Phys · respiratory
Obstructive Sleep Apnoea
Also known as obstructive sleep apnoea · sleep apnea · OSA · OSAHS · sleep-disordered breathing · apnoea-hypopnoea index · AHI · CPAP · Epworth Sleepiness Scale · hypoglossal nerve stimulation · mandibular advancement splint · STOP-BANG · upper airway resistance syndrome
Consultant-physician-depth guide to obstructive sleep apnoea (OSA) — pathophysiology of upper airway collapse, clinical features and Epworth Sleepiness Scale, cardiometabolic associations, diagnosis by polysomnography with AHI severity grading, STOP-BANG screening, and the full management ladder (lifestyle, CPAP, oral appliances, hypoglossal nerve stimulation, bariatric surgery) — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Obstructive Sleep Apnoea

The answer first
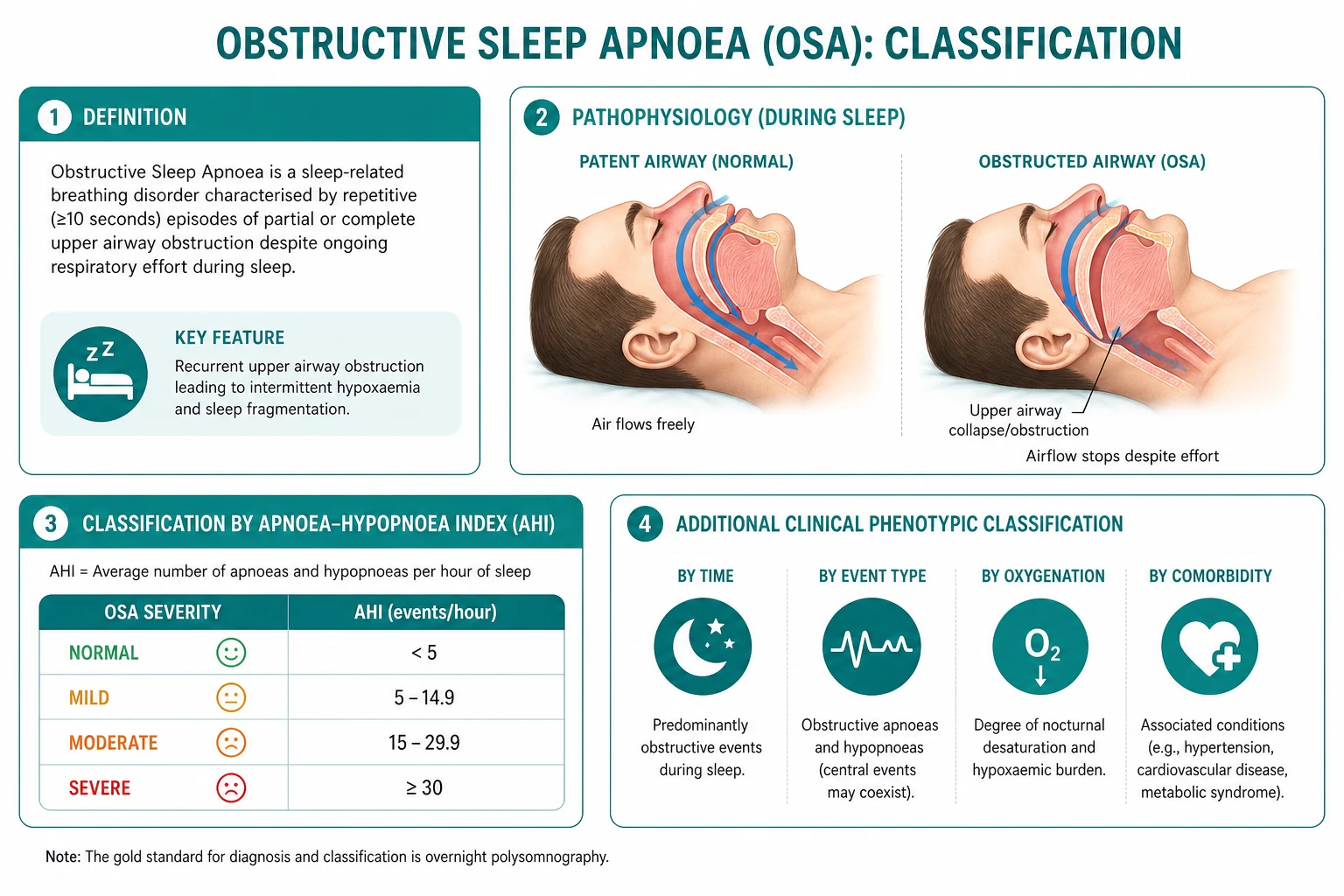
Obstructive sleep apnoea (OSA) is a chronic sleep-related breathing disorder characterised by repetitive collapse of the upper airway during sleep, producing intermittent hypoxia, recurrent arousals, and fragmented sleep. It is among the commonest chronic diseases a physician will encounter, and its burden is dominated by two consequences: excessive daytime sleepiness with impaired cognition and a markedly elevated motor vehicle accident risk, and a cluster of cardiometabolic associations — resistant hypertension, atrial fibrillation, heart failure, type 2 diabetes, and stroke. [1]
Three facts must land before everything else: [1]
- Diagnosis rests on polysomnography and the apnoea-hypopnoea index (AHI). An AHI of 5 to 15 is mild, 15 to 30 moderate, and over 30 severe. The AHI is the single number that determines severity, drives the treatment decision, and is the most commonly tested fact in written exams.
- CPAP is first-line for moderate-to-severe OSA and is highly effective for symptoms, blood pressure, and quality of life — but adherence is the central challenge, and CPAP has not been shown to prevent hard cardiovascular events in patients who already have established cardiovascular disease (the SAVE trial) [5].
- Driving is a medico-legal obligation. In Australia, a physician who diagnoses clinically significant excessive daytime sleepiness in a driver has a duty to counsel the patient and, if the patient continues to drive, to report to the licensing authority. This is a high-yield ethics and communication point that candidates consistently under-weight.
