Phys · renal
Nephrolithiasis
Also known as kidney stones · renal calculi · ureteric colic · renal colic · urolithiasis · calcium oxalate stone · struvite stone · infection stone · staghorn calculus · uric acid stone · cystine stone · brushite stone · nephrocalcinosis · enteric hyperoxaluria · cystinuria
Consultant-physician-depth guide to nephrolithiasis — stone types (calcium oxalate, calcium phosphate, uric acid, struvite, cystine), epidemiology, risk factors, pathophysiology (Randall plaque, supersaturation), clinical presentation of renal colic, investigation strategy (non-contrast CT KUB, ultrasound, metabolic evaluation), acute management (NSAIDs, medical expulsive therapy, ESWL, ureteroscopy, PCNL), prevention (fluid, diet, thiazides, citrate, allopurinol), and systemic associations. Structured for FRACP DWE and DCE, MRCP, and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Nephrolithiasis
The answer first
Nephrolithiasis (kidney stones) is a common condition with a lifetime risk of approximately 10 per cent, a male-to-female ratio of 2:1, and a recurrence rate of about 50 per cent at 10 years without preventive measures [7]. Stone formation occurs when urinary solutes — calcium, oxalate, uric acid, cystine, or struvite — exceed their solubility product (supersaturation), leading to crystal nucleation, growth and retention [1].
