Phys · respiratory
Lung Cancer
Also known as bronchogenic carcinoma · non-small-cell lung cancer · NSCLC · small-cell lung cancer · SCLC · solitary pulmonary nodule · SPN · lung adenocarcinoma · squamous cell carcinoma of lung · lung cancer screening · LDCT
Consultant-physician-depth guide to lung cancer — the solitary pulmonary nodule workup, tissue and mediastinal staging, stage-mapped treatment intent, biomarker-first stage IV NSCLC therapy (EGFR, ALK, ROS1, KRAS G12C, PD-L1), SCLC as a fundamentally different disease, LDCT screening eligibility, oncological emergencies and early palliative care — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Lung Cancer

The answer first
Lung cancer is managed as two different diseases that happen to share an organ, and every exam answer starts by saying which one you are dealing with [7]. Non-small-cell lung cancer (NSCLC — about 85% of cases) is a staging and biomarker disease: stage decides whether the intent is cure or control, and molecular testing decides which drug comes first in advanced disease [14] [18]. Small-cell lung cancer (SCLC — about 15%) is a tempo disease: it is systemic at diagnosis, exquisitely chemosensitive, and almost always relapses — so it has its own two-stage system (limited vs extensive), its own regimen, and its own rules [22].
Three working rules carry most DWE and DCE answers [14] [26]:
- Tissue first, and enough of it. Diagnosis is histological, and in non-squamous NSCLC the biopsy must be large enough for molecular testing (EGFR, ALK, ROS1, KRAS, PD-L1 at minimum) — treatment in advanced disease now waits for those results [7].
- Stage decides intent; biomarkers decide drugs. Surgery or stereotactic radiation for early disease, chemoradiotherapy plus durvalumab for unresectable stage III, and biomarker-directed therapy for stage IV — a sequence you should be able to recite as one sentence [12] [18].
- Palliation is not the alternative to treatment — it runs beside it. Early palliative care alongside active treatment in metastatic NSCLC improved quality of life and, remarkably, survival in the landmark Temel trial [26].
Two diseases, one organ
The single most common exam error in lung cancer is treating SCLC like NSCLC. They differ in cell of origin, doubling time, metastatic behaviour, staging, drugs and prognosis — different diseases in every meaningful sense [22].
| Feature | NSCLC (about 85%) | SCLC (about 15%) |
|---|---|---|
| Histologies | Adenocarcinoma, squamous cell, large cell | Small-cell (neuroendocrine) carcinoma [7] |
| Typical location | Adenocarcinoma peripheral; squamous central | Central, perihilar mass with bulky nodes |
| Tempo | Months; metastasis later | Weeks; systemic at diagnosis |
| Staging | TNM stage groups I–IV | Limited vs extensive (TNM underlies it) |
| Curative-intent options | Surgery, SBRT, chemoRT + durvalumab | Concurrent chemoRT (limited stage only) |
| First-line systemic driver | Biomarker (EGFR/ALK/ROS1/KRAS/PD-L1) | Platinum–etoposide ± atezolizumab [22] |
| Paraneoplastic signature | Hypercalcaemia (squamous, PTHrP), clubbing/HPOA | SIADH, Lambert-Eaton, ACTH [25] |
| Surgery | Central to early-stage cure | Almost never a role |
The 2021 WHO classification now treats molecular profiling as integral to the pathology report rather than an add-on: lung adenocarcinoma is described alongside its driver genotype, and the report you request should anticipate that [7].
How lung cancer presents
Presentation divides into local, metastatic and paraneoplastic — and the examiner wants you to walk all three shelves, because a cough is how it starts but SIADH is how the DWE tests it [25].
| Shelf | Features | The trap it sets |
|---|---|---|
| Local | Persistent new cough, haemoptysis, dyspnoea, chest wall pain, post-obstructive pneumonia, hoarseness (recurrent laryngeal nerve), stridor | Pneumonia that recurs in the same lobe or fails to clear is an obstructing tumour until scoped [25] |
| Metastatic | Bone pain or fracture, neurological symptoms (brain), weight loss, anorexia, hepatomegaly, supraclavicular node | Back pain with any neurology is cord compression until MRI proves otherwise |
| Paraneoplastic | SIADH (SCLC), hypercalcaemia via PTHrP (squamous), Lambert-Eaton myasthenic syndrome (SCLC), clubbing and hypertrophic pulmonary osteoarthropathy, dermatomyositis, ACTH production | Lambert-Eaton: proximal weakness that improves with activity, autonomic dry mouth, hyporeflexia — the reverse of myasthenia [25] |
Apical (Pancoast) tumours deserve their own sentence: shoulder and arm pain from C8–T2 invasion, Horner syndrome (ptosis, miosis, anhidrosis) from sympathetic chain involvement, and wasting of the hand muscles — a superior sulcus tumour until proven otherwise [25].
