovascular disease in mortality, and the lifelong nature of the commitment. [1]
Regional guideline anchoring
- ANZ primary: Kidney Health Australia, the Australian and New Zealand Society of Nephrology (ANZSN), the Transplantation Society of Australia and New Zealand (TSANZ), and the ANZDATA Registry, which reports national transplant outcomes annually.
- UK secondary: the British Transplantation Society guidelines and the National Institute for Health and Care Excellence guidance on renal transplantation.
- US tertiary: KDIGO (the global standard), the American Society of Transplantation, and the Organ Procurement and Transplantation Network (OPTN) allocation policy. [1]
The standard maintenance regimen (tacrolimus plus mycophenolate plus prednisolone) is the same across ANZ, UK and US practice. Regional deltas exist mainly in donor pool and allocation (Australia has a strong living-donor and ABO-incompatible programme; the US uses the kidney allocation system with priority for sensitised patients; the UK uses a points-based national matching scheme). [1]
Key references and guideline bodies
The anchor evidence: Wolfe's survival study [1]; Hariharan's improved graft survival cohort [2]; the KDIGO candidate guideline [3]; Nashan's basiliximab trial [4]; the SYMPHONY study of tacrolimus-based regimens [5]; the Banff 2005 meeting report [6]; the third international CMV consensus [7]; the second international BK polyomavirus consensus [8]; and the Taylor PTLD review [9]. The governing guideline bodies in ANZ are KDIGO, ANZSN, TSANZ and the ANZDATA Registry; in the UK, the British Transplantation Society and NICE; in the US, KDIGO, the American Society of Transplantation and OPTN.
References
- [1]Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant N Engl J Med, 1999.PMID 10580071
- [2]Hariharan S, Johnson CP, Bresnahan BA, Taranto SE, McIntosh MJ, Stablein D Improved graft survival after renal transplantation in the United States, 1988 to 1996 N Engl J Med, 2000.PMID 10699159
- [3]Chadban SJ, Ahn C, Axelrod DA, et al. KDIGO Clinical Practice Guideline on the Evaluation and Management of Candidates for Kidney Transplantation Transplantation, 2020.PMID 32301874
- [4]Nashan B, Moore R, Amlot P, Schmidt AG, Abeywickrama K, Soulillou JP Randomised trial of basiliximab versus placebo for control of acute cellular rejection in renal allograft recipients. CHIB 201 International Study Group Lancet, 1997.PMID 9652559
- [5]Ekberg H, Tedesco-Silva H, Demirbas A, et al. Reduced exposure to calcineurin inhibitors in renal transplantation N Engl J Med, 2007.PMID 18094377
- [6]Solez K, Colvin RB, Racusen LC, et al. Banff '05 Meeting Report: differential diagnosis of chronic allograft injury and elimination of chronic allograft nephropathy ('CAN') Am J Transplant, 2007.PMID 17352710
- [7]Kotton CN, Kumar D, Caliendo AM, et al. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation Transplantation, 2018.PMID 29596116
- [8]Kotton CN, Hirsch HH, Razonable RR, et al. The Second International Consensus Guidelines on the Management of BK Polyomavirus in Kidney Transplantation Transplantation, 2024.PMID 38605438
- [9]Taylor AL, Marcus R, Bradley JA Post-transplant lymphoproliferative disorders (PTLD) after solid organ transplantation Crit Rev Oncol Hematol, 2005.PMID 15979320