Phys · renal
Renal Replacement Therapy: Haemodialysis and Peritoneal Dialysis
Also known as RRT · dialysis · haemodialysis · hemodialysis · peritoneal dialysis · CAPD · APD · end-stage kidney disease · ESKD · ESRF · AV fistula · Kt/V · PD peritonitis · IDEAL trial
Consultant-physician-depth guide to renal replacement therapy — the transplant-first landscape, IDEAL and symptom-based dialysis initiation, haemodialysis versus peritoneal dialysis selection by patient rather than superiority, fistula-first access and its complications, PD peritonitis diagnosis to catheter removal, the cardiovascular burden of dialysis, urgent starts, pregnancy, the frail elderly, conservative care as an active choice, and the holistic bundle — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Renal Replacement Therapy: Haemodialysis and Peritoneal Dialysis
The answer first
Renal replacement therapy is a portfolio, not a machine — transplantation, haemodialysis, peritoneal dialysis and conservative kidney management are the four options, and the consultant's job is to sequence them for each patient rather than default to the dialysis chair. Six rules carry the DWE and the long-case defence [2] [3]:
- Transplant first, always. A functioning graft gives better survival and better life than any dialysis — transplantation is the treatment of choice for every eligible patient, and dialysis exists as a bridge to it or a destination when it is impossible [3] [2].
- Start on symptoms, not a number. The IDEAL trial proved that planned early start (eGFR 10–14) confers no survival benefit over late start (eGFR 5–7) — you start dialysis when uraemia or its complications declare themselves, typically somewhere in the eGFR 5–10 band, while planning starts many months earlier [1] [2].
- Modality is chosen by the patient, not by superiority. Haemodialysis and peritoneal dialysis deliver similar survival; the choice turns on lifestyle, residual kidney function, dexterity, home support and cardiac stability — independence versus intensity [4] [2].
- Access is the Achilles heel — fistula first, and early. An arteriovenous fistula needs 6–12 weeks to mature and a meaningful share fail to mature, so it is created months before the anticipated start; a tunneled catheter is a bridge, never a destination [7] [25].
- Cardiovascular disease is what kills dialysis patients. Volume and blood-pressure management, avoiding intradialytic myocardial stunning, and the holistic bundle (ESA, binders, vaccination, diet, advance care planning) matter as much as the membrane [17] [16].
- Conservative care is an active choice, not neglect. In the elderly, frail, multimorbid patient, structured conservative kidney management can preserve quality of life with little or no survival penalty — offering it honestly is consultant-level practice, not therapeutic nihilism [18] [2].
The RRT landscape — transplant first, then bridge or destination
The end-stage kidney population has four doors, and the exam expects you to name all four before describing any [2]:
| Option | Position in the landscape | The consultant's framing |
|---|---|---|
| Kidney transplantation | Treatment of choice for every eligible patient — preemptive (before any dialysis) is best of all | Superior survival and quality of life; work-up runs in parallel with dialysis planning, not after it [3] |
| Peritoneal dialysis | Home-based, daily, continuous clearance | Best early when residual kidney function remains; independence and autonomy are the selling points [6] [26] |
| Haemodialysis | Intermittent, supervised, intense — centre, satellite or home | The default for cardiac instability, failed PD, and patients who want supervised care; home HD for the motivated [5] [10] |
| Conservative kidney management | Active, structured symptom-focused care without dialysis | A legitimate path in multimorbidity and frailty — not abandonment, and often reversible into dialysis later [18] |
The survival hierarchy is the piece of evidence the DCE probes. Wolfe's landmark registry analysis separated three cohorts — all dialysis patients, dialysis patients on the waiting list, and transplant recipients — and found that transplantation conferred a dramatic, durable mortality reduction even after adjusting for the selection of healthier patients into the waitlist and transplant groups; the benefit was greatest in the young and in diabetics, the two groups with the most life-years at stake [3]. The practical consequence the examiner wants to hear: dialysis planning and transplant work-up start together — a preemptive transplant, especially from a living donor, spares the patient access surgery, catheter-days and cardiovascular exposure entirely [2] [3].
Between HD and PD, the evidence is a draw, and quoting it correctly is a DWE favourite. Large contemporary cohorts show similar survival with haemodialysis and peritoneal dialysis, with modest time-varying patterns (PD often slightly better in the first year or two — residual function and no central catheter — then converging or favouring HD in the longer run) [4] [6]. Neither the DWE nor the DCE rewards a winner; both reward the sentence "the modalities are equivalent on survival, so the choice belongs to the patient's life, not my preference" [4] [2].