The solitary pulmonary nodule
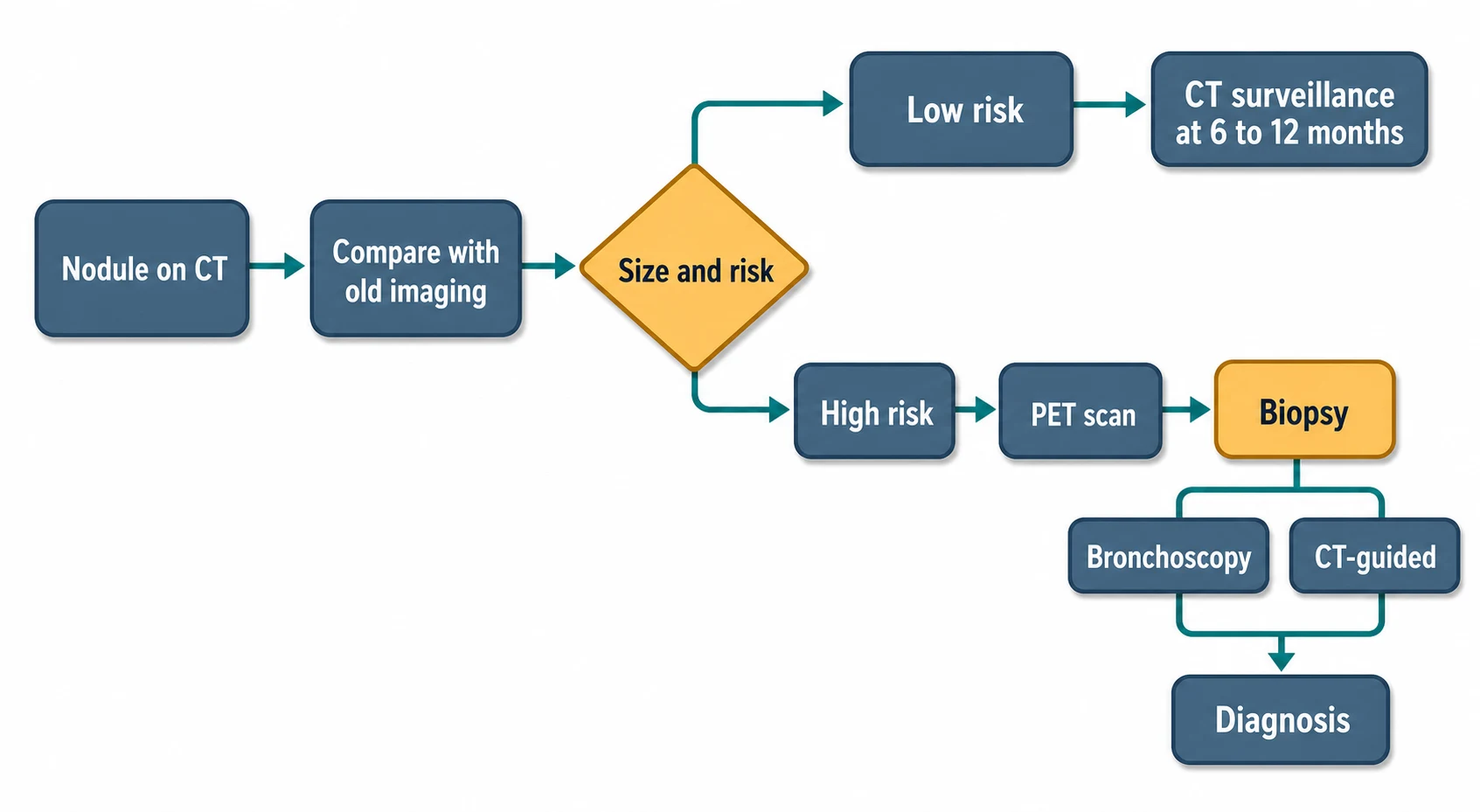
A solitary pulmonary nodule (SPN) is a rounded opacity up to 3 cm, surrounded by aerated lung, without atelectasis or adenopathy. The workup is a probability problem: estimate malignancy risk from the patient and the nodule, then choose surveillance, functional imaging or biopsy [4] [5].
The first move is always the same: find the old imaging. A solid nodule unchanged for 2 years is effectively benign; growth on serial imaging overrides every other feature [4].
