Phys · renal
Renal Cell Carcinoma AND Urothelial Malignancy
Also known as Renal Cell Carcinoma AND Urothelial Malignancy · renal cell carcinoma and urothelial malignancy
Consultant-physician depth guide to Renal Cell Carcinoma AND Urothelial Malignancy for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
Renal Cell Carcinoma AND Urothelial Malignancy is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]
Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
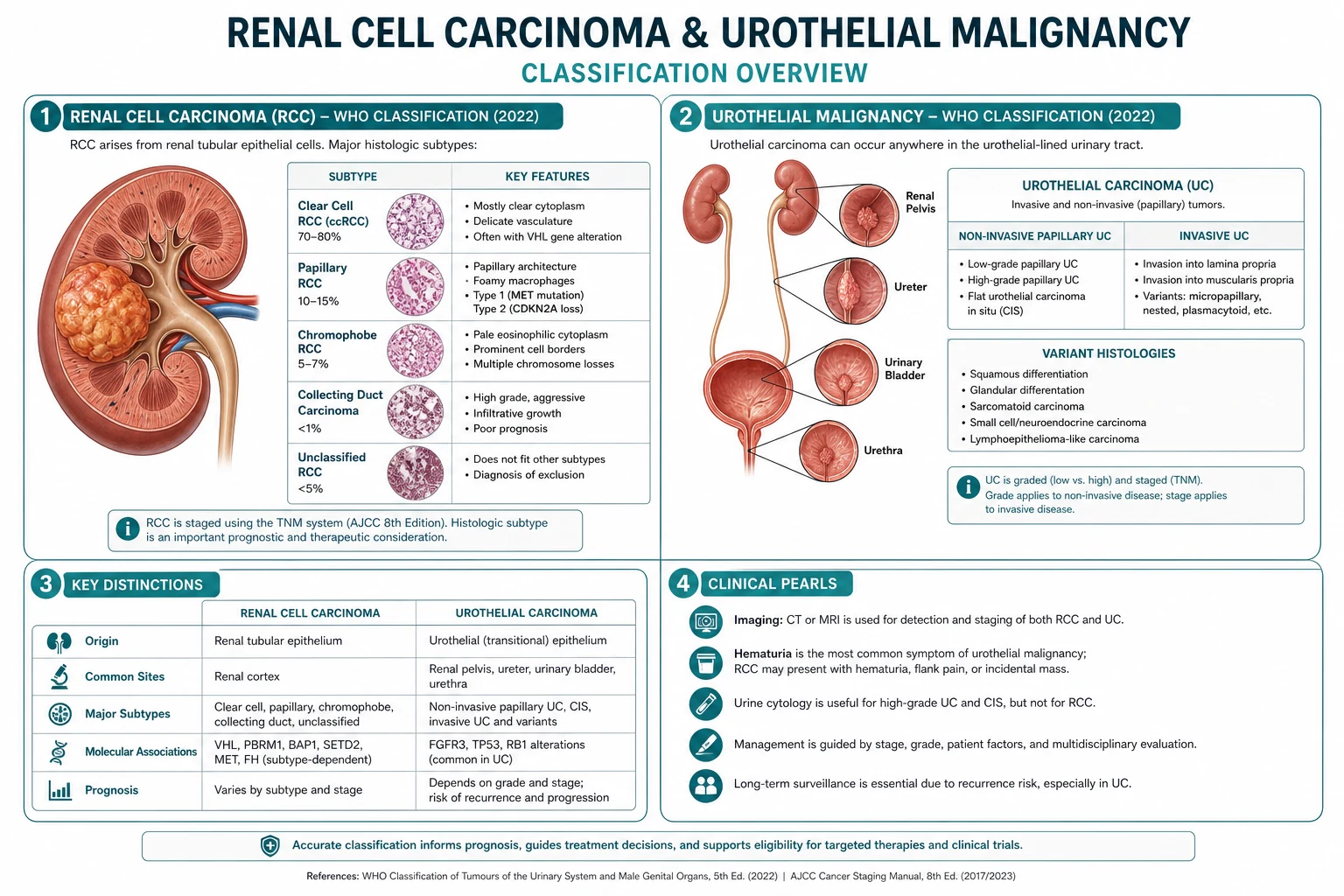
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
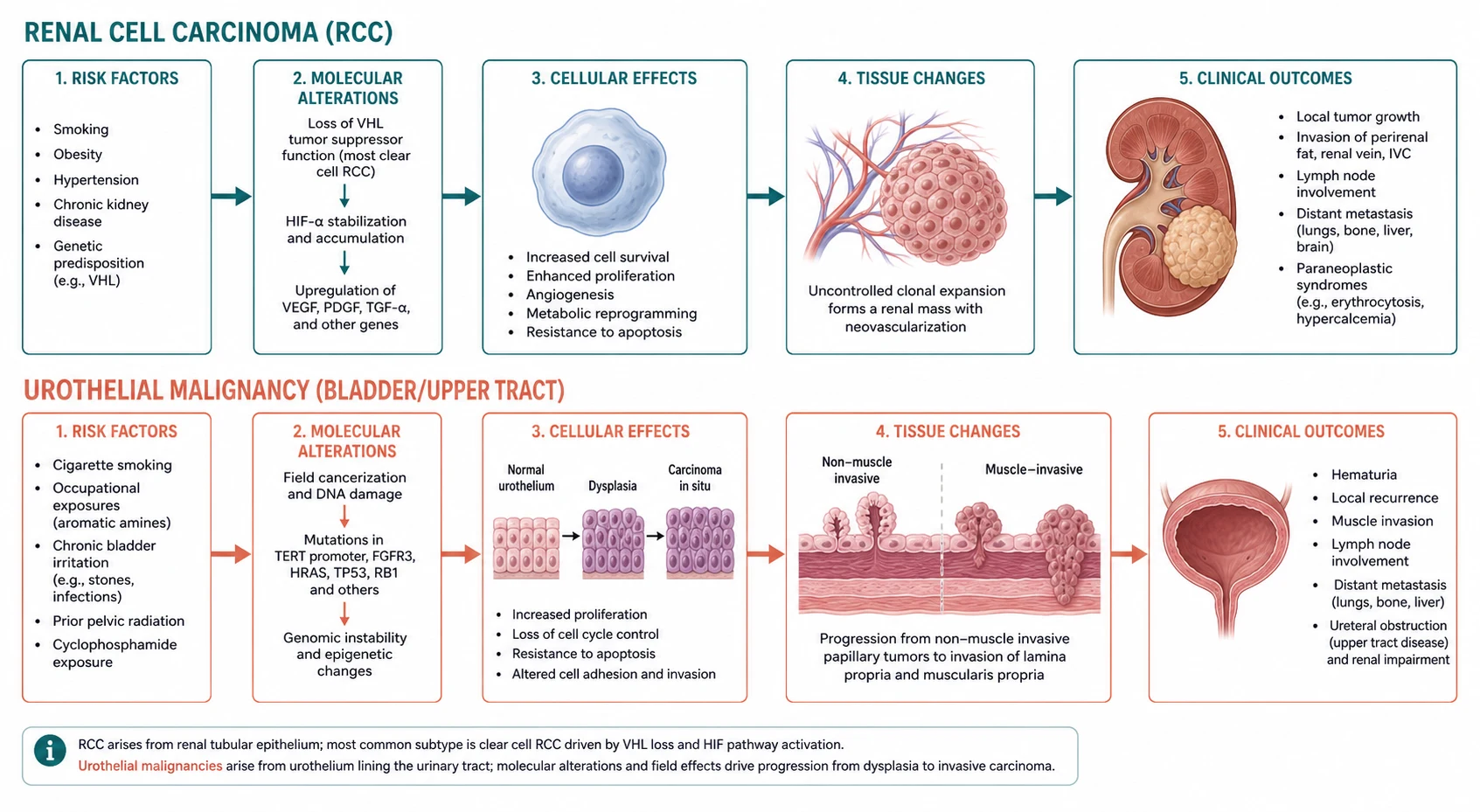
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
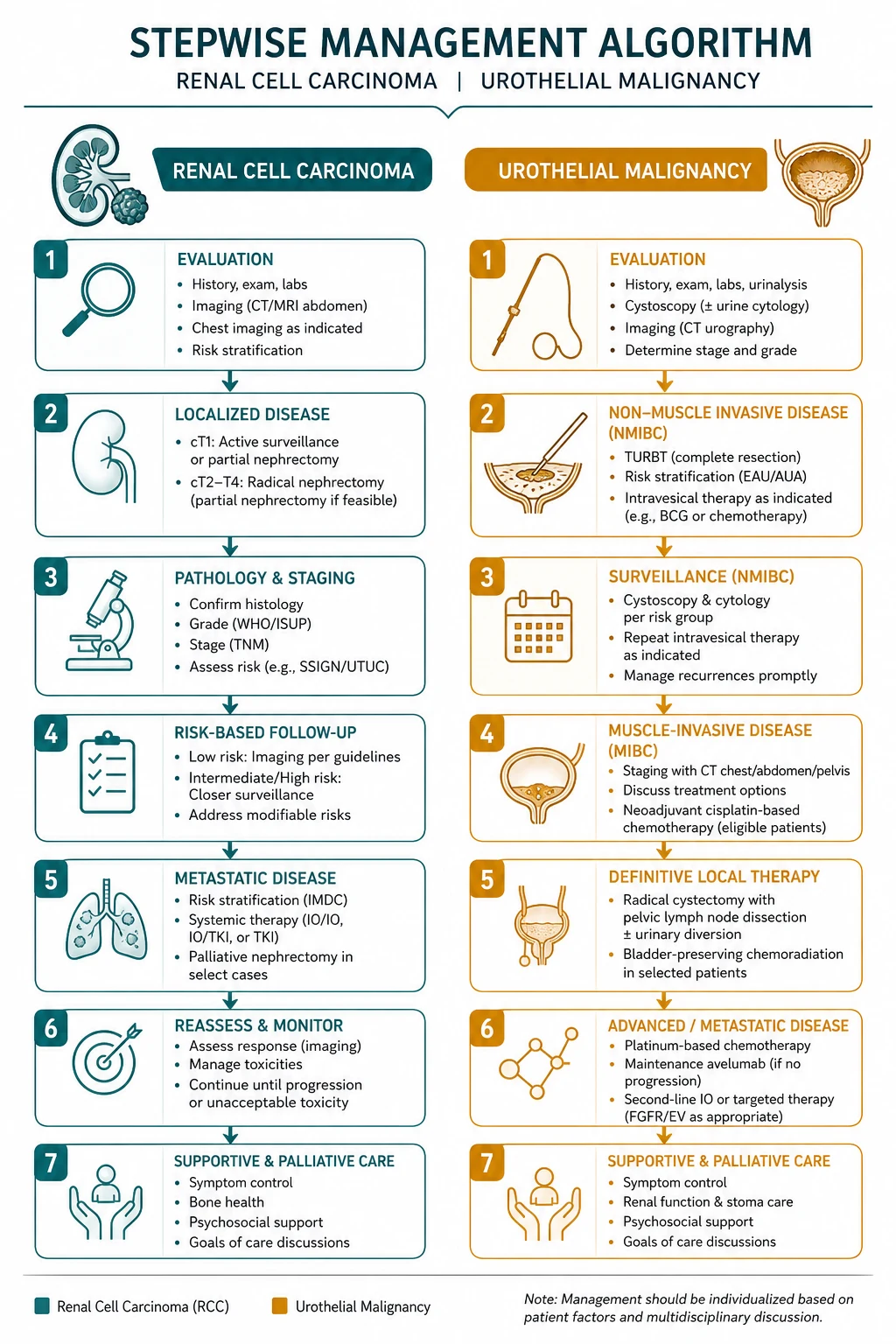
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]
Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Renal Cell Carcinoma AND Urothelial Malignancy to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Chen YS, Yu CC, Chang R, Wu SH, et al. Efficacy of checkpoint inhibitors in genitourinary cancers with advanced chronic kidney disease Cancer Immunol Immunother, 2026.PMID 42426360