Definition and epidemiology
OSA is defined by the presence of sleep-related symptoms (sleepiness, snoring, witnessed apnoeas) plus an apnoea-hypopnoea index of 5 or more events per hour on polysomnography. An apnoea is a complete cessation of airflow for at least 10 seconds; a hypopnoea is a reduction of airflow of at least 30 percent for at least 10 seconds with an oxygen desaturation of at least 3 percent (or an arousal, under the more sensitive AASM scoring rule). [1]
OSA is common and becoming commoner, tracking the obesity epidemic. The Wisconsin Sleep Cohort update by Peppard and colleagues estimated that moderate-to-severe OSA (AHI over 15) now affects approximately 10 percent of middle-aged men and 3 percent of middle-aged women, and approximately 17 percent of men and 9 percent of women aged 50 to 70 — a relative increase of roughly 25 to 50 percent over two decades, attributable largely to rising body mass index [2]. The true community prevalence is almost certainly higher, because the majority of affected individuals are never formally diagnosed.
Pathophysiology — why the airway collapses
The upper airway is a floppy, muscular tube. Unlike the trachea, it has no bony or cartilaginous scaffolding along much of its length, and it must serve the competing functions of airflow (patency) and swallowing and speech (dynamic collapse). Patency depends on the balance between the negative intraluminal pressure generated by the respiratory pump during inspiration — which sucks the airway closed — and the active contraction of upper airway dilator muscles, principally the genioglossus (tongue protrusion), which hold it open. [1]
OSA develops when this balance fails during sleep, through two converging mechanisms. [1]
A structurally narrow and collapsible airway
Anatomical factors narrow the airway and increase its tendency to collapse: [1]
- Obesity — the dominant risk factor. Fat deposition in the lateral pharyngeal walls and around the tongue (peripharyngeal fat) narrows the lumen and increases the extraluminal tissue pressure that must be overcome. Visceral and neck fat further load the airway. Approximately 80 percent of patients with OSA are overweight or obese, and a 10 percent weight gain increases the AHI by roughly 30 percent, while a 10 percent weight loss reduces it by about 20 percent.
- Craniofacial features — retrognathia (receded mandible), micrognathia, maxillary hypoplasia, and an overjet shorten the mandibular compartment and crowd the tongue into a smaller pharyngeal space. These features explain OSA in non-obese patients.
- Soft tissue enlargement — macroglossia (Down syndrome, acromegaly, hypothyroidism, amyloidosis), tonsillar and adenoidal hypertrophy (the commonest cause in children), uvulopalatal hypertrophy, and nasal obstruction (deviated septum, polyps) all narrow the airway. [1]
The result is a pharynx that closes at a less negative closing pressure — it takes less inspiratory suction to collapse. [1]
Loss of upper airway dilator muscle tone during sleep
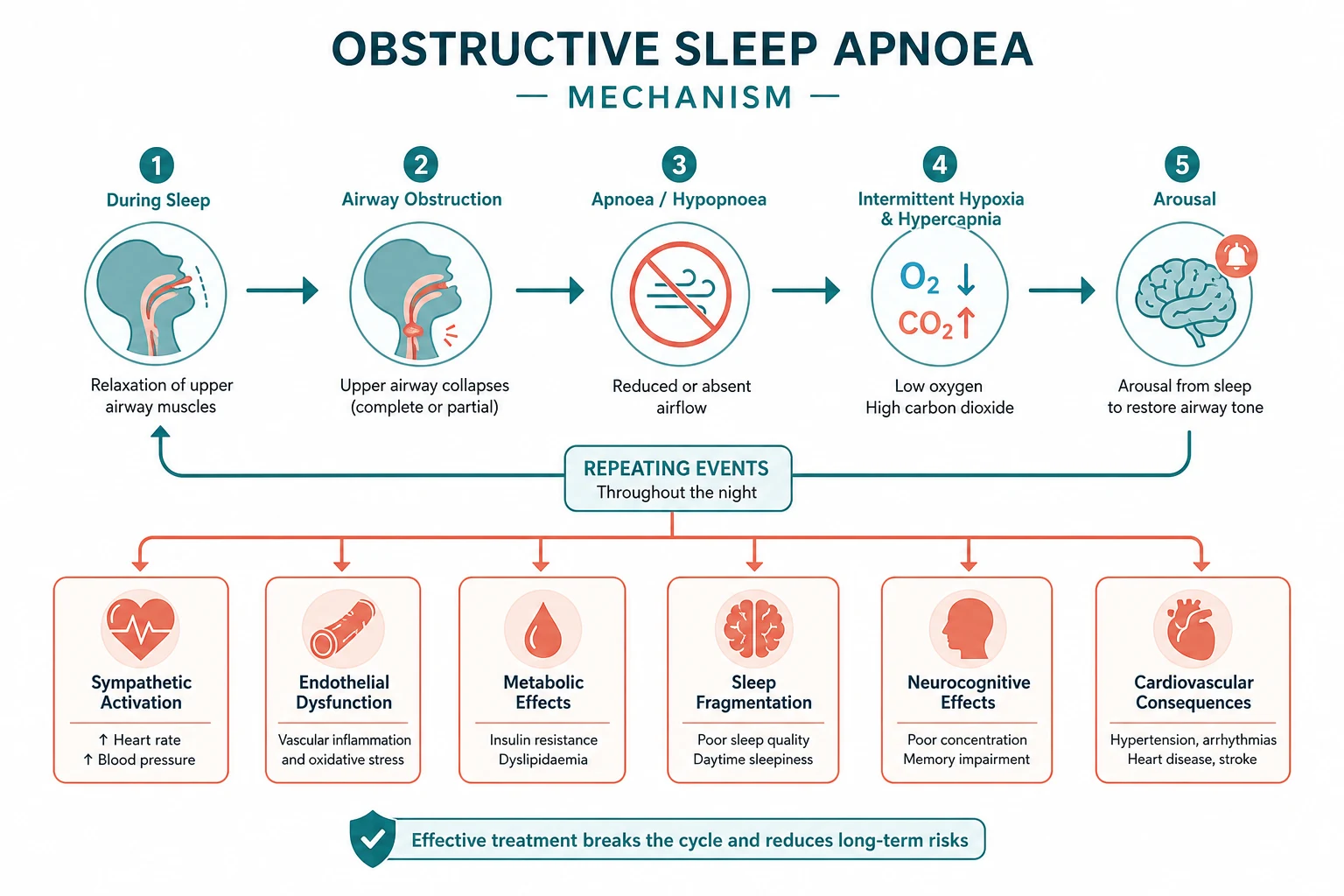
On falling asleep — and especially during REM sleep — there is a generalised reduction in skeletal muscle tone, including the genioglossus and other pharyngeal dilators. The negative inspiratory pressure now generated by the diaphragm is no longer adequately opposed, and the narrowed, already-collapsible airway occludes. Ventilation ceases. [1]
Two linked consequences follow. First, progressive asphyxia: arterial oxygen falls and carbon dioxide rises over 20 to 40 seconds, producing intermittent hypoxia, hypercapnia, and surges in sympathetic nerve activity and systemic blood pressure. Second, the rising respiratory effort against the closed airway triggers a cortical arousal. Arousal restores muscle tone, the airway reopens, a few large restorative breaths are taken — and then the patient falls back to sleep, tone falls again, and the cycle repeats. A patient with severe OSA may undergo 30 or more such cycles per hour throughout the night. [1]
The clinical damage is done by both arms of the cycle: the intermittent hypoxia and sympathetic surges drive the cardiometabolic associations, while the recurrent arousals fragment sleep architecture (with loss of slow-wave and REM sleep) and produce the daytime sleepiness and cognitive impairment that bring the patient to medical attention. [1]
Clinical features
The history is dominated by nocturnal symptoms reported largely by the bed partner, and daytime symptoms reported by the patient. Obtaining a corroborative history from the partner is essential — patients markedly under-report their own snoring and apnoeas. [1]
Nocturnal symptoms
- Loud, habitual snoring — the cardinal symptom, present in nearly all patients, often audible through closed doors or on another floor of the house
