Phys · respiratory
Pleural Disease
Also known as pleural effusion · pleural fluid · empyema · parapneumonic effusion · pneumothorax · tension pneumothorax · malignant pleural effusion · mesothelioma · pleurodesis · indwelling pleural catheter · haemothorax · chylothorax
Consultant-physician-depth guide to pleural disease — pleural effusion (transudate vs exudate, Light's criteria, pleural fluid analysis, causes and investigation), parapneumonic effusion and empyema, malignant pleural effusion and mesothelioma, pneumothorax (primary spontaneous, secondary, tension) with BTS 2023 management algorithms — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Pleural Disease

The answer first
Pleural disease encompasses three clinical entities that every physician must master: pleural effusion (fluid in the pleural space), pneumothorax (air in the pleural space), and mesothelioma (malignancy of the pleura). All three are high-yield exam topics and common ward and ED presentations. [1]
Three facts must land before everything else: [1]
-
Light's criteria is the foundation of pleural fluid interpretation. An exudate is present if any one of three conditions is met: fluid/serum protein ratio over 0.5, fluid/serum LDH ratio over 0.6, or fluid LDH over two-thirds the upper limit of normal. This single algorithm separates transudate from exudate in over 95% of cases and directs every subsequent diagnostic decision [1].
-
Tension pneumothorax is a clinical diagnosis, not a radiological one. If a patient has hypoxaemia, hypotension, tracheal deviation, hyperresonance, and absent breath sounds on one side, you decompress immediately — do not wait for a chest X-ray. Death from delayed decompression is avoidable and litigated. [1]
-
Empyema is a surgical disease that becomes harder to cure the longer it is left. A parapneumonic effusion with a pH under 7.2, glucose under 2.2 mmol/L, or positive Gram stain or culture requires immediate chest tube drainage. The combination of intrapleural tPA and DNase (Rahman NEJM 2011) revolutionised the management of loculated pleural infection by reducing surgical referral and shortening hospital stay [3].
Pleural effusion — overview
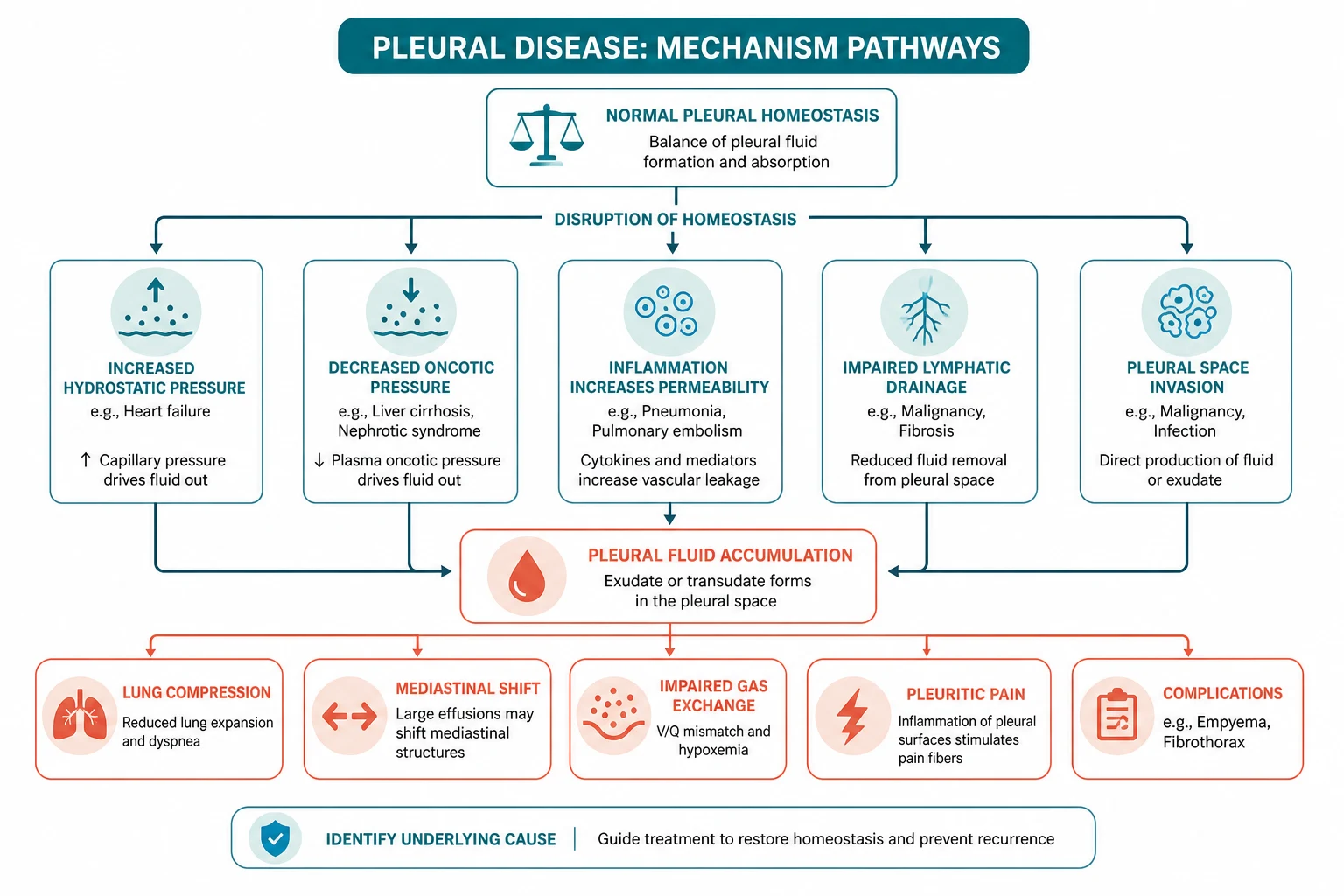
A pleural effusion is an accumulation of fluid in the pleural space. It is not a diagnosis — it is a sign of disease, and the physician's job is to find the cause. Approximately 1.5 million people develop a pleural effusion each year in the United States alone; heart failure, pneumonia, and malignancy account for the majority. [1]