Risk stratification uses patient factors (age, smoking, emphysema, family history) and nodule factors (size — the dominant variable, spiculation, upper-lobe location, part-solid morphology, growth). The Brock (PanCan) model, derived and validated in screening cohorts, combines exactly these variables into a malignancy probability and outperforms gestalt — name it in the exam [5].
| Solid nodule size (Fleischner 2017, incidental nodules, low vs high risk) | Management |
|---|---|
| Below 6 mm | Low risk: no routine follow-up. High risk: optional CT at 12 months [4] |
| 6–8 mm | CT at 6–12 months, then consider CT at 18–24 months (high risk) [4] |
| Above 8 mm | Consider CT at 3 months, PET/CT, or tissue sampling depending on risk [4] |
Sub-solid nodules behave differently and grow more slowly: a persistent pure ground-glass nodule 6 mm or larger warrants surveillance for years (adenocarcinoma spectrum moves slowly), and a part-solid nodule's solid component drives both risk and management [4].
PET is the middle step for nodules above 8 mm: FDG-avid nodules escalate to tissue; a negative PET in a small nodule lowers but does not abolish risk (false negatives in small, ground-glass and low-metabolism tumours such as carcinoid) [4].
Tissue, and enough of it
Diagnosis is histological, and the modern biopsy has two jobs: confirm malignancy and yield enough material for molecular testing. Choose the route by lesion location and by what staging information you need at the same sitting [6].
| Route | Best for | Watch for |
|---|---|---|
| CT-guided percutaneous biopsy | Peripheral nodules and masses; pleural-based lesions | Pneumothorax (commonest complication); haemorrhage |
| Bronchoscopy (with radial EBUS / navigation) | Central lesions, endobronchial disease, selected peripheral nodules | Lower yield for small peripheral targets; safer in emphysema |
| EBUS-TBNA (± EUS) | Mediastinal and hilar nodes — diagnosis AND staging in one procedure | Negative nodes in high-suspicion staging still need surgical confirmation [6] |
| Surgical biopsy (VATS) | Nodules where less invasive routes fail or the plan is resect-and-diagnose | A diagnostic step that becomes the curative step |
| Accessible metastasis (node, skin, pleura, effusion cytology) | Stage IV disease — confirms stage and histology together | Effusion cytology must still yield enough cells for molecular panels |
The mediastinum is the pivotal staging question for operability, and endosonography has replaced mediastinoscopy as the first invasive test: the ASTER randomised trial showed that starting with endosonography (EBUS plus EUS) and reserving mediastinoscopy for negative results gave higher sensitivity than mediastinoscopy alone, with fewer futile thoracotomies [6].
Staging: the intent map
NSCLC staging is TNM — T by size and local invasion, N by nodal station, M by distant spread — collapsed into stage groups that map directly onto treatment intent. Learn the map, not every T-subcategory: the exam product is the stage-to-intent sentence [12].
| Stage | Essence | Treatment intent |
|---|---|---|
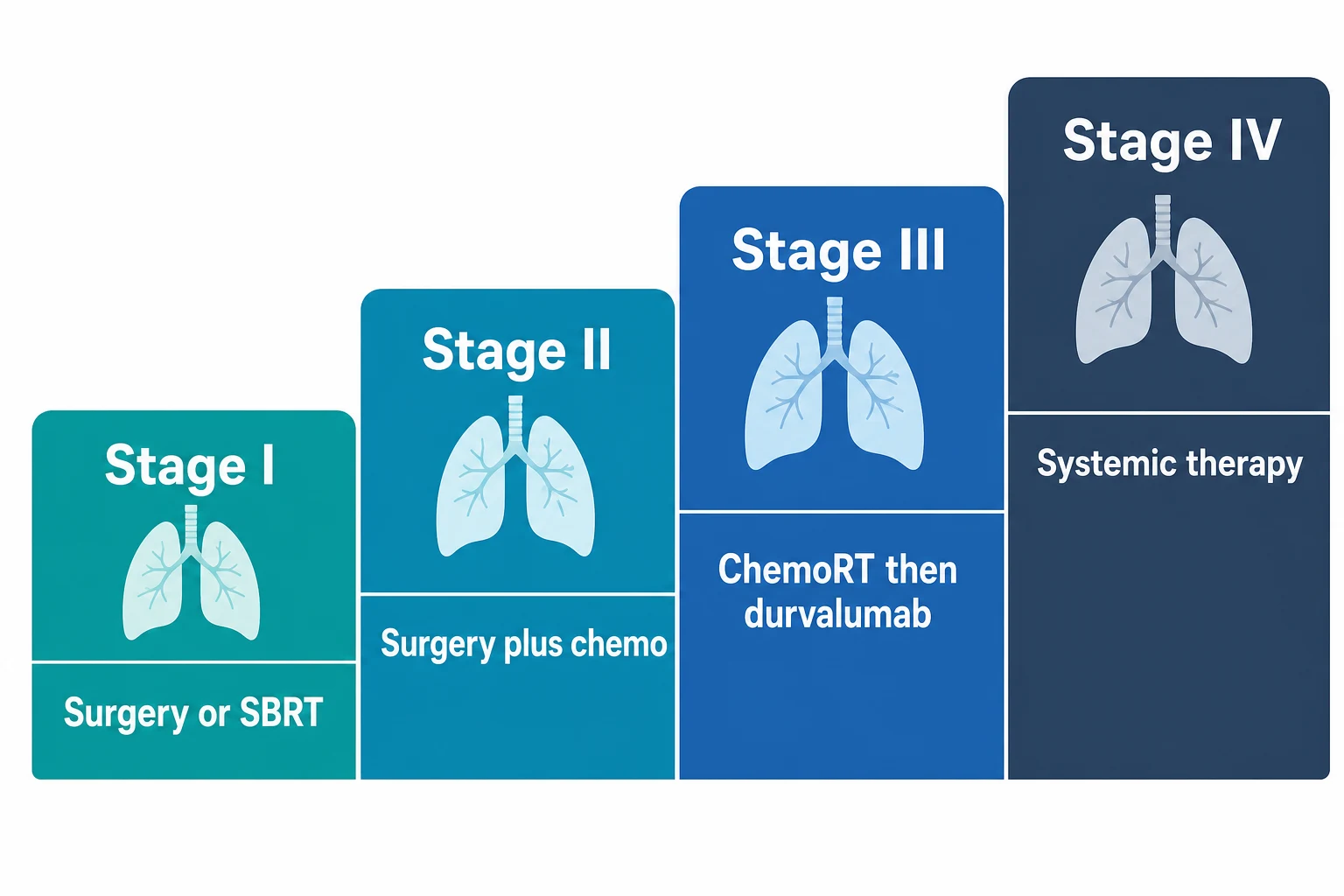
| I | Localised, no nodes | Curative: anatomical resection; SBRT if medically inoperable [8] |
| II | Larger tumour or hilar (N1) nodes | Curative: resection plus adjuvant therapy [9] |