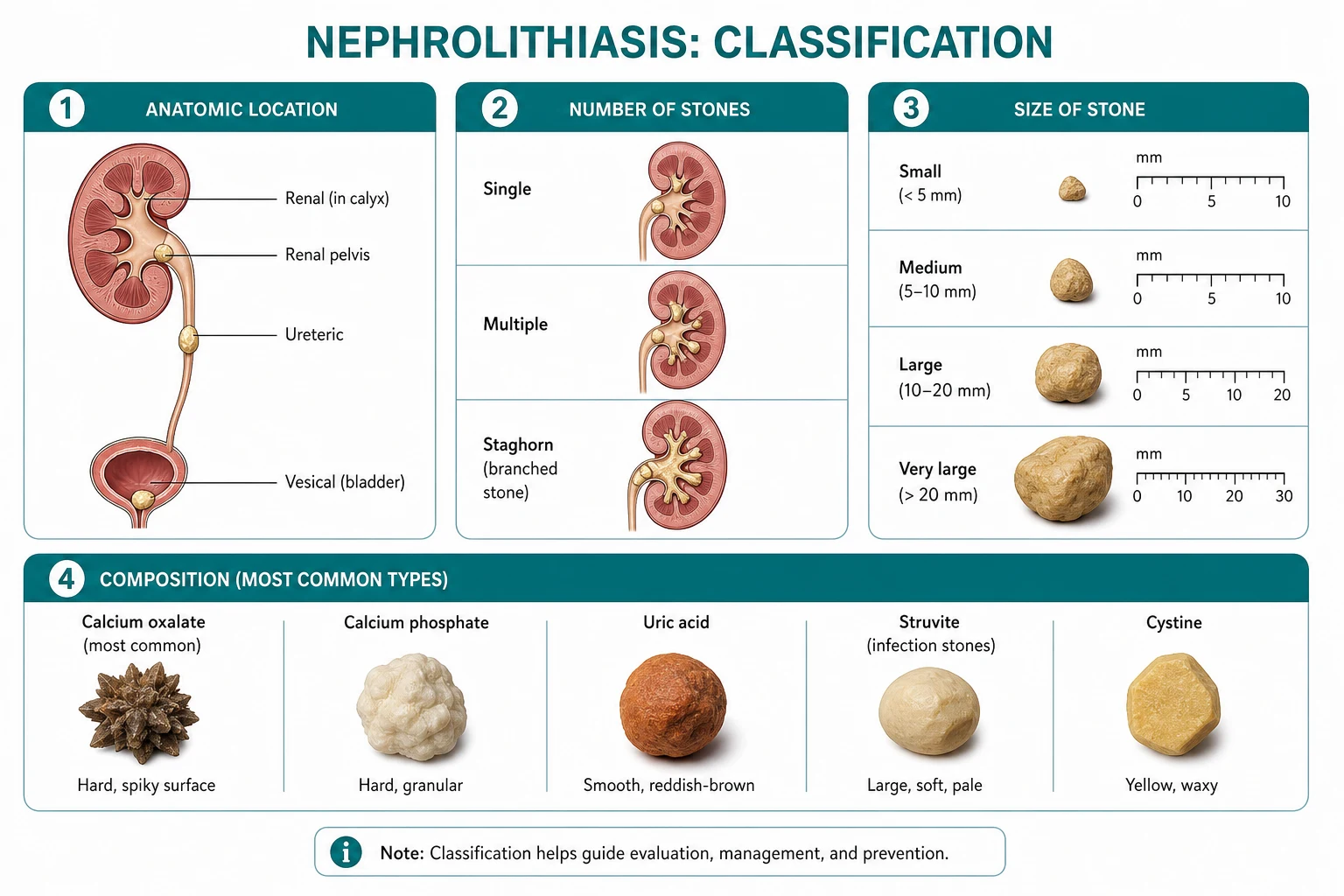
The five major stone types and their key features: [1]
| Stone type | Frequency | Radiograph | Urine pH | Key association |
|---|---|---|---|---|
| Calcium oxalate | ~75 per cent | Radiopaque | Variable | Hypercalciuria, hyperoxaluria, hypocitraturia |
| Calcium phosphate (brushite) | 5 to 10 per cent | Radiopaque | High (alkaline) | Distal RTA, hyperparathyroidism |
| Uric acid | 5 to 10 per cent | Radiolucent | Low (acidic) | Gout, myeloproliferative, low urine pH |
| Struvite (Mg ammonium phosphate) | 5 to 15 per cent | Radiopaque | High (alkaline) | Proteus, urease-producing organisms, staghorn |
| Cystine | 1 to 2 per cent | Faintly opaque | Low | Cystinuria (autosomal recessive), hexagonal crystals |
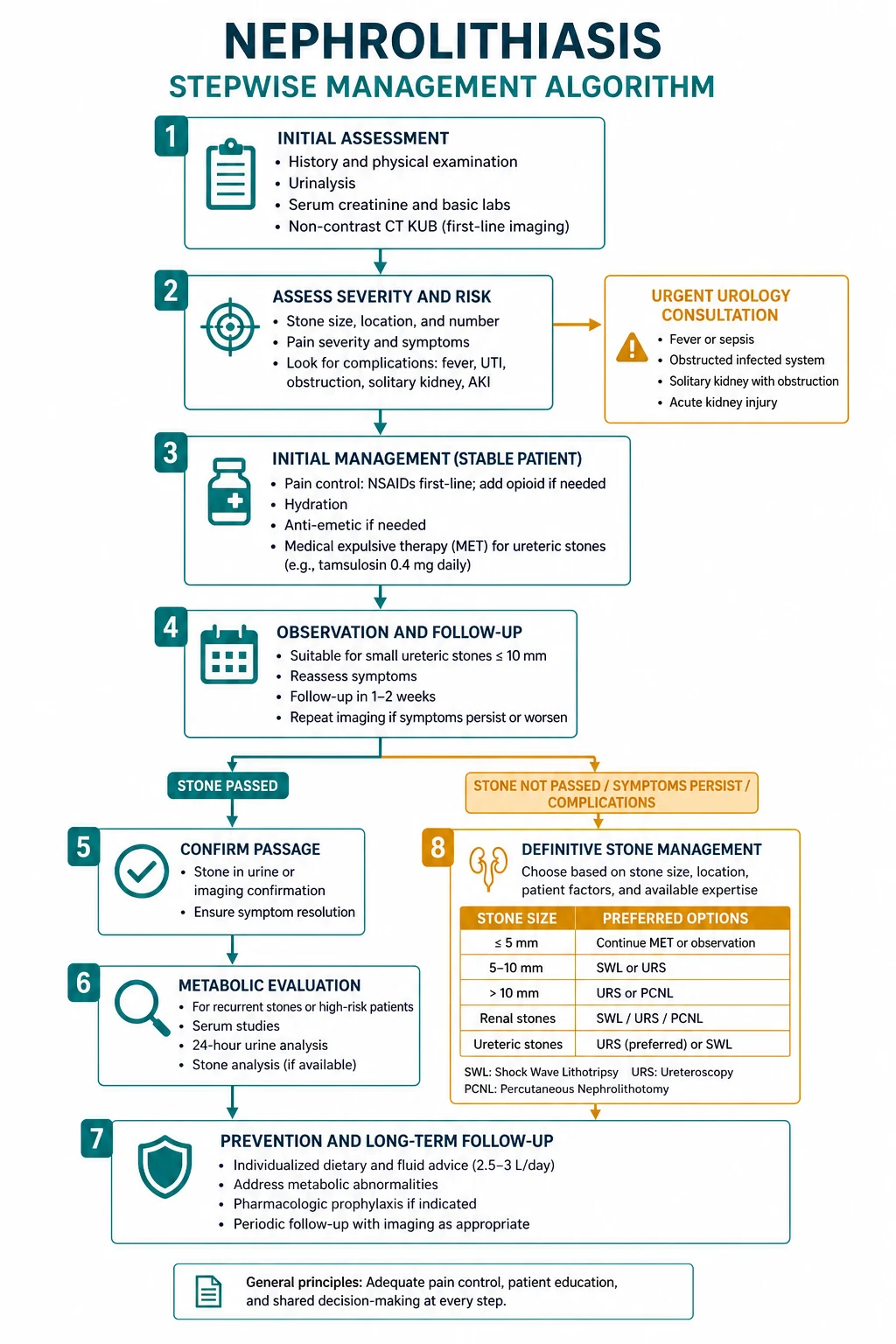
The management mandate: [1]
- Acute renal colic — NSAIDs first-line (diclofenac IM), fluids if dehydrated, antiemetics.
- Assess stone size — below 5 mm passes spontaneously in about 80 per cent; above 10 mm unlikely to pass.
- Medical expulsive therapy — tamsulosin for selected larger distal ureteric stones (contested evidence).
- Intervention when needed — ESWL (stones below 2 cm), ureteroscopy with laser, PCNL (large or staghorn).