The pathophysiology rests on Starling forces. The parietal pleura receives systemic arterial supply at a pressure of approximately 30 cm of water, while the visceral pleura (in humans) receives pulmonary capillary supply at approximately 10 cm. Fluid is produced by the parietal pleural capillaries and drained by parietal pleural lymphatics at a capacity of approximately 0.5 mL/kg/hour — twenty times the normal rate of formation. An effusion develops when formation exceeds drainage, either because of a systemic imbalance (raised hydrostatic pressure or low oncotic pressure, producing a transudate) or local pleural disease (inflammation, infection, malignancy increasing capillary permeability, or lymphatic obstruction, producing an exudate). [1]
Transudate versus exudate — Light's criteria

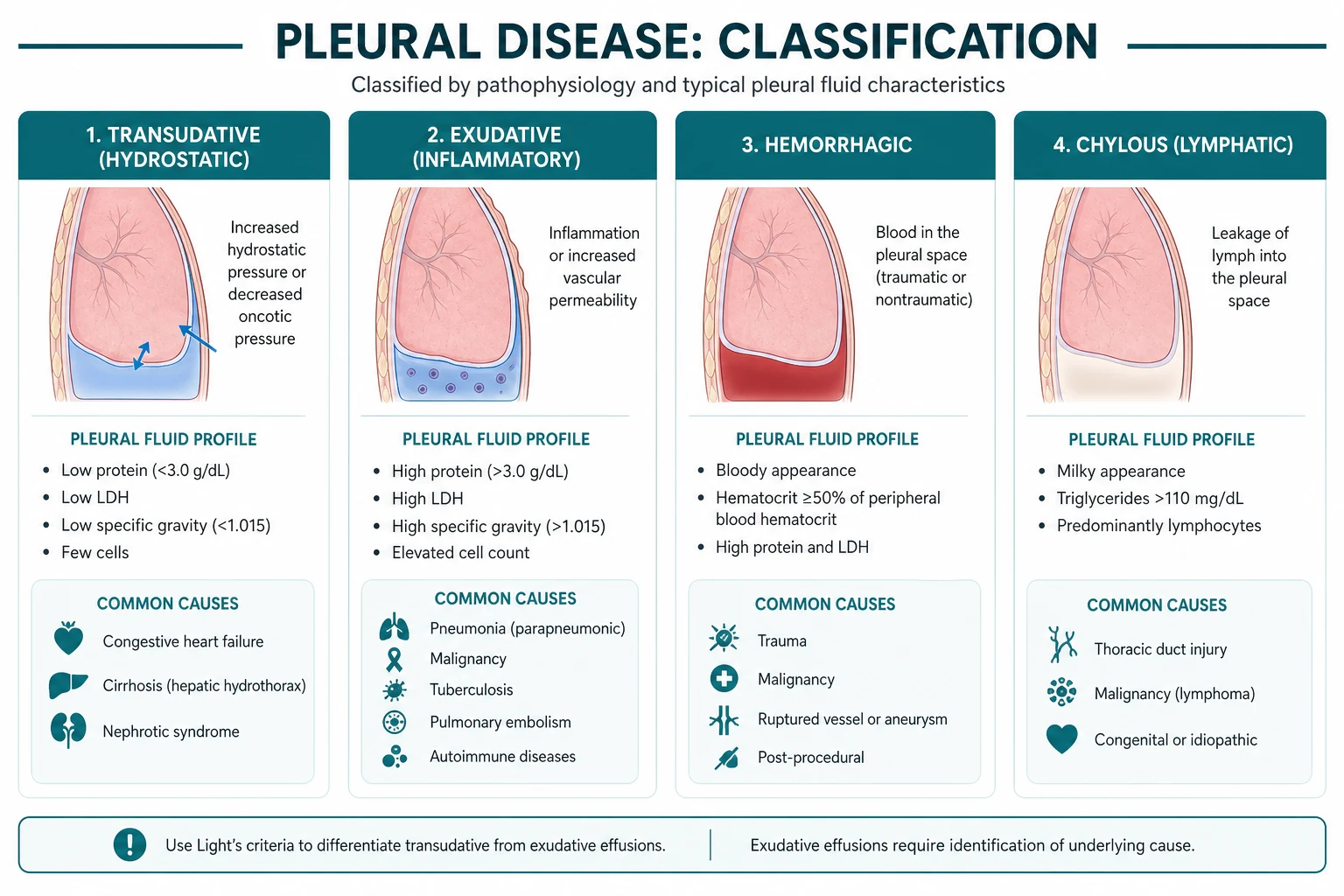
The distinction between transudate and exudate is the single most important diagnostic step after thoracentesis, because it immediately narrows the differential. Light's criteria, derived by Richard Light in 1972 and still the standard five decades later, classify an effusion as an exudate if any one of three conditions is met [1]:
| Criterion | Threshold |
|---|---|
| Pleural fluid / serum protein ratio | over 0.5 |
| Pleural fluid / serum LDH ratio | over 0.6 |
| Pleural fluid LDH | over two-thirds the upper limit of normal for serum LDH |
If none of the three is met, the effusion is a transudate. If one or more is met, it is an exudate. Using "any one" (not all three) gives a sensitivity of approximately 98% for identifying an exudate, which is what matters clinically — it is far more dangerous to miss an exudate (cancer, infection) than to over-investigate a transudate. [1]
DWE high-yield — the three Light's criteria and their thresholds. This is the most commonly tested pleural fact in written exams. Commit to memory: protein ratio 0.5, LDH ratio 0.6, LDH absolute two-thirds ULN. An exudate if any one is met. [1]
Limitations and pseudoexudates
Light's criteria are highly sensitive but imperfect. Approximately 25% of heart failure effusions are misclassified as exudates after the patient has received diuretic therapy — diuresis concentrates the protein and LDH in the pleural fluid, pushing a true transudate across the exudate threshold. This is the pseudoexudate problem. [1]
When the clinical picture suggests heart failure but Light's criteria say exudate, two rescue tests resolve it: [1]
- Pleural fluid NT-proBNP — a level over 1500 pg/mL strongly indicates a heart failure effusion, with high sensitivity and specificity. This is now the preferred rescue test.
