Phys · respiratory
Pneumonia
Also known as CAP · community-acquired pneumonia · hospital-acquired pneumonia · HAP · ventilator-associated pneumonia · VAP · lobar pneumonia · atypical pneumonia · aspiration pneumonia
Consultant-physician-depth guide to pneumonia — classification (CAP, HAP, VAP, aspiration, immunocompromised), pathogen patterns by setting, severity assessment (CURB-65, PSI, SMART-COP), investigations (CXR, urinary antigens, procalcitonin), empiric antibiotic therapy per IDSA/ATS 2019, corticosteroid adjunct in severe CAP, complications and prevention — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Pneumonia
The answer first
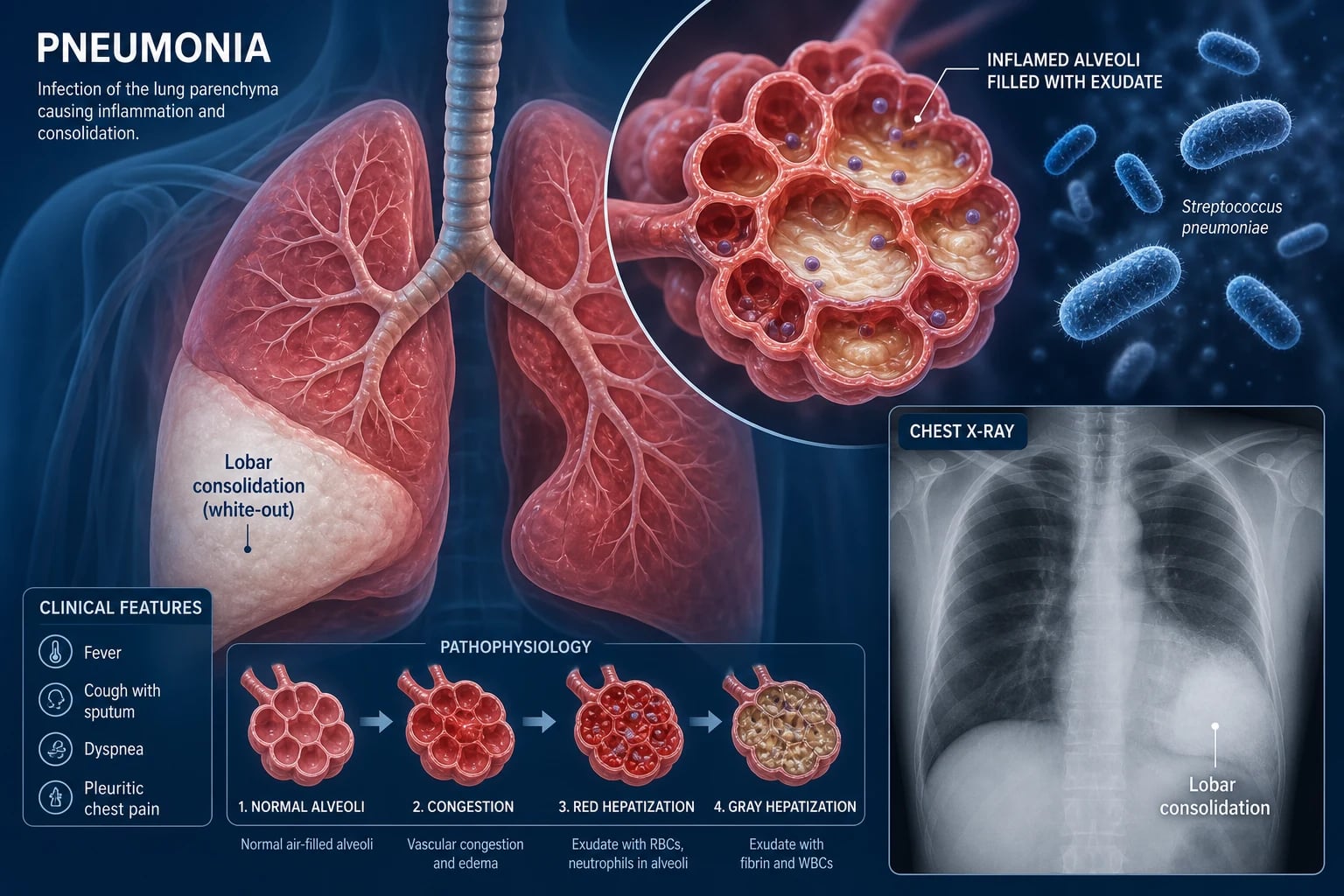
Pneumonia is an acute infection of the lung parenchyma (alveoli and distal airways) that produces cough, fever, purulent sputum, dyspnoea, and radiographic consolidation. It is one of the commonest reasons for hospital admission and a leading cause of infectious death worldwide. [1]
Three facts must land before everything else: [1]
- Severity determines everything. The first clinical decision is not which antibiotic — it is where to treat (home, ward, ICU). A validated severity score (CURB-65 or PSI) must be calculated at presentation. Missing severe pneumonia and sending a deteriorating patient home is a fatal and litigated error.
- The setting determines the organism, and the organism determines the antibiotic. Community-acquired pneumonia (CAP) is overwhelmingly Streptococcus pneumoniae, atypicals (Mycoplasma, Legionella, Chlamydia), and Haemophilus influenzae. Hospital-acquired and ventilator-associated pneumonia (HAP/VAP) shift toward Gram-negative bacilli, Pseudomonas aeruginosa, and MRSA. Empiric therapy must cover the likely organisms for that patient's setting.
- Empiric therapy is time-critical. In septic pneumonia, the first dose of antibiotics should be given within one hour of recognising sepsis. The IDSA/ATS 2019 guideline provides a clear, site-of-care-driven algorithm that works across ANZ, UK, and US practice [1].