- Witnessed apnoeas — the partner describes the snoring stopping, a silent pause of 20 to 40 seconds during which the patient appears to struggle or make ineffectual respiratory efforts, and then a loud snort or gasp as breathing resumes. This is the single most specific symptom and the closest bedside surrogate of the polysomnographic event.
- Nocturnal choking or gasping arousals
- Nocturia — two or more times per night; the mechanism is atrial natriuretic peptide release in response to the negative intrathoracic pressure swings against the closed airway
- Restless sleep, diaphoresis, and nocturnal oesophageal reflux [1]
Daytime symptoms
- Excessive daytime sleepiness — the cardinal daytime symptom, ranging from drowsiness during passive activities (reading, watching television) to irresistible sleep attacks while driving or at work. It must be quantified with a validated tool.
- Unrefreshing sleep and a sense of never being rested regardless of hours slept
- Morning headache — typically frontotemporal, dull, present on waking and resolving within an hour, attributed to nocturnal hypercapnia and vasodilation
- Dry mouth and sore throat on waking, from mouth-breathing and the pressurised airflow
- Impaired concentration, attention, and short-term memory, irritability, depression, and reduced libido or erectile dysfunction [1]
DWE high-yield — the Epworth Sleepiness Scale. Daytime sleepiness is quantified by the Epworth Sleepiness Scale (ESS), developed by Murray Johns at the Epworth Hospital in Melbourne [1]. The patient rates the likelihood of dozing in eight common situations on a 0 to 3 scale, for a total of 0 to 24. A score above 10 indicates excessive daytime sleepiness and warrants formal evaluation. The ESS cut-off and the eight-item structure are the most commonly tested sleep-medicine facts in written exams.
Examination findings
Physical examination is often unrevealing but should document: [1]
- Obesity — body mass index, waist circumference, and neck circumference (a neck over 43 cm in men or over 40 cm in women is a strong correlate of OSA)
- Blood pressure — OSA is a leading cause of resistant and non-dipping hypertension; check for an elevated or refractory reading
- Craniofacial and oropharyngeal inspection — retrognathia, overjet, tonsillar hypertrophy, a long or oedematous uvula and soft palate, a high-arched or narrowed hard palate, and macroglossia. The Mallampati score (or the Friedman tongue position) grades the visibility of the posterior pharyngeal structures and correlates with OSA severity — a high Mallampati (class 3 or 4) suggests a crowded airway.
- Nasal patency — septal deviation or polyps
- Cardiovascular signs of consequence — a loud pulmonary component of the second heart sound, a right ventricular heave, or peripheral oedema suggesting pulmonary hypertension and cor pulmonale in advanced disease [1]
Cardiometabolic associations
OSA is not merely a nuisance of snoring and sleepiness. The repetitive intermittent hypoxia and sympathetic activation impose real cardiovascular and metabolic harm, and the associations are some of the most examinable and clinically important features of the disease. [1]
Hypertension
Approximately 50 percent of patients with OSA have hypertension, and OSA is the single commonest identifiable cause of resistant hypertension (blood pressure uncontrolled on three agents, including a diuretic) — present in up to 80 percent of resistant hypertensives. The mechanism is sympathetic overdrive from the chemoreflex response to intermittent hypoxia, plus endothelial dysfunction and oxidative stress. A characteristic non-dipping nocturnal blood pressure pattern on 24-hour ambulatory monitoring is a strong clue and may normalise with CPAP. [1]
Atrial fibrillation
OSA is strongly associated with atrial fibrillation. The negative intrathoracic pressure swings stretch the atrial walls, the intermittent hypoxia and surges in afterload remodel atrial myocardium, and untreated OSA predicts both new-onset AF and recurrence after cardioversion or catheter ablation. Screening patients with AF for OSA, and vice versa, is increasingly standard. [1]
Heart failure and stroke
OSA is common in heart failure (where it overlaps with central sleep apnoea and Cheyne-Stokes respiration) and is an independent risk factor for stroke and death. Yaggi and colleagues followed over 1000 patients undergoing polysomnography and found that OSA (AHI of 5 or more) approximately doubled the hazard of stroke or death after adjustment for age, sex, and vascular risk factors [3]. The mechanism is the combination of hypertension, atrial fibrillation, paradoxical embolism through a patent foramen ovale, and the prothrombotic and inflammatory state of untreated disease.