- Urgent decompression — obstructed pyelonephritis, AKI from bilateral obstruction or solitary kidney.
- Prevent recurrence — fluid above 3 L/day, normal calcium, reduced sodium and protein, targeted pharmacotherapy. [1]
The single most important exam principle: a low-calcium diet is wrong. Normal calcium intake reduces stone risk because calcium binds intestinal oxalate. The Borghi 2002 NEJM trial proved this definitively [2].
Epidemiology

Kidney stones affect approximately 1 in 11 people in developed countries, with a lifetime risk of about 10 per cent [7]. Key epidemiological features:
- Sex: Male-to-female ratio is approximately 2:1, though the gap is narrowing (likely due to rising obesity and dietary changes in women).
- Age: Peak incidence is 20 to 50 years; stones in children or the elderly warrant aggressive metabolic evaluation.
- Recurrence: Without prevention, approximately 50 per cent of stone formers will recur within 10 years [7]. This recurrence rate is the justification for metabolic evaluation and preventive therapy.
- Rising prevalence: Linked to the metabolic syndrome, obesity, diabetes, hypertension, and dietary patterns (high sodium, high fructose, low water intake).
DWE high-yield: The epidemiological triad — 10 per cent lifetime risk, 2:1 male predominance, 50 per cent recurrence at 10 years — is a classic DWE recall question. [1]
Stone types
Calcium oxalate — the commonest stone (75 per cent)
Calcium oxalate is by far the most common stone type, accounting for approximately 75 per cent of all kidney stones. It is radiopaque, can form at any urine pH, and has the classic envelope-shaped crystal on microscopy. [1]
Risk factors:
- Hypercalciuria (the single most common metabolic abnormality — defined as above 4 mmol/kg/day in women or above 7.5 mmol/day in men on a normal diet) [1]- Hyperoxaluria (dietary: spinach, nuts, chocolate, tea; enteric: Crohn disease, short bowel, bariatric surgery)
- Hypocitraturia (citrate is the main inhibitor of calcium crystal growth — low citrate from chronic diarrhoea, distal RTA, hypokalaemia)
- High dietary sodium (sodium increases urinary calcium excretion)
- High animal protein (acid load increases calcium excretion and reduces citrate)
- Low urine volume [1]
Calcium phosphate (brushite) — 5 to 10 per cent
Calcium phosphate stones form in alkaline urine (pH above 7.0) and are strongly associated with distal (type 1) renal tubular acidosis and primary hyperparathyroidism. They are radiopaque and tend to be harder than calcium oxalate, making ESWL less effective. [1]
Exam point: If a stone former has persistently alkaline urine (pH above 7.0) with calcium phosphate stones, think distal RTA — check serum bicarbonate and potassium. Hypocitraturia from RTA drives the stones; treatment is potassium citrate. [1]
Uric acid — 5 to 10 per cent — radiolucent
Uric acid stones are radiolucent — they are not visible on plain radiographs but are seen on CT. They form in acidic urine (pH below 5.5) because uric acid is insoluble at low pH. [1]
Risk factors:
- Persistently acidic urine (chronic diarrhoea, ileostomy — loss of bicarbonate)
- Gout and hyperuricaemia