Classification by setting
The classification system is not academic — it directly drives the empiric antibiotic choice. Organisms acquired in hospital are different (and more resistant) than those acquired in the community. [1]
Community-acquired pneumonia (CAP)
CAP is pneumonia contracted outside a hospital or healthcare facility, or diagnosed within 48 hours of admission. This is the default assumption for any adult presenting from the community with an acute respiratory infection and new consolidation. [1]
Hospital-acquired pneumonia (HAP)
HAP is pneumonia occurring 48 hours or more after hospital admission, not incubating at the time of admission. The organisms shift toward enteric Gram-negative bacilli (Klebsiella, E. coli, Enterobacter), Pseudomonas aeruginosa, and Staphylococcus aureus (including MRSA). The patient has been exposed to the hospital flora and is often colonised by the time pneumonia develops. [1]
Ventilator-associated pneumonia (VAP)
VAP is pneumonia arising more than 48 hours after endotracheal intubation. It is the most intensively studied form of nosocomial pneumonia because intubation bypasses the upper airway defences and the endotracheal tube becomes a biofilm-coated nidus for infection. Pseudomonas and MRSA are the high-yield pathogens to cover empirically. [1]
Aspiration pneumonia
Aspiration pneumonia follows inhalation of oropharyngeal or gastric contents into the lower airways. It occurs in patients with impaired consciousness (stroke, seizure, intoxication, anaesthesia), dysphagia (neurological disease, oesophageal obstruction), or impaired cough. The organisms are polymicrobial — a mix of anaerobes (Bacteroides, Peptostreptoccus, Fusobacterium) and oral aerobes (Streptococcus milleri). Lower lobe predominance is typical (the right lower lobe in the upright patient, posterior upper lobe or apical lower lobe in the supine patient). [1]
Distinguish aspiration pneumonia from chemical pneumonitis (Mendelson syndrome). Mendelson syndrome is an acute chemical lung injury from sterile gastric acid aspiration — it causes immediate bronchospasm, hypoxaemia, and CXR infiltrates within hours. Antibiotics are not given initially unless infection develops over 24-48 hours. Aspiration pneumonia, by contrast, is an established bacterial infection that does require antibiotics. This distinction is a classic MRCP and FRACP trap. [1]
Immunocompromised pneumonia
The immunocompromised host (HIV, transplant, chemotherapy, immunosuppression) is susceptible to opportunistic pathogens not seen in the immunocompetent: [1]
- Pneumocystis jirovecii (PJP) — CD4 count under 200 cells/microL in HIV; subacute dyspnoea, dry cough, hypoxia out of proportion to CXR, ground-glass opacity on CT
- Cytomegalovirus (CMV) — transplant and severely immunocompromised
- Aspergillus — neutropenia, transplant, prolonged steroids — cavitating or nodular lesions with halo sign
- Mycobacterium tuberculosis and atypical mycobacteria — advanced HIV, biologic therapy (TNF inhibitors)
- Encapsulated bacteria (pneumococcus, Haemophilus influenzae type b) — hyposplenism, HIV (impaired humoral immunity) [1]
Common organisms by setting
Typical bacterial pathogens in CAP
Streptococcus pneumoniae (pneumococcus) is the single most common cause of CAP in adults — approximately 30-50% of hospitalised cases. It is a Gram-positive lancet-shaped diplococcus. It classically causes lobar consolidation with a rigor at onset. Bacteraemia occurs in 10-25% of hospitalised pneumococcal pneumonia and carries a higher mortality. Pneumococcus is also the organism most likely to cause metastatic infection — meningitis, endocarditis, septic arthritis. [1]
Haemophilus influenzae is common in patients with COPD and chronic bronchitis. It is a Gram-negative coccobacillus; nontypeable strains cause most respiratory disease (the type b capsule is prevented by vaccination). [1]
Staphylococcus aureus pneumonia is less common but aggressive. Two patterns: (1) post-viral — classically after influenza, causing a severe necrotising pneumonia with cavitation and pneumatocoeles; (2) haematogenous — septic emboli from right-sided endocarditis (IV drug use) or from distant infection. Community-acquired MRSA (Panton-Valentine leukocidin strains) can cause rapidly progressive, cavitating, haemorrhagic pneumonia in young, previously well adults. [1]
Klebsiella pneumoniae (Friedlander pneumonia) classically causes a bulging fissure, upper lobe consolidation with cavitation, and thick 'currant jelly' sputum in alcoholics and diabetics. It is a classic exam organism even though pneumococcus is far more common in practice. [1]
Atypical pathogens
The atypicals share features: they are not visible on Gram stain (they lack a cell wall or are intracellular), they do not grow on standard culture media, and they cause a distinct syndrome that may have prominent extrapulmonary features. [1]
Mycoplasma pneumoniae is the commonest atypical, especially in young adults and in outbreak settings (schools, barracks). It causes a mild, protracted 'walking pneumonia' with dry cough, low-grade fever, and prominent constitutional symptoms (malaise, headache). Extrapulmonary manifestations are a high-yield exam topic: erythema multiforme (and Stevens-Johnson syndrome), bullous myringitis, haemolytic anaemia (cold agglutinins), pericarditis, myocarditis, neurological complications (meningoencephalitis, Guillain-Barre), and arthralgia. Cold agglutinin haemolysis occurs because Mycoplasma induces cross-reacting anti-I antibodies that agglutinate red cells at low temperatures. [1]
Legionella pneumophila causes a severe, distinctive pneumonia. Legionnaires' disease classically presents with a high fever (often over 40 degrees C), relative bradycardia, confusion, hyponatraemia (SIADH), diarrhoea, and elevated transaminases and creatine kinase. It is acquired from contaminated water sources — cooling towers, spas, hot water systems, showers. The Legionella urinary antigen test is a rapid bedside diagnostic for serogroup 1 (which causes most disease). Legionella is an intracellular pathogen — it replicates inside alveolar macrophages, which is why macrolides and fluoroquinolones (which achieve high intracellular concentrations) are effective, while beta-lactams are not. [1]
DWE high-yield: The Legionella urinary antigen detects only serogroup 1 (responsible for approximately 80% of community-acquired Legionella disease). A negative test does not exclude Legionella from other serogroups, though in practice serogroup 1 dominates clinical disease. [1]
Chlamydia pneumoniae (TWAR strain) causes atypical pneumonia clinically similar to Mycoplasma but milder. It is also epidemiologically associated with atherosclerosis, though causality is unproven. [1]
Pseudomonas in bronchiectasis and cystic fibrosis
Pseudomonas aeruginosa is not a typical CAP pathogen in the immunocompetent adult without lung disease. It becomes a key pathogen when there is structural lung disease — bronchiectasis, cystic fibrosis, severe COPD with frequent antibiotic exposure — or impaired immunity. Once Pseudomonas colonises bronchiectatic airways it is difficult to eradicate and drives a cycle of infective exacerbation and progressive lung damage. Empiric therapy in these patients must include anti-pseudomonal cover (piperacillin-tazobactam, ceftazidime, cefepime, or meropenem). [1]
PJP in HIV
Pneumocystis jirovecii pneumonia (PJP) is the AIDS-defining illness that every physician must recognise. The typical presentation is a subacute onset over days to weeks of progressive exertional dyspnoea, dry cough, and fever in a patient with a CD4 count under 200 cells/microL. The CXR may be normal early or show bilateral perihilar interstitial infiltrates. The chest CT shows ground-glass opacification even when the CXR is subtle. The diagnostic clue is hypoxia out of proportion to the CXR findings — the patient is desaturating on exertion with a near-normal radiograph. Diagnosis is by induced sputum or bronchoalveolar lavage with staining (immunofluorescence or Grocott methenamine silver) for the organism. Treatment is high-dose co-trimoxazole (trimethoprim-sulfamethoxazole); adjunctive corticosteroids are given if the PaO2 is less than 70 mmHg (9.3 kPa) or the alveolar-arterial gradient is widened, to reduce the inflammatory response to dying organisms. [1]
Pathophysiology
Pneumonia develops when microorganisms reach the sterile lower respiratory tract in numbers that overwhelm local defences. Four routes of inoculation: [1]
- Microaspiration of oropharyngeal flora — the dominant mechanism. Even healthy people microaspirate during sleep, but the cough reflex, mucociliary clearance, and alveolar macrophages clear it. Pneumonia develops when the inoculum is large, the organism is virulent, or the host defences are impaired.