When to start — IDEAL, and the triggers that actually matter
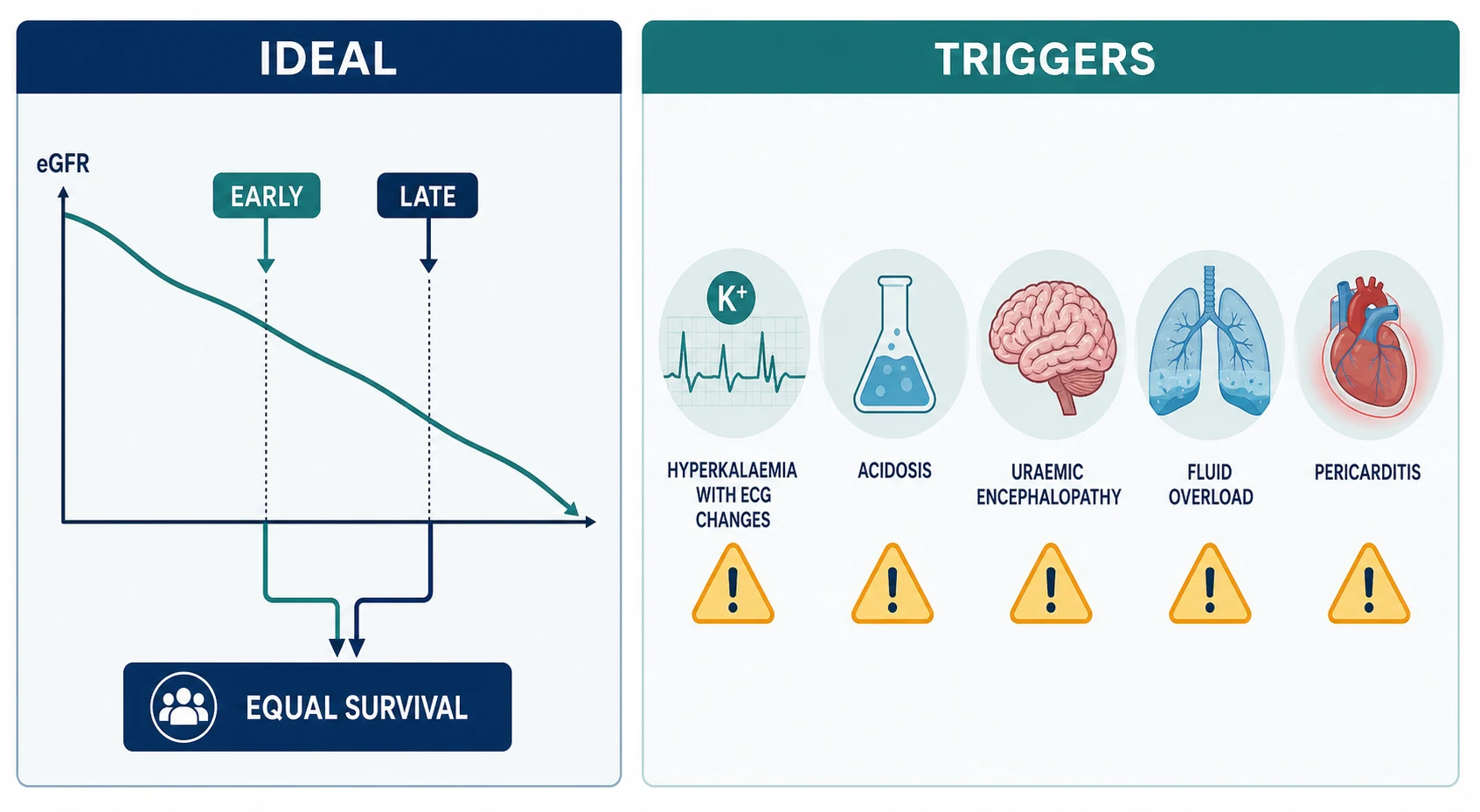
The IDEAL trial (Australia and New Zealand, 828 patients) randomised adults with progressive CKD to planned dialysis start at eGFR 10–14 (early) versus 5–7 (late), and found no difference in survival or cardiovascular and infective outcomes over a median of three and a half years — even though three quarters of the late-start group eventually began dialysis, most for symptoms [1]. The exam reading is precise: IDEAL does not license waiting for a crisis — it proves the number alone is not the trigger. The triggers are clinical [1] [2]:
- Uraemic symptoms — anorexia, nausea, weight loss, pruritus, restless legs, declining cognition or functional status, serositis [2].
- Refractory hyperkalaemia despite dietary and medical management [2].
- Refractory metabolic acidosis despite bicarbonate supplementation [2].
- Fluid overload unresponsive to diuretics — pulmonary oedema, accelerating hypertension [2].
- Uraemic pericarditis or encephalopathy — the absolute, do-not-wait indications [5].
In practice most planned starts happen with eGFR somewhere between 5 and 10, when the symptom burden arrives — which is why the planning window is measured in months, not weeks: education and modality choice, transplant work-up, and access creation all have to be finished before the eGFR reaches the starting band [2] [7]. A fistula takes 6–12 weeks to mature, and failure-to-mature rates are substantial — DOPPS data show wide international variation in fistula patency and long catheter-dependence intervals where access planning is late — so the rule of thumb is refer for access creation roughly six months before the anticipated start, and earlier in the elderly or those with difficult vessels [7] [25] [24].