- Serum-to-pleural fluid albumin gradient — a gradient of 1.2 g/dL (12 g/L) or greater indicates a transudate, analogous to the serum-ascites albumin gradient in hepatic hydrothorax. [1]
Examiner point: Always interpret Light's criteria in the clinical context. A bilateral effusion in a patient with heart failure is almost certainly a transudate even if one Light's criterion is borderline positive after diuresis. Check the NT-proBNP before chasing an exudative work-up. [1]
Causes of transudate
| Cause | Key features |
|---|---|
| Heart failure | Commonest cause. Bilateral, often larger on the right (due to the larger pleural surface area and the position of the diaphragmatic apertures). Associated with cardiomegaly, elevated JVP, peripheral oedema |
| Cirrhosis / hepatic hydrothorax | Right-sided in 70% of cases. Diaphragmatic defects allow ascitic fluid to track into the pleural space. Manage with sodium restriction, diuretics; TIPS for refractory cases. Never insert a chest tube — high mortality from protein loss and infection |
| Nephrotic syndrome | Bilateral, from hypoalbuminaemia reducing oncotic pressure. Look for heavy proteinuria, oedema |
| Chronic kidney disease | Uraemic pleuritis is actually an exudate; volume overload in CKD produces a transudate |
| Peritoneal dialysis | Dialysate tracks through diaphragmatic defects; typically right-sided |
| Atelectasis | Common postoperatively or with mucus plugging. Negative pleural pressure draws fluid in |
| Myxoedema | Rare; from hypothyroidism. Resolves with thyroid replacement |
| Constrictive pericarditis | Mimics heart failure and cirrhosis; look for Kussmaul sign, pericardial calcification |
Causes of exudate
| Cause | Key features and distinguishing fluid tests |
|---|---|
| Malignancy | Lung cancer, breast cancer, mesothelioma most common. Lymphocytic exudate, cytology positive in approximately 50-60% (more with repeat taps). CT shows pleural nodularity or thickening |
| Parapneumonic / empyema | Adjacent to pneumonia. pH under 7.2, glucose under 2.2, LDH over 1000, polymorphonuclear predominance. Gram stain and culture may be positive. Frank pus confirms empyema |
| Pulmonary embolism | Effusion in approximately 40% of PE. Can be transudate or exudate. Always consider PE in any unexplained unilateral effusion, especially in a patient with risk factors |
| Tuberculosis | Lymphocytic exudate (over 50% lymphocytes), high adenosine deaminase (over 40 U/L), low glucose, low pH. Pleural biopsy is more sensitive than fluid culture |
| Autoimmune | Rheumatoid arthritis — very low glucose (often under 1.6 mmol/L), very low pH (under 7.2), high LDH (over 1000), high rheumatoid factor titre. SLE — positive ANA, antinuclear antibodies in pleural fluid |
| Oesophageal rupture (Boerhaave) | Exudate with very low pH, high amylase (salivary), food particles, and polymicrobial. Surgical emergency |
| Chylothorax | Milky-white fluid, triglyceride over 1.1 mmol/L. From thoracic duct injury (malignancy, post-surgical, lymphangioleiomyomatosis) |
| Haemothorax | Pleural fluid haematocrit over 50% of serum haematocrit. Trauma, iatrogenic, or spontaneous (anticoagulation, aortic dissection) |
DWE high-yield — the unilateral unexplained effusion. If a patient has a unilateral pleural effusion and the obvious causes (pneumonia, heart failure) are excluded, you must consider malignancy, tuberculosis, and pulmonary embolism. These three are the classic "unilateral unexplained" causes and each requires specific investigation. Missing a PE behind an unexplained effusion is a classic and fatal error. [1]
Pleural fluid analysis — the full panel

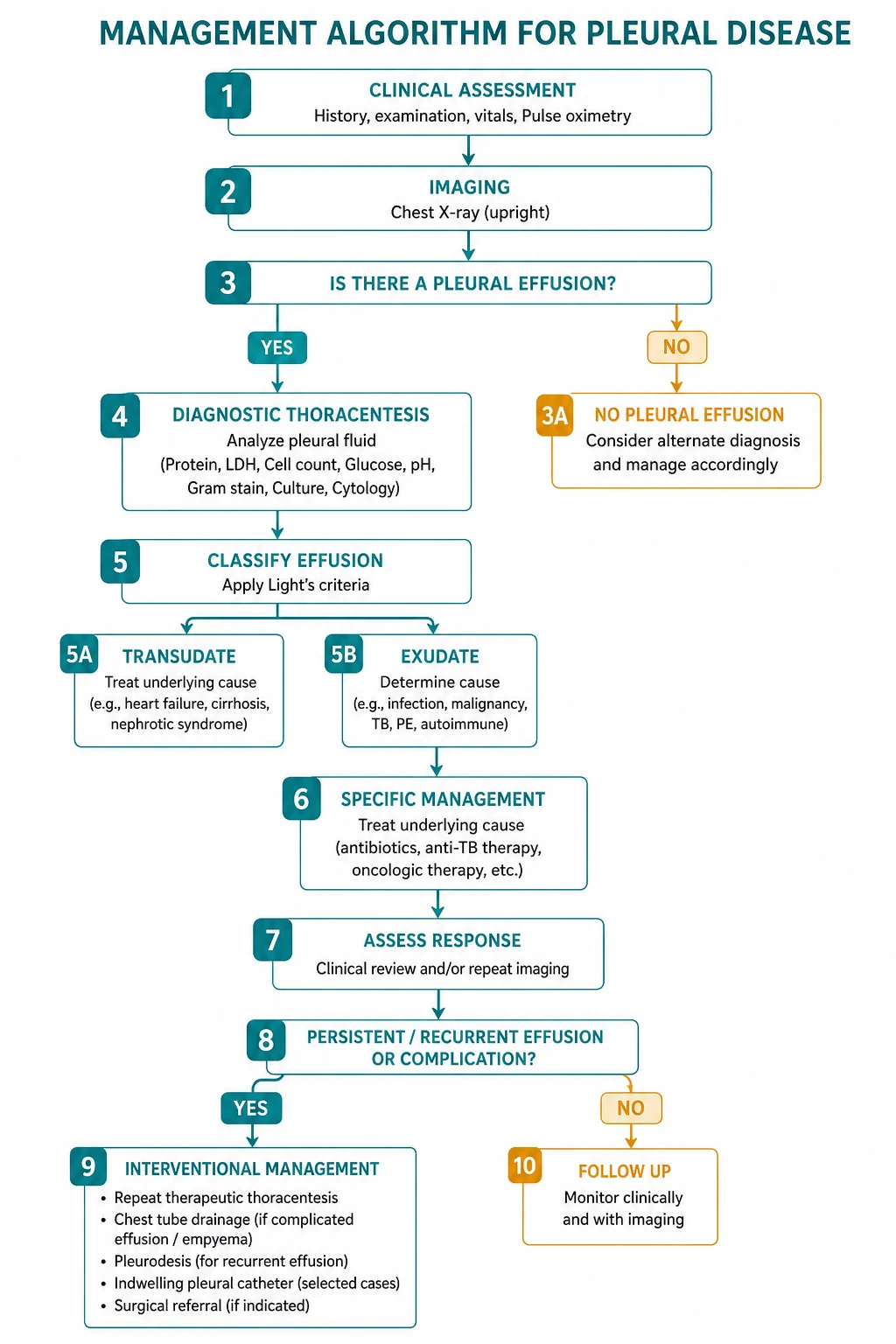
The diagnostic thoracentesis should be ultrasound-guided whenever possible — ultrasound reduces complications (pneumothorax, solid organ injury) and improves success, especially for small or loculated effusions. Send fluid for the following panel: [1]
Essential tests (every tap)
- Protein and LDH (with simultaneous serum protein and LDH) — to apply Light's criteria
- pH (in a heparinised or blood-gas syringe, kept on ice, analysed on a blood gas analyser) — a pH under 7.2 in a parapneumonic effusion mandates drainage
- Glucose — under 2.2 mmol/L suggests empyema, rheumatoid effusion, TB, or malignancy [1]- Cell count and differential — neutrophil predominance suggests bacterial infection or PE; lymphocyte predominance suggests TB or malignancy; eosinophilia is usually non-specific
- Gram stain and culture — for any suspected infection
- Cytology — for any suspected malignancy [1]
Directed tests (based on suspicion)
- Amylase — elevated in pancreatic pleuritis (pancreatic isoenzyme) and oesophageal rupture (salivary isoenzyme)
- Triglyceride — over 1.1 mmol/L confirms chylothorax; a milky effusion with a low triglyceride is a pseudochylothorax (cholesterol effusion, seen in chronic rheumatoid or TB effusions) [1]- NT-proBNP — for suspected heart failure pseudoexudate (over 1500 pg/mL)