- Inhalation of aerosolised droplets — the mechanism for Legionella, Mycobacterium tuberculosis, influenza, and most respiratory viruses.
- Haematogenous spread — septic emboli from endocarditis (Staphylococcus aureus) or thrombophlebitis.
- Direct extension — from a contiguous infection (rare; e.g. subdiaphragmatic abscess). [1]
Once organisms reach the alveoli, they provoke an inflammatory cascade. Alveolar macrophages release cytokines (TNF-alpha, IL-1, IL-6, IL-8) that recruit neutrophils. The alveoli fill with exudate rich in neutrophils, fibrin, and erythrocytes — this is the pathological substrate of consolidation and the source of purulent sputum. The cytokine response also produces the systemic features: fever, tachycardia, leukocytosis, and, if severe, septic shock from vasodilation and capillary leak. [1]
The intracellular pathogens (Legionella, Mycoplasma, Chlamydia) provoke a lymphocyte-predominant interstitial response rather than a neutrophilic alveolar exudate — which is why the CXR may show interstitial rather than lobar patterns, sputum may be scant, and Gram stain is unrevealing. [1]
Why does post-viral bacterial pneumonia occur? Influenza (and other respiratory viruses) damage the respiratory epithelium, impair mucociliary clearance, and alter alveolar macrophage function. This creates a window of vulnerability — typically 5-14 days after the viral illness — during which colonising bacteria (pneumococcus, Staphylococcus aureus, Haemophilus) invade the denuded mucosa. This is the pathophysiological basis for the increased pneumococcal and staphylococcal pneumonia seen during and after influenza seasons, and a key reason for influenza vaccination as a pneumonia-prevention strategy. [1]
Clinical presentation
Typical bacterial pneumonia
The classic presentation is acute onset of: [1]
- Cough — productive of purulent (yellow-green) sputum
- Fever — often with a shaking rigor (a rigor strongly suggests bacteraemia, typically pneumococcal)
- Dyspnoea — exertional, then at rest in severe cases
- Pleuritic chest pain — from pleural inflammation adjacent to the consolidation
- Systemic symptoms — malaise, anorexia, myalgia [1]
On examination, the patient looks unwell: tachypnoea, tachycardia, fever, and signs of consolidation if a lobe is involved (dullness to percussion, bronchial breath sounds, increased vocal resonance, crackles). Hypoxia is an ominous sign. [1]
Atypical pneumonia syndromes
The atypicals produce a more insidious onset with prominent constitutional and extrapulmonary features and a dry, non-productive cough. Sputum is scant (these organisms are not expectorated in purulent sputum). The CXR often looks worse than the patient in early Mycoplasma, or worse than expected in PJP. The distinction between 'typical' and 'atypical' syndromes is a useful heuristic but not reliable enough to guide therapy alone — the IDSA/ATS 2019 guideline no longer recommends separate empiric regimens for typical vs atypical cover, because the clinical overlap is too great [1].
Legionella — the pattern to recognise
Legionnaires' disease is the atypical pneumonia with the highest yield exam pattern. Look for the cluster of features that together is highly suggestive: [1]
- High fever (often over 40 degrees C) with relative bradycardia
- Confusion or encephalopathy (out of proportion to fever or hypoxia)
- Gastrointestinal symptoms — diarrhoea, nausea, abdominal pain
- Hyponatraemia (SIADH), often marked
- Elevated transaminases and creatine kinase
- Microscopic haematuria and mild renal impairment
- A history of exposure to aerosolised water (spa pool, cooling tower, recent travel with hotel stay) [1]
If this pattern appears, request the Legionella urinary antigen (detects serogroup 1) and ensure the empiric regimen includes a macrolide or respiratory fluoroquinolone — beta-lactams alone will not cover Legionella. [1]
Pneumonia in the elderly
Older patients may not mount a fever and may present atypically with confusion, falls, functional decline, or new incontinence as the only sign of infection. Tachypnoea is the most sensitive sign of pneumonia in the elderly — always count the respiratory rate. A CURB-65 score that includes confusion and age over 65 will already score 2 before any other feature. Do not be reassured by the absence of fever in an elderly patient with tachypnoea and a new infiltrate. [1]
Severity assessment
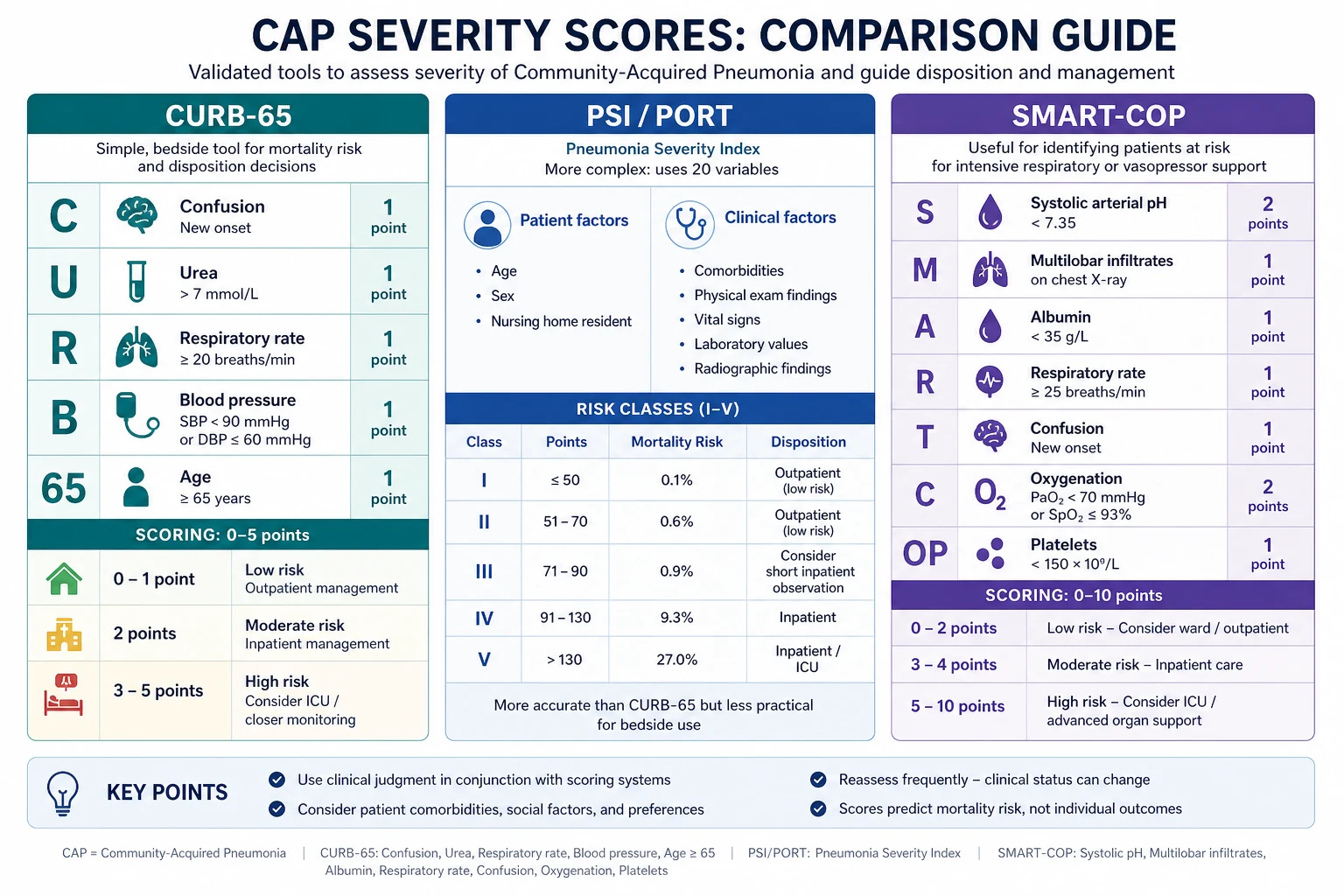
Severity assessment is the single most important clinical decision in pneumonia. It determines site of care (home, ward, ICU) and predicts mortality. The three validated scores answer slightly different questions. [1]
CURB-65
CURB-65 is the simplest and most widely used bedside score, derived by Lim et al. from the British Thoracic Society data [2]. It assigns one point each for:
| Letter | Feature | Criterion |
|---|---|---|
| C | Confusion | New disorientation in person, place, or time |
| U | Urea | Blood urea greater than 7 mmol/L (BUN greater than 20 mg/dL) |
| B | Blood pressure | Systolic under 90 mmHg or diastolic 60 mmHg or under |
| 65 | Age | 65 years or older |
Risk stratification and management: [1]
| Score | Risk | 30-day mortality | Recommended site |
|---|---|---|---|
| 0-1 | Low | 1.5% | Outpatient (consider short-stay for score 1 with comorbidity) |
| 2 | Moderate | 9.2% | Inpatient (ward) — consider hospital-at-home if available |