Dialysis initiation in five numbers
HD vs PD — selection by patient, not superiority
With survival equivalent, modality selection is an exercise in matching the therapy to a life. The dimensions the consultant weighs — and the examiner listens for — are these [4] [2]:
| Dimension | Haemodialysis | Peritoneal dialysis |
|---|---|---|
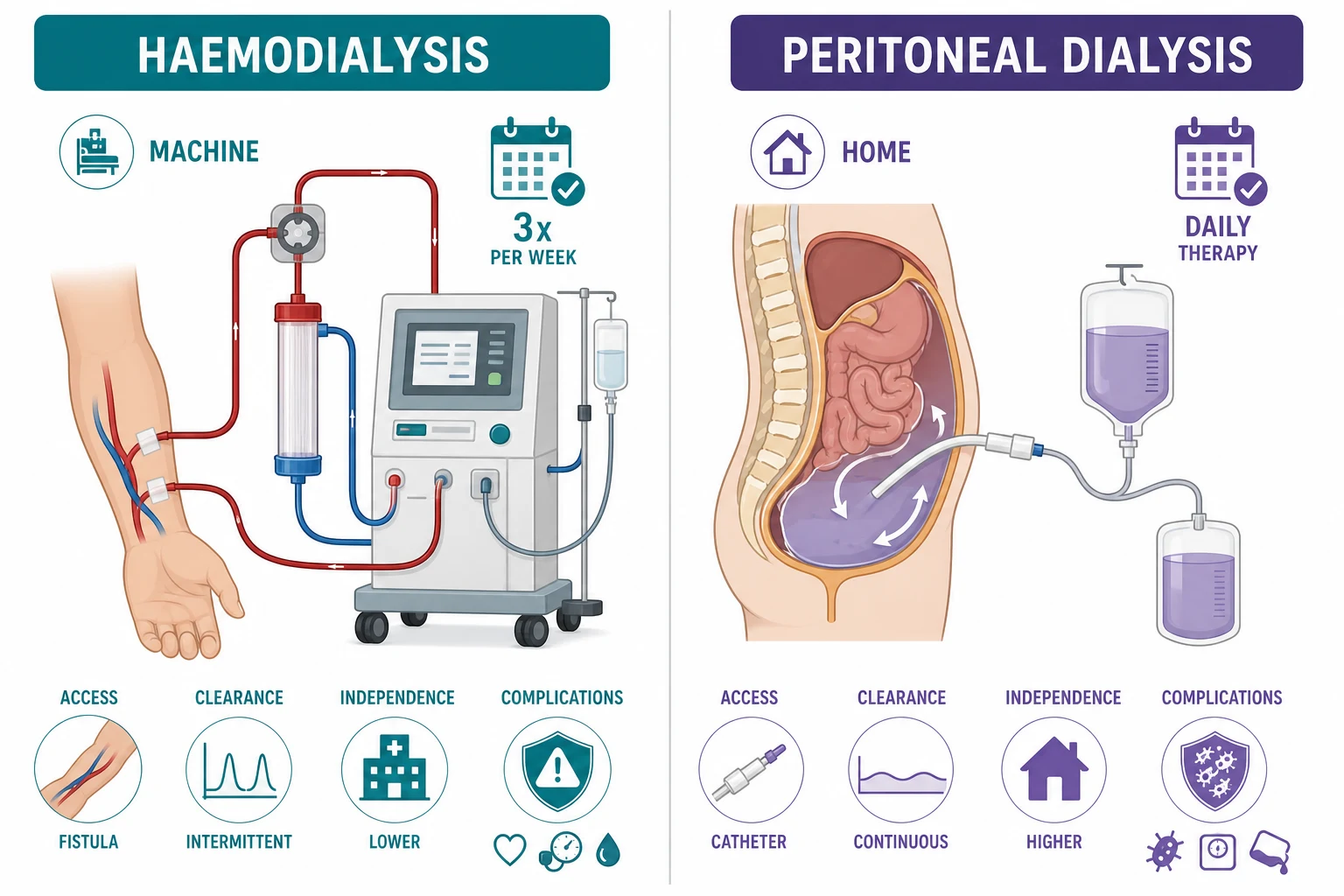
| Schedule | Intermittent — typically three sessions of about 4 hours weekly, in centre or at home | Daily and continuous — CAPD (4 manual exchanges a day) or APD (overnight cycler, days free) [5] [6] |
| Clearance pattern | Peaks and troughs — intense ultrafiltration and solute swings per session | Gentle, continuous — steadier volume and chemistry, kinder to residual function [26] |
| Access | AV fistula preferred; graft or tunneled catheter otherwise | Intraperitoneal catheter with a subcutaneous cuff; exit-site discipline required [7] [13] |
| Independence | Lower in-centre; higher at home | High — the patient (or a helper) performs therapy at home; travel-friendly with planning [6] [20] |
| Best suited to | Cardiac instability needing supervised sessions, failed PD, no suitable home environment, patient preference for supervised care | Autonomous patients with dexterity and vision, residual function worth preserving, good housing and support, needle phobia, those wanting daytime freedom [2] [6] |
| Signature complications | Intradialytic hypotension, cramps, access thrombosis and infection | Peritonitis, exit-site infection, hernias and leaks, ultrafiltration failure over time [12] [13] |
The who-suits-whom reasoning is where marks live. PD asks for manual dexterity, adequate vision, cognitive capacity, hygienic housing, and usually a support person as backstop — and it rewards the patient with autonomy, no needles, preserved residual function and gentler volume physiology [6] [26]. HD asks nothing of the patient's hands but everything of their cardiovascular system three times a week — rapid ultrafiltration in a fixed window — and rewards the patient who wants professionals in charge, or whose heart cannot tolerate intradialytic stress without monitoring [5] [16]. Absolute PD barriers are few: an abdomen that cannot host therapy (extensive adhesions, untreatable hernias, ostomy conflicts, severe inflammatory bowel disease) and the absence of any safe home setup when no assistance is available [6] [21].
Haemodialysis — prescription, adequacy and the access hierarchy
The standard prescription is three sessions per week of about four hours, using a biocompatible membrane, with blood flow, dialysate composition (sodium, potassium, calcium, bicarbonate) and ultrafiltration individualised to the patient [5]. Adequacy is quantified with spKt/V — the normalised dose of small-solute clearance per session — with the KDOQI 2015 update recommending a minimum delivered spKt/V of 1.2, and in practice targeting about 1.4 to ensure the floor is never breached; the HEMO trial had already shown that pushing spKt/V from about 1.3 toward 1.7, or switching to high-flux membranes, did not improve survival in the main analysis [8] [9]. The lesson to quote: adequacy has a floor, not a ceiling — once the dose is adequate, outcomes turn on volume, access and cardiovascular management, not on chasing clearance [9] [16].