- Myeloproliferative disorders (high cell turnover — leukaemia, lymphoma, myeloma)
- Tumour lysis syndrome
- High dietary purine intake [1]
Key management difference: Uric acid stones can be dissolved by alkalinising the urine to pH 6.5 to 7.0 with potassium citrate — unlike calcium stones, which cannot be dissolved chemically. This is a classic exam point. [1]
Struvite — infection stones — 5 to 15 per cent
Struvite (magnesium ammonium phosphate) stones are caused by urease-producing organisms, most classically Proteus mirabilis (also Klebsiella, Pseudomonas, Staphylococcus saprophyticus, and some Proteus species). Urease hydrolyses urea to ammonia, raising urine pH above 7.2 and precipitating magnesium ammonium phosphate. [1]
Key features:
- Form staghorn calculi — large branching stones that fill the renal collecting system
- Alkaline urine (pH above 7.5) with persistent infection
- Can destroy the kidney through pyonephrosis, xanthogranulomatous pyelonephritis, and progressive renal failure
- Antibiotics alone are insufficient — the stone must be completely removed (typically PCNL) to eradicate the infection nidus [1]
DWE trap: The exam question will give recurrent UTIs with Proteus, an alkaline urine, and a staghorn calculus. The answer is struvite stone from urease-producing organism. The treatment is complete surgical removal (PCNL), not antibiotics alone. [1]
Cystine — 1 to 2 per cent — inherited
Cystinuria is an autosomal recessive defect in the proximal tubular transporter for cystine and dibasic amino acids (SLC3A1 or SLC7A9 genes). Cystine is poorly soluble at physiological pH (solubility increases only above pH 7.5). [1]
Key features:
- Presents in childhood or adolescence with recurrent stones
- Hexagonal crystals on urine microscopy
- Faintly radiopaque stones (sulfur content)
- Very hard stones — ESWL is often ineffective
- Management: massive fluid intake (above 4 L/day), alkalinisation to pH above 7.5, and chelation with tiopronin or D-penicillamine for refractory cases [1]
Pathophysiology
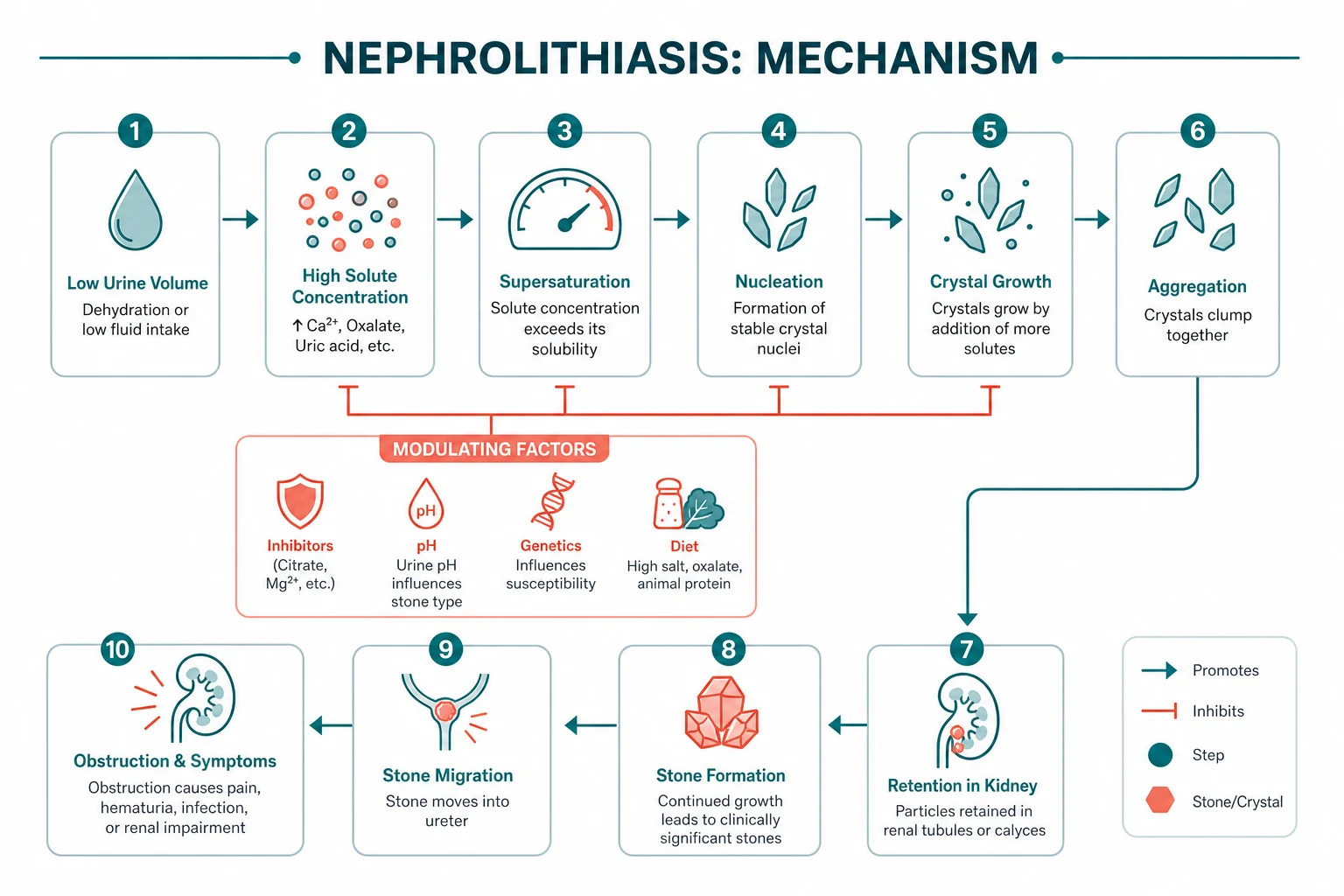
Supersaturation — the fundamental driver
Stone formation requires that urinary solutes exceed their solubility product — a state of supersaturation [1]. This is influenced by:
- Solute concentration — determined by dietary intake, intestinal absorption, and renal handling
- Urine volume — the single most modifiable factor; dilution reduces supersaturation of ALL stone types
- Urine pH — critical for uric acid (insoluble below pH 5.5) and struvite (forms above pH 7.2); less important for calcium oxalate
- Inhibitors — citrate (complexes calcium), magnesium (complexes oxalate), pyrophosphate, Tamm-Horsfall protein [1]
Randall plaques — the anatomical basis of calcium stones
Idiopathic calcium oxalate stones originate at Randall plaques — subepithelial calcium phosphate deposits at the renal papillary tip that erode through the urothelium into the urinary space, providing a surface for calcium oxalate crystal adhesion and overgrowth [1]. Randall plaque formation is strongly associated with hypercalciuria and is the anatomical mechanism by which high urinary calcium promotes stone formation.