| III | Locally advanced, mediastinal (N2/N3) nodes | Potentially curative: concurrent chemoRT then durvalumab for unresectable disease; multimodality selection for resectable disease [12] |
| IV | Distant metastases (including malignant effusion, contralateral lung nodules) | Control: biomarker-directed systemic therapy plus palliation [18] |
The staging workup is a contrast CT of chest and upper abdomen, PET-CT to find occult nodal and distant disease (and to direct biopsy), brain imaging when symptoms suggest or when stage III-or-worse disease is being staged for curative treatment, and invasive mediastinal staging when nodes are enlarged, PET-avid or centrally located [6]. Stage shifts treatment; confirm before you commit — a PET-hot node needs cytology before it denies someone surgery [6].
Early-stage NSCLC: cure is the job
Surgery — anatomical lobectomy with systematic lymph-node dissection, usually by VATS — is the standard for stage I–II (and selected IIIA) NSCLC in patients fit enough to tolerate it. Fitness is physiological, not chronological: FEV1 and DLCO (with predicted post-operative values), exercise testing where borderline, and cardiac optimisation — not the birthdate [8].
SBRT (stereotactic ablative body radiotherapy) is the answer for medically inoperable early disease: RTOG 0236 delivered local control around 90% at 3 years in inoperable stage I patients, and SBRT is now the default non-surgical curative option for small peripheral tumours [8].
Adjuvant therapy has become genotype- and stage-specific — this is where the modern DWE lives [9]:
- Platinum-doublet chemotherapy after resection of node-positive (and selected high-risk stage IB) disease — the long-standing backbone.
- Osimertinib for 3 years after resection of EGFR-mutant stage IB–IIIA disease: ADAURA showed a dramatic disease-free-survival benefit (2-year DFS 90% vs 44% in stage II–IIIA), with overall-survival benefit confirmed on follow-up — so resected tissue must be genotyped, not just histotyped [9].
- Pembrolizumab after resection (± chemotherapy) improved disease-free survival in KEYNOTE-091, establishing adjuvant immunotherapy as an option in driver-negative disease [11].
- Neoadjuvant chemo-immunotherapy moved earlier still: CheckMate 816 gave nivolumab plus platinum-doublet chemotherapy before surgery and improved event-free survival and pathological complete response (24% vs 2.2%) without delaying operations — know it as the "treat before the knife" shift [10].
Early-stage NSCLC — the current standard set
Stage III NSCLC: the consolidation concept
Unresectable stage III NSCLC used to mean concurrent chemoradiotherapy and hope. PACIFIC changed the grammar: after concurrent platinum-based chemoRT without progression, durvalumab consolidation for 12 months improved progression-free survival (16.8 vs 5.6 months) and overall survival — and is now the global standard [12].
Two exam nuances matter. First, durvalumab is consolidation after chemoRT, not a replacement for it — the sequence (platinum doublet with thoracic radiation, then immunotherapy) is the answer. Second, EGFR-mutant stage III is a special case: LAURA showed osimertinib after chemoRT dramatically improved progression-free survival in EGFR-mutant unresectable stage III disease — genotype reaches even the stage III pathway [13].