Metabolic consequences
OSA independently predicts type 2 diabetes, insulin resistance, and the metabolic syndrome, beyond what shared obesity explains. Intermittent hypoxia increases hepatic gluconeogenesis and sympathetic-mediated glycogenolysis, and oxidative stress impairs insulin signalling. [1]
Pulmonary hypertension and cor pulmonale
Sustained severe OSA can cause mild to moderate pulmonary hypertension from the cumulative effects of pulmonary vasoconstriction during hypoxic episodes, and in advanced cases progresses to right heart failure and cor pulmonale. This is less common than once thought in isolated OSA; when a patient with OSA presents with marked daytime hypercapnia, cor pulmonale, or severe pulmonary hypertension, suspect the overlap syndrome of OSA combined with COPD or obesity hypoventilation syndrome, which carries a substantially worse prognosis and requires a different ventilatory strategy. [1]
Diagnosis — polysomnography and the AHI

Polysomnography — the gold standard
In-laboratory attended polysomnography remains the gold-standard diagnostic test. It records, over a full night of sleep: [1]
- Electroencephalography, electro-oculography, and chin electromyography — to stage sleep and detect arousals
- Oronasal airflow (thermistor and nasal pressure transducer) — to detect apnoeas and hypopnoeas
- Respiratory effort (thoracic and abdominal belts) — to confirm the events are obstructive (continuing or increasing effort against a closed airway) rather than central
- Oxygen saturation by pulse oximetry — to quantify desaturation
- Electrocardiography, body position, and leg electromyography — to capture arrhythmia, positional effects, and coexisting periodic limb movements [1]
From these data the apnoea-hypopnoea index (AHI) is calculated — the average number of apnoeas plus hypopnoeas per hour of sleep — and this single number stratifies severity: [1]
| Severity | AHI (events per hour) |
|---|---|
| Mild | 5 to 15 |
| Moderate | 15 to 30 |
| Severe | Over 30 |
A diagnosis of OSA requires an AHI of 5 or more, accompanied by symptoms (or, in asymptomatic patients, an AHI of 15 or more, or of 5 or more with a comorbidity such as hypertension — the thresholds vary slightly between the AASM and ICSD-3 frameworks, but the AHI banding is consistent). [1]
DWE trap — definitions of apnoea and hypopnoea. An apnoea is a complete cessation of airflow for at least 10 seconds. A hypopnoea is a partial reduction — a drop in airflow of at least 30 percent for at least 10 seconds with either a 3 percent oxygen desaturation or an arousal. Candidates confuse the two: the apnoea is complete cessation, the hypopnoea is partial. Both are scored per hour to give the AHI. Desaturations alone, without airflow reduction, do not define OSA. [1]
Home sleep apnoea test
A home sleep apnoea test (HSAT), also called limited channel sleep study or portable monitoring, records fewer channels — typically nasal airflow, oximetry, and respiratory effort — in the patient's own bed. It is an acceptable alternative to in-laboratory polysomnography in patients with a high pre-test probability of moderate-to-severe OSA and no significant comorbidity (no moderate or severe cardiopulmonary disease, no neuromuscular disease, no suspicion of a non-respiratory sleep disorder such as narcolepsy). HSAT is less sensitive than polysomnography because it under-detects hypopnoeas (no electroencephalography to score arousals) and may underestimate severity. A negative or equivocal HSAT in a patient with a convincing clinical picture must be followed by full polysomnography — a high-yield exam point about when HSAT is and is not adequate. [1]
Screening questionnaires — STOP-BANG
The STOP-BANG questionnaire is the most widely used and best-validated screening tool, developed by Chung and colleagues for preoperative and clinic screening [7]. It comprises eight yes or no items:
- Snoring — loud snoring
- Tired — daytime fatigue or sleepiness
- Observed — witnessed apnoeas
- Pressure — treated or untreated hypertension
- BMI — over 35
- Age — over 50
- Neck circumference — over 40 cm
- Gender — male [1]
A score of 3 or more identifies intermediate to high risk; a score of 5 or more indicates a high probability of at least moderate OSA. STOP-BANG is a screening tool only — it does not diagnose OSA, which still requires polysomnography or a home study. Other tools include the Berlin Questionnaire and the Epworth Sleepiness Scale (which measures the consequence — sleepiness — rather than predicting the diagnosis). [1]
Management — the treatment ladder
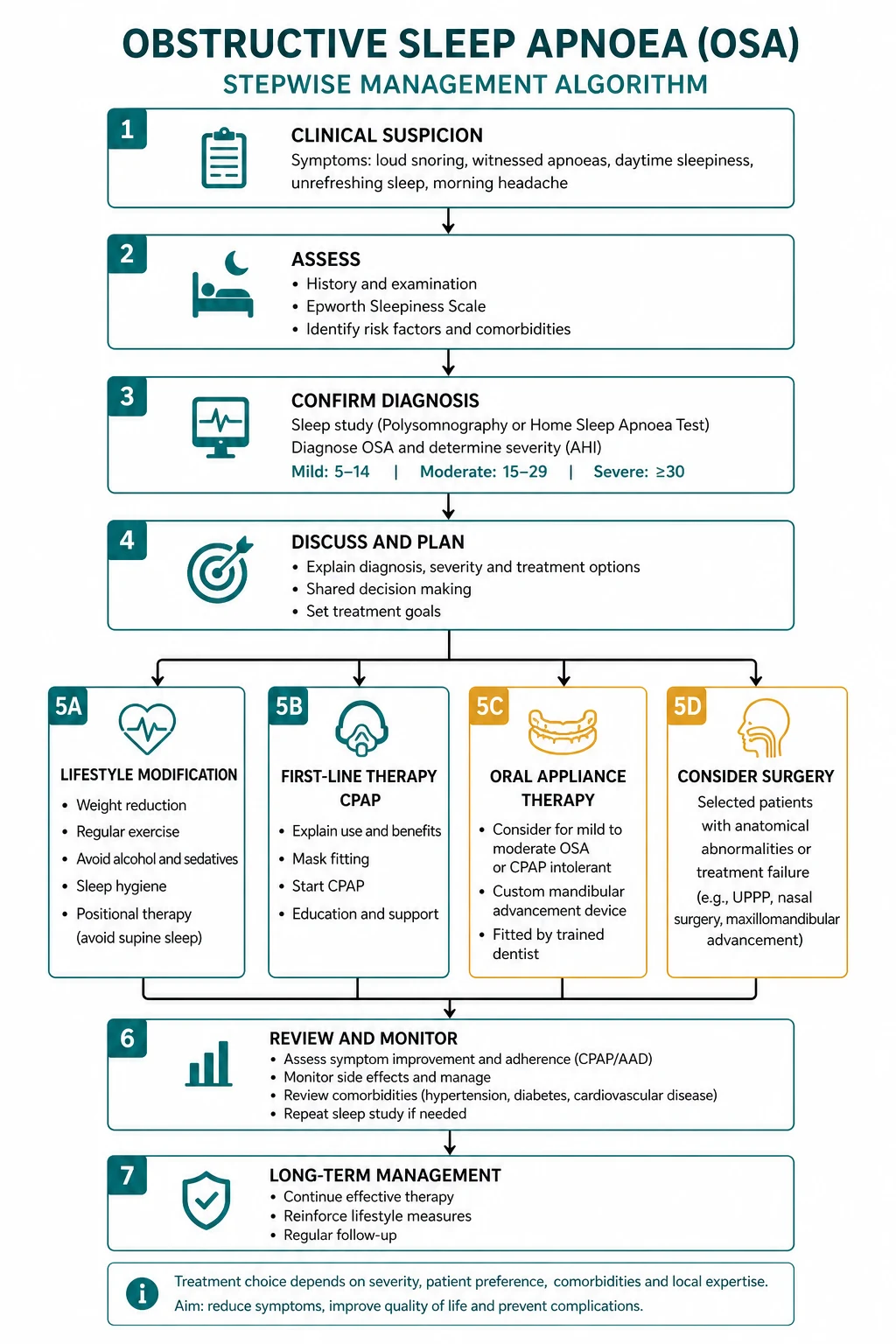
Management is staged by severity, symptom burden, and patient factors. Every patient receives lifestyle counselling; CPAP is first-line for moderate-to-severe disease; oral appliances, hypoglossal stimulation, and surgery serve defined niches. [1]