Why specific metabolic abnormalities cause stones
| Abnormality | Mechanism | Stone type |
|---|---|---|
| Hypercalciuria | Excess urinary calcium saturates the urine | Calcium oxalate/phosphate |
| Hyperoxaluria | Excess oxalate (dietary or enteric) binds calcium | Calcium oxalate |
| Hypocitraturia | Loss of the main calcium-crystallisation inhibitor | Calcium oxalate |
| Hyperuricosuria | Uric acid crystals seed calcium oxalate growth | Calcium oxalate and uric acid |
| Low urine pH | Uric acid insoluble below pH 5.5 | Uric acid |
| High urine pH with urease | Ammonia precipitates magnesium ammonium phosphate | Struvite |
Risk factors
Dietary risk factors
- Low fluid intake — the most important and most modifiable risk factor
- High dietary sodium — sodium increases urinary calcium excretion (every 100 mmol sodium increase raises urinary calcium by 25 mg) [1]- High animal protein — acid load increases calcium excretion and reduces citrate; also increases uric acid
- High dietary oxalate — spinach, rhubarb, nuts, chocolate, tea, beetroot
- Low calcium intake — paradoxically increases stone risk by increasing free oxalate absorption (the counterintuitive key point proven by Borghi [2])
- High fructose and sucrose — associated with increased stone risk in cohort studies
Metabolic and systemic risk factors
- Hypercalciuria — idiopathic or secondary (hyperparathyroidism, vitamin D excess, Cushing syndrome, thyrotoxicosis, immobilisation, corticosteroids)
- Hyperoxaluria — primary (rare genetic), enteric (Crohn disease, short bowel, bariatric surgery, pancreatic insufficiency), or dietary
- Hypocitraturia — distal RTA, chronic diarrhoea, hypokalaemia, high animal protein, thiazide use
- Hyperuricosuria — gout, myeloproliferative disorders, high purine diet, tumour lysis
- Distal renal tubular acidosis — metabolic acidosis, hypocitraturia, nephrocalcinosis, calcium phosphate stones
- Medullary sponge kidney — congenital cystic dilation of collecting ducts, predisposes to calcium stones
- Crohn disease / bowel resection — enteric hyperoxaluria (fat malabsorption frees oxalate for colonic absorption) plus hypocitraturia from chronic diarrhoea
- Hyperparathyroidism — hypercalcaemia drives hypercalciuria; surgically curable cause of recurrent stones
- Gout — hyperuricaemia and acidic urine predispose to uric acid stones
- Cystinuria — inherited tubular transport defect [1]
DCE long-case integration: In a recurrent stone former, always ask about bowel disease (Crohn, resection, bariatric surgery), gout, and family history, and always check serum calcium to exclude hyperparathyroidism. These are the surgically or metabolically correctable causes that change management. [1]
Clinical presentation
Acute renal colic — the classic presentation
The hallmark of ureteric colic is sudden onset, severe, crescendo flank pain that: [1]
- Radiates from the flank to the groin, testicle (in men) or labia (in women)
- Is colicky (comes in waves) and reaches peak intensity within 30 to 60 minutes
- Causes the patient to writhe and move — the inability to find a comfortable position distinguishes renal colic from peritonitis (where the patient lies still)
- Is accompanied by nausea, vomiting, and sweating (visceral autonomic reflex from ureteric spasm)
- Is associated with haematuria — visible in about 30 per cent and dipstick-positive in 85 to 90 per cent [1]
Pain location and stone position
| Stone location | Pain radiation | Associated symptoms |
|---|---|---|
| Renal pelvis / upper ureter | Flank, costovertebral angle | Nausea, vomiting |
| Mid-ureter | Lower abdomen, iliac fossa | May mimic appendicitis or diverticulitis |
| Distal ureter | Groin, testicle or labia | Urgency, frequency, dysuria (mimics cystitis) |
Atypical or dangerous presentations
- Fever and rigors with obstruction — obstructive pyelonephritis (urological emergency)
- Painless haematuria — consider urothelial malignancy (especially with radiolucent filling defect)
- Insidious presentation with recurrent UTIs — think staghorn calculus (struvite)
- Older patient with severe pain — always consider abdominal aortic aneurysm [1]
Investigation
Acute investigation
| Test | Purpose |
|---|---|
| Urinalysis | Haematuria (85 to 90 per cent), pH, leucocytes/nitrites (infection), crystals |
| Full blood count | Leucocytosis suggests infection (but stress leucocytosis also occurs with pain) |
| U&E, creatinine | Baseline renal function, AKI from obstruction |
| Calcium (corrected) | Exclude hyperparathyroidism — mandatory in every stone former |
| Urate | Hyperuricaemia suggests uric acid stones |
| CRP | Elevation suggests infection or significant inflammation |
| Pregnancy test (women of childbearing age) | Determines imaging choice (ultrasound if pregnant) |
Imaging — non-contrast CT KUB is the gold standard
Non-contrast helical CT KUB is the gold standard for suspected ureteric colic [3]:
- Sensitivity 97 to 100 per cent, specificity 96 to 100 per cent
- Detects all stone types except indinavir (an antiretroviral protease inhibitor)
- Measures stone size, location and density (Hounsfield units — predicts ESWL success)
- Identifies hydronephrosis, perinephric stranding, and ureteric wall thickening
- Excludes alternative diagnoses (AAA, appendicitis, cholecystitis, diverticulitis)
The STONE trial (Smith-Bindman 2014, NEJM) showed that initial ultrasound is a safe alternative to CT — there was no significant difference in serious adverse events, pain scores, or return visits between ultrasound-first and CT-first strategies, though about one-third of ultrasound patients eventually had CT [3].