- Adenosine deaminase (ADA) — over 40 U/L in a lymphocytic effusion supports tuberculosis (useful in high-prevalence settings)
- Rheumatoid factor and ANA — for suspected autoimmune pleuritis [1]
DWE trap — pH sample handling. Pleural fluid pH must be collected in a heparinised or blood gas syringe, kept on ice or at least sealed from air, and analysed on a blood gas analyser. Sending it in a plain tube, leaving air in the syringe, or contaminating it with lidocaine (which is acidic) all falsely lower the pH and may lead to unnecessary drainage. This procedural detail is a classic written and viva question. [1]
DCE long-case point — when to stop draining. A single therapeutic thoracentesis should remove no more than 1.5 L of fluid, and you must stop if the patient develops chest pain, tight cough, or worsening dyspnoea — these herald re-expansion pulmonary oedema. The mechanism is capillary stress failure from rapid lung re-expansion; the risk increases with larger volumes, faster drainage, and negative suction. If symptoms recur, re-image before draining further. [1]
Imaging
Chest X-ray
The classic sign of a pleural effusion on an erect PA film is the meniscus sign — blunting of the costophrenic angle with a concave upward border. Approximately 200 mL of fluid must accumulate before blunting is visible on a PA film; a lateral film detects as little as 50 mL. A large effusion causes mediastinal shift away from the effusion. If the mediastinum is central or shifted toward the effusion, suspect a bronchial obstruction (atelectasis causing a trapped lung) or malignant pleural involvement preventing lung collapse. [1]
A subpulmonic effusion sits beneath the lung, producing an apparent elevation of the hemidiaphragm with a lateral displacement of the dome peak — look for it on a lateral decubitus film or ultrasound. [1]
Ultrasound
Point-of-care pleural ultrasound is now essential. It is more sensitive than CXR for detecting and quantifying effusions, identifies loculation and septation (which predicts the need for surgical drainage), characterises fluid (anechoic versus echogenic), and marks a safe site for aspiration, reducing pneumothorax and organ injury. The BTS 2023 guideline mandates ultrasound guidance for all pleural procedures [5].
CT chest with contrast
CT is the gold standard for characterising the pleura and underlying lung. Perform it after drainage for the best assessment. Key findings: [1]
- Pleural nodularity, thickening, and enhancement — suggest malignancy (mesothelioma or metastatic disease). A pleural rind encasing the lung is highly suggestive of mesothelioma
- Pleural plaques — indicate asbestos exposure (calcified plaques on the parietal pleura, sparing the visceral pleura and costophrenic angles)
- Loculation and septation — define the complexity of an empyema
- Underlying lung mass or consolidation — identify the primary cause [1]
Pleural biopsy
When cytology is negative but malignancy is suspected, tissue is needed: [1]
- Image-guided cutting-needle biopsy (CT or ultrasound) — Abrams needle or Tru-cut. Sensitivity approximately 85-90% for malignancy when image-guided; lower for TB
- Medical thoracoscopy (local anaesthetic, semi-rigid) — allows direct visualisation of the pleura, targeted biopsy, and talc poudrage pleurodesis in one procedure. Sensitivity for malignancy over 90%
- VATS (video-assisted thoracoscopic surgery) — under general anaesthetic with single-lung ventilation; the gold standard for diagnosis and pleurodesis, but requires operative fitness [1]
Parapneumonic effusion and empyema
Pleural effusion complicates up to 40-60% of bacterial pneumonia. The spectrum runs through three stages, and the management changes at each [5].
Stage 1 — Simple (uncomplicated) parapneumonic effusion
Sterile, free-flowing fluid. Clear or slightly turbid. pH over 7.20, glucose over 2.2, LDH under 1000, Gram stain negative. Management: antibiotics alone — the effusion resolves as the pneumonia is treated. [1]
Stage 2 — Complicated parapneumonic effusion
Bacterial invasion of the pleural space, but not yet frank pus. Fluid becomes loculated as fibrin deposits create septations. pH 7.0-7.20, glucose under 2.2, LDH over 1000, Gram stain or culture may be positive. Management: antibiotics PLUS chest tube drainage. Loculation makes tube drainage difficult — this is where intrapleural tPA and DNase come in. [1]
Stage 3 — Empyema
Frank pus in the pleural space. pH under 7.0, glucose very low, LDH very high, Gram stain and culture usually positive (though prior antibiotics may sterilise cultures). Management: chest tube drainage PLUS consideration of surgical drainage (VATS). [1]
Intrapleural tPA and DNase — the Rahman trial
The landmark Rahman et al. trial (NEJM 2011) was a randomised, blinded, 2-by-2 factorial trial of 210 patients with pleural infection, testing intrapleural alteplase (tPA), DNase (dornase alfa), both, or placebo [3].