Lifestyle measures — for all patients
- Weight loss is the single most effective lifestyle intervention. A 10 percent reduction in body weight can reduce the AHI by approximately 50 percent and may move a patient from severe to mild or even remission. In morbidly obese patients who meet criteria, bariatric surgery produces substantial weight loss and can resolve OSA in a substantial proportion, and is an effective option in selected patients with severe obesity and OSA that is refractory to or intolerant of CPAP.
- Avoid alcohol and sedatives in the hours before sleep — these preferentially depress upper airway dilator muscle tone and worsen collapse.
- Sleep posture — supine sleep worsens OSA because gravity allows the tongue and soft palate to fall back. Lateral (side) sleeping can reduce the AHI in positional OSA; positional therapy devices (tennis-ball vests, vibrotactile trainers) help some patients.
- Smoking cessation — smoking increases upper airway inflammation and oedema and worsens snoring and OSA.
- Nasal steroids where there is rhinitis or nasal obstruction. [1]
CPAP — first-line for moderate-to-severe OSA
Continuous positive airway pressure (CPAP) is the cornerstone of treatment for moderate-to-severe OSA. It works as a pneumatic splint: a mask delivers a continuous positive pressure throughout the respiratory cycle that holds the upper airway open, preventing collapse. [1]
The benefits of CPAP, established across many randomised trials and meta-analyses, are robust and include: [1]
- Marked reduction in daytime sleepiness and improvement in Epworth Sleepiness Scale scores, cognitive function, and quality of life
- Reduction in blood pressure — a modest but real fall of approximately 2 to 3 mmHg systolic on meta-analysis, greater in patients with resistant hypertension
- Reduced frequency of nocturnal arrhythmias and improvement in some cardiovascular surrogates
- Improvement in self-reported driving simulator performance and, in observational data, a reduced motor vehicle accident rate [1]
CPAP is titrated to the lowest pressure that abolishes apnoeas, hypopnoeas, flow limitation, and snoring in all sleep stages and positions — typically 6 to 14 cm of water. Auto-titrating CPAP (APAP) adjusts pressure within a set range across the night and is an alternative for initiation in selected patients. Humidification should be offered routinely to reduce nasal dryness and mucosal irritation, which are common reasons for non-adherence. [1]
DCE long-case point — the central role of adherence. CPAP is effective only if it is used. Mean objective adherence in trials and clinics is around 4 to 5 hours per night — well short of the full sleep period — and roughly a third of patients use it poorly or abandon it within months. The keys to improving adherence are early and intensive support: correct mask selection and fitting (nasal, oronasal, or nasal-pillows, tried against the patient's anatomy and comfort), heated humidification, education about the disease and the consequences of untreated OSA, management of side-effects (mask leak, nasal congestion, claustrophobia, aerophagia), and structured follow-up in the first weeks. Adherence in the first month predicts long-term use. Counselling the long case on the adherence strategy is an expected discussion point. [1]
Oral appliances — mandibular advancement splint
A mandibular advancement splint (MAS), or oral appliance, is a custom-fitted dental device that holds the mandible forward during sleep, pulling the tongue base and soft palate anteriorly to enlarge and stabilise the pharyngeal airway. It is an appropriate first-line treatment for: [1]
- Mild OSA (AHI 5 to 15) when the patient prefers it to CPAP
- Moderate OSA where the patient is CPAP-intolerant or declines CPAP [1]
It is less effective than CPAP at reducing the AHI on average, but adherence is often better, and the two are comparable on symptom improvement in some trials — making it the main alternative for the patient who cannot tolerate CPAP. It requires dental assessment (it can cause temporomandibular joint discomfort, dental movement, and excessive salivation), and treatment response should be confirmed with a repeat sleep study with the device in place. [1]
Hypoglossal nerve stimulation
Hypoglossal nerve stimulation (upper airway stimulation) is an implantable device that delivers synchronized stimulation to the hypoglossal nerve on inspiration, protruding the tongue and opening the airway during sleep. The pivotal STAR trial by Strollo and colleagues was a multicentre prospective study of patients with moderate-to-severe OSA who had failed or could not tolerate CPAP [6]. At 12 months, the median AHI fell by 68 percent (from 29.3 to 9.0 events per hour), with significant improvements in oxygen desaturation index, Epworth Sleepiness Scale, and quality-of-life measures, and benefits were durable at 5-year follow-up.