More time and more frequency is the frontier. The Frequent Hemodialysis Network trial of in-center haemodialysis six times weekly versus three times weekly improved the composite of death or left-ventricular mass increase and blood-pressure control, at the cost of more access interventions — and long-term follow-up of the FHN nocturnal cohort suggested a mortality advantage for frequent home nocturnal dialysis, albeit with the selection caveats of a small trial [10] [11]. The consultant synthesis: frequent or extended-hour dialysis (usually home-based) is the option to offer the motivated patient with volume, phosphate or LV-mass problems that standard schedules cannot tame [10] [11].
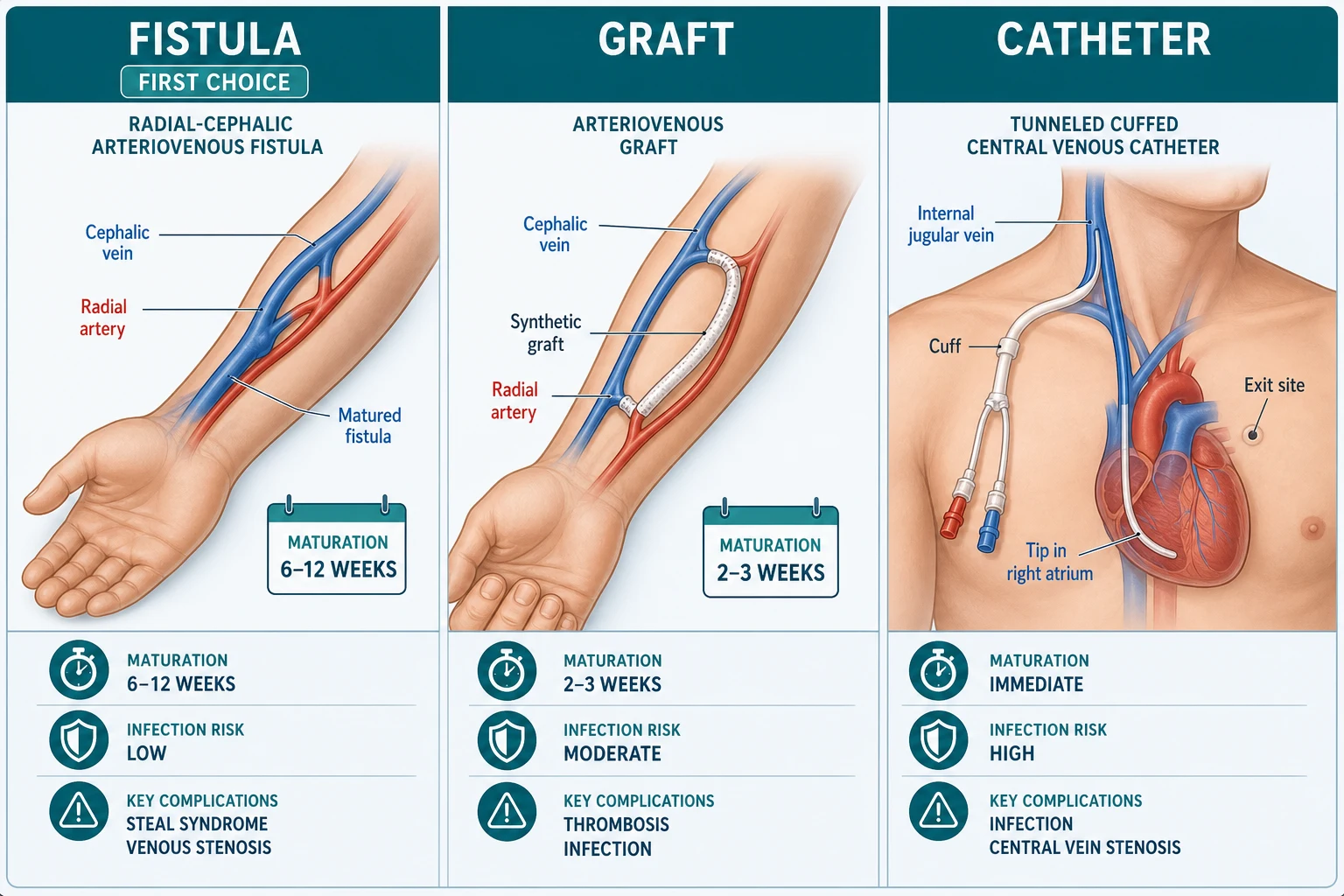
Access is the hierarchy the whole world agrees on. A native arteriovenous fistula — classically radial-cephalic at the wrist, then brachiocephalic, then brachiobasilic transposition — is first choice: best long-term patency, lowest infection risk, lowest cost [7] [24]. An arteriovenous graft is second — usable in two to three weeks but with more thrombosis and infection. A tunneled cuffed catheter is last — immediately usable but accumulating bacteraemia, central vein stenosis and mortality with every catheter-day; DOPPS comparisons drove the global fistula-first culture by showing how strongly access type tracks with outcomes [7] [24] [25]. The KDOQI 2019 update softened the old dogma into the ESKD Life-Plan — the right access for the right patient at the right time — but for the exam, "fistula first, created early; catheter as a bridge, never a destination" remains the safe core [7].