The combination of tPA and DNase significantly improved pleural fluid drainage (reduced radiographic pleural opacity at day 7), reduced the need for surgical referral at 3 months (from approximately 16% with placebo to approximately 4% with combination therapy), and shortened hospital stay. Neither agent alone was effective — tPA alone increased drainage volume but did not improve clinical outcomes, and DNase alone actually worsened outcomes (possibly by increasing fluid viscosity). [1]
The regimen: alteplase 10 mg plus dornase alfa 5 mg intrapleural, each daily for up to 3 days, instilled via the chest tube, clamped for one hour, then reopened [3].
Examiner point: The key teaching is that tPA and DNase together work; neither alone does — and DNase alone is harmful. This 2-by-2 factorial design is a methodological classic and a favourite viva topic. The combination is now standard of care for loculated complicated parapneumonic effusions and empyema that do not drain adequately through a chest tube, before resorting to surgery. [1]
When to call the surgeon
Indications for surgical drainage (VATS decortication):
- Failure of tube drainage with persistent sepsis or residual collection after 5-7 days
- Multiloculated empyema not responding to intrapleural tPA-DNase
- Thick pleural rind (peel) trapping the lung — requires decortication
- The patient who is fit enough for surgery — if not, continue medical management and consider rib resection drainage [1]
Malignant pleural effusion
A malignant pleural effusion results from pleural involvement by cancer — most commonly lung cancer (approximately 35-40%), breast cancer (approximately 20%), and mesothelioma, with lymphoma, ovarian, and gastric cancers also represented. The effusion is typically a unilateral, lymphocyte-predominant exudate, and cytology is positive in approximately 50-60% on the first tap and up to 80% with repeat sampling. [1]
A malignant effusion is usually a sign of advanced, incurable disease — median survival after diagnosis of a malignant pleural effusion is approximately 4-12 months depending on the primary tumour (shortest for lung cancer, longest for breast and ovarian). Management is therefore palliative, focused on relieving dyspnoea and preventing recurrence. [1]
Management options
-
Therapeutic thoracentesis — provides immediate symptom relief but the effusion typically recurs within 10-30 days. Useful as a one-off for prognosis assessment (does the dyspnoea actually improve?) or for patients with very short prognosis. [1]
-
Talc pleurodesis — instillation of graded sterile talc into the pleural space to create a fibrous adhesion between the visceral and parietal pleura, obliterating the space. Can be done as slurry (via chest tube) or poudrage (insufflated at thoracoscopy or VATS). Success rate approximately 70-90%. Requires that the lung fully re-expands after drainage — a trapped lung (visceral pleural restriction from tumour or fibrosis preventing re-expansion) precludes successful pleurodesis. [1]
-
Indwelling pleural catheter (IPC) — a tunneled catheter (PleurX) placed under local anaesthetic, drained at home every 1-3 days by the patient or community nursing. Spontaneous pleurodesis occurs in approximately 40-50% of patients. Ideal for patients with trapped lung (where pleurodesis cannot succeed), short prognosis, or those prefer outpatient management. [1]
The TIME2 trial
The TIME2 trial (Davies et al., JAMA 2012) randomised 106 patients with malignant pleural effusion to IPC versus chest tube plus talc pleurodesis [6].
Both approaches produced equivalent dyspnoea improvement at 42 days. However, IPC patients had:
- Fewer days in hospital (median 10 days versus 12 with talc in the initial admission, and significantly fewer total hospital days over follow-up)
- Lower treatment failure rate (need for further pleural procedures)
- But a higher rate of cellulitis around the catheter (approximately 6%) [1]
The takeaway: IPC and talc pleurodesis are equivalent first-line options for malignant pleural effusion. The choice depends on lung re-expansion (trapped lung favours IPC), prognosis (short prognosis favours IPC), and patient preference (outpatient drainage versus a hospital admission). [1]
DCE long-case trap — check lung re-expansion before pleurodesis. Always assess whether the lung re-expands after drainage before committing to pleurodesis. A trapped lung (failure to re-expand) is a contraindication to pleurodesis because the visceral and parietal pleura cannot appose. In this situation, an IPC is the correct choice. This distinction is a key decision point in the malignant effusion long case. [1]
Mesothelioma
Malignant pleural mesothelioma is an aggressive cancer arising from the mesothelial cells of the pleura, almost always caused by asbestos exposure. Australia and New Zealand have among the highest rates in the world due to historical asbestos mining (Wittenoom) and widespread industrial use. [1]
Epidemiology and pathogenesis
The latency between asbestos exposure and mesothelioma is typically 20-50 years. All types of asbestos fibres cause mesothelioma, but crocidolite (blue asbestos) and amosite (brown asbestos) are most potent. The mechanism involves frustrated phagocytosis of fibres by mesothelial cells, chronic inflammation, reactive oxygen species generation, and chromosomal damage. The risk is dose-related but there is no safe threshold — even brief or bystander exposure (washing a partner's work clothes) can cause disease. [1]
ANZ high-yield: In Australia, mesothelioma is compensable through the Dust Diseases Board / icare (NSW) and equivalent schemes in other states. The exposure history must be meticulously documented — occupations include shipbuilding, insulation, plumbing, brake/clutch fitting, demolition, and the Wittenoom mine. Always ask about a partner's occupation (secondary exposure). [1]
Clinical presentation
- Progressive dyspnoea (from effusion and restrictive lung impairment)
- Chest wall pain — often dull, persistent, and poorly localised; may be the presenting symptom
- Weight loss, fatigue, cachexia
- Unilateral pleural effusion or pleural thickening on imaging
- Clubbing is uncommon (unlike lung cancer) [1]
Diagnosis
- CT chest with contrast — pleural thickening (often nodular and circumferential), a pleural rind encasing the lung, a unilateral effusion, and volume loss of the affected hemithorax. Calcified pleural plaques indicate prior asbestos exposure but are not premalignant.
- Pleural fluid cytology — positive in only approximately 30-50% of mesothelioma (lower than metastatic adenocarcinoma). Cytology alone is often insufficient for a definitive diagnosis.