Stage IV NSCLC: biomarker first, always
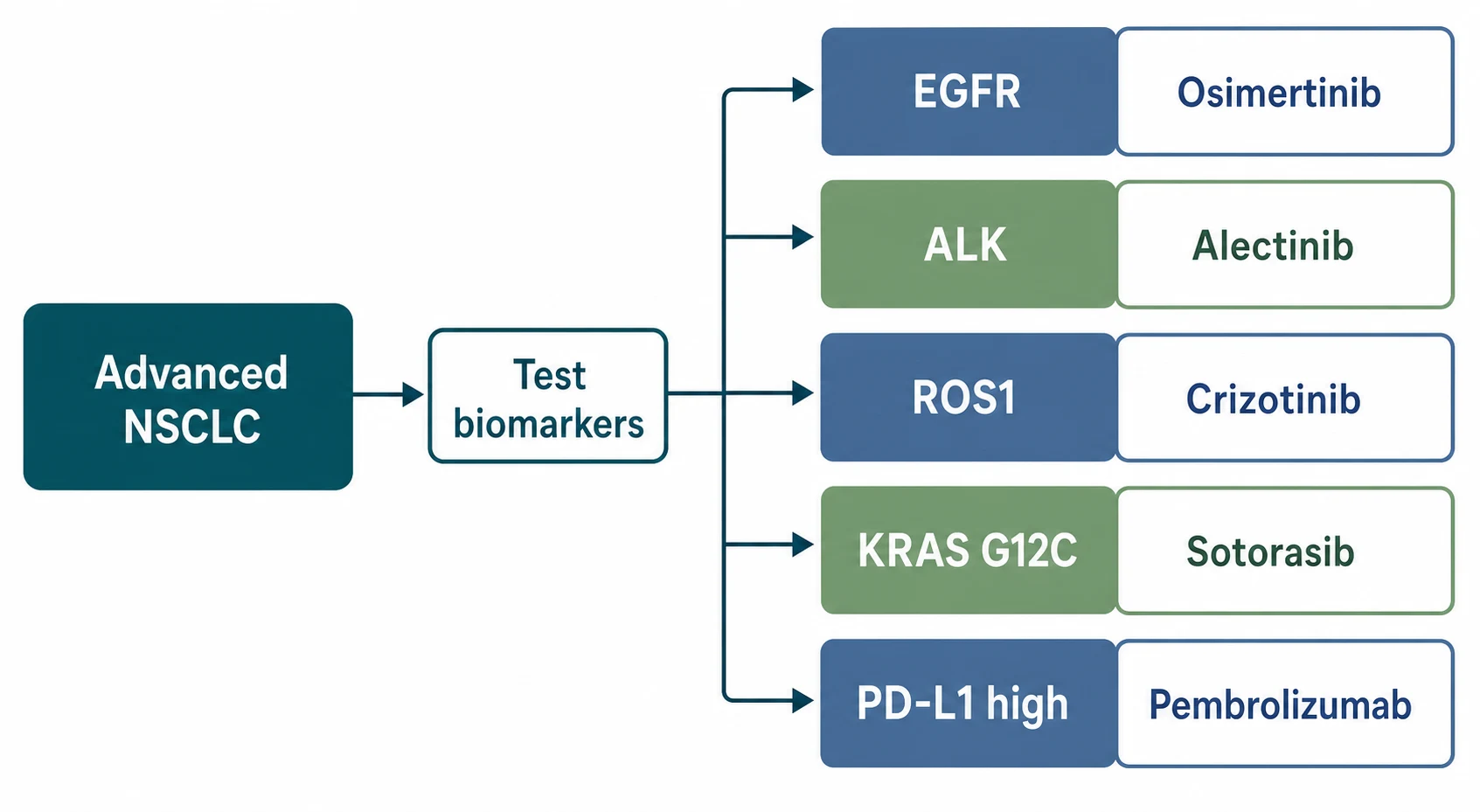
Advanced non-squamous NSCLC is a genotype-first disease. The first consultation ends with molecular results pending, not with chemotherapy started — because the right first drug roughly doubles progression-free survival compared with the wrong one [14].