The fistula complications that the short case and the DWE both test [7]:
- Failure to mature — the commonest early problem; vein mapping before surgery and early duplex after creation catch it [7] [25].
- Steal syndrome — arterial inflow diverted through the fistula leaves the hand ischaemic: cold, painful, numb hand, worse on dialysis, with trophic change in severe cases. Mild steal is observed; severe steal threatens the hand and needs intervention (banding, distal revascularisation with interval ligation, or ligation) [7].
- Aneurysmal dilatation and stenosis — from years of needling; monitored clinically and by flow surveillance, repaired before rupture risk or thrombosis [7].
- Infection — uncommon in fistulas, commoner in grafts, and the dominant complication of catheters: exit-site infection, tunnel infection, and catheter-related bacteraemia with its metastatic sequelae (endocarditis, osteomyelitis) [7] [24].
Peritoneal dialysis — dwell physiology, prescriptions and the membrane
Peritoneal dialysis uses the peritoneum as the membrane: dialysate dwells in the peritoneal cavity, solute diffuses down its gradient from blood into dialysate, and water follows the osmotic gradient created by glucose (or, for the long dwell, the glucose polymer icodextrin) [6]. The two prescriptions are CAPD — continuous ambulatory peritoneal dialysis, classically four manual exchanges of about two litres across the day with a long overnight dwell — and APD — automated peritoneal dialysis, where a cycler performs exchanges overnight and the day is free, often with a single daytime dwell [6]. The choice between them is again a life-fit: CAPD needs no machine and travels well; APD frees the day for work and family and allows more flexible clearance [6] [20].
The peritoneal equilibration test (PET) characterises the individual membrane: how fast creatinine equilibrates and glucose absorbs over a standardised dwell. Fast transporters clear solute quickly but absorb glucose and lose ultrafiltration on long dwells — they suit shorter, cycler-driven exchanges and icodextrin for the long dwell; slow transporters need longer dwells to clear solute [6]. This is the physiology behind the answer "PD prescriptions are individualised, and residual urine output is factored into the weekly target" [6] [26].
Adequacy in PD has its own landmark. The ADEMEX trial randomised PD patients to standard versus increased peritoneal clearances and found no survival benefit from pushing small-solute clearance higher — ending the era of chasing weekly Kt/V numbers and refocusing the field on volume status, residual function and clinical wellbeing [14]. The modern adequacy question in PD is "is the patient well, euvolaemic and biochemically acceptable, with residual function protected?" rather than "is the Kt/V maximal?" [14] [26].
Exit-site care is prevention, daily. The catheter exit site is the peritoneum's front door: daily cleaning, immobilisation of the catheter, prompt treatment of any erythema, crusting or discharge, and topical prophylaxis per unit protocol; exit-site and tunnel infections track directly with subsequent peritonitis and catheter loss, which is why the ISPD publishes dedicated catheter-infection recommendations [13].
PD peritonitis — cloudy bag means treat now
Peritonitis is PD's signature emergency and the exam's favourite acute scenario. The presentation is cloudy effluent — the patient often notices the bag looks like dirty water before any pain — plus abdominal pain, and sometimes fever; the diagnosis is confirmed on effluent white cell count above 100 cells per microlitre with neutrophil predominance (above 50%) after a dwell of at least two hours, and culture of the effluent, taken before antibiotics, in blood-culture bottles to maximise yield [12].
PD peritonitis — the consultant sequence
Suspect on the bag
Cloudy effluent plus or minus pain and fever — instruct patients to bring the cloudy bag, not a description of it
Sample before antibiotics
Effluent cell count and differential, Gram stain, effluent culture in blood-culture bottles; blood cultures if systemically unwell
Start empiric intraperitoneal antibiotics now
Cover gram-positive AND gram-negative organisms — e.g. vancomycin or cefazolin PLUS ceftazidime (or an aminoglycoside), dosed intraperitoneally per unit protocol
Tailor by organism
Coagulase-negative staph about 2 weeks; S. aureus, Pseudomonas and enteric gram-negatives about 3 weeks; add antifungal cover and plan removal if yeast grows
Review at day 3-5
Falling cell count and clinical improvement continue; no improvement by day 5 = refractory peritonitis — remove the catheter
Prevent the next one
Root-cause review of technique, exit site, recent procedures; retrain; antifungal prophylaxis with antibiotic courses per ISPD
Empiric therapy covers both sides of the Gram stain because touch contamination drives gram-positive disease (coagulase-negative staphylococci, Staphylococcus aureus) while bowel-source and water organisms drive gram-negative disease (including Pseudomonas); intraperitoneal dosing achieves local concentrations intravenous dosing cannot, and the patient is usually managed as an outpatient after teaching [12]. Duration is organism-directed — roughly two weeks for coagulase-negative staphylococci, three weeks for S. aureus, Pseudomonas and enteric gram-negatives — with Pseudomonas and other difficult organisms often warranting two active agents [12].
Catheter removal is the decision the DWE probes. The ISPD defines the removal triggers [12]:
- Fungal peritonitis — remove promptly; antifungals alone do not eradicate a colonised catheter, and delay worsens outcomes [12].
- Refractory peritonitis — no clinical response or falling cell count by day 5 of appropriate therapy [12].
- Relapsing peritonitis — same organism (or sterile culture) recurring within four weeks of completing antibiotics — the biofilm has won [12].
- Recurrent peritonitis — a different organism within four weeks — consider removal, especially with a second episode or a tunnel infection [12].