- Pleural biopsy — image-guided cutting-needle biopsy or thoracoscopy. Immunohistochemistry is essential to distinguish mesothelioma from metastatic adenocarcinoma:
- Mesothelioma: calretinin, WT-1, D2-40, CK5/6 positive; TTF-1, CEA, Ber-EP4 negative
- Adenocarcinoma: TTF-1 (lung primary), CEA, Ber-EP4 positive; calretinin, WT-1 negative
- Soluble mesothelin (serum biomarker) — elevated in approximately 50-60% of mesothelioma, useful for monitoring but not screening. [1]
Examiner point — do not perform a core biopsy through skin that may later be a VATS port or radiotherapy field if avoidable, because mesothelioma has a notorious tendency to seed along the biopsy tract (tract metastasis). Some centres offer prophylactic radiotherapy to the biopsy tract, though evidence for benefit is mixed. Discuss the biopsy approach with the thoracic MDT. [1]
Management and prognosis
Mesothelioma is almost always incurable at presentation. Median survival is 8-12 months from diagnosis, though epithelioid subtype (the most common) fares better (12-20 months) than sarcomatoid or biphasic subtypes (4-8 months). [1]
- Chemotherapy — the Vogelzang et al. trial (JCO 2003) established pemetrexed plus cisplatin as the standard first-line regimen, improving median survival from 9.3 months (cisplatin alone) to 12.1 months, with a response rate of 41% versus 17% [4]. Folic acid and vitamin B12 supplementation are mandatory to reduce pemetrexed toxicity (myelosuppression, mucositis). Carboplatin is substituted for cisplatin in patients with poorer renal function or performance status.
- Surgery — extrapleural pneumonectomy (EPP) and pleurectomy/decortication (P/D) are performed in highly selected, fit patients at specialist centres, usually as part of multimodality therapy (surgery plus chemotherapy plus radiotherapy). The MARS trial cast doubt on the benefit of EPP, and surgery is not standard of care outside clinical trials and expert centres.
- Radiotherapy — has a role in pain control for localised chest wall disease and may reduce tract metastasis after diagnostic procedures. It is not curative.
- Pleural effusion control — talc pleurodesis or IPC for symptom relief. Perform early, at the time of diagnostic thoracoscopy if possible.
- Symptom control — pain management is challenging (opioids, nerve blocks, palliative radiotherapy); the palliative care team is involved early.
Compensation
Mesothelioma is compensable in virtually all jurisdictions. In ANZ:
- Dust Diseases Board / icare (NSW) and equivalent statutory schemes handle compensation for medical expenses, lost income, and lump sum payments
- Common law claims against negligent employers or manufacturers may provide significant damages
- The exposure history is the foundation of the claim — document every job, every employer, and the nature of asbestos exposure, including secondary (take-home) exposure [1]
Communication high-yield: When delivering a mesothelioma diagnosis, address three things in the first conversation: the diagnosis and prognosis (median survival 8-12 months, honest but compassionate), the treatment options (chemotherapy for symptom control and modest survival benefit), and the compensation rights (the patient is entitled to compensation regardless of ability to identify a specific employer — refer to the dust diseases service and a specialist asbestos lawyer). Document the occupational history meticulously — this is both a clinical and a legal document. [1]
Pneumothorax — classification

A pneumothorax is air in the pleural space. The classification determines management. [1]
Primary spontaneous pneumothorax (PSP)
PSP occurs in a person without underlying lung disease. The typical patient is a tall, thin, young male smoker. The mechanism is rupture of apical subpleural blebs or bullae. Smoking increases the risk approximately 20-fold in men and increases it in a dose-dependent manner. The incidence is approximately 18-28 per 100,000 per year in men and 1-6 per 100,000 in women. [1]
Secondary spontaneous pneumothorax (SSP)
SSP occurs in a person with underlying lung disease. The commonest causes: [1]
- COPD — the most common cause overall (rupture of a bulla)
- Asthma — during a severe exacerbation
- Cystic fibrosis — often recurrent, may indicate need for transplant referral
- Pneumocystis jirovecii pneumonia (PJP) — in HIV with a CD4 under 200; pneumothorax is a recognised complication from cystic lung destruction
- Lymphangioleiomyomatosis (LAM) — recurrent pneumothorax in a young woman with cystic lung disease and chylothorax
- Langerhans cell histiocytosis — cystic lung disease in a smoker
- Interstitial lung disease — especially with honeycombing
- Tuberculosis, lung abscess, malignancy — necrotic lesions eroding into the pleura [1]
SSP is less well tolerated than PSP because the underlying lung disease means less respiratory reserve. Even a small SSP can cause significant dyspnoea and hypoxaemia. [1]
Traumatic and iatrogenic pneumothorax
- Traumatic — blunt or penetrating chest trauma; may be associated with haemothorax
- Iatrogenic — the commonest in-hospital pneumothorax. Causes include transthoracic needle biopsy, thoracentesis, central line insertion, transbronchial biopsy, positive pressure ventilation (barotrauma) [1]
Tension pneumothorax
Tension pneumothorax is the life-threatening form in which air enters the pleural space on inspiration but cannot escape on expiration (a one-way valve effect), progressively increasing intrapleural pressure. This collapses the lung, shifts the mediastinum to the opposite side, impairs venous return, and causes obstructive shock and cardiac arrest. [1]
Pneumothorax — clinical features
The classic presentation is sudden onset of pleuritic chest pain and dyspnoea at rest. [1]
Examination findings:
- Reduced chest expansion on the affected side
- Hyperresonant percussion note (the key discriminator from effusion, which is dull)
- Reduced or absent breath sounds on the affected side
- Reduced vocal resonance [1]
In tension pneumothorax, add:
- Severe respiratory distress
- Hypoxaemia and cyanosis
- Hypotension, tachycardia — obstructive shock
- Tracheal deviation away from the affected side (a late sign)
- Distended neck veins (from impaired venous return) [1]
Critical: Tension pneumothorax is a clinical diagnosis. Do not wait for a chest X-ray. If the patient has the clinical syndrome (shock plus hyperresonance and absent breath sounds on one side), decompress immediately. The classic teaching site is the second intercostal space, midclavicular line on the affected side, with a large-bore cannula. More recent evidence and the BTS suggest the fifth intercostal space, midaxillary line (the "safe triangle") may be more reliable because the chest wall is thinner there and the needle more likely to reach the pleural space, especially in larger patients. After immediate needle decompression, insert a formal intercostal chest drain. [1]
Pneumothorax — management
The BTS 2023 Guideline for pleural disease transformed pneumothorax management toward a symptom-driven approach, moving away from the rigid size-based algorithms of the 2010 guideline [5].