| Biomarker | First-line drug | Landmark trial | What it showed |
|---|---|---|---|
| EGFR mutation (exon 19 deletion, L858R) | Osimertinib | FLAURA | PFS 18.9 vs 10.2 months vs first-generation EGFR TKI; superior CNS penetration; OS benefit followed [14] |
| ALK rearrangement | Alectinib | ALEX | Alectinib beat crizotinib on PFS and dramatically on CNS control — next-generation ALK inhibitors became first-line [15] |
| ROS1 rearrangement | Crizotinib (entrectinib alternative) | PROFILE 1001 | High and durable response rates in ROS1-rearranged disease [16] |
| KRAS G12C | Sotorasib (after prior therapy) | CodeBreaK 100 | First proof that "undruggable" KRAS was druggable — objective responses in previously treated disease [17] |
| PD-L1 at least 50%, no driver | Pembrolizumab monotherapy | KEYNOTE-024 | Pembrolizumab beat platinum chemotherapy on PFS and OS with less toxicity [18] |
| No driver, any PD-L1 (non-squamous) | Pembrolizumab + pemetrexed-platinum | KEYNOTE-189 | Chemo-immunotherapy improved OS across PD-L1 subgroups (12-month OS 69% vs 49%) [19] |
The intellectual origin of the genotype-first rule is IPASS: gefitinib beat chemotherapy only in the EGFR-mutant subgroup and was worse in unselected patients — the trial that taught oncology to test before it treats [20].
Resistance is expected, not exceptional. EGFR-mutant disease on osimertinib progresses at a median of about 18–19 months; the consultant move is to re-biopsy at progression (tissue or liquid) to find the resistance mechanism — MET amplification, small-cell transformation, targetable second-site mutations — because a proportion of progressions have a directed next step, and oligoprogression may be managed with local therapy while the TKI continues [14].
Squamous and driver-negative non-squamous disease without a targetable lesion is immunotherapy territory: pembrolizumab alone when PD-L1 is at least 50%, chemo-immunotherapy combinations otherwise — with pemetrexed reserved for non-squamous histology, a classic prescribing-checkpoint in the DWE [18] [19].
SCLC: the other disease
SCLC announces itself as a bulky central mass with early nodal and distant spread — and the two-stage question limited or extensive replaces the TNM grammar of NSCLC. Limited means confined to one hemithorax within a tolerable radiation field; everything else is extensive [21].
Limited stage is treated with curative intent: concurrent platinum–etoposide with thoracic radiotherapy. Turrisi established that twice-daily radiation (45 Gy in 30 twice-daily fractions over 3 weeks) beat once-daily schedules — median survival 23 vs 19 months, 5-year survival 26% vs 16% — and concurrent-early radiation remains the standard [21].
Extensive stage is treated with chemo-immunotherapy: IMpower133 added atezolizumab to carboplatin–etoposide and improved overall survival (12.3 vs 10.3 months) — the first advance in the first-line treatment of extensive SCLC in decades, and now the default [22].
Prophylactic cranial irradiation (PCI) exists because the brain is SCLC's sanctuary site: Slotman showed PCI reduced brain metastases and improved survival even in extensive-stage responders — modern practice individualises PCI against MRI surveillance, especially in extensive disease and older patients [23].
The physician's honesty point: SCLC responds dramatically and relapses aggressively. First-line responses are the rule; durable control is the exception. Say so early, plan the goals-of-care conversation while treatment is working, and treat relapse as a new urgency rather than a surprise [22].
Screening: who, with what, and why
Lung cancer screening is one of the few cancer-screening programs with mortality-level randomised evidence [1] [2].
| Trial | Population | Intervention | Result |
|---|---|---|---|
| NLST | 53,454 people aged 55–74, at least 30 pack-years, current smokers or quit within 15 years | Annual low-dose CT ×3 vs chest X-ray | 20% relative reduction in lung-cancer mortality; all-cause mortality also reduced [1] |
| NELSON | People aged 50–74 with substantial smoking history | Volumetric LDCT screening vs no screening | About 24% mortality reduction in men at 10 years; volume-based nodule protocols cut false positives [2] |
The USPSTF 2021 recommendation operationalises this: annual LDCT for adults aged 50–80 with at least a 20 pack-year history who currently smoke or quit within the past 15 years — a grade B recommendation [3].
The harms belong in the same answer: false-positive nodules leading to downstream procedures, overdiagnosis of indolent tumours, and cumulative radiation. Nodule-management protocols (Lung-RADS, or volumetry as in NELSON) exist precisely to shrink the false-positive tail, and every screening conversation ends with smoking cessation — the intervention that outperforms the scan [2] [3].