- Peritonitis with concurrent exit-site or tunnel infection by the same organism, and refractory exit-site or tunnel infection, also push toward removal [12] [13].
After removal for peritonitis the patient usually converts to haemodialysis — with a defined subset returning to PD after an interval once the abdomen has settled, provided membrane function and motivation survive [12] [6].
Complications — the burden the membrane carries
Beyond peritonitis and access, four complication clusters structure the consultant's surveillance [5] [16]:
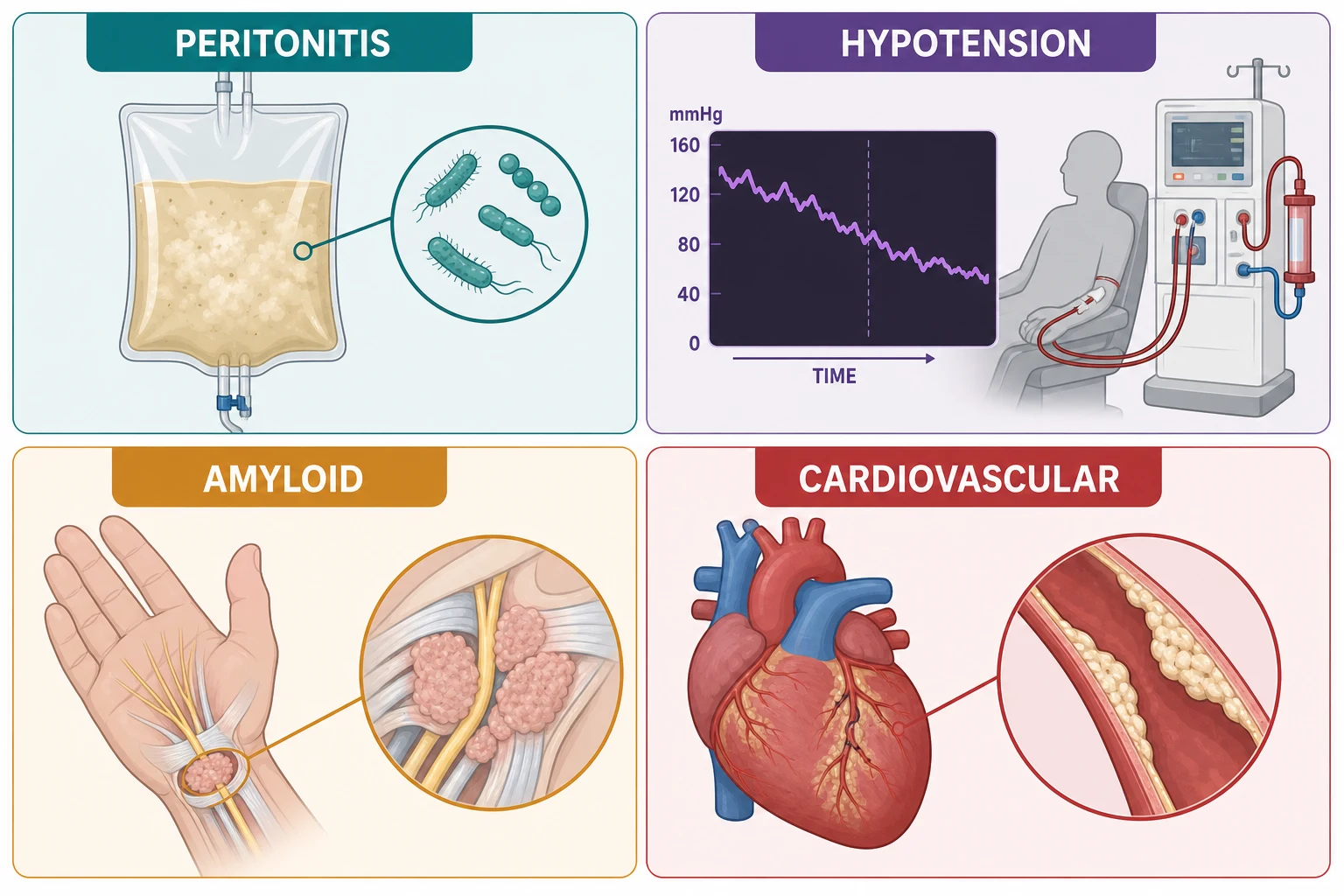
Intradialytic hypotension is the everyday cardiovascular insult — symptomatic falls in blood pressure during ultrafiltration, driven by the mismatch between fluid removal and vascular refilling, worsened by antihypertensives, food during dialysis, low dialysate sodium and cardiac disease. Its deeper significance is myocardial stunning: McIntyre's group showed that haemodialysis acutely reduces global and segmental myocardial blood flow, producing transient regional wall-motion abnormalities — a reversible ischaemia that recurs three times weekly and accumulates into fixed ventricular damage over years [16]. Management is preventive: probe dry weight cautiously, extend time or frequency rather than accelerate ultrafiltration, cool the dialysate, review antihypertensive timing, and avoid large intradialytic meals [16] [5].
The cardiovascular burden is the mortality story. Cardiovascular disease is the leading cause of death in the dialysis population — a burden established from early CKD and amplified by volume overload, hypertension, mineral-bone disorder with vascular calcification, anaemia, and the intradialytic stress itself; classic epidemiology showed the dialysis patient's cardiovascular death rate is orders of magnitude above age-matched controls [17] [16]. This is why volume and blood pressure are treated as organ-protective therapy, why dry weight is revisited monthly, and why the holistic bundle below is not housekeeping [17] [2].