| 3-5 | High | 22-57% | Inpatient — consider ICU for score 4-5 |
DWE trap: CURB-65 predicts mortality, not ICU need. A patient with a CURB-65 of 2 may still need ICU if they have septic shock or respiratory failure. CURB-65 is a guide to admission, not to escalation. Use it alongside clinical judgement and the IDSA/ATS severe criteria for ICU decisions. [1]
CRB-65 omits the urea (no blood test needed) and is used in the community: any score of 1 or more warrants hospital assessment. [1]
Pneumonia Severity Index (PSI / PORT)
The PSI, derived by Fine et al., is a 20-variable prediction rule that estimates 30-day mortality and stratifies patients into five risk classes [3]. It is more accurate than CURB-65 at identifying low-risk patients suitable for outpatient care (Class I-II, mortality under 1%), but it is more complex and requires a calculator. It is particularly useful when CURB-65 gives a borderline score of 2 — a low PSI class can support outpatient management.
The PSI includes age, nursing home residency, five comorbidities (neoplastic disease, liver disease, CHF, cerebrovascular disease, renal disease), five physical examination findings (altered mental status, RR at least 30, SBP under 90, temperature under 35 or at least 40, pulse at least 125), and seven laboratory/radiographic findings (arterial pH under 7.35, BUN at least 11 mmol/L, sodium under 130, glucose at least 14, haematocrit under 30, PaO2 under 60 or SpO2 under 90, pleural effusion). Men get -10 (protective), as do women. [1]
Examiner point: The PSI underestimates severity in young patients — a 25-year-old with bacteraemic pneumococcal pneumonia, hypotension, and multilobar infiltrates may still calculate a low PSI because age dominates the score. Always interpret the PSI in clinical context. [1]
SMART-COP — predicting ICU need
SMART-COP, developed by Charles et al. in an Australian cohort, predicts the need for intensive respiratory or vasopressor support (IRVS) — a question CURB-65 and PSI answer poorly [4]. It is the preferred score in much of ANZ practice.
| Letter | Feature | Points |
|---|---|---|
| S | Systolic BP under 90 | 2 |
| M | Multilobar CXR involvement | 1 |
| A | Albumin under 35 g/L | 1 |
| T | Tachycardia at least 125 bpm | 1 |
| C | Confusion (acute) | 1 |
| O | Oxygen: PaO2 under 60, SpO2 under 90, or PaO2/FiO2 under 250 | 2 |
| P | Arterial pH under 7.35 | 2 |
Interpretation:
- Score 0-2 — low risk of needing IRVS
- Score 3-4 — moderate risk (approximately 20% need IRVS)
- Score 5-11 — high risk (approximately 60% need IRVS) [1]
A SMART-COP of 3 or more should prompt ICU outreach or admission assessment. The two-point items (low SBP, low oxygen, low pH) correctly weight the physiological features that actually predict the need for organ support. [1]
IDSA/ATS criteria for severe CAP
The 2007 IDSA/ATS guideline (retained in 2019) defines severe CAP as requiring ICU admission when at least one major criterion or at least three minor criteria are met [8]:
Major criteria:
- Invasive mechanical ventilation required
- Septic shock requiring vasopressors [1]
Minor criteria:
- Respiratory rate at least 30/min
- PaO2/FiO2 ratio 250 or less
- Multilobar infiltration
- Confusion/disorientation
- BUN at least 7 mmol/L (20 mg/dL) [1]- Leukopenia (under 4000 cells/microL from infection)
- Thrombocytopenia (platelets under 100,000)
- Hypothermia (core temperature under 36 degrees C)
- Hypotension requiring aggressive fluid resuscitation [1]
DCE long-case point: In your opening statement, state the CURB-65 score, the PSI class, and whether the IDSA/ATS severe criteria are met. This demonstrates you have rigorously assessed severity, not merely eyeballed the patient. In ANZ, add the SMART-COP score for ICU prediction. [1]
Investigations
Essential investigations for every hospitalised patient
| Investigation | Why |
|---|---|
| Chest X-ray | Confirms the diagnosis (consolidation), localises the lobe, detects effusion, assesses severity (multilobar). CAP is a clinical diagnosis but radiographic consolidation is the radiological hallmark. |
| Full blood count | Leukocytosis (or leukopenia — an IDSA/ATS minor severity criterion); platelets (thrombocytopenia = severity) |
| Urea and electrolytes | Urea is a CURB-65 component and a marker of dehydration/severity; renal function for antibiotic dosing |
| CRP | Supports the inflammatory diagnosis; a high CRP (over 100 mg/L) suggests bacterial infection; trends guide response |
| Blood cultures | Two sets before antibiotics if possible; positive in 10-25% of pneumococcal CAP; identifies the organism and its sensitivities |
| Arterial blood gas | If SpO2 under 92%, respiratory distress, or severe pneumonia — assesses oxygenation, ventilation, and acid-base |
| ECG | Baseline cardiac rhythm; tachyarrhythmia (especially atrial fibrillation) is common in sepsis; myocardial ischaemia may coexist |
Urinary antigen tests — rapid and high-yield
Pneumococcal urinary antigen detects the C-polysaccharide cell wall antigen common to all pneumococcal serotypes. It is rapid (results within hours), has a sensitivity of approximately 70-80% and specificity over 90% in adults with bacteraemic pneumococcal pneumonia. The IDSA/ATS 2019 guideline recommends it for severe CAP and inpatient CAP [1]. It is particularly useful when sputum culture is unobtainable or the patient has already received antibiotics (culture is suppressed but antigen persists).