Stimulation is indicated for a defined and carefully selected group: adults with moderate-to-severe OSA (AHI 15 to 65) who are CPAP-intolerant or non-adherent, with a body mass index under 32 to 35, and without complete concentric airway collapse at the palate on drug-induced sleep endoscopy. It is not for mild disease, central apnoea, or the morbidly obese. The STAR trial and its selection criteria are high-yield written and viva material. [1]
Surgery
Surgery has a limited but real role: [1]
- Uvulopalatopharyngoplasty (UPPP) removes redundant uvulopalatal tissue to widen the retropalatal airway. The evidence for benefit is modest and inconsistent — it improves the AHI in a minority and is best reserved for patients with clear uvulopalatal obstruction, often alongside tonsillectomy. It is not a reliable stand-alone cure for moderate-to-severe OSA.
- Maxillomandibular advancement moves the maxilla and mandible forward to enlarge the entire pharyngeal airway; it is the most anatomically effective skeletal procedure, with higher success rates, but is a major operation.
- Nasal surgery (septoplasty, polypectomy) improves nasal patency and may improve CPAP tolerance and symptoms, though it seldom resolves OSA alone.
- Tonsillectomy is curative in many children with tonsillar hypertrophy. [1]
EPAP valves and other adjuncts
Expiratory positive airway pressure (EPAP) valves are disposable nasal or nasal-pore adhesive devices that create resistance on expiration, generating positive pressure that splints the airway. They can reduce the AHI in mild OSA or as an adjunct, but are less effective than CPAP. Positional therapy and myofascial oropharyngeal exercises (oropharyngeal muscle training) are adjuncts with modest evidence. [1]
The SAVE trial — CPAP and cardiovascular outcomes
No discussion of OSA is complete without the SAVE trial (Sleep Apnea Cardiovascular Endpoints), a landmark multicentre randomised trial led by McEvoy and published in the New England Journal of Medicine in 2016 [5]. It randomised over 2700 patients with moderate-to-severe OSA and established coronary or cerebrovascular disease to CPAP plus usual care versus usual care alone, and followed them for nearly 4 years.
The headline result was negative: CPAP did not significantly reduce the primary composite endpoint of cardiovascular death, myocardial infarction, stroke, or hospitalisation for unstable angina, heart failure, or transient ischaemic attack (hazard ratio approximately 1.10, not significant). CPAP did, however, reduce daytime sleepiness, improve mood and quality of life, and reduce snoring. [1]
The crucial caveat is adherence: mean objective CPAP use was only 3.3 hours per night, far short of the full sleep period. Whether higher adherence would have yielded cardiovascular benefit — and whether treatment of OSA before cardiovascular disease is established is protective — remain open and important questions. The SAVE trial does not negate the symptomatic, blood pressure, and quality-of-life benefits of CPAP; it specifically answers the question of secondary prevention in patients with established cardiovascular disease and modest adherence. [1]
In contrast, the observational study by Marin and colleagues (Lancet 2005) followed men from a sleep clinic for a mean of 10 years and found that untreated severe OSA had a higher incidence of fatal and non-fatal cardiovascular events, while CPAP-treated patients had event rates approaching those of healthy controls [4]. The tension between these two bodies of evidence — observational data suggesting benefit and the randomised SAVE trial showing no cardiovascular event reduction — is a classic viva discussion point. The most defensible synthesis: CPAP clearly improves symptoms, sleepiness, blood pressure, and quality of life, and observational data strongly suggest long-term cardiovascular and mortality benefit with good adherence, but the single large randomised trial in established disease was negative, partly limited by adherence.
Driving and the medico-legal duty
Excessive daytime sleepiness impairs simulated and real-world driving performance, and patients with untreated OSA have an approximately 2 to 7 fold increased risk of motor vehicle accidents, falling towards normal with effective CPAP treatment. This transforms sleepiness from a quality-of-life issue into a public-safety and medico-legal one. [1]
In Australia, the Austroads and National Transport Commission fitness-to-drive standards govern the physician's obligations: [1]
- Private vehicle drivers with OSA may continue to drive if their symptoms are well controlled (typically on effective treatment with good adherence), but must be counselled not to drive if they are sleepy. The physician has a discretionary reporting obligation in most states — report to the licensing authority if the patient continues to drive despite clinically significant sleepiness that is likely to impair safe driving and the patient has been counselled but will not modify their behaviour.