Complications and the oncological emergencies
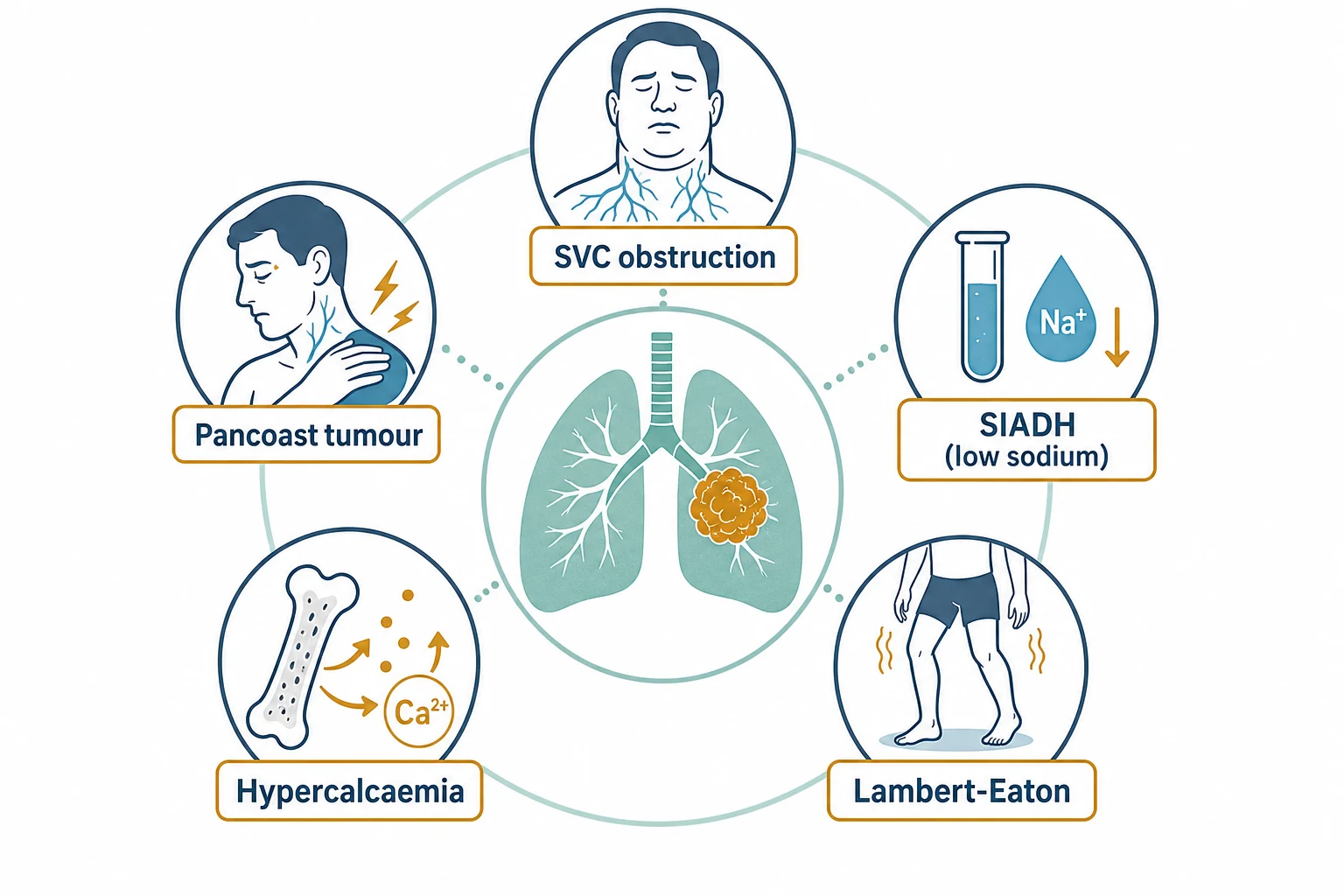
SVC obstruction is the emergency this topic owns. Lung cancer (and lymphoma) account for most malignant cases; presentation is facial and upper-limb swelling, venous engorgement, dyspnoea and headache worse on bending. Management in order: establish the diagnosis with imaging (CT with contrast), obtain tissue before definitive treatment (the pathology directs therapy — lymphoma is treated very differently from SCLC or NSCLC), consider endovascular stenting for severe or rapidly progressive obstruction (faster relief than radiotherapy), give radiotherapy or chemotherapy as disease-directed definitive treatment, and use steroids selectively rather than reflexively [24].
Spinal cord compression — back pain, weakness, sensory level, sphincter loss in a patient with known or suspected malignancy: same-day MRI of the whole spine, corticosteroids at the treating team's protocol dose, and urgent radiation-oncology ± surgical review. Delay costs neurology that does not return [25].
Malignant pleural effusion confirms stage IV disease and often provides the diagnostic specimen: therapeutic drainage for symptom relief, then definitive management of recurrence with an indwelling pleural catheter or pleurodesis — chosen with the patient's prognosis and preference in view [25].
Hypercalcaemia (PTHrP, classically squamous) presents as confusion, constipation, polyuria and dehydration: aggressive isotonic fluids first, then intravenous bisphosphonate, calcitonin for speed, and treatment of the underlying cancer as the only durable control [25].