Legionella urinary antigen detects serogroup 1 polysaccharide antigen. It is rapid, highly specific (over 95%), and reasonably sensitive (approximately 70-80%) for Legionella pneumophila serogroup 1, which causes the majority of clinical Legionnaires' disease. The IDSA/ATS 2019 guideline recommends it in severe CAP, and it should be specifically requested whenever the clinical syndrome suggests Legionella (high fever, confusion, GI symptoms, hyponatraemia, raised transaminases). [1]
Why urinary antigens over sputum culture? Speed and yield. Sputum culture takes 24-48 hours and is often contaminated by oral flora; Legionella does not grow on standard media. Urinary antigens give a same-day answer that can narrow therapy. But they detect only pneumococcus and Legionella serogroup 1 — they are not a replacement for sputum and blood cultures, which identify the full range of pathogens and their antibiotic sensitivities. [1]
Sputum culture and Gram stain
A good-quality expectorated sputum sample (before antibiotics, or as soon as possible) should be sent in:
- All hospitalised CAP patients who can produce a purulent sample (IDSA/ATS 2019: strong recommendation for severe CAP, conditional for non-severe inpatient CAP)
- Patients with a history of structural lung disease, prior antibiotic resistance, or alcoholism [1]
Gram stain guides interpretation: a predominant morphotype (e.g., Gram-positive lancet-shaped diplococci) supports pneumococcus. But Gram stain has limitations — atypicals are not visible, and oral flora contamination is common. [1]
Atypical serology and PCR
Mycoplasma is diagnosed by IgM (positive early, within the first week) or a fourfold rise in paired IgG titres 2-4 weeks apart (retrospective). PCR on respiratory specimens is increasingly available and more useful for acute diagnosis. Legionella can be cultured on specialised buffered charcoal yeast extract (BCYE) agar (slow, 3-5 days), diagnosed by urinary antigen (serogroup 1), or by a fourfold rise in antibody titre. [1]
These tests are mainly retrospective or confirmatory — empiric therapy should not await their results. [1]
Procalcitonin
Procalcitonin is a calcitonin precursor produced by extra-thyroidal tissues in response to bacterial infection (and suppressed in viral infection). It rises within 4-6 hours of bacterial challenge and falls with recovery. [1]
The patient-level meta-analysis by Schuetz et al. showed that procalcitonin-guided antibiotic decisions in acute respiratory infections safely reduced antibiotic exposure (mean 2.4 days shorter) and antibiotic-related adverse effects, with a trend to reduced mortality [7]. In practice:
- A low procalcitonin (under 0.1 microgram/L) on admission and at 6-24 hours supports not starting or early stopping antibiotics in low-severity presentations
- A high procalcitonin (over 0.5 microgram/L) supports bacterial infection and antibiotic initiation
- Serial procalcitonin (every 2-3 days) can guide the duration of therapy [1]
Examiner caveat: Procalcitonin is an adjunct to clinical judgement, not a replacement. Do not withhold antibiotics from a sick patient with a clinical diagnosis of bacterial pneumonia because the procalcitonin is low — false negatives occur (especially in early infection, with concurrent antibiotics, or in immunosuppression). Use it to support shorter courses, not to avoid treatment in the ill. [1]
CXR patterns and their pathogen associations
| CXR pattern | Likely pathogens |
|---|---|
| Unilateral lobar consolidation | Streptococcus pneumoniae (classic), Klebsiella |
| Patchy / bronchopneumonic | Staphylococcus aureus, Haemophilus influenzae, Gram-negatives |
| Bilateral interstitial | Atypicals (Mycoplasma, Chlamydia), viruses (influenza, COVID-19), PJP |
| Ground-glass opacity (CT) | PJP, viral pneumonitis, organising pneumonia |
| Cavitation | Staphylococcus aureus, Klebsiella, anaerobes (aspiration), tuberculosis, fungal (Aspergillus) |
| Pneumatocoeles | Staphylococcus aureus (especially PVL strains), PJP |
| Pleural effusion | Any — assess for parapneumonic effusion / empyema |
| Bulging fissure | Klebsiella (classic but uncommon) |
| Rapidly progressive multilobar | Influenza with bacterial superinfection, Legionella, Staphylococcus aureus, SARS-CoV-2 |
Empiric antibiotic therapy
The empiric regimen is determined by site of care and risk factors for resistant organisms. The IDSA/ATS 2019 guideline is the primary reference [1]; the BTS and NICE guidelines are broadly concordant, with regional differences in macrolide resistance and preferred fluoroquinolones.