- Commercial vehicle drivers (heavy vehicle, public passenger) are subject to stricter standards — a confirmed diagnosis of OSA requires effective treatment and demonstration of satisfactory control (often with objective CPAP adherence data) before a commercial licence is granted or renewed. Reporting obligations are more stringent. [1]
In New Zealand and the United Kingdom the principles are similar: counsel the patient, document the advice, treat the condition, and report when the patient poses an ongoing risk and will not stop driving. [1]
Communication high-yield — the driving conversation. When counselling a patient with OSA about driving, do three things. First, explain the risk honestly — that untreated sleepiness increases the chance of a crash, and that this is a safety issue, not a punishment. Second, frame treatment as the enabler — effective CPAP restores driving fitness, and most patients return to driving within weeks of starting therapy. Third, document the conversation — the advice given, the patient's response, and any decision to report. This protects both the patient and the physician. For a commercial driver, involve the licensing authority and occupational health early; do not wait for a crash. [1]
Overlap syndrome and obesity hypoventilation syndrome
A subset of patients with OSA — typically the morbidly obese — develop daytime hypercapnia (awake partial pressure of carbon dioxide over 45 mmHg) and hypoxaemia, defining obesity hypoventilation syndrome (OHS) when it occurs without another cause of hypoventilation. When OSA coexists with COPD, the combination is termed the overlap syndrome, and carries a substantially worse prognosis than either alone, with accelerated pulmonary hypertension, cor pulmonale, and hypercapnic respiratory failure. [1]
These patients often do not respond adequately to CPAP alone, because the problem is not purely obstructive — they also have a central hypoventilatory component and a blunted ventilatory response. They frequently require bilevel positive airway pressure (BPAP), which delivers a higher inspiratory than expiratory pressure to support ventilation as well as splint the airway, and supplemental oxygen when hypoxaemia persists. Identifying OHS or overlap syndrome changes management and prognosis, and is an important trap: treating these patients as straightforward OSA with CPAP alone may fail. [1]
DCE long-case approach
Opening statement (SASPOP)
"Mr Harris is a 56-year-old long-haul truck driver referred by his general practitioner for assessment of excessive daytime sleepiness. His wife reports loud snoring for many years and, over the past two years, witnessed apnoeas several times per night. He dozes off at traffic lights and has had two near-miss motor vehicle incidents in the past six months. He is overweight with a body mass index of 36, has resistant hypertension uncontrolled on three agents including a diuretic, and recently diagnosed atrial fibrillation. [1]
On examination he is obese with a neck circumference of 46 cm, a blood pressure of 156 over 94, a crowded oropharynx with a Mallampati 4 view and grade 3 tonsillar hypertrophy, and a normal cardiovascular and respiratory examination otherwise. His Epworth Sleepiness Scale score is 17. A home sleep apnoea test showed an apnoea-hypopnoea index of 42 events per hour with desaturation to 78 percent, consistent with severe obstructive sleep apnoea. [1]
His main problems are:
- Severe obstructive sleep apnoea with excessive daytime sleepiness and a high motor vehicle accident risk — primary diagnosis
- Resistant hypertension, likely driven in part by the OSA
- Atrial fibrillation, with untreated OSA promoting recurrence
- A commercial driving licence with medico-legal obligations for fitness to drive
- Obesity, the dominant modifiable risk factor [1]
My plan addresses each in turn." [1]
Integrated management plan
- Confirm and grade severity. The home study result is consistent with severe OSA in a patient with high pre-test probability and no complex comorbidity that would mandate in-laboratory polysomnography, so the diagnosis is secure. Given his cardiovascular disease, some units would still obtain a full polysomnogram to characterise the burden precisely and exclude central events — I would discuss this with the sleep laboratory.
- Initiate CPAP. With severe symptomatic OSA, CPAP is first-line. I would arrange CPAP titration (in-laboratory or auto-titrating), with attention to mask fit, heated humidification, and structured early follow-up, because adherence in the first month determines long-term success. I would set a shared adherence goal of at least 5 hours per night.
- Address the hypertension and atrial fibrillation. I would liaise with cardiology and general medicine to optimise his antihypertensives, acknowledging that CPAP may lower blood pressure modestly and improve control over months. His atrial fibrillation should be managed on its merits (rate or rhythm control, anticoagulation by CHA2DS2-VASc), with the expectation that treating the OSA may reduce recurrence after a rhythm-control strategy.
- Weight management. Refer to a multidisciplinary weight-management service, with dietary input, structured exercise, and behavioural therapy. Given his body mass index and severe refractory disease, I would discuss bariatric surgery as an effective option that can produce substantial weight loss and significantly reduce or resolve OSA.
- Driving and medico-legal. As a commercial driver, he must cease driving until his OSA is treated and he meets fitness-to-drive criteria, with documented CPAP adherence and resolution of sleepiness. I would counsel him and his employer, notify the licensing authority as required by the commercial vehicle standard, and document the conversation. I would reinstate driving once his Epworth is under 10 and objective CPAP adherence is satisfactory.