Exam point: CT KUB detects all stones except indinavir. Ultrasound is the preferred first-line in pregnancy and children. A negative ultrasound does not exclude a stone — proceed to CT if clinical suspicion is high. [1]
When to use ultrasound
- Pregnancy — radiation-free, first-line
- Children — minimise radiation
- Recurrent stone formers — limit cumulative CT radiation
- Point-of-care triage — detects hydronephrosis and larger renal stones [1]
Metabolic evaluation (recurrent stone formers)
A metabolic evaluation is recommended for:
- All recurrent stone formers (two or more stones)
- First-time stone formers with risk factors (family history, bowel disease, gout, hypercalcaemia, CKD, solitary kidney)
- Children with any stone [1]
24-hour urine collection (two samples on different days under usual diet):
- Volume (target above 2.5 L/day)
- Calcium (hypercalciuria if above 4 mmol/kg/day in women or above 7.5 mmol/day in men) [1]- Oxalate (hyperoxaluria if above 0.5 mmol/day)
- Citrate (hypocitraturia if below 1.7 mmol/day in women or below 2.5 mmol/day in men)
- Urate (hyperuricosuria if above 4.0 mmol/day)
- Sodium (high sodium drives high calcium)
- Cystine (if cystinuria suspected — cyanide-nitroprusside screen) [1]
Blood tests:
- Serum calcium and phosphate (hyperparathyroidism)
- Parathyroid hormone (if calcium elevated)
- Urate
- Bicarbonate and potassium (distal RTA)
- eGFR [1]
Stone analysis (if stone is passed or retrieved) — infrared spectroscopy or X-ray diffraction confirms composition and guides prevention. [1]
Acute management
Analgesia
NSAIDs are first-line for renal colic:
- Diclofenac 75 mg intramuscularly or intravenously (or ibuprofen 400 to 600 mg orally) [1]- NSAIDs reduce prostaglandin-mediated ureteric inflammation and renal capsular pressure
- At least as effective as opioids, with less nausea and vomiting
- Avoid NSAIDs in AKI, advanced CKD (eGFR below 30), volume depletion, active peptic ulcer disease, or pregnancy (third trimester — premature closure of ductus arteriosus) [1]
Opioids (morphine 5 to 10 mg IV or fentanyl 50 to 100 micrograms IV) are second-line or for patients in whom NSAIDs are contraindicated. [1]
Antiemetics — metoclopramide 10 mg IV or ondansetron 4 mg IV for nausea and vomiting. [1]
DWE key point: NSAIDs are first-line, NOT opioids. The classic DWE question contrasts the writhing patient with renal colic (NSAIDs) against the still patient with peritonitis (opioids). [1]
Fluids
- Intravenous fluids only if the patient is dehydrated or unable to tolerate oral intake
- Routine aggressive IV hydration does NOT promote stone passage and risks volume overload
- Encourage oral fluids once vomiting settles [1]
Stone passage — size matters
| Stone size | Spontaneous passage rate | Management |
|---|---|---|
| Below 5 mm | ~80 per cent | Expectant — analgesia, fluids, strain urine |
| 5 to 10 mm | ~50 per cent | Consider MET (tamsulosin) or elective intervention |
| Above 10 mm | Below 20 per cent | Intervention (ESWL, URS, or PCNL) |
Other factors favouring passage: distal ureteric location, smooth ureter, no prior ureteric surgery. [1]
Medical expulsive therapy — tamsulosin
The role of alpha-blocker medical expulsive therapy (MET) has been debated: [1]
- The SUSPEND trial (Pickard 2015, Lancet) — a large multicentre RCT of 1167 patients — found no significant benefit of tamsulosin or nifedipine over placebo for ureteric stones below 10 mm overall [4].
- The Hollingsworth 2016 BMJ meta-analysis — individual patient data from 55 trials — showed tamsulosin modestly increased passage for larger (5 to 10 mm) distal ureteric stones [6].