Outpatient CAP
| Patient group | Recommended regimen |
|---|---|
| No comorbidities or risk factors for resistance | Amoxicillin 1 g orally three times daily (doxycycline 100 mg BID or a macrolide — azithromycin 500 mg then 250 mg daily — if penicillin-allergic or for atypical cover) |
| With comorbidities (chronic heart, lung, liver, or renal disease; diabetes; alcoholism; malignancy; asplenia) | Amoxicillin/clavulanate 875/125 mg BID OR a cephalosporin (cefpodoxime, cefuroxime) PLUS a macrolide (azithromycin) OR doxycycline; OR a respiratory fluoroquinolone (moxifloxacin 400 mg daily, levofloxacin 750 mg daily) as monotherapy |
DWE high-yield — why amoxicillin first in uncomplicated outpatient CAP? Pneumococcus is the target organism, and amoxicillin achieves high respiratory concentrations and covers penicillin-sensitive and most intermediately-resistant pneumococci at standard doses. Macrolide monotherapy is unreliable in regions with pneumococcal macrolide resistance exceeding 25% (much of the world, including parts of ANZ). The IDSA/ATS 2019 guideline therefore prefers amoxicillin, with a macrolide or doxycycline added or substituted for atypical cover. [1]
Inpatient (non-severe) CAP — ward
| Setting | Recommended regimen |
|---|---|
| General medical ward | Ceftriaxone 1 g IV daily (or ampicillin 1-2 g IV QID, or cefotaxime) PLUS azithromycin 500 mg IV or orally daily; OR a respiratory fluoroquinolone (moxifloxacin 400 mg IV/oral daily, levofloxacin 750 mg IV/oral daily) as monotherapy |
The beta-lactam plus macrolide combination is preferred because it covers both typical (pneumococcus) and atypical (Mycoplasma, Legionella, Chlamydia) pathogens. Observational data consistently show lower mortality with combination therapy than with beta-lactam monotherapy in hospitalised CAP, possibly because of the atypical cover and the anti-inflammatory effect of macrolides. [1]
Severe CAP — ICU
| Setting | Recommended regimen |
|---|---|
| ICU without risk factors for Pseudomonas/MRSA | Beta-lactam (piperacillin-tazobactam 4.5 g IV TDS, cefepime 2 g IV TDS, or ceftriaxone 2 g IV daily) PLUS a macrolide (azithromycin 500 mg IV daily); OR a beta-lactam plus a respiratory fluoroquinolone (moxifloxacin or levofloxacin) |
| With risk factors for Pseudomonas (bronchiectasis, CF, recent hospitalisation, prior isolation) | Anti-pseudomonal beta-lactam (piperacillin-tazobactam, cefepime, ceftazidime, or meropenem) PLUS an anti-pseudomonal agent if not using two anti-pseudomonals (e.g., add ciprofloxacin or an aminoglycoside) PLUS azithromycin or a fluoroquinolone for atypical cover |
| With risk factors for MRSA (post-influenza, cavitating infiltrates, recent IV antibiotics, endocarditis risk) | Add vancomycin 15-20 mg/kg IV Q12H (or linezolid 600 mg IV BID) |
DWE high-yield — the severe CAP regimen must always cover atypicals. Even in ICU, the regimen should include a macrolide or fluoroquinolone for Legionella and Mycoplasma. Beta-lactam monotherapy is inadequate for severe CAP. The mortality benefit of macrolide-containing regimens in severe CAP is one of the most consistently reproduced findings in the pneumonia literature. [1]
Special situations
Aspiration pneumonia — cover anaerobes: amoxicillin-clavulanate (or clindamycin plus a beta-lactam, or piperacillin-tazobactam for hospitalised patients). Metronidazole alone is inadequate as it misses the aerobic oral streptococci that are often co-pathogens. [1]
PJP (HIV) — co-trimoxazole (trimethoprim 15-20 mg/kg/day + sulfamethoxazole 75-100 mg/kg/day in divided doses IV or orally for 21 days). Add prednisolone 40 mg BID (tapering) if PaO2 under 70 mmHg or A-a gradient over 35 mmHg, started within 72 hours, to reduce the inflammatory response to dying organisms. [1]
Suspected Legionella — ensure the regimen includes a macrolide (azithromycin) or respiratory fluoroquinolone (moxifloxacin/levofloxacin). Fluoroquinolones may be slightly more effective in severe Legionella. Duration is 5-10 days for azithromycin, 14-21 days for fluoroquinolones or in immunocompromised. [1]
Duration of therapy
The IDSA/ATS 2019 guideline recommends treating CAP for a minimum of 5 days, continuing until the patient is clinically stable (afebrile for 48-72 hours, normalising vital signs) and able to tolerate oral therapy [1]. For most patients with uncomplicated CAP, this means 5-7 days total.
Factors that extend duration:
- Bacteraemic pneumococcal pneumonia — 7-14 days (ensure source control, repeat cultures)
- Legionella — 5-10 days (azithromycin) or 14-21 days (fluoroquinolone, or immunocompromised)
- Staphylococcus aureus pneumonia — 14-21 days (longer if endocarditis or metastatic infection)
- PJP — 21 days
- Complicated pneumonia — empyema, lung abscess, metastatic infection — individualise, often 2-6 weeks [1]
DWE high-yield: Duration should be guided by clinical stability, not an arbitrary day count. The evidence consistently shows that shorter courses (5-7 days) are as effective as longer courses for uncomplicated CAP and reduce resistance, C. difficile, and adverse effects. Procalcitonin-guided stopping (Schuetz meta-analysis) safely shortens courses further [7].
Corticosteroid adjunct in severe CAP
The role of adjunctive corticosteroids in CAP has been clarified by the Blum et al. multicentre RCT and the Siemieniuk et al. systematic review [5] [6].
Blum et al. (Lancet 2015): Prednisone 50 mg orally daily for 7 days, versus placebo, in 785 hospitalised CAP patients. Prednisone shortened time to clinical stability by approximately 1.5 days (hazard ratio 1.38). There was a non-significant trend to reduced mortality. Adverse effects were modest — more hyperglycaemia requiring insulin, but no increase in infection, GI bleeding, or psychiatric events. [1]
Siemieniuk et al. (Ann Intern Med 2015) meta-analysis of 13 RCTs (approximately 2000 patients): Corticosteroids reduced mortality (RR 0.67), reduced the need for mechanical ventilation (RR 0.45), reduced ARDS (RR 0.24), and shortened time to stability and length of stay. The benefit was driven by the severe CAP subgroup. Hyperglycaemia was increased (RR 1.49) but there was no increase in GI haemorrhage. [1]
Practical recommendation:
- Consider prednisone 50 mg daily for 7 days (or hydrocortisone 200 mg/day IV if unable to take oral) in hospitalised CAP with severe disease — CURB-65 at least 3, PSI class IV-V, or meeting IDSA/ATS severe criteria [1]- The benefit is greatest in severe CAP; the role in mild-moderate CAP is less clear
- Avoid in patients in whom corticosteroids are harmful — uncontrolled diabetes, active GI bleeding, recent surgery — or use with caution
- The ATS/IDSA 2019 guideline suggests corticosteroids may be considered in severe CAP but does not mandate them; NICE and the BTS are more cautious [1]
Examiner point: Be able to discuss the evidence (Blum, Siemieniuk) and the regimen (prednisone 50 mg daily for 7 days). State the benefit (faster clinical stability, reduced mechanical ventilation and possibly mortality in severe CAP) and the main harm (hyperglycaemia). This is a modern, evidence-rich topic that examiners love. [1]
Complications