- [2]Petrelli F, Colombo Zefinetti L, D'Alessio A, Dottorini L, et al. Next-Generation Checkpoint Combinations: Optimizing PD-(L)1-Based Therapy Across the Advanced, Adjuvant, and Neoadjuvant Settings Curr Oncol Rep, 2026.PMID 42406187
- [3]Zhang Y, Wu G, Sun F, Wang B, et al. Radiomics and deep learning in upper tract urothelial carcinoma: advancing preoperative risk stratification and clinical decision-making Front Oncol, 2026.PMID 42404222
- [4]Jost LM, Duwe G, Kauth V, Höfner T, et al. [Artificial intelligence as decision support tool in urological oncology: current evidence and challenges] Urologie, 2026.PMID 42126599
- [5]Inoue S, Tsuboi I, Miszczyk M, Miyajima K, et al. Time-of-Day Immunotherapy Administration and Outcomes in Advanced Cancers: A Systematic Review and Meta-Analysis JAMA Netw Open, 2026.PMID 42084869
- [6]Maráz A, Koroncziová K, Rozsvai T [Immunotherapy for urological cancers in 2025] Magy Onkol, 2025.PMID 41385769
- [7]Xi Y, Yao T, Zhang C, Zhuang T Effectiveness of safety care and clinical nursing pathway in patients undergoing cardiovascular intervention: a randomized controlled trial Perioper Med (Lond), 2026.PMID 42469924