Palliation: early, integrated, evidence-based
The Temel trial is the evidence anchor for the whole philosophy: patients with newly diagnosed metastatic NSCLC randomised to early palliative care integrated with oncology had better quality of life, less depression, less aggressive end-of-life care — and lived longer (median 11.6 vs 8.9 months) [26].
Practical palliation in lung cancer includes radiotherapy for bone pain, haemoptysis and airway obstruction; stenting for airway and SVC obstruction; breathlessness management with opioids, oxygen only where hypoxaemic, and fan therapy; drainage strategies for effusions; and honest advance-care planning while the patient is well enough to lead it [26].
The DCE angles
Long case. The examiner's favourite is the patient with lung cancer and multimorbidity — COPD with an FEV1 that questions operability, ischaemic heart disease, CKD that complicates platinum, or frailty that reframes every option. The marks live in the treatment-intent conversation: stating plainly whether the goal is cure, control or comfort; how fitness (physiological reserve, performance status, patient priorities) shapes each option; and how you would say it to the patient. The second classic is the never-smoker with EGFR-mutant disease on osimertinib — sequencing at progression, re-biopsy reasoning, and the goals-of-care conversation that evolves as options narrow [9] [14].
Short case. The respiratory examination with clubbing, a supraclavicular node and signs of lobar collapse or effusion is a complete station: describe the findings in order, name the unifying diagnosis, and offer the next step (confirm with imaging, then tissue — often the node itself is the kindest biopsy). Know Horner syndrome, SVC obstruction signs (facial plethora, venous engorgement, Pemberton sign) and hypertrophic pulmonary osteoarthropathy as the differentiating extras [24] [25].
Exam traps, collected
References
- [1]National Lung Screening Trial Research Team Reduced lung-cancer mortality with low-dose computed tomographic screening N Engl J Med, 2011.PMID 21714641
- [2]de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial N Engl J Med, 2020.PMID 31995683
- [3]US Preventive Services Task Force Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement JAMA, 2021.PMID 33687470
- [4]MacMahon H, Naidich DP, Goo JM, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017 Radiology, 2017.PMID 28240562
- [5]McWilliams A, Tammemagi MC, Mayo JR, et al. Probability of cancer in pulmonary nodules detected on first screening CT N Engl J Med, 2013.PMID 24004118
- [6]Annema JT, van Meerbeeck JP, Rintoul RC, et al. Mediastinoscopy vs endosonography for mediastinal nodal staging of lung cancer: a randomized trial JAMA, 2010.PMID 21098770
- [7]Nicholson AG, Scagliotti G, Tsao MS, et al. 2021 WHO Classification of Lung Cancer: A Globally Applicable and Molecular Biomarker-Relevant Classification J Thorac Oncol, 2022.PMID 36031295
- [8]Timmerman R, Paulus R, Galvin J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer JAMA, 2010.PMID 20233825
- [9]Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer N Engl J Med, 2020.PMID 32955177
- [10]Forde PM, Spicer J, Lu S, et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer N Engl J Med, 2022.PMID 35403841
- [11]O'Brien M, Paz-Ares L, Marreaud S, et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial Lancet Oncol, 2022.PMID 36108662
- [12]Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer N Engl J Med, 2017.PMID 28885881
- [13]Lu S, Kato T, Dong X, et al. Osimertinib after Chemoradiotherapy in Stage III EGFR-Mutated NSCLC N Engl J Med, 2024.PMID 38828946
- [14]Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer N Engl J Med, 2018.PMID 29151359
- [15]Peters S, Camidge DR, Shaw AT, et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non-Small-Cell Lung Cancer N Engl J Med, 2017.PMID 28586279
- [16]Shaw AT, Ou SH, Bang YJ, et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer N Engl J Med, 2014.PMID 25264305
- [17]Skoulidis F, Li BT, Dy GK, et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation N Engl J Med, 2021.PMID 34096690
- [18]Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer N Engl J Med, 2016.PMID 27718847
- [19]Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer N Engl J Med, 2018.PMID 29658856
- [20]Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma N Engl J Med, 2009.PMID 19692680
- [21]Turrisi AT 3rd, Kim K, Blum R, et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide N Engl J Med, 1999.PMID 9920950
- [22]Horn L, Mansfield AS, Szczęsna A, et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer N Engl J Med, 2018.PMID 30280641
- [23]Slotman B, Faivre-Finn C, Kramer G, et al. Prophylactic cranial irradiation in extensive small-cell lung cancer N Engl J Med, 2007.PMID 17699816
- [24]Wilson LD, Detterbeck FC, Yahalom J, et al. Clinical practice. Superior vena cava syndrome with malignant causes N Engl J Med, 2007.PMID 17476012
- [25]Pelosof LC, Gerber DE Paraneoplastic syndromes: an approach to diagnosis and treatment Mayo Clin Proc, 2010.PMID 20810794
- [26]Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer N Engl J Med, 2010.PMID 20818875