Parapneumonic effusion and empyema
Pleural effusion complicates up to 40% of bacterial pneumonia. The spectrum runs from simple (uncomplicated) parapneumonic effusion (sterile, clear, free-flowing) through complicated parapneumonic effusion (infected but not yet purulent, often loculated, with a falling pH and glucose, rising LDH) to frank empyema (frank pus in the pleural space). [1]
Diagnosis is by diagnostic thoracentesis whenever an effusion is more than 10 mm on lateral decubitus CXR or ultrasound, especially if the patient is not responding to antibiotics. Send pleural fluid for pH (or glucose if pH unavailable), protein, LDH, cell count, Gram stain, and culture. [1]
Light's criteria for an exudate: protein ratio (pleural/serum) over 0.5, LDH ratio over 0.6, or LDH over two-thirds the upper limit of normal for serum. [1]
Management principles (the Light classification):
- Category 1-2 (minimal, free-flowing, pH over 7.20) — antibiotics alone, no drainage
- Category 3 (complicated — pH 7.0-7.20, loculated, or positive culture) — tube thoracostomy (chest drain) plus antibiotics; consider intrapleural fibrinolytics (tPA/DNase) if loculated
- Category 4 (empyema — pH under 7.0, or frank pus) — chest drain plus fibrinolytics or surgical drainage (VATS) [1]
DCE long-case trap: A patient with CAP who is not improving after 48-72 hours of appropriate antibiotics must be re-evaluated for a parapneumonic effusion or empyema. Get a lateral decubitus film or a pleural ultrasound, perform thoracentesis, and drain if the fluid is infected. Missing an empyema is a common and serious error. [1]
Lung abscess
A lung abscess is a localised collection of pus within the lung parenchyma, usually from aspiration of anaerobic oral flora or from necrotising infection (Staph aureus, Klebsiella, anaerobes). It presents with a swinging fever, foul-smelling sputum (anaerobes), weight loss, and an air-fluid level on CXR/CT within a cavitating lesion. [1]
Management: prolonged antibiotics (4-6 weeks) covering anaerobes (clindamycin or amoxicillin-clavulanate, or piperacillin-tazobactam), with percutaneous or surgical drainage for large or unresponsive abscesses. Exclude an underlying bronchial obstruction (foreign body, tumour) that may have caused the abscess. [1]
ARDS
Severe pneumonia (especially viral, Legionella, and pneumococcal) can progress to acute respiratory distress syndrome (ARDS) — bilateral pulmonary infiltrates, severe hypoxaemia (PaO2/FiO2 under 300), and non-cardiogenic pulmonary oedema. Management is lung-protective mechanical ventilation (tidal volume 6 mL/kg predicted body weight, plateau pressure under 30 cmH2O), prone positioning, and treatment of the underlying infection. [1]
Metastatic infection
Pneumococcal bacteraemia can seed distant sites. Always look for:
- Meningitis — headache, photophobia, neck stiffness, altered consciousness; perform LP if suspected (after CT if focal signs or obtunded)
- Endocarditis — new murmur, embolic phenomena, positive blood cultures; echocardiogram
- Septic arthritis — hot, swollen joint
- Peritonitis — especially in peritoneal dialysis patients or ascites [1]
The constellation of pneumonia, meningitis, and endocarditis is Austrian's triad (pneumococcal) — rare but classic and highly lethal. [1]
Prevention
Pneumococcal vaccination
Two pneumococcal vaccines are available for adults: [1]
- PCV (pneumococcal conjugate vaccine) — PCV13, PCV15, PCV20 — conjugates polysaccharide antigens to a carrier protein, producing a T-cell-dependent response that works in infants and immunocompromised hosts and generates immunological memory
- PPSV23 (pneumococcal polysaccharide vaccine) — 23-valent; covers more serotypes but produces a T-cell-independent response without memory [1]
Adult schedule (general principle, follow local guidance):
- Immunocompetent adults aged 65+ — a PCV followed by PPSV23 (timing per local guidance; at least 1 year apart)
- Immunocompromised, asplenic, CSF leak, cochlear implant — a PCV followed by PPSV23 at least 8 weeks later, then a PPSV23 booster at 5 years
- The newer PCV15 and PCV20 simplify the schedule (PCV20 alone may replace the PCV-then-PPSV23 sequence) [1]
Influenza vaccination
Annual influenza vaccination is recommended for all adults (and is the standard of care in those over 65, pregnant, or with chronic disease). Influenza vaccination reduces both viral pneumonia and post-influenza bacterial pneumonia (pneumococcal and staphylococcal) by reducing the epithelial damage that predisposes to bacterial invasion. [1]
Smoking cessation and other measures
- Smoking cessation — smoking impairs mucociliary clearance and alveolar macrophage function and is a major risk factor for pneumococcal pneumonia. Cessation reduces CAP risk substantially.
- COVID-19 vaccination — reduces viral and secondary bacterial pneumonia
- Good oral hygiene — reduces oropharyngeal colonisation with respiratory pathogens, especially in aged care
- PCP prophylaxis — co-trimoxazole in HIV with CD4 under 200, transplant patients on high immunosuppression, and certain haematology patients
- Aspiration precautions — head of bed elevation, swallowing assessment, oral care in stroke and ICU patients [1]
DCE long-case approach
Opening statement (SASPOP)
'Mrs Patel is a 72-year-old retired teacher who presents with a 3-day history of fever, rigors, productive cough with rusty sputum, and progressive dyspnoea. She was brought to the emergency department after becoming confused at home. She is a 40 pack-year smoker with COPD and type 2 diabetes. [1]
On arrival she was confused, tachypnoeic at 32 per minute, with a blood pressure of 88/52, oxygen saturation of 88% on room air, and a temperature of 38.9 degrees. Her CXR showed right middle and lower lobe consolidation with a small right pleural effusion. Her CURB-65 score is 4, PSI is class V, and she meets the IDSA/ATS criteria for severe CAP. Blood cultures grew Streptococcus pneumoniae. [1]
Her main problems are:
- Severe bacteraemic pneumococcal CAP with septic shock — immediate threat
- A parapneumonic effusion requiring assessment for drainage
- COPD and type 2 diabetes — modifying her management and prognosis
- Ongoing smoking — a key modifiable risk factor for future pneumonia
- Functional decline and need for rehabilitation [1]
Integrated management plan
- Immediate (first hour): Sepsis Six — oxygen to target SpO2 94-98% (88-92% if CO2 retention risk from COPD), two large-bore IV cannulae, 30 mL/kg crystalloid for hypotension, blood cultures, IV ceftriaxone 2 g plus azithromycin 500 mg within the hour, lactate, urine output monitoring. Assess for vasopressors (noradrenaline) if fluid-refractory shock. [1]2. Respiratory: Assess oxygenation and ventilatory need. If PaO2/FiO2 under 250, consider ICU for non-invasive or invasive ventilation. Reassess for the parapneumonic effusion with ultrasound — diagnostic thoracentesis; drain if pH under 7.2 or frank pus.
- Corticosteroids: She has severe CAP (CURB-65 4, septic shock) — start prednisone 50 mg daily for 7 days (or hydrocortisone 200 mg/day IV) per the Blum and Siemieniuk evidence, monitoring blood glucose closely given her diabetes.