Primary spontaneous pneumothorax
| Clinical scenario | Management |
|---|---|
| Small, asymptomatic or minimally symptomatic | Observation — discharge with safety-net advice and review at 2-4 weeks. The 2023 guideline endorses conservative management for minimally symptomatic PSP regardless of size, based on evidence that most resolve spontaneously |
| Symptomatic (significant dyspnoea) | Simple aspiration — aspirate 2.5-4 L via a cannula in the second intercostal space midclavicular line or safe triangle. If successful (lung re-expanded), observe; if it recurs, proceed to chest drain or IPC |
| Large or failed aspiration | Intercostal chest drain (small-bore, e.g. 8-14 Fr Seldinger) in the safe triangle. Do not routinely apply suction |
| Persistent air leak (over 5 days) | Surgical referral for VATS pleurodesis and bullectomy |
| Recurrence (second episode) | Pleurodesis — talc or surgical (VATS with mechanical pleural abrasion and bullectomy) |
Secondary spontaneous pneumothorax
SSP is less well tolerated and managed more aggressively because of limited reserve: [1]
| Clinical scenario | Management |
|---|---|
| Small, asymptomatic | Observation in hospital (not discharge) — monitor closely for deterioration |
| Symptomatic or large | Intercostal chest drain — aspiration is less likely to succeed in SSP and is not preferred as first-line |
| Persistent air leak or failure to re-expand | Early surgical referral (VATS). In CF or severe disease where surgery is contraindicated, consider medical pleurodesis (talc slurry) |
| Recurrence | Pleurodesis after the first recurrence |
The "safe triangle"
Chest drains are inserted in the safe triangle (of Petra), bounded by:
- Anterior border: lateral border of pectoralis major
- Posterior border: lateral border of latissimus dorsi
- Inferior border: line above the fifth intercostal space (the level of the nipple)
- Apex: the axilla [1]
This avoids the internal mammary artery (medially), the long thoracic nerve (posteriorly), and the diaphragm and abdominal contents (inferiorly). [1]
Surgical intervention and pleurodesis for pneumothorax
Indications for surgery (VATS):
- Second ipsilateral PSP (recurrence rate after first PSP is approximately 25-30%, rising with each event)
- First contralateral PSP (bilateral disease)
- Persistent air leak over 3-5 days despite chest drainage
- High-risk professions — pilots, divers, divers — where a recurrence in a remote or pressurised environment would be catastrophic; some advocate pleurodesis after the first PSP
- SSP with failure of conservative management [1]
The procedure is VATS bullectomy (stapling of apical blebs) plus pleurodesis (mechanical pleural abrasion or chemical talc). Recurrence rates after VATS pleurodesis are approximately 5%, compared with approximately 25% after chest-tube talc slurry and approximately 30% after aspiration alone. [1]
Special situations
- Catamenial pneumothorax — recurrent pneumothorax in women within 72 hours of menstruation, associated with endometriosis and diaphragmatic defects; usually right-sided. Management includes pleurodesis plus hormonal suppression.
- Pneumothorax in pregnancy — manage with aspiration or small-bore drain; avoid CT; surgery if recurrent.
- Pneumothorax on positive pressure ventilation — a high-risk situation. Insert a chest drain prophylactically in any ventilated patient who develops a pneumothorax, as positive pressure converts even a small pneumothorax to tension rapidly. [1]
Haemothorax and chylothorax
Haemothorax
A haemothorax is blood in the pleural space, defined by a pleural fluid haematocrit over 50% of the serum haematocrit (a lower haematocrit suggests a haemorrhagic effusion, not a true haemothorax). Causes: [1]
- Trauma — blunt or penetrating; the commonest cause
- Iatrogenic — post-thoracentesis, post-CVC insertion, post-thoracotomy
- Spontaneous — anticoagulation, aortic dissection, pulmonary infarction, malignancy [1]
Management: large-bore (28-36 Fr) chest tube drainage. Indications for surgical exploration (thoracotomy):
- Over 1500 mL initial drainage [1]- Over 200 mL per hour for 2-4 hours
- Persistent transfusion requirement
- Failure to fully drain (clotted haemothorax) — needs VATS evacuation within 7 days before organisation and fibrosis [1]
Chylothorax
A chylothorax is chyle (lymph) in the pleural space, producing a milky-white effusion with a triglyceride level over 1.1 mmol/L. Causes: [1]
- Malignancy — lymphoma is the commonest cause of non-traumatic chylothorax (mediastinal lymph node involvement obstructing the thoracic duct)
- Post-surgical — oesophagectomy, thoracic surgery, cardiothoracic surgery (thoracic duct injury)
- Lymphangioleiomyomatosis (LAM) — chylothorax and recurrent pneumothorax in a young woman
- Trauma, congenital, idiopathic [1]
Management: treat the underlying cause. Conservative measures include a low-fat medium-chain triglyceride diet (MCTs are absorbed directly into the portal vein, bypassing the lymphatics) or bowel rest with parenteral nutrition, plus octreotide (reduces lymph flow). Thoracic duct embolisation (interventional radiology) is effective for persistent leaks. Pleurodesis for refractory cases. [1]
DWE high-yield — the milky effusion. Not all milky pleural fluid is a chylothorax. A pseudochylothorax (cholesterol effusion) is also milky but has a low triglyceride and high cholesterol, seen in chronic effusions (rheumatoid pleurisy, TB). The distinction is made by the triglyceride level and the clinical context. [1]
DCE long-case approach
Opening statement (SASPOP)
"Mr Wilson is a 68-year-old former shipyard worker who presents with a 6-week history of progressive exertional dyspnoea, right-sided chest wall pain, and 8 kg of unintentional weight loss. He worked for 15 years in shipbuilding in the 1970s with significant asbestos exposure. He is a 50 pack-year smoker. [1]
On examination he is cachectic and breathless at rest, with a respiratory rate of 24, oxygen saturation 92% on room air, and dullness to percussion with absent breath sounds over the lower two-thirds of the right hemithorax. His CXR and CT chest show a large right pleural effusion with circumferential right pleural thickening and a rind encasing the right lung, with associated volume loss. There are calcified pleural plaques bilaterally. [1]
His main problems are:
- Probable malignant pleural mesothelioma secondary to asbestos exposure — primary diagnosis
- A large symptomatic right pleural effusion requiring drainage and definitive pleural control
- Severe chest wall pain requiring a multimodal analgesia plan
- Cachexia and nutritional decline
- The need for occupational history documentation, compensation referral, and family counselling regarding prognosis [1]
My plan addresses each of these in turn." [1]
Integrated management plan
-
Confirm the diagnosis. Arrange a CT-guided pleural biopsy with immunohistochemistry (calretinin, WT-1 positive in mesothelioma; TTF-1 negative), or medical thoracoscopy if feasible, which allows biopsy and talc pleurodesis in one procedure. [1]
-