Dialysis-related amyloidosis is the long-horizon complication: beta-2 microglobulin, a middle molecule poorly cleared by conventional membranes, deposits as amyloid in osteoarticular tissue over years of dialysis — the syndromes are carpal tunnel syndrome (often bilateral in the long-term dialysis patient), shoulder pain with joint effusions, destructive spondyloarthropathy and bone cysts with pathological fracture [23]. It is rarer with modern biocompatible high-flux membranes and best prevented by transplantation, but the bilateral carpal tunnel in a ten-year dialysis patient remains a DCE short-case and DWE staple [23].
The PD-specific long tail completes the picture: hernias and leaks from raised intra-abdominal pressure, weight gain and dysglycaemia from glucose absorption, ultrafiltration failure as the membrane remodels over years, and the rare but feared encapsulating peritoneal sclerosis — a cocooning fibrosis of the bowel associated with long PD vintage and severe peritonitis, presenting with obstructive symptoms and malnutrition, with high mortality [15] [6].
Special situations — urgent starts, pregnancy, the frail elderly
Urgent start without access. When a patient presents needing dialysis within days — late referral, crashed transplant, rapid decline — the standard path is a temporary or tunneled central venous catheter plus haemodialysis for the emergency indications (refractory hyperkalaemia, severe acidosis, pulmonary oedema, pericarditis, encephalopathy), with permanent access planning beginning the same week so the catheter stays a bridge [7] [27]. Urgent-start PD — catheter in, low-volume exchanges within days in a supine position — is a validated alternative in experienced centres, and meta-analytic data show comparable short-term outcomes to urgent-start HD with fewer catheter-related bloodstream infections; it suits the stable patient without urgent ultrafiltration needs and is a genuinely examinable modern nuance [27].
Pregnancy. Dialysis-dependent women can and do carry pregnancies, and outcomes have improved with intensified regimens — long, frequent haemodialysis sessions (often nocturnal, mimicking physiology, improving volume and blood-pressure control) with close maternal-fetal surveillance; a 2025 multinational cohort of dialysis initiation during pregnancy confirmed that intensive schedules and multidisciplinary care are the frame, with prematurity the dominant residual risk [22]. The consultant points: pregnancy does not contraindicate dialysis, intensity is the lever, and pre-pregnancy transplantation remains the best fertility-preserving renal replacement [22] [3].
The frail elderly patient is where modality philosophy is tested. The BOLDE study of older patients found quality of life on peritoneal dialysis at least comparable to haemodialysis, with some domains favouring PD — supporting home-based therapy in a group that struggles with thrice-weekly transport [20]. Where dexterity or cognition fails, assisted PD — a trained nurse or family member performing exchanges — extends home therapy to patients who could never do it alone, and the ISPD's 2024 position paper endorses it as standard practice rather than an exception [21]. Home haemodialysis suits the motivated few with a care partner; in-centre HD suits those who need supervision; and conservative kidney management — structured, symptom-focused, with advance care planning — is the honest offer when dialysis would add burden without meaningful benefit, with observational data showing the survival advantage of dialysis attenuates in the oldest, frailest, most comorbid patients while quality of life on the conservative pathway is preserved [18] [2].
The holistic frame — dialysis is not just a machine
The long-case examiner listens for the bundle, because it is where consultants separate from registrars [2]:
- Cardiovascular and volume care — dry-weight review, blood-pressure targets individualised, salt and fluid restriction education, echocardiographic surveillance in high-risk patients [17] [16].
- Anaemia management — iron repletion first, then an ESA titrated to avoid the fully-normalised haemoglobin that trials showed buys nothing and costs strokes: in TREAT, darbepoetin targeting a higher haemoglobin in diabetic CKD gave no cardiovascular or renal benefit and increased stroke — the ceiling principle now governs dosing [19].
- Mineral-bone disorder — dietary phosphate restriction, phosphate binders with meals, active vitamin D and calcimimetics per PTH trajectory, because vascular calcification is part of the mortality story [17] [2].
- Vaccination and infection prevention — influenza, pneumococcal, COVID-19 and hepatitis B (with post-vaccine titres given blunted responses in kidney failure) [2].
- Nutrition — adequate protein intake once on dialysis (the pre-dialysis restriction lifts), with dietetic review of potassium, phosphate, salt and fluid [2].
- Advance care planning — started at modality education, revisited at every health change, including explicit conversations about what dialysis withdrawal would look like if the balance ever tips [2] [18].
- Transplant re-evaluation — the list status, cardiovascular fitness and donor conversations reviewed periodically; dialysis is the bridge, and the bridge is not the destination [3].
DCE angles — how this topic is examined
The long case is the multimorbid patient approaching end-stage and choosing: the 58-year-old with diabetic CKD5, eGFR 9 and no symptoms yet; or the 67-year-old with ischaemic heart disease, frailty and a eGFR of 8 — transplant listing (fit? work-up?), modality reasoning (PD independence versus supervised HD versus conservative care), access timing (fistula referred six months ago — matured?), and the goals-of-care defence that integrates comorbidity, cognition, home support and the patient's own priorities [4] [18] [2]. The examiner's arc runs: start with the transplant question, reason the modality, time the access, name the triggers you would start for, manage the cardiovascular burden, and close with the advance care plan — every limb has evidence to quote [1] [3] [17].