- [8]Marks FJ, Walters SJ, Sutton L, Jacques RM What statistical methods are more appropriate for predicting recruitment at the design stage of a randomised controlled trial? Trials, 2026.PMID 42469922
- [9]Hajiaqaei M, Mohammadi A Transcranial random noise stimulation (tRNS) over the left dorsolateral prefrontal cortex ameliorates emotion dysregulation and executive function: a single-blind, randomized, sham-controlled clinical trial BMC Psychol, 2026.PMID 42469906
- [10]Loughraieb S, Guendouzi R, Terki F, Mokeddem K, et al. Invasive Renal Parenchymal Urothelial Carcinoma: A Case Report and Literature Review of Imaging Features and Spectrum of Infiltrative Renal Masses Cureus, 2026.PMID 42299196
- [11]Luo W, Song Z, Liu Z, Zhang G, et al. Soulangianolide A targets FAM120A to disrupt SREBP1-driven lipid metabolic reprogramming and suppress clear cell renal cell carcinoma J Exp Clin Cancer Res, 2026.PMID 42469889
- [12]Wang B, Liu H, Guo Y, Ma J, et al. Multi-omics profiling highlights RPLP0 as a potential biomarker for prognosis and response to immunotherapy in clear cell renal cell carcinoma BMC Cancer, 2026.PMID 42469699