Drain the effusion and assess lung re-expansion. Perform a therapeutic thoracentesis (limit 1.5 L) for symptom relief. Assess whether the lung re-expands on CT — a trapped lung precludes pleurodesis and favours an IPC. [1]
-
Establish definitive pleural control. If the lung re-expands, perform talc pleurodesis (poudrage at thoracoscopy or slurry via chest tube). If the lung is trapped, insert an indwelling pleural catheter (IPC) for outpatient drainage. [1]
-
Plan chemotherapy. Refer to the medical oncology MDT for consideration of pemetrexed plus cisplatin (or carboplatin), with folic acid and vitamin B12 supplementation. [1]
-
Manage pain. Involve the palliative care and pain teams. Options include oral and transdermal opioids, co-analgesics (gabapentinoids for neuropathic pain), intercostal nerve blocks, and palliative radiotherapy for localised chest wall disease. [1]
-
Address compensation. Document the occupational asbestos exposure meticulously. Refer to the dust diseases service (icare/Dust Diseases Board in NSW, equivalent in other states) and provide the patient with information about common-law compensation and a specialist asbestos lawyer. [1]
-
Support the patient and family. Deliver the diagnosis honestly and compassionally. Discuss prognosis (median survival 8-12 months), treatment goals (disease-modifying and palliative), and advance care planning. Arrange palliative care involvement. [1]
DCE short-case approach: respiratory examination with pleural disease
Instruction: "Examine this patient's respiratory system. He was admitted with a pleural effusion." [1]
Key signs of a pleural effusion
- Inspection: tachypnoea, reduced chest wall movement on the affected side (in a large effusion)
- Palpation: reduced chest expansion on the affected side; trachea and apex may be deviated away from the effusion if large
- Percussion: stony dull percussion note over the effusion
- Auscultation: reduced or absent breath sounds over the effusion, reduced vocal resonance (the fluid blocks sound transmission), and there may be egophony (e-to-a change) at the upper border of the effusion (compressed lung above the fluid) [1]
Presentation template
"I examined Mr Wilson's respiratory system. He is breathless at rest, with a respiratory rate of 24. He is not cyanosed. He is not clubbed. [1]
The trachea is deviated to the left. Chest wall expansion is reduced on the right. On percussion, there is stony dullness over the lower two-thirds of the right hemithorax. Tactile vocal fremitus is reduced over this area. On auscultation, breath sounds are absent over the right lower and middle zones, with reduced vocal resonance. At the upper border of the dullness, there is an egophonic e-to-a change. The left lung is clear. [1]
In summary, these findings are consistent with a large right pleural effusion." [1]
Examiner: "How does a pleural effusion differ from consolidation on examination?" — Both produce a dull percussion note, but the auscultatory findings are opposite. In a pleural effusion, the fluid blocks sound transmission: breath sounds are reduced or absent, and vocal resonance is reduced. In consolidation, the solidified lung conducts sound better: breath sounds are bronchial (tubular), and vocal resonance is increased with whispered pectoriloquy and egophony. This single contrast — reduced versus increased transmission — is the most reliable bedside discriminator and a classic PACES test. [1]
Examiner: "What would you find if this were a pneumothorax instead?" — The percussion note would be hyperresonant (not dull), and breath sounds would be reduced or absent with reduced vocal resonance. The contrast between effusion (stony dull) and pneumothorax (hyperresonant) — both with reduced breath sounds — is determined by percussion. In tension pneumothorax, add tracheal deviation and haemodynamic compromise. [1]
Key DWE MCQ patterns
- Light's criteria — know all three thresholds cold. The commonest single pleural MCQ.
- Pleural fluid pH under 7.2 in a parapneumonic effusion — mandates chest tube drainage.
- Pseudoexudate from diuretics in heart failure — rescue with NT-proBNP or albumin gradient.
- Tension pneumothorax — clinical diagnosis, immediate decompression, no imaging.
- Intrapleural tPA and DNase — combination works; neither alone (Rahman trial).
- Pemetrexed plus cisplatin — first-line chemotherapy for mesothelioma (Vogelzang trial).
- Talc pleurodesis contraindicated in trapped lung — use IPC instead.
- Amylase elevated in pleural fluid — pancreatic pleuritis or oesophageal rupture.
- Chylothorax — milky fluid, triglyceride over 1.1 mmol/L, lymphoma or thoracic duct injury.
- Haemothorax — pleural fluid haematocrit over 50% of serum. [1]
References
[1] Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med 1972. The landmark study deriving Light's criteria — still the standard for separating transudate from exudate over 50 years later.
[2] MacDuff A, Arnold A, Harvey J. Management of spontaneous pneumothorax: BTS Pleural Disease Guideline 2010. Thorax 2010. The 2010 BTS guideline that introduced the size-based and intervention-based pneumothorax algorithm, superseded by the 2023 update.
[3] Rahman NM, Maskell NA, West A, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. N Engl J Med 2011. The 2-by-2 factorial trial proving that combined tPA and DNase (but neither alone) improved drainage, reduced surgical referral, and shortened hospital stay in pleural infection.
[4] Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol 2003. The pivotal trial establishing pemetrexed plus cisplatin as standard first-line chemotherapy for mesothelioma (median survival 12.1 vs 9.3 months).
[5] Roberts ME, Woolhouse IM, Davies HE, et al. British Thoracic Society Guideline for pleural disease. Thorax 2023. The current primary guideline covering spontaneous pneumothorax, undiagnosed unilateral pleural effusion, pleural infection, and malignant pleural effusion, with the symptom-driven pneumothorax approach.
[6] Davies HE, Mishra EK, Kahan BC, et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA 2012. The trial showing IPC and talc pleurodesis produce equivalent dyspnoea relief, with IPC reducing hospital days but increasing cellulitis risk.
BTS Guideline for Pleural Disease 2023; NICE NG156 — Lung Cancer (includes mesothelioma); Therapeutic Guidelines (Australia) — Respiratory. [1]
References
- [1]Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr Pleural effusions: the diagnostic separation of transudates and exudates Ann Intern Med, 1972.PMID 4642731
- [2]MacDuff A, Arnold A, Harvey J, on behalf of the BTS Pleural Disease Guideline Group Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010 Thorax, 2010.PMID 20696690
- [3]Rahman NM, Maskell NA, West A, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection N Engl J Med, 2011.PMID 21830966
- [4]Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma J Clin Oncol, 2003.PMID 12860938
- [5]Roberts ME, Woolhouse IM, Davies HE, et al., on behalf of the BTS Pleural Disease Guideline Group British Thoracic Society Guideline for pleural disease Thorax, 2023.PMID 37553157
- [6]Davies HE, Mishra EK, Kahan BC, et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial JAMA, 2012.PMID 22610520