- Antibiotic de-escalation: Once sensitivities are known, continue ceftriaxone (pneumococcus sensitive) for a total of 7-10 days. Stop azithromycin if no atypical identified (continue if Legionella suspected).
- COPD and diabetes: Continue inhaled therapy; monitor blood glucose (steroids will raise it — may need insulin sliding scale); renal function for antibiotic dosing.
- Prevention and follow-up: Smoking cessation counselling and pharmacotherapy (varenicline or NRT); pneumococcal and influenza vaccination at discharge; repeat CXR at 6 weeks to ensure resolution and exclude an underlying lesion (especially bronchial obstruction in a smoker). [1]
DCE short-case approach: respiratory examination
Instruction: 'Examine this patient's respiratory system.' [1]
Key signs of consolidation
- Inspection: tachypnoea, use of accessory muscles, cyanosis (if hypoxaemic), splinting of the affected side with respiration
- Palpation: reduced chest expansion on the affected side; increased tactile vocal fremitus over consolidation (consolidated lung transmits vibration better than air-filled lung); trachea central (unless large effusion or collapse causes shift)
- Percussion: dullness over the consolidated area (fluid/solid tissue conducts sound less well than air)
- Auscultation: bronchial breath sounds (the pathognomonic sign — consolidated lung transmits tracheobronchial breath sounds to the periphery), coarse crackles (from exudate in airways), increased vocal resonance (with bronchophony, egophony 'e-to-a' change, and whispered pectoriloquy); a pleural rub may be present if the pleura is involved [1]
If a pleural effusion is present: reduced chest expansion, stenotic (absent) breath sounds, reduced vocal resonance (the fluid blocks transmission), stony dull percussion note. [1]
Presentation template
'I examined Mrs Patel's respiratory system. She is tachypnoeic at 28 per minute, using accessory muscles, and appears breathless at rest. There is central cyanosis. She is not clubbed. [1]
The trachea is central. Chest wall expansion is reduced on the right. On the right lower zone posteriorly, there is dullness to percussion. Tactile vocal fremitus is increased in this area. On auscultation, there are bronchial breath sounds, coarse inspiratory crackles, and increased vocal resonance with whispered pectoriloquy over the right lower lobe. There are no wheezes. [1]
In summary, these findings are consistent with right lower lobe consolidation, in keeping with a community-acquired pneumonia.' [1]
Examiner: 'What is the significance of bronchial breath sounds?' — Bronchial breath sounds heard at the periphery indicate that consolidated lung tissue is conducting the tracheobronchial breath sounds outward. Normal peripheral breath sounds are vesicular (soft, low-pitched, with a longer inspiratory than expiratory phase). The presence of bronchial breathing over an area of dullness and crackles is the auscultatory hallmark of consolidation — it has a high positive likelihood ratio for lobar pneumonia. [1]
Key DWE MCQ patterns
- Severity scoring: CURB-65 of 3 or more — admit, consider ICU. Know the five components cold.
- Outpatient antibiotic choice: Amoxicillin for uncomplicated CAP; amoxicillin-clavulanate or cephalosporin plus macrolide (or respiratory fluoroquinolone) for comorbid patients.
- Severe CAP regimen: Beta-lactam (pip-tazo or cefepime or ceftriaxone) plus macrolide or fluoroquinolone — never beta-lactam alone in ICU.
- Legionella clues: High fever, confusion, diarrhoea, hyponatraemia, raised LFTs/CK — urinary antigen covers serogroup 1.
- Post-influenza pneumonia: Staphylococcus aureus (cavitation, pneumatocoeles) — add vancomycin/linezolid.
- PJP pattern: HIV, CD4 under 200, subacute dyspnoea, dry cough, hypoxia out of proportion to CXR, ground-glass on CT — co-trimoxazole plus steroids if hypoxic.
- Duration: Minimum 5 days, until clinically stable. Procalcitonin can guide stopping.
- Parapneumonic effusion not improving: Thoracentesis — drain if pH under 7.2.
- Corticosteroids in severe CAP: Prednisone 50 mg daily for 7 days — faster stability, less mechanical ventilation. [1]
References
[1] Metlay JP, et al. ATS/IDSA 2019 Clinical Practice Guideline — Diagnosis and Treatment of Adults with CAP. Am J Respir Crit Care Med 2019. The current primary guideline; site-of-care-driven empiric therapy, severity assessment, duration, and de-escalation principles. [2] Lim WS, et al. Defining CAP severity on presentation to hospital: CURB-65. Thorax 2003. The derivation and validation of the CURB-65 score; 30-day mortality from 0.7% (score 0) to 57% (score 5). [3] Fine MJ, et al. A prediction rule to identify low-risk patients with CAP (PSI/PORT). NEJM 1997. The 20-variable PSI stratifying patients into five risk classes by 30-day mortality. [4] Charles PGP, et al. SMART-COP: predicting the need for intensive respiratory or vasopressor support in CAP. Clin Infect Dis 2008. An Australian-derived score predicting ICU need; a score of 3 or more identifies most patients requiring IRVS. [5] Siemieniuk RAC, et al. Corticosteroid therapy for patients hospitalized with CAP: a systematic review and meta-analysis. Ann Intern Med 2015. Corticosteroids reduced mortality (RR 0.67), mechanical ventilation (RR 0.45), and ARDS (RR 0.24) in severe CAP. [6] Blum CA, et al. Adjunct prednisone therapy for patients with CAP: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2015. Prednisone 50 mg daily for 7 days shortened time to clinical stability by approximately 1.5 days. [7] Schuetz P, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis. Lancet Infect Dis 2018. Procalcitonin guidance safely reduced antibiotic exposure by a mean of 2.4 days with a trend to reduced mortality. [8] Mandell LA, et al. IDSA/ATS consensus guidelines on the management of CAP in adults. Clin Infect Dis 2007. Defined the severe CAP minor/major criteria for ICU admission retained in the 2019 update.
ATS/IDSA 2019 Guideline; NICE CG191; BTS CAP Guidelines; Therapeutic Guidelines (Australia) — Antibiotic. [1]
References
- [1]Metlay JP, Waterer GW, Long AC, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America Am J Respir Crit Care Med, 2019.PMID 31573350
- [2]Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study Thorax, 2003.PMID 12728155
- [3]Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med, 1997.PMID 8995086
- [4]Charles PGP, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia Clin Infect Dis, 2008.PMID 18558884
- [5]Siemieniuk RAC, Meade MO, Alonso-Coello P, et al. Corticosteroid Therapy for Patients Hospitalized With Community-Acquired Pneumonia: A Systematic Review and Meta-analysis Ann Intern Med, 2015.PMID 26258555
- [6]Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial Lancet, 2015.PMID 25608756
- [7]Schuetz P, Wirz Y, Sager R, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis Lancet Infect Dis, 2018.PMID 29037960
- [8]Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis, 2007.PMID 17278083