Current practice: Tamsulosin 0.4 mg daily may be offered for selected patients with distal ureteric stones 5 to 10 mm while awaiting spontaneous passage or elective intervention, with counselling about the modest and debated benefit. [1]
Interventional management
ESWL — extracorporeal shock wave lithotripsy
- Indication: Stones below 2 cm in the renal pelvis or upper ureter
- Mechanism: Extracorporeal shock waves focused on the stone fragment it into passable pieces
- Advantages: Non-invasive, outpatient or day procedure
- Limitations: Less effective for hard stones (cystine, brushite), lower pole stones (fragments may not clear), obese patients, and stones above 2 cm
- Complications: Perirenal haematoma, steinstrasse (column of fragments obstructing the ureter), renal parenchymal damage [1]
Ureteroscopy with laser lithotripsy
- Indication: Ureteric stones (any location), renal stones (especially lower pole), stones failing ESWL, and stones above 2 cm in selected patients
- Mechanism: Rigid or flexible ureteroscope passed via urethra and bladder into the ureter/kidney; holmium laser fragments the stone under direct vision
- Advantages: Direct visualisation, high success rate, effective for all stone types
- Complications: Ureteric injury, stricture, avulsion (rare but devastating), post-operative infection, stent symptoms (frequency, urgency, haematuria)
- Stent: A ureteric stent (JJ stent) is usually placed for a few days after ureteroscopy [1]
PCNL — percutaneous nephrolithotomy
- Indication: Stones above 2 cm, staghorn calculi, and complex or large stones
- Mechanism: Percutaneous tract from the skin through the kidney into the collecting system; stone is fragmented and removed under direct vision
- Advantages: Highest stone-free rate for large stones; first-line for staghorn calculi
- Complications: Bleeding (may require transfusion), sepsis, injury to adjacent organs (colon, liver, spleen, pleura — causing hydrothorax or pneumothorax)
- Hospital stay: Typically 2 to 4 days [1]
Urgent decompression
Indications for urgent decompression (ureteric stent or percutaneous nephrostomy):
- Obstructive pyelonephritis — infected obstructed system (fever, rigors, sepsis)
- AKI from bilateral obstruction or obstruction of a solitary kidney
- Intractable pain or vomiting despite maximal analgesia
- Anuria from bilateral ureteric obstruction [1]
Emergency principle: An obstructed infected urinary system is a urological emergency. Antibiotics alone cannot penetrate an obstructed collecting system. Urgent decompression with a ureteric stent or percutaneous nephrostomy within hours is mandatory, with definitive stone treatment deferred until the infection resolves. [1]
Prevention

Dietary prevention — the foundation for all stone types
The Fink 2013 ACP systematic review confirmed that increased fluid intake approximately halves the risk of recurrent stones, and that thiazides, citrate, and allopurinol each reduce recurrence in recurrent calcium stone formers [5].
-
Fluid intake above 3 L per day — target urine output above 2.5 L/day (urine should be pale and dilute). This is the single most effective preventive measure, reducing recurrence by about 50 per cent [5].
-
Normal calcium intake (1000 to 1200 mg per day) — NOT low calcium. The Borghi 2002 NEJM trial proved that a normal-calcium, low-sodium, low-protein diet halved stone recurrence (relative risk 0.49) compared with a traditional low-calcium diet [2]. Calcium binds intestinal oxalate, preventing its absorption.
-
Reduce dietary sodium (below 4 to 5 g per day) — sodium increases urinary calcium excretion. [1]
-
Reduce animal protein (0.8 to 1.0 g/kg per day) — animal protein increases acid load (raising calcium excretion and lowering citrate) and increases uric acid. [1]
-
Reduce dietary oxalate — limit spinach, rhubarb, nuts, chocolate, and tea (especially in hyperoxaluria). [1]
The most important dietary exam point: A low-calcium diet INCREASES stone risk. Normal calcium intake with reduced sodium and animal protein is correct. This is the single most tested dietary fact in nephrolithiasis. [1]
Targeted pharmacotherapy
| Metabolic abnormality | Drug | Mechanism |
|---|---|---|
| Hypercalciuria (recurrent calcium stones) | Thiazide diuretic (e.g., chlorthalidone, hydrochlorothiazide) | Increases distal tubular calcium reabsorption, reduces urinary calcium |
| Hypocitraturia | Potassium citrate | Alkalinises urine and increases urinary citrate (calcium inhibitor) |
| Uric acid stones (acidic urine) | Potassium citrate (alkalinise to pH 6.5 to 7.0) ± allopurinol | Citrate raises pH (dissolves existing stones); allopurinol reduces uric acid production |
| Hyperuricosuria with calcium stones | Allopurinol | Reduces uric acid, which seeds calcium oxalate crystallisation |
| Enteric hyperoxaluria | Calcium supplements with meals + low-oxalate diet ± cholestyramine | Calcium binds intestinal oxalate; cholestyramine binds bile acids |
| Cystinuria | Potassium citrate (pH above 7.5) ± tiopronin or D-penicillamine | Alkalinisation increases solubility; chelation binds cystine |
What NOT to do
- Do NOT prescribe a low-calcium diet — it increases stone risk [2].
- Do NOT use potassium citrate in struvite stones — alkalinising an already alkaline urine promotes struvite formation.
- Do NOT rely on antibiotics alone for struvite staghorn calculi — complete surgical removal is required.
- Do NOT use routine aggressive IV fluids for stone passage — evidence does not support it and it risks overload.
- Do NOT prescribe tamsulosin routinely for all ureteric stones — the SUSPEND trial showed no overall benefit [4].