The short case is the arteriovenous fistula examination. Inspect the arm for scars (which side, which level — a radiocephalic scar at the wrist and a brachiocephalic scar at the elbow tell the access history), aneurysmal dilatation, collateral chest-wall veins (central stenosis), and trophic changes in the hand. Palpate the thrill at the anastomosis and along the vein — a continuous, machinery-like buzz means flow; a water-hammer pulse with no thrill means stenosis. Auscultate the continuous bruit with systolic accentuation. Assess steal: hand temperature, capillary refill, and relief of hand symptoms when the fistula is compressed. Then the synthesis sentence: "a functioning left radiocephalic fistula with a strong thrill and no steal, aneurysm or infection" — and offer to examine fluid status and the heart, because volume and LVH complete the dialysis examination [7] [16].
Exam traps, collected
References
- [1]Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis N Engl J Med, 2010.PMID 20581422
- [2]Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease Kidney Int, 2024.PMID 38490803
- [3]Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant N Engl J Med, 1999.PMID 10580071
- [4]Mehrotra R, Chiu YW, Kalantar-Zadeh K, et al. Similar outcomes with hemodialysis and peritoneal dialysis in patients with end-stage renal disease Arch Intern Med, 2011.PMID 20876398
- [5]Himmelfarb J, Ikizler TA. Hemodialysis N Engl J Med, 2010.PMID 21047227
- [6]Teitelbaum I, Glickman J, Neu A, et al. Peritoneal Dialysis N Engl J Med, 2021.PMID 34731538
- [7]Lok CE, Huber TS, Lee T, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update Am J Kidney Dis, 2020.PMID 32778223
- [8]National Kidney Foundation KDOQI Clinical Practice Guideline for Hemodialysis Adequacy: 2015 update Am J Kidney Dis, 2015.PMID 26498416
- [9]Eknoyan G, Beck GJ, Cheung AK, et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis N Engl J Med, 2002.PMID 12490682
- [10]FHN Trial Group, Chertow GM, Levin NW, et al. In-center hemodialysis six times per week versus three times per week N Engl J Med, 2010.PMID 21091062
- [11]Rocco MV, Lockridge RS Jr, Beck GJ, et al. Long-term Effects of Frequent Nocturnal Hemodialysis on Mortality: The Frequent Hemodialysis Network (FHN) Nocturnal Trial Am J Kidney Dis, 2015.PMID 25863828
- [12]Li PK, Chow KM, Cho Y, et al. ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment Perit Dial Int, 2022.PMID 35264029
- [13]Chow KM, Li PK, Cho Y, et al. ISPD Catheter-related Infection Recommendations: 2023 Update Perit Dial Int, 2023.PMID 37232412
- [14]Paniagua R, Amato D, Vonesh E, et al. Effects of increased peritoneal clearances on mortality rates in peritoneal dialysis: ADEMEX, a prospective, randomized, controlled trial J Am Soc Nephrol, 2002.PMID 11961019
- [15]Johnson DW, Cho Y, Livingston BE, et al. Encapsulating peritoneal sclerosis: incidence, predictors, and outcomes Kidney Int, 2010.PMID 20375981
- [16]McIntyre CW, Burton JO, Selby NM, et al. Hemodialysis-induced cardiac dysfunction is associated with an acute reduction in global and segmental myocardial blood flow Clin J Am Soc Nephrol, 2008.PMID 18003765
- [17]Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease Am J Kidney Dis, 1998.PMID 9820470
- [18]Da Silva-Gane M, Wellsted D, Greenshields H, et al. Quality of life and survival in patients with advanced kidney failure managed conservatively or by dialysis Clin J Am Soc Nephrol, 2012.PMID 22956262
- [19]Pfeffer MA, Burdmann EA, Chen CY, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease N Engl J Med, 2009.PMID 19880844
- [20]Brown EA, Johansson L, Farrington K, et al. Broadening Options for Long-term Dialysis in the Elderly (BOLDE): differences in quality of life on peritoneal dialysis compared to haemodialysis for older patients Nephrol Dial Transplant, 2010.PMID 20400451
- [21]Oliver MJ, Crabtree JH, McCarthy M, et al. Assisted peritoneal dialysis: Position paper for the ISPD Perit Dial Int, 2024.PMID 38712887
- [22]Yo JH, Jesudason S, Hewawasam E, et al. A Multinational Cohort Study of Dialysis Initiation During Pregnancy Kidney Int Rep, 2025.PMID 40677311
- [23]Scarpioni R, Ricardi M, Albertazzi V, et al. Dialysis-related amyloidosis: challenges and solutions Int J Nephrol Renovasc Dis, 2016.PMID 27994478
- [24]Pisoni RL, Young EW, Dykstra DM, et al. Vascular access use in Europe and the United States: results from the DOPPS Kidney Int, 2002.PMID 11786113
- [25]Pisoni RL, Zepel L, Fluck R, et al. International Comparisons of Native Arteriovenous Fistula Patency and Time to Becoming Catheter-Free: Findings From the Dialysis Outcomes and Practice Patterns Study (DOPPS) Am J Kidney Dis, 2021.PMID 32971192
- [26]Tanriover C, Gokal R, Kanbay M, et al. On the importance of the interplay of residual renal function with clinical outcomes in end-stage kidney disease J Nephrol, 2022.PMID 35819749
- [27]Wu J, Chen Y, Zhao X, et al. A Comparison of Clinical Outcomes in Urgent-Start Hemodialysis versus Urgent-Start Peritoneal Dialysis in End-Stage Renal Disease Patients: A Systematic Review and Meta-Analysis Blood Purif, 2025.PMID 40555200