- Cardiovascular risk reduction. Screen for and treat diabetes and dyslipidaemia, and reinforce smoking cessation if applicable. [1]
DCE short-case approach
Instruction: "Examine this patient with obstructive sleep apnoea. Concentrate on the features relevant to the diagnosis." [1]
OSA is rarely a pure short-case examination subject, but it appears in Station 5 (brief consultation) and integrated into a respiratory or general examination where the patient is obese and sleepy. The relevant findings are: [1]
Key signs
- Inspection — central obesity, a short thick neck, a plethoric or moon facies, and possibly signs of right heart failure (elevated jugular venous pressure, peripheral oedema) in advanced disease with pulmonary hypertension
- Oropharyngeal inspection — a crowded airway with a high Mallampati grade (class 3 or 4), enlarged tonsils, a large or oedematous uvula and dependent soft palate, macroglossia, and retrognathia or overjet
- Cardiovascular — elevated blood pressure (often resistant), and in advanced disease a loud pulmonary component of the second heart sound or a right ventricular heave
- Hands and general — signs of associated acromegaly (if relevant), hypothyroidism, or the metabolic syndrome [1]
Presentation template
"I examined Mr Harris. He is an obese man with a short, thick neck. His body mass index is elevated, and his neck circumference is 46 cm. His blood pressure is 156 over 94. [1]
On oropharyngeal inspection he has a Mallampati class 4 view with grade 3 tonsillar hypertrophy and a large dependent uvula, consistent with a crowded upper airway. Cardiovascular examination reveals a regular pulse but an elevated blood pressure; heart sounds are normal with no evidence of right heart failure. [1]
In summary, these findings are consistent with the obstructive sleep apnoea phenotype — central obesity with a crowded oropharynx — and the elevated blood pressure is consistent with the cardiometabolic association of his condition." [1]
Examiner: "How would you investigate him?" — "The gold-standard investigation is in-laboratory polysomnography to determine the apnoea-hypopnoea index and grade severity. A home sleep apnoea test is acceptable in a patient with a high pre-test probability of moderate-to-severe OSA and no significant cardiopulmonary comorbidity. I would also quantify his sleepiness with the Epworth Sleepiness Scale, screen for diabetes and dyslipidaemia, and obtain an electrocardiogram and, given his atrial fibrillation, an echocardiogram to assess for pulmonary hypertension and structural heart disease." [1]
Examiner: "He asks whether an operation can cure him." — "Surgery is not first-line for moderate-to-severe OSA because the evidence is limited. Uvulopalatopharyngoplasty helps a minority of patients with clear uvulopalatal obstruction but is not reliably curative and does not replace CPAP. Maxillomandibular advancement is the most effective skeletal procedure but is a major operation. Bariatric surgery, in his case, is the most evidence-supported surgical option because his OSA is obesity-driven, and substantial weight loss can markedly reduce or resolve the apnoea-hypopnoea index. I would frame any surgery as adjunctive to, not a replacement for, weight management and positive airway pressure." [1]
Key DWE MCQ patterns
- AHI severity bands — know them cold: mild 5 to 15, moderate 15 to 30, severe over 30. The commonest single OSA written fact.
- Epworth Sleepiness Scale — 8 items, 0 to 24, a score above 10 is abnormal. Developed in Melbourne by Johns.
- STOP-BANG components — Snoring, Tired, Observed, Pressure, BMI over 35, Age over 50, Neck over 40 cm, Gender male. Three or more is intermediate or high risk.
- The SAVE trial — CPAP does not reduce hard cardiovascular events in patients with established cardiovascular disease (mean adherence 3.3 hours per night); it does improve symptoms, sleepiness, blood pressure, and quality of life.
- Weight loss and AHI — a 10 percent weight loss reduces the AHI by approximately 50 percent; a 10 percent weight gain increases it by roughly 30 percent.
- Hypoglossal nerve stimulation (STAR trial) — for moderate-to-severe OSA (AHI 15 to 65), CPAP-intolerant, body mass index under 32 to 35, no concentric palatal collapse. AHI fell 68 percent.
- Resistant hypertension — OSA is the commonest identifiable cause; screen every resistant hypertensive.
- Oral appliance — mandibular advancement splint for mild OSA, or moderate OSA when CPAP-intolerant.
- Overlap syndrome and OHS — daytime hypercapnia needs bilevel support, not CPAP alone.
- Definitions — apnoea is complete cessation for at least 10 seconds; hypopnoea is at least 30 percent reduction for at least 10 seconds with 3 percent desaturation or an arousal. [1]
References
[1] Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep 1991. The eight-item, 0 to 24 self-report scale developed at the Epworth Hospital in Melbourne; a score above 10 defines excessive daytime sleepiness and remains the standard sleepiness measure worldwide.
[2] Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013. The Wisconsin Sleep Cohort update estimating that moderate-to-severe OSA affects approximately 10 percent of middle-aged men and 3 percent of middle-aged women, a 25 to 50 percent rise over two decades driven by obesity.
[3] Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005. The observational cohort study establishing OSA as an independent risk factor for stroke and death after adjustment for vascular risk factors (hazard ratio for stroke or death approximately 1.97 in adjusted analysis).
[4] Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005. The 10-year observational study showing untreated severe OSA had higher fatal and non-fatal cardiovascular events while CPAP-treated patients approached the event rate of healthy controls.
[5] McEvoy RD, Antic NA, Heeley E, et al., for the SAVE Investigators. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med 2016. The landmark randomised trial in over 2700 patients with established cardiovascular disease showing that CPAP did not reduce the composite cardiovascular endpoint (mean adherence 3.3 hours per night) while improving sleepiness, mood, and quality of life.
[6] Strollo PJ Jr, Soose RJ, Maurer JT, et al., for the STAR Trial Group. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med 2014. The multicentre prospective STAR trial of hypoglossal nerve stimulation in CPAP-intolerant moderate-to-severe OSA, showing a 68 percent median reduction in apnoea-hypopnoea index and durable benefit at 5 years, defining the selection criteria for this therapy.
[7] Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008. The original validation of the STOP and STOP-BANG screening questionnaires — Snoring, Tired, Observed, Pressure, BMI, Age, Neck, Gender — for preoperative and clinic OSA risk stratification.
American Academy of Sleep Medicine Clinical Practice Guideline for the Diagnostic Evaluation of Adult Obstructive Sleep Apnea; Thoracic Society of Australia and New Zealand Position Statement on OSA; Austroads Assessing Fitness to Drive (commercial and private vehicle driver standards). [1]
References
- [1]Johns MW A new method for measuring daytime sleepiness: the Epworth sleepiness scale Sleep, 1991.PMID 1798888
- [2]Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM Increased prevalence of sleep-disordered breathing in adults Am J Epidemiol, 2013.PMID 23589584
- [3]Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V Obstructive sleep apnea as a risk factor for stroke and death N Engl J Med, 2005.PMID 16282178
- [4]Marin JM, Carrizo SJ, Vicente E, Agusti AG Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study Lancet, 2005.PMID 15781100
- [5]McEvoy RD, Antic NA, Heeley E, et al., for the SAVE Investigators CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea N Engl J Med, 2016.PMID 27571048
- [6]Strollo PJ Jr, Soose RJ, Maurer JT, et al., for the STAR Trial Group Upper-airway stimulation for obstructive sleep apnea N Engl J Med, 2014.PMID 24401051
- [7]Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea Anesthesiology, 2008.PMID 18431116