Systemic associations — the long-case perspective
Primary hyperparathyroidism
- Causes hypercalcaemia-driven hypercalciuria with calcium oxalate or phosphate stones
- Screen with serum calcium (corrected) in every stone former; check PTH if elevated
- Treatment is parathyroidectomy — resolves hypercalcaemia, reduces hypercalciuria, and decreases stone recurrence in the majority
- Cinacalcet lowers calcium but is not first-line for stone prevention [1]
Distal renal tubular acidosis (type 1)
- Metabolic acidosis with inappropriately alkaline urine (pH above 5.5), hypocitraturia, hypercalciuria
- Causes calcium phosphate stones (alkaline urine) and nephrocalcinosis
- Check bicarbonate (low), potassium (low), and urine pH (high)
- Treatment: potassium citrate (replaces bicarbonate and citrate) [1]
Crohn disease and enteric hyperoxaluria
- Fat malabsorption causes calcium to bind fatty acids (saponification), leaving free oxalate for colonic absorption
- Chronic diarrhoea also causes hypocitraturia and low urine volume
- Management: low-oxalate low-fat diet, oral calcium with meals, cholestyramine, high fluid intake, potassium citrate [1]
Gout and hyperuricaemia
- Acidic urine and hyperuricosuria predispose to uric acid stones
- Alkalinise urine (potassium citrate to pH 6.5 to 7.0) and allopurinol for hyperuricosuria [1]
Medullary sponge kidney
- Congenital cystic dilation of collecting ducts
- Predisposes to calcium stones and recurrent UTIs
- No specific treatment beyond general stone prevention [1]
Key DWE MCQ patterns
- Stone type identification from clinical scenario: Proteus UTI + alkaline urine + staghorn = struvite; gout + acidic urine + radiolucent = uric acid; childhood onset + hexagonal crystals = cystine.
- Imaging choice: Non-contrast CT KUB is gold standard (detects all except indinavir); ultrasound first in pregnancy.
- Dietary advice: Normal calcium (NOT low) + reduced sodium + reduced animal protein — the Borghi trial.
- Acute analgesia: NSAIDs (diclofenac IM) first-line, not opioids.
- Stone size and passage: Below 5 mm passes (80 per cent); above 10 mm needs intervention.
- Medical expulsive therapy: SUSPEND trial — no overall benefit for tamsulosin; modest benefit for larger distal stones only.
- Pharmacotherapy matching: Hypercalciuria = thiazide; hypocitraturia = potassium citrate; uric acid = alkalinisation + allopurinol; cystinuria = alkalinisation + tiopronin.
- Emergency: Obstructed pyelonephritis = urgent decompression (stent or nephrostomy), not antibiotics alone.
- Metabolic screening: Every stone former gets serum calcium; recurrent formers get 24-hour urine.
- Low-calcium diet trap: Low calcium INCREASES stones (increases oxalate absorption) — the most common wrong answer. [1]
References
[1] Moe OW — Kidney stones: pathophysiology and medical management. Lancet 2006;367:333 to 344. The definitive review of stone pathophysiology — supersaturation, Randall plaques, inhibitors, and the metabolic basis of each stone type.
[2] Borghi L, et al. — Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. NEJM 2002;346:77 to 84. The landmark RCT proving that a normal-calcium, low-sodium, low-protein diet halves stone recurrence compared with a low-calcium diet (RR 0.49).
[3] Smith-Bindman R, et al. — Ultrasonography versus computed tomography for suspected nephrolithiasis. NEJM 2014;371:1100 to 1110. The STONE trial — ultrasound is a safe first-line alternative to CT, with no significant difference in serious adverse events.
[4] Pickard R, et al. — Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial (SUSPEND). Lancet 2015;386:341 to 349. No significant benefit of tamsulosin or nifedipine over placebo for ureteric stones below 10 mm overall.
[5] Fink HA, et al. — Medical management to prevent recurrent nephrolithiasis in adults: a systematic review for an ACP Clinical Guideline. Ann Intern Med 2013;158:535 to 543. Fluid intake halves recurrence; thiazides, citrate, and allopurinol each reduce recurrence in recurrent calcium stone formers.
[6] Hollingsworth JM, et al. — Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis. BMJ 2016;355:i6112. Individual-patient-data meta-analysis showing modest benefit of tamsulosin for larger (5 to 10 mm) distal ureteric stones.
[7] Curhan GC — Epidemiology of stone disease. Urol Clin North Am 2007;34:287 to 293. The epidemiological foundation — 10 per cent lifetime risk, 2:1 male predominance, 50 per cent recurrence at 10 years.
EAU Guidelines on Urolithiasis (uroweb.org); NICE NG118 (2019); Kidney Health Australia. [1]
References
- [1]Moe OW Kidney stones: pathophysiology and medical management Lancet, 2006.PMID 16443041
- [2]Borghi L, Schianchi T, Meschi T, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria N Engl J Med, 2002.PMID 11784873
- [3]Smith-Bindman R, Aubin C, Bailitz J, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis N Engl J Med, 2014.PMID 25229916
- [4]Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial Lancet, 2015.PMID 25998582
- [5]Fink HA, Wilt TJ, Eidman KE, et al. Medical management to prevent recurrent nephrolithiasis in adults: a systematic review for an American College of Physicians Clinical Guideline Ann Intern Med, 2013.PMID 23546565
- [6]Hollingsworth JM, Canales BK, Rogers MA, et al. Alpha blockers for treatment of ureteric stones: systematic review and meta-analysis BMJ, 2016.PMID 27908918
- [7]Curhan GC Epidemiology of stone disease Urol Clin North Am, 2007.PMID 17678980